Perioperative Anticoagulation Management
|
|
|
- Ferdinand Casey
- 5 years ago
- Views:
Transcription

1 Perioperative Anticoagulation Management ACP Delaware Chapter Scientific Meeting Feb 9, 2019 Andrew Dunn, MD, MPH, MACP Chief, Division of Hospital Medicine Mount Sinai Health System, NY
2 DISCLOSURES Desai Pharmaceuticals research funding Pfizer / BMS research funding BMS funding for Afib educational module
3 Goals Describe the major factors when determining whether to bridge patients on anticoagulants undergoing surgery Discuss key features in the management of direct oral anticoagulants Identify when to continue anti-platelet therapy Understand when to use antidotes for patients on anticoagulants undergoing procedures
4 Case 1 80 year-old male with a history of hypertension, DM, and atrial fibrillation. The patient has had no history of TIA/stroke or bleeding. Patient is on warfarin with well controlled INRs. The patient will undergo elective major abdominal surgery. Does this patient need to be bridged?
5 To bridge or not to bridge Risk of thromboembolism off anticoagulants Risk of postoperative bleeding after being started on fulldose anticoagulation soon after surgery Consequences of thromboembolism and bleeding Efficacy of anticoagulation Cost and inconvenience
6 6 Risk of event off AC Risk Atrial Fibrillation High CHADS 2 score of 5 or 6 Recent (within 3 mo) stroke or transient ischemic attack Rheumatic valvular heart disease Intermediate CHADS 2 score of 3 or 4 Low CHADS 2 score of 0 to 2 (assuming no prior stroke or transient ischemic attack) Douketis J, et al. Chest. 2012;14 (2 suppl):
7 Perioperative Risk for Bleeding Bridging associated with 3-4-fold increase in major bleeding Siegal D, et al. Circulation 2012;126:1630.
8 Risk of Post-Op Bleeding For certain invasive procedures, major bleeding is rare on OAC Dental extractions (4/2014, 0.2%) Arthrocentesis and joint injection (0/32, 0%) Cataract surgery (0/203, 0%) Upper endoscopy or colonoscopy, with or without biopsy (0/111, 0%). Polypectomy is considered high risk Pacemaker insertion (4%)


9 BRUISECONTROL - Results Pacemaker hematoma continue warfarin 4% interrupt warfarin + bridging 16%
10 Douketis JD, et al. N Engl J Med BRIDGE - Study Design

11 Patient Characteristics Douketis JD, et al. N Engl J Med 2015.

12 Douketis JD, et al. N Engl J Med OUTCOMES
13 13 Case 1 CHADS score? 3 80 year-old male with HTN, DM, afib. No history of TIA/stroke or bleeding. Guideline? Intermediate risk of event bridging can be considered but no certain benefit Risk of bleeding? Moderate Plan: No bridging. Stop warfarin 5 days prior to OR and restart the evening of surgery
14 Case 2 45 year-old female with a history of Crohn s Disease. Subtotal colectomy 2 years ago, which was complicated by a PE in the post-operative period. The patient was treated with warfarin uneventfully for 6 months. The patient subsequently developed a spontaneous DVT 4 months ago and has been on warfarin since that time. The patient is now scheduled for major abdominal surgery.
15 15 What next? Does this patient need to be bridged? What is her risk of recurrent DVT/PE? What is her risk of major post-op bleeding?
16 16 Risk of event off AC Risk VTE High Recent (within 3 mo) VTE Severe thrombophilia (eg, deficiency of protein C, protein S, or antithrombin; antiphospholipid antibodies; multiple abnormalities) Intermediate VTE within the past 3-12 mo Nonsevere thrombophilia (eg, heterozygous factor V Leiden or prothrombin gene mutation) Recurrent VTE Active cancer (treated within 6 mo or palliative) Low VTE >12 mo previous and no other risk factors Douketis J, et al. Chest. 2012;14 (2 suppl):
17 17 Efficacy of AC for VTE patients Treatment dose 80-90% Prophylaxis dose 66-75%
18 18 Case 2 Risk of VTE? Intermediate risk 45 year-old female Crohn s Disease, h/o VTE x2, most recently 8 months ago, now on warfarin. Bridge? Consider bridging Plan: Bridge preop, use prophylaxis dose post-op
19 19 Case 3 68M with PMH DM, HTN, AS status post mechanical AV replacement 2 years ago taking warfarin. Patient planned for nephrectomy for newly diagnosed renal cell carcinoma. What is his risk of an event off AC? Does he need to be bridged?
20 20
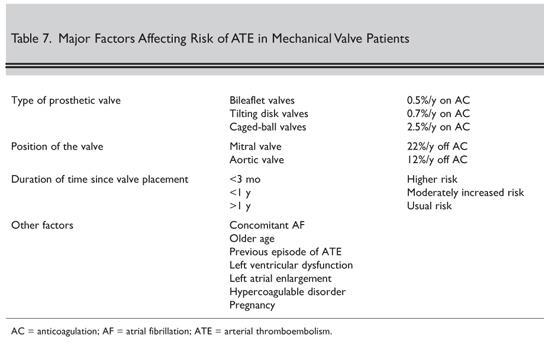
21 21 Risk of event off AC Risk Mechanical Heart Valves High Intermediate Any mitral valve prosthesis Any caged-ball or tilting disc aortic valve prosthesis Recent (within 6 mo) stroke or transient ischemic attack Bileaflet aortic valve prosthesis and one or more of the of following risk factors: atrial fibrillation, prior stroke or transient ischemic attack, hypertension, diabetes, congestive heart failure, age > 75 y Low Bileaflet aortic valve prosthesis without atrial fibrillation and no other risk factors for stroke Douketis J, et al. Chest. 2012;14 (2 suppl):
22 22 Case 3 Risk of TE event? Intermediate 68M DM, HTN, mechanical AV replacement for nephrectomy Bridge? Yes Plan: Bridge with LMWH
23 23 Summary AF / MVR / VTE Risk Example Strategy High Moderate Low VTE within 3 months VTE with severe thrombophilia Afib with CHADS 5-6 or CVA Mechanical mitral valve Older type of AVR VTE 3-12 months ago Recurrent VTE Bileaflet AVR + risk factor Afib with 3-4 stroke risk factors 1 prior VTE >12 months ago Afib with 0-2 stroke risk factors Mechanical bileaflet AVR Bridge - monitor closely for post-op bleeding Bridging can be considered but unproven benefit and possible increased risk No bridging

24 24 THE MECHANICS Hold warfarin at least 5 days prior to procedure Start LMWH 3 days prior to procedure Hold LMWH 24 hours prior to procedure Hold IV heparin 4-6 hours prior to procedure Resume warfarin hours post-op when there is adequate hemostasis Resume heparin post-op depending on risk of bleeding and risk of thrombosis hours after surgery for low bleeding risk surgery hours after surgery for high bleeding risk surgery Consider initially using prophylaxis dose for VTE patients
25 25 Anti-Platelet Agents 60M with PMH DM, HTN, CAD s/p STEMI with LCx DES placed 8 months ago. Patient now found to have colon cancer on routine colonoscopy and planned for right hemicolectomy. Reports excellent exercise tolerance without CP or DOE. Patient takes ASA and Clopidogrel Should we hold? ASA Clopidogrel Both Neither
26 26 Risk Stratification Primary prevention no known CAD Secondary prevention CAD, MI, PCI, CABG, CVA Stent BMS / DES
27 27 Primary Prevention Low risk of event Hold 7 days prior to surgery
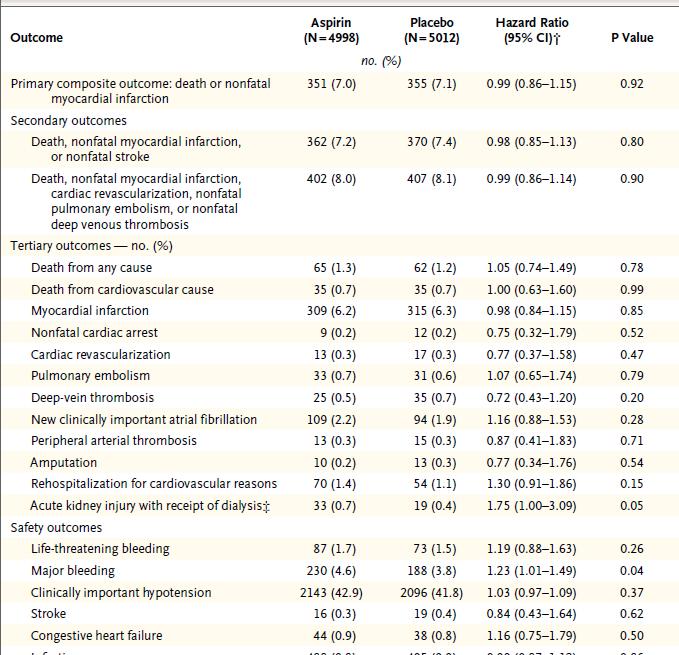
28 28 Secondary Prevention Moderate to high risk of event POISE 2 - APRIL 2014 Randomized 10,010 patients to asa or placebo Patients were at risk for vascular complications At risk defined as: Stratified to whether previously on asa (5600 patients) or were asa naïve (4400 patients) 200mg just before surgery then 100mg daily Primary outcome: Death or nonfatal MI at 30 days Devereaux PJ. NEJM. 2014;370:
29 Inclusion criteria Age >45 years and 1 or more of the following: CAD 2. PAD 3. CVA 4. Major vascular surgery 5. Any 3 of the following A. Age 70 years B. Major surgery (intraperitoneal, intrathoracic, retroperitoneal, major ortho) C. CHF D. TIA E. DM F. Hypertension G. CKD (creatinine >2.0 mg/dl) H. Smoking (within 2 years) I. Emergent/urgent surgery
30
31 Secondary Prevention - Guidelines 31 ACC / AHA cites POISE-2 and PEP as negative trials. States only 23% POISE-2 patients had CAD 2,300 subjects! Cites meta-analysis purporting to show increased MI when asa discontinued; actually found no studies comparing rates Gives 2 conflicting recommendations: May be reasonable to continue asa when the risk of potential increased cardiac events outweighs the risk of increased bleeding. Initiation or continuation of asa is not beneficial in patients undergoing elective surgery who have not had previous coronary stenting, unless the risk of ischemic events outweighs the risk of surgical bleeding. Bottom Line: Data supports holding
