PREVENTIVE AND REHABILITATIVE MANAGEMENT OF ACUTE CORONARY SYNDROMES (NSTEMI, STEMI, PCI)
|
|
|
- Alexina Reed
- 5 years ago
- Views:
Transcription

 Dato")

1 PREVENTIVE AND REHABILITATIVE MANAGEMENT OF ACUTE CORONARY SYNDROMES (NSTEMI, STEMI, PCI) Dato Dr. Balachandran Kandasamy Institut Jantung Negara 12 th November 2016
2 KEY MESSAGES 1. Initiate a long-term management plan for all patients with acute coronary syndromes (ACS) 2. Consider guideline-recommended medicines for all patients with ACS 3. Identify risk factors and refer all patients with ACS to secondary prevention programs 4. Communicate management plan to the patient, carers and the community healthcare providers
3 INITIATE A LONG-TERM MANAGEMENT PLAN FOR ALL PATIENTS WITH ACUTE CORONARY SYNDROMES Patients with ACS are at high risk of further cardiovascular events and death. For long-term management a medicines management plan, a chest pain action plan and a comprehensive cardiovascular risk reduction program are recommended. Communicate this plan to the patient and/or carer and their community healthcare providers.
4 INITIATE A LONG-TERM MANAGEMENT PLAN FOR ALL PATIENTS WITH ACUTE CORONARY SYNDROMES i. Medicines management plan ii. Chest pain action plan iii. Identify risk factors and refer to secondary prevention programs

5 i. Medicines Management Plan Consider starting guideline-recommended medicines in hospital before discharge. Provide all patients with a written medicines management plan which includes: a list of all medicines the dose and plan for any required dose titration intended duration of therapy the purpose and potential benefits of therapy potential adverse effects of each medicines schedule for follow-up and monitoring access to consumer medicine information.
6 INITIATE A LONG-TERM MANAGEMENT PLAN FOR ALL PATIENTS WITH ACUTE CORONARY SYNDROMES Communicate the management plan to patients and all those involved in care
7 ii. Identify Risk Factors And Refer To Secondary Prevention Programs Discuss the warning signs of a heart attack and an immediate plan of action, including the use of short-acting nitrates and the importance of dialling 000 if pain is not relieved. Each patient should receive a written chest pain action plan which includes: warning signs of a heart attack when and how to take the short-acting nitrate self-administration of aspirin, unless contraindicated instructions to call an ambulance if chest pain or discomfort lasts longer than 10 minutes additional instructions for patients who live in rural and remote locations
8 iii. Identify Risk Factors And Refer To Secondary Prevention Programs Actively refer to, and encourage attendance at, secondary prevention and cardiac rehabilitation programs. Provide education and set goals on lifestyle factors, including advice on smoking cessation where appropriate. Assess for depression and level of social support.
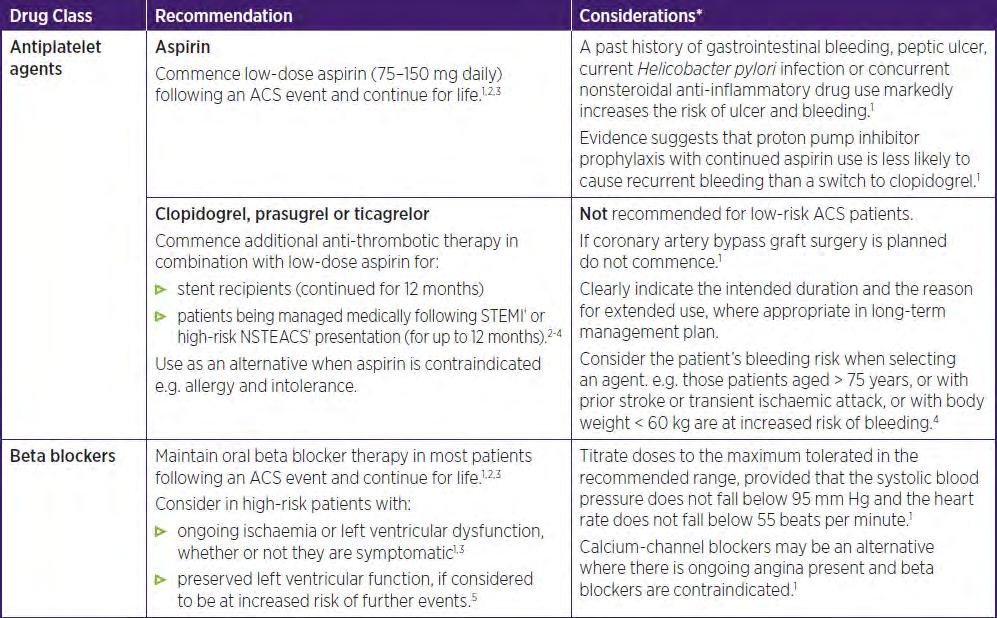
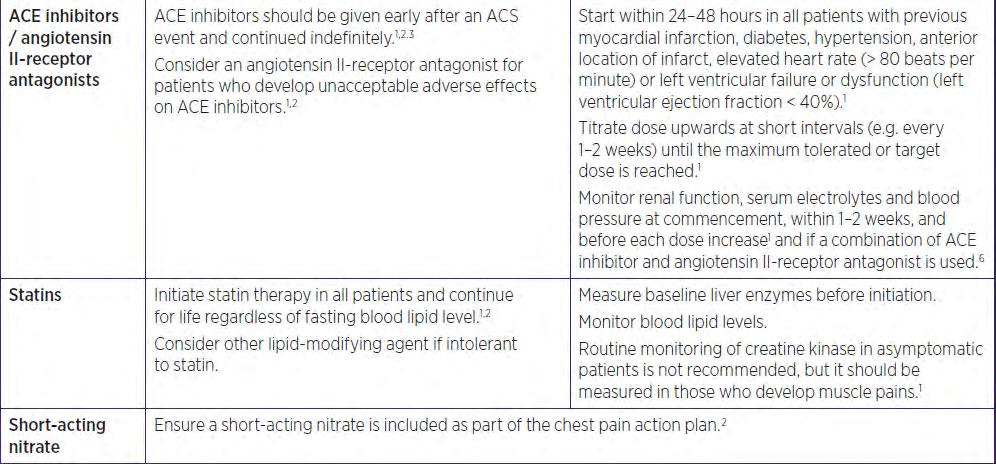
9 CONSIDER GUIDELINE-RECOMMENDED MEDICINES FOR ALL PATIENTS WITH ACS The combination of antiplatelet agents, a beta blocker, a statin and an angiotensin-converting enzyme (ACE) inhibitor is recommended for most patients, unless contraindicated. All four drug classes have been proven to reduce subsequent cardiac events and death. Individualise therapy according to known comorbidities, risk of adverse effects and clinical judgement. If the guideline-recommended therapy is not indicated for an individual, document this and the reason(s) why in the patient s medical record and long-term management plan.
10
11
12 IDENTIFY RISK FACTORS AND REFER ALL PATIENTS WITH ACS TO SECONDARY PREVENTION PROGRAMS Provide patients with a self-management plan before discharge, as patients and their families/carers are focused on promoting health and are more receptive to medical interventions immediately after an acute event. The plan should include advice on lifestyle changes that will reduce the risk of further cardiac events (including quitting smoking, good nutrition, moderating alcohol intake, regular physical activity and weight management), as appropriate. All patients should have access to, and be actively referred to, comprehensive secondary prevention and cardiac rehabilitation programs.
13 Refer All Patients to Their Closest Available Cardiac Rehabilitation Program Cardiac rehabilitation is a proven effective intervention. Attendance at cardiac rehabilitation outpatient programs reduces risk of further cardiac events. Cardiac rehabilitation, including advice about physical activity, improves individual health outcomes. Patients who participate in cardiac rehabilitation programs can improve physical activity, weight loss, smoking cessation, blood lipid levels and blood pressure control.
14 PRINCIPAL GOAL: CARDIAC REHABILITATION To lessen the risk of future coronary events, control symptoms arising from coronary disease and to return the patient to optimal or previous functional status Patient population predominantly confined to post MI, bypass graft, angioplasty & stable angina but must also be made available to heart failure patients. M.A CALDWELL & K. DRACUP, JOURNAL OF CARDIOPULMONARY REHABILITATION 2001
15 THE FOUR PHASES OF CARDIAC REHABILITATION Phase I Before discharge from hospital Phase II Early post-discharge period Phase III 4-6 weeks after an acute cardiac event Phase IV Long term maintenance of changed behaviour

16 PHYSIOTHERAPY IN IJN Inpatients & Outpatients Acute Care Cardiac Rehabilitation Programme I & II Ward Gym Patient Referral Exercise Programme
17 OTHER BENEFICIAL EFFECTS OF CARDIAC REHABILITATION FOR PATIENTS WITH CHD Improves Control of Dyslipidemia in secondary prevention B.L.,Verges et al Journal of Cardiopulmonary Rehabilitation, 1998 Weight loss intervention P.D., Savage et al Journal of Cardiopulmonary Rehabilitation, 2002 Post Myocardial infarction or CABG J. Redfern, Journal of Physiotherapy, 2011 Stable Chronic Heart Failure- can achieve significant improvement in functional capacity from a low intensity exercise training program. R. Belardinelli et al J Am Coll Cardiol, 1995 Exercise training improves exercise tolerance and LV function in patients with Dilated Cardiomyopathy K.Q., Stolen et al J Am Coll Cardiol, 2003
, resume and maintain as normal a place as possible in the community F.J.Brannon et al:cardiopulmonary rehabilitation: Basic Theory and Application 2 nd Ed, pg.")
18 WHO Definition of Cardiac Rehabilitation The Sum of Activities required to ensure the patients, the best possible physical, mental and social conditions, so that they may (by their own efforts), resume and maintain as normal a place as possible in the community F.J.Brannon et al:cardiopulmonary rehabilitation: Basic Theory and Application 2 nd Ed, pg.148(1993)

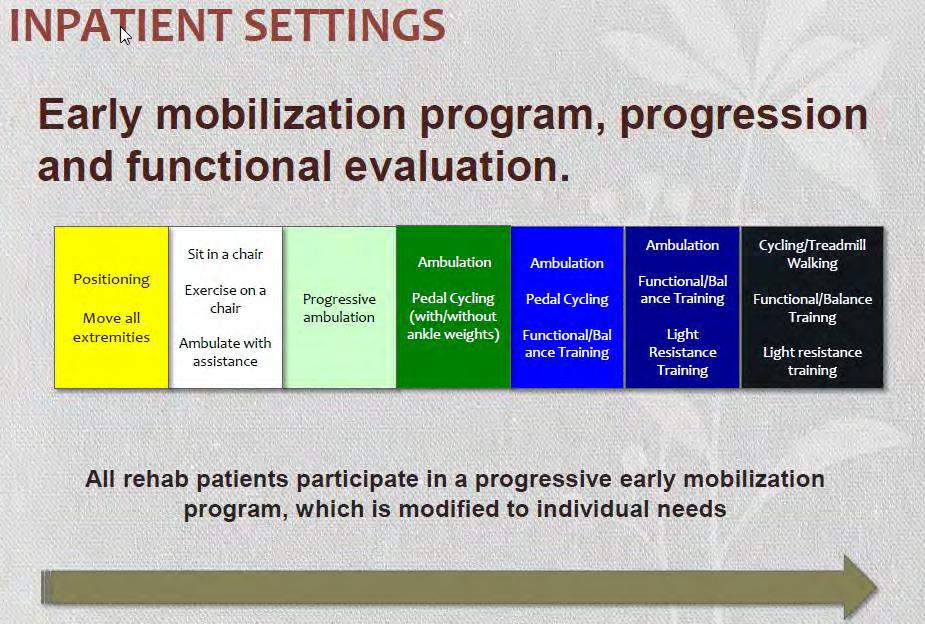
19 CARDIAC REHABILITATION PHASE I Inpatient recovery program (ICU/ WARDS/ GYM) Post MI start 2-4 days after hospitalized Post surgery start 1-2 days after surgery Lasts for 2-3 weeks Intensive medical supervision Low intensity exercise ( METS) 60% - 70% of MHR Exercise done daily- shoulder and arm exercises, gentle trunk exercises, ambulating short distances, gym & a flight of stairs without adverse symptoms
20
21
22

23
24 CARDIAC REHABILITATION PHASE II (IJN) Out patient convalescence program Starts within 2-3 weeks of discharge Lasts for 3 months Referred by physician and medically supervised Light to moderate exercise (2-5 METS) 65% - 75% of MHR 3 times per week 14/11/



")
25 PHYSIOTHERAPY & REHABILITATION DEPT., IJN, CRP PHASE II 1. Strengthening Exercises Assessment 5. Stretching and Cool down Circuit Training 2. Endurance Exercise (stationary bike or treadmill) Re-assessment 4. Exercise tolerance (walking for 6 mins) 3. Exercise Tolerance( step board) Patient Education 14/11/

26 Warm up/cool down CRP PHASE II -IJN - A gradual and progressive warm-up of 10 to 15 mins. incorporating mobility and stretching *Strenuous exertion without previous warm up produces Ischaemic ST segment changes and arrhythmias & reduction of left Ventricular ejection fraction, even In healthy individuals. (BACR, 1995 pg. 84) 14/11/

27 EXERCISE IN CARDIAC REHABILITATION Exercise, the cornerstone of CR esp. Phase II & III. Prescribe with the same precision as any medication. The ex. dose is the combination of intensity, frequency and duration of physical activity. Sufficient to produce a conditioning, but not enough to provoke complication. Aimed at enhancing cardiovascular fitness, strength, endurance and flexibility.



28 PATIENT EDUCATION (CRP I & II) One to one home counseling OR Group Education


29 CR EFFECTIVENESS IS DETERMINED BY A MULTIDISCIPLINARY APPROACH Cardiothoracic Surgeon Cardiologist Psychologist Physiotherapist/Exercise Physiologist Nurses/ Cardiac Nurse Dietician Pharmacist Diabetic Counselor Quit Smoking Counselor Patient and family
30 Provide Smoking-cessation Advice And Support To All Patients Who Smoke Smoking is one of the most significant risk factors for cardiovascular disease, including myocardial infarction (MI). Stopping smoking is associated with a substantial reduction in risk of allcause mortality among patients with coronary heart disease. Quitting smoking reduces the likelihood of a repeat cardiac event and the chances of developing other forms of cardiovascular disease. There is a rapid reduction in the risk of coronary heart disease within one year of quitting smoking. Brief educational interventions of 3 5 minutes have been shown to increase quitting rates compared with no intervention.
31 CATEGORY OF CLIENTS: QUIT SMOKING CLINIC IJN Referral case Referred by IJN Doctors ( in patient/outpatient) referral form doctor required cardiac Rehab Nurse will see patient and conduct counselling Self referred Patient call IJN for appointment slot will be given to client will be seen in clinic for counselling New referral - Outpatient / in patient ( We will see on the same day )

32 WHY IS SMOKING HARMFUL TO THE CARDIOVASCULAR SYSTEM? Increased tendency for vasoconstriction Increases level of bad cholesterol ie. LDL Reduces level of good cholesterol ie. HDL Reduces beneficial effects of medications eg. Statins, Aspirin
33 IMMEDIATE BENEFITS OF QUITTING Duration Of Abstinence Bonus 20 mins Lowers blood pressure & heart rate 8-12 hours Carbon monoxide & nicotine levels lowered by 50% 24 hours Oxygen levels normalize & immediate risks of heart attacks 48 hours Sense of smell & taste improves Nicotine disappears from body 2 weeks Circulation improves & lung function increase by 30% 4 weeks Nicotine withdrawal symptoms disappear
34 CONT.. The Right Way of Quitting Fix a date, be confident and look forward Always be positive and get support Fight your urge to smoke or use nicotine replacement therapy Drink lots of water to flush chemical Exercise > 5 minutes (stretching )or exercise Wash faces & keep hand wet Take shower more frequent Do chew gum with sugar free or vitamin C Avoid caffeine drink change to fruit juice Stop thinking about cigarette, divert to other things Distract yourself from situations which encourages smoking Do pray
 Non nicotine treatment (Non -")
 Nicotine")


35 TREATMENT AVAILABLE (PHARMACOLOGIC APPROACH) Non nicotine treatment (Non - NRT) in IJN 1.Champix tablet (varenicline) Nicotine treatment (NRT) buy from other companies 1.Nicorette tablet 2.Nicotine patch 3.Nicotin gum If patient request for NRT, send prescription slip to retail pharmacy, purchase and call patient.

36 CONT.. Choosing the right pharmacologic agent Patient preference Patient s previous experience with medication, either positive or negative Ease of administration Compliance Health care professional s familiarity with medications
37 CONT (Non NRT TAB CHAMPIX VARENICLINE TARTRATE ) Doses : 0.5 mg DLY x 3 /7 0.5 mg BD x 4/7 1.0 mg BD x 11/52 2. Treatment for 12 weeks Am dose - After light breakfast Or 11/2-2 hours after heavy breakfast Pm dose hrs. - 2 hrs. after dinner (To prevent from nausea or vomiting) NRT can take with others medication
38 COMMUNICATE MANAGEMENT PLAN TO THE PATIENT, CARERS AND THE COMMUNITY HEALTHCARE PROVIDERS Effective communication between the hospital, patients and their families/carers, and community healthcare providers enhances long-term adherence with prescribed therapies and lifestyle changes. Include the patient s GP and, as applicable, community pharmacists, community nurses and other outpatient services.
39 Adherence to Therapy Improves Survival Patients discontinuing their medicines after an MI is common, often soon after discharge. Minimise this by: Educating patients about their medicines. This is likely to improve their understanding and knowledge and thus adherence. Starting patients on secondary preventive therapies and lifestyle changes before they leave hospital. This significantly improves long-term adherence. Involving family members in educational efforts. Smoking cessation, weight loss and increased physical activity are enhanced by enlisting the support of family members. Communicating risk of future cardiovascular events.
40 Long-Term Management A discharge letter/summary should include: A complete list of medicines. Document why guideline medicines have not been prescribed and alternative medicine(s) used. Any changes to medicines being taken at admission. A plan for required dose titration (include who is responsible). Recommendations for monitoring and management of medicine-related adverse effects. Treatment goals including blood pressure, blood lipid levels, weight, HbA1c. Referral for cardiac rehabilitation. Advice given on lifestyle modifications (e.g. smoking cessation as applicable). Recommendations for use of dose-administration aids, carer support and referral for a Home Medicines Review.
41 Thank you
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Myocardial infarction: secondary prevention in primary and secondary care for patients following a myocardial infarction 1.1
2012 Core Measures. Acute Myocardial Infarction (AMI)
") 2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Subject: Outpatient Phase Ii Cardiac Rehab Individualized Treatment Plan And Exercise Prescription
 CARDIAC REHAB POLICY & PROCEDURES Policy #: CR 208 Subject: Outpatient Phase Ii Cardiac Rehab Individualized Treatment Plan And Exercise Prescription Purpose: To establish guidelines for developing and
CARDIAC REHAB POLICY & PROCEDURES Policy #: CR 208 Subject: Outpatient Phase Ii Cardiac Rehab Individualized Treatment Plan And Exercise Prescription Purpose: To establish guidelines for developing and
Cardiac Rehabilitation after Primary Coronary Intervention CONTRA
 DEBATE SESSION Is there a role for cardiac rehabilitation in the modern era of Percutaneous coronary intervention and coronary artery bypass grafting? Cardiac Rehabilitation after Primary Coronary Intervention
DEBATE SESSION Is there a role for cardiac rehabilitation in the modern era of Percutaneous coronary intervention and coronary artery bypass grafting? Cardiac Rehabilitation after Primary Coronary Intervention
This information explains the advice about the care and treatment of people with stable angina that is set out in NICE clinical guideline 126.
 Information for the public Published: 1 July 2011 nice.org.uk About this information NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
Information for the public Published: 1 July 2011 nice.org.uk About this information NICE clinical guidelines advise the NHS on caring for people with specific conditions or diseases and the treatments
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Coronary Artery Disease
 Coronary Artery Disease This information is at http://www.nhlbi.nih.gov/health/dci/diseases/cad/cad_all.html and is provided by the NHLBI, one of the Institutes of the National Institutes of Health. To
Coronary Artery Disease This information is at http://www.nhlbi.nih.gov/health/dci/diseases/cad/cad_all.html and is provided by the NHLBI, one of the Institutes of the National Institutes of Health. To
Cardiac Rehabilitation. Questions and Answers Information for Patients
 Cardiac Rehabilitation Questions and Answers Information for Patients Cardiac Rehabilitation Dept 01625 663083 Leaflet Ref: 10985 Published: 01/17 Review: 12/19 Page 1 Contacts Cardiac Rehabilitation Service
Cardiac Rehabilitation Questions and Answers Information for Patients Cardiac Rehabilitation Dept 01625 663083 Leaflet Ref: 10985 Published: 01/17 Review: 12/19 Page 1 Contacts Cardiac Rehabilitation Service
CORONARY ARTERY DISEASE (CAD) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY DISEASE (CAD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN CONARY ARTERY DISEASE (CAD) MEASURES GROUP: #6. Coronary Artery Disease (CAD): Antiplatelet
CONARY ARTERY DISEASE (CAD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN CONARY ARTERY DISEASE (CAD) MEASURES GROUP: #6. Coronary Artery Disease (CAD): Antiplatelet
Unstable angina and NSTEMI
 Issue date: March 2010 Unstable angina and NSTEMI The early management of unstable angina and non-st-segment-elevation myocardial infarction This guideline updates and replaces recommendations for the
Issue date: March 2010 Unstable angina and NSTEMI The early management of unstable angina and non-st-segment-elevation myocardial infarction This guideline updates and replaces recommendations for the
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Cardiology. Cardiac Rehabilitation
 Cardiology Cardiac Rehabilitation If you are not exercising because of a recent heart attack, cardiac rehabilitation can help to set your mind at ease. In Singapore, heart attack ranks as the second leading
Cardiology Cardiac Rehabilitation If you are not exercising because of a recent heart attack, cardiac rehabilitation can help to set your mind at ease. In Singapore, heart attack ranks as the second leading
The Role of Cardiac Rehabilitation in Recovery & Secondary Prevention. Loren M Stabile, MS Cardiac & Pulmonary Rehab Program Manager
 The Role of Cardiac Rehabilitation in Recovery & Secondary Prevention Loren M Stabile, MS Cardiac & Pulmonary Rehab Program Manager Objectives Core Components of Cardiac Rehab Program CR Indications &
The Role of Cardiac Rehabilitation in Recovery & Secondary Prevention Loren M Stabile, MS Cardiac & Pulmonary Rehab Program Manager Objectives Core Components of Cardiac Rehab Program CR Indications &
Cardiac Rehabilitation Should be Paid in Korea?
 Cardiac Rehabilitation Should be Paid in Korea? Cardiac prevention & Rehabilitation Center, Heart Institute, Asan Medical Center, Seoul, Korea Jong-Young Lee, MD. NO CONFLICT OF INTEREST TO DECLARE Before
Cardiac Rehabilitation Should be Paid in Korea? Cardiac prevention & Rehabilitation Center, Heart Institute, Asan Medical Center, Seoul, Korea Jong-Young Lee, MD. NO CONFLICT OF INTEREST TO DECLARE Before
Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126
 Stable angina: management Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Stable angina: management Clinical guideline Published: 23 July 2011 nice.org.uk/guidance/cg126 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute Coronary Syndrome- The Role of the ACS Clinic in Providing Best Practice Care
 Acute Coronary Syndrome- The Role of the ACS Clinic in Providing Best Practice Care Deborah Pora MSN, ANP-C, RCIS Objectives Review the latest treatment guidelines for adults with acute coronary syndrome
Acute Coronary Syndrome- The Role of the ACS Clinic in Providing Best Practice Care Deborah Pora MSN, ANP-C, RCIS Objectives Review the latest treatment guidelines for adults with acute coronary syndrome
Preventive Cardiology
 Preventive Cardiology 21 Volume The Preventive Cardiology and Rehabilitation Prevention Outpatient Visits 7,876 Program helps patients identify traditional and Phase I Rehab 9,932 emerging nontraditional
Preventive Cardiology 21 Volume The Preventive Cardiology and Rehabilitation Prevention Outpatient Visits 7,876 Program helps patients identify traditional and Phase I Rehab 9,932 emerging nontraditional
Ischaemic Heart Disease
 Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
Ischaemic Heart Disease Katherine Rothwell Case 1 65 yr old female PMHx : Eczema, is a smoker 20/day Comes to see you complaining of central chest pain Present past few months. Comes on when gardening
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION. Dr. Guy Letcher
 The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
The importance of follow-up after a cardiac event: CARDIAC REHABILITATION Dr. Guy Letcher The National Medicare Experience Mortality After Angioplasty 225,915 patients Mortality After Bypass Surgery 357,885
Heart Disease. Signs and Symptoms
 Heart Disease The term "heart disease" refers to several types of heart conditions. The most common type is coronary artery disease, which can cause heart attack, angina, heart failure, and arrhythmias.
Heart Disease The term "heart disease" refers to several types of heart conditions. The most common type is coronary artery disease, which can cause heart attack, angina, heart failure, and arrhythmias.
