Guidelines for Management of Peripheral Arterial Disease
|
|
|
- Judith Phelps
- 6 years ago
- Views:
Transcription

1 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas Health Care System, Dallas, TX June 10, 2017 Saturday, June 9:45-10:15 am

2 Disclosures Honoraria: Medtronic, Gore, Astra Zeneca Research grants: VA, NIH, Boston Scientific, Merck No off-label drug or device information included in the presentation


3 More Recent U.S. Adult PAD Trends PAD: peripheral arterial disease Na7onal average 5.25% 4% % 4.99% % 5.74% % 6.51% % 7.48% % >9.05% h,p:// Roger VL, Go AS, Lloyd-Jones DM, et. al. Heart Disease and Stroke StaPsPcs 2011 Update: A Report From the American Heart AssociaPon. Circula(on 2011;123:e18-e209.
4 PARTNERS: Prevalence of PAD and Other CVD in Primary Care Practices 29% of Patients in a Target Population Were Diagnosed With PAD Using An Office-Based ABI 29% 44% 56% Patients diagnosed with PAD PAD only PAD and CVD ABI=ankle-brachial index; CVD=cardiovascular disease. Hirsch, AT et al. JAMA. 2001;286:
 1 San Diego Study (PAD by noninvasive tests) 2 60 PaPents With PAD (%) 50 40 30 20 10 0 55-59 60-64 65-69 70-74 75-79 80-84 85-89 Age (years) ABI=ankle-brachial index 1.")
5 Prevalence of PAD Increases With Age Ro,erdam Study (ABI <0.9) 1 San Diego Study (PAD by noninvasive tests) 2 60 PaPents With PAD (%) Age (years) ABI=ankle-brachial index 1. Meijer WT, et al. Arterioscler Thromb Vasc Biol. 1998;18: Criqui MH, et al. Circulation. 1985;71:
6 Gender Differences in the Prevalence of PAD Prevalence (%) Consecutive Patients (61% Female) in 344 Primary Care Offices <70 Women Men >85 Age (years) Adapted from Diehm C. Atherosclerosis. 2004;172: with permission from Elsevier.
7 PAD: More Prevalent and More Deadly Than Many Leading Diseases Disease Prevalence (Millions) Five-Year Mortality Rate % % 30% 39% 30% 28% % 10% 21% 14% 2 0 Diabetes CAD PAD Cancer CHF Stroke Alzheimers 0% Colorectal Cancer PAD Stroke CAD Breast Cancer Source: American Cancer Society, American Heart Association, Alzheimers Disease Education/Referral Center, American Diabetes Association, SAGE Group
8 Risk Factors for PAD Reduced Increased Smoking Diabetes Hypertension Hypercholesterolemia Hyperhomocysteinemia Renal insufficiency Age (per 10 years) Relative Risk Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192.


9 Diabetes Increases the Risk of PAD Prevalence of PAD (%) * 22.4* 0 Normal Glucose Tolerance Impaired Glucose Tolerance Diabetes Impaired glucose tolerance was defined as oral glucose tolerance test value 140 mg/dl but <200 mg/dl. *P.05 vs. normal glucose tolerance. Lee AJ, et al. Br J Haematol. 1999;105:


10 Using the Ankle-Brachial Index (ABI) Right ABI 80/160=0.50 Left ABI 120/160=0.75 ABI (Normal >0.90) Brachial SBP 150 mm Hg Brachial SBP 160 mm Hg Highest brachial SBP PT SBP 40 mm Hg DP SBP 80 mm Hg PT SBP 120 mm Hg DP SBP 80 mm Hg Highest of PT or DP SBP ABI=ankle-brachial index; DP=dorsalis pedis; PT=posterior tibial; SBP=systolic blood pressure.


11 Interpreting the Ankle-Brachial Index ABI Interpretation Normal Borderline Mild-to-moderate disease 0.40 Severe disease 1.40 Non-compressible (DM & CKD) ACC/AHA PAD Guidelines 2011


12 Ankle Brachial Index (ABI) Diagnostic test Sensitivity Specificity ABI < % 100% Pap smear 30-87% % Fecal occult blood 37-78% 87-98% Mammography 75-90% 90-95% Arch Intern Med. 2003;163:
13
 0.61-0.70 (n=141) 0.71-0.80 (n=186) 0.81-0.90 (n=310) 0.91-1.00 (n=709) 1.")
 Age range=mid- to late-50s; ABI=ankle-brachial index; *Median duration of follow-up was 11.1 (0.1 12) years.")
14 Association Between ABI and All Cause Mortality* Total Mortality (%) N=5748 Risk increases at ABI values below 1.0 and above <0.61 (n=156) (n=141) (n=186) (n=310) (n=709) (n=1750) Baseline ABI (n=1578) (n=696) (n=156) >1.40 (n=66) Age range=mid- to late-50s; ABI=ankle-brachial index; *Median duration of follow-up was 11.1 (0.1 12) years. O Hare AM et al. Circulation. 2006;113:
 Claudication Claudication: impairs patient")
")
15 Clinical Presentation of PAD Do you have leg pain? 50% Asymptomatic ~15% Classic (Typical) Claudication Claudication: impairs patient quality of life by causing painful cramps and dysfunction while walking CLI: rest pain, non-healing or poorly healing ulcers, or gangrene 1%-2% Critical Limb Ischemia (CLI) ~33% Atypical Leg Pain (functionally limited)
 Hirsch AT, et al. Circulation.")
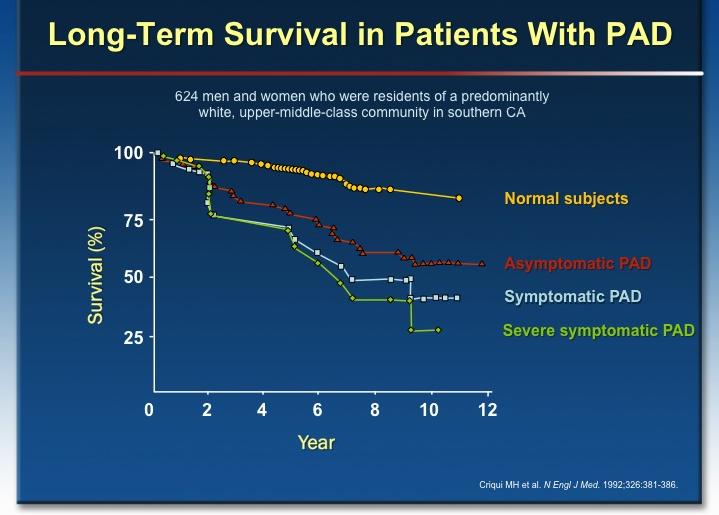
16 Natural History of Atherosclerotic Lower Extremity PAD PAD Population (50 years and older) Initial clinical presentation Asymptomatic PAD 20%-50% Atypical leg pain 40%-50% Claudication 10%-35% Critical limb ischemia 1%-2% Progressive functional impairment Alive w/ 2 limbs 50% 1-year outcomes Amputation 25% CV mortality 25% 5-year outcomes (to next slide) Hirsch AT, et al. Circulation. 2006;113:e
17 Natural History of Atherosclerotic Lower Extremity PAD For each of these PAD clinical syndromes Asymptomatic PAD 20%-50% Claudication 10%-35% Atypical leg pain 40%-50% Limb morbidity 5-year outcomes CV morbidity & mortality Stable claudication 70%-80% Worsening claudication 10%-20% Critical limb ischemia 1%-2% Amputation (see CLI data) Nonfatal CV event (MI or stroke) 20% CV causes 75% Mortality 15%-30% Non-CV causes 25% CLI=critical limb ischemia; CV=cardiovascular; MI=myocardial infarction Hirsch AT, et al. Circulation. 2006;113:e
18 Age 65 y Patients at Increased Risk of PAD Age y, with risk factors for atherosclerosis (e.g., diabetes mellitus, history of smoking, hyperlipidemia, hypertension) or family history of PAD Age <50 y, with diabetes mellitus and 1 additional risk factor for atherosclerosis Individuals with known atherosclerotic disease in another vascular bed (e.g., coronary, carotid, subclavian, renal, mesenteric artery stenosis, or AAA)
19 Resting ABI for Diagnosing PAD COR LOE Recommendations In patients with history or physical examination findings suggestive of I B-NR PAD, the resting ABI, with or without segmental pressures and waveforms, is recommended to establish the diagnosis. I IIa III: No Benefit C-LD B-NR B-NR Resting ABI results should be reported as abnormal (ABI 0.90), borderline (ABI ), normal ( ), or noncompressible (ABI >1.40). In patients at increased risk of PAD but without history or physical examination findings suggestive of PAD, measurement of the resting ABI is reasonable. In patients not at increased risk of PAD and without history or physical examination findings suggestive of PAD, the ABI is not recommended.
20 Diagnostic Testing for Suspected PAD Diagnostic Testing for Suspected PAD History and physical examination suggestive of PAD without rest pain, nonhealing wound, or gangrene (Table 4) Suspect CLI (Figure 2) Colors correspond to Class of Recommendation Noncompressible arteries ABI: >1.40 ABI with or without segmental limb pressures and waveforms (Class I) Normal ABI: Borderline ABI: Abnormal ABI: 0.90 ABI indicates ankle-brachial index; CLI, critical limb ischemia; CTA, computed tomography angiography; GDMT, guideline-directed management and therapy; MRA, magnetic resonance angiography; PAD, peripheral artery disease; and TBI, toe-brachial index. Search for alternative diagnosis (Table 5) Normal (>0.70) TBI (Class I) Abnormal ( 0.70) Abnormal Lifestyle-limiting claudication despite GDMT, revascularization considered Exertional non joint related leg symptoms Yes Exercise ABI (Class I) Normal No Search for alternative diagnosis (Table 5) Exercise ABI (Class IIa) Anatomic assessment: Duplex ultrasound CTA or MRA (Class I) Options Yes No Anatomic assessment: Invasive angiography (Class IIa) Continue GDMT (Class I) Do not perform invasive or noninvasive anatomic assessments for asymptomatic patients (Class III: Harm)
21 Diagnostic Testing for Suspected CLI Diagnostic Testing for Suspected CLI Non-compressible arteries ABI: >1.40 History and physical examination suggestive of PAD with rest pain, nonhealing wound, or gangrene (Table 4) Yes ABI (Class I) No Normal ABI: Borderline ABI: Search for alternative diagnosis (Tables 5 and 6) Abnormal ABI: 0.90 Colors correspond to Class of Recommendation in Table 1. *Order based on expert consensus. TBI with waveforms, if not already performed. ABI indicates ankle-brachial index; CLI, critical limb ischemia; CTA, computed tomography angiography; MRA, magnetic resonance angiography; TcPO 2, transcutaneous oxygen pressure; and TBI, toebrachial index. Normal (>0.70) TBI (Class I) Search for alternative diagnosis (Table 6) Abnormal ( 0.70) Perfusion assessment: TBI with waveforms TcPO 2 * Skin perfusion pressure* (Class IIa) Normal Abnormal Nonhealing wound or gangrene Yes No Search for alternative diagnosis (Table 5) Additional perfusion assessment, particularly if ABI >0.70: TBI with waveforms TcPO 2 * Skin perfusion pressure* (Class IIa) Normal Abnormal Anatomic assessment: Duplex ultrasound CTA or MRA Invasive angiography (Class I)
22 Imaging for Anatomic Assessment COR LOE Recommendations Duplex ultrasound, CTA, or MRA of the lower extremities is useful to I B-NR diagnose anatomic location and severity of stenosis for patients with symptomatic PAD in whom revascularization is considered. I IIa III: Harm C-EO C-EO B-R Invasive angiography is useful for patients with CLI in whom revascularization is considered. Invasive angiography is reasonable for patients with lifestyle-limiting claudication with an inadequate response to GDMT for whom revascularization is considered. Invasive and noninvasive angiography (i.e., CTA, MRA) should not be performed for the anatomic assessment of patients with asymptomatic PAD.
23 Screening for Atherosclerotic Disease in Other Vascular Beds for the Patient With PAD Abdominal Aortic Aneurysm COR LOE Recommendation IIa B-NR A screening duplex ultrasound for AAA is reasonable in patients with symptomatic PAD. There is no evidence to demonstrate that screening all patients with PAD for asymptomatic atherosclerosis in other arterial beds improves clinical outcome.
24 Antiplatelet Agents COR LOE Recommendations Antiplatelet therapy with aspirin alone (range mg per day) or I A clopidogrel alone (75 mg per day) is recommended to reduce MI, stroke, and vascular death in patients with symptomatic PAD. IIa IIb C-EO B-R In asymptomatic patients with PAD (ABI 0.90), antiplatelet therapy is reasonable to reduce the risk of MI, stroke, or vascular death. In asymptomatic patients with borderline ABI ( ), the usefulness of antiplatelet therapy to reduce the risk of MI, stroke, or vascular death is uncertain.
25 Antiplatelet Agents (cont d) COR LOE Recommendations The effectiveness of dual-antiplatelet therapy (aspirin and clopidogrel) to IIb B-R reduce the risk of cardiovascular ischemic events in patients with symptomatic PAD is not well established. IIb IIb C-LD B-R Dual-antiplatelet therapy (aspirin and clopidogrel) may be reasonable to reduce the risk of limb-related events in patients with symptomatic PAD after lower extremity revascularization. The overall clinical benefit of vorapaxar added to existing antiplatelet therapy in patients with symptomatic PAD is uncertain.
26 Statin Agents COR LOE Recommendations I A Treatment with a statin medication is indicated for all patients with PAD. Oral Anticoagulation COR LOE Recommendations The usefulness of anticoagulation to improve patency after lower extremity IIb B-R autogenous vein or prosthetic bypass is uncertain. III: Harm A Anticoagulation should not be used to reduce the risk of cardiovascular ischemic events in patients with PAD.
27 Smoking Cessation COR LOE Recommendations I A Patients with PAD who smoke cigarettes or use other forms of tobacco should be advised at every visit to quit. I A Patients with PAD who smoke cigarettes should be assisted in developing a plan for quitting that includes pharmacotherapy (i.e., varenicline, buproprion, and/or nicotine replacement therapy) and/or referral to a smoking cessation program. I B-NR Patients with PAD should avoid exposure to environmental tobacco smoke at work, at home, and in public places.
28 Cilostazol, Pentoxifylline, and Chelation Therapy COR LOE Recommendations Cilostazol I A Cilostazol is an effective therapy to improve symptoms and increase walking distance in patients with claudication. Pentoxifylline III: No B-R Benefit Chelation Therapy III: No B-R Benefit Pentoxifylline is not effective for treatment of claudication. Chelation therapy (e.g., ethylenediaminetetraacetic acid) is not beneficial for treatment of claudication. Homocysteine Lowering COR LOE Recommendation III: No Benefit B-R B-complex vitamin supplementation to lower homocysteine levels for prevention of cardiovascular events in patients with PAD is not recommended.
29 Structured Exercise Therapy COR LOE Recommendations In patients with claudication, a supervised exercise program is recommended I A to improve functional status and QoL and to reduce leg symptoms. I IIa IIa B-R A A A supervised exercise program should be discussed as a treatment option for claudication before possible revascularization. In patients with PAD, a structured community- or home-based exercise program with behavioral change techniques, can be beneficial to improve walking ability and functional status. In patients with claudication, alternative strategies of exercise therapy, including upper-body ergometry, cycling, and pain-free or low-intensity walking that avoids moderate-to-maximum claudication while walking, can be beneficial to improve walking ability and functional status.
30
31 Minimizing Tissue Loss in Patients With PAD COR LOE Recommendations Patients with PAD and diabetes mellitus should be counseled about self I C-LD foot examination and healthy foot behaviors. I IIa IIa IIa C-LD C-LD C-EO C-EO In patients with PAD, prompt diagnosis and treatment of foot infection are recommended to avoid amputation. In patients with PAD and signs of foot infection, prompt referral to an interdisciplinary care team (Table 8) can be beneficial. It is reasonable to counsel patients with PAD without diabetes mellitus about self-foot examination and healthy foot behaviors. Biannual foot examination by a clinician is reasonable for patients with PAD and diabetes mellitus.
32 2016 AHA/ACC Lower Extremity PAD Guideline Revascularization for Claudication COR LOE Recommendation Revascularization is a reasonable treatment option for the patient with IIa A lifestyle-limiting claudication with an inadequate response to GDMT.
33 Endovascular Revascularization for Claudication COR LOE Recommendations Endovascular procedures are effective as a revascularization option for I A patients with lifestyle-limiting claudication and hemodynamically significant aortoiliac occlusive disease. IIa IIb III: Harm B-R C-LD B-NR Endovascular procedures are reasonable as a revascularization option for patients with lifestyle-limiting claudication and hemodynamically significant femoropopliteal disease. The usefulness of endovascular procedures as a revascularization option for patients with claudication due to isolated infrapopliteal artery disease is unknown. Endovascular procedures should not be performed in patients with PAD solely to prevent progression to CLI.
34 Surgical Revascularization for Claudication COR LOE Recommendations I A When surgical revascularization is performed, bypass to the popliteal artery with autogenous vein is recommended in preference to prosthetic graft material. IIa B-NR Surgical procedures are reasonable as a revascularization option for patients with lifestyle-limiting claudication with inadequate response to GDMT, acceptable perioperative risk, and technical factors suggesting advantages over endovascular procedures. III: Harm III: Harm B-R B-NR Femoral-tibial artery bypasses with prosthetic graft material should not be used for the treatment of claudication. Surgical procedures should not be performed in patients with PAD solely to prevent progression to CLI.
35 Management of CLI Revascularization for CLI COR LOE Recommendation I B-NR In patients with CLI, revascularization should be performed when possible to minimize tissue loss. I C-EO An evaluation for revascularization options should be performed by an interdisciplinary care team before amputation in the patient with CLI.
36 Endovascular Revascularization for CLI COR LOE Recommendations Endovascular procedures are recommended to establish in-line blood flow I B-R to the foot in patients with nonhealing wounds or gangrene. IIa IIa IIb C-LD B-R B-NR A staged approach to endovascular procedures is reasonable in patients with ischemic rest pain. Evaluation of lesion characteristics can be useful in selecting the endovascular approach for CLI. Use of angiosome-directed endovascular therapy may be reasonable for patients with CLI and nonhealing wounds or gangrene.
37 Surgical Revascularization for CLI COR LOE Recommendations I A When surgery is performed for CLI, bypass to the popliteal or infrapopliteal arteries (i.e., tibial, pedal) should be constructed with suitable autogenous vein. I C-LD Surgical procedures are recommended to establish in-line blood flow to the foot in patients with nonhealing wounds or gangrene. IIa B-NR In patients with CLI for whom endovascular revascularization has failed and a suitable autogenous vein is not available, prosthetic material can be effective for bypass to the below-knee popliteal and tibial arteries. IIa C-LD A staged approach to surgical procedures is reasonable in patients with ischemic rest pain.
38 Diagnosis and Management of ALI Diagnosis and Management of ALI Acutely cold, painful leg Suspected ALI Clinical evaluation, including: symptoms, motor and sensory assessment, arterial and venous Doppler signals (Class I) Colors correspond to Class of Recommendation in Table 1. ALI indicates acute limb ischemia. Audible arterial Audible venous Inaudible arterial Audible venous Inaudible arterial Inaudible venous Revascularization (urgent) AND anticoagulation, unless contraindicated (Class I) Category I: Viable limb Normal motor function No sensory loss Intact capillary refill Motor function assessment Category III: Irreversible Complete loss of motor function Complete sensory loss Absent capillary refill Primary amputation (Class I) Intact Category IIa: Marginally threatened Slow-to-intact capillary refill Sensory loss limited to toes if present No muscle weakness Impaired Category IIb: Immediately threatened Slow-to-absent capillary refill Sensory loss more than toes and with rest pain Mild or moderate muscle weakness Salvageable if treated promptly Salvageable if treated emergently Revascularization (emergency) AND Anticoagulation, unless contraindicated (Class I) Revascularization (emergency) AND Anticoagulation, unless contraindicated (Class I)
39 Longitudinal Follow-Up COR LOE Recommendations Patients with PAD should be followed up with periodic clinical evaluation, I C-EO including assessment of cardiovascular risk factors, limb symptoms, and functional status. I IIa IIa IIb C-EO B-R C-LD B-R Patients with PAD who have undergone lower extremity revascularization (surgical and/or endovascular) should be followed up with periodic clinical evaluation and ABI measurement. Duplex ultrasound can be beneficial for routine surveillance of infrainguinal, autogenous vein bypass grafts in patients with PAD. Duplex ultrasound is reasonable for routine surveillance after endovascular procedures in patients with PAD. The effectiveness of duplex ultrasound for routine surveillance of infrainguinal prosthetic bypass grafts in patients with PAD is uncertain.
40 Conclusions PAD is highly prevalent & portends adverse cardiovascular, limb and quality of life outcomes Proactive approach to detection of PAD Guideline-based medical therapy is first-line for claudicants & revascularization reserved for refractory symptoms Early detection & prompt revascularization to prevent or limit tissue loss in critical limb ischemia


41 Register Now:
Larry Diaz, MD, FSCAI Mehdi H. Shishehbor, DO, FSCAI
 PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment
: Presentation, Diagnosis, and Treatment") Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease
 Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Interventional Cardiology and Cath Labs The Changing Landscape of Managing Patients with PAD- Update on the Evidence and Practice of Care in Patients with Peripheral Artery Disease Manesh R. Patel MD Chief,
Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD
 Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD Pranav M. Patel, MD, FACC, FSCAI Interim Chief & Associate Professor of Medicine Director, Cardiac Catheterization Lab University
Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD Pranav M. Patel, MD, FACC, FSCAI Interim Chief & Associate Professor of Medicine Director, Cardiac Catheterization Lab University
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
John E. Campbell, MD. Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Perfusion Assessment in Chronic Wounds
 Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Peripheral Arterial Disease: Screening, Evaluation and Management. Mitchel Sklar, MD, FACC, FSCAI. Cardiovascular Associates of R.I.
 Peripheral Arterial Disease: Screening, Evaluation and Management Mitchel Sklar, MD, FACC, FSCAI Cardiovascular Associates of R.I. Natural History of Intermittent Claudication/PAD: Peripheral to what?
Peripheral Arterial Disease: Screening, Evaluation and Management Mitchel Sklar, MD, FACC, FSCAI Cardiovascular Associates of R.I. Natural History of Intermittent Claudication/PAD: Peripheral to what?
Disclosures. Critical Limb Ischemia. Vascular Testing in the CLI Patient. Vascular Testing in Critical Limb Ischemia UCSF Vascular Symposium
 Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Joshua A. Beckman, MD. Brigham and Women s Hospital
 Peripheral Vascular Disease: Overview, Peripheral Arterial Obstructive Disease, Carotid Artery Disease, and Renovascular Disease as a Surrogate for Coronary Artery Disease Joshua A. Beckman, MD Brigham
Peripheral Vascular Disease: Overview, Peripheral Arterial Obstructive Disease, Carotid Artery Disease, and Renovascular Disease as a Surrogate for Coronary Artery Disease Joshua A. Beckman, MD Brigham
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Goals of Screening Programs. What is Vascular Screening? Assumptions Regarding the Potential Benefits of Screening Programs PAD
 Conflict of Interest Disclosure (Relationships with Industry) An Epidemic of : The Debate Over Population Screening Membership on an advisory board, consultant, or recipient of a research grant from the
Conflict of Interest Disclosure (Relationships with Industry) An Epidemic of : The Debate Over Population Screening Membership on an advisory board, consultant, or recipient of a research grant from the
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential
 USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
Treatment Strategies For Patients with Peripheral Artery Disease
 Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Peripheral arterial disease for primary care Ed Aboian, MD
 Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
What s New in the Management of Peripheral Arterial Disease
 What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
How Do We Optimize the Medical Therapy of Patients with Critical Limb Ischemia?
 How Do We Optimize the Medical Therapy of Patients with Critical Limb Ischemia? Ehrin J. Armstrong, MD MSc MAS Director, Interventional Cardiology Director, Vascular Laboratory VA Eastern Colorado Healthcare
How Do We Optimize the Medical Therapy of Patients with Critical Limb Ischemia? Ehrin J. Armstrong, MD MSc MAS Director, Interventional Cardiology Director, Vascular Laboratory VA Eastern Colorado Healthcare
Peripheral Arterial Disease. Westley Smith MD Vascular Fellow
 Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
When to screen for PAD? Prof. Dr.Tine De Backer Prof. Dr. Jean-Claude Wautrecht
 When to screen for PAD? Prof. Dr.Tine De Backer Prof. Dr. Jean-Claude Wautrecht How do we define asymptomatic PAD? A. ABI < 1 B. ABI < 0.9 C. ABI < 0.8 D. ABI > 1 How do we define asymptomatic PAD? A.
When to screen for PAD? Prof. Dr.Tine De Backer Prof. Dr. Jean-Claude Wautrecht How do we define asymptomatic PAD? A. ABI < 1 B. ABI < 0.9 C. ABI < 0.8 D. ABI > 1 How do we define asymptomatic PAD? A.
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Due to Perimed s commitment to continuous improvement of our products, all specifications are subject to change without notice.
 A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Early Identification of PAD: Evidence to Refute USPSTF Position on Screening
 Early Identification of PAD: Evidence to Refute USPSTF Position on Screening Mehdi H. Shishehbor, DO, MPH, PhD Director Endovascular Services Interventional Cardiology & Vascular Medicine Department of
Early Identification of PAD: Evidence to Refute USPSTF Position on Screening Mehdi H. Shishehbor, DO, MPH, PhD Director Endovascular Services Interventional Cardiology & Vascular Medicine Department of
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Imaging for Peripheral Vascular Disease
 Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE
 GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE Michael S. Conte MD Professor and Chief, Vascular and Endovascular Surgery Co-Director, Center for Limb Preservation Co-Director, Heart and Vascular
GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE Michael S. Conte MD Professor and Chief, Vascular and Endovascular Surgery Co-Director, Center for Limb Preservation Co-Director, Heart and Vascular
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Cardiovascular Update for Primary Care Providers. Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD
 Cardiovascular Update for Primary Care Providers Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD Agenda Lower Extremity pain Initial evaluation Treatment options of noncritical
Cardiovascular Update for Primary Care Providers Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD Agenda Lower Extremity pain Initial evaluation Treatment options of noncritical
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care
 Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Peripheral Arterial Disease: Objectives. Disclosure. Definition: Peripheral Arterial Disease (PAD)
") Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
Ticagrelor versus Clopidogrel in Symptomatic Peripheral Artery Disease (EUCLID Trial)
") Audience Interaction The chat box is available on the left hand side. Let us know who you are and where you re viewing from! Questions can be entered by hitting the green box with a question mark in it
Audience Interaction The chat box is available on the left hand side. Let us know who you are and where you re viewing from! Questions can be entered by hitting the green box with a question mark in it
Clinical Approach to CLI and Related Diagnostics: What You Need to Know
 Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Interventional Treatment First for CLI
 Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital
 Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
National Clinical Conference 2018 Baltimore, MD
 National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
Medical Therapy for Peripheral Artery Disease
 Medical Therapy for Peripheral Artery Disease Beau M. Hawkins, MD, FSCAI University of Oklahoma Health Sciences Center, Oklahoma City, OK Sahil A. Parikh, MD, FSCAI Columbia University Medical Center,
Medical Therapy for Peripheral Artery Disease Beau M. Hawkins, MD, FSCAI University of Oklahoma Health Sciences Center, Oklahoma City, OK Sahil A. Parikh, MD, FSCAI Columbia University Medical Center,
Medical Management of Vascular Disease KEITH E SWANSON MD ND ACADEMY OF FAMILY PHYSICIANS FAMILY MEDICINE UPDATE JANUARY 2017
 Medical Management of Vascular Disease KEITH E SWANSON MD ND ACADEMY OF FAMILY PHYSICIANS FAMILY MEDICINE UPDATE JANUARY 2017 Objectives 1. Appreciate the long term implications of PAD 2. Appreciate the
Medical Management of Vascular Disease KEITH E SWANSON MD ND ACADEMY OF FAMILY PHYSICIANS FAMILY MEDICINE UPDATE JANUARY 2017 Objectives 1. Appreciate the long term implications of PAD 2. Appreciate the
- Lecture - Recommandations ESC : messages importants P. MEYER (Saint Laurent du Var) - Controverse - Qui doit faire l'angioplastie périphérique?
 - Controverse - Qui doit faire l'angioplastie périphérique?") - Lecture - Recommandations ESC : messages importants P. MEYER (Saint Laurent du Var) - Controverse - Qui doit faire l'angioplastie périphérique? Un chirurgien E. DUCASSE (Bordeaux) Un interventionnel
- Lecture - Recommandations ESC : messages importants P. MEYER (Saint Laurent du Var) - Controverse - Qui doit faire l'angioplastie périphérique? Un chirurgien E. DUCASSE (Bordeaux) Un interventionnel
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options
 Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
TABLE OF CONTENTS. 2. LOWER EXTREMITY PERIPHERAL ARTERIAL DISEASE 2.1. Epidemiology Risk Factors
 LOWER EXTREMITY PAD The following is one of three extracted sections lower extremity, renal/mesenteric, and abdominal aortic of the ACC/AHA 2005 Guidelines for the Management of Patients With Peripheral
LOWER EXTREMITY PAD The following is one of three extracted sections lower extremity, renal/mesenteric, and abdominal aortic of the ACC/AHA 2005 Guidelines for the Management of Patients With Peripheral
Surveillance of Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes
 Surveillance of Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes Naveed Afzal, Sunghwan Sohn, Christopher G. Scott, Hongfang Liu, Iftikhar J. Kullo, Adelaide M. Arruda-Olson
Surveillance of Peripheral Arterial Disease Cases Using Natural Language Processing of Clinical Notes Naveed Afzal, Sunghwan Sohn, Christopher G. Scott, Hongfang Liu, Iftikhar J. Kullo, Adelaide M. Arruda-Olson
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
LIMB SALVAGE IN THE DIABETIC PATIENT
 LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
2016 AHA/ACC Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease: Executive Summary
 701592VMJ0010.1177/1358863X17701592Vascular MedicineGerhard-Herman et al. research-article2017 Clinical Practice Guideline: Executive Summary 2016 AHA/ACC Guideline on the Management of Patients with Lower
701592VMJ0010.1177/1358863X17701592Vascular MedicineGerhard-Herman et al. research-article2017 Clinical Practice Guideline: Executive Summary 2016 AHA/ACC Guideline on the Management of Patients with Lower
Intended Learning Outcomes
 2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
Objective assessment of CLI patients Hemodynamic parameters
 Objective assessment of CLI patients Hemodynamic parameters Worth anything in end stage patients? Marianne Brodmann Angiology, Medical University Graz, Austria Disclosure Speaker name: Marianne Brodmann
Objective assessment of CLI patients Hemodynamic parameters Worth anything in end stage patients? Marianne Brodmann Angiology, Medical University Graz, Austria Disclosure Speaker name: Marianne Brodmann
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Peripheral Arterial Disease Management A Practical Guide for Internists. EFIM Vascular Working Group
 2 Peripheral Arterial Disease Management A Practical Guide for Internists EFIM Vascular Working Group 1 Peripheral arterial disease (PAD) is a growing concern among our aging population. More than 27 million
2 Peripheral Arterial Disease Management A Practical Guide for Internists EFIM Vascular Working Group 1 Peripheral arterial disease (PAD) is a growing concern among our aging population. More than 27 million
Disclosures. TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Purpose of Practice Guidelines
 TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
Lower Extremity Artery: Physiologic Testing
 Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Resident Teaching Conference 3/12/2010
 Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia
 Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Amputation as a Last Resort A Multidisciplinary Approach to Limb Salvage
 Amputation as a Last Resort A Multidisciplinary Approach to Limb Salvage George L. Adams, MD, MHS, MBA, FACC, FSCAI Clinical Associate Professor of Medicine University of North Carolina Health System Director
Amputation as a Last Resort A Multidisciplinary Approach to Limb Salvage George L. Adams, MD, MHS, MBA, FACC, FSCAI Clinical Associate Professor of Medicine University of North Carolina Health System Director
A new era in the treatment of peripheral artery disease (PAD)?
?") A new era in the treatment of peripheral artery disease (PAD)? Prof. Dr. Jan Beyer-Westendorf Head of Thrombosis Research, University Hospital Carl Gustav Carus, TU Dresden; Germany Senior Lecturer Thrombosis
A new era in the treatment of peripheral artery disease (PAD)? Prof. Dr. Jan Beyer-Westendorf Head of Thrombosis Research, University Hospital Carl Gustav Carus, TU Dresden; Germany Senior Lecturer Thrombosis
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Overview. Arterial Disease: Carotid, Aortic and Peripheral Intensive Review in Internal Medicine 2012
 Arterial Disease: Carotid, Aortic and Peripheral Intensive Review in Internal Medicine 2012 None Disclosures / Conflicts of Interest Joshua Beckman, M.D. Vascular Medicine Section Cardiovascular Division
Arterial Disease: Carotid, Aortic and Peripheral Intensive Review in Internal Medicine 2012 None Disclosures / Conflicts of Interest Joshua Beckman, M.D. Vascular Medicine Section Cardiovascular Division
ACCF/AHA Practice Guidelines
 ACCF/AHA Practice Guidelines Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) A Report of the American College of Cardiology Foundation/American
ACCF/AHA Practice Guidelines Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) A Report of the American College of Cardiology Foundation/American
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Case Study: Chris Arden. Peripheral Arterial Disease
 Case Study: Chris Arden Peripheral Arterial Disease Patient Presentation Diane is a 65-year-old retired school teacher She complains of left calf pain when walking 50 metres; the pain goes away after she
Case Study: Chris Arden Peripheral Arterial Disease Patient Presentation Diane is a 65-year-old retired school teacher She complains of left calf pain when walking 50 metres; the pain goes away after she
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler Jones, MD September 14, 2016
 PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
SAVE LIMBS SAVE LIVES!
 SAVE LIMBS SAVE LIVES! PAD Awareness: The Key to Limb Preservation By Frank J Tursi, D.P.M., F.A.C.F.A.S. Epidemiology Over 12 million people are afflicted with PAD 11 Million of these-dm 4 Million DFU
SAVE LIMBS SAVE LIVES! PAD Awareness: The Key to Limb Preservation By Frank J Tursi, D.P.M., F.A.C.F.A.S. Epidemiology Over 12 million people are afflicted with PAD 11 Million of these-dm 4 Million DFU
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More. Spence M Taylor, M.D.
 Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Registry Assessment of Peripheral Interventional Devices (RAPID)
") Registry Assessment of Peripheral Interventional Devices (RAPID) Adding Data Sources May 2, 2018 W. Schuyler Jones, MD Duke Clinical Research Institute Duke Heart Center Disclosures Research Grants: Agency
Registry Assessment of Peripheral Interventional Devices (RAPID) Adding Data Sources May 2, 2018 W. Schuyler Jones, MD Duke Clinical Research Institute Duke Heart Center Disclosures Research Grants: Agency
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ABI. See Ankle-brachial index (ABI). Afterload, deconstructing of, in ventricular vascular interaction in heart failure, 449 Air plethysmography
Index Note: Page numbers of article titles are in boldface type. A ABI. See Ankle-brachial index (ABI). Afterload, deconstructing of, in ventricular vascular interaction in heart failure, 449 Air plethysmography
V.A. is a 62-year-old male who presents in referral
 , LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
, LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
UC SF. Disclosures. Vascular Assessment of the Diabetic Foot. What are the best predictors of wound healing? None. Non-Invasive Vascular Studies
 Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Critical Limb Ischemia: Diagnosis and Current Management
 Research Article Joseph Karam, MD Elliot J. Stephenson, MD From: Minneapolis Heart Institutet at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Joseph Karam, MD Minneapolis Heart
Research Article Joseph Karam, MD Elliot J. Stephenson, MD From: Minneapolis Heart Institutet at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Joseph Karam, MD Minneapolis Heart
Medical Therapy of Peripheral Artery Disease
 Medical Therapy of Peripheral Artery Disease Alvaro Alonso, MD Assistant Professor of Medicine Associate Director, Interven4onal Cardiology Fellowship Program Tulane University Heart & Vascular Ins4tute
Medical Therapy of Peripheral Artery Disease Alvaro Alonso, MD Assistant Professor of Medicine Associate Director, Interven4onal Cardiology Fellowship Program Tulane University Heart & Vascular Ins4tute
Pedal Bypass With Deep Venous Arterialization:
 Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
The Many Views of PAD: Imaging Modalities for the Interventionist
 The Many Views of PAD: Imaging Modalities for the Interventionist Timothy E. Yates, MD Interventional Vascular & Oncological Radiology Mount Sinai Medical Center 5 December 2015 None Disclosures Objectives
The Many Views of PAD: Imaging Modalities for the Interventionist Timothy E. Yates, MD Interventional Vascular & Oncological Radiology Mount Sinai Medical Center 5 December 2015 None Disclosures Objectives
Nurse and Technician Forum Part II Critical Limb Ischemia: Optimal care, an interdisciplinary challenge
 L E I P Z I G I N T E R V E N T I O N A L C O U R S E 2017 Nurse and Technician Forum Part II Critical Limb Ischemia: Optimal care, an interdisciplinary challenge Markus Haumer Landesklinikum Baden-Mödling
L E I P Z I G I N T E R V E N T I O N A L C O U R S E 2017 Nurse and Technician Forum Part II Critical Limb Ischemia: Optimal care, an interdisciplinary challenge Markus Haumer Landesklinikum Baden-Mödling
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease
 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease Developed in Collaboration with American Association for Thoracic Surgery, American
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
The Evolving Treatment of Peripheral Arterial Disease through Guideline-Directed Recommendations
 Journal of Clinical Medicine Review The Evolving Treatment of Peripheral Arterial Disease through Guideline-Directed Recommendations Ramez Morcos 1, Boshra Louka 2, Andrew Tseng 2, Sanjay Misra 3, Robert
Journal of Clinical Medicine Review The Evolving Treatment of Peripheral Arterial Disease through Guideline-Directed Recommendations Ramez Morcos 1, Boshra Louka 2, Andrew Tseng 2, Sanjay Misra 3, Robert
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
AAIM TRIENNIAL COURSE 124 TH ANNUAL MEETING. The Broadmoor Colorado Springs, CO
 AAIM TRIENNIAL COURSE 124 TH ANNUAL MEETING The Broadmoor Colorado Springs, CO October 2015 MAJOR ARTERIAL DISEASES ROBERT LUND MD, DBIM Two Main Types of Major Arterial Disease Atherosclerotic Peripheral
AAIM TRIENNIAL COURSE 124 TH ANNUAL MEETING The Broadmoor Colorado Springs, CO October 2015 MAJOR ARTERIAL DISEASES ROBERT LUND MD, DBIM Two Main Types of Major Arterial Disease Atherosclerotic Peripheral