Short- and long-term outcomes of the titanium-no stent registry MORRIS MOSSERI - Cardiovascular Revascularization Medicine 6 (2005) 2 6
|
|
|
- Phoebe Lang
- 6 years ago
- Views:
Transcription
1 PUBLICATIONS
2 CONTENTS RANDOMIZED STUDIES Two-year follow-up after percutaneous coronary intervention with titanium-nitride-oxide-coated stents versus paclitaxel-eluting stents in acute myocardial infarction PASI P. KARJALAINEN - Annals of Medicine. 2009, 1-9, ifirst article Titanium-nitride-oxide coated stents versus paclitaxel eluting stents in acute myocardial infarction: a 12-month follow-up report from the TITAX AMI trial P. KARJALAINEN - EuroInterv.2008;4: Randomised comparison of titanium-nitride-oxide coated stents with bare metal stents: five-year follow-up of the TiNOX trial ARIS MOSCHOVITIS - EuroInterv.2010;6:63-68 Randomized Comparison of a Titanium-Nitride-Oxide Coated Stent With a Stainless Steel Stent for Coronary Revascularization: The TiNOX Trial STEPHAN WINDECKER - Circulation. 2005;111: Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio-Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO FERNANDO MENDES SANT ANNA - Rev Bras Cardiol Invas. 2009;17(1):XX-XX. REGISTRIES Five-Year Clinical Outcome of Titanium-Nitride-Oxide-Coated Bioactive Stent Implantation in a Real-World Population: A Comparison with Paclitaxel-eluting Stents: The PORI Registry PASI P. KARJALAINEN - Journal of Interventional Cardiology Vol. **, No. **, 2010 Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population PASI P. KARJALAINEN - Int J Cardiol (2009), doi: /j.ijcard The EXTREME Registry: Titanium-Nitride-Oxide Coated Stents in Small Coronary Arteries RAUL VALDESUSO - Catheterization and Cardiovascular Interventions DOI /ccd. Titanium and Nitride Oxide-Coated Stents and Paclitaxel-Eluting Stents for Coronary Revascularization in an Unselected Population PASI P. KARJALAINEN - J Invasive Cardiol 2006;18: Real world experience with the TITAN stent: a 9-month follow-up report from The Titan PORI Registry PASI P. KARJALAINEN - EuroInterv.2006;2: The Titanium-NO Stent: results of a multicenter registry MORRIS MOSSERI - EuroInterv.2006;2: Short- and long-term outcomes of the titanium-no stent registry MORRIS MOSSERI - Cardiovascular Revascularization Medicine 6 (2005) 2 6 META ANALYSIS Pooled Analysis of Trials Comparing Titanium-Nitride-Oxide-Coated Stents with Paclitaxel-Eluting Stents in Patients Undergoing Coronary Stenting PASI P. KARJALAINEN - J Invasive Cardiol 2010;22: TITAN2 OVERVIEW ARTICLE Titanium-nitride-oxide coated Titan-2 bioactive coronary stent: a new horizon for coronary intervention PASI P. KARJALAINEN - Expert. Rev. Devices 7(5), (2010) Stent coating with titanium-nitride-oxide for prevention of restenosis STEPHAN WINDECKER - EuroInterv.2006;2:
3 Annals of Medicine. 2009, 19, ifirst article ORIGINAL ARTICLE Two-year follow-up after percutaneous coronary intervention with titanium-nitride-oxide-coated stents versus paclitaxel-eluting stents in acute myocardial infarction PASI P. KARJALAINEN 1, ANTTI YLITALO 1, MATTI NIEMELÄ 2, KARI KERVINEN 2, TIMO MÄKIKALLIO 2, MIKKO PIETILÄ 3, JUSSI SIA 4, PETRI TUOMAINEN 5, KAI NYMAN 6 & K. E. JUHANI AIRAKSINEN 3 1 Department of Cardiology, Satakunta Central Hospital, Pori, Finland, 2 Department of Internal Medicine, Division of Cardiology, University of Oulu, Oulu, Finland, 3 Department of Medicine, Turku University Hospital, Turku, Finland, 4 Department of Cardiology, Kokkola Central Hospital, Kokkola, Finland, 5 Department of Internal Medicine, Kuopio University Hospital, Kuopio, Finland, and 6 Department of Medicine, Jyväskylä Central Hospital, Jyväskylä, Finland Abstract Background and aims. The aim of this study was to evaluate the long-term effects of the titanium-nitride-oxide-coated (TITANOX) stent and the paclitaxel-eluting stent (PES) in patients who had undergone a percutaneous coronary intervention for acute myocardial infarction (MI). Methods and results. The TITAX-AMI trial randomly assigned 425 patients with MI to receive either a TITANOX stent or a PES. The primary end-point was a composite of MI, target lesion revascularization, or death from cardiac causes. At 12 months, there was no significant difference between patients receiving TITANOX stent or PES in the rate of primary endpoint (10.3% versus 12.8%, P0.5). After 2 years of follow-up, a significantly lower rate of primary end-point was observed in the TITANOX stent group compared with the PES group (11.2% versus 21.8%, HR 2.2, 95% confidence interval (CI) , P0.004). This difference was driven by a reduced rate of MI (5.1% versus 15.6%, PB0.001) and cardiac death (0.9% versus 4.7%, P0.02) in favour of the TITANOX stent. Definite stent thrombosis occurred in 0.5% and 6.2% of the patients (P0.001), respectively. Conclusions. The implantation of a TITANOX stent resulted in better clinical outcome compared with a PES during 2 years of follow-up among patients treated for acute MI. Key words: Angioplasty, DES, myocardial infarction, paclitaxel, restenosis, stent thrombosis, stenting, titanium Introduction Drug-eluting stents (DES), including the paclitaxeleluting stent (PES), have been shown to improve both early and late outcomes, as compared with bare-metal stents (BMS), predominantly as a result of a reduction in target lesion revascularization (TLR) (1,2). However, most randomized DES trials have excluded patients with acute myocardial infarction (MI), though invasive approach is currently the preferred method for treatment of acute MI (35). Previous trials and meta-analyses demonstrated that the use of DES in patients with acute ST-elevation myocardial infarction (STEMI) is safe and improves clinical outcomes mainly by decreasing the risk of reintervention compared with BMS (613). Non-ST-elevation MI (NSTEMI) and STEMI are usually considered to be different entities, but recent reports suggested that the prognosis of either subgroup of MI is similar despite different management strategies (14,15). The 1-year follow-up of the titanium-nitrideoxide-coated (TITANOX) stents versus paclitaxeleluting stents (PES) in acute MI trial (TITAX-AMI) Correspondence: Pasi P. Karjalainen MD PhD, Department of Cardiology, Satakunta Central Hospital, Sairaalantie 3, FIN-28100, Pori, Finland. Fax: pasi.karjalainen@satshp.fi (Received 11 March 2009; accepted 9 June 2009) ISSN print/issn online # 2009 Informa UK Ltd. DOI: /
4 2 P. P. Karjalainen et al. Key messages. The implantation of a titanium-nitride-oxide-coated (TITANOX) stent resulted in better clinical outcome compared with a paclitaxel-eluting stent (PES) during 2 years of follow-up among patients treated for acute myocardial infarction (MI).. The overall rate of stent thrombosis (ST) was significantly higher in PES-treated patients.. In multivariable analyses, MI, cardiac death, definite ST, and major adverse cardiac events (MACE) were predicted by the use of PES. showed no significant superiority of PES compared to TITANOX stents in MI (16). The TITAX-AMI trial indicated a higher rate of stent thrombosis (ST) in patients receiving PES. The present analysis was performed to evaluate whether clinical outcomes of TITANOX stents and PES will differ at 2 years after stent implantation for MI. The occurrence of serious adverse events caused by very late ST was the other principal interest in this analysis. There have been concerns about the safety of DES, e.g. most notably late ST. For on-label use, identical rates of ST were observed in both selected DES and BMS patients after up to 4 years according to pooled analyses of randomized DES trials (17,18). It has been postulated that delayed endothelialization and DES malapposition may lead to late ST resulting in MI or death (19). In addition, vessel healing at the culprit site in MI patients treated with DES is substantially delayed compared with the lesion site in patients receiving DES for stable angina, emphasizing the importance of the arterial response to DES (20). On the other hand, new strategies with BMS technology have also been aimed at enhanced vascular healing. The TITANOX stent seems to decrease acute surface thrombogenicity (2124) and reduce in-stent restenosis when compared with conventional stainless steel stents (21). We designed a randomized trial to determine whether TITANOX stents are safe compared to PES in the setting of acute MI as measured by major adverse cardiac events (MACE) at 2-year follow-up. Material and methods Study design and patient population The design of the original study has been previously reported (16). Briefly, the TITAX-AMI Abbreviations ARC Academic Research Consortium BMS bare-metal stent CI confidence interval DES drug-eluting stent HR hazard ratio MACE major adverse cardiac events MI myocardial infarction NSTEMI non-st-elevation myocardial infarction PCI percutaneous coronary intervention PES paclitaxel-eluting stent ST stent thrombosis STEMI ST-elevation myocardial infarction TIMI thrombolysis in myocardial infarction TITANOX titanium-nitride-oxide TLR target lesion revascularization (Titanium-Nitride-Oxide-Coated Stents versus Paclitaxel-Eluting Stents in Acute Myocardial Infarction) trial is a prospective, randomized, and multicentre trial conducted from December 2005 to November 2006 in six Finnish hospitals. The study was initiated by the investigators and conducted according to the declaration of Helsinki, and written informed consent was obtained from all patients. The study protocol was approved by the Ethics Committees of the co-ordinating centre, Satakunta Central Hospital, and the participating hospitals. The study has been registered in www. clinicaltrials.gov, number NCT All patients 18 years of age presenting with acute MI were eligible for this trial. Diagnostic criteria for NSTEMI included symptoms and signs of myocardial ischaemia, dynamic ECG changes, and detection of rise and/or fall of cardiac biomarkers (troponin) with at least one value above the 99th percentile of upper reference limit. STEMI was diagnosed if the patient had chest pain at rest 20 minutes and persistent ]1 mm of ST-segment elevation in at least two contiguous limb leads or ]2 mm in two contiguous precordial leads. Exclusion criteria included unprotected left main disease, ostial or restenotic lesions, contraindication to aspirin, clopidogrel, or heparins, life expectancy of less than 12 months, and need for a stent longer than 28 mm. According to the trial protocol, randomization was performed after visualization of the culprit lesion or a totally occluded infarct-related vessel during coronary angiography. Patients were randomly assigned to the study groups in a 1:1 fashion.
5 TITANOX stent versus PES in acute MI 3 Procedures and clinical follow-up Lesions were treated according to current interventional techniques, with the final strategy left entirely up to the operator s discretion. Angiographic success was defined as a residual stenosis B30% by visual analysis in the presence of thrombolysis in myocardial infarction (TIMI) flow grade 3. If more than one stent was needed, stents of the same type as the assigned stent were recommended. The study protocol recommended premedication with aspirin (dose mg) or a loading dose of intravenous aspirin ( mg), and clopidogrel before the procedure. If clopidogrel was not utilized before the procedure, a loading dose of mg of clopidogrel was administered immediately after the index procedure. Administration of intravenous heparin, low-molecular-weight heparin, bivalirudin, and glycoprotein IIb/IIIa receptor inhibitors were left to the investigator s discretion. The TITANOX stent (Titan-2, Hexacath, Paris, France) is a thin strut balloon expandable stent made of stainless steel and coated by plasma-enhanced vapour deposition of titanium in a prespecified gas mixture of nitrogen and oxygen in a vacuum chamber (2224). The PES (Taxus-Liberte, Boston Scientific, Natick, Massachusetts, USA) is comprised of a stainless steel stent platform, a polyolefin polymer derivative, and a microtubular stabilizing agent paclitaxel, with two-phase 30-day polymeric release kinetics that provide antiproliferative effect (2). Paclitaxel release is completed within 30 days of implantation, although a substantial portion (90%) of the paclitaxel remains within the polymer indefinitely. At discharge, 100 mg of aspirin daily indefinitely and 75 mg of clopidogrel daily for at least 6 months were prescribed for all patients. We recorded adverse events during hospitalization, and clinical follow-up was performed at 12 and 24 months. Primary and secondary end-points The primary end-point was the first occurrence of MACE within 1 year defined as the composite of TLR, recurrent MI, or death from cardiac causes. The 2-year analysis was prespecified per the protocol (follow-up data were planned to be collected yearly up to 5 years after randomization). TLR was defined as a repeat percutaneous intervention of the target lesion to treat a stenosis (50%) within the stent or in the segments 5 mm distal or proximal to the stent, driven by clinical symptoms and/or signs of myocardial ischaemia, or by-pass surgery of the target vessel due to in-stent restenosis or other complications of the target lesion. Myocardial reinfarction during the follow-up was diagnosed when a rise in the myocardial injury marker level (troponin I or T) above the upper reference limit was detected together with symptoms suggestive of acute myocardial ischaemia. For the diagnosis of myocardial reinfarction during the index hospitalization, a new rise 50% above the previously measured injury marker level was required. Cardiac death was defined as any death due to cardiac causes, unwitnessed death, or death of unknown causes. The secondary end-points of the trial included all-cause mortality, composite of cardiac death or reinfarction and ST. According to the protocol, ST was diagnosed in the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent, or in autopsy. ST was categorized as acute (B24 hours after the stenting), subacute (130 days after the stenting), or late (30 days after the stenting). Additionally, we agreed to use the definition of ST according to the Academic Research Consortium (ARC) classification as definite, probable, or possible (25). Blinded outcome assessment was performed by the independent clinical event committee. Statistical analysis The overall sample size calculation for this clinical trial has been previously reported (16). Briefly, because of the exploratory nature of the study and the consequent lack of prior knowledge about the effect size, the sample size calculation was based on analysis of the results of published registry data of TITANOX stents and PES in the real world clinical practice (22). In this registry, the incidence of MACE at 12 months in patients presenting with acute MI was 7% in the TITANOX stent group and 15% in the PES group. Given the above assumption, we estimated that a total of 200 patients would be required in each group to provide 80% power at the 5% level of significance to detect this difference of 8% in MACE between the study groups. Continuous variables are presented as means (SD), and study groups were compared by Student s unpaired t test. Categorical variables are presented as counts and percentages and were compared by the chi-square or Fisher s exact test. Univariate and multivariable logistic regression analyses were performed to identify independent predictors for MACE, TLR, cardiac death, and ST during the 2 years of follow-up. Because of multiple testing only variables with a two-sided PB0.05 in the univariate analysis were entered into multivariable models. A two-sided P-value B0.05 was required for statistical significance. The rates of MACE- and MI-free survival during the 2-year follow-up period were
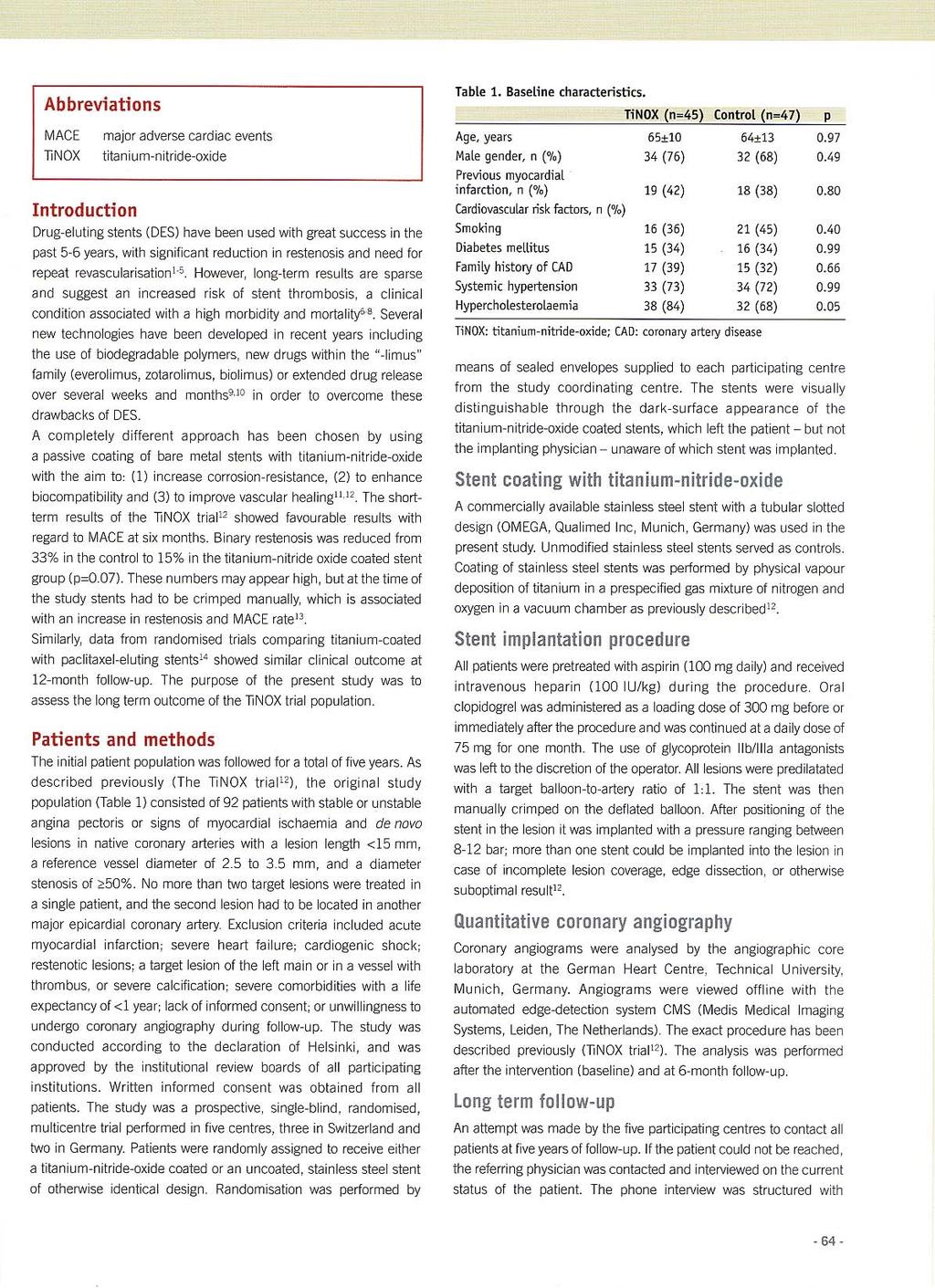
6 4 P. P. Karjalainen et al. estimated with the Kaplan-Meier method. The significance of differences between treatment groups was assessed by the log-rank test. All data were analysed with the use of SPSS version 11 (26). All analyses were done on the basis of intentionto-treat principle. The authors had full access to the data and take responsibility for its integrity. All authors have read and agreed to the manuscript as written. Results Baseline and procedural characteristics During the study period, 840 eligible patients (368 STEMI and 472 NSTEMI patients) were screened for participation in the trial. A total of 425 patients (51%) fulfilled the inclusion criteria and were randomized to the two treatment groups (214 to the TITANOX group and 211 to the PES group). Baseline characteristics of both study groups were well matched, except by a higher incidence of previous percutaneous coronary interventions (PCIs) in the TITANOX group (Table I). The baseline angiographic variables and procedural characteristics are presented in Table II. Procedural success was achieved in 99.5% of patients in the TITANOX group and in 98.1% in the PES group. Table I. Baseline clinical characteristics in TITANOX group versus PES group. TITANOX (n214) PES (n211) Age, y (SD) Male sex, n (%) 162 (76) 157 (74) 0.82 Risk Factors, n (%) Family history of CAD 103 (48) 95 (45) 0.56 Diabetes 48 (22) 33 (16) 0.08 Hypertension 122 (57) 106 (50) 0.17 Hypercholesterolaemia 141 (66) 151 (72) 0.21 History of smoking 113 (53) 97 (46) 0.18 Medical History, n (%) Myocardial infarction 33 (15) 20 (9) 0.08 PCI 22 (10) 10 (5) 0.04 CABG 16 (7) 13 (6) 0.70 Medication, n (%) Clopidogrel before PCI 44 (21) 39 (18) 0.63 Thrombolysis 26 (12) 40 (19) 0.06 GP IIb/IIIa inhibitors 116 (54) 96 (45) 0.08 Indication for PCI, n (%) NSTEMI 131 (61) 114 (54) 0.14 STEMI 83 (39) 97 (46) 0.14 CADcoronary artery disease; CABGcoronary artery by-pass grafting; GPglycoprotein. Other abbreviations are explained in the List of Abbreviations. P Clinical outcome Complete clinical follow-up data at 2 years was obtained for all patients 95% (HR 2.5, 95% CI). The cumulative incidence of MACE was 11.2% in the TITANOX group and 21.8% in the PES group (hazard ratio (HR) 2.2, 95% confidence interval (CI) , P 0.004) (Table III). This difference in MACE was driven by a reduced rate of MI (5.1% versus 15.6%, P B0.001) and cardiac death (0.9% versus 4.7%, P0.02) in favour of the TITANOX stent. Definite SToccurred in 0.5% of patients in the TITANOX group and in 6.2% of patients in the PES group (P0.001). When using ARC classification, we observed a significantly lower rate of ST in the TITANOX group (0.9% versus 8.5%, respectively, P B0.001). In 8 patients, clopidogrel was prematurely discontinued before the event of ST, and all of these patients were in the PES group (Figure 1). Four patients out of 14 (29%) who suffered ST died. A total of 245 patients presented with NSTEMI before the index procedure (131 patients in the TITANOX group versus 114 in the PES group). The rate of MACE (16.7% in NSTEMI patients versus 16.1% in STEMI patients, P 0.9), MI, cardiac death, and TLR were similar in these two subgroups of patients during the 2 years of followup. Furthermore, the rate of ST was comparable in these two subgroups of patients (2.0% versus 5.0%, P 0.1, respectively). Clopidogrel was prescribed at discharge for a mean period of 7.6 months in the TITANOX group and of 10.0 months in the PES group (PB0.001). A total of 67 patients (31%) in the TITANOX group and 138 patients (65%) in the PES group were receiving dual antiplatelet therapy with aspirin and clopidogrel at the time of the 12-month follow-up (P B0.001). In the present trial, there were no extended clopidogrel treatments beyond 12 months in either study groups. In multivariable analysis, the use of PES was an independent predictor of recurrent MI (HR 4.0, 95% CI , PB0.001), as well as of cardiac death (HR 5.9, 95% CI , P0.02), definite ST (HR 14.5, 95% CI , P 0.01), and MACE (HR 2.5, 95% CI , P0.002) after 2 years of follow-up (Table IV). Discussion Main study findings To our knowledge, the TITAX-AMI trial is the first head-to-head randomized comparison of the TITA- NOX stent and PES among patients presenting with
