2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
|
|
|
- Domenic Fleming
- 5 years ago
- Views:
Transcription

1 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine Faculty of Medicine Siriraj Hospital
2 Objective 2016 ESC/EAS Dyslipidemias guideline Current target when Rx dyslipidemias patients Evidence based on efficacy and Safety What has changes?

3 Recommendation Class: Definitions Eur Heart J 2016: doi / eurheartj/ ehv272

4 Level of Evidence: Definitions Eur Heart J 2016: doi / eurheartj/ ehv272
![Causes of death worldwide [Mackay 2004:E] Deaths (2002)* *Population: Age 60 years; CHD is the second leading cause of death in persons 15-59](/docs-images/95/125552976/images/5-0.jpg "years. Mackay J, et al. Deaths from coronary heart disease. In: The Atlas of Heart Disease and Stroke.")
5 Causes of death worldwide [Mackay 2004:E] Deaths (2002)* *Population: Age 60 years; CHD is the second leading cause of death in persons years. Mackay J, et al. Deaths from coronary heart disease. In: The Atlas of Heart Disease and Stroke. Geneva: World Health Organization; 2004:46-49.



6 Lipoproteins in Atherosclerosis: Response-to-Retention Model 1,2 1 ApoB lipoprotein retention Lipoprotein modification 2 Inflammatory response 3 Macrophage recruitment Foam cell formation Lesion progression 4 SMC migration Fibrous cap formation Macrophage necrosis 1 Modified lipoprotein ApoB lipoproteins in plasma 2 Macrophage Fibrous cap 3 Foam cell SMCs 4 Growth factors Cytokines Plaque necrosis with cholesterol crystals Apo = apolipoprotein; SMC = smooth muscle cell. 1. Tabas I et al. Circulation. 2007;116: Sherer Y et al. Nat Clin Pract Rheumatol. 2006;2:

7 Atherothrombosis Plaque Rupture Thrombosis Atherosclerosis Stable angina Intermittent Claudication Critical Limb Ischemia MI ACS Stroke/TIA Acute limb ischemia CV death Stary HC. Circulation 1995; Fuster V, et al. Vasc Med1998; 3: 231-9
8 General Concepts of Reperfusion Therapy Myocardial salvage is defined as the difference between the actual and potential infarct size : The initial area at risk during acute coronary occlusion. Gersh BJ, Stone GW, White HD, Homes DR Jr. JAMA 293:979, 2005.

9 Consequences of the reperfusion at various time after coronary adhesion Robbins and Cotran PATHOLOGIC BASIS OF DISEASE 8 th edition, 2009

 MADIT 1 NEJM 1996;")

10 Ischemic Cardiomyopathy- Disease that utilize high cost/resource but still has a poor outcome Cost Mortality (Baht) MADIT 1 NEJM 1996; 335: ; DINAMIT NEJM 2004; 351: , STICH NEJM 2011; 364:
11
12

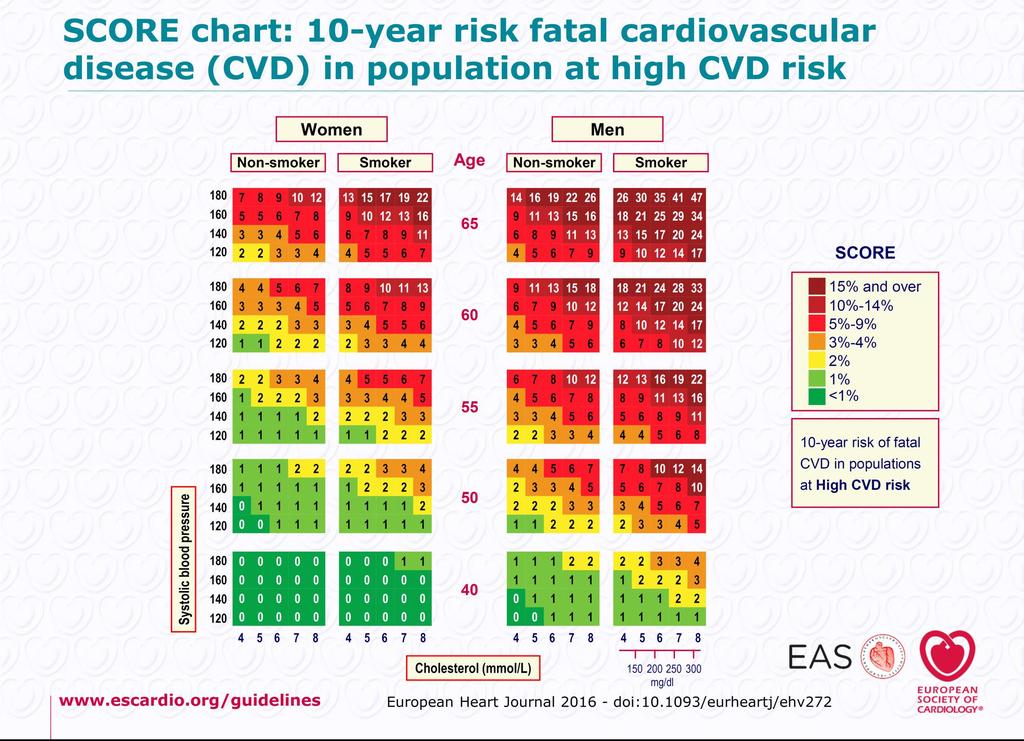
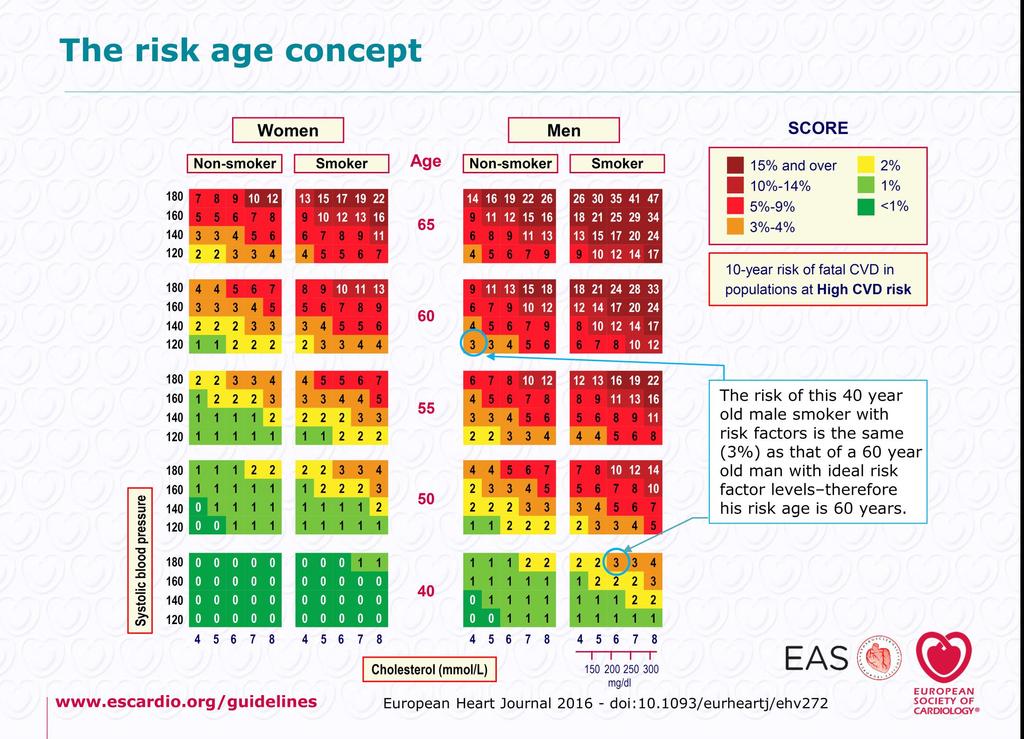
13 Risk Estimation Eur Heart J 2016: doi / eurheartj/ ehv272

