Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
|
|
|
- Pierce Sparks
- 5 years ago
- Views:
Transcription



1 Yuanlin Song, M.D.

2 Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS
3 PaO2/fiO2<300 (ARDS if < 200) Bilateral alveolar or interstitial infiltrates PCWP < 18 mmhg, or no clinical evidence of increase left atrium pressure
4 Direct lung injury Pneumonia Aspiration Pulmonary contusion Near-drowning Toxic inhalation injury Indirect lung injury Sepsis Severe trauma Multiple bone fracture Flail chest Head trauma Multiple transfusion Burns Drug overdose Pancreatitis Post-cardiopulmonary bypass

5 Annual incidence: 30/100,000 for ALI and 10/100,000 for ARDS 10% ICU admission may have acute respiratory failure Morality: 40-70% worldwide In China, around 700,000 new cases per year In Shanghai, mortality was 70% in 2001 Death number comparable to HIV, CI, breast cancer
6 Sepsis Pneumonia Trauma Multiple transfusion Aspiration Drug over dose Risk factors Old age Chronic alcohol abuse Metabolic acidosis Severity of critical illness Protective factors Diabetes

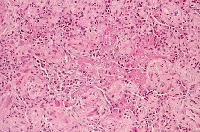
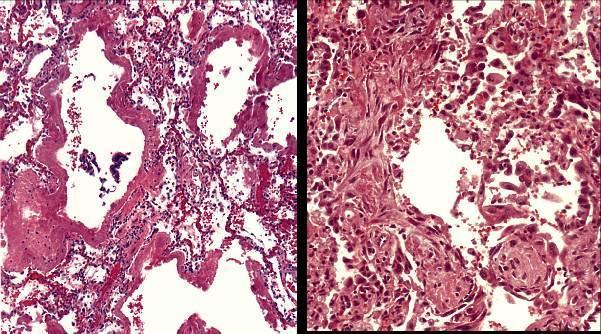
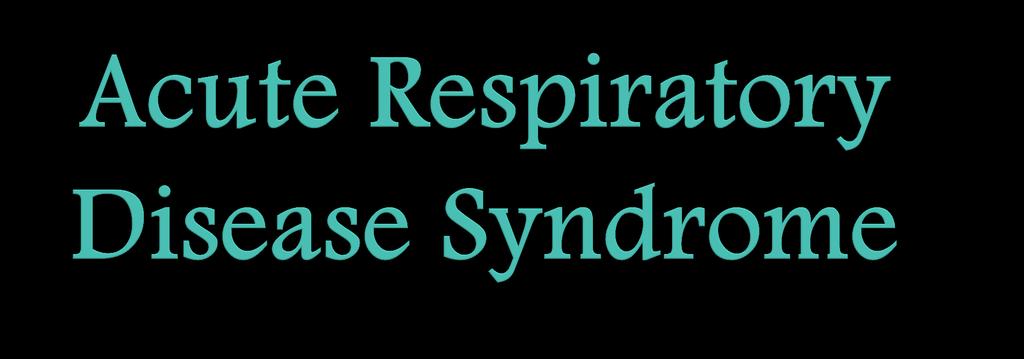
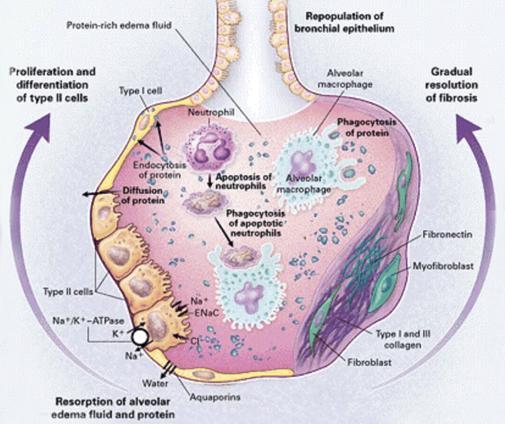
7 Exudative phase Proliferative phase Fibrotic phase
8
9 Treatment Principle: 1. Underlying disease control 2. Reduce Ventilator induced lung injury 3. Prevention of venous thromboembolism, GI bleeding, catheter infection 4. Prevent and recognition of HAP 5. Support therapy: nutrition, ventilation, fluid, antibiotics
10 Mechanical ventilation strategy principles 1. Selection of non-invasive and invasive ventialtion 2. Management of artificial airways 3. Ventilation mode: IPPV, PSV, SIMV, PRV, NAVA, 4. PEEP: 5. Ventilation parameters: Volume, RR, 6. Other methods: HFV, ECMO, PLV
11 VILI Original disease:sepsis,aspiration, pneumonia, and trauma etc + MV 1 2 High volume, open-close inflammation Immune function ATPase Barrier disruption Local- systemic Macrophage Alveolar-capillary permeability Alveolar flooding, interstitial edema bacteremia,sepsis SIRS,MOF
12 Pressure-volume curve volume Hyper inflation Safety window Alveoli close pressure

13 Alveoli structure:stability airway airway alveoli alveoli T w =P TP Xr/2
14 Lung recruitment maneuver 1.Selection of PEEP 2.Position 3.IRV
15 Other therapies 1. Steroid application 2. Fluid management 3. Anti-inflammation therapy: NAC, ambroxol 4. NO inhalation 5. APC infusion 6. Stem cell therapy
16 ARDS pharmacotherapy Drug name Action Results Source Prostaglandin E1 Pulmonary vasodilation Decrease neutrophils activation, decrease platelet aggregation No difference for early mortality, inconclusive for later mortality 693 patients N-acetylcysteine and procysteine Antioxidant No difference for early mortality 235 patients Surfactant Ketoconazole Restore normal mechanical properties No difference for early mortality 1416 patients Beta2-agonist indomethacin Anti-inflammation Iv injection showed decreased lung water, no changes for mortality Nitric oxide (inhalation) Pulmonary vasodialator Reduce shut, pulmonary artery pressure but no benefit for mortality 208 patients Activated protein C (IV) Inhibit PAI-1, promote fibrinolysis of hayline membrane No difference for mortality, ventfree days 75 Corticosteroid Multiple anti-inflammation No difference for early mortality 1416 patients
17 ARDS ventilation/support therapy 1. Small tidal volume: 6ml/kg vs 12 ml/kg, when applying 6ml/kg, Pplat set 25-30cmH2O, decrease mortality (40% vs 31%), increase ventilation free days, reduce plasma cytokines, reduce organ failure days 2. FiO2/PEEP: 0.3-1/5-24cmH2O: high PEEP strategy: increase oxygen transfer function, increase lung compliance, but no difference in mortality. PEEP maybe not be more than 10 cmh2o for a typical ARDS patients. 3. NPPV: early intervention, increase oxygenation, may reduce intubation rate (on going clinical trial in Chaoyang Hospital). 4. Ventilation mode: ARDSnet 6ml/kg, may reduce barotrauma, but may decrease alveoli recruitment. ARPV could maintain minimum airway pressure while keep alveoli recruitment. On going clinical trial
18 Ventilation/support therapy 1. Liquid ventilation: both low dose (10mg/kg) and high dose (20ml/kg) of perfluocarbon does not provide any benefit compared to CMV. 2. High frequency ventilation:no clear benefit compared to CMV mode. 3. Prone-position ventilation: improve oxygenation, maybe useful in severe ARDS patients. 4. Nutrition: Ongoing clinical trial including OMGA-3 5. Fluid: 1000 patients, main finding: no difference in clinical outcome, but fluid conservative trial significantly increased ventilation-free days. 6. Control infection:
19 Stem cell therapy Endothelial and epithelial repair Ang-1, KGF, Produce growth factors, regulate cytokines ARDS Hypoxia, cytokines and growth factor release Stem cell mobilization from bone marrow Translocation to injury area Exogenous stem cell Antimcrobial peptide production immune cell interaction Modulate inflammatory cells Integrated to repair endothelium and epithelium Cell-cell contact, mitochondria genetic information transfusion
20 Prognosis 1.Mortality 2.Biomarker study 3.Long term follow up
21 Biomarker and lung injury Biomarkers for: cardiac infarction-ldh, Procalcitonion; liver cancer: FP; Why no biomarkers for lung injury? Complexity, non-specific inflammation.. We need good biomarkers for ARDS diagnosis, prognosis, indication for therapy. Potential biomarkers: Cell specific receptor/antigen:kl-6, RAGE Released or synthesized during injury/repair: SPA-D, MMP, CRP Cytokines: IL-1,6, 8, 10 Cell adherence molecules: ICAM-1,
22 Biomarkers for ALI/ARDS name Significance Source author VWF Independent predictor for hospital mortality in ALI CCM, 2001, AJCCM 2004 Ware ICAM-1 May predict outcomes(cut off) AJCCM 2001 kayal SPA,SPD SPA-predict ARDS Dev Chest 1999 Greene SPD-correlates with LTV Thorax 2003 Eisner RAGE Associated with mortality Thorax, 2008 Griffts PC Reduced PC Correlates with increased mortality AJP 2003 Ware PAI-1 Independent predictor for mortality Ajp, 2003 Prabhak aran KL-6 (mucin like protein expressed on ATII cell) Increased plasma level associated with severe lung injury and high mortality ERJ, 2004 Sato
23 Quiz (correct answer is yellow one) The typical feature of ARDS 1. Increased vascular permeability 2. Increased alveolar epithelium permeability 3. Heterogeneous Lung damage 4. Un-controlled lung inflammation 5. All above Which is the most beneficial treatment of ARDS 1. Fluid restriction 2. Anti-coagulation 3. Steroid application 4. Protective ventilation strategy 5. Nutrition and support therapy
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Novel pharmacotherapy in ARDS
 Novel pharmacotherapy in ARDS Danny McAuley Royal Victoria Hospital and Queen s University of Belfast Critical Care Cananda Forum October 2012 Disclosures GSK; consultancy and participate in research funded
Novel pharmacotherapy in ARDS Danny McAuley Royal Victoria Hospital and Queen s University of Belfast Critical Care Cananda Forum October 2012 Disclosures GSK; consultancy and participate in research funded
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Is ARDS Important to Recognize?
 Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Intravenous Vitamin C. Severe Sepsis Acute Lung Injury
 Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES
 DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES This lecture covers two topics: neonatal respiratory distress syndrome (neonatal RDS) and adult respiratory
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES This lecture covers two topics: neonatal respiratory distress syndrome (neonatal RDS) and adult respiratory
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Transfusion Related Respiratory Complications:
 Transfusion Related Respiratory Complications: An Update on TRALI, TACO and TAD Marla C. Troughton, MD Medical Director Alabama and Central Gulf Coast Region Disclosure I have no real or apparent conflict
Transfusion Related Respiratory Complications: An Update on TRALI, TACO and TAD Marla C. Troughton, MD Medical Director Alabama and Central Gulf Coast Region Disclosure I have no real or apparent conflict
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
MANAGEMENT OF THORACIC TRAUMA. Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA
 MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
MANAGEMENT OF THORACIC TRAUMA Luis H. Tello MV, MS DVM, COS Portland Hospital Classic Banfield Pet Hospital - USA luis.tello@banfield.com Chest Trauma: Big threat!!!! CAUSES OF THORACIC TRAUMA Blunt Trauma
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Introduction Definition Etiology Epidemiology Lung injury prediction score. Pathophysiology Diagnosis Clinical presentation Management Conclusion
 Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Oxygen:..Nothing is without poison.. the poison is in the dose..
 Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
Postoperative chest x-ray May Mats Beckman Emergency Radiology. Shutter use!
 Postoperative chest x-ray May 2009 Mats Beckman Emergency Radiology Shutter use! 2Postoperative chest x-ray May 2009 Exposure/ window settings Quick resorption of infiltrations= water logged lung 3Postoperative
Postoperative chest x-ray May 2009 Mats Beckman Emergency Radiology Shutter use! 2Postoperative chest x-ray May 2009 Exposure/ window settings Quick resorption of infiltrations= water logged lung 3Postoperative
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY
 EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
INTRODUCTION. Acute respiratory distress syndrome (ARDS) is a common complication of critical illness
 is a common complication of critical illness") Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Adult Respiratory Distress Syndrome
 Critical Care Medicine Adult Respiratory Distress Syndrome Leonard J. Sonne, MD, FACP, FCCP* *Chief, Division of Pulmonary Physiology and Medicine, Department of Medicine, King Faisal Specialist Hospital
Critical Care Medicine Adult Respiratory Distress Syndrome Leonard J. Sonne, MD, FACP, FCCP* *Chief, Division of Pulmonary Physiology and Medicine, Department of Medicine, King Faisal Specialist Hospital
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
9/17/2014. Good Morning! 14th Annual Western Kansas Respiratory Care Seminar. 14th Annual Western Kansas Respiratory Care Seminar 28th
 Good Morning! 14th Annual Western Kansas Respiratory Care Seminar Current Status of Extracorporeal Membrane Oxygenation (ECMO) in Infants and Adults Kelly D. Hedlund, MS, CCP Chief Perfusionist Michael
Good Morning! 14th Annual Western Kansas Respiratory Care Seminar Current Status of Extracorporeal Membrane Oxygenation (ECMO) in Infants and Adults Kelly D. Hedlund, MS, CCP Chief Perfusionist Michael
Lutheran Medical Center Department of Surgery
 Lutheran Medical Center Department of Surgery Morbidity & Mortality Conference Case & Topic Presentation Baiju C. Gohil, M.D. April 9, 2004 FAT EMBOLISM SYNDROME INTRODUCTION Fat emboli were first noted
Lutheran Medical Center Department of Surgery Morbidity & Mortality Conference Case & Topic Presentation Baiju C. Gohil, M.D. April 9, 2004 FAT EMBOLISM SYNDROME INTRODUCTION Fat emboli were first noted
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM
 REFERRAL FORM") Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
Patient Label This form is accessible on www.royalpapworth.nhs.uk Intensive Care Unit EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) REFERRAL FORM Please always phone Papworth ECMO Coordinator on 01480 830541,
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
OLB (Open Lung Biopsy) in ARDS
 in ARDS") OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Effect of ARDS Severity and Etiology on Short-Term Outcomes
 Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
How can human models of ALI inform clinical trials
 How can human models of ALI inform clinical trials Danny McAuley Royal Victoria Hospital and Queen s University of Belfast Critical Care Cananda Forum October 2012 Disclosures GSK; consultancy and participate
How can human models of ALI inform clinical trials Danny McAuley Royal Victoria Hospital and Queen s University of Belfast Critical Care Cananda Forum October 2012 Disclosures GSK; consultancy and participate
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Alma Mater University of Bologna. Respiratory and Critical Care Sant Orsola Hospital, Bologna, Italy
 Alma Mater University of Bologna Respiratory and Critical Care Sant Orsola Hospital, Bologna, Italy Conflict of Interest I have affiliations with, special interests, or have conducted business with the
Alma Mater University of Bologna Respiratory and Critical Care Sant Orsola Hospital, Bologna, Italy Conflict of Interest I have affiliations with, special interests, or have conducted business with the
Sepsis and Shock States
 Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Sepsis and Shock States Presented By: Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com CNEA 2009 1 INFECTION Inflammatory response to microorganisms, or Invasion of normally sterile tissues SYSTEMIC
Acute respiratory distress syndrome and acute lung injury
 1 Critical Care Research Unit, Southampton University Hospital, Southampton, UK 2 Division of Developmental Origins of Health and Disease, School of Medicine, University of Southampton, Southampton University
1 Critical Care Research Unit, Southampton University Hospital, Southampton, UK 2 Division of Developmental Origins of Health and Disease, School of Medicine, University of Southampton, Southampton University
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care