Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
|
|
|
- Charleen Foster
- 5 years ago
- Views:
Transcription

1 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with normal values Integrate with clinical presentation into meaningful conclusion ECG Rate and Rhythm Normal rate for adults 60 to 100 bpm Speed Reading Normal, Slow, Fast Normal rhythm for adults Sinus with less than 10% variability of beat to beat Remember hiding premature atrial or ectopic beats can affect rhythm regularity Review p wave morphologies to determine if the rhythm is truly sinus 1
 P axis: 0-60º QRS axis: -30 to 90º T axis generally follows the QRS axis except in the precordial leads where T waves should be upright from V2-6 Speed Reading Intervals & Axes")
2 Normal Intervals & Axes PR 0.12 to 0.20 sec QRS - < 0.10; 0.11 to 0.12 incomplete IVCD; abnormal > 0.12 sec QT c < 0.44 sec (QT c = QT/ RR) P axis: 0-60º QRS axis: -30 to 90º T axis generally follows the QRS axis except in the precordial leads where T waves should be upright from V2-6 Speed Reading Intervals & Axes PR < one large box QRS < 3 small boxes QT < 50% of RR interval (not to used in AFib) Axes: P upright in I & II QRS positive in Leads I & II = normal LAD QRS isoelectric or negative in II RAD QRS isoelectric or negative in I T waves Same direction as major QRS vector in limb leads Upright in V yo man awaken by chest pain 2
3 Question #1 Which is the correct answer? 1. This ECG excludes an Acute MI 2. This ECG can be seen in STEMI 3. This ECG is a Right-Sided ECG 4. This ECG represents Arm Lead Reversal Electrically silent MI s Right Ventricular MI Right sided ECG High Lateral MI V7, V8, V9 Small Apical MI 3



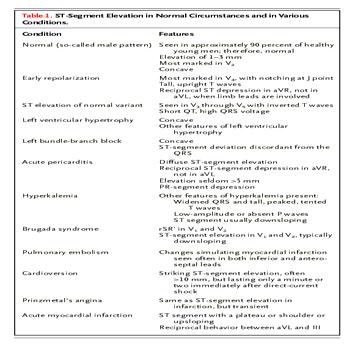
4 78 yo man with intracerebral hemorrhage Einthoven s Triangle - ECG RA-RL rev II 4

5 RA RL Cable Reversal Far Field Signal in II No structural abnormality can explain this finding The Technician s Test 55 yo man admitted for abdominal pain Sinus Arrhythmia 1.0 sec 0.8 sec 5

 43 yo obese man admitted with")
6 Sinus Rhythm Variations Normal Sinus Rhythm HR bpm Sinus Bradycardia HR < 60 bpm Sinus Tachycardia HR > 100 bpm Sinus Arrhythmia >10% change from longest to shortest P P interval Irregular sinus rhythm (Sinus arrhythmia of the elderly) 43 yo obese man admitted with chest pain. 6


7 LVH LBBB PCard K+ AMI RB+AMI Brugada 7

8 STEMI - ACS If the patient s history and clinical presentation is consistent with ACS IT DOESN T MATTER WHAT THE ECG LOOKS LIKE! THE WORRISOME CLINICAL PRESENTATION OF CONCERN IS THIS PATIENT LOOKS LIKE!! ST Elevation Common Causes Acute myocardial injury pattern Acute pericarditis Early Repolarization / Normal Variant + 0.1mV in any lead Up to 0.3mV in young men in early precordial leads Myocardial aneurysm Acute Pericarditis 8

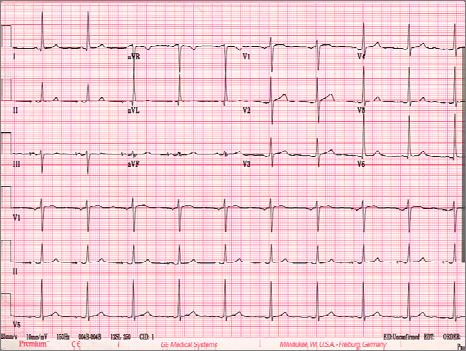
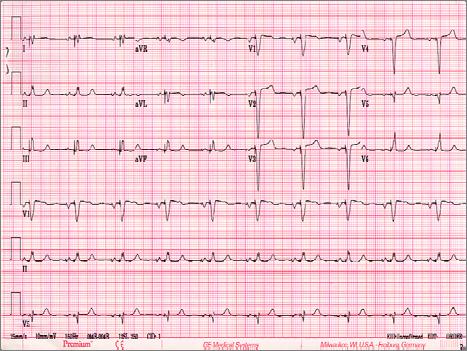
9 45 yo woman with nausea and vomiting RBBB Which of the following is not true about RBBB? A. RBBB occurs in up to 29% of AMI B. The most common cause in children is post open heart surgery for Tetralogy of Fallot repair C. Post MI patients with persistent RBBB are at the same risk for cardiac mortality D. Transient RBBB is a complication of right heart catheterization Differential Dx of Tall R wave in V1 Definition R/S ratio > 1 in V1 or V2 RBBB RVH True Posterior MI WPW Brugada s Abnormality 9

 Hereditary bundle branch defect Autosomal")

10 65 yo Asian man who presents with recurrent syncope. Echo was normal. Brugada Syndrome Brugada Abnormality is defined as RBBB with ST elevation and occurrence of sudden cardiac death or syncope due to polymorphous VT (1990) Hereditary bundle branch defect Autosomal dominant trait with variable expression Diagnosis by EPS with procainamide stimulation TX: AICD Brugada Pattern Patterns of ST segment elevation in brugada syndrome 10
 T Wave Inversion Myocardial")

11 36 yo woman presenting to the ED with acute dyspnea. RVH 79 yo man admitted with CVA Diffuse ( Global ) T Wave Inversion Myocardial Ischemia (Evolving MI is focal) CNS event Apical HCM Pericarditis Myocarditis Takatsubo s Cardiomyopathy Cardiac metastases Carotid endarterectomy Cocaine abuse Pheochromocytoma Acute illness in women 11


12 84 yo woman with pneumonia Which of the following answers about LBBB is not true? A. LBBB can be caused by toxic, inflammatory changes, hyperkalemia, or digitalis toxicity B. In most patients with LBBB, septal wall motion abnormalities can exist without coronary artery disease C. In patients presenting to the ED with chest pain and a LBBB, the management is observe with frequent ECGs, treat pain and await enzymes D. The QRS duration is at least 0.12 seconds 32 yo woman from Viet Nam presents with dyspnea on exertion. What is the diagnosis? Biatrial Abnormality 12

13 The most likely diagnosis is: A. Primary Pulmonary Hypertension B. Atrial Septal Defect C. Ventricular Septal Defect D. Mitral Stenosis E. Aortic Stenosis Biatrial Abnormality o A large diphasic P in V 1 with the positive component > 1.5 mm and the terminal negative component reaching 1mm in amplitude, > 0.04 sec in duration or both o Tall peaked P wave (>1.5mm) in the right precordial lead and a wide notched P wave in the limb leads or lateral leads (V 5-6 ) o Increase in both the amplitude (>2.5mm) and duration(>0.12 sec) of the P wave in the limb leads Non Conducted PAC s 13


14 56 yo man presents with flu Rate-Related RBBB This ECG represents: 1. Acute Myocardial Infarction with alternating bundles 2. Sinus rhythm with PVC s 3. Ashman s Phenomenon 4. He s got more going on than a flu 5. A cardiac emergency requiring pacemaker implantation 70 yo woman admitted for weakness Giant U waves 14


15 24 yo woman with FHX of SCD presents with syncope Prolonged QTc = 498 msec 78 yo man with hx of HF presents with nausea Afib with AV Dissociation What is the most appropriate next test? 1. Serial Troponins 2. Serial CK with iso s 3. Digoxin level 4. Serum potassium level 5. I don t know 15


16 AFib with AV Dissociation AFib or AFib/Aflutter or Aflutter? AFib What is the rhythm? What is the treatment? 2 nd AVB Mobitz 1 16


17 What is the rhythm? What is the treatment? p-p pr nd AVB Mobitz 1 What is the rhythm? What is the treatment? 2 nd AVB Mobitz2 AVNRT 17


18 Supraventricular Tachycardias: Which statement is true? 1. If hemodynamically stable, acute management includes Adenosine by slow IV push 2. The majority of SVT is AVNRT 3. AVRT does not involve accessory bypass tracts 4. If the patient after adenosine converts from a narrow complex tachycardia to a wide complex tachycardia, the patient has most likely degenerated to ventricular tachycardia Slow-fast form of AVNRT Generation of ECG in Common form of AVNRT 18

19 Narrow QRS Tachy response to Adenosine Rx of Hemodynamically stable tachycardia 34 yo woman with idiopathic cardiomyopathy became dizzy and came to the ED. 19

20 Wide QRS-complex tachycardia (QRS > 120 ms) Regular or irregular? Regular Is QRS identical to that during SR? If yes, consider: Vagal maneuvers SVT and BBB or Antidromic AVRT Adenosine Previous MI or structural heart disease? If yes, VT is likely 1:1 AV relationship? Irregular Atrial Fibrillation Atrial Flutter/AT with variable conduction and a) BBB or b) Antegrade conduction via AP Yes or unknown No QRS morphology in precordial leads Next slide V rate faster than A rate VT A rate faster than V rate Atrial Tachycardia Atrial Flutter Wide QRS-complex tachycardia I Wide QRS-complex tachycardia (QRS > 120 ms) Regular 1:1 AV relationship? Previous MI or structural heart disease? If yes, VT is likely Yes or unknown QRS morphology in precordial leads Typical RBBB or LBBB = SVT Precordial leads VT Concordant No R/S pattern Onset of R to nadir > 100 ms RBBB pattern VT qr, Rs or Rr in V1 Frontal plane axis range from +90 degrees to 90 degrees LBBB pattern VT R in V1 > 30 ms R to nadir of S in V1 > 60 ms qr or qs in V6 Wide QRS-complex tachycardia II A fib with WPW 20
21 82 yo man presents with chronic fatigue. Why is he on your service? CHB The correct diagnosis is: 1. Acute anterior myocardial infarction 2. Congestive Heart Failure 3. Sick Sinus Syndrome 4. Complete Heart Block with an artifact 5. Wandering Atrial Pacemaker 82 yo man presents with chronic fatigue. Why is he on your service? CHB with Answer Artifact 21

22 75 yo AA male presents with prolonged CP nonstemi & avr Prognostic Value of Lead avr in Patients with a First Non-ST segment Elevation Acute Myocardial Infarction 70.00% 60.00% 50.00% 40.00% 30.00% 20.00% In-house Mort LM/3v CAD 10.00% 0.00% without mv > 0.1 mv Odds ratio for death in groups 2 and and 6.6 Barrabes, JA et al. Circ 2003; 108: TriFasicular Block 22

23 First Degree AV Block Generally benign Bad prognostic sign in: Bifascicular Block RBBB + LAFB RBBB + LPFB LBBB Infectious endocarditis Q: Had this patient suffered a myocardial infarction? 1. No! 2. Yes. Inferior 3. Yes. Posterior 4. Yes. Septal 5. Yes. Localization not possible due to RBBB 75 yo man presents with palpitations Blocked PAC s 23
24 24
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Blocks & Dissociations. Reading Assignment (p47-52 in Outline )
") Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
Blocks & Dissociations Reading Assignment (p47-52 in Outline ) Objectives Who are Wenckebach and Mobitz? Review SA and AV Blocks AV Dissociations: learning who s the boss and why 2 nd degree SA Block:
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
General Introduction to ECG. Reading Assignment (p2-16 in PDF Outline )
") General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
General Introduction to ECG Reading Assignment (p2-16 in PDF Outline ) Objectives 1. Practice the 5-step Method 2. Differential Diagnosis: R & L axis deviation 3. Differential Diagnosis: Poor R-wave progression
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
402 Index. B β-blockers, 4, 5 Bradyarrhythmias, 76 77
 Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Index A Acquired immunodeficiency syndrome (AIDS), 126, 163 Action potentials, 1, 5, 27 Acute coronary syndromes, 123t, 129 Adenosine, intravenous, 277 Alcohol abuse, as T wave inversion cause, 199 Aneurysm,
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Conduction Problems / Arrhythmias. Conduction
 Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
Conduction Problems / Arrhythmias Conduction Wolf-Parkinson White Syndrome (WPW) and Lown-Ganong-Levine (LGL): Atrial impulses bypass the AV node through an accessory pathway or bypass tract (bundle of
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
ECG Interpretation. Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction
 * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction") ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
ECG to save Babies ECG Interpretation Best to have a system to methodically evaluate ECG (from Dubin) * Rate * Rhythm * Axis * Intervals * Hypertrophy * Infarction Electrical Activity in the heart 5 events
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019
 THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG?
 Objectives What s in an ECG?") Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
Reading Assignment (p1-91 in Outline ) Objectives What s in an ECG? The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic
How To Think About Rhythms and Conduction
 How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
Miscellaneous Stuff Keep reading the Outline
 Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
Miscellaneous Stuff Keep reading the Outline Welcome to the 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements:
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Paediatric ECG Interpretation
 Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
Paediatric ECG Interpretation Dr Sanj Fernando (thanks to http://lifeinthefastlane.com/ecg-library/paediatric-ecginterpretation/) 3 yo boy complaining of abdominal pain and chest pain Child ECG vs Adult
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
December 2018 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)
 PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70. Sinus bradycardia with one ventricular escape (*)") 1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
1? HR: 50 bpm (Sinus) PR: 280 ms QRS: 120 ms QT: 490 ms Axis: -70 1 Sinus P waves? 2 sinus cycles The pause (2 sinus cycles) suggests that the sinus fired (?) but did not conduct to the atria (i.e., missing
Chapter 2 Practical Approach
 Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
Chapter 2 Practical Approach There are beginners in electrocardiogram (ECG) analysis who are fascinated by a special pattern (e.g., a bundle-branch block or a striking Q wave) and thereby overlook other
6/19/2018. Background Athlete s heart. Ultimate question. Applying the International Criteria for ECG
 Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Applying the International Criteria for ECG Interpretation in Athletes to a preparticipation screening program DAVE SIEBERT, MD, CAQSM ASSISTANT PROFESSOR DEPARTMENT OF FAMILY MEDICINE UNIVERSITY OF WASHINGTON
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
Dr. Schroeder has no financial relationships to disclose
 Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
Valerie A Schroeder MD MS Assistant Professor University of Kansas Medical Center READING THE WAVES- THE HEART S ELECTRICAL MESSAGE FINANCIAL DISCLOSURE Dr. Schroeder has no financial relationships to
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
Junctional Premature Contraction (JPC)
") Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
Where s the PAC? Junctional Premature Contraction (JPC) A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern.
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
Electrocardiography Abnormalities (Arrhythmias) 7. Faisal I. Mohammed, MD, PhD
 7. Faisal I. Mohammed, MD, PhD") Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
Electrocardiography Abnormalities (Arrhythmias) 7 Faisal I. Mohammed, MD, PhD 1 Causes of Cardiac Arrythmias Abnormal rhythmicity of the pacemaker Shift of pacemaker from sinus node Blocks at different
, David Stultz, MD.
 http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
http://www.dilbert.com EKG Rounds Handouts available at http://www.drstultz.com January 5, 2004 David Stultz, MD Cardiology Fellow, PGY 4 Overview of Topics How to read an EKG Normal EKG Determination
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
2017 EKG Workshop Basic. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
2017 EKG Workshop Basic Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part I - Objectives Discuss a systematic approach to EKG interpretation
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Ben Taylor, PhD, PA-C
 Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Ben Taylor, PhD, PA-C The patient is a 23-year-old white male with a history of polysubstance abuse who was found unresponsive, last seen the day before. Classic signs of systemic hypothermia with prominent
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
January 2019 Tracings
 Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Tracings Tracing 1 Tracing 4 Tracing 1 Answer Tracing 4 Answer Tracing 2 Tracing 5 Tracing 2 Answer Tracing 5 Answer Tracing 3 Tracing 6 Tracing 3 Answer Tracing 6 Answer Questions? Contact Dr. Nelson
Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida
 S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
S306- Pediatric Electrocardiography: A Potpourri Ronald J. Kanter, MD Director, Electrophysiology Miami Children s Hospital Professor Emeritus, Duke University Miami, Florida Disclosure of Relevant Relationship
EKG Practice. Homan Wai
 EKG Practice Homan Wai Objectives Learn EKG by Examples Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Details
EKG Practice Homan Wai Objectives Learn EKG by Examples Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Learn by repetition Details
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
Rapid Fire ECG Challenge: Putting Your Interpretation Skills to the Test. Evert Torrejon, MD Sociedad Peruana Cardiologia Presenter
 Rapid Fire ECG Challenge: Putting Your Interpretation Skills to the Test Evert Torrejon, MD Sociedad Peruana Cardiologia Presenter Male 36 years old, athlete, with prior to start swimming, gastric discomfort
Rapid Fire ECG Challenge: Putting Your Interpretation Skills to the Test Evert Torrejon, MD Sociedad Peruana Cardiologia Presenter Male 36 years old, athlete, with prior to start swimming, gastric discomfort
Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst
 Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst 1. Patient K.P., male, 68 years Fatigue Exercise intolerance for
Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst 1. Patient K.P., male, 68 years Fatigue Exercise intolerance for
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
ECG interpretation basics
 ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
ECG interpretation basics Michał Walczewski, MD Krzysztof Ozierański, MD 21.03.18 Electrical conduction system of the heart Limb leads Precordial leads 21.03.18 Precordial leads Precordial leads 21.03.18
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
Making Sense of Those Little Lines Advanced ECG Interpretation
 Making Sense of Those Little Lines Advanced ECG Interpretation Cara Solodky-Hardy, ND, ANP-BC, AACC MD24 House Call Cardiology My patients www.ecglibrary.com Image Sources The Alan E. Lindsay Ecg Learning
Making Sense of Those Little Lines Advanced ECG Interpretation Cara Solodky-Hardy, ND, ANP-BC, AACC MD24 House Call Cardiology My patients www.ecglibrary.com Image Sources The Alan E. Lindsay Ecg Learning
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC
, FACC") Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants
 Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
Relax and Learn at the FARM 2012: Session 8: 12 Lead ECG 401: ECG Variants A Ship in the Harbor is Safe But that is not what ships are built for. Karen Marzlin DNP, RN, CCNS, CCRN-CMC, CHFN Cardiovascular
ECG Practice Strips Discussion part 1:
 ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG Practice Strips Discussion part 1: The first 20 strips are for teaching various abnormalities of the morphology of the waves of the ECG. Strips 21 and following are for teaching some abnormalities
ECG INTERPRETATION MANUAL
 Lancashire & South Cumbria Cardiac Network ECG INTERPRETATION MANUAL THE NORMAL ECG Lancashire And South Cumbria Cardiac Physiologist Training Manual THE NORMAL ECG E.C.G CHECKLIST 1) Name, Paper Speed,
Lancashire & South Cumbria Cardiac Network ECG INTERPRETATION MANUAL THE NORMAL ECG Lancashire And South Cumbria Cardiac Physiologist Training Manual THE NORMAL ECG E.C.G CHECKLIST 1) Name, Paper Speed,