7 TITANOX stent versus PES in acute MI 5 Table II. Baseline angiographic variables and procedural characteristics. TITANOX (n214) PES (n211) P Lesion characteristics Left anterior descending artery, n (%) 98 (46) 91 (43) 0.63 Bifurcated lesion, n (%) 53 (25) 50 (24) 0.82 Reference diameter, (mm, SD) Lesion length, (mm, SD) TIMI flow grade, n (%) 0 46 (21) 45 (21) (5) 14 (7) (29) 38 (18) (45) 114 (54) 0.08 Procedural characteristics Direct stenting, n (%) 26 (12) 32 (15) 0.48 Post-dilatation, n (%) 89 (42) 73 (35) 0.16 Nominal stent size (mm, SD) Stent length (mm, SD) Total stent length (mm, SD) No. of stents implanted per culprit lesion (SD) Final TIMI flow grade 3, n (%) 211 (98.6) 204 (96.7) 0.22 Multivessel PCI, n (%) 30 (14) 19 (9) 0.13 Maximum creatine kinase MB (mg/litre) a Maximum troponin I (mg/litre) b Maximum troponin T (mg/litre) c a Available in 145 patients in TITANOX group and in 141 patients in PES group. b Available in 140 patients in TITANOX group and in 145 patients in PES group. c Available in 72 patients in TITANOX group and in 61 patients in PES group. Abbreviations are explained in the List of Abbreviations. acute MI. The main finding of this trial is a significantly higher rate of MI, cardiac death, and overall MACE in patients who received PES. Secondly, the overall rate of ST was significantly higher in PES-treated patients. In multivariable analyses, MI, cardiac death, definite ST, and MACE were predicted by the use of PES. Previous studies The STRATEGY, TYPHOON, and SESAMI trials compared sirolimus-eluting stent (SES) to BMS in the clinical setting of acute STEMI. The 1-year follow-up of these trials indicated a significant benefit of SES over BMS (68). However, longerterm follow-up data from the TYPHOON and SESAMI trials are lacking. In the STRATEGY trial, the cumulative incidence of MI, death, and target vessel revascularization at 2 years was 24.2% in patients who received SES (27), which is comparable to our findings when using PES in acute MI. As for the use of PES, the PASSION trial showed no significant superiority of PES compared to BMS after 2 years of follow-up, although there was a trend towards a lower rate of TLR in the PES group (28). In the present trial, the cumulative incidence of primary end-points in the PES group was 21.8%, which is in contrast to the results from the PASSION trial (11.2%). There are various salient differences between the TITAX-AMI trial and previous MI trials (TY- PHOON/PASSION). The present trial included patients with NSTEMI and STEMI, whereas previous studies included only patients with STEMI. Therefore it may be difficult to compare the present study with the STEMI studies. However, recent reports suggest that the prognosis of NSTEMI and STEMI are similar despite different management strategies (14,15). The BASKET-LATE trial reported a trend towards a higher rate of death or recurrent MI in patients treated with DES after thienopyridine discontinuation as compared with BMS (29). This observation is in line with the findings of the present trial, since after the clopidogrel withdrawal we observed a significantly higher incidence of thrombotic events in the PES group compared to the TITANOX group (i.e. MI, definite ST, and MACE). Stent thrombosis In the present study, the incidence of definite ST was 6.2% in the PES group, which is higher than in the PASSION trial (2.1%) (28). On the other hand,
8 6 P. P. Karjalainen et al. Table III. Clinical events during 2 years of follow-up. TITANOX (n214) PES (n211) HR 95% CI P MI, n (%) Patient with any event 11 (5.1) 33 (15.6) B to 12 months after index PCI 9 (4.2) 17 (8.1) to 24 months after index PCI 2 (0.9) 16 (7.6) Cardiac death, n (%) Patient with any event 2 (0.9) 10 (4.7) to 12 months after index PCI 1 (0.5) 4 (1.9) to 24 months after index PCI 1 (0.5) 6 (2.8) TLR, n (%) Patient with any event 20 (9.3) 21 (10.0) to 12 months after index PCI 20 (9.3) 15 (7.1) to 24 months after index PCI 0 (0) 6 (2.8) 0.01 MACE, n (%) Patient with any event 24 (11.2) 46 (21.8) to 12 months after index PCI 22 (10.3) 27 (12.8) to 24 months after index PCI 2 (0.9) 19 (9.0) B0.001 ST, n (%) a Patient with any event 1 (0.5) 13 (6.2) to 12 months after index PCI 1 (0.5) 7 (3.3) to 24 months after index PCI 0 (0) 6 (2.8) 0.01 ST according to ARC, n (%) b Patient with any event 2 (0.9) 18 (8.5) B to 12 months after index PCI 2 (0.9) 9 (4.3) to 24 months after index PCI 0 (0) 9 (4.3) MI or cardiac death, n (%) 11 (5.1) 40 (19.0) B0.001 All-cause death, n (%) Patient with any event 10 (4.7) 15 (7.1) to 12 months after index PCI 5 (2.3) 6 (2.8) to 24 months after index PCI 5 (2.3) 9 (4.3) a Per protocol stent thrombosis. b Stent thrombosis defined according to Academic Research Consortium (ARC) classification. HRhazard ratio; CIconfidence interval. Other abbreviations are explained in the List of Abbreviations. after the 2 years of follow-up, the incidence of definite ST in the TITANOX group was low (0.5%), especially considering the thrombotic environment at the time of the stent deployment and the inclusion of patients with thrombolysis therapy in the present trial. Recently, a rate of infarct-related artery ST (3.2%) in STEMI patients at 2 years was reported (30). This analysis also demonstrated a remarkably high incidence of ST (8.2%) in patients with a large thrombus burden before the stent implantation. A higher rate of late ST was observed in MI patients than in stable patients in post-mortem analysis of patients who died after DES implantation (20). This analysis suggests that the culprit lesion morphology influences local vascular healing after DES placement. Greater delay in arterial healing as manifested by poor endothelialization and persistent peristrut fibrin deposition may extend the risk of ST far beyond 30 days after DES implantation. Late ST is potentially due to a mismatch between the stent and the vessel and may be related to stent malapposition, overlapping stent placement, penetration of necrotic core, excessive stent length, bifurcation lesions, hypersensitivity to drug or polymer, or thrombogenic surface (19,31). Premature antiplatelet therapy discontinuation has been the most important predisposing factor for late ST (29), which was also seen in the present trial. Previously, late ST was reported to occur at an annual rate of 0.6% up to 4 years after DES implantation (32,33), while acute coronary syndrome and PES implantation were associated with late ST (32). New strategies with BMS technology have also been aimed at enhanced vascular healing. Titanium features better biocompatibility when compared with stainless steel, gold, or other surface coatings (34). In vitro titanium-nitride-oxide showed diminished platelet adhesion and fibrinogen binding in comparison to stainless steel. In addition, metallic sheaths coated with titanium-nitride or titaniumoxide exhibited higher cell density values on their
9 TITANOX stent versus PES in acute MI 7 Figure 1. Antiplatelet utilization at the time of the outcome event of definite stent thrombosis (ST). A: Antiplatelet therapy in 14 patients suffering definite ST. B: Time of the event and the utilization of clopidogrel during the definite ST. a Dual antiplatelet therapy with aspirin and clopidogrel. Dark colour indicates the duration of clopidogrel withdrawal. surface compared to those without coating, supporting the view that deployment of stents with these coatings may achieve earlier complete endothelial coverage (35). These findings reinforce our present report demonstrating a lower incidence of MI and late ST in TITANOX stent-treated patients compared with PES-treated patients. Study limitations The sample size was based on a small real-life cohort, and therefore the present trial is underpowered to reveal potential small differences in primary and individual end-points, although we chose the setting of acute MI known to predispose to clinical complications. The design of our study did not include angiographic follow-up or routine non-invasive testing for myocardial ischaemia, and therefore we probably underestimated the incidence of silent or angiographic restenosis. On the other hand, by relying on clinical follow-up only, the chance of unnecessary TLR due to the oculostenotic reflex or patient s unjustified anxiety was avoided. In addition, the stenting was performed in patients with relatively large infarct-related arteries with low risk of in-stent restenosis. Conclusions In conclusion, the implantation of TITANOX stents resulted in better clinical outcome compared with PES during 2 years of follow-up among patients treated for acute MI. Acknowledgements The authors thank Tuija Vasankari, RN, Eija Niemelä, RN, and Marja-Liisa Sutinen, RN, for their support in the conduct of this study. Funding sources: This work (Dr Airaksinen) was supported by grants from the Finnish Foundation for Cardiovascular Research, Helsinki, Finland. Clinical trial registration information: URL: clinicaltrials.gov. Unique identifier: NCT
10 8 P. P. Karjalainen et al. Table IV. Independent predictors of clinical outcomes. Variable HR 95% CI P Myocardial infarction a Previous CABG B0.001 PES B0.001 Culprit lesion in LAD Cardiac death b PES Previous CABG MACE c PES Hypercholesterolaemia Reference vessel diameter Lesion in bifurcation Definite ST d Culprit lesion in LAD PES Nominal stent diameter a Additional variables entered in the multivariable model but not found to be significant were: nominal stent diameter, lesion in bifurcation, and reference vessel diameter. b Additional variable entered in the multivariable model but not found to be significant was: age. c Additional variables entered in the multivariable model but not found to be significant were: nominal stent diameter, culprit lesion in LAD, and female gender. d Additional variables entered in the multivariable model but not found to be significant was: reference vessel diameter. HRhazard ratio; CABGcoronary artery by-pass grafting; CIconfidence interval; LADleft anterior descending artery. Other abbreviations are explained in the List of Abbreviations. Declaration of interest: All authors state that no conflict of interest exists. References 1. Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O Shaughnessy C, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349: Stone GW, Ellis SG, Cox DA, Hermiller J, O Shaughnessy C, Mann JT, et al. One-year clinical results with the slow-release, polymer-based, paclitaxel-eluting TAXUS stent: the TAXUS-IV trial. Circulation. 2004;109: Silber S, Albertson P, Aviles FF, Camici PG, Colombo A, Hamm C, et al. Guidelines for percutaneous coronary interventions. The task force for percutaneous coronary interventions of the European society of cardiology. Eur Heart J. 2005;26: Mehta SR, Cannon CP, Fox KA, Wallentin L, Boden WE, Spacek R, et al. Routine vs selective invasive strategies in patients with acute coronary syndromes: a collaborative metaanalysis of randomized trials. JAMA. 2005;293: Boersma E; The Primary Coronary Angioplasty vs. Thrombolysis (PCAT)-2 Trialist Collaborative Group. Does time matter? A pooled analysis of randomized clinical trials comparing primary percutaneous coronary intervention and in-hospital fibrinolysis in acute myocardial infarction patients. Eur Heart J. 2006;27: Valgimigli M, Percoco G, Malagutti P, Campo G, Ferrari F, Barbieri D, et al. Tirofiban and sirolimus-eluting stents vs abciximab and bare-metal stent for acute myocardial infarction. JAMA. 2005;293: Spaulding C, Henry P, Teiger E, Beatt K, Bramucci E, Carrie D, et al. Sirolimus-eluting versus uncoated stents in acute myocardial infarction. N Engl J Med. 2006;355: Menichelli M, Parma A, Pucci E, Fiorilli R, De Felice F, Nazzaro M, et al. Randomized trial of sirolimus-eluting stent versus bare-metal stent in acute myocardial infarction (SE- SAMI). J Am Coll Cardiol. 2007;49: Laarman GJ, Suttorp MJ, Dirksen MT, van Heerebeek L, Kiemeneij F, Slagboom T, et al. Paclitaxel-eluting versus uncoated stents in primary percutaneous coronary intervention. N Engl J Med. 2006;355: Tanimoto S, Tsuchida K, Daemen J, Boersma E. Drugeluting stent implantation in acute myocardial infarction. Do we need another randomised trial? EuroIntervention. 2006;2: Pasceri V, Patti G, Speciale G, Pristipino C, Richichi G, Di Sciascio G. Meta-analysis of clinical trials on use of drugeluting stents for treatment of acute myocardial infarction. Am Heart J. 2007;153: Moreno R, Spaulding C, Laarman GJ, Tierala I, Kaiser CA, Lopez-Sendon J-L. Effectiveness and safety of paclitaxeleluting stents in patients with ST-segment elevation acute myocardial infarction. EuroIntervention. 2007;3: Kastrati A, Dibra A, Spaulding C, Laarman GJ, Menichelli M, Valgimigli M, et al. Meta-analysis of randomized trials on drug-eluting stents vs. bare-metal stents in patients with acute myocardial infarction. Eur Heart J. 2007;28: Terkelsen CJ, Lassen JF, Norgaard BL, Gerdes JC, Jensen T, Gotzsche L, et al. Mortality rates in patients with STelevation vs. non-st-elevation acute myocardial infarction: observations from an unselected cohort. Eur Heart J. 2005;26: Montalescot G, Dallongeville J, van Belle E, Rouanet S, Baulac C, Degrandsart A, et al. STEMI and NSTEMI: are they so different? 1 year outcomes in acute myocardial
11 TITANOX stent versus PES in acute MI 9 infarction as defined by the ESC/ACC definition (the OPERA registry). Eur Heart J. 2007;28: Karjalainen P, Ylitalo A, Niemelä M, Kervinen K, Mäkikallio T, Pietilä M, et al. Titanium-nitride-oxide coated stents versus paclitaxel-eluting stents in acute myocardial infarction: A 12-month follow-up report from the TITAX AMI trial. EuroIntervention. 2008;4: Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice M-C, et al. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med. 2007;356: Mauri L, Hsieh W, Massaro JM, Ho K, D Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drugeluting stents. N Engl J Med. 2007;356: Finn AV, Nakazawa G, Joner M, Kolodgie FD, Mont EK, Gold HK, et al. Vascular responses to drug eluting stents. Importance of delayed healing. Arterioscler Thromb Vasc Biol. 2007;27: Nakazawa G, Finn AV, Joner M, Ladich E, Kutys R, Mont EK, et al. Delayed arterial healing and increased late stent thrombosis at culprit sites after drug-eluting stent placement for acute myocardial infarction patients. Circulation. 2008;118: Windecker S, Simon R, Lins M, Klauss V, Eberli FR, Roffi M, et al. Randomized comparison of a titanium-nitride oxide-coated stent with a stainless steel stent for coronary revascularization. The TINOX trial. Circulation. 2005;111: Karjalainen PP, Ylitalo A, Airaksinen KEJ. Titanium and nitride oxide coated stents and paclitaxel eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol. 2006;18: Karjalainen P, Ylitalo A, Airaksinen KEJ. Real world experience with TITAN stent: A 9-month follow-up report from the Titan PORI Registry. EuroIntervention. 2006;2: Mosseri M, Miller H, Tamari I, Plich M, Hasin Y, Brizines M, et al. The titanium-no stent: results of a multicenter registry. EuroIntervention. 2006;2: Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es G-A, et al. Clinical end points in coronary stent trials. A case for standardized definitions. Circulation. 2007;115: Buehl A, Zoefel P. SPSS 11: Introduction in modern data analysis, 8th ed. Munich, Germany: Addison-Wesley, Valgimigli M, Campo G, Arcozzi C, Malagutti P, Carletti R, Ferrari F, et al. Two-years clinical follow-up after sirolimuseluting versus bare-metal stent implantation assisted by systematic glycoprotein IIb/IIIa inhibitor infusion in patients with myocardial infarction. Results from the STRATEGY study. J Am Coll Cardiol. 2007;50: Dirksen MT, Vink MA, Suttorp MJ, Tijssen JGP, Patterson MS, Slagboom T, et al. Two year follow-up after primary PCI with a paclitaxel-eluting stent versus a bare-metal stent for acute ST-elevation myocardial infarction (the PASSION trial): a follow-up study. EuroIntervention. 2008;4: Pfisterer M, Brunner-La Rocca HP, Buser PT, Rickenbacher P, Hunziker P, Mueller C, et al. Late clinical events after clopidogrel discontinuation may limit the benefit of drugeluting stents. An observational study of drug-eluting versus bare-metal stents (BASKET-LATE). J Am Coll Cardiol. 2006;48: Sianos G, Papafaklis MI, Daemen J, Vaina S, van Mieghem CA, van Domburg RT, et al. Angiographic stent thrombosis after routine use of drug-eluting stents in ST-elevation myocardial infarction. J Am Coll Cardiol. 2007;50: Virmani R, Guagliumi G, Farb A, Musumeci G, Grieco N, Motta T, et al. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: should we be cautious? Circulation. 2004;109: Wenaweser P, Daemen J, Zwahlen M, van Domburg R, Juni P, Vaina S, et al. Incidence and correlates of drug-eluting stent thrombosis in routine clinical practice. J Am Coll Cardiol. 2008;52: Daemen J, Wenaweser P, Tsuchida K, Abrecht L, Vaina S, Morger C, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study. Lancet. 2007;369: Giraud-Sauveur Y. Titan 2 bio-active stent (BAS) with titanium-no. EuroIntervention. 2007;3: Yeh HI, Lu SK, Tian TY, Hong RC, Lee WH, Tsai CH. Comparison of endothelial cells grown on different stent materials. J Biomed Mater Res. 2006;76:83541.
12 Clinical research Titanium-nitride-oxide coated stents versus paclitaxeleluting stents in acute myocardial infarction: a 12-months follow-up report from the TITAX AMI trial Pasi P. Karjalainen 1 *, MD, PhD; Antti Ylitalo 1, MD, PhD; Matti Niemelä 2, MD, PhD; Kari Kervinen 2, MD, PhD; Timo Mäkikallio 2, MD, PhD; Mikko Pietilä 3, MD, PhD; Jussi Sia 4, MD; Petri Tuomainen 5, MD, PhD; Kai Nyman 6, MD; K.E. Juhani Airaksinen 3, MD, PhD 1. Department of Cardiology, Satakunta Central Hospital, Pori, Finland; 2. Department of Internal Medicine, Division of Cardiology, University of Oulu, Oulu, Finland; 3. Department of Medicine, Turku University Hospital, Turku, Finland; 4. Department of Cardiology, Kokkola Central Hospital, Kokkola, Finland; 5. Department of Internal Medicine, Kuopio University Hospital, Kuopio, Finland; 6. Department of Medicine, Jyväskylä Central Hospital, Jyväskylä, Finland The authors have no conflict of interest to declare. KEYWORDS Myocardial infarction, titanium, paclitaxel, restenosis, stent thrombosis Abstract Aims: The aim of this study was to evaluate the effectiveness of titanium-nitride-oxide (TITANOX) -coated stent and paclitaxel-eluting stent (PES) in patients presenting with acute myocardial infarction (MI). Methods and results: A total of 425 patients presenting with acute non-st-elevation MI or ST-elevation MI were randomly assigned to receive TITANOX-coated stent or PES. The primary end point was a composite of MI, target lesion revascularisation (TLR) or death from cardiac causes. At 12 months, there was no significant difference between patients receiving TITANOX-coated stent or PES in the rates of primary end point (10.3% vs. 12.8%, P=0.5), MI (4.2% vs. 8.1%, P=0.1), or TLR (9.3% vs. 7.1%, P=0.5), respectively. The incidence of stent thrombosis, defined according to Academic Research Consortium classification, was significantly lower in the TITANOX group compared to the PES group (0.9% vs. 4.3%, P=0.03). Conclusions: TITANOX-coated stent and PES resulted in comparable clinical outcomes during 12 months follow-up among patients treated for acute MI. * Corresponding author: Satakunta Central Hospital, Sairaalantie 3, 28500, Pori, Finland pasi.karjalainen@satshp.fi Europa Edition All rights reserved. EuroInterv.2008;4:
13 TITAX AMI trial 12-month follow-up Introduction Drug-eluting stents (DES) have been shown to reduce in-stent restenosis after percutaneous coronary intervention (PCI) compared to bare metal stents (BMS). 1,2 However, most randomised DES trials have excluded patients with acute myocardial infarction (MI), though invasive approach is currently the preferred method for treatment of acute MI. 3-9 Five randomised trials and four meta-analyses of the clinical trials on the use of DES for treatment of acute ST-elevation MI (STEMI) demonstrated that the use of DES in patients with acute STEMI is safe and improves clinical outcomes mainly by decreasing the risk of reintervention compared with BMS However, in acute MI, the use of DES is still considered to be an off-label indication. Non-ST-elevation MI (NSTEMI)and STEMI are usually considered to be different entities, but recent reports suggested that the prognosis of either subgroup of MI is similar despite different management strategies. 19,20 Recently, there have been concerns about the safety of DES e.g. most notably stent thrombosis (ST). For on-label use, identical rates of ST were observed in both selected DES and BMS patients up to four years according to pooled analyses of randomised DES trials. 21,22 On the other hand, stent coating with compounds like titanium-nitride-oxide seem to decrease acute surface thrombogenicity, and reduce in-stent restenosis when compared with conventional stainless steel stents. 23 Moreover, titanium-nitride-oxide-coated stent (TITANOX) are associated with comparable clinical outcomes compared to paclitaxel-eluting stent (PES) in the real world clinical practice of high-risk patients. 24 We designed a prospective, randomised, multicentre trial with the main purpose of evaluating the effectiveness of TITANOX-coated stents and PES in patients presenting with acute MI. We report 12 months follow-up results of the trial. Methods Study design and patient population The TITAX AMI (titanium-nitride-oxide coated stents versus paclitaxel-eluting stents in acute myocardial infarction) trial is a prospective, randomised, multicentre trial conducted from December 2005 to November 2006 in six Finnish hospitals. The study was initiated by the investigators and conducted according to the declaration of Helsinki and written informed consent was obtained from all patients. Study protocol was approved by the Ethics Committees of the coordinating centre Satakunta Central Hospital and the participating hospitals. Patients >18 years of age presenting with acute MI were eligible for this trial. Diagnostic criteria for NSTEMI included symptoms and signs of myocardial ischaemia, dynamic ECG changes and detection of rise and/or fall of cardiac biomarkers (troponin) with at least one value above the 99th percentile of upper reference limit. STEMI was diagnosed if patient had chest pain at rest >20 minutes and persistent > 1 mm of ST-segment elevation in at least two contiguous limb leads or > 2 mm in two contiguous precordial leads. All patients receiving thrombolysis therapy were eligible for the trial, and it was recommended to perform intra-coronary stenting <24 hours after the admission. Exclusion criteria included unprotected left main disease, ostial or restenotic lesions, contraindication to aspirin, clopidogrel or heparins, life expectancy of less than 12 months and need for a stent longer than 28 mm. According to the trial protocol, randomisation was performed after visualisation of the culprit lesion or a totally occluded infarct-related vessel during coronary angiography. Patients were randomly assigned to the study groups in a 1:1 fashion. Procedures and clinical follow-up Culprit lesions were treated according to current interventional techniques, with the final strategy (thrombectomy devices, direct stenting, postdilatation, intravascular ultrasound) left entirely up to the operator s discretion. Angiographic success was defined as a residual stenosis <30% by visual analysis in the presence of thrombolysis in myocardial infarction (TIMI) flow grade 3. If more than one stent was needed, stents of the same type as the assigned stent were recommended. The study protocol recommended premedication with aspirin (dose mg) or a loading dose of intravenous aspirin ( mg), and clopidogrel before the procedure. If clopidogrel was not utilised before the procedure, a loading dose of mg of clopidogrel was administered immediately after the index procedure. Administration of intravenous heparin, low-molecular-weight-heparin, bivalirudin and glycoprotein IIb/IIIa-receptor inhibitors were left to the investigator s discretion. Titan (Hexacath, Paris, France) stent is a thin strut balloon expandable stent made of stainless steel and coated with TITANOX by plasma enhanced vapour deposition of titanium in a prespecified gas mixture of nitrogen and oxygen in a vacuum chamber TITANOX-coated stents were available in lengths of 7, 10, 13, 16, 19, 22 and 28 mm, and in diameters of 2, 2.25, 2.50, 2.75, 3.0, 3.5, 4.0 and 4.5 mm. Taxus-Liberte stent (Boston Scientific, Natick, MA, USA) is comprised of a stainless steel stent platform, a polyolefin polymer derivative, and a microtubular stabilising agent paclitaxel, with two-phase 30-day polymeric release kinetics that provides antiproliferative effect. 2 Paclitaxel release is completed within 30 days of implantation, although a substantial portion (>90%) of the paclitaxel remains within the polymer indefinitely. PES s were available in lengths of 8, 12, 16, 20, 24, and 28 mm, and in diameters of 2.25, 2.50, 2.75, 3.0, 3.5, 4.0 and 4.5 mm. At discharge, 100 mg of aspirin daily indefinitely and 75 mg of clopidogrel daily at least six months were prescribed for all patients. We recorded adverse events during hospitalisation and clinical follow-up was performed at 30 days, and six and 12 months. Primary and secondary end points The primary end point was the first occurrence of major adverse cardiac event (MACE) at 12 months defined as the composite of target lesion revascularisation (TLR), recurrent MI, or death from cardiac causes. TLR was defined as a repeat percutaneous intervention of the target lesion to treat a stenosis (>50%) within the stent or in the segments 5 mm distal or proximal to the stent, driven
14 Clinical research by clinical symptoms and/or signs of myocardial ischaemia, or bypass surgery of the target vessel due to the in-stent restenosis or other complications of the target lesion. Myocardial reinfarction during the follow-up was diagnosed when a rise in the myocardial injury marker level (troponin I or T) >upper reference limit was detected together with symptoms suggestive of acute myocardial ischaemia. For the diagnosis of myocardial reinfarction during the index hospitalisation, a new rise >50% above the previously measured injury marker level was required. Cardiac death was defined as any death due to cardiac causes, unwitnessed death or death of unknown causes. The secondary endpoints of the trial included all-cause mortality, composite of cardiac death or reinfarction and ST. According to the protocol, ST was diagnosed in the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent, or in autopsy. ST was categorised as acute (<24 hours after the stenting), subacute (1-30 days after the stenting), or late (>30 days after the stenting). Additionally, we agreed to use the definition of ST according to the Academic Research Consortium (ARC) classification as definite, probable, or possible. 27 Blinded outcome assessment was performed by the independent clinical event committee. Statistical analysis In the current literature, there are no published data on the utilisation of TITANOX-coated stent or PES in the setting of acute MI comprising both NSTEMI and STEMI. Because of the exploratory nature of the study and the consequent lack of a prior knowledge about the effect size, the sample size calculation was based on subgroup analysis of the results of previously published registry data of TITANOX-coated stents and PES in the real world clinical practice. 24 In this registry, the incidence of MACE at 12 months in patients presenting with acute MI before the index PCI was ~7% in TITANOX group and ~15% in PES group. We estimated that a total of 200 patients would be required in each group to provide 80% power at the 5% level of significance to detect this difference of 8% in primary end point between the study groups. All analyses were done on the basis of intention-to-treat principle, i.e., the analyses were based on all patients, as randomised. Continuous variables are presented as means (SD) and study groups were compared by Student s unpaired test. Categorical variables are presented as counts and percentages and were compared by the chi square or Fisher s exact test. In order to identify the independent predictors for primary end point, TLR, and ST during the 12 months follow-up, first univariate logistic regression for each baseline clinical characteristics and procedural variables was applied. At the second stage, the variables significantly (P<0.05) associated with dependent variables in univariate analyses were included in multivariable analyses. A two-sided P value <0.05 was required for statistical significance. The rate of survival free from primary end point during the 12 months follow-up period were estimated with the Kaplan-Meier method. The 95% confidence interval (CI) for the relative risk was calculated with the use of standard errors from the Kaplan-Meier curve. The significance of differences between treatment groups was assessed by the log-rank test. All data were analysed with the use of SPSS version The authors had full access to the data and take responsibility for its integrity. All authors have read and agreed to the manuscript as written. Results Baseline and procedural characteristics Between December 2005 and November 2006, a total of 425 patients were randomised to the two treatment groups (214 to the TITANOX group and 211 to the PES group). Baseline characteristics were comparable between the study groups, except by a higher incidence of previous PCI s in the TITANOX group (Table 1). The baseline angiographic variables and procedural characteristics are presented in Table 2. Procedural success was achieved in 99.5% of patients in the TITANOX group and in 98.1% in the PES group. The mean peak value of the creatine kinase MB isoenzyme (64±101 µg/l in TITANOX group vs. 71±117 µg/l in PES group, P=0.5) and troponin I (35±77 µg/l vs. 27±59 µg/l, respectively, P=0.3) were similar in both study groups. Clinical outcome At 30 days (Table 3), the incidence of recurrent MI was lower in the TITANOX group than in the PES group (P=0.03). ST occurred in one patient (0.5%) in the TITANOX group and in 5 (2.4%) patients in the PES group (P=0.10). At 12 months, complete follow-up was Table 1. Baseline clinical characteristics. TITANOX PES P (n=214) (n=211) Value Age (yrs) 64±11 64± Male sex 162 (76) 157 (74) 0.8 Risk factors Family history of CAD 103 (48) 95 (45) 0.6 Diabetes 48 (22) 33 (16) 0.08 Hypertension 122 (57) 106 (50) 0.2 Hypercholesterolaemia 141 (66) 151 (72) 0.2 History of smoking 113 (53) 97 (46) 0.2 Medical history Myocardial infarction 33 (15) 20 (9) 0.08 PCI 22 (10) 10 (5) 0.04 CABG 16 (7) 13 (6) 0.7 Stroke 6 (3) 9 (4) 0.4 Renal disease 3 (1) 3 (1) 1.0 Medication Thrombolysis 26 (12)* 40 (19)# 0.06 GP IIb/IIIa inhibitors 116 (54) 96 (45) 0.08 Indication for PCI NSTEMI 131 (61) 114 (54) 0.1 STEMI 83 (39) 97 (46) 0.1 Data are number (%) or mean (±standard deviation). TITANOX: titaniumnitride-oxide-coated stent; PES: paclitaxel-eluting stent; CAD: coronary artery disease; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; GP: glycoprotein; NSTEMI: non-st-elevation myocardial infarction; STEMI: ST-elevation myocardial infarction * Seven patients had rescue PCI, and in 19 patients PCI was done >24 hours after administration of fibrinolytics. # Eleven patients had rescue PCI, and in 29 patients PCI was done >24 hours after administration of fibrinolytics
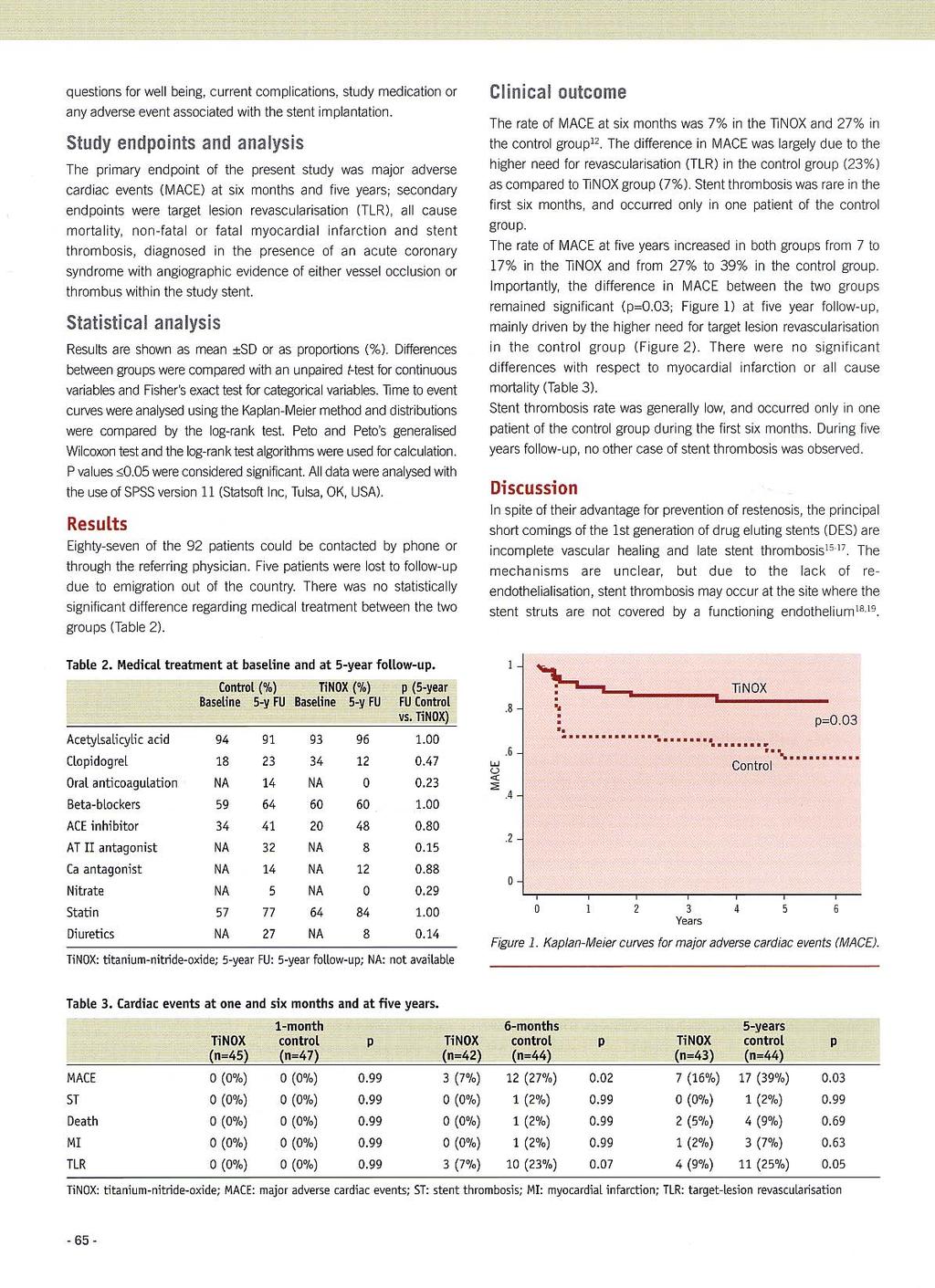
15 TITAX AMI trial 12-month follow-up Table 2. Baseline angiographic variables and procedural characteristics. TITANOX PES P (n=214) (n=211) Value Coronary Disease 1 Vessel 115 (54) 126 (60) Vessels 74 (35) 65 (31) Vessels 25 (12) 20 (9) 0.5 Infarct-Related Vessel Left anterior descending artery 98 (46) 91 (43) 0.6 Left circumflex artery 44 (21) 50 (24) 0.5 Right coronary artery 62 (29) 60 (28) 0.9 Left main stem 0 (0) 1 (0.5) 0.5 Saphenous-vein graft 10 (5) 9 (4) 0.8 Lesion Characteristics Bifurcated lesion 53 (25) 50 (24) 0.8 Reference diameter, (mm) 3.16± ± Lesion length, (mm) 13.6± ± TIMI flow grade 0 46 (21) 45 (21) (5) 14 (7) (29) 38 (18) (45) 114 (54) 0.08 Procedural characteristics Direct stenting 26 (12) 32 (15) 0.5 Post-dilatation 89 (42) 73 (35) 0.2 Nominal stent size, (mm) 3.16± ± Stent length, (mm) 17.4± ± Total stent length, (mm) 18.5± ± No. of stents implanted per culprit lesion 1.1± ± Final TIMI flow grade (98.6) 204 (96.7) 0.2 Acute procedural success 213 (99.5) 207 (98.1) 0.2 Multivessel PCI 30 (14) 19 (9) 0.1 Maximum creatine kinase MB*, (µg /litre) 63.8± ± Maximum troponin I#, (µg /litre) 34.7± ± Maximum troponin T, (µg /litre) 5.1± ± Data are number (%) or mean (±standard deviation). TITANOX: titaniumnitride-oxide-coated stent; PES: paclitaxel-eluting stent; TIMI: thrombolysis in myocardial infarction; PCI: percutaneous coronary intervention. *Available in 145 patients in TITANOX group and in 141 patients in PES group. #Available in 140 patients in TITANOX group and in 145 patients in PES group. Available in 72 patients in TITANOX group and in 61 patients in PES group. obtained from all patients in both study groups (Table 3). The cumulative incidence of primary endpoint was 10.3% in the TITANOX group and 12.8% in the PES group (relative risk 1.28, 95% CI , P=0.5, Figure 1). A total of 20 patients (9.3%) in the TITANOX group and 15 patients (7.1%) in PES group underwent TLR (P=0.5). Clinical in-stent restenosis requiring repeat intervention occurred in 18 patients (8.4%) in the TITANOX group and in nine patients (4.3%) in the PES group (relative risk 0.49, 95% CI , P=0.1). During 12 months follow-up, the incidence of ST according to the study protocol was 0.5% in the TITANOX group and 3.3 % in the PES group (P=0.03). When using Event-free survival (%) p=0.5 TITANOX 89.7% 87.2% PES No. at risk Days after index procedure TITANOX PES Figure 1. Kaplan-Meier curve of event-free survival in patients randomised to titanium-nitride-oxide-coated stent (TITANOX) vs paclitaxel-eluting stent (PES). P=0.5 by the log-rank test. Table 3. Clinical follow-up at 30 days and 12 months. TITANOX PES P (n=214) (n=211) Value Follow-up at 30 days Primary endpoint 3 (1.4) 12 (5.7) Target lesion revascularisation 3 (1.4) 6 (2.8) 0.3 Myocardial infarction* 2 (0.9) 9 (4.3) Death from cardiac causes 0 (0) 2 (0.9) 0.2 Secondary endpoints All cause death 3 (1.4) 3 (1.4) 1.0 Myocardial infarction or cardiac death 2 (0.9) 10 (4.7) Stent thrombosis (per protocol) 1 (0.5) 5 (2.4) 0.1 ARC classification 1 (0.5) 6 (2.8) 0.06 Definite stent thrombosis 1 (0.5) 5 (2.4) 0.1 Probable stent thrombosis 0 (0) 1 (0.5) 0.3 Possible stent thrombosis 0 (0) 0 (0) NS Follow-up at 12 months Primary endpoint 22 (10.3) 27 (12.8) 0.5 Target lesion revascularisation 20 (9.3) 15 (7.1) 0.5 Myocardial infarction 9 (4.2) 17 (8.1) 0.1 Death from cardiac causes 1 (0.5) 4 (1.9) 0.2 Secondary endpoints All cause death 5 (2.3) 6 (2.8)# 0.7 Myocardial infarction or cardiac death 9 (4.2) 18 (8.5) 0.08 Stent thrombosis (per protocol) 1 (0.5) 7 (3.3) ARC classification 2 (0.9) 9 (4.3) Definite stent thrombosis 1 (0.5) 7 (3.3) Probable stent thrombosis 0 (0) 1 (0.5) 0.3 Possible stent thrombosis 1 (0.5) 1 (0.5) 1.0 Data are number (%). TITANOX: titanium-nitride-oxide-coated stent; PES: paclitaxel-eluting stent; ARC: academic research consortium. *One patient in the TITANOX group and seven patients in the PES group suffered ST-elevation myocardial infarction. Target lesion revascularisation was due to clinical in-stent restenosis in 18 patients in the TITANOX group and in nine patients in the PES group. Two patients in the TITANOX group and 9 patients in the PES group suffered ST-elevation myocardial infarction. One patient died of pneumonia, one of pulmonary distress and two patients of cerebrovascular disease. #One patient died of pulmonary embolism, one of metastatic cancer of unknown origin
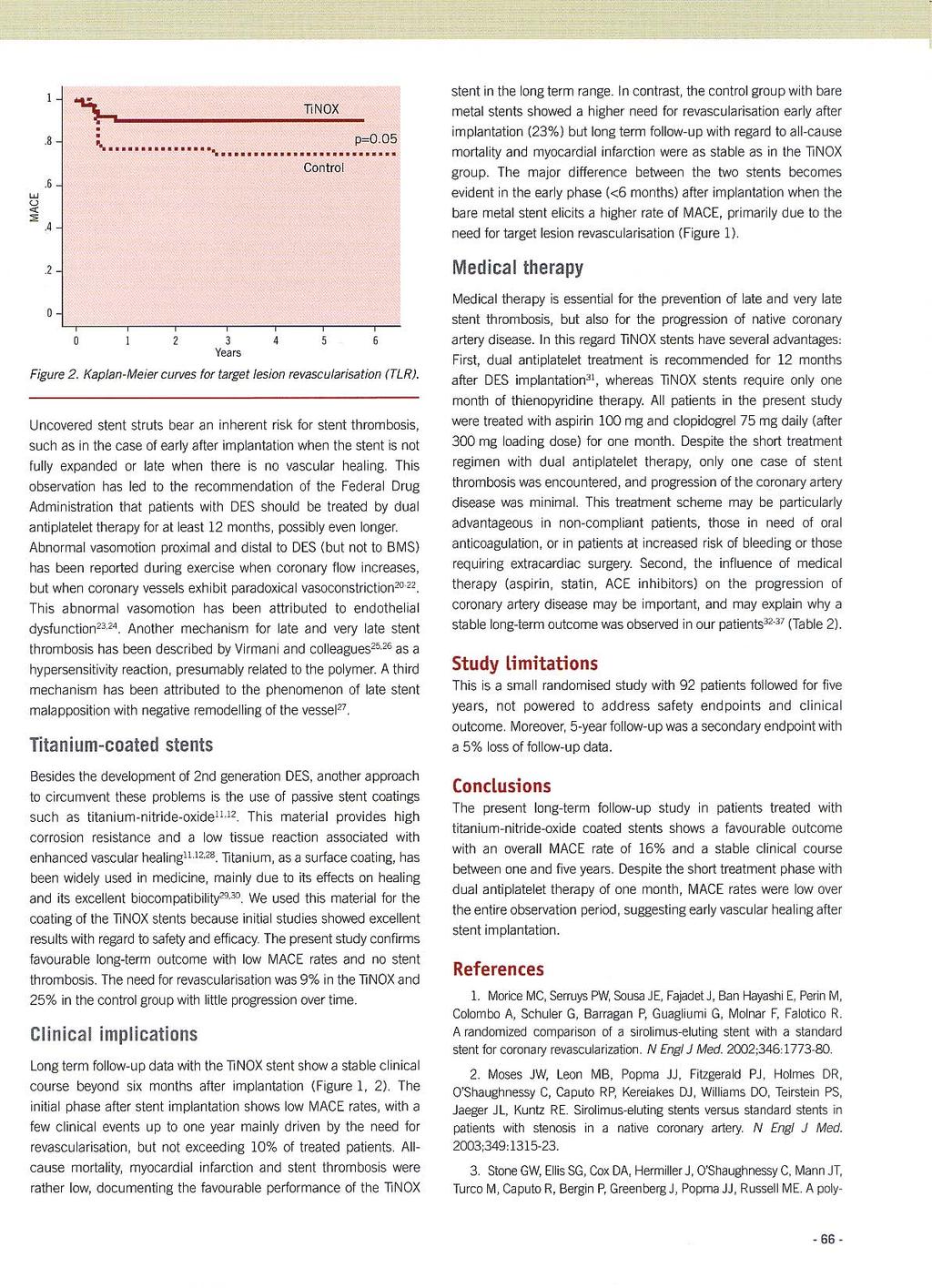
16 Clinical research ARC classification, we observed a lower rate of ST in the TITANOX group (0.9% vs. 4.3%, respectively, P=0.03, Table 3). Characteristics of individual cases of ST are shown in Table 4. In the PES group, ST occurred in 4 (10%) patients who received thrombolysis therapy before index procedure, of which three had subacute ST (range 1-8 days), and one had late ST (day 115). In three patients, clopidogrel was prematurely discontinued before the event of ST, and all of these patients were in the PES group. Four patients out of 11 who suffered ST died. Clopidogrel was prescribed after the discharge for a mean length of 7.6 months in TITANOX group and of 10.0 months in PES group (P<0.001). A total of 67 patients (31%) in TITANOX group and 138 patients (65%) in PES group were receiving dual antiplatelet therapy with aspirin and clopidogrel at the time of the twelve months follow-up (P<0.001). In multivariable analysis, there were no independent predictors for the primary end point, TLR, cardiac death or ST. Recurrent MI was predicted by older age (OR 1.1, CI , P=0.02). Outcomes in patients presenting with NSTEMI or STEMI A total of 245 patients presented with NSTEMI before the index procedure (131 patients in TITANOX group vs. 114 in PES group). These patients were more likely to have diabetes (P=0.001), hypertension (P=0.04) and prior PCI (P=0.04) in their medical history than patients presenting with STEMI. The occurrence of the primary end point (12.2% in NSTEMI patients vs. 10.6% in STEMI patients, P=0.6), MI, cardiac death and TLR were similar in these two subgroups of patients during the 12 months follow-up. Furthermore, the rate of ST was comparable in these two subgroups of patients (2.0% vs. 3.3%, P=0.5, respectively). In addition, patients presenting with NSTEMI and receiving PES were more likely to have recurrent MI during the follow-up (P=0.03, Figure 2). There was a slight but non-significant tendency to increased % % ,1 * 9,6 6 6,2 7,6 12 9,6 # 4,1 0,8 0,9 0 3,1 9,2 Figure 2. Effect of titanium-nitride-oxide-coated stent (TITANOX) and paclitaxel-eluting stent (PES) on subsequent outcome events in patients presenting with NSTEMI or STEMI before the index procedure. At 12 months follow-up, the incidence of myocardial infarction was increased in PES patients presenting with NSTEMI before the index procedure (A). In patients who presented with STEMI, there was a slight but non-significant difference in TLR for PES vs. TITANOX stent (B) ,8 9,3 0,8 MI TLR SCD MACE ST Patients presenting with non ST-elevation MI 1,2 MI TLR SCD MACE ST Patients presenting with ST-elevation MI MI : myocardial infarction; TLR : target lesion revascularisation; SCD : sudden cardiac death; ST : stent thrombosis. * P=0.032 vs. TITANOX group (OR 3.39, 95% CI ). # P=0.055 vs. TITANOX group (OR 0.31, 95% CI ). Titanox (n=131) PES (n=114) 3,5 Titanox (n=83) PES (n=97) 5,2 incidence in TLR in the TITANOX group compared with the PES group in patients who presented with STEMI before the index procedure (P=0.055). Table 4. Characteristics of individual cases of stent thrombosis. Age, Indication CLO* Nominal stent Total stent Thrombo- GP Time, Findings Clinical sex for PCI diameter (mm) length (mm) lysis days and therapy outcome TITANOX 1 82, F STEMI NSTEMI Died 2 66, F NSTEMI STEMI, PCI Alive PES 1 74, M NSTEMI STEMI, PCI Alive 2 54, M NSTEMI STEMI, PCI Alive 3 54, F STEMI STEMI, PCI Alive 4 78, M NSTEMI STEMI, PCI Alive 5 81, F STEMI STEMI Alive 6 59, M STEMI STEMI Alive 7 78, M STEMI STEMI Died 8 65, M STEMI STEMI, PCI Died 9 52, M NSTEMI STEMI Died PCI: percutaneous coronary intervention; CLO: clopidogrel; GP: glycoprotein IIb/IIIa inhibitor; TITANOX: titanium-nitride-oxide-coated stent; PES: paclitaxel-eluting stent; F: female; M: male; NSTEMI: non-st-elevation myocardial infarction; STEMI: ST-elevation myocardial infarction. *Clopidogrel prescription (months)
17 TITAX AMI trial 12-month follow-up Discussion Main study findings To our knowledge, TITAX AMI trial is the first head to head randomised comparison of TITANOX-coated stent and PES among patients with acute MI (NSTEMI or STEMI). The main finding of this trial is that both stent types resulted in comparable incidence of primary end point during 12 months follow-up. Secondly, although the overall rate of ST was fairly low, there was a trend towards a higher rate of ST in PES treated patients. However, in multivariable analyses, no independent predictors for primary endpoint or ST were found. Previous studies A total of six observational studies on DES implantation in acute STEMI patients have been published Four of the studies compared sirolimus-eluting stent (SES) to BMS At six months, the rate of MACE among SES treated patients was ~6-9%. Hofma et al conducted observational comparison of SES and PES implantation for the treatment of acute MI. After 12 months there was no difference between groups in MACE-free survival, 34 but with the use of PES, the incidence of MACE at 12 months was higher than in present study. At present, a total of five randomised trials comparing of DES and BMS in STEMI have been published The STRATEGY trial is a prospective, single-blind and randomised trial with the main purpose of evaluating impact of single high-dose bolus tirofiban plus SES versus abciximab plus BMS in patients with MI. 10 In this small trial (n=175), the rate of MACE was surprisingly high in both stent arms at 12 months follow-up (18% vs. 32%, respectively). Similarly, in MULTISTRATEGY trial in 745 STEMI patients, highdose bolus tirofiban plus SES implantation was associated with a significantly lower risk of MACE (7.8% vs. 14.5%) than abciximab plus BMS within eight months after intervention. 11 In addition, there are two moderately large, randomised trials comparing SES to BMS (TYPHOON and SESAMI) in the clinical setting of acute STEMI. 12,13 In both of these studies, the incidence of MACE was ~7% during 12 months follow-up with the use of SES, which is distinctively lower than observed in present study. However, the main limitation with SESAMI trial was that the primary endpoint was binary restenosis instead of clinical endpoint such as MACE. As for the use of PES, the PASSION trial is the only randomised trial comparing PES and BMS for acute STEMI. 14 PES tended to reduce the incidence of serious adverse cardiac events at one year and the use of PES was associated with a lower rate of MACE (8.8%) than the present study in both stent arms. Recently, four meta-analyses of the clinical trials on the use of DES for treatment of acute STEMI have been published These analyses showed, that the use of DES in patients with acute STEMI is safe and improves clinical outcomes mainly by decreasing the risk of reintervention compared with bare BMS. Stent thrombosis In the present study, the incidence of definite ST was 3.3% in the PES group. This rate is comparable to the previous observational and randomised studies with DES implantation in patients with acute MI (0-3.4%). However, since the sample size is small and patients with thrombolysis therapy were included in this analysis, no valid conclusions can be drawn. The incidence of definite ST in the TITANOX group was low (0.5%), given the thrombotic environment at the time of the stent deployment and the inclusion of patients with thrombolysis therapy in the present trial. It has been suggested that thrombolysis therapy preceding coronary stenting predisposes to ischaemic cardiac complications, such as early reinfarction, ST or urgent target vessel revascularisation. Facilitated regimens with thrombolytic therapy lead to urgent target vessel revascularisation more often compared with primary intervention (4% vs. 1%) and in the ASSENT-4 trial, a strategy of full-dose tenecteplase plus stenting within one to three hours, was associated with a higher incidence of MACE compared with stenting alone strategy in patients presenting with STEMI. 35,36 Study limitations There are various salient differences between the TITAX AMI trial and previous MI trials (TYPHOON/PASSION). The inclusion and exclusion criteria differed considerably. TITAX AMI trial included patients with NSTEMI and STEMI, which are usually considered to be different entities, whereas previous studies included only patients with STEMI. Therefore it may be difficult to compare the present study with the STEMI studies. However, recent reports suggest that the prognosis of NSTEMI and STEMI are similar despite different management strategies. 19,20 Similarly, in the present study, 12 months outcome was comparable in these two subgroups of patients, despite the fact that NSTEMI patients tended to have more co-morbidities. In addition, the TYPHOON and PASSION trials excluded patients who received thrombolysis therapy, whereas the TITAX AMI trial included them. Notably, four patients (10%) with thrombolysis and PES experienced ST. In the present trial, PES was chosen to be a control stent, whereas most previous studies with positive results were performed with SES. The sample size was based on a small real life cohort and the present trial is underpowered to reveal potential small differences in primary and individual end points, although we chose the setting of acute MI known to predispose to clinical complications. In addition, TITAX AMI trial did not reach its primary endpoint, and therefore much larger sample size is needed to demonstrate the non-inferiority of TITANOX stent compared with PES. In the present trial, the randomisation was performed after visualisation of culprit lesion, and this strategy may have had the flaw of possible selection bias by the operator who excludes patients with certain angiographic characteristics, e.g., large thrombus. The design of our study did not include angiographic follow-up or routine non-invasive testing for myocardial ischaemia and therefore we certainly underestimated the incidence of silent or angiographic restenosis. On the other hand, by relying on clinical follow-up only, the chance of unnecessary TLR due to the oculostenotic reflex or patient s unjustified anxiety was avoided. In addition, the stenting was performed in patients with relatively large infarct related arteries with low risk of in-stent restenosis
18 Clinical research Conclusions In conclusion, in patients presenting with acute MI, both TITANOX coated stent and PES resulted in similar clinical outcome at 12 months. The overall risk of ST was low during dual antiplatelet treatment, but there was a non-significant trend towards less ST in the TITANOX group. Clinical trial registration information Clinical trial registration information: URL: Unique identifier: NCT Funding sources: This work (Dr Airaksinen) was supported by grants from the Finnish Foundation for Cardiovascular Research, Helsinki, Finland. Acknowledgements The authors thank Tuija Vasankari, RN, Eija Niemelä, RN, and Marja- Liisa Sutinen, RN, for their support in the conduct of this study. References 1. Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS, Jaeger JL, Kuntz RE. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349: Stone GW, Ellis SG, Cox DA, Hermiller J, O Shaughnessy C, Mann JT, Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME. Oneyear clinical results with the slow-release, polymer-based, paclitaxel-eluting TAXUS stent: the TAXUS-IV trial. Circulation. 2004;109: Grines CL, Cox DA, Stone GW, Garcia E, Mattos LA, Giambartolomei A, Brodie BR, Madonna O, Eijgelshoven M, Lansky AJ, O Neill W, Morice M- C. Coronary angioplasty with or without stent implantation for acute myocardial infarction. N Engl J Med. 1999;341: Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Griffin JJ, Guagliumi G, Stuckey T, Turco M, Carroll JD, Rutherford BD, Lansky AJ. Comparison of angioplasty with stenting, with or without abciximab, in acute myocardial infarction. N Engl J Med. 2002;346: Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361: Silber S, Albertson P, Aviles FF, Camici PG, Colombo A, Hamm C, Jorgensen E, Marco J, Nordrehaug J-E, Ruzyllo W, Urban P, Stone GW, Wijns W. Guidelines for percutaneous coronary interventions. The task force for percutaneous coronary interventions of the European society of cardiology. Eur Heart J. 2005;26: Mehta SR, Cannon CP, Fox KA, Wallentin L, Boden WE, Spacek R, Widimsky P, McCullough PA, Hunt D, Braunwald E, Yusuf S. Routine vs selective invasive strategies in patients with acute coronary syndromes: a collaborative meta-analysis of randomized trials. JAMA. 2005;293: Bhatt DL. To cath or not to cath: that is no longer the question. JAMA. 2005;293: Boersma E and The Primary Coronary Angioplasty vs. Thrombolysis (PCAT)-2 trialist collaborative Group. Does time matter? A pooled analysis of randomized clinical trials comparing primary percutaneous coronary intervention and in-hospital fibrinolysis in acute myocardial infarction patients. Eur Heart J. 2006;27: Valgimigli M, Percoco G, Malagutti P, Campo G, Ferrari F, Barbieri D, Cicchitelli G, McFadden EP, Merlini F, Ansani L, Guardigli G, Bettini A, Parrinello G, Boersma E, Ferrari R. Tirofiban and sirolimus-eluting stents vs abciximab and bare-metal stent for acute myocardial infarction. JAMA. 2005;293: Valgimigli M, Campo G, Percoco G, Bolognese L, Vassanelli C, Colangelo S, de Cesare N, Rodriguez AE, Ferrario M, Moreno M, Piva T, Sheiban I, Pasquetto G, Prati F, Nazzarro MS, Parrinello G, Ferrari R. Comparison of angioplasty with infusion of tirofiban or abciximab and with implantation of sirolimus-eluting or uncoated stents for acute myocardial infarction. JAMA 2008;299: Spaulding C, Henry P, Teiger E, Beatt K, Bramucci E, Carrie D, Slama MS, Merkely B, Erglis A, Margheri M, Varenne O, Cebrian A, Stoll H-P, Snead DB, Bode C. Sirolimus-eluting versus uncoated stents in acute myocardial infarction. N Engl J Med. 2006;355: Menichelli M, Parma A, Pucci E, Fiorilli R, De Felice F, Nazzaro M, Giulivi A, Alborino D, Azzellino A, Violini R. Randomized trial of sirolimuseluting stent versus bare-metal stent in acute myocardial infarction (SESAMI). J Am Coll Cardiol. 2007;49: Laarman GJ, Suttorp MJ, Dirksen MT, van Heerebeek L, Kiemeneij F, Slagboom T, van der Wieken L, Tijssen J, Rensing BJ, Patterson M. Paclitaxel-eluting versus uncoated stents in primary percutaneous coronary intervention. N Engl J Med. 2006;355: Tanimoto S, Tsuchida K, Daemen J, Boersma E. Drug-eluting stent implantation in acute myocardial infarction. Do we need another randomised trial? Eurointerv. 2006;2: Pasceri V, Patti G, Speciale G, Pristipino C, Richichi G, Di Sciascio G. Meta-analysis of clinical trials on use of drug-eluting stents for treatment of acute myocardial infarction. Am Heart J. 2007;153: Moreno R, Spaulding C, Laarman GJ, Tierala I, Kaiser CA, Lopez- Sendon J-L. Effectiveness and safety of paclitaxel-eluting stents in patients with ST-segment elevation acute myocardial infarction. Eurointerv. 2007;3: Kastrati A, Dibra A, Spaulding C, Laarman GJ, Menichelli M, Valgimigli M, Di Lorenzo E, Kaiser C, Tierala I, Mehilli J, Seyfarth M, Varenne O, Dirksen MT, Percoco C, Varricchio A, Pittl U, Syvänne M, Suttorp MJ, Violini R, Schömig A. Meta-analysis of randomized trials on drug-eluting stents vs. bare-metal stents in patients with acute myocardial infarction. Eur Heart J. 2007;28: Terkelsen CJ, Lassen JF, Norgaard BL, Gerdes JC, Jensen T, Gotzsche L, Nielsen TT, Andersen HR. Mortality rates in patients with STelevation vs. non-st-elevation acute myocardial infarction: observations from an unselected cohort. Eur Heart J. 2005;26: Montalescot G, Dallongeville J, van Belle E, Rouanet S, Baulac C, Degrandsart A, Vicaut E. STEMI and NSTEMI: are they so different? 1 year outcomes in acute myocardial infarction as defined by the ESC/ACC definition (the OPERA registry). Eur Heart J. 2007;28: Stone GW, Moses JW, Ellis SG, Schofer J, Dawkins KD, Morice M-C, Colombo A, Schampaert E, Grube E, Kirtane AJ, Cutlip DE, Fahy M, Pocock SJ, Mehran R, Leon MB. Safety and efficacy of sirolimus- and paclitaxel-eluting coronary stents. N Engl J Med. 2007;356: Mauri L, Hsieh W, Massaro JM, Ho K, D Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356: Windecker S, Simon R, Lins M, Klauss V, Eberli FR, Roffi M, Pedrazzini G, Moccetti T, Wenaweser P, Togni M, Tuller D, Zbinden R, Seiler C, Mehilli J, Kastrati A, Meier B, Hess OM. Randomized compari
19 TITAX AMI trial 12-month follow-up son of a titanium-nitride oxide-coated stent with a stainless steel stent for coronary revascularization. The TINOX trial. Circulation. 2005;111: Karjalainen PP, Ylitalo A, Airaksinen KEJ. Titanium and nitride oxide coated stents and paclitaxel eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol. 2006;18: Karjalainen P, Ylitalo A, Airaksinen KEJ. Real World Experience with TITAN(r) Stent: A 9- month Follow-up Report from The Titan PORI Registry. Eurointerv. 2006;2: Mosseri M, Miller H, Tamari I, Plich M, Hasin Y, Brizines M, Frimerman A, Jefary J, Guetta V, Solomon M, Lotan C. The Titanium-NO Stent: results of a multicenter registry. Eurointerv. 2006;2: Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es G-A, Steg PG, Morel M-A, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M, Krucoff MW, Serruys PW. Clinical end points in coronary stent trials. A case for standardized definitions. Circulation. 2007;115: Buehl A, Zoefel P. SPSS 11: Introduction in Modern Data Analysis. 8th ed. Munich, Germany:Addison-Wesley; Saia F, Lemos PA, Lee CH, Arampatzis CA, Hoye A, Degertekin M, Tanabe K, Sianos G, Smits PC, McFadden E, Hofma SH, van der Giessen WJ, de Feyter PJ, van Domburg RT, Serruys PW. Sirolimus-eluting stent implantation in ST-elevation acute myocardial infarction. Circulation. 2003;108: Lemos PA, Saia F, Hofma SJ, Daemen J, Ong A, Arampatzis CA, Hoye A, McFadden E, Sianos G, Smits PC, van der Giessen WJ, de Feyter P, van Domburg RT, Serruys PW. Short- and long-term clinical benefit of sirolimus-eluting stents compared to conventional bare stents for patients with acute myocardial infarction. J Am Coll Cardiol. 2004;43: Weber F, Schneider H, Schwarz C, Holzhausen C, Petzsch M, Nienaber CA. Sirolimus-eluting stents for percutaneous coronary intervention in acute myocardial infarction lesson from a case-controlled comparison of bare metal versus drug-eluting stents in thrombus-laden lesions. Z Kardiol. 2004;93: Cheneau E, Rha SW, Kuchulakanti PK, Stabile E, Kinnaird T, Torguson R, Pichard AD, Satler LF, Kent KM, Waksman R. Impact of sirolimus-eluting stents on outcomes of patients treated for acute myocardial infarction by primary angioplasty. Catheter Cardiovasc Interv. 2005;65: Margheri M, Giglioli C, Comeglio M, Valente S, Chechi T, Falai M, Becherini R, Vittori G, Parigi E, Lazzeri C, Gensini GF. Early outcome after paclitaxel-eluting stents in patients with acute and subacute myocardial infarction. A clinical study. Ital Heart J. 2004;5: Hofma SH, Ong AT, Aoki J, van Mieghem CAG, Rodriguez Granillo GA, Valgimigli M, Regar E, de Jaegere PPT, McFadden EP, Sianos G, van der Giessen WJ, de Feyter PJ, van Domburg RT, Serruys PW. One year clinical follow up of paclitaxel eluting stents for acute myocardial infarction compared with sirolimus eluting stents. Heart. 2005;91: Keeley EC, Boura JA, Grines CL. Comparison of primary and facilitated percutaneous coronary interventions for ST-elevation myocardial infarction: quantitative review of randomised trials. Lancet. 2006;367: Assessment of the safety and efficacy of a new treatment strategy with percutaneous coronary intervention (ASSENT-4 PCI) investigators. Primary versus tenecteplase-facilitated percutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction: randomized trial. Lancet. 2006;367:
20
21
22
23
24
25
26 Interventional Cardiology Randomized Comparison of a Titanium-Nitride-Oxide Coated Stent With a Stainless Steel Stent for Coronary Revascularization The TiNOX Trial Stephan Windecker, MD; Rüdiger Simon, MD; Markus Lins, MD; Volker Klauss, MD; Franz R. Eberli, MD; Marco Roffi, MD; Giovanni Pedrazzini, MD; Tiziano Moccetti, MD; Peter Wenaweser, MD; Mario Togni, MD; David Tüller, MD; Rainer Zbinden, MD; Christian Seiler, MD; Julinda Mehilli, MD; Adnan Kastrati, MD; Bernhard Meier, MD; Otto M. Hess, MD Background Stent coating with titanium-nitride-oxide has been shown to reduce neointimal hyperplasia in the porcine restenosis model. We designed a prospective, randomized, clinical study to investigate the safety and efficacy of titanium-nitride-oxide coated stents compared with stainless steel stents. Methods and Results Ninety-two patients with de novo lesions were randomly assigned to treatment with titaniumnitride-oxide coated stents (n 45) or stainless steel stents of otherwise identical design (n 47; control). Baseline characteristics were similar in both groups. At 30 days, no stent thromboses or other adverse events had occurred in either group. Quantitative coronary angiography at 6 months revealed lower late loss ( versus mm, P 0.03) and percent diameter stenosis (26 17% versus 36 24%, P 0.04) in lesions treated with titanium-nitride oxide coated than in control stents. Binary restenosis was reduced from 33% in the control group to 15% in the titanium-nitride oxide coated stent group (P 0.07). Intravascular ultrasound studies at 6 months showed smaller neointimal volume in titanium-nitride-oxide coated stents than in control stents (18 21 versus mm 3, P ). Major adverse cardiac events at 6 months were less frequent in titanium-nitride-oxide coated stents than in control stent treated patients (7% versus 27%, P 0.02), largely driven by a reduced need for target-lesion revascularization (7% versus 23%, P 0.07). Conclusions Revascularization with titanium-nitride-oxide coated stents is safe and effective in patients with de novo native coronary artery lesions. Titanium-nitride-oxide coated stents reduce restenosis and major adverse cardiac events compared with stainless steel stents of otherwise identical design. (Circulation. 2005;111:-.) Key Words: stents restenosis revascularization Restenosis has been the principal limitation of percutaneous coronary interventions, associated with an increased need for repeat revascularization and thus considerable healthcare cost. 1 3 Although bare-metal stents eliminate constrictive arterial remodeling and elastic recoil, neointimal hyperplasia typically exceeds that seen after balloon angioplasty alone, resulting in in-stent restenosis in approximately 20% to 30% of patients. 4,5 Modifications in stent geometry, 6 strut thickness, 7 and surface material 8 have been shown to influence the restenosis rate after bare-metal stent implantation. Stent coating has been used to reduce restenosis, but the use of some materials, ie, gold, 9 11 has unexpectedly been shown to be associated with an increase in both late loss and need for repeat revascularization compared with stainless steel. A potential mechanism for this observation was found in experimental data, which revealed increased inflammatory reactions in gold-coated as opposed to stainless steel stents. More recently, patients with nickel allergy have been reported to be at increased risk for restenosis after stent implantation. 12 Nickel constitutes an important component of stainless steel, which again suggests that stent material plays an important role in the vascular repair mechanisms after stent-mediated arterial injury. Titanium, a material frequently used for biomedical implants, features superior biocompatibility compared with stainless steel, gold, or other surface coatings. 13,14 As a nitride-oxide alloy, titanium can be easily deployed by Received June 22, 2004; revision received November 3, 2004; accepted February 15, From University Hospital Bern (S.W., P.W., M.T., D.T., R.Z., C.S., B.M., O.M.H.), University Hospital Zurich (F.R.E., M.R.), and Cardiocentro Lugano (G.P., T.M.), Switzerland; and University Hospital Munich (Innenstadt) (V.K.), University Hospital Kiel (R.S., M.L.), and German Heart Center and Technical University (J.M., A.K.), Munich, Germany. Correspondence to Stephan Windecker, MD, Director, Invasive Cardiology, Department of Cardiology, University Hospital Bern, 3010 Bern, Switzerland. stephan.windecker@insel.ch 2005 American Heart Association, Inc. Circulation is available at DOI: /CIRCULATIONAHA
27 2 Circulation May 24, 2005 physical vapor deposition on the surface of stainless steel stents. In vitro examinations of titanium-nitride-oxide showed diminished platelet adhesion and fibrinogen binding compared with stainless steel. In addition, neointimal hyperplasia was reduced by 50% for titanium-nitride-oxide coated compared with stainless steel stents in the porcine restenosis model at 6 week follow-up. 15 To further explore the potential of titanium-nitride-oxide for stent coating, we performed a prospective randomized trial comparing safety and efficacy of titanium-nitride-oxide coated stents with stainless steel stents of otherwise identical design for revascularization of patients with de novo native coronary artery lesions. Methods Patient Population Patients who were at least 18 years of age with stable or unstable angina pectoris or signs of myocardial ischemia were eligible for the study. De novo lesions in native coronary arteries with a lesion length 15 mm, a reference vessel diameter of 2.5 to 3.5 mm, and a diameter stenosis of at least 50% by visual estimate suitable for percutaneous coronary intervention were treated. No more than 2 target lesions were treated in a single patient, and the second lesion had to be located in another major epicardial coronary artery. Exclusion criteria included acute myocardial infarction; severe heart failure; cardiogenic shock; restenotic lesions; a target lesion of the left main or in a vessel with thrombus, or severe calcification; severe comorbidities with a life expectancy of 1 year; lack of informed consent; or unwillingness to undergo coronary angiography during follow-up. The study was conducted according to the declaration of Helsinki and was approved by the institutional review boards of all participating institutions. Written informed consent was obtained from all patients. The study was a prospective, single-blind, randomized, multicenter trial performed in 5 centers in Switzerland (n 3) and Germany (n 2). Patients were randomly assigned to receive either a titanium-nitride-oxide coated stent or an uncoated, stainless steel stent of otherwise identical design. Randomization was performed by means of sealed envelopes supplied to each participating center from the study coordinating center. The stents were visually distinguishable through the dark-surface appearance of the titanium-nitrideoxide coated stents, which left the patient but not the implanting physician unaware of which stent would be implanted. Stent Coating With Titanium-Nitride-Oxide A commercially available stainless steel stent with a tubular slotted design (OMEGA, Qualimed Inc) was used in this study. Unmodified stainless steel stents served as controls. Coating of stainless steel stents was performed by physical vapor deposition of titanium in a prespecified gas mixture of nitrogen and oxygen in a vacuum chamber. Titanium-nitride-oxide coated stents were then immersed in an albumin solution to prevent oxidation of the surface coating and sterilized. Titanium-nitride-oxide coated stents and uncoated control stents were shipped to the participating sites and stored at room temperature. Stent Implantation Procedure All patients were pretreated with aspirin (100 mg daily) and received intravenous heparin (100 IU/kg) during the procedure. Oral clopidogrel was administered as a loading dose of 300 mg before or immediately after the procedure and was continued at a daily dose of 75 mg for 1 month. The use of glycoprotein IIb/IIIa antagonists was left to the discretion of the operator. The stent implantation procedure was standardized according to the following guidelines: (1) predilation of the lesion with a standard balloon dilation catheter was mandatory in all patients, with a target balloon-to-artery ratio of 1:1. (2) Stent length (10, 14, or 17 mm) was chosen to cover the entire lesion with a single stent. (3) Stents were manually crimped on a balloon dilation catheter. (4) Stents were then advanced into the predilated lesion and expanded by adjusting the balloon inflation pressure to achieve an angiographic appearance of the expanded stents that was slightly larger than the reference vessel segment. (5) More than 1 stent could be implanted into the lesion in case of incomplete lesion coverage, edge dissection, or otherwise suboptimal result. Quantitative Coronary Angiography Coronary angiograms were analyzed by the angiographic core laboratory at the German Heart Center, Technical University, Munich, Germany. Angiograms were viewed offline with the automated edge-detection system CMS (Medis Medical Imaging System). The operators performing the quantitative coronary analysis were unaware of the treatment allocation. The contrast-filled, nontapered tip of the guiding catheter was used as a scaling device to obtain absolute dimensions. The same views and calibration techniques were used during follow-up examinations. Measurements of the target lesion at baseline, immediately after stent implantation, and at 6-month angiographic follow-up were obtained in at least 2 orthogonal views after intracoronary administration of 0.1 to 0.2 mg of nitroglycerin. The analyzed segment comprised the stent segment and the proximal and distal stent edges, defined as 5 mm proximal or distal to the stent. End-diastolic frames showing maximal severity of stenosis were chosen for measurements of minimal luminal diameter and percent diameter stenosis. Late loss in luminal diameter was defined as the difference in minimal luminal diameter immediately after stent implantation and that measured at follow-up. Binary restenosis was defined as stenosis of 50% at follow-up examination. Quantitative Intravascular Ultrasound At follow-up, stented vessel segments were examined in a subgroup of 56 patients at 2 study sites with intravascular ultrasonography (In Vision Plus, Imaging System, Volcano Therapeutics Inc) with an automated pullback device at 0.5 mm/s. Data were stored on CD-ROM. Quantitative analysis was performed offline by an experienced investigator who was unaware of the study group and who used a dedicated software package (TapeMeasure, INDEC Systems Inc). The cross-sectional area of lumen and stent was manually traced in steps of 2 mm in the stented segment. Total stent and lumen volume were calculated as V n i 1 A i H, where V is volume, A is total stent or lumen area in a given cross-sectional image, H is thickness of the coronary artery slice, and n is the number of slices. Neointimal hyperplasia was calculated as stent volume minus lumen volume. Study End Points and Analysis An independent clinical research organization (IMECO AG, Zurich, Switzerland) verified all data on case record forms. Patients were evaluated by telephone interview at 30 days and clinical evaluation with an ECG and repeat coronary angiography at 6 months. The primary end point of the study was in-stent luminal late loss as assessed by quantitative coronary angiography. Secondary end points were device success, binary restenosis and minimal luminal diameter of the stented segment at 6 months, neointimal volume as assessed by intravascular ultrasound at 6 months, and a composite of major adverse cardiac events at 30 days and 6 months after the index procedure. Device success was defined as successful implantation of the assigned study stent into the target lesion with a residual stenosis 20% and TIMI 3 flow at the termination of the procedure. Major adverse cardiac events were a composite of death, Q-wave or non Q-wave myocardial infarction, clinically driven revascularization of the target lesion by either CABG surgery or repeat percutaneous coronary intervention, and stent thrombosis. A non Q-wave myocardial infarction was defined by ischemic chest pain with an increase in the creatine kinase (CK) level to more than twice the upper limit of normal, accompanied by an increased level of CK-MB or troponin, and the absence of new Q waves on the ECG. Q-wave myocardial infarction was defined as the development of new Q
28 Windecker et al TiNOX Stent Coating 3 TABLE 1. Clinical Characteristics TABLE 2. Lesion Characteristics TiNOX (n 45) Control (n 47) P Age, y Male gender, n (%) 34 (76) 32 (68) 0.49 Previous myocardial infarction, n (%) 19 (42) 18 (38) 0.80 Cardiovascular risk factors, n (%) Smoking 16 (36) 21 (45) 0.40 Diabetes mellitus 15 (34) 16 (34) 0.99 Family history of CAD 17 (39) 15 (32) 0.66 Systemic hypertension 33 (73) 34 (72) 0.99 Hypercholesterolemia 38 (84) 32 (68) 0.05 Medical treatment, n (%) Acetylsalicylic acid 42 (93) 44 (94) Blockers 27 (60) 26 (59) 0.68 ACE inhibitor 9 (20) 16 (34) 0.16 Lipid-lowering agents 29 (64) 27 (57) 0.53 Clopidogrel 15 (34) 18 (38) 0.67 TiNOX indicates titanium-nitride-oxide; CAD, coronary artery disease. waves in at least 2 contiguous leads, accompanied by a significant increase in CK and CK-MB levels. Target-lesion revascularization was considered to be clinically driven if the stenosis of the target lesion was at least 50%, with ischemic symptoms or a functional study that indicated ischemia, or in the absence of symptoms, if the stenosis was at least 70%. Stent thrombosis was diagnosed in the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent. Results are shown as mean SD or as proportions (%). Differences between groups were compared with an unpaired t test for continuous variables and Fisher exact test for categorical variables. Statistical significance was assumed with a probability value All data were analyzed with the use of SPSS version The sample size of the study was based on the hypothesis that late loss by quantitative coronary angiography would be decreased by 0.4 mm with a common SD of 0.5 mm for the titanium-nitride-oxide coated stent compared with the control stent. Detection of this difference with 80% power and a 2-sided -error of 5% would require a sample size of 41 patients per study group. We assumed 90% adherence to the 6-month angiographic follow-up, and thus the sample size was increased to 90 patients. A total of 92 patients were included in the study, and no patient was excluded from the analysis. All patients were solicited to undergo a control angiogram at 6 months, and 82 (89%) ultimately underwent angiographic follow-up. There were no significant differences with respect to age, number of treated lesions, and type of implanted stents between patients undergoing and those refusing angiography at 6 months. Clinical follow-up was complete in 91 patients (100%) at 1 month, and 6 patients (6.6%) were lost to follow-up at 6 months. Results Clinical characteristics were well balanced between the 2 groups and were notable for a high prevalence of diabetes (33%; Table 1). A total of 96 native coronary artery lesions were treated, with angiographic characteristics summarized in Table 2. There was no difference with regard to the treated target vessel between the 2 groups; however, there was a lower prevalence of type A lesions (9% versus 31%, P 0.03) in the titanium-nitride-oxide group compared with the control group (Table 2). Device success after predilation of the lesion TiNOX Control P No. of lesions Target vessel, n (%) 0.10 LAD 25 (53) 15 (30) RCA 12 (26) 20 (41) LCx 10 (22) 14 (29) ACC/AHA class, n (%) 0.03 Type A 4 (9) 15 (31) Type B1 18 (39) 10 (20) Type B2 22 (48) 21 (43) Type C 3 (7) 3 (6) TiNOX indicates titanium-nitride-oxide; LAD, left anterior descending coronary artery; LCx, left circumflex coronary artery; RCA, right coronary artery; and ACC/AHA, American College of Cardiology/American Heart Association. was 46 (100%) and 49 (100%) in lesions treated with a titanium-nitride-oxide coated and control stent, respectively. There were no differences between groups with respect to lesion length ( versus mm, P 0.90), reference vessel diameter ( versus mm, P 0.45), stent-to-lesion length ( versus , P 0.90), maximal inflation pressure ( versus bar, P 58), and number of implanted stents per lesion ( versus , P 0.33). Quantitative Coronary Angiography Reference vessel diameter, minimal luminal diameter, and percent diameter stenosis were similar for both groups at baseline (Table 3). At 6-month follow-up, the primary end point of late loss was significantly lower in lesions treated with a titaniumnitride-oxide coated stent than in those treated with a control stent ( versus mm, P 0.03). Percent diameter stenosis (26 17% versus 36 24%, P 0.04) and binary angiographic restenosis (15% versus 33%, P 0.07) were lower in titanium-nitride-oxide coated stents than in control stents. No edge effect proximal or distal of the stent was observed in either group, and there were no differences in the pattern of restenosis between stent groups (Table 3). The cumulative distribution of percent diameter stenosis for both stent groups is depicted in the Figure. Intravascular Ultrasound There were no differences in stent volume between groups. Lumen volume ( versus mm 3, P 0.01) was significantly larger and neointimal volume (18 21 versus mm 3, P ) significantly smaller in titaniumnitride-oxide coated stents than in control stents (Table 4). Clinical Follow-Up Clinical events during 6-month follow-up are shown in Table 5. At 30 days, no adverse events and no stent thrombosis had occurred. At 6 month follow-up, a significantly higher incidence of major adverse cardiac events was found in patients assigned to control compared with titanium-nitride-oxide coated stents (27% versus 7%, P 0.02). This difference was largely driven by the more frequent need for target lesion
29 4 Circulation May 24, 2005 TABLE 3. Quantitative Coronary Angiography Data TABLE 4. Follow-Up Intravascular Ultrasonography Data TiNOX Control P No. of lesions Lesion length, mm Reference vessel diameter, mm Before procedure Minimal lumen diameter, mm Diameter stenosis, % After procedure Minimal lumen diameter, mm Diameter stenosis, % Follow-up No. of patients No. of lesions Minimal lumen diameter, mm Proximal edge In-stent Distal edge Diameter stenosis, % Late loss, mm Binary ( 50%) restenosis, n (%) 6 (15) 14 (33) 0.07 Pattern of restenosis, n 0.73 Focal 2 5 Diffuse 4 9 Proliferative or total occlusion 0 0 TiNOX indicates titanium-nitride-oxide. revascularization in control compared with titanium-nitrideoxide coated stents (23% versus 7%, P 0.07). Cumulative distribution curve for percent diameter stenosis stratified according to stent type. TiNOX indicates titanium-nitride-oxide. TiNOX Control P No. of patients No. of lesions Stent volume, mm Lumen volume, mm Neointimal volume, mm TiNOX indicates titanium-nitride-oxide. Discussion Stent coating with titanium-nitride-oxide reduced angiographic and ultrasonic measures of restenosis compared with stainless steel control stents of otherwise identical design in this prospective, randomized, multicenter trial. The favorable effect on restenosis was associated with fewer major adverse cardiac events at 6 months, mainly driven by a reduced need for target-lesion revascularization. At the same time, titanium-nitride-oxide coated stents demonstrated an excellent safety profile comparable to that of uncoated control stents. Of note, these beneficial results were achieved in a population with a relatively high cardiovascular risk profile. The prevalence of diabetes (34%), the most important clinical risk factor for restenosis, was similar to that reported in the SIRIUS (Sirolimus-coated Bx Velocity balloon-expandable stent in the treatment of patients with de novo coronary artery lesions) and TAXUS-IV (Treatment of de novo coronary disease using a single paclitaxel eluting Stent) trials. 17,18 The binary restenosis rate of 33% for the control group was similar to the 35% reported for the bare-metal BX Velocity stent in the SIRIUS trial. These stents have a relatively unfavorable stent design, with a strut thickness of 140 m. 19 In contrast, the 15% binary restenosis rate for titaniumnitride-oxide coated stents represents a 55% reduction compared with the control group. Late loss, a more appropriate measure of neointimal hyperplasia, was reduced by 39% from mm in the control group to mm in the titanium-nitride-oxide group, and neointimal volume was reduced from to mm 3 (63% reduction). To the best of our knowledge, this constitutes the first study reporting reduced restenosis attributable to a novel stent-surface material in humans. 8 TABLE 5. Major Adverse Cardiac Events During 6 Months of Follow-Up TiNOX Control P 1-Month MACE No. of patients Overall, n (%) 0 (0) 0 (0) 0.99 Stent thrombosis, n (%) 0 (0) 0 (0) Month MACE No. of patients Overall, n (%) 3 (7) 12 (27) 0.02 Death 0 (0) 1 (2) 0.99 Myocardial infarction 0 (0) 1 (2) 0.99 Q-wave 0 (0) 1 (2) 0.99 Non Q-wave 0 (0) 0 (0) 0.99 TLR 3 (7) 10 (23) 0.07 PCI 2 (5) 10 (23) 0.03 CABG 1 (2) 0 (0) 0.99 Stent thrombosis 0 (0) 1 (2) 0.99 TiNOX indicates titanium-nitride-oxide; MACE, major adverse cardiac events; TLR, target-lesion revascularization; and PCI, percutaneous coronary intervention.
30 Windecker et al TiNOX Stent Coating 5 Impact of Stent Material on Restenosis Modifications of stent surface and material properties have important implications for neointimal hyperplasia after stent implantation. Stainless steel constitutes the principal material in 85% of commercially available stents. The advantages of stainless steel are its excellent hoop strength, ease of processing, and low cost; however, limited visibility at the time of stent implantation and the relatively high restenosis rate fostered an interest in alternative stent materials. Furthermore, patients with nickel allergy have been found to be at increased risk for restenosis after stent implantation. Koster and colleagues 12 reported a greater need for target-lesion revascularization (100%) in patients with positive patch-test reactions to nickel than in those without nickel allergy (69%). Because inflammatory reactions at the vascular injury site have been associated with the severity of neointimal hyperplasia in experimental restenosis models, it has been hypothesized that patients with nickel allergy may have more pronounced local inflammation and thus neointimal hyperplasia. Gold has been investigated intensively as a potential stent-surface material because of its noble material properties, its high metal density (which translates into improved radiopacity during stent implantation), and its excellent malleability; however, Kastrati and colleagues 9 reported increased binary restenosis and target-lesion revascularization in a randomized, clinical trial comparing gold-coated with stainless steel stents of identical design. These findings have been corroborated in 2 other randomized trials with gold-coated stents, which revealed increased restenosis and greater need for target-lesion revascularization. 10,11 More recently, an experimental study confirmed exaggerated neointimal hyperplasia with gold-coated stents than with stainless steel stents in the porcine restenosis model. 20 The likely mechanism was increased inflammatory cell recruitment and incomplete healing induced by gold-coated stents. These data demonstrate the importance of surface modifications for restenosis after stent implantation. Titanium has been widely accepted as the material of choice for biomedical implants, namely, orthopedic and dental prostheses, because of its superior biocompatibility and high corrosion resistance. 13,14,21 Although solid titanium might be used for manufacturing, the metal processing proves difficult, and manufacturing costs are prohibitive. In contrast, titanium alloys such as titanium-nitride-oxide can be used more easily and applied to stainless steel surfaces by physical vapor deposition. The thin layer of titanium-nitride-oxide proves durable even after stent expansion and can be realized at reasonable cost. Initial in vitro examinations of titaniumnitride-oxide coated surfaces revealed reduced platelet and fibrinogen binding compared with stainless steel. More importantly, neointimal hyperplasia was reduced by 50% in the porcine restenosis model at 6 weeks compared with stainless steel stents of otherwise identical design. 15 The magnitude of reduction in neointimal hyperplasia observed with titaniumnitride-oxide coated stents in the experimental setting was comparable to those reported by Suzuki et al 22 for sirolimuseluting stents in pigs. The present clinical study confirms the beneficial effect of titanium-nitride-oxide coated stents in patients with de novo native coronary artery lesions. Titanium-Nitride-Oxide Coated Stents in the Era of Drug-Eluting Stents A pressing question concerns the potential role of titaniumnitride-oxide coated stents in the new era of drug-eluting stents. Both sirolimus-eluting stents 17 and paclitaxel-eluting stents 18 have recently demonstrated dramatic reductions in binary restenosis (sirolimus 8.9%, paclitaxel 7.9%) and late loss (sirolimus 0.24 mm versus paclitaxel 0.39 mm) compared with stainless steel stents over a wide range of lesions and patients. The binary restenosis rate of 15% and the mean late loss of 0.55 mm for titanium-nitride-oxide coated stents are favorable but clearly not sufficient to supplant drugeluting stents. Notwithstanding, the following strategies will help to define the utility of titanium-nitride-oxide coated stents in future investigations. First, the combination of titaniumnitride-oxide stent coating with a modified stent design, notably a thin strut construction, may allow for further reduction in restenosis. Clinical studies comparing thick versus thin strut stent designs revealed reduced restenosis and target-lesion revascularization. 7,19 Therefore, it is of interest whether thin struts in conjunction with titanium-nitride-oxide stent coating are able to reduce late loss in an additive fashion. Optimization of stent design for restenosis reduction could become an economically attractive alternative to drugeluting stents. Second, coronary artery stenoses at low risk for restenosis, ie, short lesions with a reference vessel diameter 3.0 mm, 23 may be more cost-effectively treated with a titanium-nitrideoxide coated stent. The rate of target-lesion revascularization in short lesions with large diameter was 5% for titaniumnitride-oxide coated stents in the present study compared with 4% for sirolimus-eluting stents in the SIRIUS trial. Third, stent thrombosis may be a particular problem for drug-eluting stents because of their thrombogenic surface. 24 Polymer coatings 25 and drugs in high doses 26 have been reported as potentially prothrombogenic, resulting in local inflammation and enhanced thrombus formation. Study Limitations The findings of the present study have to be interpreted in the context of the following limitations. (1) The present study was designed as a safety and efficacy trial and is therefore too small to qualify as a clinical end-point study. (2) The study included lesions 15 mm in length because of a limitation in the available stent lengths. Investigation in more complex lesions and patients will require further study. (3) The intravascular ultrasound study was performed in only 56 patients at 2 centers because of limited funding; however, given the higher sensitivity of intravascular ultrasound for neointimal volume measurements, fewer patients were required to undergo the procedure. (4) The proportion of patients lost to follow-up is relatively high given the small size of the study population. We attempted to contact all patients by phone, but some patients were inaccessible because of their move to an unknown location. (5) The study
31 6 Circulation May 24, 2005 design was single blind because of the different surface appearance of the titanium-nitride oxide coated stent, which left the patient but not the implanting physician unaware of the allocated treatment. A comparison of titanium-nitrideoxide with drug-eluting stents may help to identify the role of this novel surface coating in the current era of drug-eluting stents. Conclusions Revascularization with titanium-nitride-oxide coated stents is safe and effective in patients with de novo coronary artery lesions. Titanium-nitride-oxide coated stents reduce restenosis and major adverse cardiac events compared with stainless steel stents of otherwise identical design. Acknowledgments This study was supported by an educational grant of the University of Bern and Scolmed Inc, Munich, Germany. References 1. Serruys PW, Luijten HE, Beatt KJ, Geuskens R, de Feyter PJ, van den Brand M, Reiber JH, ten Katen HJ, van Es GA, Hugenholtz PG. Incidence of restenosis after successful coronary angioplasty: a time-related phenomenon: a quantitative angiographic study in 342 consecutive patients at 1, 2, 3, and 4 months. Circulation. 1988;77: Peterson ED, Cowper PA, DeLong ER, Zidar JP, Stack RS, Mark DB. Acute and long-term cost implications of coronary stenting. J Am Coll Cardiol. 1999;33: Al Suwaidi J, Berger PB, Holmes DR Jr. Coronary artery stents. JAMA. 2000;284: Kastrati A, Hall D, Schömig A. Long-term outcome after coronary stenting. Curr Control Trials Cardiovasc Med. 2000;1: Gershlick AH. Role of stenting in coronary revascularization. Heart. 2001;86: Garasic JM, Edelman ER, Squire JC, Seifert P, Williams MS, Rogers C. Stent and artery geometry determine intimal thickening independent of arterial injury. Circulation. 2000;101: Kastrati A, Mehilli J, Dirschinger J, Dotzer F, Schuhlen H, Neumann FJ, Fleckenstein M, Pfafferott C, Seyfarth M, Schömig A. Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation. 2001;103: Babapulle MN, Eisenberg MJ. Coated stents for the prevention of restenosis: part II. Circulation. 2002;106: Kastrati A, Schömig A, Dirschinger J, Mehilli J, von Welser N, Pache J, Schuhlen H, Schilling T, Schmitt C, Neumann FJ. Increased risk of restenosis after placement of gold-coated stents: results of a randomized trial comparing gold-coated with uncoated steel stents in patients with coronary artery disease. Circulation. 2000;101: vom Dahl J, Haager PK, Grube E, Gross M, Beythien C, Kromer EP, Cattelaens N, Hamm CW, Hoffmann R, Reineke T, Klues HG. Effects of gold coating of coronary stents on neointimal proliferation following stent implantation. Am J Cardiol. 2002;89: Park SJ, Lee CW, Hong MK, Kim JJ, Park SW, Tahk SJ, Jang YS, Seung KB, Yang JY, Jeong MH. Comparison of gold-coated NIR stents with uncoated NIR stents in patients with coronary artery disease. Am J Cardiol. 2002;89: Koster R, Vieluf D, Kiehn M, Sommerauer M, Kahler J, Baldus S, Meinertz T, Hamm CW. Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet. 2000;356: Steinemann SG. Titanium: the material of choice? Periodontol ;17: Steinemann SG. Metal implants and surface reactions. Injury. 1996; 27(suppl 3):SC16 SC Windecker S, Mayer I, De Pasquale G, Maier W, Dirsch O, De Groot P, Wu YP, Noll G, Leskosek B, Meier B, Hess OM. Stent coating with titanium-nitride-oxide for reduction of neointimal hyperplasia. Circulation. 2001;104: Buehl A, Zoefel P. SPSS 11: Introduction in Modern Data Analysis. 8th ed. Munich, Germany: Addison-Wesley; Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS, Jaeger JL, Kuntz RE. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003; 349: Stone GW, Ellis SG, Cox DA, Hermiller J, O Shaughnessy C, Mann JT, Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med. 2004;350: Pache J, Kastrati A, Mehilli J, Schuhlen H, Dotzer F, Hausleiter J, Fleckenstein M, Neumann FJ, Sattelberger U, Schmitt C, Muller M, Dirschinger J, Schomig A. Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO-2) trial. J Am Coll Cardiol. 2003;41: Edelman ER, Seifert P, Groothuis A, Morss A, Bornstein D, Rogers C. Gold-coated NIR stents in porcine coronary arteries. Circulation. 2001; 103: Steinemann S, Eulenberger P, Mäusli A, Schröder A. Adhesion of bone to titanium. In: Christel P, Meunier A, Lee A, eds. Biological and Biomechanical Performance of Biomaterials. Amsterdam, Netherlands: Elsevier; 1986: Suzuki T, Kopia G, Hayashi S, Bailey LR, Llanos G, Wilensky R, Klugherz BD, Papandreou G, Narayan P, Leon MB, Yeung AC, Tio F, Tsao PS, Falotico R, Carter AJ. Stent-based delivery of sirolimus reduces neointimal formation in a porcine coronary model. Circulation. 2001; 104: Serruys PW, Kay IP, Disco C, Deshpande NV, de Feyter PJ. Periprocedural quantitative coronary angiography after Palmaz-Schatz stent implantation predicts the restenosis rate at six months: results of a metaanalysis of the BElgian NEtherlands Stent study (BENESTENT) I, BENESTENT II Pilot, BENESTENT II and MUSIC trials: Multicenter Ultrasound Stent In Coronaries. J Am Coll Cardiol. 1999;34: McFadden EP, Stabile E, Regar E, Cheneau E, Ong AT, Kinnaird T, Suddath WO, Weissman NJ, Torguson R, Kent KM, Pichard AD, Satler LF, Waksman R, Serruys PW. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet. 2004;364: Virmani R, Guagliumi G, Farb A, Musumeci G, Grieco N, Motta T, Mihalcsik L, Tespili M, Valsecchi O, Kolodgie FD. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: should we be cautious? Circulation. 2004;109: Walpoth BH, Pavlicek M, Celik B, Nicolaus B, Schaffner T, Althaus U, Hess OM, Carrel T, Morris RE. Prevention of neointimal proliferation by immunosuppression in synthetic vascular grafts. Eur J Cardiothorac Surg. 2001;19:
32 Rev Bras Cardiol Invas. 2009;17(1):xx-xx. Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. Artigo Original Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio-Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO Fernando Mendes Sant Anna 1, Leonardo Alves Batista 1, Marcelo Bastos Brito 1, Sérgio Menezes 1, Fábio Machado Ventura 1, Leonardo Buczynski 1, Carlos Alberto Mussel Barrozo 1 RESUMO Introdução: O stent recoberto por titânio-óxido nítrico (Titan) mostrou-se eficaz para redução da hiperplasia neointimal comparado ao stent convencional em animais e seres humanos. Foi elaborado um estudo clínico prospectivo e randomizado do stent Titan versus stent de aço inoxidável, cujo objetivo foi comparar o índice de eventos cardíacos adversos maiores (ECAM) após dois anos. Método: No período de outubro de 2005 a maio de 2006, 200 pacientes (228 lesões) foram submetidos a implante de stent eletivo e randomizados para dois grupos: I) stent metálico (100) e II) stent Titan (100). O acompanhamento dos doentes foi realizado por consulta clínica. ECAM foram definidos como: morte, infarto agudo do miocárdio ou nova revascularização da lesão-alvo. As sobrevidas livres de ECAM e angina após dois anos foram comparadas entre os dois grupos. Resultados: Foi obtido sucesso em todos os procedimentos. As características clínicas e angiográficas foram similares nos dois grupos. O período médio de seguimento foi de 482 ± 264 dias. Aos 30 dias, o índice de ECAM foi de 2% no grupo I e de 1% no grupo II (P = 0,32). Após dois anos, a sobrevida livre de ECAM foi melhor no grupo Titan que no grupo stent metálico (93,6% vs. 82,4%; P = 0,036), assim como a sobrevida livre de angina (84% vs. 71%; P = 0,02). Conclusões: O implante do stent Titan em pacientes com insuficiência coronariana crônica é seguro e efetivo, e cursa com índices de ECAM e angina após dois anos menores que os do stent de aço inoxidável. DESCRITORES: Contenedores. Stents farmacológicos. Reestenose coronária. ABSTRACT Randomized Comparison of Percutaneous Coronary Intervention with Titanium-Nitride-Oxide- Coated Stents Versus Stainless Steel Stents in Patients with Coronary Artery Disease: RIO Trial Background: Stent coating with titanium-nitride oxide (Titan) has been shown to reduce neointimal hyperplasia in both animals and humans. A prospective, randomized, clinical study was designed to compare the incidence of major adverse cardiac events (MACE) after two years in patients with the Titan stent versus the stainless steel stent. Methods: Two hundred patients (228 stenosis) submitted to stent implantation between October 2005 and May 2006 were randomized into two groups: I) Bare metal stent (100); II) Titan (100) and followed clinically. MACE was defined as a composite of death, acute myocardial infarction or clinically driven revascularization of target lesion. MACE and angina free survival after 2 years were compared between the two groups. Results: All procedures were successful in both groups. Baseline clinical and angiographic characteristics were similar in both groups. Mean followup period was 482 ± 264 days. After 30 days, MACE was 2% in group I and 1% in group II (P = 0.32). MACE free survival at 2 years was significantly better in the Titan group than in the bare metal stent group (93.6% vs. 82.4%, P = 0.036) as well as angina free survival (84% vs. 71%, P = 0.02). Conclusions: Revascularization with Titan stent in chronic coronary artery disease is safe, effective, and reduces the incidence of MACE and angina after two years when compared with the bare metal stent. DESCRIPTORES: Stents. Drug-eluting stents. Coronary restenosis. 1 Hospital Santa Helena Cabo Frio, RJ, Brasil. Correspondência: Fernando Mendes Sant Anna. Rua Safira, 20 Portinho Cabo Frio, RJ, Brasil CEP fmsantanna@bol.com.br Recebido em: 22/2/2009 Aceito em: 20/3/2009 1
33 Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. Areestenose permanece ainda como o calcanhar de Aquiles da angioplastia 1,2. Os stents de aço inoxidável eliminaram o problema do remodelamento arterial e da retração elástica do vaso, mas a hiperplasia neointimal decorrente do implante desse tipo de stent é responsável por índice de reestenose em torno de 30% 3. Os stents farmacológicos diminuíram substancialmente a reestenose 4, porém o custo elevado limita sua utilização a apenas uma pequena parcela dos pacientes atendidos em nosso País. Modificações na geometria do stent 5, na espessura das hastes 6 e na cobertura de sua superfície 7 também têm se mostrado úteis na redução da reestenose intrastent, porém sem atingir resultados satisfatórios. Recentemente, demonstrou-se que pacientes com história de alergia ao níquel apresentavam taxas de reestenose elevadas após implante de stents metálicos 8. O níquel é um componente importante do aço inoxidável, o que sugere que o material de que é feito o stent tem papel importante nos mecanismos de reparo vascular após a injúria arterial provocada pelo implante da prótese. O titânio, um material frequentemente utilizado em próteses biológicas, apresenta biocompatibilidade superior ao ouro, ao aço inoxidável e a outros produtos utilizados na superfície dos stents 9. Ligado ao óxido nítrico, o titânio pode ser facilmente depositado por meio de vaporização na superfície dos stents de aço inoxidável. Estudos in vitro demonstraram que stents recobertos por titânio-óxido nítrico (Titan) apresentavam diminuição da adesão plaquetária e ligação de fibrinogênio, quando comparados aos stents convencionais de aço inoxidável 10. Um estudo em animais demonstrou redução importante da hiperplasia neointimal em porcos que receberam stent recoberto por titânioóxido nítrico em relação ao stent de aço inoxidável, num período de seguimento de 6 semanas 11. Em seres humanos, diversos estudos publicados recentemente demonstraram índices reduzidos de reestenose e eventos cardíacos adversos maiores após seis meses a um ano em pacientes submetidos a implante de stent recoberto por titânio-óxido nítrico (entre 7% e 11%) No único estudo randomizado no qual o stent Titan foi comparado aos stents de aço inoxidável, a redução foi bem mais significativa (7% vs. 27%; P = 0,02) 12. Num estudo prospectivo, observacional, no qual o Titan foi comparado ao stent recoberto por paclitaxel, o índice de eventos cardíacos adversos maiores após um ano foi semelhante nos dois grupos (10,9% vs. 13,7%; P = 0,40) 15. O objetivo do estudo RIO, prospectivo e randomizado, foi comparar, em pacientes submetidos a implante de stent eletivo num período consecutivo de tempo, o índice de eventos cardiovasculares adversos maiores após dois anos em dois grupos de pacientes, um deles recebendo stent recoberto por titânio-óxido nítrico (stent Titan, Hexacath Rueil-Malmaison, França) e o outro, stent convencional de aço inoxidável. MÉTODO A casuística desse estudo constituiu-se de 200 pacientes encaminhados para nosso Serviço, no período de outubro de 2005 a maio de 2006, para angioplastia coronariana eletiva. Os critérios de inclusão foram: 1) presença de sintomas ou sinais objetivos de isquemia miocárdica; e 2) lesão maior que 50% (pela estimativa visual) em artéria coronária principal (direita, circunflexa ou descendente anterior) ou ramo de grande importância. Como critérios de exclusão, foram adotados: 1) infarto agudo do miocárdio; 2) lesão igual ou maior que 50% no tronco da artéria coronária esquerda; 3) história de alergia ou contraindicação ao uso de ácido acetilsalicílico (AAS) ou clopidogrel e/ou ticlopidina; 4) paciente com menos de 21 anos de idade; 5) gravidez; e 6) recusa em assinar o termo de consentimento. É importante mencionar que pacientes com angina instável só foram incluídos no estudo depois de estabilizados clinicamente e tratados eletivamente, conforme conduta adotada em nosso Serviço. O tamanho da amostra de nosso estudo foi determinado partindo-se da seguinte premissa: de acordo com dados da literatura, o índice de eventos cardíacos adversos maiores em pacientes submetidos a implante de stents convencionais de aço inoxidável varia entre 22% e 27% 3,4,12, enquanto em pacientes submetidos a implante de stent recoberto por titânio-óxido nítrico esse índice varia entre 6% e 10% Considerandose a incidência de eventos cardíacos adversos maior que 7% para o grupo Titan e de 25% para o grupo stent convencional, para um poder do teste de 0,8 com nível de significância de 5%, seriam necessários 64 pacientes em cada grupo (total: 128). Para trabalharmos com boa margem de segurança, resolvemos incluir no estudo 200 pacientes. Antes da intervenção, os pacientes foram randomizados, por meio de números sequenciais gerados aleatoriamente por computador (com emprego do software Stata SE), para receber stent metálico de aço inoxidável (grupo stent convencional) ou stent recoberto por titânio-óxido nítrico (grupo Titan). Cada número aleatório correspondia a um grupo. Esses números/ grupos foram colocados dentro de envelopes opacos e foram lacrados (colados), no próprio centro onde se desenvolveu o estudo, por uma secretária que não tinha conhecimento do propósito do estudo. Os envelopes, abertos sequencialmente à medida que os pacientes eram recrutados para o estudo (de forma consecutiva), continham o grupo ao qual o paciente pertenceria. O objetivo primário do estudo era determinar o índice de eventos cardíacos adversos maiores nos dois grupos após dois anos. Como eventos cardíacos adversos maiores definiu-se o composto de morte, infarto 2
34 Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. agudo do miocárdio ou nova revascularização da lesãoalvo. O objetivo secundário foi determinar a quantidade de pacientes livres de angina nesse mesmo período. Definiu-se como infarto agudo do miocárdio a elevação dos níveis de creatina quinase fração MB (CK-MB) após o procedimento maior que 2,5 vezes o valor basal, com ou sem alteração de eletrocardiograma. Como revascularização da lesão-alvo definiu-se necessidade de se realizar nova intervenção percutânea na lesão antes tratada ou encaminhamento do paciente para tratamento cirúrgico em decorrência de reestenose intrastent naquela lesão. O seguimento foi realizado por meio de consulta clínica ou telefone em 30 dias, 6 meses, 1 ano e 2 anos após o procedimento ou sempre que necessário. Esse estudo foi projetado de acordo com as Diretrizes e Normas Regulamentadoras de Pesquisas Envolvendo Seres Humanos (Resolução 196/1996 do Conselho Nacional de Saúde) e foi aprovado pelo Comitê de Ética em Pesquisa do hospital em que foi realizado. Todos os pacientes assinaram um termo de consentimento pós-informado. Intervenção coronária percutânea O implante dos stents nos pacientes do estudo foi realizado por via femoral, utilizando-se cateteres-guia 6 F ou 7 F. Antes da angioplastia, eram administradas UI de heparina endovenosa e 0,5 mg de nitroglicerina intracoronariana. Todos os pacientes faziam uso prévio de AAS e ticlopidina ou clopidogrel iniciados três dias antes do procedimento. Caso o paciente não fizesse esse preparo, era administrada dose de ataque de 300 mg de clopidogrel e 100 mg de AAS antes do procedimento. Após o procedimento, os pacientes eram orientados a manter o AAS indefinidamente e o outro antiagregante por apenas 30 dias. Sempre que possível, foi realizado implante direto do stent. Os stents eram escolhidos de modo a cobrir inteiramente a lesão e mais de um stent era permitido em caso de dissecção de borda, cobertura incompleta da lesão ou resultado subótimo. Os modelos de stent utilizados foram semelhantes, porém não totalmente idênticos. Apesar disso, não existem diferenças significativas na evolução clínica de pacientes tratados pelos tipos de stent utilizados nesse estudo na literatura. Foram eles: Helistent (Hexacath Rueil-Malmaison, França), BX Sonic (Cordis Miami, Estados Unidos), Liberté ou Express (Boston Scientific Natick, Estados Unidos) e Driver (Medtronic Minneapolis, Estados Unidos). Todos esses stents foram utilizados em porcentuais semelhantes no grupo dos stents convencionais. Os critérios de sucesso adotados para os procedimentos foram: grau de estenose do vaso após a intervenção menor que 50% e ausência de complicações maiores (morte ou infarto agudo do miocárdio) nas primeiras 24 horas após o procedimento. Angiografia coronariana quantitativa A angiografia coronariana quantitativa foi realizada off-line, tomando-se a projeção na qual se podia demonstrar a lesão mais grave, utilizando-se software com algoritmo de detecção automática de contorno (CAAS II, Pie Medical Imaging Maastricht, Holanda), conforme descrito previamente 16. Análise estatística Todas as variáveis foram testadas para normalidade pelo teste de Shapiro-Wilks. Na análise descritiva, as variáveis numéricas foram apresentadas como média ± desvio padrão ou medianas e interquartis e as categóricas, como números (n) e porcentagens (%). O teste de qui-quadrado e o teste exato de Fisher foram usados para variáveis categóricas; o teste t de Student não-pareado e o teste de Mann-Whitney foram usados para variáveis contínuas. As características clínicas e angiográficas foram comparadas entre os grupos Titan e stent convencional. As curvas de sobrevida para ausência de eventos cardiovasculares adversos maiores e angina foram construídas pelo método de Kaplan- Meier e comparadas pelo teste de log-rank. A análise estatística foi realizada com os programas Stata SE 10 (Stata Corporation Houston, Estados Unidos) e R Valores de P < 0,05 foram considerados estatisticamente significativos, sendo todos os testes bicaudais. RESULTADOS Durante um período de 8 meses consecutivos, 243 pacientes foram admitidos no Serviço para se submeterem a angioplastia coronariana com implante de stent. Desses pacientes, 23 apresentaram infarto agudo do miocárdio, 5 apresentaram alergia ao AAS ou à ticlopidina, e 15 se recusaram a participar do protocolo do estudo, sem mencionar motivos específicos. Dessa forma, 200 pacientes foram incluídos no estudo. As características clínicas desses pacientes podem ser analisadas na Tabela 1. A maioria dos pacientes apresentava angina estável (59,5%) e doença multiarterial (uniarteriais: 32%; biarteriais: 47,5%; triarteriais: 20,5%). Diabetes estava presente em 24% dos pacientes do grupo stent convencional e em 28% dos pacientes do grupo Titan (P = 0,63). Não houve diferença significativa entre as características clínicas nos dois grupos. As características angiográficas das lesões podem ser observadas na Tabela 2. A maior parte das lesões (58,3%) era do tipo B2/C. Não houve diferença entre os diâmetros de referência ou em relação ao comprimento da lesão entre os grupos stent convencional e Titan (15,5 mm vs. 15,3 mm; P = 0,52). Todos os procedimentos nos dois grupos foram bem-sucedidos. No grupo stent convencional foi implantado 1,2 stent por paciente e no grupo Titan, 1,1. 3
35 Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. TABELA 1 Características clínicas dos pacientes Pacientes Grupos (n = 200) Stent metálico (n = 100) Titan (n = 100) P Idade, anos 61,2 ± 10,1 60,6 ± 10 61,9 ± 10,2 0,34 Sexo feminino, % 35, ,37 Sintomas, n (%) 0,841 Angina estável 119 (59,5) 59 (59) 61 (61) Isquemia silenciosa 44 (22) 24 (24) 20 (20) Angina instável 37 (18,5) 17 (17) 20 (20) Fatores de risco, n (%) Hipertensão arterial 158 (79) 84 (84) 74 (74) 0,12 Dislipidemia 110 (55) 53 (53) 57 (57) 0,67 HF de DAC 80 (40) 38 (38) 42 (42) 0,66 Tabagismo 50 (25) 29 (29) 21 (21) 0,25 Diabetes 52 (26) 24 (24) 28 (28) 0,63 IAM prévio, n (%) 101 (50,5) 51 (51) 50 (50) > 0,99 ICP prévia, n (%) 16 (8) 4 (4) 12 (12) 0,06 RM prévia, n (%) 2 (1) 1 (1) 1 (1) > 0,99 Fração de ejeção, % 59, , , ,94 Doença multiarterial, n (%) 136 (68) 67 (67) 69 (69) 0,88 Variáveis contínuas representadas por média ± desvio padrão. HF de DAC = história familiar de doença arterial coronariana; IAM = infarto agudo do miocárdio; ICP = intervenção coronária percutânea; n = número de pacientes; RM = cirurgia de revascularização do miocárdio. TABELA 2 Características angiográficas: análise por lesão Grupos Lesões (n = 228) Stent convencional (n = 120) Titan (n = 108) P Artéria coronária, n (%) Descendente anterior 133 (58,3) 77 (64,2) 56 (51,8) 0,08 Circunflexa 41 (18) 23 (19,2) 18 (16,7) 0,73 Coronária direita 54 (23,7) 20 (23,2) 34 (28,8) 0,01 ACC/AHA B2/C, n (%) 133 (58,3) 70 (58,3) 63 (58,3) > 0,99 Diâmetro de referência pré-icp, mm 2,81 (2,4; 3,2) 2,84 (2,5; 3,2) 2,76 (2,4; 3,1) 0,15 Diâmetro luminal mínimo pré-icp, mm 0,84 (0,64; 1,04) 0,85 (0,61; 1,07) 0,83 (0,68; 1,04) 0,71 Grau de estenose pré-icp, % 70 (63; 76) 71 (64; 78) 70 (62; 75) 0,20 Comprimento da lesão, mm 15,4 (10,1; 20,6) 15,5 (10,6; 20,8) 15,3 (9,3; 20,1) 0,52 Diâmetro de referência pós-icp, mm 3,1 ± 0,49 3,09 ± 0,51 3,13 ± 0,48 0,52 Diâmetro luminal mínimo pós-icp, mm 2,76 ± 0,48 2,75 ± 0,42 2,76 ± 0,44 0,83 Grau de estenose pós-icp, % 12 (8; 15) 11,5 (8; 15) 12 (9; 15) 0,47 Variáveis contínuas representadas por média ± desvio padrão ou mediana (interquartis). ACC/AHA = American College of Cardiology/ American Heart Association; ICP = intervenção coronária percutânea; n = número de lesões. Seguimento clínico A Tabela 3 demonstra o seguimento clínico aos 30 dias e 2 anos. Ao analisar os eventos após 30 dias, verificou-se trombose subaguda no grupo Titan, que ocorreu 36 horas após o procedimento, tratada com sucesso por meio de angioplastia com balão. Os dois eventos no grupo stent convencional foram infarto agudo do miocárdio não-q, caracterizados pelo aumento dos níveis de CK-MB maiores que 2,5 vezes o valor basal. Ambos os casos foram conduzidos clinicamente. 4
36 Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. TABELA 3 Seguimento clínico Grupos Pacientes Stent metálico Titan P ECAM 1 mês, n (%) Número de pacientes Morte/IAM/RLA 3 (1,5) 2 (2) 1 (1) 0,56 Morte NA IAM 3 (1,5) 2 (2) 1 (1) 0,56 RLA 1 (0,5) 0 1 (1) > 0,99 Trombose subaguda 1 (0,5) 0 1 (1) > 0,99 ECAM 2 anos, n (%) Número de pacientes Morte/IAM/RLA 16 (12,2) 12 (17,6) 4 (6,4) 0,036 IAM/RLA 13 (10) 11 (16,2) 2 (3,2) 0,02 Morte 3 (2,3) 1 (1,5) 2 (3,2) 0,61 IAM 7 (5,3) 6 (8,8) 1 (1,6) 0,12 RLA 7 (5,3) 5 (7,4) 2 (3,2) 0,44 Angina (2 anos), n (%) 30 (23) 20 (29,4) 10 (15,9) 0,02 ECAM = eventos cardíacos adversos maiores; IAM = infarto agudo do miocárdio; n = número de pacientes; RLA = revascularização da lesão-alvo. Após 2 anos pode-se observar incidência maior de eventos cardiovasculares adversos maiores no grupo stent convencional, quando comparado ao grupo Titan, principalmente quanto aos eventos combinados infarto agudo do miocárdio/nova revascularização da lesão-alvo (16,2% vs. 3,2%; P = 0,02). A Figura 1 mostra a curva de sobrevida livre de eventos cardíacos nos dois grupos, significativamente melhor no grupo Titan quando comparado ao grupo stent convencional (93,6% vs. 82,4%; P = 0,036). Em relação à presença de angina, também podemos observar vantagem do grupo Titan (15,9% vs. 29,4%; P = 0,02). Ambos os óbitos que ocorreram no grupo Titan foram decorrentes de causas não-cardíacas. Como os pacientes desse estudo eram oriundos de diferentes cidades, houve perda de 34,5% dos pacientes no seguimento de 2 anos. A perda no grupo Titan foi de 37% e de 32% no grupo stent convencional (P = 0,55). DISCUSSÃO Os resultados desse estudo confirmam que a utilização do stent Titan no tratamento percutâneo da insuficiência coronariana crônica confere vantagens em relação ao stent convencional de aço inoxidável, cursando com taxas de sobrevida livre de eventos cardiovasculares adversos maiores e angina significativamente maiores. O estudo RIO é, até onde se sabe, o maior estudo clínico randomizado em insuficiência coronariana crônica envolvendo a utilização do stent recoberto por titânio-óxido nítrico até o momento, com seguimento de 2 anos. Figura 1 - Curva de sobrevida livre de eventos cardíacos adversos maiores (ECAM) após dois anos. A primeira característica importante desse estudo foram os baixos índices de trombose subaguda do stent com base nos critérios da Academic Research Consortium (ARC) 17, apesar de todos os pacientes em ambos os grupos terem feito uso apenas de ticlopidina ou clopidogrel durante 30 dias associados ao AAS indefinidamente. Alguns estudos demonstraram que os stents recobertos por titânio-óxido nítrico parecem ter superfície menos trombogênica que os stents convencionais ou mesmo que os stents eluidores de fármacos Outro dado importante é o impacto econômico que isso produz, pois pacientes que se submetem ao implante de stents farmacológicos, além do 5
37 Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. elevado custo da endoprótese, têm também que fazer uso de clopidogrel por no mínimo um ano, o que representa aumento ainda maior do custo total do procedimento 18. O único estudo clínico randomizado na insuficiência coronariana crônica comparando o stent Titan com o stent de aço inoxidável foi publicado por Windecker et al. 12 (TiNOX Trial). Esse estudo, elaborado com o intuito de investigar a segurança e a eficácia do Titan comparado ao stent convencional, demonstrou baixos índices de eventos cardiovasculares adversos maiores no grupo Titan, em comparação com o grupo stent convencional (7% vs. 27%; P = 0,02), principalmente pela necessidade de nova revascularização da lesão-alvo (7% vs. 23%; P = 0,07). Todos os pacientes desse estudo foram submetidos a controle angiográfico, o que talvez explique os índices relativamente altos de nova intervenção nos pacientes do grupo stent convencional, bem maiores que os encontrados em nosso estudo. De qualquer maneira, podemos observar nesse estudo taxas de eventos cardiovasculares adversos maiores no grupo Titan semelhantes às encontradas em nossa casuística (7% vs. 6,4%), o que corrobora o bom desempenho clínico do stent Titan. Nosso estudo, por contar com mais pacientes e tempo maior de seguimento, foi mais apropriado para analisar os desfechos clínicos que o estudo de Windecker et al. 12, cujo objetivo primário era analisar a segurança e a eficácia do stent Titan. Foram publicados, até o momento, três registros clínicos sobre a utilização do stent Titan em doença arterial coronariana no mundo real, dois registros multicêntricos descrevendo a experiência com a utilização do Titan na prática diária (Titan-PORI e Titanium- NO) 13,14, e um terceiro registro prospectivo (TITANOX) comparando o stent Titan com o stent eluidor de paclitaxel 15. É interessante observar que todos esses registros incluíram pacientes com infarto agudo do miocárdio, que responderam por pelo menos um terço da população desses estudos. O estudo Titan-PORI 13 investigou a incidência de eventos cardiovasculares adversos maiores 9 meses após implante do stent Titan em 193 pacientes (210 lesões). A taxa de eventos cardiovasculares adversos maiores desse registro foi de 10,4% (4,1%, infarto agudo do miocárdio; 0%, óbito; e 8,3%, revascularização da lesão-alvo). O estudo Titanium-NO 14 analisou a incidência de eventos cardiovasculares adversos maiores 6 meses após implante do Titan em 296 pacientes (333 lesões) e seus achados foram semelhantes aos do Titan-PORI (7,6% de eventos cardiovasculares adversos maiores: 0,7%, infarto agudo do miocárdio; 0,7%, óbito; e 5,4%, revascularização da lesão-alvo). Já o registro TITANOX comparou 201 pacientes (218 lesões) que receberam o Titan com 204 pacientes (224 lesões) que receberam o stent eluidor de paclitaxel no mesmo período, analisando seus índices de eventos cardiovasculares adversos maiores após 30 dias e 1 ano. As taxas de eventos cardiovasculares adversos maiores após 1 ano foram semelhantes nos dois grupos (10,9% Titan vs. 13,7% stent eluidor de paclitaxel; P = 0,40), sendo as taxas de revascularização da lesão-alvo nos dois grupos de 5% e 4,9%, respectivamente. Chama a atenção nesse estudo a diferença dos índices de infarto agudo do miocárdio entre os dois grupos (4,5% Titan vs. 10,3% stent eluidor de paclitaxel; P = 0,025), decorrente do alto índice de trombose subaguda do stent no grupo stent eluidor de paclitaxel (3,4%) contra 0% no grupo Titan. Talvez isso se deva ao fato de grande parte da população do estudo ter sido de pacientes cuja indicação de intervenção percutânea foi infarto agudo do miocárdio. Outro dado que merece ser destacado foram os baixos índices de eventos cardiovasculares adversos maiores em todos esses registros, principalmente se levarmos em conta a complexidade clínica dos pacientes tratados. Nosso estudo demonstrou taxas de eventos cardiovasculares adversos maiores bastante semelhantes a esses registros clínicos, o que o aproxima adequadamente do chamado mundo real. Limitações Existem algumas limitações no presente estudo. Em primeiro lugar, o alto índice de perda de pacientes no seguimento tardio. Infelizmente, a maioria de nossos pacientes provinha de diferentes cidades, algumas muito distantes. Isso, aliado ao fato de serem também pacientes carentes e com poucas condições financeiras para ficar se locomovendo de um local a outro, levou a essa perda relativamente alta. Em segundo lugar, esse estudo não foi duplo cego. O médico sabia qual stent estava sendo implantado em determinado paciente. Apesar disso, como os eventos foram analisados ao longo de 2 anos e os pacientes foram sorteados, não cremos que esse fato tenha alterado nossos resultados. Em terceiro lugar, o desenho de nosso estudo não incluiu controle angiográfico ou acompanhamento de rotina por testes não-invasivos. Assim, certamente as taxas de isquemia silenciosa ou reestenose angiográfica foram subestimadas. Por outro lado, basear nosso seguimento em critérios clínicos certamente evitou revascularizações da lesão-alvo desnecessárias decorrentes do reflexo óculo-estenótico ou mesmo à ansiedade extrema dos pacientes nesses casos. Em quarto lugar, o tamanho de nossa amostra foi relativamente pequeno, principalmente em decorrência de perda tardia. Ainda assim, o total dos pacientes seguidos ao longo de 2 anos (131) foi superior ao número necessário para que nossos resultados fossem válidos estatisticamente (128 pacientes, 64 em cada grupo). De qualquer maneira, é importante que um estudo maior e mais robusto seja conduzido, de modo a confirmar esses resultados. Em quinto lugar, o grupo dos stents convencionais utilizou três stents de empresas diferentes, todos de aço inoxidável, porém com desenhos ligeiramente diversos. Todavia, os resultados da literatura referentes à utilização desses stents 6
38 Sant Anna FM, et al. Estudo Randomizado e Comparativo da Intervenção Coronária Percutânea com Stents Recobertos por Titânio- Óxido Nítrico ou de Aço Inoxidável em Pacientes com Doença Arterial Coronariana: Estudo RIO. Rev Bras Cardiol Invas. 2009;17(1):XX-XX. mostram-se semelhantes em termos de eventos clínicos precoces e tardios. E, em sexto e último lugar, comparamos o stent Titan com o stent convencional de aço inoxidável e não com o stent farmacológico, que hoje é o padrão de referência no tratamento percutâneo da doença aterosclerótica coronariana. No entanto, a utilização do stent convencional ainda é a rotina na maior parte dos centros de cardiologia em nosso País, por ser esse o único stent coberto pelo Sistema Único de Saúde. Buscamos com isso realizar um estudo que refletisse adequadamente nossa prática diária. CONCLUSÃO Esse estudo demonstrou que a utilização do stent recoberto por titânio-óxido nítrico no tratamento percutâneo de pacientes com insuficiência coronariana crônica cursa com baixos índices de eventos cardiovasculares adversos maiores e angina após 2 anos, apresentando resultados melhores que os obtidos com o stent de aço inoxidável. CONFLITO DE INTERESSES Os autores declararam inexistência de conflito de interesses. REFERÊNCIAS BIBLIOGRÁFICAS 1. Peterson ED, Cowper PA, DeLong ER, Zidar JP, Stack RS, Mark DB. Acute and long-term cost implications of coronary stenting. J Am Coll Cardiol. 1999;33(6): Al Suwaidi J, Berger PB, Holmes DR Jr. Coronary artery stents. JAMA. 2000;284(14): Kastrati A, Hall D, Schömig A. Long-term outcome after coronary stenting. Curr Control Trials Cardiovasc Med. 2000; 1(1): Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O Shaughnessy C, et al.; SIRIUS Investigators. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349(14): Garasic JM, Edelman ER, Squire JC, Seifert P, Williams MS, Rogers C. Stent and artery geometry determine intimal thickening independent of arterial injury. Circulation. 2000;101(7): Kastrati A, Mehilli J, Dirschinger J, Dotzer F, Schühlen H, Neumann FJ, et al. Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR- STEREO) trial. Circulation. 2001;103(23): Babapulle MN, Eisenberg MJ. Coated stents for the prevention of restenosis. Part II. Circulation. 2002;106(22): Köster R, Vieluf D, Kiehn M, Sommerauer M, Kähler J, Baldus S, et al. Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet. 2000; 356(9245): Steinemann SG. Titanium: the material of choice? Periodontol ;17: Steinemann SG. Metal implants and surface reactions. Injury. 1996;27(Suppl 3):SC Windecker S, Mayer I, De Pasquale G, Maier W, Dirsch O, De Groot P, et al; Working Group on Novel Surface Coating of Biomedical Devices (SCOL). Stent coating with titaniumnitride-oxide for reduction of neointimal hyperplasia. Circulation. 2001;104(8): Windecker S, Simon R, Lins M, Klauss V, Eberli FR, Roffi M, et al. Randomized comparison of a titanium-nitride-oxidecoated stent with a stainless steel stent for coronary revascularization: the TINOX trial. Circulation. 2005;111(20): Karjalainen PP, Ylitalo A, Airaksinen JK. Real world experience with the TITAN stent: a 9-month follow-up report from The Titan PORI Registry. EuroIntervention. 2006;2: Mosseri M, Miller H, Tamari I, Plich M, Hasin Y, Brizines M. The titanium-no stent: results of a multicenter registry. EuroIntervention. 2006;2: Karjalainen PP, Ylitalo A, Airaksinen JK. Titanium and nitride oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol. 2006;18(10): Reiber JH, Serruys PW, Kooijman CJ, Wijns W, Slager CJ, Gerbrands JJ, et al. Assessment of short-, medium-, and longterm variations in arterial dimensions from computer-assisted quantitation of coronary cineangiograms. Circulation. 1985;71(2): Applegate RJ, Sacrinty MT, Little WC, Santos RM, Gandhi SK, Kutcher MA. Incidence of coronary stent thrombosis based on academic research consortium definitions. Am J Cardiol. 2008;102(6): Cowper PA, Udayakumar K, Sketch MH Jr, Peterson ED. Economic effects of prolonged clopidogrel therapy after percutaneous coronary intervention. J Am Coll Cardiol. 2005; 45(3):
39 C 2010, Wiley Periodicals, Inc. DOI: /j x Five-Year Clinical Outcome of Titanium-Nitride-Oxide-Coated Bioactive Stent Implantation in a Real-World Population: A Comparison with Paclitaxel-eluting Stents: The PORI Registry PASI P. KARJALAINEN, M.D., PH.D., 1 ANTTI YLITALO, M.D., PH.D., 1 JUHANI KE AIRAKSINEN, M.D., PH.D., FESC, 2 and WAIL NAMMAS, M.D. 3 From the 1 Department of Cardiology, Satakunta Central Hospital, Sairaalantie 3, FIN-28100, Pori, Finland; 2 Department of Medicine, Turku University Hospital, Turku, Finland; and 3 Department of Cardiology, Ain Shams University Hospitals, Cairo, Egypt Aims: We sought to present the 5-year clinical outcome of the titanium-nitride-oxide-coated bioactive stents (BAS), as compared to paclitaxel-eluting stents (PES), in a real-world patient population. Methods: From May 2003 to November 2004, we enrolled 405 consecutive patients who underwent percutaneous coronary intervention with either BAS or PES implantation. Patients were prospectively followed up for 5 years. The primary end-point was major adverse cardiac events (MACE) at 5-year follow-up including cardiac death, nonfatal myocardial infarction (MI), or target lesion revascularization. Results: A total of 201 patients received BAS (218 lesions/221 stents) while 204 patients received PES (244 lesions/247 stents). Clinical follow-up for 5 years was completed in all patients. Cumulative MACE at the end of 5-year follow-up occurred in 34 (16.9%) patients in the BAS group, as compared to 53 (26%) in the PES group (OR 1.7, 95% CI , P = 0.03). This difference was mainly driven by a lower incidence of MI in the BAS group as compared with the PES group (9.5% vs. 20.6%, OR 2.5, 95% CI , P = 0.002). Stent thrombosis occurred in 16 (7.8%) patients in the PES group, while no one suffered stent thrombosis in the BAS group. Conclusion: BAS implantation in a real-world patient population achieves an excellent clinical outcome over 5-year follow-up, with a significantly lower incidence of MI, MACE, and stent thrombosis as compared to PES. (J Interven Cardiol 2010; :1 8) Introduction Coronary stent implantation has clearly improved procedural safety and promoted a better outcome of percutaneous coronary interventions (PCI) as compared to balloon angioplasty alone. 1,2 Nevertheless, since the first introduction of coronary stents, in-stent restenosis (ISR) has always been the Achilles heel of this technique, ending up with repeat revascularization and a subsequent increase in health care cost. 3,4 The incidence of ISR after bare metal stent implantation may Address for reprints: Pasi P. Karjalainen, M.D., Satakunta Central Hospital, Department of Cardiology, Sairaalantie 3, FIN-28100, Pori, Finland. Fax: ; pasi.karjalainen@satshp.fi approach 30% in several subgroups of patients, including diabetics, patients with small coronary vessels, and those with long lesions. 5,6 The recent introduction of drug-eluting stents (DES) has, actually, revolutionized the practice of coronary angioplasty, since it has reduced the incidence of ISR by 50 70%. 7,8 However, recent data from meta-analyses and registries have questioned the longterm safety of DES, raising concerns about a higher risk of late stent thrombosis (ST), a potentially lifethreatening complication The safety of titanium-nitride-oxide-coated bioactive stents (BAS) has been confirmed in several studies in real-life unselected populations, as well as in the most challenging indications such as diabetic patients, small coronary vessels, and acute myocardial Vol. **, No. **, 2010 Journal of Interventional Cardiology 1
40 KARJALAINEN, ET AL. infarction (MI) Surprisingly, recent data have demonstrated an even better long-term outcome of BAS in comparison with paclitaxel-eluting stents (PES) in the real-world setting of unselected patients with high-risk clinical features and complex lesion characteristics. 17,18 The purpose of this study was to present the 5-year clinical outcome of BAS implantation, as compared to PES, in this single-center, realworld population with unrestricted use of both types of stents. Patients and Methods Study Design and Patient Selection. The design of the original study has been previously reported. 17,18 Briefly, the PORI Registry was a prospective nonrandomized single-center registry, with the chief aim to evaluate the efficacy and safety of BAS (Titan2 R,Hexacath, Paris, France) as compared to PES in real-world unselected patients in everyday practice. From May 2003 to November 2004, we enrolled a total of 405 consecutive patients with symptomatic ischemic heart disease admitted to undergo PCI. We considered patients eligible for enrollment if they were above 18 years, with at least one significant de novo lesion (defined as at least 50% diameter stenosis by visual estimation) in a native coronary artery or coronary bypass graft. Treatment of more than one vessel was permissible and the stenting indication was determined by operator s discretion. The study population included 201 patients who received BAS and 204 who received PES (Taxus TM, Boston Scientific, Calway, Ireland). This patient population comprised 63% of all patients who underwent PCI during the index study period. Before inclusion, an informed written consent was obtained from each patient after full explanation of the study protocol. Collected data were given a code number for every patient to ensure patients anonymity. The study protocol was reviewed and approved by the Ethics Committee of Satakunta Central Hospital as it conforms to the ethical guidelines of the 1964 Declaration of Helsinki, as revised in Device Used. A commercially available stainless steel tubular stent with the unique helicoidal design was used in this study. Titan2 R stent is a thin strut ( mm) balloon-expandable stent made of stainless steel and coated with titanium-nitride-oxide that completely prevents discharge of nickel, chromium, and molybdenum ions. The coating process is performed by plasma-enhanced vapor deposition of titanium in a prespecified gas mixture of nitrogen and oxygen in a vacuum chamber. Stents were available in lengths of 7, 10, 13, 16, 19, and 22 mm and in diameters of 2.5, 2.75, 3.0, 3.5, and 4.0 mm. Coronary Stenting Procedure. All included patients were already pretreated with aspirin (100 mg daily). Oral clopidogrel was initiated in a loading dose of 300 mg before or immediately after the procedure and continued thereafter at a daily dose of 75 mg. For patients treated with PES, it was prescribed for a minimum of 6 months, according to randomized clinical trials. 8 For patients treated with BAS, it was prescribed for at least 3 months. During the procedure, enoxaparine (1 mg/kg) was given intravenously. Use of periprocedural glycoprotein IIb/IIIa inhibitors was left entirely up to operator s discretion. The medical treatment of coronary artery disease was optimized according to the contemporary guidelines. Lesions were treated according to the contemporary interventional techniques. Predilatation was left to operator s discretion. The operator decided the appropriate diameter to be implanted aiming at a stent: vessel ratio of 1.1:1 prior to stent placement (using nominal pressure). Stents were expanded by adjusting the balloon inflation pressure to achieve an angiographic appearance of the expanded stent slightly larger than the reference vessel segment. After stent deployment, postdilatation was allowed as necessary (at operator s discretion). An additional stent could be deployed in overlap with the first one in case of edge dissection, incomplete lesion coverage, or otherwise suboptimal result (always dictated by operator s discretion). Clinical Follow-up. All patients were observed during hospital stay for the occurrence of the clinical end-points prespecified by the study protocol. Thereafter, patients were prospectively followed up by means of clinic visits or telephone interviews by cardiologists at 1, 3, and 5 years following the index procedure. Follow-up coronary angiography was performed for patients who develop recurrent symptoms during follow-up. The decision to perform further revascularization for the index lesion was based on clinical justification. All patient data available from hospital records, institutional electronic database, or referring physicians were entered into an electronic database, and checked at the end of the follow-up period (November 2009). Study End-points and Definitions. The primary end-point was major adverse cardiac events (MACE), defined as the first occurrence of any of the following 2 Journal of Interventional Cardiology Vol. **, No. **, 2010
41 BIOACTIVE VERSUS PACLITAXEL-ELUTING STENTS during follow-up: cardiac death, nonfatal MI (including Q wave and non-q wave MI), or target lesion revascularization (TLR). Q wave MI was defined as either (1) the occurrence of chest pain or other acute symptoms consistent with myocardial ischemia in the presence of new pathologic Q waves in 2 contiguous leads, or (2) elevated creatine kinase levels >2 times the upper limit of normal lab reference, associated with any elevation above the upper limit of normal of creatine kinase-mb levels, in the presence of new pathologic Q waves. Non-Q wave MI was defined as an elevated creatine kinase >2 times the upper limit of normal lab reference, associated with any elevation above the upper limit of normal of creatine kinase- MB levels. TLR was defined as any repeat intervention (surgical or percutaneous) to treat a significant luminal stenosis within the stent or in the 5-mm distal or proximal segments adjacent to the stent. Revascularization was regarded as clinically-driven if it was motivated by anginal symptoms and/or proven myocardial ischemia in the target vessel territory by noninvasive testing. ST was diagnosed by the occurrence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the index stent, or in autopsy. Angiographic restenosis was defined as 50% diameter stenosis (by visual estimation) within the stent or in the 5-mm distal or proximal segments adjacent to the stent, at follow-up coronary angiography. Statistical Analysis. Continuous variables were presented as mean ± SD, while categorical variables were described with absolute and relative (percentage) frequencies. Comparisons between the two individual groups were performed using the unpaired t-test for continuous, and the Pearson s chi-square test or Fisher s exact test for categorical variables. Propensity scores were used to adjust for potential bias in the comparison between nonrandomized BAS and PES groups. Propensity scores were calculated as the predicted probability that a patient was treated with PES as opposed to BAS using logistic regression. The differences between BAS and PES groups in outcome variables were compared after adjustment for propensity score (linear term) by using Cox regression analysis. Variables included in propensity score model and Cox regression models were age, gender, diabetes, current smoking, hypercholesterolemia, hypertension, previous MI, previous PCI, previous coronary artery bypass grafting (CABG), multivessel disease, acute ST-elevation MI, acute non-st-elevation MI, unstable angina, stent diameter, stent length, and glycoprotein IIb/IIIa inhibitor. Receiver operating characteristic (ROC) curve analysis was used to estimate the area under the curve (AUC) of the model predicting the probability of being included in any of the study groups. The calculated propensity score was used for one-toone matching as well as to adjust for other variables in estimating their impact on the postoperative outcome. Matching between study groups was done according to a difference in the propensity score < MACE, MI, TLR, and ST were analyzed by means of Kaplan Meier survival curves during 5 years of follow-up and the differences between the groups were compared using log-rank test. Cox proportional hazards regression models were included in multivariable Cox regression analysis to identify independent predictors of clinical events during the 5-year follow-up. All tests were two-sided and a probability value of P <0.05 was considered statistically significant. All data were analyzed with the use of SPSS version and SAS system for Windows version 9.1 (SAS Institute Inc., Cary, NC, USA). Results Baseline Characteristics. Between May 2003 and November 2004, 201 patients (218 lesions/221 stents) were treated with BAS, and 204 patients (244 lesions/247 stents) with PES. Baseline clinical characteristics of the study population and the main angiographic and procedural characteristics have been previously detailed. 17 Briefly, patients treated with BAS were older, had more often hypercholesterolemia and hypertension, presented more frequently with acute MI, and had more complex (type B and C) lesions, as compared to those treated with PES, however, the total stent length was, significantly longer in the PES group, as compared to the BAS group, as shown in Tables 1 and 2. Five-Year Follow-Up Data. Clinical follow-up for 5 years was completed in all patients. Clinical follow-up data are presented in Table 3 and Figure 1. Cumulative MACE at the end of 5-year follow-up occurred in 34 (16.9%) patients in the BAS group, as compared to 53 (26%) patients in the PES group (OR 1.7, 95% CI , P = 0.03). Similarly, the incidence of recurrent MI alone was again significantly lower in the BAS group, as compared to the PES group (9.5% vs. 20.6% respectively, OR 2.5, 95% CI , P = Vol. **, No. **, 2010 Journal of Interventional Cardiology 3
42 KARJALAINEN, ET AL. Table 1. Baseline Clinical Characteristics of the 2 Individual Study Groups BAS Group PES Group Variable (N = 201) (N = 204) P Value Age (years) 67 ± ± Male gender 143 (71) 147 (72) 0.85 Diabetes mellitus 34 (17) 37 (18) 0.78 Current smoking 58 (29) 53 (26) 0.31 Hypercholesterolemia 181 (90) 167 (82) Hypertension 133 (66) 110 (54) Prior MI 89 (44) 65 (32) Prior PCI 29 (14) 49 (24) Prior CABG 25 (12) 20 (10) 0.40 Acute STEMI 62 (31) 41 (20) Primary angioplasty 22 (11) 10 (5) Rescue angioplasty 40 (20) 31 (15) 0.21 Acute NSTEMI 52 (26) 49 (24) 0.67 Unstable angina 20 (10) 20 (10) 0.96 Continuous variables are presented as mean ± SD, while categorical variables are presented as frequency (percentage). BAS = bioactive stent; CABG = coronary artery bypass grafting; MI = myocardial infarction; NSTEMI = non-st-elevation myocardial infarction; PCI = percutaneous coronary revascularization; PES = paclitaxel-eluting stent; STEMI = ST-elevation myocardial infarction ). Moreover, 16 (7.8%) patients developed ST in the PES group, of whom nine cases occurred after 1 year from the index procedure (very late stent thrombosis). Meanwhile, no case of ST was observed in the BAS group during follow-up. The c-statistic 0.84 for the propensity score model indicated good discrimination. Several baseline and procedural variables were imbalanced before adjusting for propensity score, but afterwards the differences between BAS and PES groups were nonsignificant, and the balance was achieved. Logistic regression identified the length of stent, ST-elevation MI, any previous MI, any previous PCI, hypercholesterolemia, hypertension as well as older age as independent risk factors of these patients for having been included in the BAS or PES groups. ROC analysis showed an AUC of the calculated propensity score of 0.75 (95% CI , S.E , P < 0.001). After adjustment for propensity score, the differences in MACE (P = 0.005) and in MI or cardiac death (P < 0.001) between the two groups remained significant. In multivariable analysis, older age (HR 1.04, 95% CI , P = 0.02), previous MI (HR 1.6, 95% CI , P = 0.03), non-st-elevation MI as a presenting condition (HR 1.7, 95% CI , P = 0.02) and Table 2. Angiographic and Procedural Characteristics of 2 Individual Study Groups BAS Group PES Group Variable (N = 201) (N = 204) P Value Target vessel LAD 100 (46) 124 (51) 0.29 LCx 48 (22) 37 (15) RCA 54 (25) 68 (28) 0.45 Leftmain 7(3) 7(3) 7(3) Bypass graft 9 (4) 8 (3) 0.63 Lesion type A 26 (12) 54 (22) B 137 (63) 171 (70) 0.10 C 55 (25) 19 (8) <0.001 Reference vessel diameter 2.95 ± ± (mm) Lesion length (mm) 13.1 ± ± Stent diameter (mm) 2.98 ± ± Stent length (mm) 15.6 ± ± 6.7 <0.001 Total stent length per 16.0 ± ± 6.8 <0.001 lesion (mm) Direct stenting 48 (22) 46 (19) 0.40 GP IIb/IIIa inhibitor 54 (27) 49 (24) 0.38 Clopidogrel duration (months) 7.7 ± ± Continuous variables are presented as mean ± SD, while categorical variables are presented as frequency (percentage). LAD = left anterior descending; LCx = left circumflex; RCA = right coronary artery. the use of PES (HR 1.8, 95% CI , P = 0.01) were independent predictors for MACE at 5 years, whereas MI or cardiac death was predicted by older age (HR 1.04, 95% CI , P = 0.001), previous PCI (HR 2.0, 95% CI , P = 0.01) and the use of PES (HR 3.1, 95% CI , P = 0.001). When multivariable models were adjusted for propensity score, the differences in MACE (HR 2.1, 95% CI , P = 0.009) and MI or cardiac death (HR 4.0, 95% CI , P < 0.001) between groups remain significant. Discussion Major Findings. The current study presents the 5- year follow-up of the PORI registry comparing the use of BAS and PES in real-world everyday clinical practice. To the best of the authors knowledge, it represents the longest-term follow-up of such a comparison ever reported in literature. It has demonstrated that 4 Journal of Interventional Cardiology Vol. **, No. **, 2010