32 Secondary Prevention What to Do 32 Minor surgery / procedures: Doubtful any benefit but can continue given lack of harm Major surgery: Preferably hold anti-platelet agent; Clinician flexibility given need to work with other disciplines (Anesthesia)
33 33 Intracoronary Stents Patients are on DAPT for variable duration RCT in peri-op period none Safety of holding thienopyridine uncertain Determine risk off DAPT
34 DAPT Trial 12 vs 30 months DAPT after DES All receive 12 months thienopyridine (clopidogrel or prasugrel) and asa All patients cont asa Randomized to continue thienopyridine or placebo for 18 months Primary efficacy end points: Stent thrombosis Major adverse cardiovascular and cerebrovascular events (death, MI, or CVA) Mauri L et al. N Engl J Med. 2014;371:

35 DAPT OUTCOMES Mauri L et al. N Engl J Med. 2014;371:
36 DAPT Longer vs Shorter Duration Impact on Mortality Meta-analysis of longer- versus shorter-duration DAPT (aspirin plus a P2Y12 inhibitor) after DES 36 Main outcomes - Mortality, MI, Major bleeding. Spencer FA, et al. Ann Int Med
37 Longer Versus Shorter Duration Dual-Antiplatelet Therapy After Drug-Eluting Stent Placement: A Systematic Review and Meta-analysis MORTALITY Spencer FA, et al. Ann Int Med
38 Longer Versus Shorter Duration Dual-Antiplatelet Therapy After Drug-Eluting Stent Placement: A Systematic Review and Meta-analysis MI Spencer FA, et al. Ann Int Med
; p value for ES=0.02 D+L: p value for ES=0.02 1.32 (0.49, 3.55) 0.75 (0.56, 1.02) 0.71 (0.45, 1.10) 0.57 (0.17, 1.")
39 Mortality with Extended Duration DAPT After DES: Meta-Analysis of 10 RCTs and 31,666 Pts Study All-cause Death HR (95% CI) Weight (%) Events Group 1 Events Group 2 ARTIC Interruption DAPT DES LATE EXCELLENT ISAR SAFE ITALIC OPTIMIZE PRODIGY RESET SECURITY I-V (I 2 =0.0%, p=0.93); p value for ES=0.02 D+L: p value for ES= (0.49, 3.55) 0.75 (0.56, 1.02) 0.71 (0.45, 1.10) 0.57 (0.17, 1.95) 0.66 (0.27, 1.63) 1.14 (0.41, 3.15) 0.95 (0.63, 1.45) 0.91 (0.61, 1.37) 0.62 (0.20, 1.88) 1.00 (0.37, 2.66) 0.82 (0.69, 0.98) 0.82 (0.69, 0.98) /624 74/ /2514 4/722 8/1997 8/912 43/ /751 5/1059 8/ / /635 98/ /251 7/721 12/2003 7/910 45/ /750 8/1058 8/ / Shorter DAPT better Longer DAPT better MI: No diff Palmerini T, et al. JACC. 2015;65:
40 Palmerini T, et al. JACC. 2015;65: Mortality with Extended Duration DAPT After DES: Meta-Analysis of 10 RCTs and 31,666 Pts Study Cardiac Death HR (95% CI) Weight (%) Events Group 1 Events Group 2 DAPT DES LATE EXCELLENT ITALIC OPTIMIZE PRODIGY RESET SECURITY I-V (I 2 =0.0%, p=0.85); p value for ES=0.52 D+L: p value for ES= (0.70, 1.53) 0.68 (0.38, 1.23) 0.67 (0.11, 3.99) 1.67 (0.40, 6.97) 0.90 (0.55, 1.49) 0.92 (0.53, 1.58) 0.50 (0.91, 2.73) 1.64 (0.41, 6.59) 0.93 (0.73, 1.17) 0.93 (0.73, 1.17) / /2514 2/722 5/912 29/ /751 2/1059 5/ / / /2531 3/721 3/910 32/ /750 4/1058 3/ / Shorter DAPT better Longer DAPT better
41 Palmerini T, et al. JACC. 2015;65: Mortality with Extended Duration DAPT After DES: Meta-Analysis of 10 RCTs and 31,666 Pts Study Non-cardiac Death HR (95% CI) Weight (%) Events Group 1 Events Group 2 DAPT DES LATE EXCELLENT ITALIC OPTIMIZE PRODIGY RESET SECURITY I-V (I 2 =0.0%, p=0.71); p value for ES=0.006 D+L: p value for ES= (0.29, 0.76) 0.68 (0.34, 1.37) 0.50 (0.09, 2.74) 0.75 (0.17, 3.30) 1.07 (0.50, 2.28) 0.90 (0.49, 1.65) 0.73 (0.16, 3.26) 0.60 (0.15, 2.42) 0.67 (0.51, 0.89) 0.67 (0.51, 0.89) / / / /2531 2/722 4/721 3/912 4/910 14/ / /751 22/750 3/1059 4/1058 3/682 5/717 80/ 119/ Shorter DAPT better Longer DAPT better
42 42 Intracoronary Stents BOTTOM LINE Complex and mixed results 6 months DAPT likely offers equal protection against MI compared to 12 months, and 12 months DAPT decreases MI and stent thrombosis but increases mortality and major bleeding.
43 ACC/AHA Guideline Update on Duration of Dual Antiplatelet Therapy in CAD 43 In patients with CAD treated with a DES, clopidogrel should be given for at least 6 months (Class I) In patients with CAD treated with a BMS, clopidogrel should be given for at least 1 month (Class I) Levine GN. J Am Coll Cardiol
44 44 Intracoronary Stents Delay surgery for at least 1 month after BMS and 6 months after DES. When outside this window, cont ASA and hold Clopidogrel If unable to delay, discuss continuing dual antiplatelet therapy with Surgery If <1 month for BMS or <6 months for DES (<12 months if placed in setting of ACS) and unable to delay or to continue DAPT, consider bridging with IV cangrelor
45 45 Direct Oral Anticoagulants Dabigatran Rivaroxaban Apixaban Edoxaban Peri-operative benefits: Short half life No monitoring Drawbacks: Not short enough No monitoring
46 CASE 4 78-yr female with AF on dabigatran, 150 mg BID, scheduled for elective hip replacement CHADS score = 4 (prior TIA, age >75, htn) CrCl = 45 ml/min (moderate CKD)
47 47 DOAC Management Peri-Op Depends on renal function and type of surgery GFR >50 Low Bleed Risk Surgery Pre-op: Hold 1 day prior to OR Post-op: Resume 1 day after OR High Bleed Risk Surgery Pre-op: Hold 2 days prior to OR Post-op: Resume 2-3 days after OR GFR <50 Pre-op: Hold 2 days prior to OR Post-op: Resume 1 day after OR Pre-op: Hold 3-4 days prior to OR Post-op: Resume 2-3 days after OR * Neuraxial anesthesia Timing varies by agent and dose.
48 DOACs: Implications of Irreversibility Fatal Bleeding Case Fatality Rate ATRIAL FIBRILLATION VKA DOAC NNT 0.51% 0.27% % 5.8% trials N = 100,324 Fatal Bleeding Case Fatality Rate VENOUS THROMBOEMBOLISM VKA DOAC NNT 0.16% 0.06% % 5.2% NS Caldeira D, et al. Heart. 2015;101:
49 GROUP A: Serious bleeding (n=51) GROUP B: Urgent procedure (n=39) Pollack CV. New Engl J Med. 2015;373;
50 Normalized clotting time 88% to 98% patients; Onset within minutes. Group A Hemostasis restored: median of 11.4 hours. Group B Normal intra-operative hemostasis: 33/36

51 Reversal Agents Factor Xa Inhibitors Andexanet alfa: F-Xa Inhibitor Antidote Factor Xa decoy - Targets and sequesters Factor Xa inhibitors Once bound, Factor Xa inhibitors unable to bind native Factor Xa Demonstrated reversal of Factor Xa inhibitors by biomarkers

52 Acute major bleeding N = 67 Bolus plus 2 hour infusion Connolly SJ. New Engl J Med. 2015;375;
53 4-Factor PCC in Patients on VKA with Major Bleeding Randomized to 4F-PCC or FFP Primary analyses: 24-hour hemostatic efficacy INR correction ( 1.3) at 30 minutes N = 202 patients Median INR: 3.9 PCC group and 3.6 FFP group Sarode R. Circulation. 2013;128:
54 4-Factor PCC in Patients on VKA with Major Bleeding RESULTS Effective hemostasis achieved in 72% and 65% of patients, noninferior (CI, 5.8 to 19.9) Rapid INR reduction: 62% of patients receiving 4F-PCC versus 9% receiving FFP (P<.05) Coagulation factors higher in the PCC group from 0.5 to 3 hours after infusion start (P<0.02) Adverse events, thromboembolic events, and deaths - No diff Sarode R. Circulation. 2013;128:

55 Steiner T. Lancet Neurol. 2016;15:
56 Chest Guidelines Anticoagulation & Thrombosis 9 th Edition (AT9) 9.3. For patients with VKA-associated major bleeding, we suggest rapid reversal of anticoagulation with 4-factor prothrombin complex concentrate rather than with plasma (2C). Holbrook A, et al. Chest. 2012;e152S-e184S.
 Zahir H. Circulation.")
57 4-Factor PCC for DOAC Bleeding 4F-PCC vs placebo in volunteers given anti-fxa inhibitor Edoxaban 60mg vs Placebo, N=93 Punch biopsy - Bleeding duration fully corrected with the highest dose of 4F-PCC evaluated (50 U/kg) Zahir H. Circulation. 2015;131:82-90.
58 TAKE HOME POINTS 58 AFIB - Don t bridge (most patients) Mech valves Bridge (except lone A-valve) VTE Bridge high risk patients and consider postop proph dose after major surgery Antiplatelets: Primary prevention hold 7 days; secondary prevention hold for most patients DAPT DES Wait 6-12 months then hold thienopyridine DOAC Bridging rarely indicated; Restart post-op as for LMWH
59 Questions? 59
Atrial Fibrillation. 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018
 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Predicting & Managing Cardiac Risk A 70-y.o. man with progressive
Anticoagulation Transitions: Perioperative Care
 Anticoagulation Transitions: Perioperative Care Alan Brush, MD, FACP Clinical Co-Director, Anticoagulation Management Service Harvard Vanguard Medical Associates Four Questions for each Consultation 1.
Anticoagulation Transitions: Perioperative Care Alan Brush, MD, FACP Clinical Co-Director, Anticoagulation Management Service Harvard Vanguard Medical Associates Four Questions for each Consultation 1.
Anticoagulation Overview Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita
 Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
Anticoagulation Overview 2018 Jed Delmore, MD, FACS, FACOG Professor Obstetrics and Gynecology University of Kansas School of Medicine, Wichita The ideal lecture is like a miniskirt. Short enough to get
ANTICOAGULATION: THE DO'S AND DON'TS OF BRIDGE THERAPY
 ANTICOAGULATION: THE DO'S AND DON'TS OF BRIDGE THERAPY SATURDAY/11:30AM-12:30PM ACPE UAN: 0107-9999-17-236-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon
ANTICOAGULATION: THE DO'S AND DON'TS OF BRIDGE THERAPY SATURDAY/11:30AM-12:30PM ACPE UAN: 0107-9999-17-236-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon
WARFARIN: PERI OPERATIVE MANAGEMENT
 WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin treated patients who require an elective or urgent surgery/procedure. To provide an approach
Managing Perioperative Anticoagulation. Edie Shen MD
 Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
WARFARIN: PERI-OPERATIVE MANAGEMENT
 WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
WARFARIN: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide an approach to the perioperative management of warfarin-treated patients who require an elective or urgent surgery/procedure. To provide an approach
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Challenging Anticoagulation Case Studies. Earl J. Hope, M.D. Tower Health Cardiology
 Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
Challenging Anticoagulation Case Studies Earl J. Hope, M.D. Tower Health Cardiology Financial Disclosures Nothing to disclose Objectives: 1. Understand indications for heparin bridging. 2. Recognize the
2017 Bryan Health Primary Care Conference. Dale Hansen MD Bryan Heart 5/20/17
 2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
2017 Bryan Health Primary Care Conference Dale Hansen MD Bryan Heart 5/20/17 I have no financial disclosures or conflicts of interest Bridging Anticoagulation Primum Non Nocere 67 y.o. male with mechanical
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Disclosures. Overview. Have you ever. The Perioperative Management of Anticoagulants. No financial conflicts of interest to disclose
 Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Disclosures No financial conflicts of interest to disclose The Perioperative Management of Anticoagulants Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical
Endoscopy and the Anticoagulated Patient
 Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Endoscopy and the Anticoagulated Patient John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School Objectives To accurately assess the risk
Bridging anticoagulation definition
 Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Bridging anticoagulation definition Giving a short-acting anticoagulant, consisting of sc LMWH or ev UFH for 10 to 12 day period during interruption of VKA therapy when the INR is not within therapeutic
Update in Perioperative Anticoagulation and Antiplatelet management
 Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
Update in Perioperative Anticoagulation and Antiplatelet management Grand Rounds October 31, 2014 Brooke Hall, MD Steve Kornfeld, MD Bruce McLellan, MD Nothing to disclose Objectives Describe the updates
Clinical Practice Guideline for Anticoagulation Management
 Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
Clinical Practice Guideline for Anticoagulation Management This guideline is to inform practitioners of the Standard of Care for providing safe and effective anticoagulation management for ambulatory patients.
