Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
|
|
|
- Camilla Arnold
- 5 years ago
- Views:
Transcription

1 Submassive PE
2 Pulmonary Embolism Epidemiology: Incidence VTE: /100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk = 20% Mortality: High-risk: ~20% Intermediate risk: ~2-5% Low-risk ~1% Morbidity: Intermediate risk ~30% Risk Factors: Acute: surgery, trauma, pregnancy, burns, CVC, paralysis & immobility Chronic: age, smoking, obesity, OCP, hormone replacement, malignancy, CCF, Lupus-anticoagulant Genetic: deficiency of Protein C&S or AT3, FV Leiden mutation, hyperhomocysteinaemia
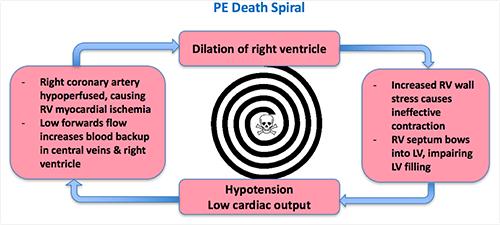
3 Pathophysiology
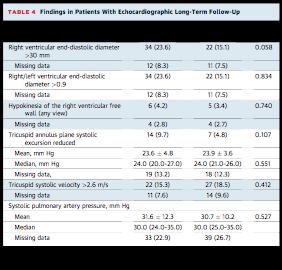
4 Classification 1.Massive PE: acute PE + obstructive shock (SBP<90) 2.Submassive PE: acute PE + RV dysfunction OR myocardial necrosis ECG: RV stain new RBBB, anteroseptal TwI, anterior STE or depression BNP >90 CT: RV diameter/lv diameter >0.9 TTE: RV diameter/lv diameter >0.9 or RVED diameter>30mm OR RV systolic dysfunction OR tricuspid systolic velocity >2.6 m/s 3.Non-massive PE: haemodynamically stable without objective evidence of RV dysfunction
5 Systemic Thrombolysis Biological Rationale: clot burden LV filling + RV dysfunction chronic pulmonary HTN Advantages: mortality + morbidity Adverse effects: ICH major bleeding risk of recurrent PE

 Pharmacokinetics: >50% cleared by the liver within 5 minutes of infusion")
6 Systemic Thrombolysis Pharmacodynamics: fibrinolytic agents accelerate clot lysis by converting clot bound plasmin to plasminogen which degrades the fibrin structure of the clot. rtpa Dose (2014 ESC guidelines): 0.9mg/kg (up to 100mg) -> 10% IV bolus + 90% infusion over 2hrs OR 0.6mg/kg over 15mins (max 50mg) Pharmacokinetics: >50% cleared by the liver within 5 minutes of infusion cessation, ~80% in 10mins
7 Systemic thrombolysis Indications: 1. Cardiac arrest + proven or suspected PE 2. High risk PE 3. Intermediate risk PE: less well established -> Consider monitoring and Rx if deteriorating with half dose. Can be performed as late as 14 days. Contraindications Absolute: Risk of ICH: Any prior ICH, structural cerebrovascular disease or malignant intracranial neoplasm, ischaemic CVA<3/12, recent spinal or intracranial surgery, recent TBI with radiographic evidence of brain injury or bony # Risk of uncontrollable bleeding: Aortic dissection, active bleeding Relative: HPC: Pregnancy, uncontrolled HTN, Traumatic or prolonged CPR PMHx: >75yrs, dementia or remote ischaemic CVA, Hx severe poorly controlled HTN, major surgery within 3 weeks or recent internal bleeding <1/12 Meds: current use of anticoagulation
![Fibrinolysis should be considered in all adult patients with cardiac arrest with proven or suspected PE [weak recommendation, very low quality of evidence] If a](/docs-images/95/124143220/images/8-0.jpg "fibrinolytic drug is given in these circumstances, consider performing CPR for at least 60-90min before termination of resuscitation attempts [Class A; Expert consensus")
8 Fibrinolysis should be considered in all adult patients with cardiac arrest with proven or suspected PE [weak recommendation, very low quality of evidence] If a fibrinolytic drug is given in these circumstances, consider performing CPR for at least 60-90min before termination of resuscitation attempts [Class A; Expert consensus opinion].
9 Wan et al (2004, Circulation): Systematic review (11 studies, n=748) comparing thrombolysis Vs anticoagulation alone High risk haemodynamically unstable PE: recurrent PE or death = 19% -> 9.4% (OR=0.45) 55%, NNT=10 Unselected PE: mortality = 9.6% -> 6.7% (OR = 0.67) major bleeding = 6.1% -> 9.1% (OR=1.42) non-major bleeding = 10% -> 22% (OR=2.63) Unselected PE - high risk PE: mortality = 5.3% -> 4.8% (OR=1.07)
: MRCT (n=83) in submassive PE: LMWH + full-dose TPA or placebo Adverse outcome @ 90 days (death, shock")
10 TOPCOAT trial (2014, J. Thromb Haem): MRCT (n=83) in submassive PE: LMWH + full-dose TPA or placebo Adverse 90 days (death, shock intubation, major bleeding, recurrent PE, poor functional capacity): 37% -> 15% with trial terminated early
 or placebo Death or haemodynamic compensation: 5.6% -> 2.6% (p=0.")
 Bleeding ICH: 0.2% -> 2.0% (p=0.003) Major Extracranial bleeding: 1.2% -> 6.3% (p<0.001) ISTH Major bleeding : 2.")
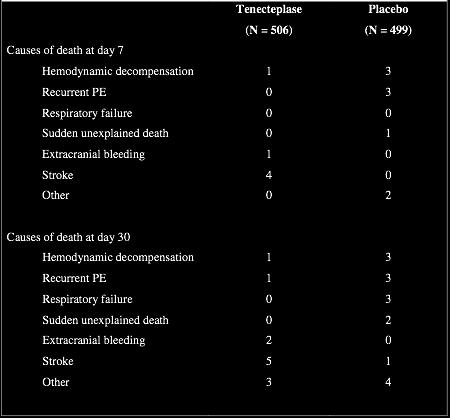
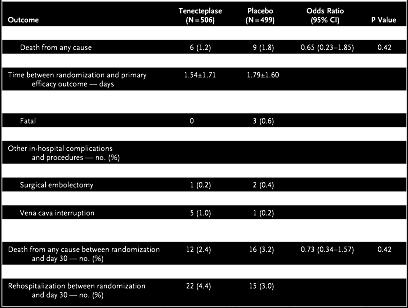
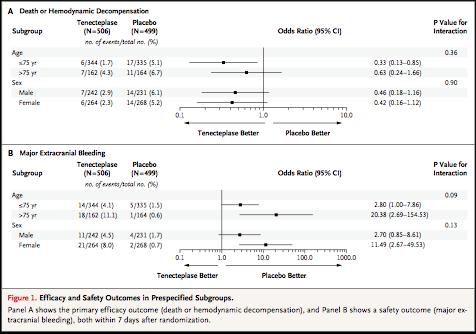
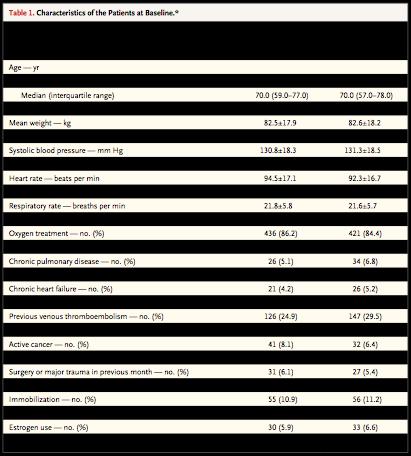
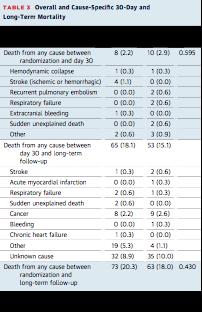
11 PEITHO trial (2014) multi-centre RCT (n=1006) in intermediate risk PE (RV strain + TnI/T): anticoagulation + full-dose Tenectaplase (30mg - 50mg) or placebo Death or haemodynamic compensation: 5.6% -> 2.6% (p=0.02) 7 day haemodynamic decompensation: 5% -> 1.6% (p=0.002) 7 day mortality: 1.8 -> 1.2% (p=0.42) 30 day mortality: 3.2% -> 2.4% (p=0.42) Bleeding ICH: 0.2% -> 2.0% (p=0.003) Major Extracranial bleeding: 1.2% -> 6.3% (p<0.001) ISTH Major bleeding : 2.4% -> 11.5% Minor bleeding: 8.6% -> 32%
12
13
14


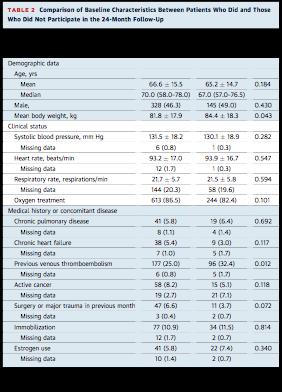
15 Follow-up at 28 of original PEITHO study sites (n=709) after 24 months (median reassessment = 37.8 months) Long-term Mortality & cause of death: ~98% Clinical assessment after 24 months: ~50% Echocardiographic assessment after 24 months: ~41%
16 PEITHO patients Inclusion Criteria: >18yrs Objectively confirmed PE with onset of symptoms <16 days + RV dysfunction confirmed by TTE or CT Myocardial injury confirmed by TnI/T Exclusion Criteria Haemodynamic decompensation at presentation Known significant bleeding risk (but not anti-plts) Uncontrolled HTN (BP>180/110) Pregnancy, lactation or parturition within 30 days Previous thrombolysis, vena cava filter or pulmonary thrombectomy within 4 days Known hypersensitivity to any of the agents used
17

18 Treatment Protocol 1. Anticoagulation: Immediate unfractionated heparin bolus + infusion targeting APTT x2-2.5 baseline OR other anticoagulation according to local practice no other anticoagulants <48hr 2. Thrombolysis Vs Placebo: administered over 5-10 seconds
19
20 Morbidity Assessment Persistent dyspnoea or functional limitation: Thrombolysis = 36% Vs Placebo = 30.1% (p=0.23) Morbidity Mild exertional dyspnoea: 87% & 90% NYHA class 3 or 4: 12 & 10.9% Peripheral oedema: 5.1% & 2.2% Other signs or symptoms of pulmonary HTN: <2% pre-syncope, syncope tactile RV impulse, JVP, accentuated or splitting 2nd HS, S3 or S4, hepatomegally or ascites
21

22
23 Critique Strengths: large double blinded multi-centre RCT first large study of long-term morbidity and mortality outcome in such a trial Weaknesses: Dosing of thrombolytics: 2% ICH is a high rate and full dose rtpa + full dose anticoagulation may be seen to be too aggressive in this group 30 day mortality from respiratory failure & recurrent PE Vs acute bleeding - PEITHO demonstrated 30 day mortality with placebo Robustness of long-term morbidity comparison: baseline assessment was not for pulmonary HTN and therefore treatment groups may have been significantly different. Robustness of long-term morbidity assessment: only 50% of the 703 patients selected were clinically assessed. Does this represent a selection bias by the patients themselves?
24 Assessment: High Risk Submassive PE Identifying patients at high risk of PEA arrest Unstable symptoms Severe dyspnoea or hypoxia Lack of cardiovascular reserve: syncope or presyncope Progressive sympathetic compensation: shock index (HR/SBP) >1, lactate >4 Looks terrible: pale, diaphoretic, impending doom Identifying patients at high mortality risk for respiratory failure & recurrent PE PMHx of conditions pre-disposing to pulmonary HTN: OSA, obesity, COPD, lung diseases Significant residual clot burden +/- proximal DVT Identifying patients at high risk for massive bleeding Management Alternatives to systemic thrombolysis IVC filter Catheter directed thrombolysis Pulmonary thrombectomy Pre-emptive Vs Rescue systemic thrombolysis Systematic review of studies demonstrates a non-significant 1.4% mortality benefit with pre-emptive thrombolysis (Nakamura, 2014)? safe -dose thrombolysis +/- fibrinogen levels to guide Rx? avoiding or delaying concommittent anticoagulation
25 MOPPETT trial (2013, Am. J. Cardiol.): single centre RCT (n=121) in moderate PE (clinical signs + radiologically defined clot burden) anticoagulation + 0.5mg/kg alteplase or placebo Results: Mortality + recurrent PE: 10% -> 1.6% (but neither end point significant independently) Acute pulmonary HTN: 57% -> 16% Hospital LOS: 4.9 days -> 2.2 days Chronic pulmonary HTN + recurrent 18 months: 63% -> 16% Major Bleeding: No major bleeding in either group
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: Physicians managing adult patients with massive and submassive pulmonary emboli in the
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS.
 DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
DRAFT-2018 UPDATES RECOMMENDATIONS FOR THE MANAGEMENT OF MASSIVE AND SUBMASSIVE PULMONARY EMBOLISM IN ADULT PATIENTS. Target Audience: MultiCare physicians managing adult patients with massive and submassive
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis
 Receiving Catheter- Directed Thrombolysis") Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Single-Center, Retrospective, Observational Analysis of Patients with Submassive Pulmonary Embolism (PE) Receiving Catheter- Directed Thrombolysis John A. Phillips, M.D. OhioHealth Heart and Vascular Physicians
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
National Institute for Health and Care Excellence IP1243 Ultrasound enhanced catheter-directed thrombolysis for pulmonary embolism Consultation Comments table IPAC date: Thursday 12 March 2015 1 1 Manufacturer
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Catheter Directed Interventions for Pulmonary Embolism
 Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Catheter Directed Interventions for Pulmonary Embolism Rabih A. Chaer, MD, MSc Professor of Surgery, UPMC Residency Program Director Site chief, Presbyterian campus Division of Vascular Surgery Pittsburgh,
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Guideline for Thrombolysis Therapy in Pulmonary Embolism
 Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Guideline for Thrombolysis Therapy in Pulmonary Embolism Dr Jane Strong Consultant Haematologist Trust ref: B24/2016 1. Introduction / Scope All Patients with pulmonary embolism (PE) require rapid risk
Management of sub-massive and massive pulmonary embolism:
 Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Management of sub-massive and massive pulmonary embolism: Evidence and Controversy Boonsong Patjanasoontorn, MD, FCCP, FCCM Immediate Past President, Thai Society of Critical Care Medicine(TSCCM) Chief,
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Management of Pulmonary Embolism
 Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Acute Management of Pulmonary Embolism Dr Alex West Respiratory Consultant Guy s and St Thomas Hospital London Declarations - none Order of Play Up date in Diagnostic Imaging - CTPA and V:Q SPECT Sub-massive
Surgical Thrombectomy for PE: Is it Making a Comeback
 Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
Surgical Thrombectomy for PE: Is it Making a Comeback Prashanth Vallabhajosyula, MD MS The University of Pennsylvania Health System Philadelphia, PA Case - 84 year old female presents with submassive right
9/24/2013. Thrombolytics in 2013: Never Say Never. September 19 th, 2013 Scott M Lilly, MD PhD. Clinical Case
 September 19 th, 2013 Scott M Lilly, MD PhD Thrombolytics in 2013: Never Say Never Clinical Case 2 1 Evolution of STEMI Therapy The importance of absolute rest in bed for several days is clear James B
September 19 th, 2013 Scott M Lilly, MD PhD Thrombolytics in 2013: Never Say Never Clinical Case 2 1 Evolution of STEMI Therapy The importance of absolute rest in bed for several days is clear James B
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
TXA. Things Change. Tranexamic Acid TXA. Resuscitation 2017 TXA In The ED March 31, MAST Trousers. High Flow IV Fluids.
 Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
Resuscitation 2017 In The ED March 31, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN SECURE THE ABC S MAST
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
Catheter-directed Thrombolysis for Pulmonary Embolism
 Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Catheter-directed Thrombolysis for Pulmonary Embolism Is It Good Advice to Lyse? Texas Society of Health-System Pharmacists April 7, 2018 Rebecca L. Attridge, PharmD, MSc, BCPS Associate Professor, University
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Effectiveness and cost-effectiveness of thrombolysis in submassive pulmonary embolism Perlroth D J, Sanders G D, Gould M K
 Effectiveness and cost-effectiveness of thrombolysis in submassive pulmonary embolism Perlroth D J, Sanders G D, Gould M K Record Status This is a critical abstract of an economic evaluation that meets
Effectiveness and cost-effectiveness of thrombolysis in submassive pulmonary embolism Perlroth D J, Sanders G D, Gould M K Record Status This is a critical abstract of an economic evaluation that meets
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolectomy:
 Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
Pulmonary Embolectomy: Recommendation for early surgical intervention Tomas A. Salerno, M.D. Professor of Surgery, University of Miami Miller School of Medicine and Jackson Memorial Hospital Epidemiology
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Epidemiology of Pulmonary Embolism (PE)
") Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Why Treat Submassive PE Abstract: Massive Pulmonary Embolism (PE) requires immediate lifesaving intervention for the patient. For the submassive PE patient, characterized by presence of right ventricular
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC
 David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC") Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Intraoperative Pulmonary Embolus
 PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
PBLD Table #5 Intraoperative Pulmonary Embolus Holly Richter, M.D. and Sean Benton, D.O. Objectives 1. Determine patients who are at risk for perioperative pulmonary embolism 2. Form a differential diagnosis
ST Elevation Myocardial Infarction (STEMI) Reperfusion Order Set
 Reperfusion Order Set") Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Form Title Form Number CH-0454 2018, Alberta Health Services, CKCM This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. The license does not
Interventional Management of Acute Pulmonary Embolism
 Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Interventional Management of Acute Pulmonary Embolism Prof. Nils Kucher Angiology & Cardiology University Hospital Bern Inselspital nils.kucher@insel.ch DECLARATION OF CONFLICT OF INTEREST Consultant to
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Interventional Treatment VTE: Radiologic Approach
 Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Interventional Treatment VTE: Radiologic Approach Hae Giu Lee, MD Professor, Dept of Radiology Seoul St. Mary s Hospital The Catholic University of Korea Introduction Incidence High incidence: 250,000-1,000,000/year
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment
 Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Severe pulmonary embolism: Catheter-based thrombolysis and medical treatment Rolf P. Engelberger, MD Division of Angiology Cantonal Hospital Fribourg & University Hospital Bern, Switzerland Overview Reperfusion
Scenario Development Template
 Scenario Development Template Scenario Title: Inf STEMI, ICH, PEA Arrest Author: E. Merrick Last edit: April 12, 2018 Set up: Confederates: Duration: Scenario 20 min Debriefing 30 min Learning Objectives:
Scenario Development Template Scenario Title: Inf STEMI, ICH, PEA Arrest Author: E. Merrick Last edit: April 12, 2018 Set up: Confederates: Duration: Scenario 20 min Debriefing 30 min Learning Objectives:
Sinus Venous Thrombosis
 Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
Sinus Venous Thrombosis Joseph J Gemmete, MD FACR, FSIR, FAHA Professor Departments of Radiology and Neurosurgery University of Michigan Hospitals Ann Arbor, MI Outline Introduction Medical Treatment Options
National Institute for Health and Care Excellence
 National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
National Institute for Health and Care Excellence IP1219 Ultrasound enhanced catheter-directed thrombolysis for deep vein thrombosis Consultation table IPAC date: Thursday 12 March 2015 Com. 1 3 NHS Professional
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients
 The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
The OPTALYSE PE Trial Reducing thrombolytic dose and treatment times with EKOS in the treatment of pulmonary embolism patients Keith M. Sterling, M.D. Director, Cardiovascular & Interventional Radiology
Catheter Interventions for pulmonary embolism:
 Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Catheter Interventions for pulmonary embolism: From Directed tpa Drips to Suction Thrombectomy Efthymios Avgerinos, MD Associate Professor of Surgery Division of Vascular Surgery University of Pittsburgh
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
VTE & Medical Patients: Case Scenario
 The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
The Saudi Association for Venous Thromboembolism SAVTE The 2 nd SAVTE Symposium 1-3 May, 2012 Casablanca, Morocco VTE & Medical Patients: Case Scenario Majdy Idrees Riyadh, Saudi Arabia Majdy M Idrees,
Pulmonary and Critical Care Year in Review
 Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Pulmonary and Critical Care Year in Review Heath E Latham, MD Assistant Professor University of Kansas Dept of Internal Medicine Division of Pulmonary and Critical Care None Disclosure Lung Cancer Screening
Is Oral Rivaroxaban Safe and Effective in the Treatment of Patients with Symptomatic DVT?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Recent advances in the management of pulmonary embolism. Kodati Rakesh SR Pulmonary medicine
 Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Recent advances in the management of pulmonary embolism Kodati Rakesh SR Pulmonary medicine Clinical decision rules & D dimer Outpatient anticoagulation Thrombolysis Anticoagulation Catheter directed therapies
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Critical Review Form Therapy
 Critical Review Form Therapy Alteplase versus heparin in acute pulmonary embolism: randomised trial assessing right-ventricular function and pulmonary perfusion Lancet 1993; 341:501-511 Objective: To determine
Critical Review Form Therapy Alteplase versus heparin in acute pulmonary embolism: randomised trial assessing right-ventricular function and pulmonary perfusion Lancet 1993; 341:501-511 Objective: To determine
COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP)
") The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
Massive Pulmonary Embolism
 Massive Pulmonary Embolism Objectives 1. Review the pathophysiology of a pulmonary embolism. 2. Describe the signs and symptoms of a patient experiencing a pulmonary embolism. 3. Identify treatment modalities
Massive Pulmonary Embolism Objectives 1. Review the pathophysiology of a pulmonary embolism. 2. Describe the signs and symptoms of a patient experiencing a pulmonary embolism. 3. Identify treatment modalities
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go?
 Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski. Department of Surgery Grand Rounds March 24, 2008
 Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
Inferior Venacaval Filters Valuable vs. Dangerous Valuable Annie Kulungowski Department of Surgery Grand Rounds March 24, 2008 History of Vena Cava Filters Virchow-1846-Proposes PE originate from veins
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
STEMI and Cardiogenic Shock. The rules and solution. Dave Kettles St Dominics and Frere Hospitals East London ZA
 STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
STEMI and Cardiogenic Shock. The rules and solution Dave Kettles St Dominics and Frere Hospitals East London ZA Definitions: Shock is a life threatening, but initially reversible state of cellular and
How and Why to Form a PERT, Pulmonary Embolism Response Team
 Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
Disclosures How and Why to Form a PERT, Pulmonary Embolism Response Team Rachel P. Rosovsky, MD, MPH No disclosures Rachel P. Rosovsky, MD, MPH April 21, 2017 AC Forum 2017 2 Agenda Pulmonary Embolism
PULMONARY EMBOLISM AND PERT. Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology
 PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
PULMONARY EMBOLISM AND PERT Jonathon Kirkland, DO OSU Department Chair, Radiology Head of Interventional Radiology No financial disclosures 1. What are the clinical signs/symptoms of submassive PE? 2.
ST Elevated Myocardial Infarction- Latest AHA recommendations
 ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
L embolia polmonare ad alto rischio, dalla diagnosi alla terapia riperfusiva.
 L embolia polmonare ad alto rischio, dalla diagnosi alla terapia riperfusiva. Centro di riferimento regione toscana per la diagnosi e la terapia della tromboembolia polmonare Dip Emergenza Urgenza- Careggi
L embolia polmonare ad alto rischio, dalla diagnosi alla terapia riperfusiva. Centro di riferimento regione toscana per la diagnosi e la terapia della tromboembolia polmonare Dip Emergenza Urgenza- Careggi
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
8/16/2012. Pulmonary Embolism
 Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
The spectrum of clinical outcome of PE
 Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
Practical treatment approach for patients with PE Cecilia Becattini University of Perugia The spectrum of clinical presentation of PE PE-related shock Mild clinical symptoms The spectrum of clinical outcome
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACTIVASE (t-pa) INFUSION PROTOCOL FOR ACUTE MYOCARDIAL INFARCTION
 INFUSION PROTOCOL FOR ACUTE MYOCARDIAL INFARCTION") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACTIVASE (t-pa) FOR ACUTE MYOCARDIAL INFARCTION I. PURPOSE: A. To reduce the extent of myocardial infarction by lysing the clot in
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACTIVASE (t-pa) FOR ACUTE MYOCARDIAL INFARCTION I. PURPOSE: A. To reduce the extent of myocardial infarction by lysing the clot in
Year in Review 2014: Critical Care Medicine
 Disclosures Year in Review 2014: Critical Care Medicine I receive laboratory support from CytoVale Diagnostics for research on early sepsis diagnostics Eric J. Seeley, M.D., F.C.C.P. Assistant Professor
Disclosures Year in Review 2014: Critical Care Medicine I receive laboratory support from CytoVale Diagnostics for research on early sepsis diagnostics Eric J. Seeley, M.D., F.C.C.P. Assistant Professor
Pulmonary embolism. Paweł Balsam MD, PhD
 Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
When the learner has completed this module, she/he will be able to:
 Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Thrombolytics and Myocardial Infarction WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Pulmonary embolism: Acute management. Cecilia Becattini University of Perugia, Italy
 Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
Pulmonary embolism: Acute management Cecilia Becattini University of Perugia, Italy Acute pulmonary embolism: Acute management Diagnosis Risk stratification Treatment Non-high risk PE: diagnosis 3-mo VTE
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center
 Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Ryan Walsh, MD Department of Emergency Medicine Madigan Army Medical Center The opinions expressed herein are solely those of the author and do not represent the official views of the Department of Defense
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU