Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
|
|
|
- Sybil Sharp
- 5 years ago
- Views:
Transcription
1 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1. Disorder of ventilation 1.1 Decreased ventilatory drive - oversedation - CNS problems 1.2 Obstructed ventilation - bronchospasm - dislodgement of ET tube - mucus plugging of airways or ET tube 1
2 Causes of oxygen desaturation 2. Disorder of oxygenation 2.1 pulmonary causes - ARDS - pneumonia, atelectasis - pneumothorax - pulmonary embolus - aspiration pneumonitis Causes of oxygen desaturation 2. Disorder of oxygenation 2.2 Non-pulmonary causes - iatrogenic fluid overload - heart failure 3. Effects on interventions, procedures - chest physical therapy, endotracheal suctioning - changes in body positioning - peritoneal dialysis, hemodialysis - thoracocentesis Causes of oxygen desaturation 5. Medication - bronchodilators - vasodilators -β-blockers 6. Ventilator-related problems - ventilator circuit - function of ventilator itself - inappropriate ventilator settings 2
3 Management desaturation 1. Increased FiO 2 to 100% 2. Check ET tube (obstruction, dislodgement) 3. Briefly physical examination unilateral decreased breath sounds suggest pneumothorax or right main stem bronchus intubation distended neck vein with bilateral lung crackles suggest volume overload Management desaturation 3. Briefly physical examination wheezing represents bronchospasm (can be associated with cardiogenic problems) decreased mental status suggests hypoventilation 4. If cause is not obvious, manually ventilate patient with 100% O 2 to exclude ventilator malfunction Management desaturation 5. Treat underlying cause 6. Alter ventilator settings to improve oxygenation (increase PEEP) 7. CXR (if the cause is still not clear) 3
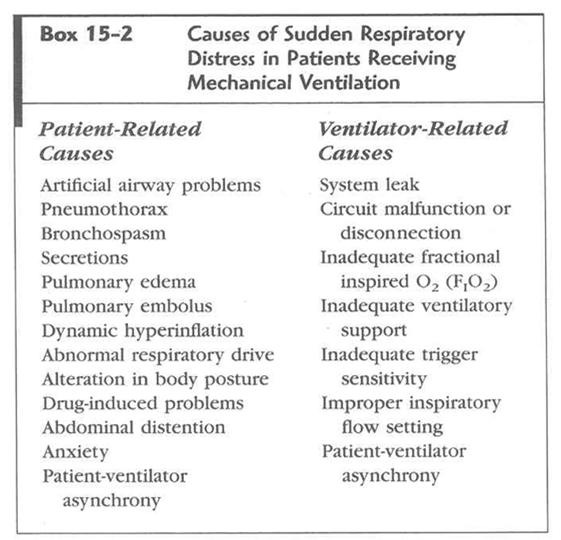
4 Patient fighting ventilator Fighting ventilator acute respiratory distress Patient and ventilator are breathing out of synchrony (patient shows signs and symptoms of acute respiratory distress, multiple ventilator alarms eg. low tidal volume, high pressure alarm or low pressure alarm, hemodynamic instability, cardiac rhythm changes and abnormal gas exchange) * Physiological effects of patient ventilator dyssynchrony 1. Discomfort 2. Increased work of breathing 3. Increased oxygen consumption 4. Increased minute ventilation 5. Increased cardiac work 6. Respiratory muscle fatigue 4
5 5
6 Patient s expression of fear, feeling of panic can be explored by using direct questions that patient can answer with head nodding or pointing. Primary goal of management - to ensure adequate ventilation / oxygenation and to prevent complications of mechanical ventilation, eg. barotrauma, reduction CO Steps in the management sudden respiratory distress in patients receiving mechanical ventilation 1. Remove patient from ventilator 2. Manual ventilation using self-inflating resuscitation bag containing 100% O 2 (if patient s distress goes away, problem is in ventilator - check circuit for air leaks or condensation that accumulated, adjust setting) Steps in the management sudden respiratory distress in patients receiving mechanical ventilation 2. Manual ventilation using self-inflating resuscitation bag containing 100% O 2 (if distress does not go away, problem is in the patient) 3. rapid physical examination, check cuff pressure 4. assess monitored indices, alarm and graphic waveform 6
7 7
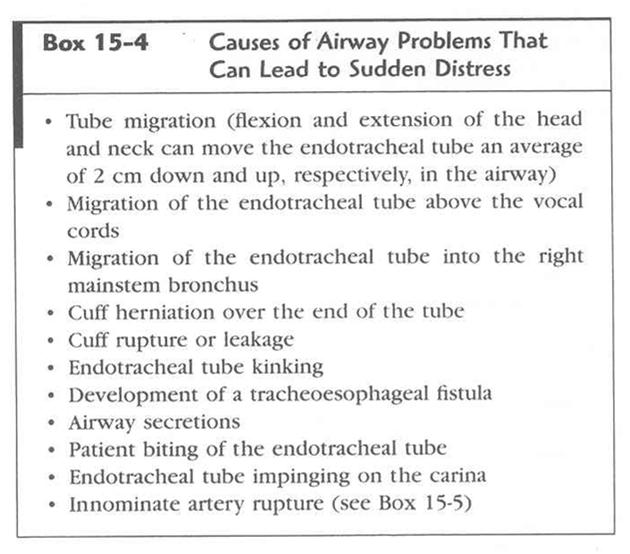
8 Pressure-volume, flow-volume loops: Expiratory volume curve does not go to zero leak in the system Steps in the management sudden respiratory distress in patients receiving mechanical ventilation 5. Check patency of airway, pass suction catheter if catheter cannot pass biting on the tube, obstruction ET tube if obstruction cannot be cleared, ET tube must be removed, mask ventilation until reintubation Steps in the management sudden respiratory distress in patients receiving mechanical ventilation 6. If death appears imminent, consider and treat most likely causes: pneumothorax, airway obstruction (needle inserted into second intercostal space at mid-clavicular line, followed by tube thoracostomy) 7. Once patient is stabilized, perform more detailed assessment and management 8
9 Steps in the management sudden respiratory distress in patients receiving mechanical ventilation 8. Some patient-ventilator dyssynchrony may result from patient s feeling of panic, fear or pain - manually ventilating, instructing how to relax while breathing with ventilator on adjunctive therapy with sedation, analgesic Type of patient ventilator dyssynchrony 1. Trigger dyssynchrony - difficult to trigger ventilator to initiate inspiration Causes 1.1 insensitive trigger high trigger threshold 1.2 autopeep 2. Flow dyssynchrony - ventilator flow not match patient s flow need (VC mode) 9
10 Type of patient ventilator dyssynchrony 3. Termination dyssynchrony - Patient s inspiratory time and ventilator inspiratory time not coincide Causes 3.1 premature breath termination 3.2 delayed breath termination 4. Expiratory dyssynchrony - Due to shortened or prolonged expiratory time, patient s effort during expiration Respiratory acidosis * ph < 7.35 with PaCO 2 > 45 mm Hg 10
11 Hypotension 11
12 Causes of hypotension soon after initiation mechanical ventilation 1. Relative hypovolemia application positive pressure ventilation intrathoracic pressure venous return, preload, cardiac output Causes of hypotension soon after initiation mechanical ventilation 2. Drug induced vasodilatation and myocardial depression 3. Gas trapping (dynamic hyperinflation) 4. Tension pneumothorax Management hypotension - Treat loss vascular tone - vasoconstrictors - Treat lowered stroke volume fluid bolus - Hypotension due to relative hypovolemia or anesthetic induction agents responds rapidly to fluid - Gas trapping disconnecting - Tension pneumothorax chest tube insertion 12
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR
 CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
CAE Healthcare Human Patient Simulator (HPS)
") CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
Capnography (ILS/ALS)
") Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
EMS System for Metropolitan Oklahoma City and Tulsa 2017 Medical Control Board Treatment Protocols
 S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Ventilator curves. Fellowonderwijs 2 feb 2012
 Ventilator curves Fellowonderwijs 2 feb 2012 Mechanical ventilation Supported Ventilator affects patients respiratory drive Monitor interaction patient - ventilator Controlled Monitor interatcion patient
Ventilator curves Fellowonderwijs 2 feb 2012 Mechanical ventilation Supported Ventilator affects patients respiratory drive Monitor interaction patient - ventilator Controlled Monitor interatcion patient
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
and Noninvasive Ventilatory Support
 Chapter 2 Mechanical Ventilation and Noninvasive Ventilatory Support Megan L. Anderson and John G. Younger PERSPECTIVE Invasive and noninvasive ventilation are essential tools for treatment of critically
Chapter 2 Mechanical Ventilation and Noninvasive Ventilatory Support Megan L. Anderson and John G. Younger PERSPECTIVE Invasive and noninvasive ventilation are essential tools for treatment of critically
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
CAE Healthcare istan. Neurological Features Anatomy, Physiology and Clinical signs
 CAE Healthcare istan NYSIM has two wireless istans available for your sessions. We also have them preprogrammed with the NLN Nursing These are available for you to review at the NYSIM Center. They can
CAE Healthcare istan NYSIM has two wireless istans available for your sessions. We also have them preprogrammed with the NLN Nursing These are available for you to review at the NYSIM Center. They can
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital
 Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Therapist Written RRT Examination Detailed Content Outline
 I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
Adult Intubation Skill Sheet
 Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
An introduction to mechanical ventilation. Fran O Higgins, Adrian Clarke Correspondence
 Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
COMMISSION ON ACCREDITATION FOR RESPIRATORY CARE TMC DETAILED CONTENT OUTLINE COMPARISON
 A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Post-Anesthesia Care In the ICU
 Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Post-Anesthesia Care In the ICU The following is based on current research and regional standards of care. At completion you will be able to identify Basic equipment needed at the bedside. Aldrete scoring
Troubleshooting of Nursing Practice for Mechanically Ventilated Patients
 Troubleshooting of Nursing Practice for Mechanically Ventilated Patients *1 Dr. Hanan Mohammed Mohammed, 2 Dr. Abeer El-Said Hassan 1 Assistant Professor of Medical-Surgical Nursing Department, Faculty
Troubleshooting of Nursing Practice for Mechanically Ventilated Patients *1 Dr. Hanan Mohammed Mohammed, 2 Dr. Abeer El-Said Hassan 1 Assistant Professor of Medical-Surgical Nursing Department, Faculty
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL
 PROTOCOL") AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Bronchoscopy SICU Protocol
 Bronchoscopy SICU Protocol Updated January 2013 Outline Clinical indications Considerations Preparation Bronchoscopy technique Bronchoalveolar Lavage (BAL) Post-procedure Purpose Bronchoscopy is a procedure
Bronchoscopy SICU Protocol Updated January 2013 Outline Clinical indications Considerations Preparation Bronchoscopy technique Bronchoalveolar Lavage (BAL) Post-procedure Purpose Bronchoscopy is a procedure
Asthma Management in ICU. by DrGary Au From KWH
 Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Practical Application of CPAP
 CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Ventilator Dyssynchrony - Recognition, implications, and management
 Ventilator Dyssynchrony - Recognition, implications, and management Gavin M Joynt Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong Dyssynchrony Uncoupling of mechanical delivered
Ventilator Dyssynchrony - Recognition, implications, and management Gavin M Joynt Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong Dyssynchrony Uncoupling of mechanical delivered
Protocol for performing chest clearance techniques by nursing staff
 Protocol for performing chest clearance techniques by nursing staff Rationale The main indications for performing chest clearance techniques (CCT) are to assist in the removal of thick, tenacious secretions
Protocol for performing chest clearance techniques by nursing staff Rationale The main indications for performing chest clearance techniques (CCT) are to assist in the removal of thick, tenacious secretions
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
EMS Subspecialty Certification Review Course. Learning Objectives. Upon the completion of this program participants will be able to:
 EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
EMS Subspecialty Certification Review Course 1.3.1 1.3.1.1 Shortness of Breath 1.3.1.1.1 Use of portable non invasive ventilation devices 1.3.1.1.2 Field Identification of COPD 1.3.1.1.3 Assisted Ventilation
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Learning Objectives: continued
 Learning Objectives: Describe the importance of a comprehensive assessment of a critically ill patient Describe how to assess the efficacy of breathing, work of breathing and adequacy of ventilation Discuss
Learning Objectives: Describe the importance of a comprehensive assessment of a critically ill patient Describe how to assess the efficacy of breathing, work of breathing and adequacy of ventilation Discuss
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care
 Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
Ventilating the paediatric patient. Lizzie Barrett Nurse Educator November 2016
 Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
Ventilating the paediatric patient Lizzie Barrett Nurse Educator November 2016 Acknowledgements Kate Leutert NE PICU Children's Hospital Westmead Dr. Chloe Tetlow VMO Anaesthetist and Careflight Overview
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
By Nichole Miller, BSN Direct Care Nurse, ICU Dwight D Eisenhower Army Medical Center Fort Gordon, Ga.
 Set the stage for ventilator 2.0 ANCC CONTACT HOURS Are you puzzled by ventilator modes? We help you differentiate between invasive and noninvasive ventilation and understand the common settings for each.
Set the stage for ventilator 2.0 ANCC CONTACT HOURS Are you puzzled by ventilator modes? We help you differentiate between invasive and noninvasive ventilation and understand the common settings for each.
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal and Anterior Mediastinal Abscess
 Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
Hindawi Case Reports in Pediatrics Volume 2017, Article ID 1848945, 4 pages https://doi.org/10.1155/2017/1848945 Case Report Complete Obstruction of Endotracheal Tube in an Infant with a Retropharyngeal
QUICK REFERENCE GUIDE CAPNOGRAPHY DURING PROCEDURAL SEDATION
 QUICK REFERENCE GUIDE CAPNOGRAPHY DURING PROCEDURAL SEDATION Changes in capnography values and waveforms may help clinicians understand a patient s level of comfort, sedation, and respiratory function
QUICK REFERENCE GUIDE CAPNOGRAPHY DURING PROCEDURAL SEDATION Changes in capnography values and waveforms may help clinicians understand a patient s level of comfort, sedation, and respiratory function
OWN THE AIRWAY. Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP. Paramedic Program
 OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Sign up to receive ATOTW weekly
 PULSE OXIMETRY PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 124 9 TH MARCH 2009 Dr. Iain Wilson Royal Devon & Exeter Hospital, UK Correspondence to iain.wilson@rdeft.nhs.uk The WFSA has been working on information
PULSE OXIMETRY PART 2 ANAESTHESIA TUTORIAL OF THE WEEK 124 9 TH MARCH 2009 Dr. Iain Wilson Royal Devon & Exeter Hospital, UK Correspondence to iain.wilson@rdeft.nhs.uk The WFSA has been working on information
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
TRACHEOSTOMY EMERGENCIES
 TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
TRACHEOSTOMY EMERGENCIES MODULE: AIRWAY TARGET: ALL ANAESTHETISTS, INTENSIVISTS, ED & ACUTE PHYSICIANS, FOUNDATION DOCTORS BACKGROUND: Around 16% of ICU patients may have a tracheostomy. Life- threatening
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Altered Respiratory Function Lecture 3. Nicole Tinny, RN, MSN Lake Sumter State College
 Altered Respiratory Function Lecture 3 Nicole Tinny, RN, MSN Lake Sumter State College Rhinitis Inflammation of nasal mucosa Due to infection or allergens Allergic rhinitis (hayfever) Rebound rhinitis
Altered Respiratory Function Lecture 3 Nicole Tinny, RN, MSN Lake Sumter State College Rhinitis Inflammation of nasal mucosa Due to infection or allergens Allergic rhinitis (hayfever) Rebound rhinitis
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient
 Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Shifting Atelectasis: A sign of foreign body aspiration in a pediatric patient Diana L Mark, RRT Pediatric Clinical Specialist Respiratory Care Wesley Children s Hospital Discuss when foreign body aspiration
Patient Ventilator Interactions. Patient-Ventilator Interactions. Assisted vs Controlled MV. Ventilatory Muscle Fatigue Recovery
 Patient Ventilator Interactions Patient-Ventilator Interactions Neil MacIntyre MD Duke Uni versity Medi cal Center Durham NC, USA Newer a pproaches to improving intera ctions Assisted vs Controlled MV
Patient Ventilator Interactions Patient-Ventilator Interactions Neil MacIntyre MD Duke Uni versity Medi cal Center Durham NC, USA Newer a pproaches to improving intera ctions Assisted vs Controlled MV