14 Risk Categories Eur Heart J 2016: doi / eurheartj/ ehv272
15 ESC/EAS 2011 Guidelines for the Management of Dyslipidemia Very High Risk Documented cardiovascular disease by Invasive or noninvasive testing for atherosclerosis Previous MI Acute coronary syndrome Coronary revascularization Ischemic stroke Peripheral artery disease Type 2 DM, or type 1 DM with target organ damage (such as microalbuminuria). Type 2 DM with CVD or CKD. Type 2 DM aged >40 yr with at least 1 other CV risk factor. Moderate-to-severe CKD (glomerular filtration rate <60 ml/min/1.73 m 2 ) 10-year risk SCORE 10% Cardiovascular Risk Levels High Risk Markedly elevated single risk factors (eg, familial dyslipidemia and severe hypertension) 10-year risk SCORE 5% to <10% Moderate Risk 10-year risk SCORE 1% to <5% Low Risk 10-year risk SCORE <1% ESC guideline 2011 Management for Dyslipidaemias. EHJ 2011; 32:
16 Cardiovascular Event Rate, % Risk Pattern for Subsequent CV Events Over a Range of LDL-C Values LDL, mg/dl CHD + Diabetes CHD + MS or IFG CHD No MS or IFG Diabetes No CVD No Diabetes No CVD CV = cardiovascular; CHD = coronary heart disease; MS = metabolic syndrome; IFG = impaired fasting glucose; CVD = CV disease. 1. Robinson JG et al. Am J Cardiol. 2006;98:
17 Proportional Reduction in Vascular Event Rate (95% CI), % CTT Meta-analysis: Proportional Reduction in Major Vascular Events vs Absolute LDL-C Reduction More vs less (5 trials) Statin vs control (21 trials) % risk reduction per 1 mmol/l (39 mg/dl) P< Mean LDL-C Difference Between Treatment Groups, mg/dl CTT = Cholesterol Treatment Trialists; CI = confidence interval. 1. Cholesterol Treatment Trialists (CTT) Collaboration. Lancet. 2010;376:

18 Lipid Analysis Eur Heart J 2016: doi / eurheartj/ ehv272
19 Non HDL-C Is a Risk Factor for CHD Non HDL-C represents the cholesterol content of all apob-containing lipoproteins, including VLDL, IDL, LDL, Lp(a), and chylomicrons and chylomicron remnants 1,2 Non HDL-C = total cholesterol HDL-C 1 When TG levels are 200 mg/dl, non HDL-C may better represent the concentration of all atherogenic lipoproteins than does LDL-C alone 1 Multiple prospective cohort studies have shown that non HDL-C may be superior to LDL-C for CV risk assessment 3 Non HDL-C 1,3,4 HDL-C 1,5 Chylomicrons TG C apob-48 Chylomicron remnants TG C apob-48 VLDL TG C apob- 100 IDL TG C apob- 100 Large buoyant LDL C apob- 100 Small dense LDL C apob- 100 C Lp(a) apob- 100 HDL C apo A1 Adapted with permission from Walldius G et al. 6 Other major risk factors (beyond dyslipoproteinemia) include smoking, hypertension, and family history of premature CAD. CHD = coronary heart disease; ApoB = apolipoprotein B; VLDL = very low-density lipoprotein; IDL = intermediate-density lipoprotein; Lp(a) = lipoprotein (a); TG = triglyceride; CV = cardiovascular; C = cholesterol; CAD = coronary artery disease. 1. NCEP ATP III Expert Panel. Circulation. 2002;106: Rana JS et al. Curr Opin Cardiol. 2010;25: Hoenig MR. Vasc Health Risk Manag. 2008;4: Chapman M et al. Eur Heart J Suppl. 2004;6(suppl A):A43 A Barter P. In: Ballantyne CM. Clinical Lipidology: A Companion to Braunwald s Heart Disease. Saunders, an imprint of Elsevier Inc; 2009: Walldius G et al. J Intern Med. 2004;255:
20 Previous Guideline Recommendations for Managing LDL-C in Patients With CHD (Stable or ACS) Previous Guideline Risk Group Classification Recommended LDL-C Goal or Treatment NCEP ATP III Very high risk a LDL-C <100 mg/dl (<70 mg/dl is a therapeutic option) (2004 update) 1 High risk b LDL-C <100 mg/dl Current Guidelines European 2012 CVD Prevention Guidelines 2 ACC/AHA 2013 Blood Cholesterol Guideline 3 Risk Group Classification Very high risk c Clinical ASCVD d (high risk) Recommended LDL-C Goal or Treatment LDL-C <1.8 mmol (<~70 mg/dl) or a 50% LDL-C reduction when target level cannot be reached Aged 75 years: high-intensity statin therapy (anticipated to achieve 50% LDL-C reduction from untreated baseline) e Aged >75 years OR not a candidate for high-intensity statin: moderate-intensity statin therapy (anticipated to achieve 30% to <50% LDL-C reduction from untreated baseline) e a Established CVD plus multiple risk factors (especially diabetes); severe and poorly controlled risk factors (especially cigarette smoking); multiple risk factors of the metabolic syndrome; patients with ACS. 1 b CHD or CHD risk equivalent (diabetes, other atherosclerotic disease [eg, peripheral arterial disease, >50% carotid artery stenosis], or 10-year risk for hard CHD >20%). 1 c Documented CVD by invasive or noninvasive testing, previous MI, ACS, coronary or other revascularization procedure, ischemic stroke, PAD, diabetes mellitus with 1 cardiovascular risk factor and/or target organ damage, severe CKD, or a calculated 10-year risk SCORE 10%. 2 d Clinical ASCVD includes ACS, history of MI, stable or unstable angina, coronary or other arterial revascularization, stroke, TIA, or PAD presumed to be of atherosclerotic origin; high-risk individuals include those with ASCVD, those with LDL-C 190 mg/dl, and individuals with diabetes. 3 e Clinicians treating high-risk patients who have a less-than-anticipated response to statins may consider the addition of a nonstatin cholesterol-lowering therapy. 3 CHD = coronary heart disease; ACS = acute coronary syndrome; NCEP ATP III = National Cholesterol Education Program Adult Treatment Panel III; CVD = cardiovascular disease; ACC = American College of Cardiology; AHA = American Heart Association; ASCVD = atherosclerotic CVD; MI = myocardial infarction, PAD = peripheral artery disease; CKD = chronic kidney disease; SCORE = Systematic Coronary Risk Evaluation; TIA = transient ischemic attack. 1. Grundy SM et al. Circulation. 2004;110: Perk J et al. Eur Heart J. 2012;33: Stone NJ et al. Circulation. 2014;129(suppl 2):S1 S45.
21 Key point from American Guideline Standpoint Science is not compare treating to target of each LDL level systematically but comparing high versus nonhigh intensity statin Establishment of a specific target level of LDL would be arbitrary because risk is continuous and express by regression line
22 Proportional Reduction in Vascular Event Rate (95% CI), % CTT Meta-analysis: Proportional Reduction in Major Vascular Events vs Absolute LDL-C Reduction More vs less (5 trials) Statin vs control (21 trials) % risk reduction per 1 mmol/l (39 mg/dl) P< Mean LDL-C Difference Between Treatment Groups, mg/dl CTT = Cholesterol Treatment Trialists; CI = confidence interval. 1. Cholesterol Treatment Trialists (CTT) Collaboration. Lancet. 2010;376:
 LDL-C: <130 mg/dl Atorvastatin 10 mg")
23 TNT (Treating to New Targets) Patient population: CHD LDL-C: mg/dl TGs 600 mg/dl Screening and wash-out (n=18 469) Open-label run-in (n= ) Baseline Primary efficacy outcome measure: Occurrence of a major CV event: CHD death Nonfatal, non-procedure-related MI Resuscitated cardiac arrest Fatal or nonfatal stroke Double-blind period (n=10 001) LDL-C: <130 mg/dl Atorvastatin 10 mg n=5006 Atorvastatin 10 mg LDL-C target: 100 mg/dl n=4995 Atorvastatin 80 mg LDL-C target: 75 mg/dl 1 8 weeks 8 weeks Median follow-up=4.9 years LaRosa JC, et al. N Engl J Med 2005;352:
24 Cumulative incidence (%) TNT Incidence of major CVD events Atorvastatin 10 mg (n=5006). Mean LDL-C during study 101 mg/dl Atorvastatin 80 mg (n=4995). Mean LDL-C during study 77 mg/dl 22% RRR HR % CI 0.69 to 0.89 (p<0.001) ARR=2.2% NNT 45 over 4.9 years Time (years) Atorvastatin 80 mg reduced the risk of hospitalization for HF by 26% (HR 0.74; 95% CI ; p=0.01) relative to atorvastatin 10 mg LaRosa JC, et al. N Engl J Med 2005;352: From New England Journal of Medicine, LaRosa JC, et al. Intensive Lipid Lowering with Atorvastatin in Patients with Stable Coronary Disease, 352, Copyright (2005) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
25 Patients (%) TNT Increasing LDL-C Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5 (<64 mg/dl) (64 <77 mg/dl) (77 <90 mg/dl) (90 <106 mg/dl) ( 106 mg/dl) p<0.0001* 10 8 p<0.0001* p<0.01* p<0.05* 0 *p-value for trend across LDL-C (continuous variable) Major CV events CHD death Nonfatal MI Stroke LaRosa JC, et al. Am J Cardiol 2007;100: Reprinted from American Journal of Cardiology, Vol 100, LaRosa JC et al. Safety and Efficacy of Atorvastatin-Induced Very Low-Density Lipoprotein Cholesterol Levels in Patients With Coronary Heart Disease (a Post Hoc Analysis of the Treating to New Targets [TNT] Study), Copyright (2007), with permission from Elsevier
26 Risk reduction vs atorvastatin 10 mg (%) TNT: High-intensity atorvastatin 80 mg reduced CV events vs moderate-intensity atorvastatin in patients with CHD 0 Fatal or nonfatal Nonfatal MI 1 stroke 1 Revasc. 2 Hosp. for CHF 1 Angina % p= % p= % p= % 26% p=0.01 p< Mean LDL-C values during the study were 77 mg/dl for atorvastatin 80 mg and 101 mg/dl for atorvastatin 10 mg 1. LaRosa JC, et al. N Engl J Med 2005;352: Data on file. Pfizer Inc, New York, NY
27 PROVE-IT TIMI 22: Atorvastatin for reduction of CV risk in patients with ACS Study design highlights Patient population: Enrolled at 349 sites in eight countries Men and women, aged 18 years Hospitalized for an ACS in the preceding 10 days Total-C 240 mg/dl or total-c 200 mg/dl if receiving lipid-lowering therapy Primary endpoint: Time to the first occurrence of a major CV event 4162 patients Double-blind period Atorvastatin 80 mg/day Pravastatin 40 mg/day Mean 2-year follow-up (925 primary events) Cannon CP, et al. N Engl J Med 2004;350:
28 Death or major CV event (%) PROVE-IT: Atorvastatin reduces CV risk in patients with ACS PROVE-IT: atorvastatin 80 mg reduced the risk of death or a major CV event by 16% (p=0.005) compared with pravastatin 40 mg in patients with ACS Incidence of death or major CV events * 16% RRR 95% CI 5 to 26% (p=0.005) ARR 3.9% NNT 26 over 2 years *Major CV events: MI, unstable angina requiring hospitalization, revascularization, and stroke 5 0 Pravastatin 40 mg (n=2063). Median LDL-C 95 mg/dl Atorvastatin 80 mg (n=2099). Median LDL-C 62 mg/dl Time (years) Cannon CP, et al. N Engl J Med 2004;350:
29 Death, MI, or rehospitalization for ACS (%) PROVE-IT: Benefit of atorvastatin over pravastatin was evident at 30 days PROVE-IT: atorvastatin 80 mg reduced the composite triple endpoint (death, MI, or rehospitalization for ACS) within 30 days of randomization This benefit remained stable from 30 days onward ARR 1.2% NNT=83 over 30 days 28% RRR HR % CI 0.52 to 0.99 (p=0.046) 1 0 Pravastatin 40 mg (n=2063). Mean LDL-C at 30 days=88 mg/dl Atorvastatin 80 mg (n=2099). Mean LDL-C at 30 days=60 mg/dl Time (days following randomization) Ray K, et al. JACC 2005;46:

30 MIRACL: Atorvastatin for reduction of CV events in patients with ACS Patient population: Enrolled at 122 sites Men and women with unstable angina or non-q-wave acute MI Randomized within hours of hospital admission 3086 patients Atorvastatin 80 mg/day 16-week double-blind treatment phase Placebo plus usual care Primary end point: Time to first ischemic event* *Death, nonfatal acute MI, cardiac arrest with resuscitation, or recurrent symptomatic myocardial ischemia Schwartz GG, et al. JAMA 2001;285:
31 MIRACL: Atorvastatin reduces stroke within 16 weeks in patients with ACS MIRACL: Atorvastatin 80 mg reduced the risk of fatal or non-fatal stroke by 50% (p=0.045) compared with placebo Atorvastatin 80 mg (n=1538) Placebo (n=1548) Fatal or nonfatal stroke % RRR HR % CI, (p=0.045) Nonfatal stroke % RRR HR % CI, (p=0.048) Patients experiencing strokes over 16 weeks (%) Schwartz GG, et al. JAMA 2001;285:
32 Treatment Goal for LDL Eur Heart J 2016: doi / eurheartj/ ehv272

33 Treatment Target and Goals for CV disease prevention Eur Heart J 2016: doi / eurheartj/ ehv272


34 Impact of Life style Change on Lipid Level Eur Heart J 2016: doi / eurheartj/ ehv272

35 Impact of Life style Change on Lipid Level Eur Heart J 2016: doi / eurheartj/ ehv272

36 Dietary Recommend to Lower LDL Eur Heart J 2016: doi / eurheartj/ ehv272

37 Treatment Goal for LDL Eur Heart J 2016: doi / eurheartj/ ehv272

38 Meta-Analysis of Therapeutic Equivalent Dose of Statins Weng TC et al. J Clin Pharm Ther 2010; 35: , Mukhtar RY et al. Int J Clin Prac 2005; 59: , Eur Heart J 2016: doi / eurheartj/ ehv272
39 Atorvastatin is well tolerated across the dosage range Data from a pooled analysis involving patients from 49 trials AE, % Atorvastatin 10 mg (n=7258) Atorvastatin 80 mg (n=4798) Placebo (n=2180) Withdrawals due to treatmentrelated AEs Serious treatment-related nonfatal AEs Myalgia Treatment-related myalgia Persistent ALT or AST >3 ULN * Persistent CK >10 ULN * Rhabdomyolysis Albuminuria Hematuria *Based on the number of patients with laboratory measurements CK, creatine kinase Newman C, et al. Am J Cardiol 2006;97:61 67
40 High-intensity atorvastatin is well tolerated in patients aged 65 years Pooled analysis of data from 50 randomized clinical trials AE, % Atorvastatin 10 mg (n=2042) Atorvastatin 80 mg (n=1698) Placebo (n=995) Treatment-related AEs Withdrawals due to treatment-related AEs Serious, treatmentrelated nonfatal AEs Death Hey-Hadavi JH, et al. Am J Geriatr Pharmacother 2006;4:

41 Pharmacologic treatment of Hypercholesterolemia Eur Heart J 2016: doi / eurheartj/ ehv272
42 What has change? Focus on specific LDL cholesterol target Patients at very high risk for cardiovascular events to an LDL cholesterol target < 70 mg/dl, or to achieve at least a 50% reduction in LDL cholesterol if baseline levels range between 70 and 135 mg/dl (class 1, level of evidence B). Patient with high risk for cardiovascular events, the LDL cholesterol target <100 mg/dl, or with the aim of achieving at least a 50% reduction in LDL cholesterol if baseline levels range between 100 and 200 mg/dl (class I, level of evidence B). DM without target organ damage and moderate CKD are placed in high risk ESC/EAS recommending the highest dose tolerable to achieve treatment goals (class I, level of evidence A). For patients who are statin intolerant, ezetimibe or a bile-acid sequestrant should be considered (class IIa, level of evidence C), while statins and ezetimibe can be considered for patients not at goal (class IIa, level of evidence B). Indication for PCSK9 inhibitors

43 Drug Treatment of Hypertriglyceridaemia Eur Heart J 2016: doi / eurheartj/ ehv272

44 Drug Treatment of Low HDL Eur Heart J 2016: doi / eurheartj/ ehv272

45 Treatment of Dyslipidemia in DM Eur Heart J 2016: doi / eurheartj/ ehv272
46 Patients with major CV events (%) TNT: High- vs moderate-intensity atorvastatin reduces major CV events in patients with CHD and diabetes Subgroup analysis 1501 patients in TNT had diabetes (and stable CHD) Incidence of major CV events Atorvastatin 10 mg (n=753). Final mean LDL-C 99 mg/dl Atorvastatin 80 mg (n=748). Final mean LDL-C 77 mg/dl 25% RRR HR % CI 0.58 to 0.97 (p=0.026) ARR 4.1% NNT 24 over 4.9 years Time (years) 6 Shepherd J, et al. Diabetes Care 2006;29: American Diabetes Association, Effect of Lowering LDL Cholesterol Substantially Below Currently Recommended Levels in Patients With Coronary Heart Disease and Diabetes, American Diabetes Association, Copyright and all rights reserved. Material from this publication has been used with the permission of American Diabetes Association.
47 Rate of acute cardiac events (%) PROVE-IT: Atorvastatin reduces acute cardiac events in patients with ACS and diabetes PROVE-IT (sub-analysis): Atorvastatin 80 mg reduced the risk of acute cardiac events by 25% (p=0.03) compared with pravastatin 40 mg in a post-hoc analysis of patients with recent ACS and type 2 diabetes 30 Incidence of acute cardiac events * 25% *Death, MI, and unstable angina requiring hospitalization % Median LDL-C at 30 days: 57 mg/dl 26.6% Median LDL-C at 30 days: 81 mg/dl Atorvastatin 80 mg Pravastatin 40 mg n=499 n=479 RRR (p=0.03) ARR 5.5% NNT 18 over 2 years Ahmed S, et al. Acute coronary syndromes and diabetes: is intensive lipid lowering beneficial? Results of the PROVE IT-TIMI 22 trial. European Heart Journal, 2006, 27(19), , by permission of Oxford University Press

48 Lipid Lowering for Primary and Secondary Prevention of stroke Eur Heart J 2016: doi / eurheartj/ ehv272

49 SPARCL: High-intensity atorvastatin for reduction of CV events in high-risk patients with previous stroke/tia Patient population: Enrolled at 205 sites worldwide Men and women with previously documented TIA or stroke A modified Rankin Score of 3 LDL-C levels 100 mg/dl and 190 mg/dl Primary endpoint: Time to the first occurrence of a fatal or nonfatal stroke 4731 patients Double-blind period Atorvastatin 80 mg/day Placebo Median follow-up 4.9 years Amarenco P, et al. N Engl J Med 2006;355:
50 Fatal or nonfatal stroke (%) SPARCL: High-intensity atorvastatin reduces stroke in high-risk patients with previous stroke/tia SPARCL: atorvastatin 80 mg provided 16% RRR in the primary endpoint of fatal or nonfatal stroke in patients with recent stroke or TIA and no CHD compared with placebo (p=0.03) Incidence of fatal or nonfatal stroke ARR 2.2%; NNT=45 over 5 years 16% RRR HR % CI 0.71 to 0.99 (p=0.03) 4 0 Placebo (n=2366). Mean LDL-C during study 128 mg/dl Atorvastatin 80 mg (n=2365). Mean LDL-C during study 73 mg/dl Time (years since randomization) Amarenco P, et al. N Engl J Med 2006;355: From New England Journal of Medicine, Amarenco P, et al. High-Dose Atorvastatin after Stroke or Transient Ischemic Attack, 355, Copyright (2006) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society

51 Lipid Lowering in Patients with PAD Eur Heart J 2016: doi / eurheartj/ ehv272
52 Conclusion Very high risk patients: LDL-C goal <70 mg/dl or a reduction of at least 50% if baseline LDL-C between mg/dl High risk patients: LDL-C goal <100 mg/dl or a reduction of at least 50% if baseline LDL-C between mg/dl High dose atorvastatin (80/40) showed feasibility to reach the 50% reduction target as well as reduction in CV events as evidence by TNT, MIRACLE, PROVE-IT, SPARCL trial etc Guideline recoomend maximal tolerated dose of statin to achieve treatment goal High intensity of atorvastatin is well tolerated
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
10/15/2012. Lessons Learned from Tim Russert: Investigating Residual Risk. Tim Russert: Residual CV Risk?
 Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Lessons Learned from Tim Russert: Investigating Residual Risk Peter H. Jones, MD, FACP Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Houston, Texas Tim Russert:
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Dyslipidemia and the Use of Statins. Troy L Randle, DO, FACC, FACOI
 Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your
Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice
 Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
LIPID GUIDELINES: 2015
 LIPID GUIDELINES: 2015 D P Mikhailidis BSc MSc MD FCPP FCP FRSPH FFPM FRCP FRCPath Academic Head Dept. of Clinical Biochemistry (Vascular Disease Prevention Clinics) Royal Free campus University College
LIPID GUIDELINES: 2015 D P Mikhailidis BSc MSc MD FCPP FCP FRSPH FFPM FRCP FRCPath Academic Head Dept. of Clinical Biochemistry (Vascular Disease Prevention Clinics) Royal Free campus University College
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo?
 Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
LDL and the Benefits of Statin Therapy
 LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
Comparison of Original and Generic Atorvastatin for the Treatment of Moderate Dyslipidemic Patients
 Comparison of Original and Generic Atorvastatin for the Treatment of Moderate Dyslipidemic Patients Cardiology Department, Bangkok Metropolitan Medical College and Vajira Hospital, Bangkok, Thailand Abstract
Comparison of Original and Generic Atorvastatin for the Treatment of Moderate Dyslipidemic Patients Cardiology Department, Bangkok Metropolitan Medical College and Vajira Hospital, Bangkok, Thailand Abstract
CETP inhibition: pros and cons. Philip Barter The Heart Research Institute Sydney, Australia
 CETP inhibition: pros and cons Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies or membership of advisory boards from:
CETP inhibition: pros and cons Philip Barter The Heart Research Institute Sydney, Australia Philip Barter Disclosures Received honorariums for lectures, consultancies or membership of advisory boards from:
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
NICE QIPP about Lipitor. Robert Trotter. Clinical Effectiveness Consultant
 NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Prevention Updates and Paradigm Shifts
 Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
Prevention Updates and Paradigm Shifts Andrew Freeman, MD, FACC Director of Clinical Cardiology and Operations National Jewish Health Assistant Professor of Medicine National Jewish Health and University
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Curriculum Vitae Name : Prof. DR. Dr. Idrus Alwi SpPD, K-KV, FACC, FESC, FAPSIC, FINASIM, FACP. Current Position : Professor of Internal Medicine,
 Curriculum Vitae Name : Prof. DR. Dr. Idrus Alwi SpPD, K-KV, FACC, FESC, FAPSIC, FINASIM, FACP. Current Position : Professor of Internal Medicine, Faculty of Medicine, UI Medical Student : Faculty of Medicine
Curriculum Vitae Name : Prof. DR. Dr. Idrus Alwi SpPD, K-KV, FACC, FESC, FAPSIC, FINASIM, FACP. Current Position : Professor of Internal Medicine, Faculty of Medicine, UI Medical Student : Faculty of Medicine
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis?
 Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients