Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
|
|
|
- Eleanore Murphy
- 5 years ago
- Views:
Transcription

1 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
2 Disclosures No relevant financial relationships to disclose
3 Objectives and Outline Define heart failure and its public health significance Describe different classifications of HF Review the diagnostic evaluation of HF patients Discuss principles of guideline-directed management of chronic HF Recognize special considerations for treatment of patients hospitalized with HF
4 Definition of HF Heart failure is a complex disease that is the result of cardiac injury that impairs the heart s ability to eject or fill with blood This manifests with typical symptoms: Fatigue and shortness of breath that limit the patient s ability to exercise Fluid retention that can cause elevated jugular venous pressure, pulmonary or peripheral edema Symptoms can vary if HF is acute or chronic HF patients can have preserved or reduced ejection fraction (EF) Yancy C et al. J Am Coll Cardiol 2013;62:
5 Epidemiology of HF Over 5 million Americans suffer from HF at present 650,000 new cases annually Over 1 million hospital visits every year 20% of Americans older than 40 years will develop HF HF incidence is about 20 per 1000 people years old HF incidence rises with age and is greater than 80 per 1000 people 85 years old or older Djousse L et al. JAMA 2009;302: Go AS et al. Circulation 2013;127:e6-245 Curtis LH et al. Arch Intern Med 2008;168:
 Hypertension 66.2 72.7 58.6 15.1 (7.3-23.7) Diabetes 18.5 16.8 20.5 9.8 (5-18.6) Obesity 24.5 23.2 26.1 16.1 (10.1-20.4) Ever smoker 51.2 33.7 71.")
6 Risk Factors for the Development of HF Risk Factor Prevalence among cases (%) Overall (n=962) Women (n=517) Men (n=445) Time From RF to HF Onset in years, median (25 th -75 th percentile) Coronary artery disease ( ) Hypertension ( ) Diabetes (5-18.6) Obesity ( ) Ever smoker Dunlay SM C et al. Am J Med 2009;122:
7 Pathophysiology of HF MI HTN Arrhythmias Valve disease Diabetes Toxins Sympathetic NS Renin-Angiotensin- Aldosterone System Natriuretic Peptide System Mann DL et al. Circulation 2005;111:

8 Natural History of HF ONSET SUDDEN DEATH DECOMPENSATIONS PUMP FAIL Allen LA et al. Circulation 2012;125:
 1.")
9 Hospital Discharges for HF by Gender (US ) 1.1M 720k CMS
10 Roger VL et al. JAMA 2004;292: HF 5-year Mortality 5-year mortality: 50% 5-year mortality: 46%
11 Classification of HF Based on EF Heart failure with reduced ejection fraction (HFrEF) Heart failure with preserved ejection fraction (HFpEF) HFpEF-borderline HFpEF-improved Based on symptom severity upon assessment NYHA class I-IV Based on disease progression ACCF/AHA Stages A-D Yancy C et al. J Am Coll Cardiol 2013;62:
12 Classification of HF by EF Classification EF (%) Description 1. HF with reduced EF (HFrEF) 40 Systolic HF. Most available clinical trials include patients with HFrEF 2. HF with preserved EF (HFpEF) 50 Diastolic HF. No known effective therapies a. HFpEF-borderline New intermediate group. Appear to be more similar to HFpEF b. HFpEF-improved >40 Patients with reduced EF who have improvement who may have different characteristics to HFrEF and HFpEF Yancy C et al. J Am Coll Cardiol 2013;62:
13 Classification of HF by Symptom Severity NYHA Class Description Class I No limitation of physical activity. Ordinary activity does not cause HF symptoms Class II Slight limitation of physical activity. Comfortable at rest, but ordinary activity results in HF symptoms Class III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes HF symptoms Class IV Unable to carry out any physical activity without HF symptoms or symptoms of HF at rest The Criteria Committee of the NY Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9 th Ed. Boston: Little & Brown; 1994

14 Classification of HF by Disease Stage ACCF/AHA Stage Description Stage A At high risk for HF but without structural heart disease or HF symptoms Stage B Structural heart disease is present but never had HF symptoms Stage C Structural heart disease present with HF symptoms now or in the past Stage D Refractory HF symptoms requiring advanced therapies Hunt SA et al. J Am Coll Cardiol 2009;53:e1-90
15 Chronic HF Management by Disease Stage Hunt SA et al. J Am Coll Cardiol 2005;112:e
16 Evaluation of HF Patients HF is a purely clinical diagnosis Thorough history and physical examination should be obtained in all patients Assess severity of activity limitations (NYHA class) Presence of orthopnea HR, BP and changes in weight Assess jugular venous pressure and extent of edema Laboratory testing CBC Serum electrolytes and glucose BUN/creatinine Fasting lipids Liver function tests Thyroid function tests Yancy C et al. J Am Coll Cardiol 2013;62:
17 Evaluation of HF Patients 12-lead electrocardiogram Chest X-ray 2D echocardiogram with Doppler Follow up echocardiogram if: Significant changes in clinical status Suspected recovery after a clinical event Suspected recovery due to medical therapy To assess eligibility for device therapy Routine follow up echocardiograms are not recommended Cardiac MR is an alternative to echocardiography When CAD is suspected, non-invasive stress testing or coronary angiography is reasonable unless the patient is not a candidate for revascularization Yancy C et al. J Am Coll Cardiol 2013;62:
18 Biomarkers in HF BNP or NT-proBNP can be helpful when the cause of dyspnea is uncertain BNP or NT-proBNP should be checked to assess prognosis/disease severity Entresto can increase BNP, but not NT-proBNP Elevated Troponin T or I indicate poor prognosis in patients hospitalized with HF, even in the absence of acute coronary syndrome Soluble ST-2, galectin-3 and high-sensitivity troponin are markers of cardiac injury/fibrosis and are associated with risk of hospitalization and death Tang WH et al. Circulation 2003;108: Anand IS et al. Circulation 2003;107: Manzano-Fernandez S et al. Am J Cardiol 2011;107: Shah RV et al. Eur J Heart Fail 2010;12:

19 Biomarkers in Prevention, Diagnosis and Risk-Stratification of HF Yancy C et al. J Am Coll Cardiol 2017;70:
20 Principles of Chronic HF Management The treatment of HFrEF includes pharmacologic and nonpharmacologic components Pharmacologic treatment involves several medication classes which have combined effects that reduce HF mortality and morbidity The foundation of medical therapy are ACEi/ARBs and evidencebased beta-blockers Achieving guideline-directed doses of these medications is the primary goal of dose adjustment Non-pharmacologic treatments are just as important and include lifestyle modification/self-care behaviors and device-based therapies The treatment requirements change as disease progresses from Stage A to Stage D

21 Management of Chronic HF Evolves by Stage Jessup M et al. N Engl J Med 2003;348:

22 Classification of Recommendations and Levels of Evidence Yancy C et al. J Am Coll Cardiol 2017;70:
23 Pathophysiology of HF MI HTN Arrhythmias Valve disease Diabetes Toxins Neurohormones Sympathetic NS Renin-Angiotensin- Aldosterone System Natriuretic Peptide System Mann DL et al. Circulation 2005;111:
24 Management of Stage A Chronic HF Aggressive management of HF risk factors Hypertension and abnormal lipids should be treated according to current guidelines Diabetes, obesity and smoking should be treated as well Avoid cardiotoxic exposures as possible: alcohol, certain cancer therapies, radiation therapy to the chest Yancy C et al. J Am Coll Cardiol 2013;62:
25 Management of Stage B Chronic HF Patients with a history of MI, recent or remote, and a low EF, should be treated with ACEi/ARB or evidence-based beta-blockers to decrease the likelihood of HF onset Post-MI patients should be treated with statins to prevent HF In patients with LVH, hypertension should be treated according to current guidelines ACEi/ARB and evidence-based beta-blockers should be used in all patients with low EF to prevent HF An ICD is reasonable in post-mi patients without HF symptoms if they are at least 40 days post-mi, have an EF 30%, and are on guideline-directed medical therapy Yancy C et al. J Am Coll Cardiol 2013;62:
26 Management of Stage B Chronic HF Diltiazem, verapamil Yancy C et al. J Am Coll Cardiol 2013;62:
27 Management of Stage C Chronic HF Non-Pharmacologic Interventions Education on HF self-care behaviors Dietary sodium and fluid restriction Reduce congestive symptoms Compliance with medications and follow-up Reduce hospitalization risk Daily weight Early calls to healthcare providers with volume retention Exercise training and cardiac rehabilitation Improves functional capacity, quality of life and reduces mortality Yancy C et al. J Am Coll Cardiol 2017;70:
 N Engl J Med 1987;316:1429-1435 (2) N Engl J Med 2001;344:1651-1658 (3) N Engl J Med 1999;341:709-717 (4) N Engl J Med 2005;352:225-237 (5) N Engl J Med")
28 Mortality reduction (%) Management of Stage C Chronic HF Pharmacologic Interventions Enalapril(1) Carvedilol(2) Spironolactone(3) HZN/ISDN(4) Entresto (5) (1) N Engl J Med 1987;316: (2) N Engl J Med 2001;344: (3) N Engl J Med 1999;341: (4) N Engl J Med 2005;352: (5) N Engl J Med 2014;371:
29 Management of Stage C Chronic HF Yancy C et al. J Am Coll Cardiol 2013;62:
30 Entresto (Sacubitril-Valsartan) New drug class (ARNI) ARB (Valsartan) combined with neprilysin inhibitor (Sacubitril) Neprilysin breaks down BNP, bradykinin and other vasoactive peptides Use of Entresto resulted in further 20% reduction in HF mortality and HF hospitalization compared to enalapril Patients who can tolerate and ACEi or ARB should be transitioned to Entresto Discontinue ACEi/ARB for AT LEAST 36 HOURS before starting Entresto to decrease risk of angioedema Dosed 24/26 mg (50 mg), 49/51 mg (100 mg) and 97/103 mg (200 mg) tabs McMurray JJV et al. N Engl J Med 2014;371: Yancy C et al. J Am Coll Cardiol 2017;70:
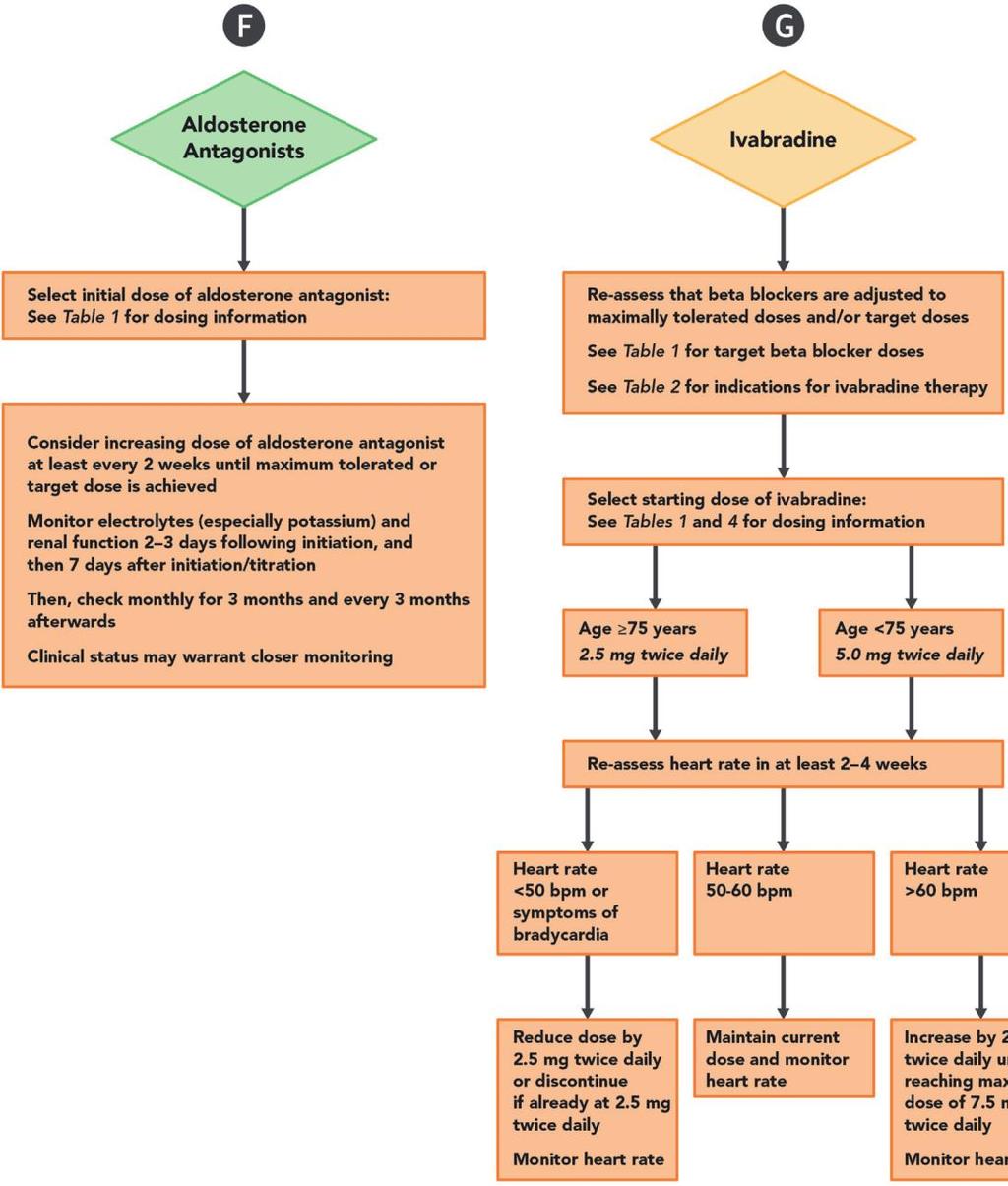
31 Other Beneficial Drugs Digoxin Can be used in HFrEF to reduce HF hospitalizations Ivabradine Can be used in NYHA II-III HFrEF who are on GDMT, receiving a beta-blocker at maximally-tolerated dose, who remain in sinus rhythm with heart rate 70 bpm Omega-3 Fatty Acids May reduce mortality and cardiovascular hospitalizations Digitalis Investigation Group. N Engl J Med 1997;336: Tavazzi L et al. Lancet 2008;372: Swedverg K et al. Lancet 2010;376:

32 Guideline-Directed Management & Therapy of Stage C Chronic HF Yancy C et al. J Am Coll Cardiol 2017;71:

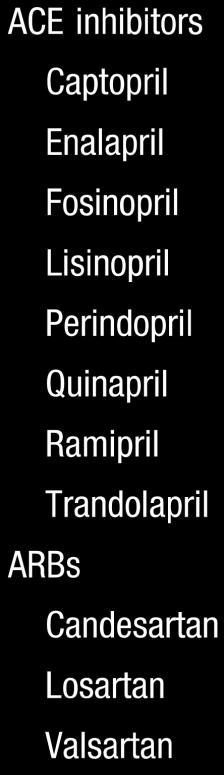
33 Guideline-Directed Management & Therapy ACEi/ARB/ARNI ACEi/ARB/ARNI Starting Dose Maximum Dose Mean Dose Achieved in Trial Captopril 6.25 mg TID 50 mg TID mg/day Enalapril 2.5 mg BID 10 to 20 mg BID 16.6 mg/day Lisinopril 2.5 to 5 mg Daily 20 to 40 mg Daily 32.5 to 35 mg/day Candesartan 4 to 8 mg Daily 32 mg Daily 24 mg/day Losartan 25 to 50 mg Daily 50 to 150 mg Daily 129 mg/day Valsartan 20 to 40 mg BID 160 mg BID 254 mg/day Entresto 50 to 100 mg BID 200 mg BID 375 mg/day N Engl J Med 1987;316: N Engl J Med 2001;344: N Engl J Med 1999;341: N Engl J Med 2005;352: N Engl J Med 2014;371:

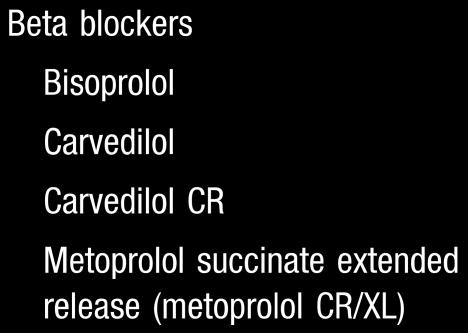
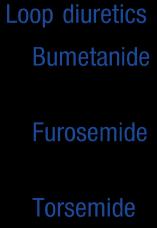
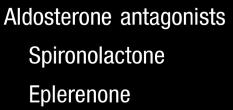
34 Guideline-Directed Management & Therapy Beta-Blockers/HZN-ISDN/Aldo B BB/HZN-ISDN/Aldo B Starting Dose Maximum Dose Mean Dose Achieved in Trial Bisoprolol 1.25 mg Daily 10 mg Daily 8.6 mg/day Carvedilol mg BID 25 mg BID 37 mg/day Metoprolol Succinate 12.5 to 25 mg Daily 200 mg Daily 159 mg/day Hydralazine 25 to 50 mg TID 100 mg TID 175 mg/day Isosorbide Dinitrate 20 to 30 mg TID 40 mg TID 90 mg/day Spironolactone 12.5 to 25 mg BID 25 mg Daily or BID 26 mg/day Eplerenone 25 mg Daily 50 mg Daily 42.6 mg/day N Engl J Med 1987;316: N Engl J Med 2001;344: N Engl J Med 1999;341: N Engl J Med 2005;352: N Engl J Med 2014;371:
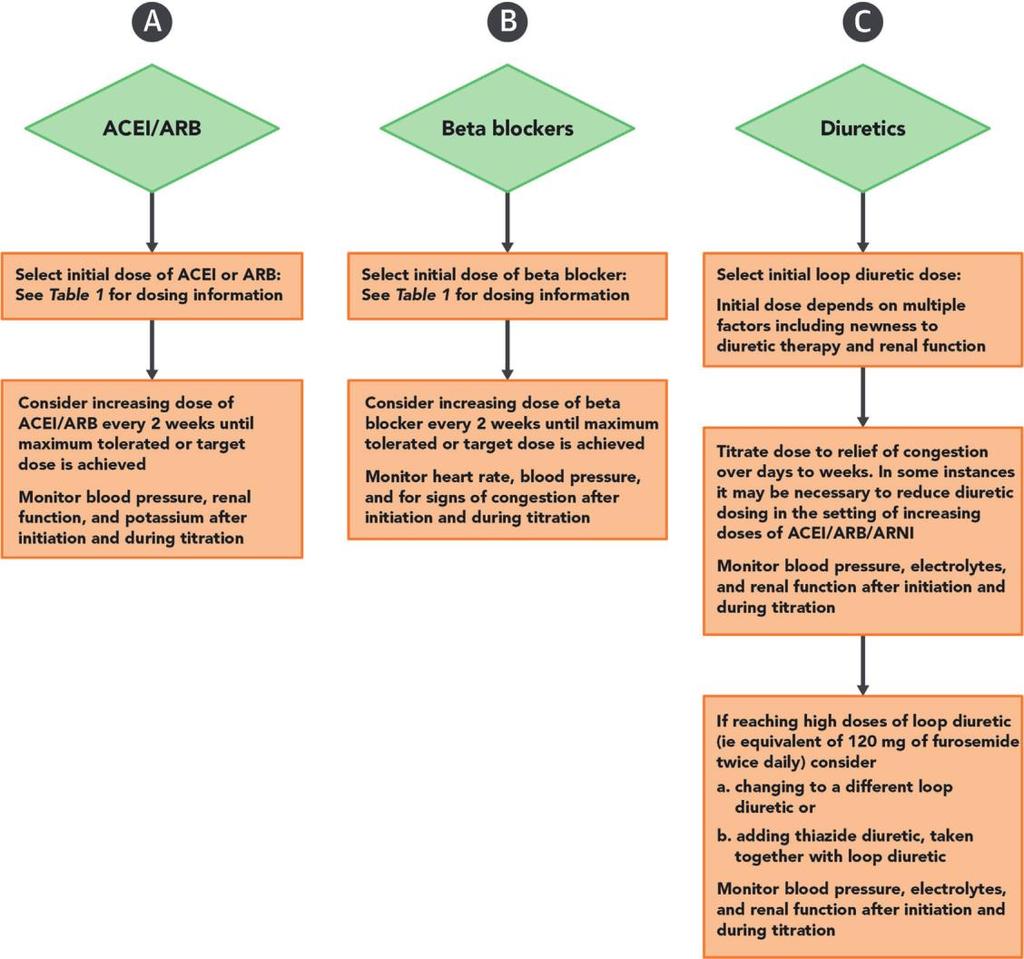
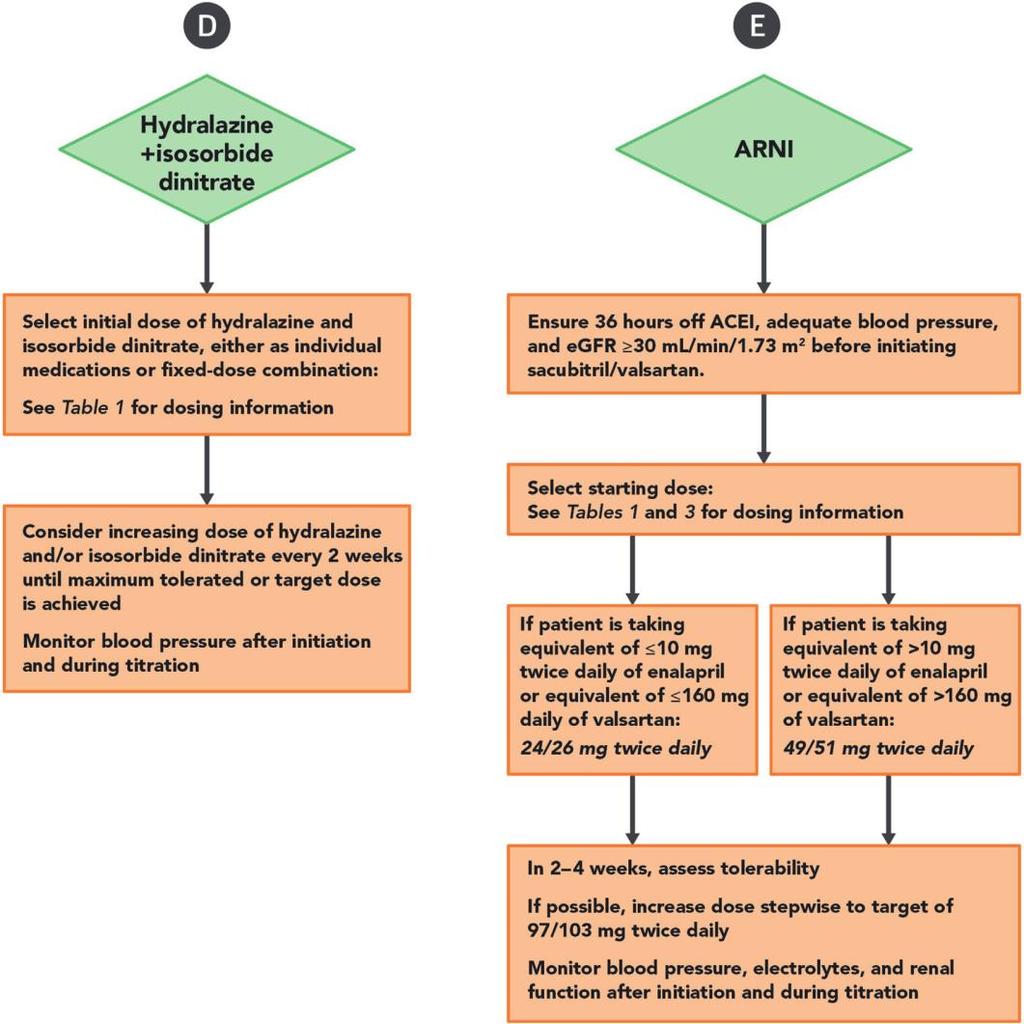
35 Recommendations for Medical Optimization Yancy C et al. J Am Coll Cardiol 2017;71:
36 ICDs and Cardiac Resynchronization Are Important Components of GDMT Moss AJ et al. N Engl J Med 2002;346: Abraham WT et al. N Engl J Med 2002;346: Moss AJ et al. N Engl J Med 1996;335:

37 Early Recognition of Stage D Heart Failure Repeated ( 2) hospitalizations or ED visits for HF in 1 year Progressive decline in renal function Weight loss with unknown cause (cardiac cachexia) Referral to HF specialist for consideration of candidacy for advanced therapies such as LVAD or cardiac transplantation Intolerance to ACEi/ARB/ARNI due to hypotension or worsening renal function Intolerance to beta-blockers due to hypotension or worsening HF Frequent SBP < 90 mmhg Dyspnea with bathing and dressing Unable to walk 1 block without dyspnea or fatigue High diuretic needs (i.e., > furosemide 160 mg/day) Progressive decline in serum sodium Frequent ICD shocks Yancy C et al. J Am Coll Cardiol 2013;62:
38 Acute-on-Chronic Heart Failure: The Hospitalized HF Patient Inability to maintain simultaneous optimal volume and perfusion status as determined by symptoms, signs or hemodynamic measures
39 Acute vs. Chronic Heart Failure Acute Heart Failure Hemodynamic derangement due to sudden ventricular dysfunction Chronic Heart Failure Progressive decline in ventricular function with hemodynamic adaptation
40 Acute vs. Acute-on-Chronic Heart Failure Truly Acute Major end-organ changes, minor LV dysfunction Signs/symptoms usually obvious Usually ischemic Acute-on-Chronic Variable end-organ changes, major LV dysfunction Signs/symptoms often subtle, misleading All etiologies
41 Precipitating Factors Medication/dietary non-adherence Acute coronary syndromes Arrhythmias Non-cardiac diseases COPD, renal failure, infections Pacemaker/ICD malfunction Recreational drugs and alcohol abuse Medication misadventures Disease progression
42 Principles of Management of Acute-on-Chronic Heart Failure Re-establish optimal volume status Intravenous diuretics Re-establish optimal end-organ perfusion Vasodilators or intravenous inotropes Reduction in beta-blocker dose Achieve all of the above simultaneously and as quickly as possible Achieve all of the above in a way that can be maintained in the outpatient setting
43 Principles of Management of Acute-on-Chronic Heart Failure Outpatient GDMT should be continued during the hospitalization in the absence of hypotension or other contraindications If the patient is not on beta-blockers, evidence-based beta-blockers can be started once volume status is normal and the patient is no longer on vasoactive drips When in doubt, do not hesitate to consult your heart failure cardiologist
44 Beta-blocker Caveats in Acute-on-Chronic Heart Failure Try to continue home dose if the patient has adequate perfusion Decrease by 50% if the patient has signs of poor perfusion Discontinue completely if the patient is in cardiogenic shock or requires vasoactive drips or mechanical support Avoid the urge to give beta-blockers for sinus tachycardia in patients with HFrEF
45 Summary HF is a major health problem that carries a high risk of 5-year mortality (~50%) About half of patients suffer from HFrEF and about half suffer from HFpEF NYHA class allows us to assign symptom severity -- class changes with clinical status ACCF/AHA stages reflect disease progression and are helpful in focusing treatment goals
46 Summary Evaluation of HF patients relies on a thorough history and physical examination Key labs assess organ function and prognosis Echocardiography should be obtained in all patients Follow up echocardiograms only in specific scenarios
47 Summary The management of chronic HF involves several drug classes aimed at neurohormones that influence HF progression Optimal medical therapy means that doses used in clinical trials have been achieved medications must be uptitrated over time Transition symptomatic patients who can tolerate ACEi/ARB to Entresto Patients with Stage D HF should be considered for LVAD/heart transplant
48 Summary Patients with acute-on-chronic heart failure are mainly treated with volume management and, if needed, vasodilators/inotropes Continue GDMT uninterrupted, if possible Beta-blockers should be started at low dose only after volume status is normal and the patient is stable off all drips No beta-blockers for sinus tachycardia in HFrEF

49 p h o n e t o l l - f r e e F H T r a n s p l a n t.c o m f a c e b o o k.com/ F H Orlando y o u t u b e.com/flhospit alorlando Thank you
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Disclosures. This speaker has indicated there are no relevant financial relationships to be disclosed.
 Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Disclosures This speaker has indicated there are no relevant financial relationships to be disclosed. And the Beat Goes On: New Medications for Heart Failure Alison M. Walton, PharmD, BCPS The Case of
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Heart Failure: Current Management Strategies
 Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Heart Failure: Current Management Strategies CSHP Fall Education Session- September 30th, 2017 Carolyn MacKinnon & Tamara Matchett BscPharm, ACPR Candidates Objectives 1. Describe the pathophysiology &
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction
 for the treatment of heart failure with reduced ejection fraction") Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Cardio-Metabolic Franchise Entresto Development of sacubitril/valsartan (LCZ696) for the treatment of heart failure with reduced ejection fraction Randy L Webb, PhD Rutgers Workshop October 21, 2016 Heart
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
Congestive Heart Failure 2015
 Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
ENTRESTO (sacubitril and valsartan) oral tablet
 oral tablet") ENTRESTO (sacubitril and valsartan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
ENTRESTO (sacubitril and valsartan) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation
 Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
Ventricular Assist Device: Are Early Interventions Superior? Hamang Patel, MD Section of Cardiomyopathy & Heart Transplantation Objectives Current rationale behind use of MCS Patient Selection Earlier?