A multicenter tobacco cessation program in acute coronary syndrome
 A multicenter tobacco cessation program in acute coronary syndrome PD Nicolas Rodondi, MD, MAS Research Fellow: Reto Auer, MD Head of the Cardiovascular Prevention & Lipid Clinic Department of Ambulatory
A multicenter tobacco cessation program in acute coronary syndrome PD Nicolas Rodondi, MD, MAS Research Fellow: Reto Auer, MD Head of the Cardiovascular Prevention & Lipid Clinic Department of Ambulatory
Clinical Practice Guideline
 Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
YOUR GUIDE TO. Understanding Your Angina Diagnosis and Treatment
 YOUR GUIDE TO Understanding Your Angina Diagnosis and Treatment Our goal at the Mercy Health Heart Institute is to help you be well. Our experienced team includes cardiologists, cardiovascular surgeons,
YOUR GUIDE TO Understanding Your Angina Diagnosis and Treatment Our goal at the Mercy Health Heart Institute is to help you be well. Our experienced team includes cardiologists, cardiovascular surgeons,
Smoking Cessation Self-Management Plan and Care Plan
 Smoking Cessation Self-Management Plan and Care Plan I understand the following items will be beneficial to the treatment of my tobacco abuse, have discussed this with my provider and I agree to implement
Smoking Cessation Self-Management Plan and Care Plan I understand the following items will be beneficial to the treatment of my tobacco abuse, have discussed this with my provider and I agree to implement
Repeat ischaemic heart disease audit of primary care patients ( ): Comparisons by age, sex and ethnic group
: Comparisons by age, sex and ethnic group") Repeat ischaemic heart disease audit of primary care patients (2002-2003): Comparisons by age, sex and ethnic group Baseline-repeat ischaemic heart disease audit of primary care patients: a comparison
Repeat ischaemic heart disease audit of primary care patients (2002-2003): Comparisons by age, sex and ethnic group Baseline-repeat ischaemic heart disease audit of primary care patients: a comparison
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
5. Offer pharmacotherapy to all smokers who are attempting to quit, unless contraindicated.
 0 11 Key Messages 1. Ask and document smoking status for all patients. 2. Provide brief advice on quit smoking at every visit to all smokers. 3. Use individual, group and telephone counselling approaches,
0 11 Key Messages 1. Ask and document smoking status for all patients. 2. Provide brief advice on quit smoking at every visit to all smokers. 3. Use individual, group and telephone counselling approaches,
Smokefree Wiltshire. Information leaflet. Planning to quit? Find the right support for you.
 Smokefree Wiltshire Information leaflet Planning to quit? Find the right support for you www.wiltshire.gov.uk/smokefree Support for smokers Smokefree Wiltshire offers tailored stop smoking support for
Smokefree Wiltshire Information leaflet Planning to quit? Find the right support for you www.wiltshire.gov.uk/smokefree Support for smokers Smokefree Wiltshire offers tailored stop smoking support for
Patients First. Acute Coronary Syndrome (ACS): Discharge Guidelines. If you have any questions or concerns, please ask your doctor or nurse.
: Discharge Guidelines. If you have any questions or concerns, please ask your doctor or nurse.") Patient Education CONDITIONS AND DISEASES Acute Coronary Syndrome (ACS): Discharge Guidelines (Heart Attack, Myocardial Infarction, Unstable Angina) If you have any questions or concerns, please ask your
Patient Education CONDITIONS AND DISEASES Acute Coronary Syndrome (ACS): Discharge Guidelines (Heart Attack, Myocardial Infarction, Unstable Angina) If you have any questions or concerns, please ask your
Primary and Secondary Prevention of Cardiovascular Disease. Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group
 Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Primary and Secondary Prevention of Cardiovascular Disease Frank J. Green, M.D., F.A.C.C. St. Vincent Medical Group AHA Diet and Lifestyle Recommendations Balance calorie intake and physical activity to
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
PRESENTED BY BECKY BLAAUW OCT 2011
 PRESENTED BY BECKY BLAAUW OCT 2011 Introduction In 1990 top 5 causes of death and disease around the world: Lower Respiratory Tract Infections Diarrhea Conditions arising during pregnancy Major Depression
PRESENTED BY BECKY BLAAUW OCT 2011 Introduction In 1990 top 5 causes of death and disease around the world: Lower Respiratory Tract Infections Diarrhea Conditions arising during pregnancy Major Depression
Practice-Level Executive Summary Report
 PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
CAMBRIDGESHIRE & PETERBOROUGH STOP SMOKING SERVICE S. Stop Smoking Pharmacological Products Guidance
 CAMBRIDGESHIRE & PETERBOROUGH STOP SMOKING SERVICE S Stop Smoking Pharmacological Products Guidance This guidance is for use by Cambridgeshire Stop Smoking Service (CAMQUIT), Peterborough Stop smoking
CAMBRIDGESHIRE & PETERBOROUGH STOP SMOKING SERVICE S Stop Smoking Pharmacological Products Guidance This guidance is for use by Cambridgeshire Stop Smoking Service (CAMQUIT), Peterborough Stop smoking
1973: No-smoking sections introduced. 1990: No-smoking on all U.S. domestic flights
 Going Smoke Free 1 Going Smoke Free in STAGES 1973: No-smoking sections introduced. 1990: No-smoking on all U.S. domestic flights under 6 hours 2 Going Smoke Free in STAGES All Hospital locations in Michigan
Going Smoke Free 1 Going Smoke Free in STAGES 1973: No-smoking sections introduced. 1990: No-smoking on all U.S. domestic flights under 6 hours 2 Going Smoke Free in STAGES All Hospital locations in Michigan
WHAT IS ATHEROSCLEROSIS?
 ATHEROSCLEROSIS WHAT IS ATHEROSCLEROSIS? Atherosclerosis is a narrowing of the arteries that can significantly reduce the blood supply to vital organs such as the heart, brain and intestines. In atherosclerosis,
ATHEROSCLEROSIS WHAT IS ATHEROSCLEROSIS? Atherosclerosis is a narrowing of the arteries that can significantly reduce the blood supply to vital organs such as the heart, brain and intestines. In atherosclerosis,
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 Assessment and immediate management of suspected acute coronary syndrome bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They
Assessment and immediate management of suspected acute coronary syndrome bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They
Course: Exercise and Aging for Special Populations
 Copyright EFS Inc. All Rights Reserved. Course: Exercise and Aging for Special Populations Session 2: Cardiovascular and Metabolic Disease Considerations for Exercise Program Design Presentation Created
Copyright EFS Inc. All Rights Reserved. Course: Exercise and Aging for Special Populations Session 2: Cardiovascular and Metabolic Disease Considerations for Exercise Program Design Presentation Created
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Your heart attack procedure explained
 Patient information Your heart attack procedure explained i Important information for all patients. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
Patient information Your heart attack procedure explained i Important information for all patients. Golden Jubilee National Hospital Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
2017 MSSP Clinical Quality Measures
 *The information contained in this document relies heavily on information supplied by CMS. GPRO CARE-1 (NQF 0097): Medication Reconciliation Post-Discharge DESCRIPTION: Percentage of discharges from any
*The information contained in this document relies heavily on information supplied by CMS. GPRO CARE-1 (NQF 0097): Medication Reconciliation Post-Discharge DESCRIPTION: Percentage of discharges from any
Quality Payment Program: Cardiology Specialty Measure Set
 Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Reducing risk in heart disease
 Reducing risk in heart disease An expert guide to clinical practice for secondary prevention of coronary heart disease Prof Patricia Davidson (chair) Prof Nigel Stocks Dr Anu Aggarwal Ms Jill Waddell Ms
Reducing risk in heart disease An expert guide to clinical practice for secondary prevention of coronary heart disease Prof Patricia Davidson (chair) Prof Nigel Stocks Dr Anu Aggarwal Ms Jill Waddell Ms
Coronary Artery Disease Clinical Practice Guidelines
 Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
Coronary Artery Disease Clinical Practice Guidelines Guidelines are systematically developed statements to assist patients and providers in choosing appropriate healthcare for specific clinical conditions.
NHS QIS National Measurement of Audit Acute Coronary Syndrome
 NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
NHS QIS National Measurement of Audit Acute Coronary Syndrome Things have changed based on the experience and feedback from the first cycle of measurement and, for the better we think! The Acute Coronary
the high CVD risk smoker
 Smoking Cessation: population and patients A comprehensive approach to the smoker the high CVD risk smoker Catriona Jennings Cardiovascular Specialist Research Nurse Imperial College London European Society
Smoking Cessation: population and patients A comprehensive approach to the smoker the high CVD risk smoker Catriona Jennings Cardiovascular Specialist Research Nurse Imperial College London European Society
Intermittent claudication exercise programme
 Intermittent claudication programme This leaflet explains about an programme that is offered to patients with intermittent claudication. If you have any questions or concerns, please ask a member of staff
Intermittent claudication programme This leaflet explains about an programme that is offered to patients with intermittent claudication. If you have any questions or concerns, please ask a member of staff
A Guide to Help You Reduce and Stop Using Tobacco
 Let s Talk Tobacco A Guide to Help You Reduce and Stop Using Tobacco Congratulations for taking this first step towards a healthier you! 1-866-710-QUIT (7848) albertaquits.ca It can be hard to stop using
Let s Talk Tobacco A Guide to Help You Reduce and Stop Using Tobacco Congratulations for taking this first step towards a healthier you! 1-866-710-QUIT (7848) albertaquits.ca It can be hard to stop using
Management of Stable Ischemic Heart Disease. Vinay Madan MD February 10, 2018
 Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
Management of Stable Ischemic Heart Disease Vinay Madan MD February 10, 2018 1 Disclosure No financial disclosure. 2 Overview of SIHD Diagnosis Outline of talk Functional vs. Anatomic assessment Management
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Derbyshire Formulary for Nicotine Replacement Therapy (NRT) 1. Supporting Smokers to stop smoking The most effective method to quit smoking is by quitting
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Derbyshire Formulary for Nicotine Replacement Therapy (NRT) 1. Supporting Smokers to stop smoking The most effective method to quit smoking is by quitting
Cardiovascular Disease Risk Factors:
 Cardiovascular Disease Risk Factors: Risk factors are traits or habits that increase a person's chances of having cardiovascular disease. Some risk factors can be changed. These risk factors are high blood
Cardiovascular Disease Risk Factors: Risk factors are traits or habits that increase a person's chances of having cardiovascular disease. Some risk factors can be changed. These risk factors are high blood
Associate Professor Gerry Devlin
 Associate Professor Gerry Devlin Clinical Cardiologist and Interventional Cardiologist NZ Heart Foundation Hamilton 9:00-9:15 Secondary Prevention of IHD The Challenge of Secondary Prevention Associate
Associate Professor Gerry Devlin Clinical Cardiologist and Interventional Cardiologist NZ Heart Foundation Hamilton 9:00-9:15 Secondary Prevention of IHD The Challenge of Secondary Prevention Associate
A new model for prescribing varenicline
 Pharmacist Independent Prescribers in partnership with A new model for prescribing varenicline Dear Stop Smoking Advisor You will be aware of the stop smoking drug varenicline that goes under the brand
Pharmacist Independent Prescribers in partnership with A new model for prescribing varenicline Dear Stop Smoking Advisor You will be aware of the stop smoking drug varenicline that goes under the brand
Smoking It s never too late to quit
 Smoking It s never too late to quit Patient Education Improving Health Through Education Making a change for your health Choosing a healthy lifestyle is the best thing you can do to protect your health
Smoking It s never too late to quit Patient Education Improving Health Through Education Making a change for your health Choosing a healthy lifestyle is the best thing you can do to protect your health
Guide to Cardiology Care at Scripps
 Guide to Cardiology Care at Scripps Cardiology is the word in health care associated with heart, but the body s vascular system is also an important part of heart care. Your body has more than 60,000 miles
Guide to Cardiology Care at Scripps Cardiology is the word in health care associated with heart, but the body s vascular system is also an important part of heart care. Your body has more than 60,000 miles
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
Cardiac Rehabilitation Exercise Programs Diabetic Management & Weight Loss Exercise Programs
 Cardiac Rehabilitation Exercise Programs Diabetic Management & Weight Loss Exercise Programs Information for participants Welcome to our cardiac rehabilitation, diabetic & weight loss exercise programs.
Cardiac Rehabilitation Exercise Programs Diabetic Management & Weight Loss Exercise Programs Information for participants Welcome to our cardiac rehabilitation, diabetic & weight loss exercise programs.
TWIN VALLEY BEHAVIORAL HEALTHCARE CLINICAL GUIDELINES FOR MANAGEMENT OF SMOKING CESSATION
 Appendix G PHASE OF MANAGEMENT NOTIFICATION ASSESSMENT TWIN VALLEY BEHAVIORAL HEALTHCARE CLINICAL GUIDELINES FOR MANAGEMENT OF SMOKING CESSATION ACTIONS All patients will be advised on admission that :
Appendix G PHASE OF MANAGEMENT NOTIFICATION ASSESSMENT TWIN VALLEY BEHAVIORAL HEALTHCARE CLINICAL GUIDELINES FOR MANAGEMENT OF SMOKING CESSATION ACTIONS All patients will be advised on admission that :
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
On my way through success!
 MINI-GUIDE TO QUIT SMOKING DISCOVER THE WINNING CONDITIONS On my way through success! QUITTING SMOKING IS ONE OF THE MOST PRECIOUS GIFTS YOU CAN GIVE YOURSELF TO IMPROVE YOUR HEALTH THE BENEFITS BEGIN
MINI-GUIDE TO QUIT SMOKING DISCOVER THE WINNING CONDITIONS On my way through success! QUITTING SMOKING IS ONE OF THE MOST PRECIOUS GIFTS YOU CAN GIVE YOURSELF TO IMPROVE YOUR HEALTH THE BENEFITS BEGIN
SMART STEPS towards a tobacco-free life
 SMART STEPS towards a tobacco-free life Ready to Quit Smoking? You decide when. We ll show you how. Smart steps... Ready to Put Tobacco Behind You? Congratulations on deciding to quit! Quitting tobacco
SMART STEPS towards a tobacco-free life Ready to Quit Smoking? You decide when. We ll show you how. Smart steps... Ready to Put Tobacco Behind You? Congratulations on deciding to quit! Quitting tobacco
Heart Disease (Coronary Artery Disease)
") Heart Disease (Coronary Artery Disease) Understanding how the heart works To understand heart disease, you must first know how the heart works. The heart is like any other muscle, requiring blood to supply
Heart Disease (Coronary Artery Disease) Understanding how the heart works To understand heart disease, you must first know how the heart works. The heart is like any other muscle, requiring blood to supply
CARDIAC REHABILITATION PROGRAMME:- MEDICATION
 CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
Medicines Management Optimisation Achieving your 5 a day post-mi Medication WORKSHOP
 Medicines Management Optimisation Achieving your 5 a day post-mi Medication WORKSHOP What is Medicines Optimisation? the safe and effective use of medicines to enable the best possible outcomes NICE ng
Medicines Management Optimisation Achieving your 5 a day post-mi Medication WORKSHOP What is Medicines Optimisation? the safe and effective use of medicines to enable the best possible outcomes NICE ng
all about your heart...
 For a healthy heart If you smoke, stop smoking. Eat lots of fruit and vegetables and less fat. Be more active every day. Be a healthy weight. Relax take time out for yourself. Local contact: For more information
For a healthy heart If you smoke, stop smoking. Eat lots of fruit and vegetables and less fat. Be more active every day. Be a healthy weight. Relax take time out for yourself. Local contact: For more information
The life after myocardial infarction: a long quiet river?
 The life after myocardial infarction: a long quiet river? Cardiac rehabilitation: for whom and how? Dr. Barnabas GELLEN MD, PhD, FESC Poitiers JESFC 2018 - Paris Conflicts of interest Speaker honoraria
The life after myocardial infarction: a long quiet river? Cardiac rehabilitation: for whom and how? Dr. Barnabas GELLEN MD, PhD, FESC Poitiers JESFC 2018 - Paris Conflicts of interest Speaker honoraria
Smoking Counselling and Cessation Service in Hospital Authority 7 May HA Convention 2014
 Smoking Counselling and Cessation Service in Hospital Authority 7 May 2014 - HA Convention 2014 On behalf of COC (Family Medicine) Dr Maria Leung Consultant, Department of Family Medicine New Territories
Smoking Counselling and Cessation Service in Hospital Authority 7 May 2014 - HA Convention 2014 On behalf of COC (Family Medicine) Dr Maria Leung Consultant, Department of Family Medicine New Territories
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Smoke-free Hospitals. Linda A. Thomas, MS University of Michigan Health System Tobacco Consultation Service
 Smoke-free Hospitals Linda A. Thomas, MS University of Michigan Health System Tobacco Consultation Service Today s Subjects 5A s and Clinician Training and Use with the Hospitalized Patient NRT use in
Smoke-free Hospitals Linda A. Thomas, MS University of Michigan Health System Tobacco Consultation Service Today s Subjects 5A s and Clinician Training and Use with the Hospitalized Patient NRT use in
Smoking and CVD. .what role for the Cardiologist? Dr Sandeep Gupta, MD, FRCP
 Smoking and CVD.what role for the Cardiologist? Dr Sandeep Gupta, MD, FRCP Consultant Cardiologist Whipps Cross/BartsHealth NHS Trusts Hospitals, London, UK Therapeutic Advances in the Treatment of Cardiovascular
Smoking and CVD.what role for the Cardiologist? Dr Sandeep Gupta, MD, FRCP Consultant Cardiologist Whipps Cross/BartsHealth NHS Trusts Hospitals, London, UK Therapeutic Advances in the Treatment of Cardiovascular
Best Practice for Smoking Cessation: Pharmacotherapy. Emma Dean Acting Population Health and Health Promotion Coordinator Lead Pharmacist- Smokefree
 Best Practice for Smoking Cessation: Pharmacotherapy Emma Dean Acting Population Health and Health Promotion Coordinator Lead Pharmacist- Smokefree Why is it so hard to quit? People who smoke aren t weak
Best Practice for Smoking Cessation: Pharmacotherapy Emma Dean Acting Population Health and Health Promotion Coordinator Lead Pharmacist- Smokefree Why is it so hard to quit? People who smoke aren t weak
Value of cardiac rehabilitation Prof. Dr. L Vanhees
 Session: At the interface of hypertension and coronary heart disease haemodynamics, heart and hypertension Value of cardiac rehabilitation Prof. Dr. L Vanhees ESC Stockholm August 2010 Introduction There
Session: At the interface of hypertension and coronary heart disease haemodynamics, heart and hypertension Value of cardiac rehabilitation Prof. Dr. L Vanhees ESC Stockholm August 2010 Introduction There
Care Facilitation Quality Improvement Report
 Disease Management Program Clinical Outcomes for Reporting Period: 2006 Diabetes 100.0% 90.0% % of participants with diabetes 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% % participants with at
Disease Management Program Clinical Outcomes for Reporting Period: 2006 Diabetes 100.0% 90.0% % of participants with diabetes 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% 0.0% % participants with at
Examples of what to say when intervening with smoking clients. Do you smoke cigarettes or tobacco at all, or have you ever smoked regularly?
 Manual of Smoking Cessation Andy McEwen, Peter Hajek, Hayden McRobbie & Robert West 2006 by McEwen, Hajek, McRobbie and West Appendix 5 Examples of what to say when intervening with smoking clients Below
Manual of Smoking Cessation Andy McEwen, Peter Hajek, Hayden McRobbie & Robert West 2006 by McEwen, Hajek, McRobbie and West Appendix 5 Examples of what to say when intervening with smoking clients Below
Patient Navigator Program: Focus MI Diplomat Hospital Metrics
 Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Patient Navigator Program: Focus MI Diplomat Hospital Metrics Goal Statement: To reduce avoidable hospital readmissions for patients discharged with acute myocardial infarction (AMI) by supporting a culture
Returning to fitness after a coronary stent procedure
 Returning to fitness after a coronary stent procedure A patient s guide 1 Returning to fitness after a coronary stent procedure The first few days and weeks following your discharge from Royal Papworth
Returning to fitness after a coronary stent procedure A patient s guide 1 Returning to fitness after a coronary stent procedure The first few days and weeks following your discharge from Royal Papworth
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Physician Orders ADULT: Acute MI/Acute Coronary Syndrome Adult Plan
 Initiate Orders Phase Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Acute MI/Acute Coronary Syndrome Adult Phase, When to Initiate: Acute MI/Acute Coronary Syndrome Adlt Phase Non Categorized
Initiate Orders Phase Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Acute MI/Acute Coronary Syndrome Adult Phase, When to Initiate: Acute MI/Acute Coronary Syndrome Adlt Phase Non Categorized
Long-Term Management Of the ACS Patient: State-of-the-Art. Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA
 Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Advice to patients having an angioplasty
 What is an angioplasty? Advice to patients having an angioplasty An angioplasty is an x ray procedure to open a narrowed or blocked artery in order to improve blood flow. It involves inserting a long tube
What is an angioplasty? Advice to patients having an angioplasty An angioplasty is an x ray procedure to open a narrowed or blocked artery in order to improve blood flow. It involves inserting a long tube
Rexall Ready-2-Quit. Continuous Care with Rexall
 Rexall Ready-2-Quit Continuous Care with Rexall Congratulations on your decision to quit smoking! Stopping smoking may be difficult, but it can be done, and there are many ways to make quitting easier.
Rexall Ready-2-Quit Continuous Care with Rexall Congratulations on your decision to quit smoking! Stopping smoking may be difficult, but it can be done, and there are many ways to make quitting easier.
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
Challenging clinical cases in cardiac rehabilitation: one size fits all? - women -
 Challenging clinical cases in cardiac rehabilitation: one size fits all? - women - Prof. Dr. Birna Bjarnason-Wehrens Institute for Cardiology and Sports medicine German Sportuniversity Colgne Secondary
Challenging clinical cases in cardiac rehabilitation: one size fits all? - women - Prof. Dr. Birna Bjarnason-Wehrens Institute for Cardiology and Sports medicine German Sportuniversity Colgne Secondary
Control Your Risk Factors
 Control Your Risk Factors The causes of CAD are called risk factors. Most risk factors are related to choices you make. Some risk factors you cannot control: family history, gender, and age. My Risk Factors
Control Your Risk Factors The causes of CAD are called risk factors. Most risk factors are related to choices you make. Some risk factors you cannot control: family history, gender, and age. My Risk Factors
4. Which survey program does your facility use to get your program designated by the state?
 STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
STEMI SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and STEMI
Cardiology Pharmacist. Melanie Madorsky, PharmD, BCPS TSHP Annual Meeting April 7, 2018
 Cardiology Pharmacist Melanie Madorsky, PharmD, BCPS TSHP Annual Meeting April 7, 2018 Melanie.Madorsky@memorialhermann.org Objectives Explain the daily responsibilities of the Cardiology Pharmacist Identify
Cardiology Pharmacist Melanie Madorsky, PharmD, BCPS TSHP Annual Meeting April 7, 2018 Melanie.Madorsky@memorialhermann.org Objectives Explain the daily responsibilities of the Cardiology Pharmacist Identify
ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP: #204. Ischemic Vascular Disease (IVD):
ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP: #204. Ischemic Vascular Disease (IVD):
Chapter # 4 Angina. Know what to do if you feel angina
 Chapter # 4 Angina Know what to do if you feel angina You will learn: 1) What angina is 2) How angina affects you 3) How to prevent and manage angina during exercise Chapter 4 Angina pg. 23 What is Angina?
Chapter # 4 Angina Know what to do if you feel angina You will learn: 1) What angina is 2) How angina affects you 3) How to prevent and manage angina during exercise Chapter 4 Angina pg. 23 What is Angina?
Clinical Considerations of High Intensity Interval Training (HIIT)
") Clinical Considerations of High Intensity Interval Training (HIIT) Jenna Taylor Exercise Physiologist & Dietitian The Wesley Hospital PhD Candidate The University of Queensland What is High Intensity Interval
Clinical Considerations of High Intensity Interval Training (HIIT) Jenna Taylor Exercise Physiologist & Dietitian The Wesley Hospital PhD Candidate The University of Queensland What is High Intensity Interval
Dr Joan Leighton. Professor Gerry Devlin. 14:00-14:55 WS #106: Whats Topical in Cardiology 15:05-16:00 WS #116: Whats Topical in Cardiology (Repeated)
") Professor Gerry Devlin Clinical Cardiologist and Interventional Cardiologist NZ Heart Foundation Hamilton Dr Joan Leighton General Practitioner Heart Foundation Christchurch 14:00-14:55 WS #106: Whats
Professor Gerry Devlin Clinical Cardiologist and Interventional Cardiologist NZ Heart Foundation Hamilton Dr Joan Leighton General Practitioner Heart Foundation Christchurch 14:00-14:55 WS #106: Whats
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Using Stop Smoking Medicines
 Using Stop Smoking Medicines This training standard was developed for the National Training Service (NTS) Alliance in consultation with subject matter experts. The purpose of this training standard is
Using Stop Smoking Medicines This training standard was developed for the National Training Service (NTS) Alliance in consultation with subject matter experts. The purpose of this training standard is
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
SECTION 17: NICOTINE REPLACEMENT. Formulary and Prescribing Guidelines
 SECTION 17: NICOTINE REPLACEMENT Formulary and Prescribing Guidelines 17.1 Introduction These guidelines should be used in conjunction with EPUT No Smoking Policy (HRP20) for service users who are 12 years
SECTION 17: NICOTINE REPLACEMENT Formulary and Prescribing Guidelines 17.1 Introduction These guidelines should be used in conjunction with EPUT No Smoking Policy (HRP20) for service users who are 12 years