Supplementary Online Content
|
|
|
- Lorraine Freeman
- 5 years ago
- Views:
Transcription
1 Supplementary Online Content McEvoy JW, Chen Y, Ndumele CE, et al. Six-year change in high-sensitivity cardiac troponin T and risk of subsequent coronary heart disease, heart failure, and death. JAMA Cardiol. Published online June 8, doi: /jamacardio etable 1. Study Population for the Primary Analysis Evaluating the Association of hs-ctnt Change Between ARIC Visit 2 and Visit 4 With subsequent CHD, HF, or Death Occurring After Visit 4 etable 2. Crude Incidence Rates (per 1000 Person-years) and Adjusted* Hazard Ratios (95% CIs) for Incident Coronary Heart Disease, Heart Failure Hospitalization, or Death According To Sex-Specific Categories of 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (N=8838) etable 3. Adjusted* Hazard Ratios (95% CIs) for Incident Coronary Heart Disease, Heart Failure, or Death According to Categories of 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) With and Without Further Adjustment for Either Change in NT-proBNP or Visit 4 hs-ctnt etable 4. Crude Incidence Rates (per 1000 Person-years) and Adjusted* Hazard Ratios (95% CIs) for Incident Coronary Heart Disease, Heart Failure Hospitalization, or Death According to 25% Relative Change of 6-Year Change in hs-ctnt etable 5. Net Reclassification Improvement for Coronary Heart Disease, Heart Failure and Death With the Addition of the First and Second hs-ctnt Values to a Traditional Risk Factor Prediction Model etable 6. Adjusted* Hazard Ratios (95% CIs) for Heart Failure Subtypes (HFrEF and HFpEF) Adjudicated After 2005 According to Categories of 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt): Full Model With and Without Further Adjustment for 6-Year Change in NT-proBNP efigure 1. Cumulative Survival Free of Coronary Heart Disease, Heart Failure Hospitalization, or Death Stratified by Categories of Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) During 6 Years (Incident Detectable, Incident Elevated, or Percent Relative Change*) efigure 2. Restricted Cubic Splines for Adjusted* Hazard Ratios (95% CIs) of Incident Coronary Heart Disease (CHD), Heart Failure (HF) Hospitalization, or Death According to Absolute 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in ng/l) efigure 3. Restricted Cubic Splines for Adjusted* Hazard Ratios (95% CIs) of (a) Incident Coronary Heart Disease (CHD) (B) Heart Failure (HF) Hospitalization, or (C) Death According to Absolute 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in ng/l) and Stratified by Visit 2 Concentration Groups (<5 ng/l, 5-13 ng/l, and 14 ng/l) efigure 4. Restricted Cubic Splines for Adjusted* Hazard Ratios (95% CIs) of Incident HFrEF or HFpEF according to Absolute 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in ng/l) This supplementary material has been provided by the authors to give readers additional information about their work.
2 etable 1. Study Population for the Primary Analysis Evaluating the Association of hs-ctnt Change Between ARIC Visit 2 and Visit 4 With subsequent CHD, HF, or Death Occurring After Visit 4 Exclusion Process Exclusion Population Participates at visit Prevalent CHD and HF at or prior to visit Missing model covariates at visit Missing hs-ctnt data at either visit 2 or visit Missing follow-up information for events after visit Non black or white, race-center exclusion Study population 8838
3 etable 2. Crude Incidence Rates (per 1000 Person-years) and Adjusted* Hazard Ratios (95% CIs) for Incident Coronary Heart Disease, Heart Failure Hospitalization, or Death According To Sex-Specific Categories of 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (N=8838) Outcomes Absolute hs-ctnt change according to Gender MEN Incident Elevated (Baseline <24ng/L, Follow-up 24ng/L) WOMEN Incident Elevated (Baseline <14ng/L, Follow-up 14ng/L) No (N=3500) Yes (N=83) No (N=5040) Yes (N=108) Heart Failure n=367 n=31 n=489 n=41 Incidence Rate 8.3 ( ) 40.1 ( ) 7.4 ( ) 39.3 ( ) Demographic Model* ( ) ( ) ( ) ( ) Coronary Heart Disease n=652 n=29 n=416 n=23 Incidence Rate 15.9( ) 39.4 ( ) 6.3 ( ) 20.8 ( ) Demographic Model* ( ) ( ) ( ) ( ) Death n=870 n=45 n=791 n=53 Incidence Rate 19.2( ) 52.4 ( ) 11.6 ( ) 43.9 ( ) Demographic Model* ( ) ( ) ( ) ( ) * Demographic Model- Adjusted for age, race-center; Full Model- Adjusted for age,, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterollowering medication (yes or no), estimated GFR (ml/min/1.73m2), and left ventricular hypertrophy (yes or no, by Cornell criteria).
4 etable 3. Adjusted* Hazard Ratios (95% CIs) for Incident Coronary Heart Disease, Heart Failure, or Death According to Categories of 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) With and Without Further Adjustment for Either Change in NT-proBNP or Visit 4 hs-ctnt Outcomes Absolute hs-ctnt change among all participants Incident Detectable (Baseline <5ng/L, Follow-up 5ng/L) No (N=3888) Yes (N=2152) Incident Elevated (Baseline <14ng/L, Follow-up 14ng/L) No (N=8155) Relative change among persons with measurable hs-ctnt values >50% Decrease Change 50% >50% Increase Yes (N=443) (N=74) (N=2227) (N=1147) Heart Failure n=235 n=260 n=761 n=134 n=10 n=309 n=234 Additional adjustments Coronary Heart Disease Additional adjustments 1.96 ( ) 1.86 ( ) 2.78 ( ) 2.54 ( ) 0.49 ( ) 0.94 ( ) 1.60 ( ) 1.34 ( ) n=330 n=301 n=969 n=119 n=9 n=374 n= ( ) 1.37 ( ) 1.75 ( ) 1.68 ( ) 0.47 ( ) 0.79 ( ) 1.28 ( ) 1.14 ( ) Death n=508 n=486 n=1496 n=209 n=17 n=584 n=392 Additional adjustments 1.50 ( ) 1.46 ( ( ) 1.97 ( ) 0.57 ( ) 0.89 ( ( ) 1.23 ( ) 1.68) 1.46) * Full Model- Adjusted for age, sex, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterol-lowering medication (yes or no), estimated GFR (ml/min/1.73m2), and left ventricular hypertrophy (yes or no, by Cornell criteria). Sample (N=3448) includes only those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Relative change is calculated as a percent of baseline hs-ctnt. The full model for this relative change exposure is further adjusted for visit 2 hsctnt. Additional adjustment is for 1) continuous absolute change in NT-proBNP (in pg/ml) between visits 2 and 4 for the incident detectable and incident elevated models and 2) both adjusting for absolute change in NT-proBNP and for visit 4 hs-ctnt instead of visit 2 hs-ctnt for the relative change model.
5 etable 4. Crude Incidence Rates (per 1000 Person-years) and Adjusted* Hazard Ratios (95% CIs) for Incident Coronary Heart Disease, Heart Failure Hospitalization, or Death According to 25% Relative Change of 6-Year Change in hs-ctnt Outcomes Relative change among persons with measurable hs-ctnt values >25% Decrease Change 25% >25% Increase (N=414) (N=1377) (N=1657) Heart Failure n=50 n=185 n=318 Incidence Rate Demographic Model* 0.88 ( ) 1.53 ( ) 0.83 ( ) 1.54 ( ) Coronary Heart Disease n=69 n=226 n=327 Incidence Rate Demographic Model* 1.07 ( ) 1.24 ( ) 1.04 ( ) 1.21 ( ) Death n=96 n=357 n=540 Incidence Rate Demographic Model* 0.93 ( ) 1.29 ( ) 0.86 ( ) 1.29 ( ) * Demographic Model- Adjusted for age, sex, race-center; Full Model- Adjusted for age, sex, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterol-lowering medication (yes or no), estimated GFR (ml/min/1.73m2), left ventricular hypertrophy (yes or no, by Cornell criteria) and visit 2 hs-ctnt. Relative change sample (N=3448) only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Relative change is calculated as a percent of baseline hs-ctnt.
6 etable 5. Net Reclassification Improvement for Coronary Heart Disease, Heart Failure and Death With the Addition of the First and Second hs-ctnt Values to a Traditional Risk Factor Prediction Model Continuous NRI Coronary heart disease Heart failure All-cause mortality Model Overall NRI p value Overall NRI p value Overall NRI p value Model 1 (vs. base model*) -2% % % Model 2 (vs. model 1) +7% % % *Base model is adjusted for age, sex, race-center, smoking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDLcholesterol (mg/dl), HDL-cholesterol (mg/dl) *Model 1 is base model + v4 hs-ctnt. *Model 2 is base model + v4 hs-ctnt +v2 hs-ctnt.
7 etable 6. Adjusted* Hazard Ratios (95% CIs) for Heart Failure Subtypes (HFrEF and HFpEF) Adjudicated After 2005 According to Categories of 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt): Full Model With and Without Further Adjustment for 6-Year Change in NT-proBNP Heart Failure Subtypes Absolute hs-ctnt change among all participants Incident Detectable (Baseline <5ng/L, Follow-up 5ng/L) No (n=3599) Yes (n=1867) Incident Elevated (Baseline <14ng/L, Follow-up 14ng/L) No (n=7306) Relative change among persons with measurable hs-ctnt values >50% Decrease Change 50% >50% Increase Yes (n=286) (n=71) (n=2038) (n=996) HFrEF n=88 n=72 n=256 n=30 n=5 n=121 n=77 Additional adjustment for 6-year change in NT-proBNP 1.54 ( ) 1.43 ( ) 2.43 ( ) 2.31 ( ) 0.85 ( ) 0.87 ( ) 1.26 ( ) 1.24 ( ) HFpEF n=69 n=67 n=199 n=17 n=3 n=76 n=46 Additional adjustment for 6-year change in NT-proBNP 1.72 ( ) 1.68 ( ) 1.80 ( ) 1.70 ( ) 1.06 ( ) 1.10 ( ) 1.16 ( ) 1.09 ( ) * Demographic Model- Adjusted for age, sex, race-center; Full Model- Adjusted for age, sex, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterol-lowering medication (yes or no), estimated GFR (ml/min/1.73m2), and left ventricular hypertrophy (yes or no, by Cornell criteria). Sample (N=3448) only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Relative change is calculated as a percent of baseline hs-ctnt. The full model for this exposure is further adjusted for visit 2 hs-ctnt.

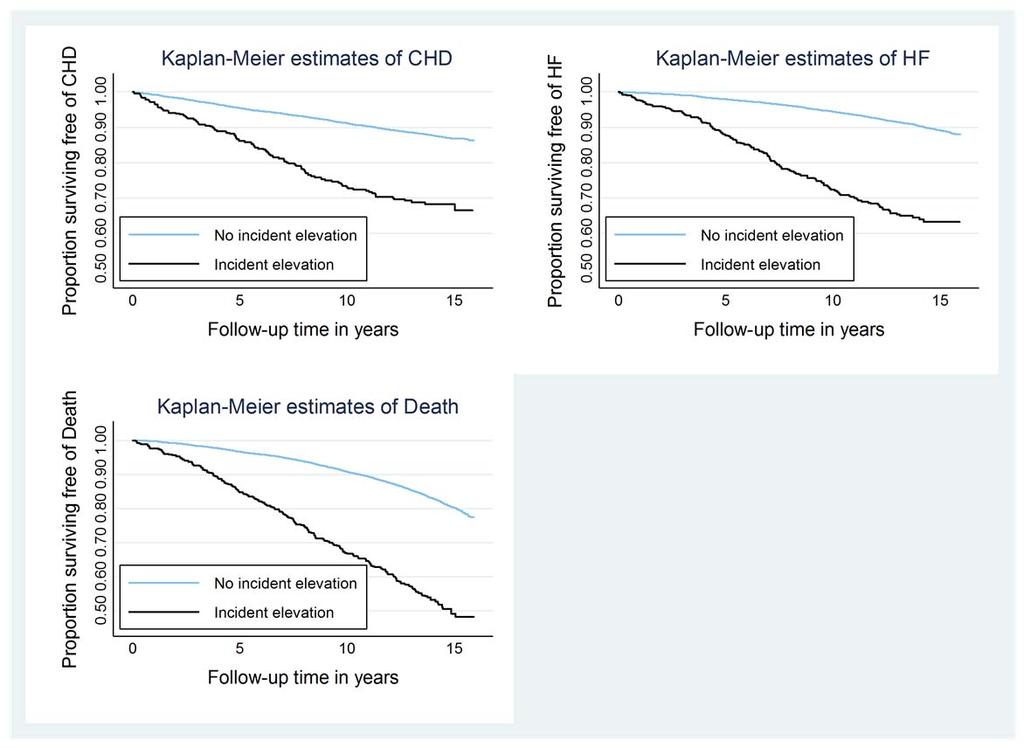
8 efigure 1. Cumulative Survival Free of Coronary Heart Disease, Heart Failure Hospitalization, or Death Stratified by Categories of Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) During 6 Years (Incident Detectable, Incident Elevated, or Percent Relative Change*)
9
 only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits.")
10 *Incident Detectable=Baseline <5ng/L, Follow-up 5ng/L; Incident Elevated=Baseline <14ng/L, Follow-up 14ng/L. Percent relative change sample (N=3448) only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Relative change is calculated as a percent of baseline hs-ctnt
 of Incident Coronary Heart Disease (CHD), Heart Failure (HF) Hospitalization, or Death According to Absolute 6-Year Change in")
, systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl),")
11 efigure 2. Restricted Cubic Splines for Adjusted* Hazard Ratios (95% CIs) of Incident Coronary Heart Disease (CHD), Heart Failure (HF) Hospitalization, or Death According to Absolute 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in ng/l) *Adjusted for age, sex, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterol-lowering medication (yes or no), estimated GFR (ml/min/1.73m2), left ventricular hypertrophy (yes or no, by Cornell criteria), and visit 2 hs-ctnt (ng/l). Sample (N=3448) only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Background histogram displays the frequency distribution of hs-ctnt change in the sample. Splines are centered at the median of hs-ctnt change and are truncated at the 1 st and 99 th percentile.
 of (a) Incident Coronary Heart Disease (CHD) (B) Heart Failure (HF) Hospitalization, or (C) Death According to Absolute")
12 efigure 3. Restricted Cubic Splines for Adjusted* Hazard Ratios (95% CIs) of (a) Incident Coronary Heart Disease (CHD) (B) Heart Failure (HF) Hospitalization, or (C) Death According to Absolute 6-Year Change in High- Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in ng/l) and Stratified by Visit 2 Concentration Groups (<5 ng/l, 5-13 ng/l, and 14 ng/l) A- CHD

13 B- Heart Failure
14 C- Death (All-cause Mortality) *Adjusted for age, sex, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterol-lowering medication (yes or no), estimated GFR (ml/min/1.73m2), and left ventricular hypertrophy (yes or no, by Cornell criteria). Sample (N=3448) only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Background histogram displays the frequency distribution of hs-ctnt change in the sample. Splines are centered at the median of hs-ctnt change and are truncated at the 1 st and 99 th percentile.
 of Incident HFrEF or HFpEF according to Absolute 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in")
, current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current")
15 efigure 4. Restricted Cubic Splines for Adjusted* Hazard Ratios (95% CIs) of Incident HFrEF or HFpEF according to Absolute 6-Year Change in High-Sensitivity Cardiac Troponin T (hs-ctnt) (per Unit Increase in ng/l) - HFREF - HFPEF *Adjusted for age, sex, race-center, body mass index (kg/m3), C-reactive protein (mg/l), smoking (current; former; never), drinking (current; former; never), systolic blood pressure (mmhg), current use of blood pressure-lowering medication (yes or no), diagnosed diabetes (yes or no), LDL-cholesterol (mg/dl), HDL-cholesterol (mg/dl), triglycerides (mg/dl), and current use of cholesterol-lowering medication (yes or no), estimated GFR (ml/min/1.73m2), left ventricular hypertrophy (yes or no, by Cornell criteria), and visit 2 hs-ctnt (ng/l). Sample (N=3448) only includes those who have measurable hs-ctnt values ( 3 ng/l) at both visits. Background histogram displays the frequency distribution of hs-ctnt change in the sample. Splines are centered at the median of hs-ctnt change and are truncated at the 1 st and 99 th percentile.
Supplementary Online Content
 Supplementary Online Content Clair C, Rigotti NA, Porneala B, et al. Association of smoking cessation and weight change with cardiovascular disease among people with and without diabetes. JAMA. doi:10.1001/jama.2013.1644.
Supplementary Online Content Clair C, Rigotti NA, Porneala B, et al. Association of smoking cessation and weight change with cardiovascular disease among people with and without diabetes. JAMA. doi:10.1001/jama.2013.1644.
Supplemental Table S2: Subgroup analysis for IL-6 with BMI in 3 groups
 Supplemental Table S1: Unadjusted and Adjusted Hazard Ratios for Diabetes Associated with Baseline Factors Considered in Model 3 SMART Participants Only Unadjusted Adjusted* Baseline p-value p-value Covariate
Supplemental Table S1: Unadjusted and Adjusted Hazard Ratios for Diabetes Associated with Baseline Factors Considered in Model 3 SMART Participants Only Unadjusted Adjusted* Baseline p-value p-value Covariate
Long-term prognostic value of N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) changes within one year in patients with coronary heart disease
 changes within one year in patients with coronary heart disease") Long-term prognostic value of N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) changes within one year in patients with coronary heart disease D. Dallmeier 1, D. Rothenbacher 2, W. Koenig 1, H. Brenner
Long-term prognostic value of N-Terminal Pro-Brain Natriuretic Peptide (NT-proBNP) changes within one year in patients with coronary heart disease D. Dallmeier 1, D. Rothenbacher 2, W. Koenig 1, H. Brenner
Supplementary Online Content
 Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients with Stable Coronary Heart Disease: KAROLA Study 8 Year FU
 ESC Congress 2011 Paris, France, August 27-31 KAROLA Session: Prevention: Are biomarkers worth their money? Abstract # 84698 High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients
ESC Congress 2011 Paris, France, August 27-31 KAROLA Session: Prevention: Are biomarkers worth their money? Abstract # 84698 High-sensitivity Troponin T Predicts Recurrent Cardiovascular Events in Patients
Know Your Number Aggregate Report Single Analysis Compared to National Averages
 Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Supplementary Online Content
 Supplementary Online Content Malik S, Zhao Y, Budoff M, et al. Coronary artery calcium score for long-term risk classification in individuals with type 2 diabetes and metabolic syndrome from the Multi-Ethnic
Supplementary Online Content Malik S, Zhao Y, Budoff M, et al. Coronary artery calcium score for long-term risk classification in individuals with type 2 diabetes and metabolic syndrome from the Multi-Ethnic
Supplementary Online Content
 Supplementary Online Content Pokharel Y, Tang F, Jones PG, et al. Adoption of the 2013 American College of Cardiology/American Heart Association Cholesterol Management Guideline in cardiology practices
Supplementary Online Content Pokharel Y, Tang F, Jones PG, et al. Adoption of the 2013 American College of Cardiology/American Heart Association Cholesterol Management Guideline in cardiology practices
Supplementary Online Content
 Supplementary Online Content Nikolova AP, Hitzeman TC, Baum R, et al. Association of a novel diagnostic biomarker, the plasma cardiac bridging integrator 1 score, with heart failure with preserved ejection
Supplementary Online Content Nikolova AP, Hitzeman TC, Baum R, et al. Association of a novel diagnostic biomarker, the plasma cardiac bridging integrator 1 score, with heart failure with preserved ejection
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Troponin Assessment. Does it Carry Clinical Message? Stefan Blankenberg. University Heart Center Hamburg
 Biomarkers for Optimal Management of Heart Failure Troponin Assessment Does it Carry Clinical Message? Stefan Blankenberg University Heart Center Hamburg Congress of the European Society of Cardiology
Biomarkers for Optimal Management of Heart Failure Troponin Assessment Does it Carry Clinical Message? Stefan Blankenberg University Heart Center Hamburg Congress of the European Society of Cardiology
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Supplementary Online Content. Abed HS, Wittert GA, Leong DP, et al. Effect of weight reduction and
 1 Supplementary Online Content 2 3 4 5 6 Abed HS, Wittert GA, Leong DP, et al. Effect of weight reduction and cardiometabolic risk factor management on sympton burden and severity in patients with atrial
1 Supplementary Online Content 2 3 4 5 6 Abed HS, Wittert GA, Leong DP, et al. Effect of weight reduction and cardiometabolic risk factor management on sympton burden and severity in patients with atrial
A: Epidemiology update. Evidence that LDL-C and CRP identify different high-risk groups
 A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
A: Epidemiology update Evidence that LDL-C and CRP identify different high-risk groups Women (n = 27,939; mean age 54.7 years) who were free of symptomatic cardiovascular (CV) disease at baseline were
Supplementary Online Content
 Supplementary Online Content Pedersen SB, Langsted A, Nordestgaard BG. Nonfasting mild-to-moderate hypertriglyceridemia and risk of acute pancreatitis. JAMA Intern Med. Published online November 7, 2016.
Supplementary Online Content Pedersen SB, Langsted A, Nordestgaard BG. Nonfasting mild-to-moderate hypertriglyceridemia and risk of acute pancreatitis. JAMA Intern Med. Published online November 7, 2016.
Supplementary Online Content
 Supplementary Online Content Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011;305(15):1553-1559. eequation. Applying the
Supplementary Online Content Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011;305(15):1553-1559. eequation. Applying the
Supplementary Online Content
 Supplementary Online Content Aung T, Halsey J, Kromhout D, et al. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77 917 individuals.
Supplementary Online Content Aung T, Halsey J, Kromhout D, et al. Associations of omega-3 fatty acid supplement use with cardiovascular disease risks: meta-analysis of 10 trials involving 77 917 individuals.
Correlation of novel cardiac marker
 Correlation of novel cardiac marker and mortality in EGAT population. Soluble ST2 hscrp Poh Chanyavanich, MD SukitYamwong, MD Piyamitr Sritara, MD Ramathibodi hospital Background hscrp - the most widely
Correlation of novel cardiac marker and mortality in EGAT population. Soluble ST2 hscrp Poh Chanyavanich, MD SukitYamwong, MD Piyamitr Sritara, MD Ramathibodi hospital Background hscrp - the most widely
Supplementary Table 1. Baseline Characteristics by Quintiles of Systolic and Diastolic Blood Pressures
 Supplementary Data Supplementary Table 1. Baseline Characteristics by Quintiles of Systolic and Diastolic Blood Pressures Quintiles of Systolic Blood Pressure Quintiles of Diastolic Blood Pressure Q1 Q2
Supplementary Data Supplementary Table 1. Baseline Characteristics by Quintiles of Systolic and Diastolic Blood Pressures Quintiles of Systolic Blood Pressure Quintiles of Diastolic Blood Pressure Q1 Q2
How will new high sensitive troponins affect the criteria?
 How will new high sensitive troponins affect the criteria? Hugo A Katus MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Even more sensitive: The new
How will new high sensitive troponins affect the criteria? Hugo A Katus MD Abteilung Innere Medizin III Kardiologie, Angiologie, Pulmologie Universitätsklinikum Heidelberg Even more sensitive: The new
HIGH SENSITIVITY CARDIAC TROPONIN-T IS ASSOCIATED WITH INCIDENT HYPERTENSION. John W. McEvoy
 HIGH SENSITIVITY CARDIAC TROPONIN-T IS ASSOCIATED WITH INCIDENT HYPERTENSION by John W. McEvoy A thesis submitted to Johns Hopkins University in conformity with the requirements for the degree of Master
HIGH SENSITIVITY CARDIAC TROPONIN-T IS ASSOCIATED WITH INCIDENT HYPERTENSION by John W. McEvoy A thesis submitted to Johns Hopkins University in conformity with the requirements for the degree of Master
Know Your Number Aggregate Report Comparison Analysis Between Baseline & Follow-up
 Know Your Number Aggregate Report Comparison Analysis Between Baseline & Follow-up... Study Population: 340... Total Population: 500... Time Window of Baseline: 09/01/13 to 12/20/13... Time Window of Follow-up:
Know Your Number Aggregate Report Comparison Analysis Between Baseline & Follow-up... Study Population: 340... Total Population: 500... Time Window of Baseline: 09/01/13 to 12/20/13... Time Window of Follow-up:
Supplementary Online Content
 Supplementary Online Content Ebbing M, Bønaa KH, Nygård O, et al. Cancer incidence and mortality after treatment with folic acid and vitamin B 1. JAMA. 9;3(19):119-1. etable 1. Circulating Levels of B
Supplementary Online Content Ebbing M, Bønaa KH, Nygård O, et al. Cancer incidence and mortality after treatment with folic acid and vitamin B 1. JAMA. 9;3(19):119-1. etable 1. Circulating Levels of B
Supplementary Online Content
 Supplementary Online Content Åsvold BO, Vatten LJ, Bjøro T, et al; Thyroid Studies Collaboration. Thyroid function within the normal range and risk of coronary heart disease: an individual participant
Supplementary Online Content Åsvold BO, Vatten LJ, Bjøro T, et al; Thyroid Studies Collaboration. Thyroid function within the normal range and risk of coronary heart disease: an individual participant
Learning Objectives. Predicting and Preventing Cardiovascular Disease. ACC/AHA Cholesterol Guidelines Key differences vs ATP III
 Presenter Disclosure Information 10:30 11:15am Predicting and Preventing Cardiovascular Disease: Can we put the Cardiologist out of business? The following relationships exist related to this presentation:
Presenter Disclosure Information 10:30 11:15am Predicting and Preventing Cardiovascular Disease: Can we put the Cardiologist out of business? The following relationships exist related to this presentation:
Supplementary Online Content
 Supplementary Online Content Den Ruijter HM, Peters SA, Anderson TJ, et al. Common carotid intimamedia thickness measurements in cardiovascular risk prediction. JAMA. doi:10.1001/jama.2012.9630. etable
Supplementary Online Content Den Ruijter HM, Peters SA, Anderson TJ, et al. Common carotid intimamedia thickness measurements in cardiovascular risk prediction. JAMA. doi:10.1001/jama.2012.9630. etable
(n=6279). Continuous variables are reported as mean with 95% confidence interval and T1 T2 T3. Number of subjects
. Continuous variables are reported as mean with 95% confidence interval and T1 T2 T3. Number of subjects") Table 1. Distribution of baseline characteristics across tertiles of OPG adjusted for age and sex (n=6279). Continuous variables are reported as mean with 95% confidence interval and categorical values
Table 1. Distribution of baseline characteristics across tertiles of OPG adjusted for age and sex (n=6279). Continuous variables are reported as mean with 95% confidence interval and categorical values
Supplementary table 1 Demographic and clinical characteristics of participants by paraoxonase-1 (PON-1) gene polymorphisms
 gene polymorphisms") Supplementary table 1 Demographic and clinical characteristics of participants by paraoxonase-1 (PON-1) gene polymorphisms QQ QR/RR n = 36 n = 80 Men (%) 20 (55) 54 (67) 0.216 Age (years) 57 ± 10 56 ±
Supplementary table 1 Demographic and clinical characteristics of participants by paraoxonase-1 (PON-1) gene polymorphisms QQ QR/RR n = 36 n = 80 Men (%) 20 (55) 54 (67) 0.216 Age (years) 57 ± 10 56 ±
Supplementary Online Content
 Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Pitavastatin 4 mg vs. Pravastatin 40 mg in HIV Dyslipidemia: Post- Hoc Analysis of the INTREPID Trial Based on the Independent CHD Risk Factor for Age
 Pitavastatin 4 mg vs. Pravastatin 40 mg in HIV Dyslipidemia: Post- Hoc Analysis of the INTREPID Trial Based on the Independent CHD Risk Factor for Age Craig A. Sponseller, Masaya Tanahashi, Hideki Suganami,
Pitavastatin 4 mg vs. Pravastatin 40 mg in HIV Dyslipidemia: Post- Hoc Analysis of the INTREPID Trial Based on the Independent CHD Risk Factor for Age Craig A. Sponseller, Masaya Tanahashi, Hideki Suganami,
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
SMARTool clinical and biohumoral results. Chiara Caselli IFC-CNR
 SMARTool clinical and biohumoral results Chiara Caselli IFC-CNR SMARTool Flow chart EVINCI and ARTreat Populations SMARTool: WP1 and WP2 WP1 Objective: To collect retrospective EVINCI clinical and imaging
SMARTool clinical and biohumoral results Chiara Caselli IFC-CNR SMARTool Flow chart EVINCI and ARTreat Populations SMARTool: WP1 and WP2 WP1 Objective: To collect retrospective EVINCI clinical and imaging
Improving Diagnostic, Prognostic & Therapeutic Biomarkers in Heart Disease. Professor Mark Richards Medicine, University of Otago, Christchurch
 Improving Diagnostic, Prognostic & Therapeutic Biomarkers in Heart Disease Professor Mark Richards Medicine, University of Otago, Christchurch BNP / NT-ProBNP H 2 N 1 Pro-BNP Cardiomyocyte 76 77 108 COOH
Improving Diagnostic, Prognostic & Therapeutic Biomarkers in Heart Disease Professor Mark Richards Medicine, University of Otago, Christchurch BNP / NT-ProBNP H 2 N 1 Pro-BNP Cardiomyocyte 76 77 108 COOH
Supplementary Online Content
 Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
Supplementary Online Content Valle JA, Tamez H, Abbott JD, et al. Contemporary use and trends in unprotected left main coronary artery percutaneous coronary intervention in the United States: an analysis
ARIC Manuscript Proposal # PC Reviewed: 2/10/09 Status: A Priority: 2 SC Reviewed: Status: Priority:
 ARIC Manuscript Proposal # 1475 PC Reviewed: 2/10/09 Status: A Priority: 2 SC Reviewed: Status: Priority: 1.a. Full Title: Hypertension, left ventricular hypertrophy, and risk of incident hospitalized
ARIC Manuscript Proposal # 1475 PC Reviewed: 2/10/09 Status: A Priority: 2 SC Reviewed: Status: Priority: 1.a. Full Title: Hypertension, left ventricular hypertrophy, and risk of incident hospitalized
Central pressures and prediction of cardiovascular events in erectile dysfunction patients
 Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Central pressures and prediction of cardiovascular events in erectile dysfunction patients N. Ioakeimidis, K. Rokkas, A. Angelis, Z. Kratiras, M. Abdelrasoul, C. Georgakopoulos, D. Terentes-Printzios,
Statin therapy in patients with Mild to Moderate Coronary Stenosis by 64-slice Multidetector Coronary Computed Tomography
 Statin therapy in patients with Mild to Moderate Coronary Stenosis by 64-slice Multidetector Coronary Computed Tomography Hyo Eun Park 1, Eun-Ju Chun 2, Sang-Il Choi 2, Soyeon Ahn 2, Hyung-Kwan Kim 3,
Statin therapy in patients with Mild to Moderate Coronary Stenosis by 64-slice Multidetector Coronary Computed Tomography Hyo Eun Park 1, Eun-Ju Chun 2, Sang-Il Choi 2, Soyeon Ahn 2, Hyung-Kwan Kim 3,
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY. Harvey D White on behalf of The STABILITY Investigators
 STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
Är dagens troponinmetoder tillräckligt känsliga?
 Är dagens troponinmetoder tillräckligt känsliga? Per Venge, MD PhD Professor Department of Medical Sciences Uppsala University and Department of Clinical Chemistry and Pharmacology University Hospital
Är dagens troponinmetoder tillräckligt känsliga? Per Venge, MD PhD Professor Department of Medical Sciences Uppsala University and Department of Clinical Chemistry and Pharmacology University Hospital
ARIC Manuscript Proposal #2099. PC Reviewed: 3/12/13 Status: A Priority: 2 SC Reviewed: Status: Priority:
 ARIC Manuscript Proposal #2099 PC Reviewed: 3/12/13 Status: A Priority: 2 SC Reviewed: Status: Priority: 1. a. Full Title: Utility of biomarker panel, hstnt, NT-proBNP, and cystatin C to prediction of
ARIC Manuscript Proposal #2099 PC Reviewed: 3/12/13 Status: A Priority: 2 SC Reviewed: Status: Priority: 1. a. Full Title: Utility of biomarker panel, hstnt, NT-proBNP, and cystatin C to prediction of
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Supplementary Online Content
 Supplementary Online Content Leibowitz M, Karpati T, Cohen-Stavi CJ, et al. Association between achieved low-density lipoprotein levels and major adverse cardiac events in patients with stable ischemic
Supplementary Online Content Leibowitz M, Karpati T, Cohen-Stavi CJ, et al. Association between achieved low-density lipoprotein levels and major adverse cardiac events in patients with stable ischemic
Supplementary Online Content
 Supplementary Online Content James MT, Neesh P, Hemmelgarn BR, et al. Derivation and external validation of prediction models for advanced chronic kidney disease following acute kidney injury. JAMA. doi:10.1001/jama.2017.16326
Supplementary Online Content James MT, Neesh P, Hemmelgarn BR, et al. Derivation and external validation of prediction models for advanced chronic kidney disease following acute kidney injury. JAMA. doi:10.1001/jama.2017.16326
Supplementary Online Content
 Supplementary Online Content Xu X, Qin X, Li Y, et al. Efficacy of folic acid therapy on the progression of chronic kidney disease: the Renal Substudy of the China Stroke Primary Prevention Trial. JAMA
Supplementary Online Content Xu X, Qin X, Li Y, et al. Efficacy of folic acid therapy on the progression of chronic kidney disease: the Renal Substudy of the China Stroke Primary Prevention Trial. JAMA
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
Supplementary Online Content
 Supplementary Online Content Yang Q, Zhang Z, Gregg EW, Flanders WD, Merritt R, Hu FB. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern Med. Published online February
Supplementary Online Content Yang Q, Zhang Z, Gregg EW, Flanders WD, Merritt R, Hu FB. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern Med. Published online February
Supplemental table 1. Dietary sources of protein among 2441 men from the Kuopio Ischaemic Heart Disease Risk Factor Study MEAT DAIRY OTHER ANIMAL
 ONLINE DATA SUPPLEMENT 1 SUPPLEMENTAL MATERIAL Pork Bacon Turkey Kidney Cream Cottage cheese Mutton and lamb Game (elk, reindeer) Supplemental table 1. Dietary sources of protein among 2441 men from the
ONLINE DATA SUPPLEMENT 1 SUPPLEMENTAL MATERIAL Pork Bacon Turkey Kidney Cream Cottage cheese Mutton and lamb Game (elk, reindeer) Supplemental table 1. Dietary sources of protein among 2441 men from the
Supplementary Online Content
 Supplementary Online Content Anagnostou E, Aman MG, Handen BL, et al. Metformin for treatment of overweight induced by atypical antipsychotic medication in young people with autistic spectrum disorder:
Supplementary Online Content Anagnostou E, Aman MG, Handen BL, et al. Metformin for treatment of overweight induced by atypical antipsychotic medication in young people with autistic spectrum disorder:
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial
: A Randomized Clinical Trial") Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Renal Optimization Strategies Evaluation in Acute Heart Failure (ROSE AHF): A Randomized Clinical Trial Horng H Chen MD on behalf of the NHLBI Heart Failure Clinical Research Network Background AHF + Renal
Supplementary Online Content
 Supplementary Online Content Rubini Giménez M, Twerenbold R, Boeddinghaus J, et al. Clinical effect of sex-specific cutoff values of high-sensitivity cardiac troponin T in suspected myocardial infarction.
Supplementary Online Content Rubini Giménez M, Twerenbold R, Boeddinghaus J, et al. Clinical effect of sex-specific cutoff values of high-sensitivity cardiac troponin T in suspected myocardial infarction.
High Sensitivity Troponin Improves Management. But Not Yet
 High Sensitivity Troponin Improves Management But Not Yet Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
High Sensitivity Troponin Improves Management But Not Yet Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory Medicine
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Solomon SD, Uno H, Lewis EF, et al. Erythropoietic response
The good and bad of exercise
 The good and bad of exercise Dr Baris Gencer, MD Division of Cardiology Geneva University Hospitals Baris.gencer@hcuge.ch SGK Annual Meeting June 16th, 2016 In order for man to succeed in life, God provided
The good and bad of exercise Dr Baris Gencer, MD Division of Cardiology Geneva University Hospitals Baris.gencer@hcuge.ch SGK Annual Meeting June 16th, 2016 In order for man to succeed in life, God provided
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Supplementary Online Content
 Supplementary Online Content Zusterzeel R, Selzman KA, Sanders WE, et al. Cardiac resynchronization therapy in women: US Food and Drug Administration meta-analysis of patientlevel data. Published online
Supplementary Online Content Zusterzeel R, Selzman KA, Sanders WE, et al. Cardiac resynchronization therapy in women: US Food and Drug Administration meta-analysis of patientlevel data. Published online
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content
 Supplementary Online Content Hales CM, Fryar CD, Carroll MD, Freedman DS, Aoki Y, Ogden CL. Differences in obesity prevalence by demographic characteristics and urbanization level among adults in the United
Supplementary Online Content Hales CM, Fryar CD, Carroll MD, Freedman DS, Aoki Y, Ogden CL. Differences in obesity prevalence by demographic characteristics and urbanization level among adults in the United
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Defining rise and fall of cardiac troponin values
 Defining rise and fall of cardiac troponin values Doable but Not Simple Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
Defining rise and fall of cardiac troponin values Doable but Not Simple Allan S. Jaffe, MD.* Consultant - Cardiology & Laboratory Medicine Professor of Medicine Chair, CCLS Division, Department of Laboratory
SUPPLEMENTAL MATERIAL. Supplemental Methods. Duke CAD Index
 SUPPLEMENTAL MATERIAL Supplemental Methods Duke CAD Index The Duke CAD index, originally developed by David F. Kong, is an angiographic score that hierarchically assigns prognostic weights (0-100) based
SUPPLEMENTAL MATERIAL Supplemental Methods Duke CAD Index The Duke CAD index, originally developed by David F. Kong, is an angiographic score that hierarchically assigns prognostic weights (0-100) based
40% minimum reduction from
 160 Circulatory Disease Mortality Target: Death rates in England 1993-2006 Persons under 75 Death / 100,000 population A fall of 44% over 10 years 140 120 100 80 60 40 20 141.0 84.2 Immortality guaranteed
160 Circulatory Disease Mortality Target: Death rates in England 1993-2006 Persons under 75 Death / 100,000 population A fall of 44% over 10 years 140 120 100 80 60 40 20 141.0 84.2 Immortality guaranteed
Serum levels of galectin-1, galectin-3, and galectin-9 are associated with large artery atherosclerotic
 Supplementary Information The title of the manuscript Serum levels of galectin-1, galectin-3, and galectin-9 are associated with large artery atherosclerotic stroke Xin-Wei He 1, Wei-Ling Li 1, Cai Li
Supplementary Information The title of the manuscript Serum levels of galectin-1, galectin-3, and galectin-9 are associated with large artery atherosclerotic stroke Xin-Wei He 1, Wei-Ling Li 1, Cai Li
pulmonary artery vasoreactivity in patients with idiopathic pulmonary arterial hypertension
 Supplementary material Jonas K, Magoń W, Waligóra M, et al. High density lipoprotein cholesterol levels and pulmonary artery vasoreactivity in patients with idiopathic pulmonary arterial hypertension Pol
Supplementary material Jonas K, Magoń W, Waligóra M, et al. High density lipoprotein cholesterol levels and pulmonary artery vasoreactivity in patients with idiopathic pulmonary arterial hypertension Pol
Rikshospitalet, University of Oslo
 Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Rikshospitalet, University of Oslo Preventing heart failure by preventing coronary artery disease progression European Society of Cardiology Dyslipidemia 29.08.2010 Objectives The trends in cardiovascular
Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution
 and females (n=130). Box plots represent the quartiles distribution") Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution of A: total cholesterol (TC); B: low-density lipoprotein
Figure S1. Comparison of fasting plasma lipoprotein levels between males (n=108) and females (n=130). Box plots represent the quartiles distribution of A: total cholesterol (TC); B: low-density lipoprotein
Risk modeling for Breast-Specific outcomes, CVD risk, and overall mortality in Alliance Clinical Trials of Breast Cancer
 Risk modeling for Breast-Specific outcomes, CVD risk, and overall mortality in Alliance Clinical Trials of Breast Cancer Mary Beth Terry, PhD Department of Epidemiology Mailman School of Public Health
Risk modeling for Breast-Specific outcomes, CVD risk, and overall mortality in Alliance Clinical Trials of Breast Cancer Mary Beth Terry, PhD Department of Epidemiology Mailman School of Public Health
Natriuretic Peptides The Cardiologists View. Christopher defilippi, MD University of Maryland Baltimore, MD, USA
 Natriuretic Peptides The Cardiologists View Christopher defilippi, MD University of Maryland Baltimore, MD, USA Disclosures Research support: Alere, BG Medicine, Critical Diagnostics, Roche Diagnostics,
Natriuretic Peptides The Cardiologists View Christopher defilippi, MD University of Maryland Baltimore, MD, USA Disclosures Research support: Alere, BG Medicine, Critical Diagnostics, Roche Diagnostics,
Supplementary Table 1. Patient demographics and baseline characteristics (treated patients).
.") Supplementary Table 1. Patient demographics and baseline characteristics (treated patients). Placebo (n=188) 10 mg (n=186) 25 mg (n=189) Total (n=563) Gender, n (%) Male 75 (40) 97 (52) 84 (44) 256 (45)
Supplementary Table 1. Patient demographics and baseline characteristics (treated patients). Placebo (n=188) 10 mg (n=186) 25 mg (n=189) Total (n=563) Gender, n (%) Male 75 (40) 97 (52) 84 (44) 256 (45)
CARDIOVASCULAR RISK ASSESSMENT ADDITION OF CHRONIC KIDNEY DISEASE AND RACE TO THE FRAMINGHAM EQUATION PAUL E. DRAWZ, MD, MHS
 CARDIOVASCULAR RISK ASSESSMENT ADDITION OF CHRONIC KIDNEY DISEASE AND RACE TO THE FRAMINGHAM EQUATION by PAUL E. DRAWZ, MD, MHS Submitted in partial fulfillment of the requirements for the degree of Master
CARDIOVASCULAR RISK ASSESSMENT ADDITION OF CHRONIC KIDNEY DISEASE AND RACE TO THE FRAMINGHAM EQUATION by PAUL E. DRAWZ, MD, MHS Submitted in partial fulfillment of the requirements for the degree of Master
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Mihai Gheorghiade MD
 Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Mihai Gheorghiade MD Center for Cardiovascular Innovation, Northwestern University Feinberg School of Medicine, Chicago, Illinois On behalf of: Stephen J Greene MD; Javed Butler MD MPH MBA; Gerasimos Filippatos
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Biomarkers in Heart Disease. Felix J. Rogers, DO, FACOI April 29, 2018
 Biomarkers in Heart Disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,
Biomarkers in Heart Disease Felix J. Rogers, DO, FACOI April 29, 2018 Biomarkers NIH: A biomarker is a characteristic that is objectively measured and evaluated as an indicator of normal biological processes,
Copeptin in heart failure: Associations with clinical characteristics and prognosis
 Copeptin in heart failure: Associations with clinical characteristics and prognosis D. Berliner, N. Deubner, W. Fenske, S. Brenner, G. Güder, B. Allolio, R. Jahns, G. Ertl, CE. Angermann, S. Störk for
Copeptin in heart failure: Associations with clinical characteristics and prognosis D. Berliner, N. Deubner, W. Fenske, S. Brenner, G. Güder, B. Allolio, R. Jahns, G. Ertl, CE. Angermann, S. Störk for
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use
 Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
Evidence of Baroreflex Activation Therapy s Mechanism of Action
 Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
Evidence of Baroreflex Activation Therapy s Mechanism of Action Edoardo Gronda, MD, FESC Heart Failure Research Center IRCCS MultiMedica Cardiovascular Department Sesto S. Giovanni (Milano) Italy Agenda
Oscar L. Lopez, M.D. Departments of Neurology and Psychiatry Alzheimer s Disease Research Center University of Pittsburgh School of Medicine
 14th Annual Mild Cognitive Impairment Symposium The Wien Center for Alzheimer's Disease and Memory Disorders, Mount Sinai Medical Center Miami, Florida Markers of inflammation and immune activation, small
14th Annual Mild Cognitive Impairment Symposium The Wien Center for Alzheimer's Disease and Memory Disorders, Mount Sinai Medical Center Miami, Florida Markers of inflammation and immune activation, small
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD
 Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
ST2 in Heart Failure. ST2 as a Cardiovascular Biomarker. Competitive Model of ST2/IL-33 Signaling. ST2 and IL-33: Cardioprotective
 ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ST2 as a Cardiovascular Biomarker Lori B. Daniels, MD, MAS, FACC Professor of Medicine Director, Coronary Care Unit University of California, San Diego ST2 and IL-33: Cardioprotective ST2: member of the
ESCBM meeting 2018, Prague Utility of Cardiac Biomarkers in Clinical Heart Failure Care. Md. Shahidul Islam, M.D., Ph.D
 ESCBM meeting 2018, Prague Utility of Cardiac Biomarkers in Clinical Heart Failure Care Md. Shahidul Islam, M.D., Ph.D shaisl@me.com 2 3 Circulating Biomarkers in Heart Failure. Berezin AE. Adv. Exp. Med.
ESCBM meeting 2018, Prague Utility of Cardiac Biomarkers in Clinical Heart Failure Care Md. Shahidul Islam, M.D., Ph.D shaisl@me.com 2 3 Circulating Biomarkers in Heart Failure. Berezin AE. Adv. Exp. Med.
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials
 AHA Nov 18, 2014 Update on Randomized Trials") Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
BioRemarkable Symposium
 Autor Kurztitel der Präsentation Nr. 1 BioRemarkable Symposium The Use of High/Ultra Sensitivity Troponin as Cardiac Risk Marker in the Population Stefan Blankenberg University Heart Center Hamburg London,
Autor Kurztitel der Präsentation Nr. 1 BioRemarkable Symposium The Use of High/Ultra Sensitivity Troponin as Cardiac Risk Marker in the Population Stefan Blankenberg University Heart Center Hamburg London,
The Framingham Risk Score (FRS) is widely recommended
 is widely recommended") C-Reactive Protein Modulates Risk Prediction Based on the Framingham Score Implications for Future Risk Assessment: Results From a Large Cohort Study in Southern Germany Wolfgang Koenig, MD; Hannelore
C-Reactive Protein Modulates Risk Prediction Based on the Framingham Score Implications for Future Risk Assessment: Results From a Large Cohort Study in Southern Germany Wolfgang Koenig, MD; Hannelore
Overweight and Obesity in Older Persons: Impact Upon Health and Mortality Outcomes
 Overweight and Obesity in Older Persons: Impact Upon Health and Mortality Outcomes Gordon L Jensen, MD, PhD Senior Associate Dean for Research Professor of Medicine and Nutrition Objectives Health outcomes
Overweight and Obesity in Older Persons: Impact Upon Health and Mortality Outcomes Gordon L Jensen, MD, PhD Senior Associate Dean for Research Professor of Medicine and Nutrition Objectives Health outcomes
Supplementary Online Content
 Supplementary Online Content Shurraw S, Hemmelgarn B, Lin M, et al. Association between glycemic control and adverse outcomes in people with diabetes mellitus and chronic kidney disease: a population-based
Supplementary Online Content Shurraw S, Hemmelgarn B, Lin M, et al. Association between glycemic control and adverse outcomes in people with diabetes mellitus and chronic kidney disease: a population-based
2013 Hypertension Measure Group Patient Visit Form
 Please complete the form below for 20 or more unique patients meeting patient sample criteria for the measure group for the current reporting year. A majority (11 or more) patients must be Medicare Part
Please complete the form below for 20 or more unique patients meeting patient sample criteria for the measure group for the current reporting year. A majority (11 or more) patients must be Medicare Part
DECLARATION OF CONFLICT OF INTEREST. Nothing to disclose
 DECLARATION OF CONFLICT OF INTEREST Nothing to disclose Four-Year Clinical Outcomes of the OLIVUS (Impact of OLmesartan on progression of coronary atherosclerosis; evaluation by IntraVascular UltraSound
DECLARATION OF CONFLICT OF INTEREST Nothing to disclose Four-Year Clinical Outcomes of the OLIVUS (Impact of OLmesartan on progression of coronary atherosclerosis; evaluation by IntraVascular UltraSound
2017 ACC/AHA/HFSA HF guidelines. Advances in the Use of Biomarkers in Heart Failure Patients. Outline
 Advances in the Use of Biomarkers in Heart Failure Patients Lori B. Daniels, MD, MAS, FACC, FAHA Professor of Medicine Director, Cardiovascular Intensive Care Unit Sulpizio Cardiovascular Center UC San
Advances in the Use of Biomarkers in Heart Failure Patients Lori B. Daniels, MD, MAS, FACC, FAHA Professor of Medicine Director, Cardiovascular Intensive Care Unit Sulpizio Cardiovascular Center UC San
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Supplementary Online Content
 Supplementary Online Content Li S, Chiuve SE, Flint A, et al. Better diet quality and decreased mortality among myocardial infarction survivors. JAMA Intern Med. Published online September 2, 2013. doi:10.1001/jamainternmed.2013.9768.
Supplementary Online Content Li S, Chiuve SE, Flint A, et al. Better diet quality and decreased mortality among myocardial infarction survivors. JAMA Intern Med. Published online September 2, 2013. doi:10.1001/jamainternmed.2013.9768.
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016
 SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
SGK 2016 Session: Postgraduate Course in Heart Failure Lausanne, 15. June 2016 Heart Failure Guidelines 2016 Matthias Nägele, MD University Hospital Zurich Disclosures I have nothing to disclose. The new
Online Appendix (JACC )
") Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis
Beta blockers in Heart Failure Collaborative Group Online Appendix (JACC013117-0413) Heart rate, heart rhythm and prognostic effect of beta-blockers in heart failure: individual-patient data meta-analysis