Hypertension mechanisms
|
|
|
- Shauna Robertson
- 5 years ago
- Views:
Transcription
1 הטיפול בלחץ דם בעזרת תרופות מישלב
2 Hypertension mechanisms ESH Task Force Document. J Hypertens 2009
3 The history of development of antihypertensive drugs ESH Task Force Document. J Hypertens 2009
4 הטיפול ביתר לחץ דם STROKE = 40% CHD = 15-20% CHF = 50%
5 ? כיצד להוריד לחץ דם
6 Monotherapy versus combination strategies Mild BP elevation Low/moderate CV risk Conventional BP target Choose between Marked BP elevation High/very CV high risk Lower BP target Single agent at low dose Two drug combination at low dose If goal BP not achieved Previous agent at Switch to different Previous combination at Add a third drug at lld full dose agent at low dose full dose low dose If goal BP not achieved Two to three drug Full dose Two three drug combination at Two to three drug combination at full dose monotherapy full doses
7 Current Guidelines Acknowledge that Combination Therapy is Required by the Majority of Patients to Reach BP Goal JNC 7 guidelines state 1 : Although effective BP control can be achieved in most patients who are hypertensive, the majority will require two or more antihypertensive drugs. ESH/ESC guidelines state 2 : Evidence has continued to grow that t in the vast majority of hypertensive patients, effective BP control can only be achieved by combination of at least two antihypertensive drugs. Whenever possible, use of fixed dose (or single pill) combinations should be preferred, because simplification of treatment carries advantages for compliance to treatment. ESH = European Society of Hypertension ESC = European Society of Cardiology JNC = Joint National Committee 1 Chobanian et al. Hypertension 2003;42: Mancia et al. Blood Pressure 2009;18:
8 ACCOMPLISH: Trial Design Prospective, randomized, double-blind, event-driven trial Target BP <140/90 mmhg; <130/80 mmhg in patients with diabetes or renal insufficiency Screening Random mization 11,506 patients Benazepril 20 mg + Amlodipine 5 mg Benazepril 20 mg + HCTZ 12.5 mg Forced titration Benazepril 40 mg + Amlodipine 5 mg Benazepril 40 mg + HCTZ 12.5 mg Benazepril 40 mg + Amlodipine 10 mg Benazepril 40 mg + HCTZ 25 mg Free add-on* Free add-on* 2 Weeks Day 1 Month 1 Month 2 Month 3 Year 5 8 *Beta blockers; alpha blockers; clonidine; loop diuretics; HCTZ = hydrochlorothiazide Follow up at 6 months and every 6 months thereafter Jamerson K, et al. J Clin Hypertens 2003;5(4 Suppl 3):29 35 Jamerson K, et al. Am J Hypertens 2004;17: Jamerson K, et al. Blood Press 2007;16:80 6
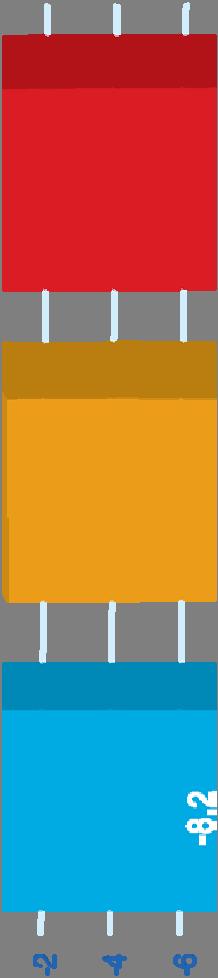
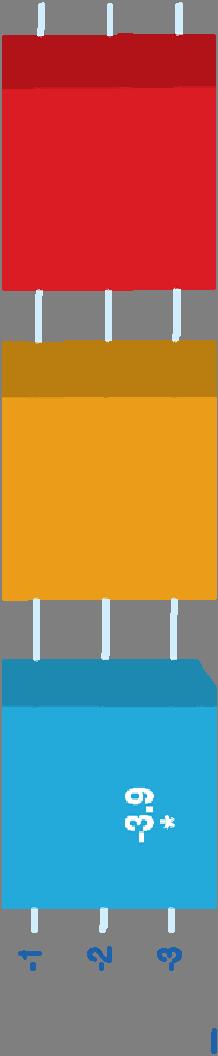
9 FIXED COMBINATION ACHIEVEMENTS ACCOMPLISH STUDY n engl j med 359; BP 131 2/73 4 mmhg
 rate Cumula ative event 0.12 0.08 0.04 HR 0.80 (95%CI 0.72 0.90); p<0.")
 Benazepril/amlodipine l i 5,512512 5,317 5,141 4,959 4,739 2,826 1,447 Benazepril/HCTZ 5,483 5,274 5,082 4,892")
10 ACCOMPLISH: Primary Endpoint 0.16 Benazepril/amlodipine (552 patients with events: 9.6%) Benazepril/HCTZ (679 patients with events: 11.8%) rate Cumula ative event HR 0.80 (95%CI ); p< % relative risk reduction ,096 1,277 Time to first CV mortality/morbidity (days) Months Patients at risk (N) Benazepril/amlodipine l i 5, ,317 5,141 4,959 4,739 2,826 1,447 Benazepril/HCTZ 5,483 5,274 5,082 4,892 4,655 2,749 1, Jamerson K, et al. N Engl J Med 2008;359:
11 ACCOMPLISH: Conclusion The ACCOMPLISH trial demonstrates that excellent BP control rates can be achieved with RAS blocker-based single-pill combination therapies The combination of a RAS blocker (benazepril) + CCB (amlodipine) reduced the risk of CV morbidity and mortality more than a RAS blocker (benazepril) + diuretic (HCTZ) combination in high-risk hypertensive patients These findings support the use of a RAS blocker + CCB single-pill combination when combination therapy is required in high-risk hypertensive patients 11 Jamerson K, et al. N Engl J Med 2008;359:
12 12
13 ACCOMPLISH: Conclusion The ACCOMPLISH trial demonstrates that excellent BP control rates can be achieved with RAS blocker-based single-pill combination therapies The combination of a RAS blocker (benazepril) + CCB (amlodipine) reduced the risk of CV morbidity and mortality more than a RAS blocker (benazepril) + diuretic (HCTZ) combination in high-risk hypertensive patients These findings support the use of a RAS blocker + CCB single-pill combination when combination therapy is required in high-risk hypertensive patients 13 Jamerson K, et al. N Engl J Med 2008;359:
14
15
16
17 Aortic Stiffening and Early Wave Reflection Diastole Young compliant arteries : Normal PW velocity (8 m/sec) (1) Ventricular-Vascular coupling (2) coronary blood flow Systole Elderly stiff arteries with ISH : Increased PW velocity (12 m/sec) (1) Ventricular-vascular mismatch (2) The reflected wave increases or augments central SBP during late systole:
18
19
20 Meta-analysis analysis of placebo-controlled controlled trials of monotherapy: 1- in unselected hypertensives,6 reports average (placebo corrected) showed blood pressure responses to single agents of: 9.1 mmhg for systolic blood pressure 5.5 mmhg for diastolic blood pressure.
21 Monotherapy vs Combination therapy, Wald et al, AJM 2009
22 Ratio of observed to expected incremental blood pressure-lowering effects of adding a drug or doubling the dose according to the class of drug (Wald et al, AJM 2009)
23 Treatment of Systolic/Diastolic Hypertension Without Other Compelling Indications
24 CBPM 140/90 mmhg & ABPM/HBPM 135/85 mmhg Stage 1 hypertension CBPM 160/100 mmhg & ABPM/HBPM 150/95 mmhg Stage 2 hypertension Care pathway 2011 If target organ damage present or 10- year cardiovascular risk > 20% Offer antihypertensive drug treatment If younger than 40 years Consider specialist referral Offer lifestyle interventions Offer patient education and interventions to support adherence to treatment Offer annual review of care to monitor blood pressure, provide support and discuss lifestyle, symptoms and medication

25 Aged under 55 years Aged over 55 years or black person of African or Caribbean family origin of any age C 2 A Step 1 Summary of antihypertensive drug treatment A + C 2 Step 2 A + C + D Step 3 Resistant hypertension A + C + D + consider further diuretic 3, 4 or alpha- or beta-blockerblocker 5 Consider seeking expert advice Step 4 Key A ACE inhibitor or low-cost angiotensin II receptor blocker (ARB) 1 C Calcium-channel blocker (CCB) D Thiazide-like diuretic See slide notes for details of footnotes 1-5
26 ESH/ESC guidelines state 2011 Use of fixed combinations of two drugs can directly follow initial monotherapy when addition of a second drug is required to control blood pressure, or be the first treatment step when a high C.V. risk makes easy control desirable New evidence favours, whenever possible, the use of fixed combinations of two drugs in a single tablet because of the advantage of simplification of the treatment regimen
27 drug combinations for hypertension treatment in patients without specific compelling indications Preferred combinations Renin angiotensin aldosterone system inhibitors [ARB/ACEi] and calcium channel blockers Renin angiotensin aldosterone system inhibitors [ARB/ACEi] and diuretics Acceptable combinations Beta-blocker/diuretic CCB (dihydropyridine)/beta-blocker CCB/diuretic Renin inhibitor/diuretic Renin inhibitor/ccb Dihydopyridine CCB/non-dihydropyridine CCB Beta blockers and Alpha Blockers [personal opinion, only for patients with high degree of anxiety] Unacceptable/ineffective combinations Dual renin angiotensin aldosterone system blockade Renin angiotensin aldosterone system blocker and beta-blockers Beta-blockers and antiadrenergic drugs [normopresan]
28 Renin angiotensin aldosterone system inhibitors [ARB/ACEi] and calcium channel blockers in Israel 1 Exforge (Amlodipine+Valsartan) 2 Vasodip Combo (lercanidipine+enalapril)
29 Amlodipine/Valsartan: BP Lowering Across All Grades of Hypertension Mean change in mean sitting systolic BP from baseline (mmhg) 0 10 Mild HTN 1 Moderate HTN 1 Severe HTN mmhg 2 Systolic BP n=69 n=140 n=64 n= Diastolic BP reduction (mmhg) Data from Smith et al. J Clin Hypertens 2007;9: (Dose 10/160 mg) 2 Data from Poldermans et al. Clin Ther 2007;29: (Dose 5 10/160 mg)
30 Amlodipine/valsartan ABPM (1) Blood Pressure Monitoring 2011, 16:87 95
31 BP reduction- baseline Vs. end of treatment VASODIP COMBO 10/20
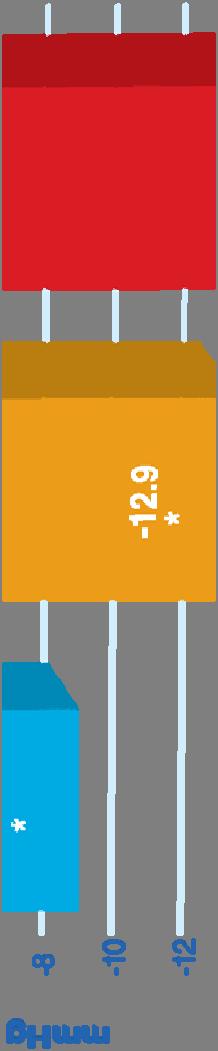
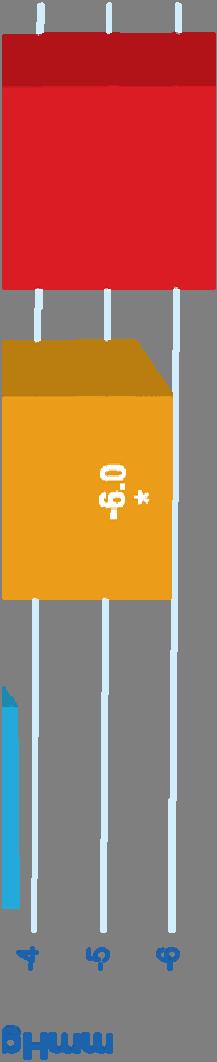

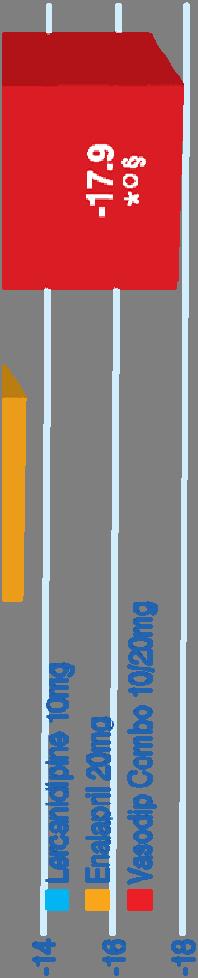

32 Significant reduction of ABPM values 24-hour SPB 24-hour DPB Piug JG et al. J Hum Hypertens. 2007; 21:




33 ACEI Vs ARB
34 Vol. 17, No. 8 October 2011 JMCP Supplement to Journal of Managed Care Pharmacy



35
36 Discussion written by the authors it should be emphasized that we did not design this meta-analysis to make a head-to-head comparison between ACE inhibitors and ARBs. The finding that the beneficial effect is seen in the ACE inhibitor population as opposed to the ARB population should be considered a post hoc observation. Given the nature of meta-analyses, which are per definition data-driven, driven, the differential effect between ACE inhibitors and ARBs should be interpreted with caution to avoid overstating this subgroup finding vis-a`-vis the a priori hypothesis. In this respect it should also be noted that the difference in effect on cardiovascular mortality between ACE inhibitors and ARBs was not statistically significant
37 RAAS inh & diuretics
38 Obesity paradox observed with hydrochlorothiazide, not amlodipine: ACCOMPLISH (ASH 2012) A single tablet benazepril/amlodipine p combination reduced the risk of morbidity and mortality by 20% /Stratifying patients in the entire cohort by BMI, the primary end point (CV, death, MI, and stroke) occurred in the 24.7% of patients with iha normal BMI, 20.5% of patients considered overweight (BMI 25 30), and in 17.2% of patients considered obese (BMI>30) >30). In a head to head comparison of the amlodipine treated patients with those treated withhydrochlorothiazide, hydrochlorothiazide, there was no difference in the primary end point in the obese patients. In the overweight and normal BMI cohorts, treatment favored amlodipine, Hypertension in obese patients is associated with excess volume, and a number of people have shown this, so thiazide therapy, as well as calcium channel blocker l therapy, is appropriate in those patients,"
39 Treatment of Hypertension in Patients 80 Years of Age or Older (N Engl J Med 2008;358)
40 ESH/ESC guidelines state 2011 Use of fixed combinations of two drugs can directly follow initial monotherapy when addition of a second drug is required to control blood pressure, or be the first treatment step when a high C.V. risk makes easy control desirable New evidence favours, whenever possible, the use of fixed combinations of two drugs in a single tablet because of the advantage of simplification of the treatment regimen
41 אז, אפשר להפסיק את הטיפול, דוקטור? לחץ דם שלך התאזן, מר לוי מצב מוכר
42 Canadian Recommendations 2011
43 Medication Persistence Beyond One Year is Even lower 39% used anti-hypertensive medications continuously over 10-years 39% discontinued permanently 22% discontinued temporarily Van Wijk BL et al. J Hypertens. 2005; 23:
44 Improved compliance with single-pill combination therapy compared with free-combination therapy P< Defined as the total number of days of therapy for medication dispensed/365 days of study follow-up Gerbino & Shoheiber Am J Health System Pharm 2007; 64:
45 Blood Pressure Reduction of 2 mmhg Decreases the Risk of Cardiovascular Events by 7 10% Meta-analysis of 61 prospective, observational studies 1 million adults 12.7 million person-years 2 mmhg decrease in mean SBP 7% reduction in risk of ischaemic heart disease mortality 10% reduction in risk of stroke mortality Lewington et al. Lancet 2002;360:
46 Prevalence and Correlates of Low Medication Adherence in Apparent Treatment-Resistant Hypertension, The Journal of Clinical Hypertension Vol 14 No 10 October 2012
47 Uncontrolled hypertension carries the same CV risk as untreated hypertension Third National Health and Nutrition Examination Survey (NHANES III) Not treated BP uncontrolled 48% (n = 2,458) Both are at equally increased risk compared with controlled BP (p>0.05) 35% (n = 1,756) BP controlled 17% (n = 872) Gu Q, et al. Am J Hypertens 2009; doi: /ajh
48 Adherence to antihypertensive medications and cardiovascular morbidity among newly diagnosed hypertensive patients Multivariable analysis of the association of patients characteristics with first-ever acute cardiovascular event estimated by Cox proportional-hazards models Adherence within 6 mo after diagnosis HR* (95% Cl) P Model 1 Low (PDC <40%) 1.00 < Intermediate (PDC, 40% to 79%) 0.87( ) Model 2 High (PDC 80%) 0.50 ( ) < Low (PDC <40%) 1.00 < Intermediate (PDC, 40% to 79%) 0.86( ) High (PDC 80%) 0.62 ( ) Circulation. 2009; 120:
49 Patients Taking FDCs (Fixed Dose Combinations) Use Fewer Healthcare Resources than Patients on Free Combinations In three one-year retrospective ti 7000 studies, total annual healthcare cost per patient was significantly less with 6000 an FDC (amlodipine/benazepril) 5000 compared with an equivalent free combination (DHP-CCB + ACEI) Reduced costs were linked to: fewer outpatient visits lower drug costs lower hospitalization costs r patient (US S$/yr) Total healthc care cost pe *** * * One pill* ** Two pills* ** * *One pill: combination of amlodipine and benazepril; two pills: combination of dihydropyridine CCB and ACEI. ACEI: angiotensin-converting genzyme inhibitor; DHP-CCB: dihydropyridine calcium channel blocker; FDC: fixed-dose combination 1. Dickson M, Plauschinat CA. J Manag Care Pharm; Am. J Cardiovasc drugs Taylor AA, Shoheiber O. Congest Heart Fail. 2003;9: Ngan GC et al. J Clin Hypertens. 2006;8(5, Suppl A):S >6 Charlson co-morbidity index *p<0.05; **p<0.01; ***p<0.001 two pills vs. one pill Graph based on ref. 2
50 לא לשכוח Disadvantages of a Fixed Dose Combination as Antihypertensive Therapy Loss of dose flexibility Fixed dose combinations may not contain appropriate doses when treating hypertension and a comorbid condition
51 לזכור אבל Advantages of a Fixed Dose Combination as Antihypertensive Therapy All of the advantages of giving 2 3 drugs individually, plus: Simplification of the regimen Improved adherence Reduced pill burden Potential for reduced cost
52 Combinations of More than Two Drugs No less than 15% 20% of the patients need more than two antihypertensive drugs to achieve an effective BP reduction The combination of a RAS blocker, a CA and a thiazide is a rational three drug combination. It will arrive to Israel in the 21th century
53 תודה רבה
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Rationale for the use of Single Pill Combination. Yong Jin Kim, MD Seoul National University Hospital
 Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Rationale for the use of Single Pill Combination Yong Jin Kim, MD Seoul National University Hospital Unmet Need of Hypertension Treatment Hypertension # 1 Risk Factor for Global Mortality 0 1 2 3 4 5 6
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC
 and Asian data of ARB/CCB SPC") Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Rationale for the use of Single Pill Combination (SPC) and Asian data of ARB/CCB SPC Seung Woo Park, MD Samsung Medical Center BP Control Rates in Asia BP controlled BP uncontrolled 24.3% 36.6% 19% Turkey
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
First line treatment of primary hypertension
 First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
First line treatment of primary hypertension Dr. Vijaya Musini Assistant Professor, Dept. Anesthesiology, Pharmacology and Therapeutics Manager, Drug Assessment Working Group Therapeutics Initiative Editor,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017
 Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Which antihypertensives are more effective in reducing diastolic hypertension versus systolic hypertension? May 24, 2017 The most important reason for treating hypertension in primary care is to prevent
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London
 Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email:
Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email:
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION
 EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION Khemchandani D. 1 and * Arif A. Faruqui 2 1 Bairagarh,
EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION Khemchandani D. 1 and * Arif A. Faruqui 2 1 Bairagarh,
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Managing hypertension: a question of STRATHE
 (2005) 19, S3 S7 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE Managing hypertension: a question of STRATHE Department of Cardiovascular Disease,
(2005) 19, S3 S7 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE Managing hypertension: a question of STRATHE Department of Cardiovascular Disease,
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Clinical cases with Coversyl 10 mg
 Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Clinical cases Coversyl 10 mg For upgraded benefits in hypertension A Editorial This brochure, Clinical cases Coversyl 10 mg for upgraded benefits in hypertension, illustrates a variety of hypertensive
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico
 Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Update sulla terapia antiipertensiva e antiaggregante nel paziente cardiometabolico G. Mazzanti UO Cardiologia Ospedale SS. Annunziata, Cento (FE) AUSL di Ferrara Antiplatelet therapy Aspirin Aspirin:
Director of the Israeli Institute for Quality in Medicine Israeli Medical Association July 1st, 2016
 The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Nurse-sensitive factors in hypertension management
 Nurse-sensitive factors in hypertension management Hypertension treatment State of the Art Copper Hall 14:45-15:04 02/04/2011 Philippe van de Borne, MD, PhD Department of cardiology ULB-Erasme Hospital
Nurse-sensitive factors in hypertension management Hypertension treatment State of the Art Copper Hall 14:45-15:04 02/04/2011 Philippe van de Borne, MD, PhD Department of cardiology ULB-Erasme Hospital
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Hypertension Guidelines: International; African,?Kenyan
 Hypertension Guidelines: International; African,?Kenyan Elijah N. Ogola University of Nairobi Kenya Cardiac Society Symposium 24 th 25 th February 2017 Eldoret Outline Background Overview of international
Hypertension Guidelines: International; African,?Kenyan Elijah N. Ogola University of Nairobi Kenya Cardiac Society Symposium 24 th 25 th February 2017 Eldoret Outline Background Overview of international
The Hypertension Clinic is a part of the Internal Medicine
 Original Article Hypertension Registry at the Bangkok Hospital Medical Center: The First 7 Months Experience OBJECTIVE: The Hypertension Registry at the Bangkok Hospital Medical Center was established
Original Article Hypertension Registry at the Bangkok Hospital Medical Center: The First 7 Months Experience OBJECTIVE: The Hypertension Registry at the Bangkok Hospital Medical Center was established
Central Pressures and Prehypertension
 Central Pressures and Prehypertension Charalambos Vlachopoulos Associate Professor of Cardiology 1 st Cardiology Dept Athens Medical School Central Pressures and Prehypertension Charalambos Vlachopoulos
Central Pressures and Prehypertension Charalambos Vlachopoulos Associate Professor of Cardiology 1 st Cardiology Dept Athens Medical School Central Pressures and Prehypertension Charalambos Vlachopoulos
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011)
") Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Thiazide or Thiazide Like? Choosing Wisely Academic Detailing Conference Digby Pines October 12-14
 Thiazide or Thiazide Like? Choosing Wisely Academic Detailing Conference Digby Pines October 12-14 Disclosures Pam McLean-Veysey, Team Leader Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance
Thiazide or Thiazide Like? Choosing Wisely Academic Detailing Conference Digby Pines October 12-14 Disclosures Pam McLean-Veysey, Team Leader Drug Evaluation Unit DEU funded by the Drug Evaluation Alliance
The underestimated risk of
 Earn 3 CPD Points online The underestimated risk of hypertension Dr David Webb Johannesburg Introduction The high and increasing worldwide burden of hypertension is a major global health challenge. Hypertension
Earn 3 CPD Points online The underestimated risk of hypertension Dr David Webb Johannesburg Introduction The high and increasing worldwide burden of hypertension is a major global health challenge. Hypertension
REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT
 REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT Vida Stankus 1, Brenda Hemmelgarn 2, Norm RC Campbell 2, Guanmin Chen 2, Finlay A McAlister 1, Ross T Tsuyuki 1 1 EPICORE Centre, Department of Medicine,
REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT Vida Stankus 1, Brenda Hemmelgarn 2, Norm RC Campbell 2, Guanmin Chen 2, Finlay A McAlister 1, Ross T Tsuyuki 1 1 EPICORE Centre, Department of Medicine,
High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension
 (2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
(2005) 19, 491 496 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE High-dose monotherapy vs low-dose combination therapy of calcium channel blockers
Comparative review of NICE, JNC8, SAHS and ISHIB. Brian Rayner, Division of Hypertension, University of Cape Town
 Comparative review of NICE, JNC8, SAHS and ISHIB Brian Rayner, Division of Hypertension, University of Cape Town Scope of Problem Deaths attributable to high blood pressure in males, South Africa 2000
Comparative review of NICE, JNC8, SAHS and ISHIB Brian Rayner, Division of Hypertension, University of Cape Town Scope of Problem Deaths attributable to high blood pressure in males, South Africa 2000
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique
 ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique Adherence, compliance, persistence: definitions Adherence
ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique Adherence, compliance, persistence: definitions Adherence
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management
 Changing the Landscape of BP Management") Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy
Amlodipine/Valsartan (Exforge ) Changing the Landscape of BP Management Bum-Kee Hong Yongdong Severance Hospital Yonsei University College of Medicine Rationale for Multiple-Mechanism Therapy Inadequacy