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery. Alex C. Spyropoulos MD, FACP, FCCP, FRCPC
 who Need Elective Surgery. Alex C. Spyropoulos MD, FACP, FCCP, FRCPC") The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery Alex C. Spyropoulos MD, FACP, FCCP, FRCPC Professor of Medicine Hofstra Northwell School of Medicine
The Management of Patients on Chronic Oral Anticoagulant Therapy (VKA and DOAC) who Need Elective Surgery Alex C. Spyropoulos MD, FACP, FCCP, FRCPC Professor of Medicine Hofstra Northwell School of Medicine
Anti-thrombotics and Colonoscopy. Anna Rahmani, MD. Ph.D. FRCPC
 Anti-thrombotics and Colonoscopy Anna Rahmani, MD. Ph.D. FRCPC DICLOSURES: consultations fees: Servier and Sanofi Pharmaceuticals Thrombosis Clinic Educational Fund: Servier CONFLICT OF INTEREST: NONE
Anti-thrombotics and Colonoscopy Anna Rahmani, MD. Ph.D. FRCPC DICLOSURES: consultations fees: Servier and Sanofi Pharmaceuticals Thrombosis Clinic Educational Fund: Servier CONFLICT OF INTEREST: NONE
DISCLOSURE. What I am Talking About. Rational Use of Antiplatelet Agents. Aspirin. Tom DeLoughery, MD MACP FAWM
 Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Rational Use of Antiplatelet Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University What I am Talking About 1. Current
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K. B. Cosmi
 Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Gestione peri-operatoria del paziente in terapia con antagonisti della vitamina K B. Cosmi Department of Angiology and Blood Coagulation S. Orsola-Malpighi University Hospital Bologna, Italy Overview Background
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Perioperative Management of Warfarin Interruption
 Perioperative Management of Warfarin Interruption Victoria Lambert, PharmD, CACP Medication Management Pharmacist William W. Backus Hospital Faculty Disclosures There are no actual or potential conflicts
Perioperative Management of Warfarin Interruption Victoria Lambert, PharmD, CACP Medication Management Pharmacist William W. Backus Hospital Faculty Disclosures There are no actual or potential conflicts
t. Recommendations for periprocedural anticoagulation are available lhrough the American College of Chest Physicians Clinical Practice Guidelines.
 Name or Policy: Policy Number: 3364-133-116 Department: Approving Officer: Responsible Agent: cope: x Management of Anticoagulation with Invasive Procedures Pharmacy Chief Operating Officer Director of
Name or Policy: Policy Number: 3364-133-116 Department: Approving Officer: Responsible Agent: cope: x Management of Anticoagulation with Invasive Procedures Pharmacy Chief Operating Officer Director of
Do s and Don t of DOACs DISCLOSURE
 Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Do s and Don t of DOACs Tom DeLoughery, MD MACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none Content Expert: Elsevier
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
on Anti-coagulants -- Is It Safe? And When to Stop?
 Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Endoscopy for Your Patient on Anti-coagulants -- Is It Safe? And When to Stop? John R. Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical
Clinical Practice Committee Anticoagulation Bridging Document
 Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Original: 10/23/06 Last Updated: 10/30/07 Clinical Practice Committee Do patients on long term oral anticoagulant therapy who require short term interruption of warfarin for an elective invasive procedure
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Preoperative Cardiac Evaluation:
 Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
Preoperative Cardiac Evaluation: The New Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Disclosures No financial relationships with pharmaceutical
To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin
 To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin Omprakash Pansara, MD Brian Kline, MD St. Joseph s Health Family Medicine Residency Program, Syracuse, NY Case 75yr old male, who
To Bridge or Not to Bridge? Preop Evaluation of the Patient on Coumadin Omprakash Pansara, MD Brian Kline, MD St. Joseph s Health Family Medicine Residency Program, Syracuse, NY Case 75yr old male, who
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center
 The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
The INR: No Need Anymore? Daniel Blanchard, MD Professor of Medicine Director, Cardiology Fellowship Program UCSD Sulpizio Cardiovascular Center What is the INR? Tissue Factor (Factor III) is added to
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Clinical Controversies in Perioperative Medicine
 Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Evaluation: New Guidelines A 70-y.o. man with progressive
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Joost van Veen Consultant Haematologist
 Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
CASE IN... Anticoagulation: When to Start,When to Stop. The management of patients who require an. Meet Tracey. Anticoagulation
 Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
Anticoagulation: When to Start,When to Stop Ebtisam Bakhsh, MD; and James D. Douketis, MD, FRCPC Presented at McMaster University s Thrombosis and Hematology Update, October 2006. CASE IN... Anticoagulation
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Slide 1: Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
Perioperative Management of Anticoagulation by Steven L. Cohn, MD, FACP Director, Medical Consultation Service, Kings County Hospital Center, Clinical Professor of Medicine, SUNY Downstate, Brooklyn, NY
NOACS/DOACS*: PERI-OPERATIVE MANAGEMENT
 NOACS/DOACS*: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide guidance for the peri-operative management of patients who are receiving a newer direct oral anticoagulant (DOAC) and require an elective surgery/procedure.
NOACS/DOACS*: PERI-OPERATIVE MANAGEMENT OBJECTIVE: To provide guidance for the peri-operative management of patients who are receiving a newer direct oral anticoagulant (DOAC) and require an elective surgery/procedure.
Low-Molecular-Weight Heparin
 Low-Molecular-Weight Heparin Policy Number: Original Effective Date: MM.04.019 10/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO 10/28/2011 Section: Prescription Drugs Place(s) of Service:
Low-Molecular-Weight Heparin Policy Number: Original Effective Date: MM.04.019 10/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO 10/28/2011 Section: Prescription Drugs Place(s) of Service:
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients
 4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
4.7 Algorithm for the Peri-operative Management of Anticoagulants and Antiplatelet agents in Adult patients Assess Thrombosis risk: baseline risk in an individual patient plus additional thrombotic risk
Preoperative Management of Patients Receiving Antithrombotics
 Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Preoperative Management of Patients Receiving Antithrombotics Bleeding complications remain an important concern for most surgical procedures. Attempts to minimize the risk of these complications by removing
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Perioperative Management. Perioperative Management of Cardiovascular Medications
 of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
of Cardiovascular Medications Carmine D Amico, D.O. Overview Learning objectives Beta-blockers Statins Alpha-2 agonists Calcium channel blockers ACE inhibitors and ARB s Anticoagulants Antiplatelet agents
Perioperative Management of Anticoagulation
 Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Perioperative Management of Anticoagulation Presented By: Nibal R. Chamoun, PharmD, BCPS Clinical Assistant Professor, Clinical Coordinator Lebanese American University, School of Pharmacy Presented at:
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
ANTICOAGULANTS AND HIP FRACTURE SURGERY. Jon Antrobus Anaesthetist Borders General Hospital
 ANTICOAGULANTS AND HIP FRACTURE SURGERY Jon Antrobus Anaesthetist Borders General Hospital Anticoagulation is common amongst the hip fracture patient population (6-10%) Anticoagulation signifies co-morbidity
ANTICOAGULANTS AND HIP FRACTURE SURGERY Jon Antrobus Anaesthetist Borders General Hospital Anticoagulation is common amongst the hip fracture patient population (6-10%) Anticoagulation signifies co-morbidity
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Bleeding Management Strategies. Aiming for the best Outcomes August 27, Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM
 Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Bleeding Management Strategies Aiming for the best Outcomes August 27, 2016 Amit Gupta, MD FACC FSCAI Interventional Cardiologist CANM Learning Objectives Review the use of anti-coagulants in patients
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
The Direct Oral Anticoagulants: Practical Considerations. David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015
 The Direct Oral Anticoagulants: Practical Considerations David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015 Disclosure Occasional consultant to : BMS, Pfizer, Daiichi
The Direct Oral Anticoagulants: Practical Considerations David Garcia, MD University of Washington Seattle Cancer Care Alliance September 2015 Disclosure Occasional consultant to : BMS, Pfizer, Daiichi
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Preoperative Evaluation Guidelines and Work up
 Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
Preoperative Evaluation Guidelines and Work up Wesley Fiser, MD Disclosures: None 1 Case An 80 year old woman with osteoarthritis of the hip, DM, CKD (Cr 2.1), and HTN is diagnosed with an obstructing
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
Update on Oral Anticoagulation for Mechanical Heart Valves
 Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Controversies in Perioperative Medicine
 Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Controversies in Perioperative Medicine Staying Abreast & Ahead of the Guidelines Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Controversies in Perioperative
Low-Molecular-Weight Heparin
 Low-Molecular-Weight Heparin Policy Number: Original Effective Date: MM.04.019 10/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2016 Section: Prescription Drugs
Low-Molecular-Weight Heparin Policy Number: Original Effective Date: MM.04.019 10/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 05/01/2016 Section: Prescription Drugs
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Stolling en anesthesie. Erik Vandermeulen MD, PhD Dept. of Anesthesia
 Stolling en anesthesie Erik Vandermeulen MD, PhD Dept. of Anesthesia Preoperative use of anticoagulation Vitamin K-antagonists (VKA) Fenprocoumon (Marcoumar ) Warfarin (Marevan ) Acenocoumarol (Sintrom
Stolling en anesthesie Erik Vandermeulen MD, PhD Dept. of Anesthesia Preoperative use of anticoagulation Vitamin K-antagonists (VKA) Fenprocoumon (Marcoumar ) Warfarin (Marevan ) Acenocoumarol (Sintrom
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Direct Oral Anticoagulants: Knocking Down the DOAC Barriers Ohio ACP Chapter Meeting October 2018
 Direct Oral Anticoagulants: Knocking Down the DOAC Barriers Ohio ACP Chapter Meeting October 2018 Andrew Dunn, MD, MPH Professor of Medicine Chief, Division of Hospital Medicine Mount Sinai Health System
Direct Oral Anticoagulants: Knocking Down the DOAC Barriers Ohio ACP Chapter Meeting October 2018 Andrew Dunn, MD, MPH Professor of Medicine Chief, Division of Hospital Medicine Mount Sinai Health System
Peri-Procedural Management of Antithrombotic Agents
 u Peri-Procedural Management of Antithrombotic Agents An Integrated Care Pathway of the Collaborative Care Network Subject Matter Experts: Will Maxted, MD Veronica Kerner, PharmD Pathway Custodian: Pat
u Peri-Procedural Management of Antithrombotic Agents An Integrated Care Pathway of the Collaborative Care Network Subject Matter Experts: Will Maxted, MD Veronica Kerner, PharmD Pathway Custodian: Pat
New Antithrombotic Agents
 New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
New Antithrombotic Agents Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None What I am Talking About 1. New Antithrombotic
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı
 ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
ANTITHROMBOTIC THERAPY 2010 Antitrombotik tedavi alan hastalarda operasyon hazırlığı Dr. Sabri DEMİRCAN Ondokuz Mayıs Üniversitesi Tıp Fakültesi Kardiyoloji ABD, Samsun Copyright 2001 Harcourt Canada Ltd.
3/19/2012. What is the indication for anticoagulation? Has the patient previously been on warfarin? If so, what % of the time was the INR therapeutic?
 Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Abigail E. Miller, PharmD, BCPS Clinical Specialist, Cardiology University of North Carolina Hospitals I have no personal financial relationships with the manufacturers of the products to disclose. Boehringer
Nanik Hatsakorzian Pharm.D/MPH
 Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
Pharm.D/MPH 2014 1 Therapeutics FDA indication & Dosing Clinical Pearls Anticoagulants Heparin Antiphospholipid antibody syndrome Cerebral thromboembolism Prosthetic heart valve Acute coronary syndrome
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
DOAC and NOAC are terms for a novel class of directly acting oral anticoagulant drugs including Rivaroxaban, Apixaban, Edoxaban, and Dabigatran.
 Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Guideline for Patients on Direct Oral Anticoagulant Therapy Requiring Urgent Surgery for Hip Fracture Trust Ref:C10/2017 1. Introduction This guideline is for the clinical management of patients on direct
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Perioperative management of Anticoagulant and Antiplatelet medication GL067
 Perioperative management of Anticoagulant and Antiplatelet medication GL067 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair, Anaesthetics Clinical November
Perioperative management of Anticoagulant and Antiplatelet medication GL067 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair, Anaesthetics Clinical November
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
New Oral Anticoagulants in Everyday Practice: Addressing Common Clinical Scenarios and Questions not covered by the big trials
 New Oral Anticoagulants in Everyday Practice: Addressing Common Clinical Scenarios and Questions not covered by the big trials James Douketis, MD, FRCPC Specialty: Internal Medicine Professor, Department
New Oral Anticoagulants in Everyday Practice: Addressing Common Clinical Scenarios and Questions not covered by the big trials James Douketis, MD, FRCPC Specialty: Internal Medicine Professor, Department
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture
 Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Consensus Statement for Management of Anticoagulants and Antiplatelet drugs in Patients with Hip Fracture Patients with hip fractures should be operated on within 36 hours of presentation wherever possible.
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Update on Oral Anticoagulants. Dr. Miten R. Patel Cancer Specialists of North Florida Cell
 Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Update on Oral Anticoagulants Dr. Miten R. Patel Cancer Specialists of North Florida Cell 904-451-9820 Email miten.patel@csnf.us Overview Highlights of the 4 new approved oral anticoagulants Results from
Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline
 Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline A. Scope (disease/condition, treatment, clinical specialty) 1. Adult patients undergoing a procedure or surgery
Periprocedural Anticoagulation Adult Inpatient and Ambulatory Clinical Practice Guideline A. Scope (disease/condition, treatment, clinical specialty) 1. Adult patients undergoing a procedure or surgery
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Drug Class Monograph
 Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial