Gastrointestinal bleed- what saves life?
|
|
|
- Veronica Hunter
- 5 years ago
- Views:
Transcription
1 Gastrointestinal bleed- what saves life? Prof Sauid Ishaq Gastroenterologist, DGH BCU, SGU and Fudan University Physician Associates conference Friday 16 February 2018
2 Reality What is the mortality of Acute anterior MI? <30% (CCU) What is the Mortality of sick bleeder? 30-50% No bleeding unit
3 GI bleed-is it serious? 10-15% mortality In patient mortality higher Aging population NSAID Anti-platlet
4 GI bleed- why patient dye

")
5 Mortality (SI = HR/Sys BP- 0.7) NCEPOD 2015

6 Delay in recognition of bleed 6

7 Initial risk assessment score used 7
8 Time to OGD NICE QS suspected UGIB OGD < 24hours All patients = time of admission or presentation (IPs) 65% (205/316) < 24 hours 8
9 GI bleed presentation Melaena / haematemesis Collapse Dizziness Hypotension

10 What is coffee grounds?
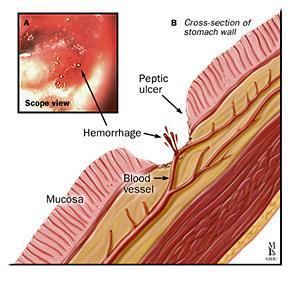
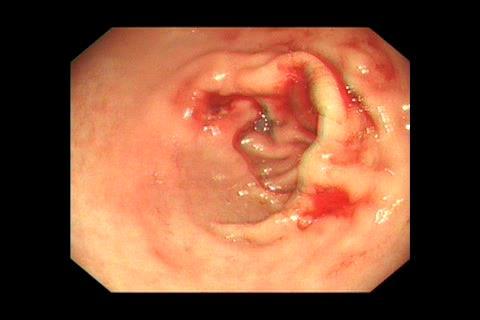
11 Causes of acute upper gastrointestinal haemorrhage Diagnosis Approx % Peptic ulcer % Gastroduodenal erosions 8-15 % Oesophagitis 5-15 % Mallory Weiss tear 15% Varices 5-10 % GI cancer
12 Who is at risk- assessment In patient Vs acute admissions Increasing age Co-morbidity IHD, Renal/Liver/cancer Shock BP < 100, HR > 100 (drugs) Anti-PL, NSAIDs, warfarin Endoscopic findings- spurter, vessel
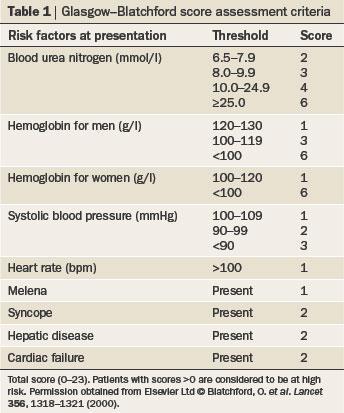
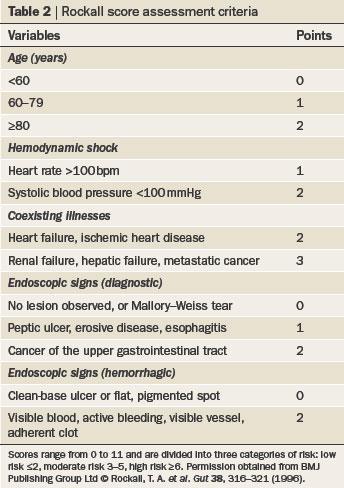
13 RS VS GBS
14 What saves life Resuscitation IV access- grey VFX2 What Fluid- D/W, N/S, Colloid, Blood? What to Monitor (BP >100) Proton pump inhibitors? When to endoscope
15 Introduction Gastrointestinal bleeding is one of the commonest medical emergencies The incidence rate of 1.33/1000 population equates to approximately 85,000 cases/year in the UK or one gastrointestinal bleed every 6 minutes 15
16 A Common Clinical Problem 1-2% of all hospital admissions Most common diagnosis of new ICU admissions 5-10% mortality 80% of GI bleeds stop spontaneously Those with massive bleeding need urgent intervention 16
17 Introduction Second commonest medical reason for transfusion, accounting for 14% of all blood transfusions Early treatment can reduce the number of units of blood received and complications Managed by both medical and surgical teams Traditionally split into upper GI and lower GI bleeding 17
18 GIB6
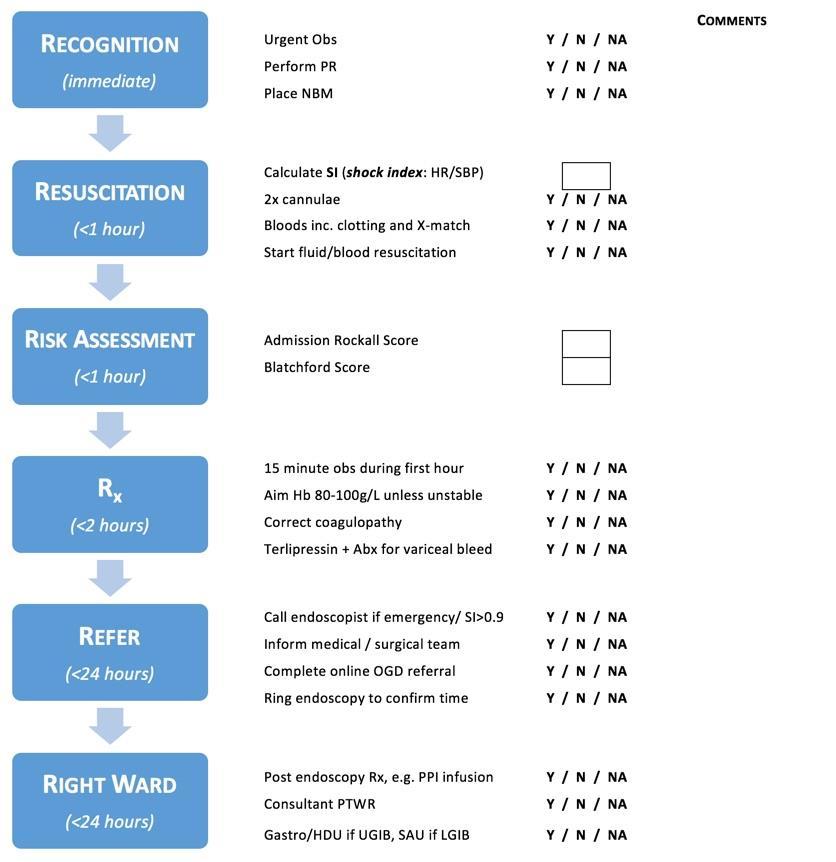
19 1 - Recognition Immediately Haematemesis, Melaena, Bright red rectal bleeding PR examination (all patients with confirmed or suspected GI bleed should have PR examination performed on arrival)
20 2 - Assessment Immediately a) ABCDE approach: consider Shock index (SI): ratio between HR and systolic BP >0.9 - detect early haemorrhagic shock b) Risk assessment: Use Blatchford score (use Rockall post endoscopy) Blatchford score - assess probability for intervention (blood transfusion, endoscopy)- Score 0 - low risk, consider early discharge Score >0 - manage as in patient Score >5 - high risk for intervention c) Blood sampling for ABG (Hb, PH, Lactate), FBC, Clotting, U&Es, LFTs and cross match, ECG, Drugs History - Clopidogrel, aspirin, warfarin, NOAC
21 3 - Resuscitation to start within 30 minutes Two large venflon - O2, fluid resuscitation - saline colloid/ Blood transfusion - (consider activating massive haemorrhage protocol early if ongoing shock or massive haemorrhage) a) Aim - systolic BP >100 ( systolic in variceal bleed), satisfactory urine output, Use fluid boluses, reassess after each bolus b) Aim HB 8-10 (for variceal bleed, HB7): Avoid over or under transfusion. Blood transfusion for: Hb less than 7.0, ongoing shock/ haemorrhage c) Monitoring every 15 minutes for the first hour d) Keep patient NBM e) If suspected peptic ulcer bleed give bolus IV PPI (not in NICE guidance, but emerging evidence), variceal bleed, give terlipressin 2mg (antibiotics in suspected variceal bleed) f) Patient on anticoagulant - high INR - need urgent correction (discuss lower limit in high risk patient, recurrent PE, MVR), offer prothrombin complex concentrate to patient on warfarin and high INR g) Offer FFP for patients who are actively bleeding with PT and/or aptt more than 1.5 normal, offer cryoprecipitate to patients with persistent fibrinogen level of less than 1.5g/l despite initial resuscitation
22 Is the patient shocked? Vol loss (ml) Vol loss (%) Class I Class II Class III Class IV < > >40 Systolic Normal Normal Low V Low Diastolic Normal Raised Low V Low Pulse Slight tachy thready >120, v thready Resp rate Normal Normal >20 >20 Mental state Alert Anxious / aggressive Drowsy Confused / unconscious

23 What size cannula?
24 What size cannula? Flow Rates through Cannulae (ml/min) Colour Gauge Flow rate (ml/min) Pink Green Grey Orange Triple lumen CVP line 16 50
25 What fluid replacement? Blood if >30% volume loss?o-negative?group specific?cross-matched
26 Crystalloid or colloid? No comparative studies in UGIB Probably makes no difference
27 Inaproppriate use of blood

28 Appropriate blood product use 28
29 Serious Hazards of Transfusion 2012 data Transfusion caused or contributed to death Major morbidity definitely or probably related to transfusion Minor or no morbidity as result of transfusion reaction Risk of death 3.1 per components transfused Risk of major morbidity 46.5 per
30 4 - Time to Endoscopy All patient with a GI bleed and haemodynamic instability should have 24/7 access to an OGD within two hours of optimal resuscitation (NICE recomndation) Endoscopy within 24 hours (ideally within 6-12 hours within working hours, if space and skilled endoscopist available - this potentially prevent further bleed and possibly blood transfusion). Patient with BRRB with shock index >1 - urgent OGD -
31
 Heater probe (MP) ADr + C or H")
32 Spurter Endoscopin treatment Clips Adrenaline MPEC (MTP) Heater probe (MP) ADr + C or H Bands

33
34
 HP used to low power 15-30J ( lower in Duo) Caution- cavitating lesion, repeat therapy, if plane")
35 Thermal treatment Heater probe MP Gold probe BP ( depth is sallow and more predictable) Coupled with injection therapy Coaptive coagulation- firm pressure Until area black and cavitated (severl pulses) HP used to low power 15-30J ( lower in Duo) Caution- cavitating lesion, repeat therapy, if plane parallel
36 Controversial areas IV PPI before OGD (Lu et al nejm) Cost-effectiveness study in canada in favour of IBV PPI AP&T 2003 Combination Vs single modality Pre procedure erythromycin- clear views Next day re- look high risk patient GI bleed plus - Acute coronary event Clot removal 11a Vs 11b ( visible vessel) Octreotide in conjunction with PPI
37 Hemospray is licenced for : a UPPER GI non-varaceal BLEEDS CONTRA INDICATIONS : Perforations Fistulae

38 Easy as Activate CO2 2. Open 3. Deploy
39
40 When to suspect Variceal bleed Melaena / haematemesis Jaundice Ascites Splenomegaly Spider naevi Alcohol misuse INR,Bil, PL
41
42 Variceal bleed- how resuscitation is different Do not over-transfuse- rebleeding risk No Saline if ascites Dextrose/colloid, packed cell, PCC (Octaplex 1ml/kg) (Liver failure/thrombombotic tendencies avoid) BP > 90 mmhg, Hb > 8gm/dl Terlipressin 1-2mg QDS- for 5 days IV antibiotics- Tazocin Early endoscopy/sengstaken tube)
43 Oesophageal Variceal Bleeding - Specific Measures Endoscopic Injection sclerotherapy Band ligation Pharmacological Vasopressin analogues Somatostatin Somatostatin analogues Rescue Measures Tamponade TIPSS Surgery
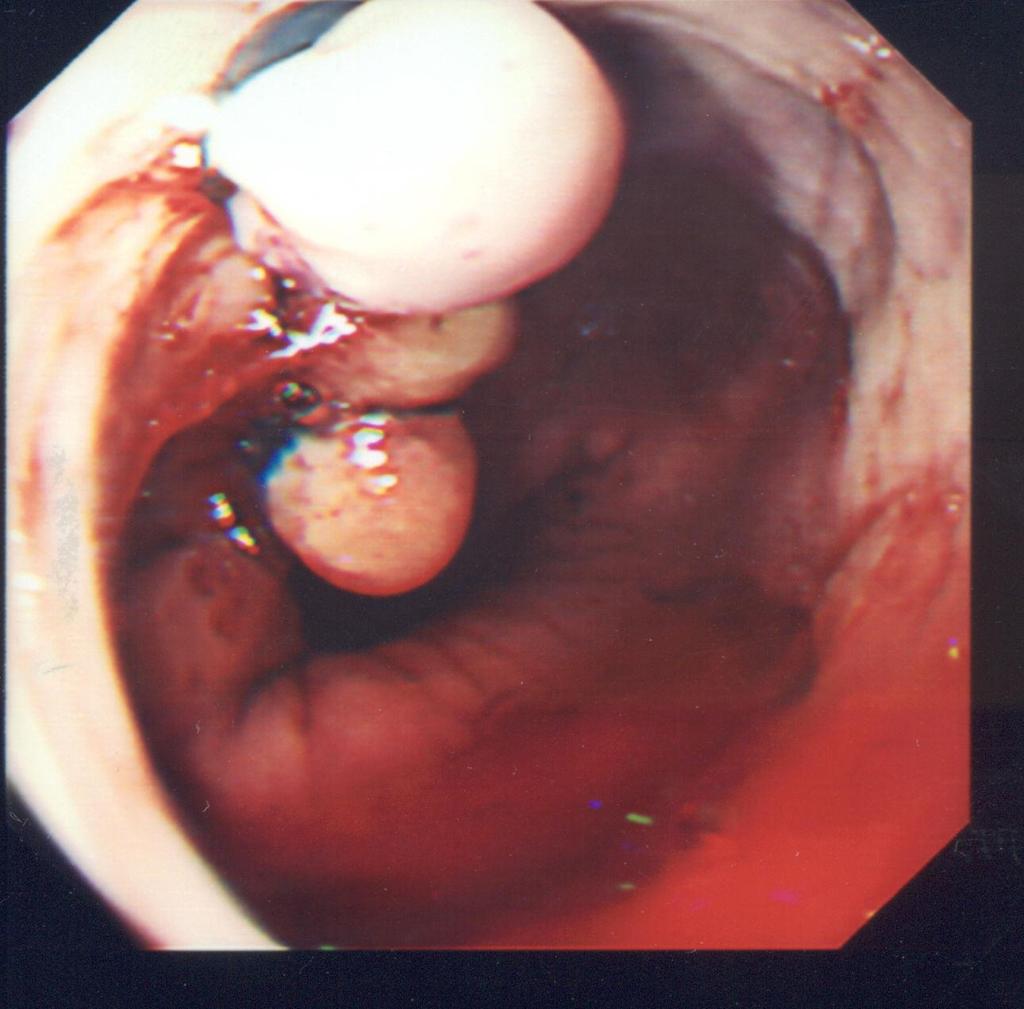
44 Banding
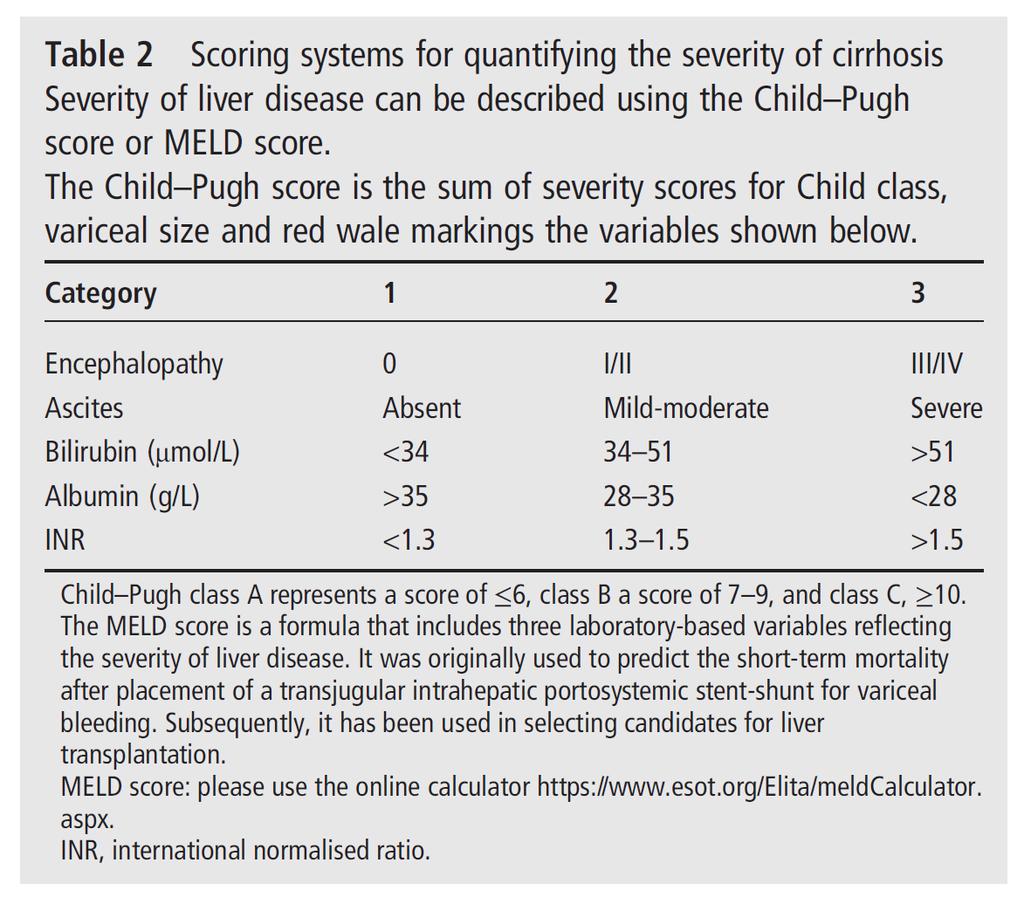
45 TIPSS 115 patients 61% Childs grade C Technical success rate 94% 30 day mortality 30% Rebleeding in 33%, usually due to shunt insufficiency 1 yr survival 52% Saravanan R, 2005
46 Special situations Warfarin (MVR, mechanical valve thromboembolic episode) Aspirin / Clopidogrel NSAID Exsanguinations; (too fast to replace) Rare blood group Jehovah's Witness

, pulmonary embolism (PE) at Russells Hall Hospital (RHH) since 2012 and deep venous thrombosis (DVT) since 2013 Trial data")
 versus warfarin (2.2%), p < 0.")





47 The risk of gastrointestinal bleeding with novel oral anticoagulants in a large cohort of patients at a district general hospital Aditi Kumar 1, Benjamin R Disney 1, Rupert Hipkins 2, Sarah Hughes 2, Steven Jenkins 2, & Sauid Ishaq 1 1 Department of Gastroenterology, Dudley Group NHS Foundation Trust, Russells Hall Hospital, Dudley UK 2 Department of Haematology, Dudley Group NHS Foundation Trust, Russells Hall Hospital, Dudley UK BACKGROUND: Rivaroxaban, apixaban and dabigatran compile the novel oral anticoagulants (NOAC). NOACs are used as first line treatment for atrial fibrillation (AF), pulmonary embolism (PE) at Russells Hall Hospital (RHH) since 2012 and deep venous thrombosis (DVT) since 2013 Trial data regarding risk of gastrointestinal (GI) bleeding is conflicting In the ROCKET-AF study, the rate of GI bleeding was significantly higher in the group randomised to receive rivaroxaban (3.2%) versus warfarin (2.2%), p < ) EINSTEIN-DVT and EINSTEIN-PE studies showed similar bleeding rates for rivaroxaban and warfarin although GI bleeding was not specifically addressed A meta-analysis of NOACs found an increased risk of GI bleeding with NOAC as opposed to warfarin (2.3% vs 1.3%, p = 0.036) Although trials have shown increased risk of GI bleeding with NOACs, little is known about its incidence in the real world setting. We aimed to ascertain the incidence of GI bleeding, endoscopic findings, time of onset of bleeding and the need for intervention in patients commencing NOACs METHODS: A retrospective review was performed of all patients at RHH who received NOACs These patients were identified from the anticoagulation database and cross referenced with the GI endoscopy database and patient notes. Basic demographic, clinical and laboratory data and endoscopic findings were collated. STRENGTHS Largest cohort worldwide Single center experience LIMITATIONS: Due to the small sample size of patients on apixaban and dabigatran, difficult to compare with the trial data as well as between the NOACs Severity of upper GI bleed using the Rockall score or Blatchford score was not performed A multivariate analysis needs to be performed with patients on warfarin over the same time period at RHH to ensure there are no confounding variables. Alcohol, concomitant medications, symptoms, comorbidities CONCLUSIONS Prevalence of bleed more common >75 yrs of age Whilst there appeared to be a higher incidence of GI bleeding as compared to that observed in RCTs thus far, There were no deaths directly as a result of the GI bleed Only 11.5% required endoscopic intervention The use of blood products was relatively low at 34.4% Further studies need to be performed to provide a more accurate analysis for apixaban and dabigatran REFERENCES 1. Patel MR et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Eng J Med (10): Buller HR et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Eng J Med (14): Bauersachs R et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Eng J Med (26): Capodanno et al. Novel oral anticoagulants versus warfarin in non-valvular atrial fibrillation: a meta-analysis of patients. Int J Cardiol (4): Table 1: Comparison between the NOACs Non-bleeders (n= 2487) Bleeders (n= 61) Mean age (yrs) Graph 1: Endoscopic findings of all patients on NOACs RESULTS 74 +/ /- 8 P < Gender Females 1175 (47.2%) Males 1312 (52.8%) NOAC therapy Rivaroxaban 2332 (93.8%) Apixaban 77 (3.1%) Dabigatran 77 (3.1%) Females 41 (67.2%) Males 20 (32.8%) Rivaroxaban 54 (88.5%) Apixaban 4 (6.6%) Dabigatran 3 (4.9%) *2.45% bleeds in total at time of study. Since then, increased to 2.57% Table 3: Endoscopy findings upper GI vs lower GI bleeds Upper GI bleed* (n) Lower GI bleed** (n) Normal (6) Diverticular disease (16) Peptic ulcer disease (6) Haemorrhoids (12) Gastritis (6) Polyps (colonic/rectal) (7) Oesophagitis (5) Normal (5) *30/61 (49.2%) 16/30 (53%) required blood transfusion 20% 10% 0% *31/61 (51.8%) 5/31 (16%) required blood transfusion Some patients had multiple findings on endoscopy whereas others had more than one investigation. *UGIB is defined as patients who presented with either fresh haematemesis, malaena and/or coffee ground vomiting **LGIB is defined as patients who presented with fresh PR bleeding 26.2% patients with endoscopic findings compatible with active/recent bleeding 11.5% patients had active bleeding at time of endoscopy, all treated successfully Table 2: Bloods on admission INR Percentage INR > % INR > % Hb < % Hb < % prbcs required in 34.4% Median units needed: 4 IQR 2, range 1-8 There was no correlation between INR and blood transfusion requirement ALL PATIENTS ON NOACs: The most common type of bleed presentation was PR bleeding (48%) followed by melaena (37%),haematemesis (10.9%) and coffee ground vomit (1.6%) The median time in days from when patients were started on NOAC therapy to the date of their endoscopy was 204 days (6.7 months) with a range of 2 days to 19.7 months Table 4: Risk of bleeding between NOACs Risk of Bleeding Clinical significance Dabigatran vs Apixaban Apixaban vs Rivaroxaban Dabigatran vs Rivaroxaban *Fisher s test Graph 2: Age range of all patients that had a bleeding episode whilst on NOAC. Median age was 79.6 Age MORTALITY NS (p = 0.71) NS (p = 0.43) 30 day mortality rate was 10.9% (n=11) No deaths due to severe GI haemorrhage Causes of death: Cancer Sepsis Unknown Pneumonia (5% vs 2%, p = 0.11)
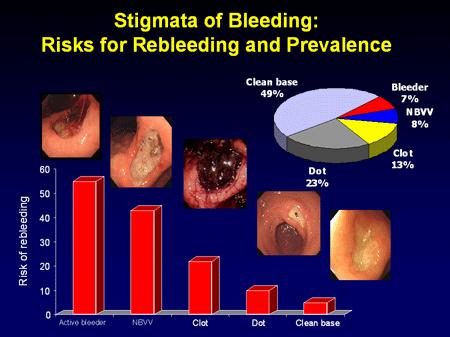
48 Resuscitate adequately Summary Risk assessment- Rockall, GBS Early GI team ownership If suspect varices terlipressin/abx/ early endoscopy If non variceal- with 24 hour ( early in shock) Intravenous PPI infusion if peptic ulcer bleed with stigmata of haemorrhage Restrictive blood transfusion Monitor for rebleeding Joint management- bleeding uit
49 Thank you Questions
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
Risk assessment in UGIB: recent PCI & ACS. Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass
 Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Blood and guts.. Haemodynamics / resuscitation. Haemodynamics / resuscitation. Blood and guts. Dr Jonathan Hoare
 Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
NICE Pathways bring together all NICE guidance, quality standards and other NICE information on a specific topic.
 bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
bring together all NICE guidance, quality standards and other NICE information on a specific topic. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published.
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Transfusion / resuscitation Anticoagulants new and old..
Picking up their Pieces: Emergency Management of GI Bleeds
 Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban
 Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Guidance for management of bleeding in patients taking the new oral anticoagulant drugs: rivaroxaban, dabigatran or apixaban Purpose The aim of this guidance is to outline the management of patients presenting
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Clinical guideline Published: 13 June 2012 nice.org.uk/guidance/cg141
 Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute Gastrointestinal Haemorrhage. Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield
 Acute Gastrointestinal Haemorrhage Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield Scope of Talk Introduction Upper GI haemorrhage-non variceal - Pathology/ risk stratification/management
Acute Gastrointestinal Haemorrhage Dr Reena Sidhu Consultant Gastroenterologist Hon Sen Lecturer University of Sheffield Scope of Talk Introduction Upper GI haemorrhage-non variceal - Pathology/ risk stratification/management
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Upper GI Bleeds. AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM
 Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
Antiplatelets in cardiac patients with suspected GI bleeding
 Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Antiplatelets in cardiac patients with suspected GI bleeding Acute GI bleeding is a common major medical emergency. In the 2007 UK-wide audit, overall mortality of patients admitted with acute GI bleeding
Management of acute upper gastrointestinal bleeding
 1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
1 Department of Gastroenterology, Glasgow Royal Infirmary, Glasgow G4 OSF, UK 2 Section of Digestive Diseases, Yale School of Medicine, New Haven, and VA Connecticut Healthcare System, West Haven, Connecticut,
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Note No nausea or vomiting before collapse increases the risk of an arrhythmia. A
 174 40 TACHYCARDIAS SYMPTOMS AND SIGNS Think about cardiac arrhythmias in patients with: palpitations D dyspnoea B chest pain D dizziness or syncope D cardiac arrest. D Ask about: any nausea or vomiting
174 40 TACHYCARDIAS SYMPTOMS AND SIGNS Think about cardiac arrhythmias in patients with: palpitations D dyspnoea B chest pain D dizziness or syncope D cardiac arrest. D Ask about: any nausea or vomiting
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Scottish Medicines Consortium
 Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Guideline for the Management of Upper Gastrointestinal Bleeding in Children
 Guideline for the Management of Upper Gastrointestinal Bleeding in Children 1. Introduction Upper gastrointestinal (UGI) bleeding in children poses a challenge to paediatricians and paediatric surgeons.
Guideline for the Management of Upper Gastrointestinal Bleeding in Children 1. Introduction Upper gastrointestinal (UGI) bleeding in children poses a challenge to paediatricians and paediatric surgeons.
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants. Helen Williams Consultant Pharmacist for CV Disease South London
 An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
An Overview of Non Vitamin-K Antagonist Oral Anticoagulants Helen Williams Consultant Pharmacist for CV Disease South London Contents Drugs and drug classes Licensed indications and NICE recommendations
Management of haemorrhage in patients taking DOACs/ NOACs (direct/ novel oral anticoagulants) Guideline. Contents
 Guideline. Contents") Management of haemorrhage in patients taking DOACs/ NOACs (direct/ novel oral anticoagulants) Guideline Classification: Clinical Guideline Lead Author: Dr Rowena Thomas-Dewing, Consultant Haematologist
Management of haemorrhage in patients taking DOACs/ NOACs (direct/ novel oral anticoagulants) Guideline Classification: Clinical Guideline Lead Author: Dr Rowena Thomas-Dewing, Consultant Haematologist
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING
 DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
DIRECT ORAL ANTICOAGULANTS: WHEN TO USE, WHICH TO CHOOSE AND MANAGEMENT OF BLEEDING KATHERINE STIRLING CONSULTANT PHARMACIST ANTICOAGULATION AND THROMBOSIS DR LISHEL HORN CONSULTANT HAEMATOLOGIST HAEMOSTASIS
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT
. Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT") Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Direct Oral Anticoagulants (DOACs). Dr GM Benson Director NI Haemophilia Comprehensive Care Centre and Thrombosis Unit BHSCT OAC WARFARIN Gold standard DABIGATRAN RIVAROXABAN APIXABAN EDOXABAN BETRIXABAN
Managing acute upper gastrointestinal bleeding in the acute assessment unit
 Clinical Medicine, Vol, No : 589 59 Managing acute upper gastrointestinal bleeding in the acute assessment unit Lotte Dinesen, SpR in gastroenterology; Martin Benson, consultant gastroenterologist and
Clinical Medicine, Vol, No : 589 59 Managing acute upper gastrointestinal bleeding in the acute assessment unit Lotte Dinesen, SpR in gastroenterology; Martin Benson, consultant gastroenterologist and
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary
 Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
Dr Shikha Chattree Haematology Consultant Sunderland Royal infirmary Increasing use of Novel Oral Anticoagulants (NOACs) in the management of prophylaxis and management of venous thromboembolism and in
Drug Class Review Newer Oral Anticoagulant Drugs
 Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
Drug Class Review Newer Oral Anticoagulant Drugs Final Original Report May 2016 The purpose of reports is to make available information regarding the comparative clinical effectiveness and harms of different
INTRODUCTION Indication and Licensing
 City and Hackney Clinical Commissioning Group Homerton University Hospital Foundation Trust DRUG NAME: Apixaban (Eliquis ) Transfer of Care document Indication: Treatment of acute venous thromboembolism
City and Hackney Clinical Commissioning Group Homerton University Hospital Foundation Trust DRUG NAME: Apixaban (Eliquis ) Transfer of Care document Indication: Treatment of acute venous thromboembolism
Guidelines for the Management of Upper gastrointestinal bleeding
 Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
Guidelines for the Management of Upper gastrointestinal bleeding By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Upper gastrointestinal bleeding is
ABDOMINAL PAIN (SEE ALSO ABDOMINAL AORTIC ANEURYSM)
") ABDOMINAL PAIN (SEE ALSO ABDOMINAL AORTIC ANEURYSM) Evaluating abdominal pain is difficult misdiagnosis of this symptom generates more formal complaints than any other clinical mistake made in our department.
ABDOMINAL PAIN (SEE ALSO ABDOMINAL AORTIC ANEURYSM) Evaluating abdominal pain is difficult misdiagnosis of this symptom generates more formal complaints than any other clinical mistake made in our department.
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Oakland K, Jairath V, Uberoi R, et al. Derivation
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Oral anti-thrombotic therapy-management in patients requiring endoscopy
 Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Oral anti-thrombotic therapy-management in patients requiring endoscopy Management of anti-thrombotic therapy in patients requiring endoscopy This guideline suggests appropriate management of patients
Appendix IV - Prescribing Guidance for Apixaban
 Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Appendix IV - Prescribing Guidance for Apixaban Patient Factors Dose of Apixaban If your patient has any of the following MAJOR risk factors: Hypersensitivity to the active substance or to any of the excipients
Low risk upper GI bleeding pathway
 Low risk upper GI bleeding pathway Background Low risk upper GI bleeding may be safely managed without an emergency admission to NUH following presentation to the ED. NUH uses the Glasgow Blatchford score
Low risk upper GI bleeding pathway Background Low risk upper GI bleeding may be safely managed without an emergency admission to NUH following presentation to the ED. NUH uses the Glasgow Blatchford score
Oral anticoagulant agent-associated bleeding events reporting system (ORANGE study)
") Oral anticoagulant agent-associated bleeding events reporting system (ORANGE study) Laura Green 1,2,3, Joan Morris 1, Raza Alikhan 4, Nicola Curry 5, Rhona Maclean 6, Khalid Saja 7, Simon Stanworth 3,5,
Oral anticoagulant agent-associated bleeding events reporting system (ORANGE study) Laura Green 1,2,3, Joan Morris 1, Raza Alikhan 4, Nicola Curry 5, Rhona Maclean 6, Khalid Saja 7, Simon Stanworth 3,5,
Management of acute upper GI bleeding
 BJA Education, 17 (4): 117 123 (2017) Matrix reference 1A01, 2A05, 3C00 doi: 10.1093/bjaed/mkw054 Advance Access Publication Date: 10 December 2016 Management of acute upper GI bleeding Ingi Adel Salah
BJA Education, 17 (4): 117 123 (2017) Matrix reference 1A01, 2A05, 3C00 doi: 10.1093/bjaed/mkw054 Advance Access Publication Date: 10 December 2016 Management of acute upper GI bleeding Ingi Adel Salah
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
Major Haemorrhage Protocol. Commentary
 Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Hairmyres Hospital Monklands Hospital Wishaw General Hospital Major Haemorrhage Protocol Commentary N.B. There is a separate NHSL protocol for the Management of Obstetric Haemorrhage Authors Dr Tracey
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant. Lab Matters study day Oake Manor, Taunton, 8 th July 2015
 Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
Alister Jones Patient Blood Management Practitioner NHS Blood and Transplant Lab Matters study day Oake Manor, Taunton, 8 th July 2015 NPSA Rapid Response Report 2010 Transfusion of blood and blood components
2 Summary of NICE TA 249: Atrial fibrillation - Dabigatran Etexilate
 Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
Service Notification in response to DHSSPS endorsed NICE Technology Appraisals NICE TA 249: Atrial fibrillation - Dabigatran Etexilate 1 Name of Commissioning Team Long Term Conditions Commissioning Team
Rivaroxaban film coated tablets are available in 2 strengths for this indication: 15mg and 20mg.
 Primary Care Prescriber Information RIVAROXABAN (XARELTO ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Rivaroxaban is a non-vitamin K antagonist
Primary Care Prescriber Information RIVAROXABAN (XARELTO ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Rivaroxaban is a non-vitamin K antagonist
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Primary Care Prescriber Information EDOXABAN (LIXIANA ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism
 Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism") Primary Care Prescriber Information EDOXABAN (LIXIANA ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Edoxaban is a non-vitamin K antagonist oral
Primary Care Prescriber Information EDOXABAN (LIXIANA ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism INDICATION Edoxaban is a non-vitamin K antagonist oral
Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine -
 Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
CONTROLLED DOCUMENT. Cirrhosis Care Bundle CATEGORY: Clinical Guidelines. CLASSIFICATION: Clinical. Controlled Document CG201 Number:
 Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Comparison of novel oral anticoagulants (NOACs)
") Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
Comparison of novel oral anticoagulants (NOACs) For guidance for full information refer to individual SPCs available at www.medicines.org.uk Licensed indications for NOACs Prevention of stroke and systemic
DRUG NAME: EDOXABAN (LIXIANA ) Transfer of Care document Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism
 Transfer of Care document Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism") City and Hackney Clinical Commissioning Group Homerton University Hospital Foundation Trust DRUG NAME: EDOXABAN (LIXIANA ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism
City and Hackney Clinical Commissioning Group Homerton University Hospital Foundation Trust DRUG NAME: EDOXABAN (LIXIANA ) Treatment of acute venous thromboembolism and prevention of recurrent venous thromboembolism
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
ANTICOAGULANTS AND HIP FRACTURE SURGERY. Jon Antrobus Anaesthetist Borders General Hospital
 ANTICOAGULANTS AND HIP FRACTURE SURGERY Jon Antrobus Anaesthetist Borders General Hospital Anticoagulation is common amongst the hip fracture patient population (6-10%) Anticoagulation signifies co-morbidity
ANTICOAGULANTS AND HIP FRACTURE SURGERY Jon Antrobus Anaesthetist Borders General Hospital Anticoagulation is common amongst the hip fracture patient population (6-10%) Anticoagulation signifies co-morbidity
HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised
 DABIGATRAN RECOMMENDED What it is Indications Date decision last revised") Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Name: generic (trade) Dabigatran etexilate (Pradaxa ) HERTFORDSHIRE MEDICINES MANAGEMENT COMMITTEE (HMMC) DABIGATRAN RECOMMENDED What it is Indications Date decision last revised Direct thrombin inhibitor
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
North East Essex Medicines Management Committee
 Colchester Hospital University NHS Foundation Trust North East Essex Clinical Commissioning Group North East Essex Medicines Management Committee ORAL ANTICOAGULANT (Vit K antagonist only) MANAGEMENT GUIDELINES
Colchester Hospital University NHS Foundation Trust North East Essex Clinical Commissioning Group North East Essex Medicines Management Committee ORAL ANTICOAGULANT (Vit K antagonist only) MANAGEMENT GUIDELINES
Hi doctor, can you come and see my patient, she s just had a coffee ground vomit. Dr Rhona Hurley, FY2
 Hi doctor, can you come and see my patient, she s just had a coffee ground vomit. Dr Rhona Hurley, FY2 Ask for more information What now? o What might you ask? o Do you have enough information about this
Hi doctor, can you come and see my patient, she s just had a coffee ground vomit. Dr Rhona Hurley, FY2 Ask for more information What now? o What might you ask? o Do you have enough information about this
Guidelines for the management of warfarin reversal in adults
 SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
SharePoint Location Clinical Policies and Guidelines SharePoint Index Directory General Policies and Guidelines Sub Area Haematology and Transfusion Key words (for search purposes) Warfarin, Bleeding Central
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Article Upper Gastrointestinal Bleeding in Children: A Tertiary United Kingdom Children s Hospital Experience
 Article Upper Gastrointestinal Bleeding in Children: A Tertiary United Kingdom Children s Hospital Experience Omar Nasher 1, *, David Devadason 2 and Richard J. Stewart 1 1 Department of Paediatric Surgery,
Article Upper Gastrointestinal Bleeding in Children: A Tertiary United Kingdom Children s Hospital Experience Omar Nasher 1, *, David Devadason 2 and Richard J. Stewart 1 1 Department of Paediatric Surgery,
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Edoxaban Treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism (NICE TA354)
") Rationale for Initiation, Continuation and Discontinuation (RICaD) Edoxaban Treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism (NICE TA354) This document supports the
Rationale for Initiation, Continuation and Discontinuation (RICaD) Edoxaban Treatment and secondary prevention of deep vein thrombosis and/or pulmonary embolism (NICE TA354) This document supports the
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
DOAC the story so far... Dr GM Benson Director NI Haemophilia and Thrombosis Centre BHSCT
 DOAC the story so far... Dr GM Benson Director NI Haemophilia and Thrombosis Centre BHSCT A rose by any other name.. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC
DOAC the story so far... Dr GM Benson Director NI Haemophilia and Thrombosis Centre BHSCT A rose by any other name.. Recommendation on the nomenclature for oral anticoagulants: communication from the SSC
Controversies in Anticoagulation : Optimizing Outcome in NOACs for GI Bleeding Risk
 Controversies in Anticoagulation : Optimizing Outcome in NOACs for GI Bleeding Risk Boyoung Joung, MD, PhD Professor, Division of Cardiology Director of Electrophysiology Laboratory Severance Cardiovascular
Controversies in Anticoagulation : Optimizing Outcome in NOACs for GI Bleeding Risk Boyoung Joung, MD, PhD Professor, Division of Cardiology Director of Electrophysiology Laboratory Severance Cardiovascular
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY
 ASWAN UNIVERSITY") New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
New Oral Anticoagulants in treatment of VTE, PE DR.AMR HANAFY (LECTURER OF CARDIOLOGY ) ASWAN UNIVERSITY Fact VTE is deadly! It nibbles after it bites! The 30-day mortality rates for first-time DVT or
Appendix 3 PCC Warfarin Reversal
 Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
Appendix 3 PCC Warfarin Reversal Reversal of Warfarin and Analogues 1. Principle of Procedure Guidelines for the Reversal of Oral-anticoagulation in the Event of Life Threatening Haemorrhage Prothrombin
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway
 Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
pat hways Key therapeutic topic Published: 26 February 2016 nice.org.uk/guidance/ktt16
 pat hways Anticoagulants, including non-vitamin K antagonist oral anticoagulants (NOACs) Key therapeutic topic Published: 26 February 2016 nice.org.uk/guidance/ktt16 Options for local implementation NICE
pat hways Anticoagulants, including non-vitamin K antagonist oral anticoagulants (NOACs) Key therapeutic topic Published: 26 February 2016 nice.org.uk/guidance/ktt16 Options for local implementation NICE