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
2/3/2017. Objectives. Effective Heart Failure Management through Evidence Based Practice and Innovation
 Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Disclosure Statement. Heart Failure: Refreshers and Updates. Objectives. CHF: Chronic Heart Failure. Definitions. Definitions 2/19/2018
 Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Disclosure Statement Heart Failure: Refreshers and Updates Tracy K. Pettinger, PharmD Clinical Associate Professor College of Pharmacy The planners and presenter of this presentation have disclosed no
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
I have no disclosures. Disclosures
 I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
Objectives. Outline 4/3/2014
 Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
WHAT S NEW IN HEART FAILURE
 WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
WHAT S NEW IN HEART FAILURE Drugs, Devices and Diagnostics John M. Herre, MD, FACC, FACP Director, Advanced Heart Failure Program Sentara Helathcare Professor of Medicine Eastern Virginia Medical School
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure. Elizabeth Pogge, PharmD, MPH, BCPS, FASCP
 Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
Sacubitril/valsartan: A New Management Strategy for the Treatment of Heart Failure Elizabeth Pogge, PharmD, MPH, BCPS, FASCP Disclosure Elizabeth Pogge reports no actual or potential conflicts of interest
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham
 Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
Diagnosis and management of Chronic Heart Failure in 2018: What does NICE say? PCCS Meeting Issues and Answers Conference Nottingham NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Chronic heart failure
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Advanced Care for Decompensated Heart Failure
 Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Advanced Care for Decompensated Heart Failure Sara Kalantari MD Assistant Professor of Medicine, University of Chicago Advanced Heart Failure, Mechanical Circulatory Support and Cardiac Transplantation
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses
 Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Topic Page: congestive heart failure
 Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Topic Page: congestive heart failure Definition: congestive heart f ailure from Merriam-Webster's Collegiate(R) Dictionary (1930) : heart failure in which the heart is unable to maintain an adequate circulation
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers
 Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
Risk Stratification in Heart Failure: The Role of Emerging Biomarkers David G. Grenache, PhD Associate Professor of Pathology, University of Utah Medical Director, ARUP Laboratories Salt Lake City, UT
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Heart Failure, Anticoagulants, and Medication Reconciliation
 Change in Condition: Heart Failure, Anticoagulants, and Medication Reconciliation Lindsay Holland, MHA Director, Care Transitions Health Services Advisory Group (HSAG) Pouya Afshar, MD, MBA Hospitalist,
Change in Condition: Heart Failure, Anticoagulants, and Medication Reconciliation Lindsay Holland, MHA Director, Care Transitions Health Services Advisory Group (HSAG) Pouya Afshar, MD, MBA Hospitalist,
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
HEART FAILURE KEEPING YOUR PATIENT AT HOME
 HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much?
 2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
2017 CCS HF Guidelines Medical Therapy for HFrEF When What Order and How Much? Dr. Shelley Zieroth University of Manitoba @ShelleyZieroth @CanHFSociety Disclosures Consulting/Advisory Board: Amgen, Astra
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
HEART FAILURE IN WOMEN. Marian Limacher, MD Division of Cardiovascular Medicine University of Florida
 HEART FAILURE IN WOMEN Marian Limacher, MD Division of Cardiovascular Medicine University of Florida Outline Epidemiology Clinical Overview Why HF is such a challenge State of the Field Heart Failure Adjudication
HEART FAILURE IN WOMEN Marian Limacher, MD Division of Cardiovascular Medicine University of Florida Outline Epidemiology Clinical Overview Why HF is such a challenge State of the Field Heart Failure Adjudication
Balanced information for better care. Heart failure: Managing risk and improving patient outcomes
 Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
Balanced information for better care Heart failure: Managing risk and improving patient outcomes Heart failure increases hospitalization Heart failure is the most common medical reason for hospitalization
New CHF Patient in my Office: What Should I Do?
 New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support No disclosures Disclosures Clinical Presentation 38 year
New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support No disclosures Disclosures Clinical Presentation 38 year