1. RHEUMATIC FEVER 2. CHAGAS DISEASE 3. Myocarditis
|
|
|
- Jennifer Craig
- 5 years ago
- Views:
Transcription

1
2 Although the vast majority of cardiac diseases relate to the presence of atherosclerosis in the vessels supplying blood and oxygen to the heart, there are certain conditions in which immunological events play an important role. 1. RHEUMATIC FEVER 2. CHAGAS DISEASE 3. Myocarditis

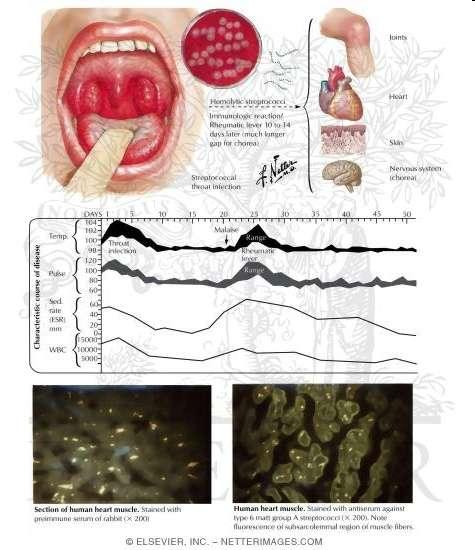
3 Rheumatic fever Rheumatic fever is an inflammatory disease that occurs following a A streptococcus infection. Is a delayed, nonsuppurative sequela of a pharyngeal infection with the group A streptococcus
4 Epidemiology Ages 5-15 yrs are most susceptible Rare <3 yrs Girls>boys Common in 3rd world countries Incidence more during fall,winter & early spring
5 Manifestations A latent period of two to three weeks follows the initial streptococcal pharyngitis. The onset of disease is usually characterized by an acute febrile illness, which may manifest itself in one of three classical ways: (1)The patient may present with migratory arthritis predominantly involving the large joints of the body. (2) Carditis and valvulitis, or carditis and valvulitis may be the only signs of an acute episode. (3) There may be involvement of the central nervous system, manifesting itself as Sydenham s chorea.
6 MOLECULAR MIMICRY IN RHEUMATIC FEVER Many of the antigens present in the group A streptococcus cross-react with antigens present in mammalian tissues. Thus, antibodies present in the sera of ARF patients bind to cardiac tissue or cells in the caudate nucleus or to human kidney tissues.
7

8
9 Pathogenesis Although there is little evidence for the direct involvement of group A streptococci in the affected tissues of ARF patients, a large body of epidemiological and immunological evidence indirectly implicates the group A streptococcus in the initiation of the disease process: (1) It is well known that outbreaks of ARF closely follow epidemics of either streptococcal sore throats or scarlet fever. (2) Adequate treatment of a documented streptococcal pharyngitis markedly reduces the incidence of subsequent ARF. (3) Appropriate antimicrobial prophylaxis prevents the recurrences of disease in known patients with acute ARF.
10 Etiologic Considerations At least three main theories have been proposed: The first theory : Is concerned with the question of whether persistence of the organism is important. No investigators have been able to consistently and reproducibly demonstrate live organisms in rheumatic fever joints, cardiac tissues, or valves.
11 The second theory: Is concerned with deposition of toxic products is required certain streptococcal pyrogenic exotoxins (A and C) may act as superantigens. These antigens may stimulate large numbers of T cells through their unique bridging interaction with T-cell receptors and class II MHC molecules. Once activated, these cells elaborate tumor necrosis factor, gamma interferon, and a number of interleukin moieties, thereby contributing to the initiation of pathological damage
12 The third theory: Perhaps the best evidence to date favors the theory of an abnormal host immune response (both humoral and cellular) in the genetically susceptible individual to those streptococcal antigens cross-reactive with mammalian tissues. The evidence supporting this theory can be divided into three broad categories: 1.The presence of heart-reactive antibodies in ARF sera. 2. Sera from patients with ARF also contain increased levels of antibodies to both myosin and tropomyosin, and keratin as compared with sera from patients with pharyngeal streptococcal infections that do not develop ARF. These myosin-affinity purified antibodies also cross-react with M protein moieties (known to share amino acid homology with myosin), suggesting this molecule could be the antigenic stimulus for the production of myosin antibodies in these sera.
13 3.Finally, as indicated earlier, autoimmune antibodies are a prominent finding in another major clinical manifestation of ARF, namely, Sydenham s chorea, and these antibodies are directed against the cells of the caudate nucleus. A number of chorea patients presented with behavioral disorders such as tics or obsessive-compulsive disorders (OCD). Streptococci and probably other microbes may induce antibodies, which functionally disrupt the basal ganglia pathways leading not only to classical chorea but also to other behavioral disorders in these children without evidence of classical chorea.
14 4. In all cases in which autoreactive antibodies are seen (heart, brain, cardiac valves, kidney), they can be absorbed with streptococcal antigens, notably those streptococcal antigens of the M protein that share homology with human myosin, tropomyosin, keratin, and so on.
15 At a cellular level : There is now ample evidence for the presence of both lymphocytes and macrophages at the site of pathological damage in the heart valves in patients with ARF. The cells are predominantly CD4+ helper lymphocytes during acute stages of the disease. The ratio of CD4+/CD8+ lymphocytes (2:1) more closely approximatesthe normal ratio in chronic valvular specimens. This abnormal reactivity peaks at six months after the attack but may persist for as long as two years after the initial episode. Once again, the reactivity was specific only for those strains associated with ARF.
16 o all rheumatic fever patients express abnormal levels of D8/17- positive B cells, especially during the acute attack. o Monoclonal antibody D8/17 identifies a B lymphocyte antigen with expanded expression in nearly all patients with rheumatic fever and is thought to be a trait marker for susceptibility to this complication of group A streptococcal infection. o In those cases where the diagnosis of ARF has been doubtful, a strong association of the D8/17 B-cell marker with children with OCD. o presence of elevated levels of D8/17-positive B cells has proven to be helpful in establishing the correct diagnosis.



17 بسم هللا الرمحن الرحمي Reham abu Husin
18 Etiology Acute rheumatic fever is a systemic disease of childhood,often recurrent that follows group A beta hemolytic streptococcal infection It is a delayed non-suppurative sequelae to URTI with GABH streptococci. It is a diffuse inflammatory disease of connective tissue,primarily involving heart,blood vessels,joints, subcut.tissue and CNS
19 Genetics That ARF might be the result of a host genetic predisposition has intrigued investigators for over a century. It has been variously suggested that the disease gene is transmitted: in an autosomal dominant fashion, in an autosomal recessive fashion with limited penetrance, or that it is possibly related to the genes conferring blood group secretor status.
20 Renewed interest in the genetics of ARF occurred with the recognition that gene products of the human MHC (major histocompatibility complex) were associated with certain clinical disease states.
21 Using an alloserum from a multiparous donor, an increased frequency of a B-cell alloantigen was reported in several genetically distinctand ethnically diverse populations of ARF individuals and was not MHC related.
22 Most recently, a monoclonal antibody(d8/17) was prepared by immunizing mice with B cells from an ARF patient. A B-cell antigen identified by this antibody was found to be expressed on increased numbers of B cells in 100 percent of rheumatic fever patients of diverse ethnic origins and only in 10 percent of normal individuals. The antigen defined by this monoclonal antibody showed no association with or linkage to any of the known MHC haplotypes, nor did it appear to be related to B-cell activation antigens.
23 These studies are in contrast to other reports in which an increased frequency of certain human leucocytes antigens (HLAs) was seen in ARF patients. There are marked differences in the increased frequency of the HLAs, depending on the racial features of the patient group. These seemingly conflicting results concerning HLA and RF susceptibility prompt speculation that these reported associations might be of class II genes close to (or in linkage disequilibrium with) but not identical to the putatative RF susceptibility gene.
24 Alternatively, and more likely, susceptibility to ARF is polygenic, and the D8/17 antigen might be associated with only one of the genes (i.e., those of the MHC encoding for the D-related [DR] antigens) conferring susceptibility. Although the full explanation remains to be determined, the presence of the D8/17 antigen does appear to identify a population at special risk of contracting ARF.
25 Streptococcal Vaccine Candidates As early as the 1930s, researchers were pursuing the study of streptococcal vaccinations, with the injection of whole killed group A streptococci and cell walls, thereof culminating in injections of partially purified M protein extracts in the1970s. However, all interest, especially by the pharmaceutical companies, ceased at that point because the U.S. Food and Drug Administration (FDA) proclaimed that one could work on streptococcal vaccines as long as no streptococcal component was used!.
26 The FDA was afraid that induction of antibodies cross-reactive with human tissues, especially cardiac tissues,could be detrimental to the vaccine. However, it was soon apparent that many individuals had antibodies cross-reactive with a variety of human tissues and were perfectly normal.
27 In the past decade, the restriction was removed on the condition that toxicity studies in animals did not reveal any deletion effects in the animals when injected with a streptococcal vaccine candidate. This ushered in the search for an effective,safe, and inexpensive group A streptococcal vaccine, and there are now at least four prominent candidates with more in the pipeline:
28 1. Perhaps the most advanced candidate is by Dale and colleagues (1996), which is synthetic peptide sequences of a variety of M protein types taken from the variable region of the M protein and hooked together by linkers. This has induced protective immunity in animals to a number of different M protein types and is safe for use in humans. Clinical trial of its efficacy to prevent streptococcal infections is currently under way.
29 2. The use of the C-repeat constant region of the M protein advanced by Fischetti (1989) produces protection against oral colonization of the throat by group A streptococci.
30 3. A surface protein called C5 peptidase, which is present on the surface of all group A and group B streptococci, produces antibodies that block both the colonization of group A and group B streptococci in oral colonization studies.
31 4. The streptococcal group A carbohydrate (CHO) as proposed by Zabriskie and colleagues has been purifi ed and used as an immunogen to protect against streptococcal infections. This vaccine candidate promotes phagocytosis of group A streptococci of several different M types, will protect against infection using passive and active immunization studies, and also protects against oral colonization.
32 The confirmed observation of an increased frequency of a B-cell alloantigen in several populations of rheumatics suggests that it might be possible to identify individual ssusceptible to ARF at birth. If so, then from a public health standpoint, these individuals would be prime candidates for immunization with any streptococcal vaccine that might be developed in the future.
33 Directions for Future Research Do super antigens play a role in this transformation? Are particular cytokines and lymphokines present during the quiescent period? Are cellular mechanisms at work, and if so,what cells are involved? These questions are important because the answers to those questions in ARF may hold keys to unlocking other rheumatic diseases!!!
34 Finally, one of the most intriguing, unresolved questions has been: the possible association of the group A streptococcus with behavioral disorders such as OCD (Obsessive compulsive disorder ), tics, Tourette s syndrome, and anorexia nervosa????!!!
35 Even as early as the 1890s, Osler observed in his textbook of medicine that many of his former Sydenham s chorea patients (a well-known neurological manifestation of a streptococcal infection) often were later seen as patients in the behavioral disorder clinics. One can also expand these concepts to other organisms in which there may be shared antigenicity between microbial and mammalian antigens.



36
37 Brazilian physician Carlos Chagas who first discovered the parasite responsible for the signs and symptoms of the disease.
38 Also called American trypanosomiasis Caused by a protozoan Trypanosoma cruzi infects humans and animals through an insect called a kissing bug /reduviid bug.. The disease can be seen in dogs and humans and initially causes flulike signs (fever, headache), which can progress to heart failure over along period of time. Systemic protozoal disease





39

40 20 million infected 100 million at risk higher in South America
41 Accidental oral ingestion of reduviid bugs, which release metacyclic trypomastigotes to invade the oral mucosal cells Vertically from mother to child( months 5-9 of pregnancy) CONGENITAL TRANSMISSION 10% Blood transfusions 12-25%

42

43
44 Innate immune response Tissue tropism Animal models
45 Early in infection host depend on innate immune ( macrophages and (NK) Unactivated macrophages little ability to kill T. cruzi for parasite replication Within two hours of macrophage invasion, the majority of T. cruzi have escaped the phagosome and exist free in the host cytoplasm avoiding degradation by intracellular microbicidal enzymes A variety of stimuli for priming macrophages IFN-γ (IL-2, IL-3, IL-4, and IL-5) IFN-γ + purified IL-4 no better-anti-il-4 antibodies Lipopolysaccharide significantly increases the trypanocidal effect of IFN-γ on macrophages granulocyte-macrophage colony-stimulating factor
46 NK cells participate in the innate immune response secrete IFN-γ after incubation with T. cruzi in vitro Since IFN-γ activates macrophages to kill T. cruzi, the role of NK cells in T. cruzi infection would be expected to be protective IFN-γ that helps control parasite replication before the acquired immune response becomes predominant may also be involved in the immune response later in infection
47 Serum taken from an uninfected human does not lyse trypomastigotes, but serum infected patients does the complement system requires acquired immune response to T. cruzi to become operational Parasite lysis primarily via the alternative complement pathway direct association of (C3) with the parasite surface, rather than by fixation of complement by antibody Fc receptors effect of immune antibodies on complement lysis of trypomastigotes was a function of the specificity of the antigenbinding sites there was a surface component on the parasites when neutralized by immune sera the parasites susceptible to complement lysis
48 gp160 specific parasite product bound the complement component C3b and inhibited C3 convertase formation, thus inhibiting activation of the alternative complement pathway is membrane bound and shares genetic and functional similarities to the human complement regulatory protein, decay accelerating factor restrict classic complement activation The T. cruzi complement regulatory protein is stage specific in that it is only expressed by mammalian forms of the parasite
49 Growth in muscle and nervous tissue is more likely to be related to a strategy for long-term parasite survival in the host, rather than a strategy related to direct transmission to secondary hosts. IFN-γ induction of macrophage trypanocidal activity is associated with the production of hydrogen peroxide * However, treatment of activated macrophages with catalase, superoxide dismutase, or sodium benzoate to scavenge respiratory burst metabolites failed to inhibit trypanocidal activity in vitro, suggesting an oxygen-independent mechanism of T. cruzi destruction
50 Macrophages primed with IFN-γ produce NO NO may be directly toxic to T. cruzi; however, it reacts with superoxide(o2 ) to yield peroxynitrite (ONDO ), which is highly toxic In vivo, inducible nitric oxide synthase (inos) is induced at the protein and messenger RNA levels, and NO is released during acute infection The IFN- γ induced, NO-dependent mechanism of macrophage killing of T. cruzi can be inhibited by the addition of interleukin-10 or transforming growth factor-β in vitro
51 In mice, parasites apparent in blood 5-7 d after infection and rise until 3or 4 w. RAG knockout mice( deficient in both B- and T-cell function) have similar levels of parasitemia compared with wild-type mice until day 13 of infection, parasitemia level becomes higher in the RAG knockouts. This indicates that the acquired immune response has little effect until about 2w. Although anti T. cruzi antibodies are detectable at about day 7 in murine models, protective antibodies are not present until several weeks later Both IgG subclasses 1 and 2 are capable of clearing T. cruzi Antibodies mediate protection from T. cruzi by opsonization, complement activation, and antibody-dependent cellular cytotoxicity
52 Experiments in mice showed that T-cell activation correlated with resistance to infection Deficient T-cell function is associated with increased sensitivity to infection Mice that are depleted of T cells (CD4+ or CD8+) after they have survived the acute infection do not have altered parasitemia or longevity declining role of T cells and the importance of humoral immunity in controlling infection after the acute stage
53 T cells perform a variety of antiparasitic functions: provide helper T-cell function by stimulating B cells to produce parasite-specific antibody T-cell line derived from the spleens of T. cruzi infected mice was able to induce normal spleen cells to produce parasitic-directed antibodies when stimulated in vitro with T. cruzi antigen T cells produce cytokines in T. cruzi infection, which mediate important antiparasitic functions CD8+ T cells lyse T. cruzi infected host cells, which presumably interrupts the parasite life cycle, thus limiting its replication mice genetically deficient for genes controlling perforin or granzyme B mediated cytolytic pathways had parasitemia and mortality rates similar to wild-type mice, suggesting that cytolytic function, in fact, may not be the protective effector mechanism of CD8+ T cells T. cruzi specifi c CD8+ T cells produce IFN-γ and TNF-α upon stimulation, thus raising the possibility that these cells mediate their effects by cytokine release.
54 The inflammatory infiltrates consisted mainly of lymphocytes (60 90 percent) macrophages (10 40 percent). The lymphocytes primarily carried the T-cell marker, Thy1.2 Thy1.2+ cells were the major lymphocyte population in tissues (cardiac and skeletal muscle) during acute infection. Both CD4+ and CD8+ T cells were present in the infiltrates of skeletal muscle, sciatic nerve, and spinal cord. a slight predominance of CD8+ cells over CD4+, during the early chronic and late chronic stages CD8+ T cells (47 59 percent) dominated over CD4+ T cells (9 19 percent). B cells and macrophages each represented less than 1 percent
55 On standard histopathological study inflammatory lesions are found to co-localize with abundant parasites, demonstrating that inflammatory damage is directed to the parasite. Pathophysiology Disease results from an autoimmune response directed at the affected organ systems or from damage resulting from inflammation related to the persistence of the parasite autoimmune hypothesis observations that live T. cruzi parasites have been difficult to demonstrate in involved organs by conventional histological study autoimmune T cells and antibodies develop during infection with T. cruzi Some T. cruzi antigens molecularly mimic affected host tissues chronic infection leads to loss of tolerance and, combined with antigenic mimicry, results in specific autoimmune attack of cardiac, gut, and peripheral nervous tissues.
56 Other hypothesis progressive inflammation directed at parasites that reside in target organs cause the pathologic damage of chronic infection Studies that support this hypothesis have found that parasite antigens and DNA can be detected in many chronic inflammatory infiltrate and that parasitologic treatment of chronically infected animals or humans tends to lead to improvement and resolution of disease
57 The theory of autoimmunity supported by a number of observations 1- Few parasites can be demonstrated in the inflammatory lesions by conventional histological study. -This observation suggests the disease may not be driven solely by reaction to the parasite 2- Only 10 to 30 %of chronically infected people develop Chagas disease, although most can be shown to have chronic parasitemia. - This suggests that, in addition to chronic T. cruzi infection, some other factor(s) develops disease. -Susceptibility to autoimmune disease 3- Chronic Chagas disease is very organ specific, generally limited to the heart, nervous tissues, or innervation of the gut. - suggests that additional specificity of Chagas disease is imposed during infection, perhaps by the particular autoimmune response that is generated by chronic T. cruzi infecion. 4- The long lag time from infection to disease could be necessary to generate disease by autoimmunity. 5- The presence of autoimmune T cells and antibodies in infected individuals, especially when they are associated with disease, is evidence that autoimmunity may play a role in pathogenesis.
58 Autoimmune antibodies are easily demonstrated in T. cruzi-infected individuals. Antibodies to myocardium and nervous tissues are found in high levels myocardium and nervous tissues are key organs that are damaged in chronic Chagas disease, finding antibodies to these tissues could mean that these antibodies cause autoimmune damage to these tissues antigens from myocardium and nervous tissues are probably exposed by the damage of infection of these organs, and antibodies may be generated to these tissues without being pathogenic Many of the autoantibodies found in the sera of T. cruzi infected persons and mice are so-called natural autoantibodies The high levels of natural autoantibodies after T. cruzi infection may be the result of the polyclonal lymphocytic proliferative response that occurs during acute infection Levels of natural autoantibodies do not correlate with diseases in individuals who are chronically infected with T. cruzi.

59

60


61
62 Alternative theory parasites residing in chronically infected host tissue may cause chronic disease by either damaging tissues directly or focusing the inflammatory response in host tissues properties autoimmune hypothesis may also be possible with parasite-directed pathogenesis Parasites may be difficult to demonstrate in the lesions due to limitations of present techniques not all chronically infected individuals develop chronic disease reflect parasite burden, strain differences, or host variation in the immune response organ specificity due to tropism of the parasite for cardiac and neuronal tissues long lag time to develop disease due to the slowly progressive damage Two other factors support the parasite- directed damage o o First, immunosuppression exacerbates the disease process and causes worsening of the pathologic lesions of Chagas disease second factor is that treatment with antiparasitic drugs in early Chagas disease markedly lessened the progression to chronic disease, although the number of patients assigned to treatment versus placebo groups was small.


63 بسم اهلل الرحمن الرحيم
64 Myocarditis Myocarditis is an inflammation of the myocardium
65 Major features: Arrhythmia,CHF,cardiogenic shock. In ECG: Non-specific ST wave changes. Echocardiogram: Normal ventricular size but decrease contractility. chronic cases: heart enlargement with thinning of the muscle. both ventricles may be affected.
66 Diagnosis None of the clinical features described are diagnostic for myocarditis and until the use of the endomyocardial biotome, the diagnosis could only be established with certainty by postmortem examination.
67 Incidence The incidence of the disease varies from 1 to 10/100,000. Many patients recover spontaneously inter supportive treatment. five-year survival of giant cell myocarditis is only 56 %. in pediatric patients, the mortality rates may be even higher.
68 Dilated Cardiomyopathy DCM is a chronic form of heart disease. Characterized by right ventricular dilation and impaired contraction.
69 Signs and symptoms Asymptomatic cardiomopathy. severe congestive heart Failure. Arrhythmias. Systemic pulmonary vein congestion. mitral or tricuspid regurgitation.
70 Incidence incidence10/100,000. Poor outcome. five-year mortality of 46 %.
71 Etiologic Considerations of both Myocarditis and DCM In both myocarditis and DCM, there appears to be an association with prior Coxsackie virus infections. In children and infants with DCM, significantly increased titers of neutralizing antibody to the virus has been found. Coxsackie virus,b specific nucleic acid sequences have been found in the heart tissues of a small number of these patients.
72 Autoimmune Considerations There is role of autoantibodies to the heart. antibody localized on the myocyte, giving a sarcolemmal, myolemnal pattern or on the striations, producing a fibrillar pattern. myocarditis sera reacted more to myosin heavy chain. cardiomyopathy sera reacted more to muscle actin.
73 ELISA studies have revealed that autoantibodies to ANT were elevated in 24/32 patients with DCM. So many patients with myocarditis and with DCM develop autoantibodies to a number of cardiac constituents. ANT: Adenosine Nucleotide Translocator.
74 None of these antibodies to cardiac antigens is known to play a direct pathogenetic role in the disease. However, the presence of antibodies to β1- adrenergic receptors in DCM and Chagas disease is highly suggestive of a direct pathogenetic effect, since the antigen is accessible on the surface of the myocardiocyte.
75 β1-adrenergic receptor antibodies can induce apoptosis in isolated adult cardiomyocytes and antibodies activating the receptors are associated with reduced cardiac function in chronic heart failure. Antibodies to the mitochondrial antigens, ANT and BCKD, may also have adverse consequences on cardiac function. It is not clear, however, whether these antibodies have access to their target antigens in vivo. BCKD:mitochondrial branched-chain α-ketoacid dehydrogenase.
76 Genetic Features relationship with the human MHC (HLA). DCM patients had an increased frequency of HLA-DR4 and a decreased frequency of HLA-DR6. The largest study to date reconfirmed these findings and also found that DR4-Dqw4 haplotype conferred heightened risk of disease.
77 A predominance of myocarditis in males has been reported in a number of studies. The proportion of male patients is about 60 percent. In this respect, myocarditis differs from most autoimmune diseases,which predominantly affect females.
78 Environmental Features Myocarditis has both infectious and noninfectious causes. Acute myocarditis is associated with infections of many types,including bacterial, rickettsial, viral, mycotic, protozoan, and helminthic.
79 the most common agents are : enteroviruses and the adenoviruses. Coxsackie virus group B infections were associated with at least half of the acute cases of myocarditits Coxsackie virus B antigen was found in the myocardium of 30.9 % of routine autopsy specimens of myocarditis. Serotype B3 is identified most frequently.
80 Treatment and Outcome supportive therapies bed rest. treatment of heart failure, arrhythmias, and embolic events if present. Cardiac transplantation in patients with refractory heart failure.
81 immunosuppressive therapy Some individuals respond well to immunosuppression (prednisone and cyclosporine), others fail to respond or even have serious adverse reactions that preclude continued treatment.
82 The major problem at present is the difficulty in distinguishing immunemediated cardiac disease from infectious, genetic, or toxic forms of the disease. So treatment cannot be rational or capable of evaluation.
83 Future Directions for Research The future treatment of autoimmune disease in general depends on early prediction and appropriate prevention.
84 The initial goal is : to identify patients with viral myocarditis who are likely to progress to an autoimmune disorder. Susceptible strains of mice produce somewhat higher levels of certain key cytokines such as IL-1β and TNF-α. Early elevation in these or similar key cytokines may provide useful biomarkers for subsequent autoimmune disease.
85 evidence shows that inhibiting some critical cytokines at the earliest stages of pathogenesis can avoid the autoimmune sequelae of viral infection. For example, administration of either the IL-1β receptor antagonist or monoclonal antibodyto TNF-α prevents the development of autoimmune myocarditis.
86 The second goal is: to identify patients with autoimmune myocarditis who are most likely to progress to irreversible DCM. Early data suggest that two key cytokines, IFN-γ and IL- 13, exert important protective effects during autoimmune myocarditis. Consequently, mice deficient in either of these cytokine markers are likely to progress to a severe form of dilatedcardiopathy.

87
Medical Virology Immunology. Dr. Sameer Naji, MB, BCh, PhD (UK) Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University
 Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University") Medical Virology Immunology Dr. Sameer Naji, MB, BCh, PhD (UK) Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University Human blood cells Phases of immune responses Microbe Naïve
Medical Virology Immunology Dr. Sameer Naji, MB, BCh, PhD (UK) Head of Basic Medical Sciences Dept. Faculty of Medicine The Hashemite University Human blood cells Phases of immune responses Microbe Naïve
Third line of Defense
 Chapter 15 Specific Immunity and Immunization Topics -3 rd of Defense - B cells - T cells - Specific Immunities Third line of Defense Specific immunity is a complex interaction of immune cells (leukocytes)
Chapter 15 Specific Immunity and Immunization Topics -3 rd of Defense - B cells - T cells - Specific Immunities Third line of Defense Specific immunity is a complex interaction of immune cells (leukocytes)
Third line of Defense. Topic 8 Specific Immunity (adaptive) (18) 3 rd Line = Prophylaxis via Immunization!
 (18) 3 rd Line = Prophylaxis via Immunization!") Topic 8 Specific Immunity (adaptive) (18) Topics - 3 rd Line of Defense - B cells - T cells - Specific Immunities 1 3 rd Line = Prophylaxis via Immunization! (a) A painting of Edward Jenner depicts a cow
Topic 8 Specific Immunity (adaptive) (18) Topics - 3 rd Line of Defense - B cells - T cells - Specific Immunities 1 3 rd Line = Prophylaxis via Immunization! (a) A painting of Edward Jenner depicts a cow
Mohamed Waheed MBBS MSc MD. Rheumatic Fever
 Mohamed Waheed MBBS MSc MD Rheumatic Fever 2 Etiology Acute rheumatic fever is a systemic disease of childhood,often recurrent that follows group A beta hemolytic streptococcal infection It is a delayed
Mohamed Waheed MBBS MSc MD Rheumatic Fever 2 Etiology Acute rheumatic fever is a systemic disease of childhood,often recurrent that follows group A beta hemolytic streptococcal infection It is a delayed
Adaptive Immunity: Specific Defenses of the Host
 17 Adaptive Immunity: Specific Defenses of the Host SLOs Differentiate between innate and adaptive immunity, and humoral and cellular immunity. Define antigen, epitope, and hapten. Explain the function
17 Adaptive Immunity: Specific Defenses of the Host SLOs Differentiate between innate and adaptive immunity, and humoral and cellular immunity. Define antigen, epitope, and hapten. Explain the function
Cellular Pathology of immunological disorders
 Cellular Pathology of immunological disorders SCBM344 Cellular and Molecular Pathology Witchuda Payuhakrit, Ph.D (Pathobiology) witchuda.pay@mahidol.ac.th Objectives Describe the etiology of immunological
Cellular Pathology of immunological disorders SCBM344 Cellular and Molecular Pathology Witchuda Payuhakrit, Ph.D (Pathobiology) witchuda.pay@mahidol.ac.th Objectives Describe the etiology of immunological
Immunology. Lecture- 8
 Immunology Lecture- 8 Immunological Disorders Immunodeficiency Autoimmune Disease Hypersensitivities Immunodeficiency 1. Immunodeficiency --> abnormal production or function of immune cells, phagocytes,
Immunology Lecture- 8 Immunological Disorders Immunodeficiency Autoimmune Disease Hypersensitivities Immunodeficiency 1. Immunodeficiency --> abnormal production or function of immune cells, phagocytes,
Rheumatic heart disease
 Rheumatic heart disease What will we discuss today? Etiology and epidemiology of rheumatic heart disease Pathogenesis of rheumatic heart disease Morphological changes in rheumatic heart disease Clinical
Rheumatic heart disease What will we discuss today? Etiology and epidemiology of rheumatic heart disease Pathogenesis of rheumatic heart disease Morphological changes in rheumatic heart disease Clinical
Immunity. Acquired immunity differs from innate immunity in specificity & memory from 1 st exposure
 Immunity (1) Non specific (innate) immunity (2) Specific (acquired) immunity Characters: (1) Non specific: does not need special recognition of the foreign cell. (2) Innate: does not need previous exposure.
Immunity (1) Non specific (innate) immunity (2) Specific (acquired) immunity Characters: (1) Non specific: does not need special recognition of the foreign cell. (2) Innate: does not need previous exposure.
Immunology Lecture 4. Clinical Relevance of the Immune System
 Immunology Lecture 4 The Well Patient: How innate and adaptive immune responses maintain health - 13, pg 169-181, 191-195. Immune Deficiency - 15 Autoimmunity - 16 Transplantation - 17, pg 260-270 Tumor
Immunology Lecture 4 The Well Patient: How innate and adaptive immune responses maintain health - 13, pg 169-181, 191-195. Immune Deficiency - 15 Autoimmunity - 16 Transplantation - 17, pg 260-270 Tumor
All animals have innate immunity, a defense active immediately upon infection Vertebrates also have adaptive immunity
 1 2 3 4 5 6 7 8 9 The Immune System All animals have innate immunity, a defense active immediately upon infection Vertebrates also have adaptive immunity Figure 43.2 In innate immunity, recognition and
1 2 3 4 5 6 7 8 9 The Immune System All animals have innate immunity, a defense active immediately upon infection Vertebrates also have adaptive immunity Figure 43.2 In innate immunity, recognition and
Anti-infectious Immunity
 Anti-infectious Immunity innate immunity barrier structures Secretory molecules Phagocytes NK cells Anatomical barriers 1. Skin and mucosa barrier 2.hemo-Spinal Fluid barrier 3. placental barrier Phagocytic
Anti-infectious Immunity innate immunity barrier structures Secretory molecules Phagocytes NK cells Anatomical barriers 1. Skin and mucosa barrier 2.hemo-Spinal Fluid barrier 3. placental barrier Phagocytic
The Immune System: Innate and Adaptive Body Defenses Outline PART 1: INNATE DEFENSES 21.1 Surface barriers act as the first line of defense to keep
 The Immune System: Innate and Adaptive Body Defenses Outline PART 1: INNATE DEFENSES 21.1 Surface barriers act as the first line of defense to keep invaders out of the body (pp. 772 773; Fig. 21.1; Table
The Immune System: Innate and Adaptive Body Defenses Outline PART 1: INNATE DEFENSES 21.1 Surface barriers act as the first line of defense to keep invaders out of the body (pp. 772 773; Fig. 21.1; Table
The Immune System. These are classified as the Innate and Adaptive Immune Responses. Innate Immunity
 The Immune System Biological mechanisms that defend an organism must be 1. triggered by a stimulus upon injury or pathogen attack 2. able to counteract the injury or invasion 3. able to recognise foreign
The Immune System Biological mechanisms that defend an organism must be 1. triggered by a stimulus upon injury or pathogen attack 2. able to counteract the injury or invasion 3. able to recognise foreign
Immune system. Aims. Immune system. Lymphatic organs. Inflammation. Natural immune system. Adaptive immune system
 Aims Immune system Lymphatic organs Inflammation Natural immune system Adaptive immune system Major histocompatibility complex (MHC) Disorders of the immune system 1 2 Immune system Lymphoid organs Immune
Aims Immune system Lymphatic organs Inflammation Natural immune system Adaptive immune system Major histocompatibility complex (MHC) Disorders of the immune system 1 2 Immune system Lymphoid organs Immune
Topics in Parasitology BLY Vertebrate Immune System
 Topics in Parasitology BLY 533-2008 Vertebrate Immune System V. Vertebrate Immune System A. Non-specific defenses against pathogens 1. Skin - physical barrier a. Tough armor protein KERATIN b. Surface
Topics in Parasitology BLY 533-2008 Vertebrate Immune System V. Vertebrate Immune System A. Non-specific defenses against pathogens 1. Skin - physical barrier a. Tough armor protein KERATIN b. Surface
The Lymphatic System and Body Defenses
 PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Lymphatic System and Body Defenses 12PART B Adaptive Defense System: Third Line of Defense Immune
PowerPoint Lecture Slide Presentation by Patty Bostwick-Taylor, Florence-Darlington Technical College The Lymphatic System and Body Defenses 12PART B Adaptive Defense System: Third Line of Defense Immune
Fluid movement in capillaries. Not all fluid is reclaimed at the venous end of the capillaries; that is the job of the lymphatic system
 Capillary exchange Fluid movement in capillaries Not all fluid is reclaimed at the venous end of the capillaries; that is the job of the lymphatic system Lymphatic vessels Lymphatic capillaries permeate
Capillary exchange Fluid movement in capillaries Not all fluid is reclaimed at the venous end of the capillaries; that is the job of the lymphatic system Lymphatic vessels Lymphatic capillaries permeate
محاضرة مناعت مدرس المادة :ا.م. هدى عبدالهادي علي النصراوي Immunity to Infectious Diseases
 محاضرة مناعت مدرس المادة :ا.م. هدى عبدالهادي علي النصراوي Immunity to Infectious Diseases Immunity to infection depends on a combination of innate mechanisms (phagocytosis, complement, etc.) and antigen
محاضرة مناعت مدرس المادة :ا.م. هدى عبدالهادي علي النصراوي Immunity to Infectious Diseases Immunity to infection depends on a combination of innate mechanisms (phagocytosis, complement, etc.) and antigen
chapter 17: specific/adaptable defenses of the host: the immune response
 chapter 17: specific/adaptable defenses of the host: the immune response defense against infection & illness body defenses innate/ non-specific adaptable/ specific epithelium, fever, inflammation, complement,
chapter 17: specific/adaptable defenses of the host: the immune response defense against infection & illness body defenses innate/ non-specific adaptable/ specific epithelium, fever, inflammation, complement,
C. Incorrect! MHC class I molecules are not involved in the process of bridging in ADCC.
 Immunology - Problem Drill 13: T- Cell Mediated Immunity Question No. 1 of 10 1. During Antibody-dependent cell mediated cytotoxicity (ADCC), the antibody acts like a bridge between the specific antigen
Immunology - Problem Drill 13: T- Cell Mediated Immunity Question No. 1 of 10 1. During Antibody-dependent cell mediated cytotoxicity (ADCC), the antibody acts like a bridge between the specific antigen
Chapter 22: The Lymphatic System and Immunity
 Bio40C schedule Lecture Immune system Lab Quiz 2 this week; bring a scantron! Study guide on my website (see lab assignments) Extra credit Critical thinking questions at end of chapters 5 pts/chapter Due
Bio40C schedule Lecture Immune system Lab Quiz 2 this week; bring a scantron! Study guide on my website (see lab assignments) Extra credit Critical thinking questions at end of chapters 5 pts/chapter Due
The Adaptive Immune Responses
 The Adaptive Immune Responses The two arms of the immune responses are; 1) the cell mediated, and 2) the humoral responses. In this chapter we will discuss the two responses in detail and we will start
The Adaptive Immune Responses The two arms of the immune responses are; 1) the cell mediated, and 2) the humoral responses. In this chapter we will discuss the two responses in detail and we will start
SINGLE CHOICE. 5. The gamma invariant chain binds to this molecule during its intracytoplasmic transport. A TCR B BCR C MHC II D MHC I E FcγR
 A Name: Group: SINGLE CHOICE 1. Which is the most important ligand of TLR5? A endospore B flagellin C polysaccharide capsule D DNA E pilus 2. The antibody-binding site is formed primarily by... A the constant
A Name: Group: SINGLE CHOICE 1. Which is the most important ligand of TLR5? A endospore B flagellin C polysaccharide capsule D DNA E pilus 2. The antibody-binding site is formed primarily by... A the constant
Chagas disease. (American trypanosomiasis)
") Chagas disease (American trypanosomiasis) Epidemiology 7 to 8 million people worldwide are infected Endemic in Latin America and South America USA, Canada, Europe http://www.who.int/mediacentre/factsheets/fs340/en/index.html
Chagas disease (American trypanosomiasis) Epidemiology 7 to 8 million people worldwide are infected Endemic in Latin America and South America USA, Canada, Europe http://www.who.int/mediacentre/factsheets/fs340/en/index.html
Overview of the immune system
 Overview of the immune system Immune system Innate (nonspecific) 1 st line of defense Adaptive (specific) 2 nd line of defense Cellular components Humoral components Cellular components Humoral components
Overview of the immune system Immune system Innate (nonspecific) 1 st line of defense Adaptive (specific) 2 nd line of defense Cellular components Humoral components Cellular components Humoral components
I. Critical Vocabulary
 I. Critical Vocabulary A. Immune System: a set of glands, tissues, cells, and dissolved proteins that combine to defend against non-self entities B. Antigen: any non-self chemical that triggers an immune
I. Critical Vocabulary A. Immune System: a set of glands, tissues, cells, and dissolved proteins that combine to defend against non-self entities B. Antigen: any non-self chemical that triggers an immune
11/25/2017. THE IMMUNE SYSTEM Chapter 43 IMMUNITY INNATE IMMUNITY EXAMPLE IN INSECTS BARRIER DEFENSES INNATE IMMUNITY OF VERTEBRATES
 THE IMMUNE SYSTEM Chapter 43 IMMUNITY INNATE IMMUNITY EXAMPLE IN INSECTS Exoskeleton made of chitin forms the first barrier to pathogens Digestive system is protected by a chitin-based barrier and lysozyme,
THE IMMUNE SYSTEM Chapter 43 IMMUNITY INNATE IMMUNITY EXAMPLE IN INSECTS Exoskeleton made of chitin forms the first barrier to pathogens Digestive system is protected by a chitin-based barrier and lysozyme,
The Adaptive Immune Response. B-cells
 The Adaptive Immune Response B-cells The innate immune system provides immediate protection. The adaptive response takes time to develop and is antigen specific. Activation of B and T lymphocytes Naive
The Adaptive Immune Response B-cells The innate immune system provides immediate protection. The adaptive response takes time to develop and is antigen specific. Activation of B and T lymphocytes Naive
Blood and Immune system Acquired Immunity
 Blood and Immune system Acquired Immunity Immunity Acquired (Adaptive) Immunity Defensive mechanisms include : 1) Innate immunity (Natural or Non specific) 2) Acquired immunity (Adaptive or Specific) Cell-mediated
Blood and Immune system Acquired Immunity Immunity Acquired (Adaptive) Immunity Defensive mechanisms include : 1) Innate immunity (Natural or Non specific) 2) Acquired immunity (Adaptive or Specific) Cell-mediated
1. The scavenger receptor, CD36, functions as a coreceptor for which TLR? a. TLR ½ b. TLR 3 c. TLR 4 d. TLR 2/6
 Allergy and Immunology Review Corner: Cellular and Molecular Immunology, 8th Edition By Abul K. Abbas, MBBS, Andrew H. H. Lichtman, MD, PhD and Shiv Pillai, MBBS, PhD. Chapter 4 (pages 62-74): Innate Immunity
Allergy and Immunology Review Corner: Cellular and Molecular Immunology, 8th Edition By Abul K. Abbas, MBBS, Andrew H. H. Lichtman, MD, PhD and Shiv Pillai, MBBS, PhD. Chapter 4 (pages 62-74): Innate Immunity
Chapter 24 The Immune System
 Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
Chapter 24 The Immune System The Immune System Layered defense system The skin and chemical barriers The innate and adaptive immune systems Immunity The body s ability to recognize and destroy specific
Principles of Adaptive Immunity
 Principles of Adaptive Immunity Chapter 3 Parham Hans de Haard 17 th of May 2010 Agenda Recognition molecules of adaptive immune system Features adaptive immune system Immunoglobulins and T-cell receptors
Principles of Adaptive Immunity Chapter 3 Parham Hans de Haard 17 th of May 2010 Agenda Recognition molecules of adaptive immune system Features adaptive immune system Immunoglobulins and T-cell receptors
HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A
 HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A HYPERSENSITIVITY REACTIONS Are exaggerated immune response upon antigenic stimulation Individuals who have been previously exposed to an antigen are said
HYPERSENSITIVITY REACTIONS D R S H O AI B R AZ A HYPERSENSITIVITY REACTIONS Are exaggerated immune response upon antigenic stimulation Individuals who have been previously exposed to an antigen are said
The Major Histocompatibility Complex (MHC)
") The Major Histocompatibility Complex (MHC) An introduction to adaptive immune system before we discuss MHC B cells The main cells of adaptive immune system are: -B cells -T cells B cells: Recognize antigens
The Major Histocompatibility Complex (MHC) An introduction to adaptive immune system before we discuss MHC B cells The main cells of adaptive immune system are: -B cells -T cells B cells: Recognize antigens
ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY
 ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY The recognition of specific antigen by naïve T cell induces its own activation and effector phases. T helper cells recognize peptide antigens through
ACTIVATION OF T LYMPHOCYTES AND CELL MEDIATED IMMUNITY The recognition of specific antigen by naïve T cell induces its own activation and effector phases. T helper cells recognize peptide antigens through
Chapter 35 Active Reading Guide The Immune System
 Name: AP Biology Mr. Croft Chapter 35 Active Reading Guide The Immune System Section 1 Phagocytosis plays an important role in the immune systems of both invertebrates and vertebrates. Review the process
Name: AP Biology Mr. Croft Chapter 35 Active Reading Guide The Immune System Section 1 Phagocytosis plays an important role in the immune systems of both invertebrates and vertebrates. Review the process
Immunity and Infection. Chapter 17
 Immunity and Infection Chapter 17 The Chain of Infection Transmitted through a chain of infection (six links) Pathogen: Disease causing microorganism Reservoir: Natural environment of the pathogen Portal
Immunity and Infection Chapter 17 The Chain of Infection Transmitted through a chain of infection (six links) Pathogen: Disease causing microorganism Reservoir: Natural environment of the pathogen Portal
CHAPTER-VII IMMUNOLOGY R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR.
 CHAPTER-VII IMMUNOLOGY R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR. The Immune Response Immunity: Free from burden. Ability of an
CHAPTER-VII IMMUNOLOGY R.KAVITHA, M.PHARM, LECTURER, DEPARTMENT OF PHARMACEUTICS, SRM COLLEGE OF PHARMACY, SRM UNIVERSITY, KATTANKULATHUR. The Immune Response Immunity: Free from burden. Ability of an
Prof. Ibtesam Kamel Afifi Professor of Medical Microbiology & Immunology
 By Prof. Ibtesam Kamel Afifi Professor of Medical Microbiology & Immunology Lecture objectives: At the end of the lecture you should be able to: Enumerate features that characterize acquired immune response
By Prof. Ibtesam Kamel Afifi Professor of Medical Microbiology & Immunology Lecture objectives: At the end of the lecture you should be able to: Enumerate features that characterize acquired immune response
Immune System AP SBI4UP
 Immune System AP SBI4UP TYPES OF IMMUNITY INNATE IMMUNITY ACQUIRED IMMUNITY EXTERNAL DEFENCES INTERNAL DEFENCES HUMORAL RESPONSE Skin Phagocytic Cells CELL- MEDIATED RESPONSE Mucus layer Antimicrobial
Immune System AP SBI4UP TYPES OF IMMUNITY INNATE IMMUNITY ACQUIRED IMMUNITY EXTERNAL DEFENCES INTERNAL DEFENCES HUMORAL RESPONSE Skin Phagocytic Cells CELL- MEDIATED RESPONSE Mucus layer Antimicrobial
Title: NATURAL KILLER CELL FUNCTIONS AND SURFACE RECEPTORS
 LECTURE: 14 Title: NATURAL KILLER CELL FUNCTIONS AND SURFACE RECEPTORS LEARNING OBJECTIVES: The student should be able to: Describe the general morphology of the NK-cells. Enumerate the different functions
LECTURE: 14 Title: NATURAL KILLER CELL FUNCTIONS AND SURFACE RECEPTORS LEARNING OBJECTIVES: The student should be able to: Describe the general morphology of the NK-cells. Enumerate the different functions
The Immune System is the Third Line of Defense Against Infection. Components of Human Immune System
 Chapter 17: Specific Host Defenses: The Immune Response The Immune Response Immunity: Free from burden. Ability of an organism to recognize and defend itself against specific pathogens or antigens. Immune
Chapter 17: Specific Host Defenses: The Immune Response The Immune Response Immunity: Free from burden. Ability of an organism to recognize and defend itself against specific pathogens or antigens. Immune
The Immune System All animals have innate immunity, a defense active immediately
 The Immune System All animals have innate immunity, a defense active immediately upon infection Vertebrates also have adaptive immunity Figure 43.2 INNATE IMMUNITY (all animals) Recognition of traits shared
The Immune System All animals have innate immunity, a defense active immediately upon infection Vertebrates also have adaptive immunity Figure 43.2 INNATE IMMUNITY (all animals) Recognition of traits shared
Defense mechanism against pathogens
 Defense mechanism against pathogens Immune System What is immune system? Cells and organs within an animal s body that contribute to immune defenses against pathogens ( ) Bacteria -Major entry points ;open
Defense mechanism against pathogens Immune System What is immune system? Cells and organs within an animal s body that contribute to immune defenses against pathogens ( ) Bacteria -Major entry points ;open
Hematopoiesis. Hematopoiesis. Hematopoiesis
 Chapter. Cells and Organs of the Immune System Hematopoiesis Hematopoiesis- formation and development of WBC and RBC bone marrow. Hematopoietic stem cell- give rise to any blood cells (constant number,
Chapter. Cells and Organs of the Immune System Hematopoiesis Hematopoiesis- formation and development of WBC and RBC bone marrow. Hematopoietic stem cell- give rise to any blood cells (constant number,
VALVULAR HEART DISEASE
 VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
Overview of the Lymphoid System
 Overview of the Lymphoid System The Lymphoid System Protects us against disease Lymphoid system cells respond to Environmental pathogens Toxins Abnormal body cells, such as cancers Overview of the Lymphoid
Overview of the Lymphoid System The Lymphoid System Protects us against disease Lymphoid system cells respond to Environmental pathogens Toxins Abnormal body cells, such as cancers Overview of the Lymphoid
Unit 5 The Human Immune Response to Infection
 Unit 5 The Human Immune Response to Infection Unit 5-page 1 FOM Chapter 21 Resistance and the Immune System: Innate Immunity Preview: In Chapter 21, we will learn about the branch of the immune system
Unit 5 The Human Immune Response to Infection Unit 5-page 1 FOM Chapter 21 Resistance and the Immune System: Innate Immunity Preview: In Chapter 21, we will learn about the branch of the immune system
NOTES: CH 43, part 2 Immunity; Immune Disruptions ( )
") NOTES: CH 43, part 2 Immunity; Immune Disruptions (43.3-43.4) Activated B & T Lymphocytes produce: CELL-MEDIATED IMMUNE RESPONSE: involves specialized T cells destroying infected host cells HUMORAL IMMUNE
NOTES: CH 43, part 2 Immunity; Immune Disruptions (43.3-43.4) Activated B & T Lymphocytes produce: CELL-MEDIATED IMMUNE RESPONSE: involves specialized T cells destroying infected host cells HUMORAL IMMUNE
The Innate Immune Response
 The Innate Immune Response FUNCTIONS OF THE IMMUNE SYSTEM: Recognize, destroy and clear a diversity of pathogens. Initiate tissue and wound healing processes. Recognize and clear damaged self components.
The Innate Immune Response FUNCTIONS OF THE IMMUNE SYSTEM: Recognize, destroy and clear a diversity of pathogens. Initiate tissue and wound healing processes. Recognize and clear damaged self components.
For questions 1-5, match the following with their correct descriptions. (24-39) A. Class I B. Class II C. Class III D. TH1 E. TH2
 A. Class I B. Class II C. Class III D. TH1 E. TH2") Questions Made by SI ATTENDEES!! :) Page 1 of 6 Student-Made Practice Exam Activity All questions, answers, and slide numbers are based off of Monday s SI activity, where students/attendees created possible
Questions Made by SI ATTENDEES!! :) Page 1 of 6 Student-Made Practice Exam Activity All questions, answers, and slide numbers are based off of Monday s SI activity, where students/attendees created possible
RAISON D ETRE OF THE IMMUNE SYSTEM:
 RAISON D ETRE OF THE IMMUNE SYSTEM: To Distinguish Self from Non-Self Thereby Protecting Us From Our Hostile Environment. Innate Immunity Acquired Immunity Innate immunity: (Antigen nonspecific) defense
RAISON D ETRE OF THE IMMUNE SYSTEM: To Distinguish Self from Non-Self Thereby Protecting Us From Our Hostile Environment. Innate Immunity Acquired Immunity Innate immunity: (Antigen nonspecific) defense
Introduction to Immunopathology
 MICR2209 Introduction to Immunopathology Dr Allison Imrie 1 Allergy and Hypersensitivity Adaptive immune responses can sometimes be elicited by antigens not associated with infectious agents, and this
MICR2209 Introduction to Immunopathology Dr Allison Imrie 1 Allergy and Hypersensitivity Adaptive immune responses can sometimes be elicited by antigens not associated with infectious agents, and this
ANATOMY OF THE IMMUNE SYSTEM
 Immunity Learning objectives Explain what triggers an immune response and where in the body the immune response occurs. Understand how the immune system handles exogenous and endogenous antigen differently.
Immunity Learning objectives Explain what triggers an immune response and where in the body the immune response occurs. Understand how the immune system handles exogenous and endogenous antigen differently.
Streptococcus pyogenes
 Streptococcus pyogenes From Wikipedia, the free encyclopedia Streptococcus pyogenes S. pyogenes bacteria at 900x magnification. Scientific classification Kingdom: Eubacteria Phylum: Firmicutes Class: Cocci
Streptococcus pyogenes From Wikipedia, the free encyclopedia Streptococcus pyogenes S. pyogenes bacteria at 900x magnification. Scientific classification Kingdom: Eubacteria Phylum: Firmicutes Class: Cocci
Chapter 21: Innate and Adaptive Body Defenses
 Chapter 21: Innate and Adaptive Body Defenses I. 2 main types of body defenses A. Innate (nonspecific) defense: not to a specific microorganism or substance B. Adaptive (specific) defense: immunity to
Chapter 21: Innate and Adaptive Body Defenses I. 2 main types of body defenses A. Innate (nonspecific) defense: not to a specific microorganism or substance B. Adaptive (specific) defense: immunity to
Physiology Unit 3. ADAPTIVE IMMUNITY The Specific Immune Response
 Physiology Unit 3 ADAPTIVE IMMUNITY The Specific Immune Response In Physiology Today The Adaptive Arm of the Immune System Specific Immune Response Internal defense against a specific pathogen Acquired
Physiology Unit 3 ADAPTIVE IMMUNITY The Specific Immune Response In Physiology Today The Adaptive Arm of the Immune System Specific Immune Response Internal defense against a specific pathogen Acquired
Scott Abrams, Ph.D. Professor of Oncology, x4375 Kuby Immunology SEVENTH EDITION
 Scott Abrams, Ph.D. Professor of Oncology, x4375 scott.abrams@roswellpark.org Kuby Immunology SEVENTH EDITION CHAPTER 13 Effector Responses: Cell- and Antibody-Mediated Immunity Copyright 2013 by W. H.
Scott Abrams, Ph.D. Professor of Oncology, x4375 scott.abrams@roswellpark.org Kuby Immunology SEVENTH EDITION CHAPTER 13 Effector Responses: Cell- and Antibody-Mediated Immunity Copyright 2013 by W. H.
1. Lymphatic vessels recover about of the fluid filtered by capillaries. A. ~1% C. ~25% E. ~85% B. ~10% D. ~50%
 BIOL2030 Huaman A&P II -- Exam 3 -- XXXX -- Form A Name: 1. Lymphatic vessels recover about of the fluid filtered by capillaries. A. ~1% C. ~25% E. ~85% B. ~10% D. ~50% 2. Special lymphatic vessels called
BIOL2030 Huaman A&P II -- Exam 3 -- XXXX -- Form A Name: 1. Lymphatic vessels recover about of the fluid filtered by capillaries. A. ~1% C. ~25% E. ~85% B. ~10% D. ~50% 2. Special lymphatic vessels called
M.Sc. III Semester Biotechnology End Semester Examination, 2013 Model Answer LBTM: 302 Advanced Immunology
 Code : AS-2246 M.Sc. III Semester Biotechnology End Semester Examination, 2013 Model Answer LBTM: 302 Advanced Immunology A. Select one correct option for each of the following questions:- 2X10=10 1. (b)
Code : AS-2246 M.Sc. III Semester Biotechnology End Semester Examination, 2013 Model Answer LBTM: 302 Advanced Immunology A. Select one correct option for each of the following questions:- 2X10=10 1. (b)
Properties & Overview of IRs Dr. Nasser M. Kaplan JUST, Jordan. 10-Jul-16 NM Kaplan 1
 Properties & Overview of IRs Dr. Nasser M. Kaplan JUST, Jordan 10-Jul-16 NM Kaplan 1 Major components of IS & their properties Definitions IS = cells & molecules responsible for: 1- Physiologic; protective
Properties & Overview of IRs Dr. Nasser M. Kaplan JUST, Jordan 10-Jul-16 NM Kaplan 1 Major components of IS & their properties Definitions IS = cells & molecules responsible for: 1- Physiologic; protective
Nonspecific External Barriers skin, mucous membranes
 Immune system Chapter 36 BI 103 Plant-Animal A&P Levels of Defense Against Disease Nonspecific External Barriers skin, mucous membranes Physical barriers? Brainstorm with a partner If these barriers are
Immune system Chapter 36 BI 103 Plant-Animal A&P Levels of Defense Against Disease Nonspecific External Barriers skin, mucous membranes Physical barriers? Brainstorm with a partner If these barriers are
Introduction to Immunology and the Immune System
 Introduction to Immunology and the Immune System Assistant professor Dr. Aida R. Al-Derzi M.B.Ch.B; M.Sc; FICM/Path Dept. of Microbiology/College of Medicine/Baghdad University Introduction to Immunology
Introduction to Immunology and the Immune System Assistant professor Dr. Aida R. Al-Derzi M.B.Ch.B; M.Sc; FICM/Path Dept. of Microbiology/College of Medicine/Baghdad University Introduction to Immunology
Overview: The immune responses of animals can be divided into innate immunity and acquired immunity.
 GUIDED READING - Ch. 43 - THE IMMUNE SYSTEM NAME: Please print out these pages and HANDWRITE the answers directly on the printouts. Typed work or answers on separate sheets of paper will not be accepted.
GUIDED READING - Ch. 43 - THE IMMUNE SYSTEM NAME: Please print out these pages and HANDWRITE the answers directly on the printouts. Typed work or answers on separate sheets of paper will not be accepted.
How the Innate Immune System Profiles Pathogens
 How the Innate Immune System Profiles Pathogens Receptors on macrophages, neutrophils, dendritic cells for bacteria and viruses Broad specificity - Two main groups of bacteria: gram positive, gram-negative
How the Innate Immune System Profiles Pathogens Receptors on macrophages, neutrophils, dendritic cells for bacteria and viruses Broad specificity - Two main groups of bacteria: gram positive, gram-negative
Pathophysiologic Basis of Autoimmune Disorders
 Pathophysiologic Basis of Autoimmune Disorders Linda Felver, Ph.D., R.N. Associate Professor School of Nursing Oregon Health & Science University The immune system has two arms: Adaptive (Acquired) Immune
Pathophysiologic Basis of Autoimmune Disorders Linda Felver, Ph.D., R.N. Associate Professor School of Nursing Oregon Health & Science University The immune system has two arms: Adaptive (Acquired) Immune
AGAINST VIRAL INFECTIONS. Identify the types of immunity involve in the mechanisms of protection against viral infections.
 LECTURE: 02 Title: THE IMMUNOLOGICAL PROTECTIVE MECHANISMS AGAINST VIRAL INFECTIONS LEARNING OBJECTIVES: The student should be able to: Identify the types of immunity involve in the mechanisms of protection
LECTURE: 02 Title: THE IMMUNOLOGICAL PROTECTIVE MECHANISMS AGAINST VIRAL INFECTIONS LEARNING OBJECTIVES: The student should be able to: Identify the types of immunity involve in the mechanisms of protection
COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16
 COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16 Tumor Immunology M. Nagarkatti Teaching Objectives: Introduction to Cancer Immunology Know the antigens expressed by cancer cells Understand
COURSE: Medical Microbiology, PAMB 650/720 - Fall 2008 Lecture 16 Tumor Immunology M. Nagarkatti Teaching Objectives: Introduction to Cancer Immunology Know the antigens expressed by cancer cells Understand
immunity produced by an encounter with an antigen; provides immunologic memory. active immunity clumping of (foreign) cells; induced by crosslinking
 cells; induced by crosslinking") active immunity agglutination allografts immunity produced by an encounter with an antigen; provides immunologic memory. clumping of (foreign) cells; induced by crosslinking of antigenantibody complexes.
active immunity agglutination allografts immunity produced by an encounter with an antigen; provides immunologic memory. clumping of (foreign) cells; induced by crosslinking of antigenantibody complexes.
Warm-up. Parts of the Immune system. Disease transmission. Disease transmission. Why an immune system? Chapter 43 3/9/2012.
 Warm-up Objective: Explain how antigens react with specific lymphocytes to induce immune response and immunological memory. Warm-up: Which of the following would normally contain blood with the least amount
Warm-up Objective: Explain how antigens react with specific lymphocytes to induce immune response and immunological memory. Warm-up: Which of the following would normally contain blood with the least amount
I. Lines of Defense Pathogen: Table 1: Types of Immune Mechanisms. Table 2: Innate Immunity: First Lines of Defense
 I. Lines of Defense Pathogen: Table 1: Types of Immune Mechanisms Table 2: Innate Immunity: First Lines of Defense Innate Immunity involves nonspecific physical & chemical barriers that are adapted for
I. Lines of Defense Pathogen: Table 1: Types of Immune Mechanisms Table 2: Innate Immunity: First Lines of Defense Innate Immunity involves nonspecific physical & chemical barriers that are adapted for
Diseases-causing agents, pathogens, can produce infections within the body.
 BIO 212: ANATOMY & PHYSIOLOGY II 1 CHAPTER 16 Lecture: Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. LYMPHATIC and IMMUNE Systems Body Defenses Against
BIO 212: ANATOMY & PHYSIOLOGY II 1 CHAPTER 16 Lecture: Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. LYMPHATIC and IMMUNE Systems Body Defenses Against
Immune response Lecture (9)
") Immune response Lecture (9) Dr.Baha,Hamdi.AL-Amiedie Ph.D.Microbiolgy Primary Immune Response: Primary Immune Response to initial antigenic stimulus is slow, sluggish, short live with low antibody titer
Immune response Lecture (9) Dr.Baha,Hamdi.AL-Amiedie Ph.D.Microbiolgy Primary Immune Response: Primary Immune Response to initial antigenic stimulus is slow, sluggish, short live with low antibody titer
Campbell's Biology: Concepts and Connections, 7e (Reece et al.) Chapter 24 The Immune System Multiple-Choice Questions
 Chapter 24 The Immune System Multiple-Choice Questions") Campbell's Biology: Concepts and Connections, 7e (Reece et al.) Chapter 24 The Immune System 24.1 Multiple-Choice Questions 1) The body's innate defenses against infection include A) several nonspecific
Campbell's Biology: Concepts and Connections, 7e (Reece et al.) Chapter 24 The Immune System 24.1 Multiple-Choice Questions 1) The body's innate defenses against infection include A) several nonspecific
Body Defense Mechanisms
 BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 13 Body Defense Mechanisms Lecture Presentation Anne Gasc Hawaii Pacific University and University of
BIOLOGY OF HUMANS Concepts, Applications, and Issues Fifth Edition Judith Goodenough Betty McGuire 13 Body Defense Mechanisms Lecture Presentation Anne Gasc Hawaii Pacific University and University of
Medical Bacteriology- Lecture: 6
 Medical Bacteriology- Lecture: 6 Gram Positive Cocci Streptococcal Disease Streptococcus pyogenes Classification of Streptococci based on (1- Hemolysis reactions on blood agar) (Brown in 1903) The type
Medical Bacteriology- Lecture: 6 Gram Positive Cocci Streptococcal Disease Streptococcus pyogenes Classification of Streptococci based on (1- Hemolysis reactions on blood agar) (Brown in 1903) The type
General Overview of Immunology. Kimberly S. Schluns, Ph.D. Associate Professor Department of Immunology UT MD Anderson Cancer Center
 General Overview of Immunology Kimberly S. Schluns, Ph.D. Associate Professor Department of Immunology UT MD Anderson Cancer Center Objectives Describe differences between innate and adaptive immune responses
General Overview of Immunology Kimberly S. Schluns, Ph.D. Associate Professor Department of Immunology UT MD Anderson Cancer Center Objectives Describe differences between innate and adaptive immune responses
~ons~ecific Bod~ Defenses and Immunity
 ~ons~ecific Bod~ Defenses and Immunity The human body continually attempts to maintain homeostasis by counteracting harmful or disease-producing organisms called pathoqens or the toxins they produce. The
~ons~ecific Bod~ Defenses and Immunity The human body continually attempts to maintain homeostasis by counteracting harmful or disease-producing organisms called pathoqens or the toxins they produce. The
3. Lymphocyte proliferation (fig. 15.4): Clones of responder cells and memory cells are derived from B cells and T cells.
: Clones of responder cells and memory cells are derived from B cells and T cells.") Chapter 15 Adaptive, Specific Immunity and Immunization* *Lecture notes are to be used as a study guide only and do not represent the comprehensive information you will need to know for the exams. Specific
Chapter 15 Adaptive, Specific Immunity and Immunization* *Lecture notes are to be used as a study guide only and do not represent the comprehensive information you will need to know for the exams. Specific
Chapter 13 Lymphatic and Immune Systems
 The Chapter 13 Lymphatic and Immune Systems 1 The Lymphatic Vessels Lymphoid Organs Three functions contribute to homeostasis 1. Return excess tissue fluid to the bloodstream 2. Help defend the body against
The Chapter 13 Lymphatic and Immune Systems 1 The Lymphatic Vessels Lymphoid Organs Three functions contribute to homeostasis 1. Return excess tissue fluid to the bloodstream 2. Help defend the body against
Immunology for the Rheumatologist
 Immunology for the Rheumatologist Rheumatologists frequently deal with the immune system gone awry, rarely studying normal immunology. This program is an overview and discussion of the function of the
Immunology for the Rheumatologist Rheumatologists frequently deal with the immune system gone awry, rarely studying normal immunology. This program is an overview and discussion of the function of the
Cell Mediated Immunity CELL MEDIATED IMMUNITY. Basic Elements of Cell Mediated Immunity (CMI) Antibody-dependent cell-mediated cytotoxicity (ADCC)
 Antibody-dependent cell-mediated cytotoxicity (ADCC)") Chapter 16 CELL MEDIATED IMMUNITY Cell Mediated Immunity Also known as Cellular Immunity or CMI The effector phase T cells Specificity for immune recognition reactions TH provide cytokines CTLs do the
Chapter 16 CELL MEDIATED IMMUNITY Cell Mediated Immunity Also known as Cellular Immunity or CMI The effector phase T cells Specificity for immune recognition reactions TH provide cytokines CTLs do the
Structure and Function of Antigen Recognition Molecules
 MICR2209 Structure and Function of Antigen Recognition Molecules Dr Allison Imrie allison.imrie@uwa.edu.au 1 Synopsis: In this lecture we will examine the major receptors used by cells of the innate and
MICR2209 Structure and Function of Antigen Recognition Molecules Dr Allison Imrie allison.imrie@uwa.edu.au 1 Synopsis: In this lecture we will examine the major receptors used by cells of the innate and
Macrophage Activation & Cytokine Release. Dendritic Cells & Antigen Presentation. Neutrophils & Innate Defense
 Macrophage Activation & Cytokine Release Dendritic Cells & Antigen Presentation Neutrophils & Innate Defense Neutrophils Polymorphonuclear cells (PMNs) are recruited to the site of infection where they
Macrophage Activation & Cytokine Release Dendritic Cells & Antigen Presentation Neutrophils & Innate Defense Neutrophils Polymorphonuclear cells (PMNs) are recruited to the site of infection where they
What is Autoimmunity?
 Autoimmunity What is Autoimmunity? Robert Beatty MCB150 Autoimmunity is an immune response to self antigens that results in disease. The immune response to self is a result of a breakdown in immune tolerance.
Autoimmunity What is Autoimmunity? Robert Beatty MCB150 Autoimmunity is an immune response to self antigens that results in disease. The immune response to self is a result of a breakdown in immune tolerance.
What is Autoimmunity?
 Autoimmunity What is Autoimmunity? Robert Beatty MCB150 Autoimmunity is an immune response to self antigens that results in disease. The immune response to self is a result of a breakdown in immune tolerance.
Autoimmunity What is Autoimmunity? Robert Beatty MCB150 Autoimmunity is an immune response to self antigens that results in disease. The immune response to self is a result of a breakdown in immune tolerance.
Immunology lecture: 14. Cytokines: Main source: Fibroblast, but actually it can be produced by other types of cells
 Immunology lecture: 14 Cytokines: 1)Interferons"IFN" : 2 types Type 1 : IFN-Alpha : Main source: Macrophages IFN-Beta: Main source: Fibroblast, but actually it can be produced by other types of cells **There
Immunology lecture: 14 Cytokines: 1)Interferons"IFN" : 2 types Type 1 : IFN-Alpha : Main source: Macrophages IFN-Beta: Main source: Fibroblast, but actually it can be produced by other types of cells **There
LYMPHOCYTES & IMMUNOGLOBULINS. Dr Mere Kende, Lecturer SMHS
 LYMPHOCYTES & IMMUNOGLOBULINS Dr Mere Kende, Lecturer SMHS Immunity Immune- protection against dangers of non-self/invader eg organism 3 components of immune system 1 st line: skin/mucosa/cilia/hair/saliva/fatty
LYMPHOCYTES & IMMUNOGLOBULINS Dr Mere Kende, Lecturer SMHS Immunity Immune- protection against dangers of non-self/invader eg organism 3 components of immune system 1 st line: skin/mucosa/cilia/hair/saliva/fatty
WHY IS THIS IMPORTANT?
 CHAPTER 16 THE ADAPTIVE IMMUNE RESPONSE WHY IS THIS IMPORTANT? The adaptive immune system protects us from many infections The adaptive immune system has memory so we are not infected by the same pathogen
CHAPTER 16 THE ADAPTIVE IMMUNE RESPONSE WHY IS THIS IMPORTANT? The adaptive immune system protects us from many infections The adaptive immune system has memory so we are not infected by the same pathogen
Chapter 24 The Immune System
 Chapter 24 The Immune System PowerPoint Lectures for Biology: Concepts & Connections, Sixth Edition Campbell, Reece, Taylor, Simon, and Dickey Lecture by Edward J. Zalisko Introduction: The Kissing Disease?!?
Chapter 24 The Immune System PowerPoint Lectures for Biology: Concepts & Connections, Sixth Edition Campbell, Reece, Taylor, Simon, and Dickey Lecture by Edward J. Zalisko Introduction: The Kissing Disease?!?
RAISON D ETRE OF THE IMMUNE SYSTEM:
 RAISON D ETRE OF THE IMMUNE SYSTEM: To Distinguish Self from Non-Self Thereby Protecting Us From Our Hostile Environment. Innate Immunity Adaptive Immunity Innate immunity: (Antigen - nonspecific) defense
RAISON D ETRE OF THE IMMUNE SYSTEM: To Distinguish Self from Non-Self Thereby Protecting Us From Our Hostile Environment. Innate Immunity Adaptive Immunity Innate immunity: (Antigen - nonspecific) defense
Antigen Presentation and T Lymphocyte Activation. Abul K. Abbas UCSF. FOCiS
 1 Antigen Presentation and T Lymphocyte Activation Abul K. Abbas UCSF FOCiS 2 Lecture outline Dendritic cells and antigen presentation The role of the MHC T cell activation Costimulation, the B7:CD28 family
1 Antigen Presentation and T Lymphocyte Activation Abul K. Abbas UCSF FOCiS 2 Lecture outline Dendritic cells and antigen presentation The role of the MHC T cell activation Costimulation, the B7:CD28 family
Guided Reading Activities
 Name Period Chapter 24: The Immune System Guided Reading Activities Big idea: Innate immunity Answer the following questions as you read modules 24.1 24.2: 1. Bacteria, viruses, and other microorganisms
Name Period Chapter 24: The Immune System Guided Reading Activities Big idea: Innate immunity Answer the following questions as you read modules 24.1 24.2: 1. Bacteria, viruses, and other microorganisms
IMMUNITY AND DISEASE II
 IMMUNITY AND DISEASE II A. Evolution of the immune system. 1. Figure 1--57.25, p. 1167 from Raven and Johnson Biology 6 th ed. shows how the immune system evolved. Figure 1. How the immune system evolved.
IMMUNITY AND DISEASE II A. Evolution of the immune system. 1. Figure 1--57.25, p. 1167 from Raven and Johnson Biology 6 th ed. shows how the immune system evolved. Figure 1. How the immune system evolved.
1. Overview of Adaptive Immunity
 Chapter 17A: Adaptive Immunity Part I 1. Overview of Adaptive Immunity 2. T and B Cell Production 3. Antigens & Antigen Presentation 4. Helper T cells 1. Overview of Adaptive Immunity The Nature of Adaptive
Chapter 17A: Adaptive Immunity Part I 1. Overview of Adaptive Immunity 2. T and B Cell Production 3. Antigens & Antigen Presentation 4. Helper T cells 1. Overview of Adaptive Immunity The Nature of Adaptive
I. Defense Mechanisms Chapter 15
 10/24/11 I. Defense Mechanisms Chapter 15 Immune System Lecture PowerPoint Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Defense Mechanisms Protect against
10/24/11 I. Defense Mechanisms Chapter 15 Immune System Lecture PowerPoint Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Defense Mechanisms Protect against
The Immune System. by Dr. Carmen Rexach Physiology Mt San Antonio College
 The Immune System by Dr. Carmen Rexach Physiology Mt San Antonio College What is the immune system? defense system found in vertebrates Two categories Nonspecific specific provides protection from pathogens
The Immune System by Dr. Carmen Rexach Physiology Mt San Antonio College What is the immune system? defense system found in vertebrates Two categories Nonspecific specific provides protection from pathogens
The Adaptive Immune Response: T lymphocytes and Their Functional Types *
 OpenStax-CNX module: m46560 1 The Adaptive Immune Response: T lymphocytes and Their Functional Types * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution
OpenStax-CNX module: m46560 1 The Adaptive Immune Response: T lymphocytes and Their Functional Types * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution
Immunity. Avian Physiology
 Immunity Avian Physiology The Perfect World The Real World HELP ME! CHICKEN POX FLU STOMACH UPSET HELP! COLD HELP ME! Immunity Definition The Latin term IMMUNIS means EXEMPT, referring to protection against
Immunity Avian Physiology The Perfect World The Real World HELP ME! CHICKEN POX FLU STOMACH UPSET HELP! COLD HELP ME! Immunity Definition The Latin term IMMUNIS means EXEMPT, referring to protection against