43 BIOACTIVE VERSUS PACLITAXEL-ELUTING STENTS Table 3. Clinical Events at 5-Year Follow-Up OR (95% CI) BAS PES OR Adjustment for (N = 201) (N = 204) (95% CI) P Propensity Score P MACE 34 (16.9) 53 (26.0) 1.7 ( ) ( ) MI 19 (9.5) 42 (20.6) 2.5 ( ) ( ) <0.001 TLR 12 (6.0) 21 (10.3) 1.8 ( ) ( ) 0.4 Cardiac death 4 (2.0) 9 (4.4) 2.3 ( ) ( ) 0.3 All-cause death 17 (8.5) 17 (8.3) 1.0 ( ) ( ) 0.9 MI or cardiac death 20 (10.0) 47 (23.0) 2.7 ( ) < ( ) <0.001 Stent thrombosis 0 (0) 16 (7.8) <0.001 <0.001 Fisher s exact test. Variables are presented as frequency (percentage). MACE = major adverse cardiac events; MI = myocardial infarction; TLR = target lesion revascularization. the implantation of BAS in de novo coronary lesions achieves a better long-term outcome as compared to PES. During a 5-year follow-up period, the use of BAS was associated with a lower incidence of MI and total MACE, in comparison with PES, a difference that occurred chiefly during the first 2 years of follow-up. Moreover, the present study demonstrated a fairly high rate of ST, associated with the use of PES in real-world practice. On the other hand, no ST occurred with the use of BAS over 5 years of follow-up. Late Stent Thrombosis after PES Implantation. The incidence of ST associated with PES implantation in the current study was higher than previously reported in studies and registries using PES This relatively higher rate of ST can be attributed, at least in part, to premature discontinuation of clopidogrel. In the current study, 9 patients in the PES group suffered ST after the clopidogrel discontinuation. Most of the patients actually received dual antiplatelet therapy for less than 12 months. Thus, the findings of the current work would also underscore the importance of extended dual antiplatelet therapy following DES implantation. Moreover, total stent length was particularly longer in the PES group in the current study as compared to the BAS group, a fact that might contribute to an elevated ST rate. Pooled analyses of randomized clinical trials of DES demonstrated that on-label use of DES culminates in ST rates identical to those reported with bare metal stents over a 4-year follow-up period. 20,21 Yet, recent data on unrestricted use of first-generation DES in routine clinical practice have shown that late ST occurred at a steady rate of 0.6% per year at 4-year follow-up. 22 Indeed, late ST has emerged as a distinct clinical feature of DES as compared to bare metal stents. Greater delay in arterial healing, as manifested by poor endothelialization and persistence of peristrut fibrin deposition, associated with the implantation of DES may extend the risk of ST far beyond 30 days. Other potential factors predisposing to late ST include stent-vessel mismatch, stent malapposition, overlapping stents, penetration of a necrotic core, excessive stent length, bifurcation lesions, hypersensitivity to drug or polymer, or a thrombogenic surface. 25,26 Premature discontinuation of antiplatelet therapy was recently recognized as the most important predisposing factor for late ST. 27 The obviously higher rate of late ST associated with the use of PES in the current study may well account for the increased rates of MI and total MACE in the PES group. Yet, the incidence of cardiac and all-cause death, and TLR was not different between the two groups. Nevertheless, it should be highlighted that DES are not equal, and the results of the current study using PES might not be extrapolated to the other DES. In this concern, recently released data from the TIDE trial similarly demonstrated an equivalent clinical outcome between titanium-nitride-oxide-coated BAS and a zotarolimusbased DES (Endeavor R, Medtronic, Minneapolis, MN, USA) at 2-year follow-up, including death, MI, TLR, TVR, and ischemia-driven TVR. At 6 8 months angiographic follow-up, however, in-stent late loss was significantly lower in the zotarolimus-eluting stent group. 28 Current Strategy for Reduction of Restenosis. Currently, the use of DES is the state-of-the-art means of reducing ISR in randomized clinical trials including selected patient populations. 7,8,29 Several Vol. **, No. **, 2010 Journal of Interventional Cardiology 5
44 KARJALAINEN, ET AL. A B C D MACE (%) Myocardial Infarction (%) TLR (%) ST (%) log-rank, p= log-rank, p= log-rank, p=0.11 log-rank, p< Figure 1. Kaplan Meier curves representing the estimated 5-year cumulative incidence of total major adverse cardiac events (A), myocardial infarction (B), target lesion revascularization (C), and stent thrombosis (D) 5 years following the implantation of Titan2 R bioactive stent in comparison with Taxus TM paclitaxel-eluting stent. MACE indicates major adverse cardiac events; MI = myocardial infarction; TLR = target lesion revascularization; ST = stent thrombosis. 0 0 randomized controlled studies comparing bare metal stents with the FDA-approved DES demonstrated a significant reduction of ISR with the use of DES, which translated into lower TVR and TLR rates. 7,8,30 Nevertheless, after years of real-life experience with DES, the improvement of restenosis rate was not converted into a reduction of the most powerful hard clinical end-points: death and MI. Additionally, recent worrisome data showed a significant increase of such serious events with the use of DES in predetermined clinical scenarios and/or lesion or procedural characteristics, chiefly due to late and very late ST. 9 11,31,32 Since the dawn of PCI, it was known that ISR is a soft nonlife-threatening event; otherwise, it would have been impossible for PCI to feasibly replace surgical revascularization. Therefore, in our search for a therapeutic strategy that effectively reduces ISR, we cannot accept any increase in the hard end-points as a price paid to reach such a goal. Bioactive Stents. Titanium exhibits a better biocompatibility as compared to stainless steel, gold, or other surface coating materials. 33 Metallic sheaths coated with titanium nitride or titanium oxide demonstrated higher endothelial cell density values on their surfaces in comparison with those without these coatings, suggesting that the use of stents covered with these coatings may accomplish an earlier complete endothelialization. 34 The safety of titanium-nitrideoxide-coated BAS has been validated in several clinical trials in both unselected populations as well as in the most complex indications such as diabetic patients and those presenting with acute MI Recently, a randomized study has demonstrated an even better outcome with BAS implantation in comparison with PES in patients presenting with acute MI. 35,36 Clinical Implications. A cost-effectiveness analysis of DES based on the BASKET trial justified the use of DES only in high-risk patients. 37 Achievement of the goal of reducing TLR to a degree similar to DES, without taking the risk of life-threatening hard end-points of late and very late ST, would be an appealing strategy in combating ISR. Furthermore, unlike DES, which need maintenance clopidogrel therapy for at least 12 months (sometimes even for more extended periods), with BAS, this therapy is required for no more than 1 month. In this context, BAS appear to open a new horizon for revascularization of coronary atherosclerosis. Study Strengths and Limitations. The strength of this single-center registry is the fact that Satakunta 6 Journal of Interventional Cardiology Vol. **, No. **, 2010
45 BIOACTIVE VERSUS PACLITAXEL-ELUTING STENTS Central Hospital is the only center with a coronary angiography facility in the referral area. In this rural area, population is stationary enabling complete and extended follow-up of an unrestricted patient population undergoing coronary revascularization in daily clinical practice. The PORI registry was not randomized, and hence it was liable for selection bias. Propensity adjustment cannot be expected to completely compensate for group differences when one is dealing with only around 200 patients in each group with the relatively low incidence of end-points studied. Additionally, it bears an inherent limitation of any registry, namely, the nonblinded outcome assessment. Furthermore, whether the outcome of the PES in this registry can be extrapolated to the other members of the DES family remains to be determined. Finally, TLR was clinically driven, and this may underestimate the actual incidence of restenosis, however, it would avoid unnecessary interventions in borderline lesions due to the oculostenotic reflex or undue patients anxiety. Conclusions BAS implantation in a real-world patient population achieves an excellent clinical outcome over 5-year follow-up, with a significantly lower incidence of MI, MACE, and ST as compared to PES. References 1. Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331: Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331: Peterson ED, Cowper PA, DeLong ER, et al. Acute and longterm cost implications of coronary stenting. J Am Coll Cardiol 1999;33: Al Suwaidi J, Berger PB, Holmes DR Jr. Coronary artery stents. JAMA 2000;284: Abizaid A, Kornowski R, Mintz GS, et al. The influence of diabetes mellitus on acute and late clinical outcomes following coronary stent implantation. J Am Coll Cardiol 1998;32: Kastrati A, Hall D, Schömig A. Long-term outcome after coronary stenting. Curr Control Trials Cardiovasc Med 2000;1: Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349: Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med 2004;350: Nordmann AJ, Briel M, Bucher HC. Mortality in randomized controlled trials comparing drug-eluting vs. bare metal stents in coronary artery disease: A meta-analysis. Eur Heart J 2006;27: Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first generation drug-eluting stents: A cause for concern. Circulation 2007;115: Lagerqvist B, James SK, Stenestrand U, et al. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N Engl J Med 2007;356: Windecker S, Simon R, Lins M, et al. Randomized comparison of a titanium-nitride oxide-coated stent with a stainless steel stent for coronary revascularization. The TINOX trial. Circulation 2005;111: Karjalainen PP, Ylitalo A, Airaksinen KE. Real world experience with the TITAN stent: A 9-month follow-up report from the Titan PORI registry. EuroInterv 2006;2: Mosseri M, Miller H, Tamari I, et al. The titanium-no stent: Results of a multicenter registry. EuroInterv 2006;2: Mosseri M, Tamari I, Plich M, et al. Short and long term outcome of the Titanium-NO stent registry. Cardiovasc Revasc Med 2005;6: Giraud-Sauveur Y. Titan 2 Bioactive stent (BAS) with titanium- NO. EuroInterv 2007;3: Karjalainen PP, Ylitalo A, Airaksinen JK. Titanium and nitride oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol 2006;18: Karjalainen PP, Annala AP, Ylitalo A, et al. Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. Int J Cardiol 2009; doi: /j.ijcard Buehl A, Zoefel P. SPSS 11: Introduction in Modern Data Analysis. 8th ed. Munich, Germany: Addison-Wesley, Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and paclitaxel eluting coronary stents. N Engl J Med 2007;356: Mauri L, Hsieh W, Massaro JM, et al. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med 2007;356: Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxeleluting stents in routine clinical practice: Data from a large two-institutional cohort study. Lancet 2007;369: Daemen J, Tanimoto S, García-García HM, et al. Comparison of three-year clinical outcome of sirolimus- and paclitaxel-eluting stents versus bare metal stents in patients with ST-segment elevation myocardial infarction (from the RESEARCH and T-Search Registries). Am J Cardiol 2007;99: Wenaweser P, Daemen J, Zwahlen M, et al. Incidence and correlates of drug-eluting stent thrombosis in routine clinical practice. J Am Coll Cardiol 2008;52: Virmani R, Guagliumi G, Farb A, et al. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious? Circulation 2004;109: Finn AV, Nakazawa G, Joner M, et al. Vascular responses to drug eluting stents. Importance of delayed healing. Arterioscler Thromb Vasc Biol 2007;27: Daemen J, Serruys PW. Drug-eluting stent update 2007: Part II: Unsettled issues. Circulation 2007;116: Vol. **, No. **, 2010 Journal of Interventional Cardiology 7
46 KARJALAINEN, ET AL. 28. Windecker S. Randomized Comparison of Titanium-nitrideoxide Coated Stents with Zotarolimus-eluting Stents for Coronary Revascularization. Paris, France: EuroPCR, Babapulle MN, Joseph L, Belisle P, et al. A hierarchical Bayesian meta-analysis of randomized clinical trials of drugeluting stents. Lancet 2004;364: Morice MC, Serruys PW, Sousa JE, et al Randomized study with the sirolimus-coated Bx velocity balloon-expandable stent in the treatment of patients with de novo native coronary artery lesions. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346: Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: Results from the PREMIER registry. Circulation 2006;113: Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293: Steinemann SG. Metal implants and surface reactions. Injury 1996;27(Suppl. 3):SC Hung-I Y, Shao-Kou L, Tin-Yi T, et al. Comparison of endothelial cells grown on different stent materials. J Biomed Mater Res A 2006;76: Karjalainen PP, Ylitalo A, Niemelä M, et al. Titaniumnitride-oxide coated stents versus paclitaxel-eluting stents in acute myocardial infarction: A 12-months follow-up report from the TITAX AMI trial. EuroInterv 2008;4: Karjalainen PP, Ylitalo A, Niemela M, et al. Two-year followup after percutaneous coronary intervention with titaniumnitride-oxide-coated stents versus paclitaxel-eluting stents in acute myocardial infarction. Ann Med 2009;21: Kaiser C, Brunner-La Rocca HP, Buser PT, et al. Incremental cost-effectiveness of drug-eluting stents compared with a third-generation bare-metal stent in a real-world setting: Randomised Basel Stent Kosten Effektivitäts Trial (BASKET). Lancet 2005;366: Journal of Interventional Cardiology Vol. **, No. **, 2010


47 IJCA-11970; No of Pages 5 ARTICLE IN PRESS International Journal of Cardiology xxx (2009) xxx xxx Contents lists available at ScienceDirect International Journal of Cardiology journal homepage: Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population Pasi P. Karjalainen a,, Antti-Pekka Annala a, Antti Ylitalo a, Tero Vahlberg b, K.E. Juhani Airaksinen c a Department of Cardiology, Satakunta Central Hospital, Sairaalantie 3, FIN-28100, Pori, Finland b Department of Biostatistics, University of Turku, Turku, Finland c Department of Medicine, Turku University Hospital, Turku, Finland article info abstract Article history: Received 24 June 2008 Received in revised form 7 January 2009 Accepted 26 March 2009 Available online xxxx Keywords: Titanium-nitride-oxide-coated stent Paclitaxel-eluting stent Restenosis Stent thrombosis Background: The aim of this study was to evaluate long-term clinical events in patients treated with titaniumnitride-oxide-coated bio-active stents (BAS) and paclitaxel-eluting stents (PES) in routine clinical practice. Methods: All patients undergoing percutaneous coronary intervention (PCI) were eligible for this singlecentre registry between May 2003 and November The primary end point of the study was major adverse cardiac events (MACE) at 3 years including myocardial infarction (MI), cardiac death and target vessel revascularization (TVR). Results: A total of 201 patients received BAS and 204 patients PES. In addition, during the same study period, 184 patients were treated with bare-metal stents (BMS) and 125 patients underwent CABG. Complete follow-up datasets were available in all patients. After 3 years of follow-up, the rate of MACE was 13.9% for BAS and 23.5% for PES (adjusted HR 2.0, 95% CI , p =0.006). This difference was mainly driven by a higher incidence of MI in the PES group (19.1%) compared with the BAS (7.5%) group (adjusted HR 3.2, 95% CI , pb0.001). The rate of MACE was 31.5% in the BMS group and 4% in the CABG group. At 3 years, stent thrombosis occurred in 15 patients in the PES (7.4%) group. There was no stent thrombosis in the BAS group. Conclusions: After the 3 year follow-up, BAS resulted in better long-term outcome compared with PES with infrequent need for TVR Elsevier Ireland Ltd. All rights reserved. 1. Introduction The three major milestones in the evolution of interventional cardiology were the development of the balloon angioplasty, the introduction of coronary-artery stents and most recently, the development of drug eluting stents (DES). Although the implantation of coronary-artery stents has reduced the risk of periprocedural complications, in-stent restenosis (ISR) is still a clinical problem of bare-metal stents (BMS) [1,2]. At present, the use of DES is the most effective way to reduce ISR according to randomized controlled trials in selected patient groups [1 4]. With the increasing utilization of DES during the last few years, there have been concerns that some patients develop stent thrombosis (ST), a life threatening complication, unusually late after the implantation of DES [4,5]. Titanium features superior biocompatibility when compared with stainless steel, gold, or other surface coatings [6]. Metallic sheaths coated with titanium nitride or titanium oxide exhibited higher cell density values on their surface compared to those without coating, This work was supported by grants from the Finnish Foundation for Cardiovascular Research, Helsinki, Finland. Corresponding author. Tel.: ; fax: address: pasi.karjalainen@satshp.fi (P.P. Karjalainen). supporting the view that deployment of stents with these coatings may achieve earlier complete endothelial coverage [7]. The safety of titanium-nitride-oxide-coated Titan-2 bio-active-stent (BAS) has been confirmed by several clinical studies in both unselected populations as well as in the most complex indications such as diabetics, small vessels and acute myocardial infarction (MI) [8 11]. Paclitaxel, a lipophilic molecule derived from the Pacific yew tree Taxus brevifolia, is capable of inhibiting cellular division, motility, activation, secretory processes, and signal transduction [12,13]. A polymer-based, paclitaxel-eluting stent (PES) reduced the rate of ISR as compared with BMS [2,4]. Previously, both the BAS and PES resulted in similar 12 month clinical outcome with infrequent need for repeat interventions in the real-world setting of high-risk patients and complex coronary lesions [9]. The aim of this study was to report long-term clinical outcome of this patient population with unrestricted use of BAS and PES(s). 2. Materials and methods 2.1. Patient population The design of the original study has been previously reported [9]. Briefly, the main purpose of this prospective single-center registry was to evaluate the safety and efficacy of BAS and PES implantation for consecutive unselected patients treated in everyday /$ see front matter 2009 Elsevier Ireland Ltd. All rights reserved. doi: /j.ijcard Please cite this article as: Karjalainen PP, et al, Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population, Int J Cardiol (2009), doi: /j.ijcard
48 ARTICLE IN PRESS 2 P.P. Karjalainen et al. / International Journal of Cardiology xxx (2009) xxx xxx clinical practice. Between May 2003 and November 2004, all consecutive patients with symptoms or signs of myocardial ischemia and de novo coronary lesion(s) scheduled for stent implantation were considered for this registry. A total of 405 patients fulfilled the criteria and entered this study. A total of 201 patients received exclusively one or more BAS, and 204 received only one or more PES. This patient population comprised 63% of all patients who underwent percutaneous coronary intervention (PCI) during the study period. In addition to original study population, we also gathered baseline data on patients receiving BMS(s) during the index study period in our centre, and these patients were also followed up to 3 years. The similar data from patients undergoing coronary-artery bypass grafting (CABG) were also collected. We also wanted to evaluate clinical events after clopidogrel discontinuation in all patients undergoing PCI with stent implantation. All patients who were MACE free at the time of the clopidogrel discontinuation were followed for an additional 12 months after the clopidogrel withdrawal. The study was conducted according to the declaration of Helsinki and written informed consent was obtained from all patients. This protocol was approved by the Ethics Committee of Satakunta Central Hospital Study procedures All patients were pre-treated with aspirin (100 mg daily) and received intravenous enoxaparine (1 mg/kg) during the procedure. Oral clopidogrel was administered as a loading dose of 300 mg before or immediately after the procedure. Patients treated with PES were prescribed for a minimum of 6 months of clopidogrel (75 mg/day), based on randomized controlled trials [2]. For patients treated with BAS, clopidogrel was prescribed for a minimum of 3 months. Lesions were treated according to current standard interventional techniques, with the final strategy (thrombectomy devices, direct stenting, postdilatation, periprocedural glycoprotein IIb/IIIa inhibitor, intravascular ultrasound) left entirely up to the operator's discretion. Angiographic success was defined as a residual stenosis b30% by visual analysis in the presence of Thrombolysis In Myocardial Infarction (TIMI) flow grade 3. The choice of an individual stent in BMS group was left at the discretion of the operator and these patients received at least 1 month duration of clopidogrel treatment after the index procedure. CABG was done according to current standard surgical techniques. After the CABG all patients were treated with aspirin indefinitely and the clopidogrel prescription was left to the decision of consulting surgeon Patients follow-up All patients underwent clinical follow-up. Adverse events were monitored at hospital discharge and by office visits or telephone interviews by the cardiologist at 1 and 3 years. In addition, all data available from hospital records, the institutional electronic clinical database, and the referring physicians were checked at the end of the follow-up period (November 2007) and entered into the computer database. Follow-up angiography was clinically driven by symptoms or signs suggestive of myocardial ischemia. Indication for repeat revascularization was a significant luminal stenosis (N50% diameter stenosis) in the presence of anginal symptoms and/or proven myocardial ischemia in the target vessel territory End point definitions The primary end point was major adverse cardiac events (MACE), defined as the first occurrence of any of the following during the follow-up: death from cardiac causes, Q-wave or non-q-wave myocardial infarction (MI), or revascularization of the target vessel (emergency or elective coronary-artery bypass grafting or repeated coronary angioplasty). Q-wave MI was defined as either (1) the presence of chest pain or other acute symptoms consistent with myocardial ischemia and new pathologic Q waves in 2 continuous electrocardiographic leads, or (2) elevated cardiac enzyme levels N2 times the upper limit of normal associated with any elevation above the upper limit of normal in creatine kinase-mb levels in the presence of new pathologic Q waves. Non-Qwave MI was defined as an elevated creatine kinase N2 times the upper limit of normal associated with any elevation above the upper limit of normal in creatine kinase-mb levels. Target lesion revascularization (TLR) was defined as a repeat intervention to treat a stenosis within the stent or in the segments 5 mm distal or proximal to the stent. Target vessel revascularization (TVR) was defined as a reintervention driven by any lesion located in the stented vessel. ST per-protocol was diagnosed in the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent, or in autopsy Statistical analysis Continuous variables are presented as mean (SD) and groups were compared by Student's unpaired t-test. Categorical variables are presented as counts and percentages and associations between categorical variables were compared by the chi-square or Fisher's exact test. Variables significantly (pb0.05) associated with clinical events in univariate Cox proportional hazards regression models, were included in multivariable Cox regression analysis to identify independent predictors for clinical events during the 3 year follow-up. Propensity scores were used to adjust for potential bias in the comparison between non-randomized BAS and PES groups. Propensity scores were calculated as the predicted probability that patient was treated by PES as opposed to BAS using logistic regression. The differences between BAS and PES groups in outcome variables were compared after adjustment for propensity score (linear term) by using Cox regression analysis. Propensity score was also included in multivariable models. Variables included in propensity score model and Cox regression models were age, gender, diabetes, current smoking, hypercholesterolemia, hypertension, previous MI, previous PCI, previous CABG, multivessel disease, acute ST-elevation MI, acute non-st-elevation MI, unstable angina, stent diameter, stent length and glycoprotein IIb/IIIa inhibitor. A two- Table 1 Clinical events during 3 years of follow-up. BAS (N=201) PES (N=204) HR (95% CI) Cox regression p HR (95% CI) adjustment for propensity score p MI, n (%) Patient with any event 15 (7.5) 39 (19.1) 2.8 ( ) b ( ) b to 12 months after index PCI 9 (4.5) 21 (10.3) 0.03 N12 months after index PCI 6 (3.0) 18 (8.8) 0.01 Cardiac death, n (%) Patient with any event 2 (1.0) 7 (3.4) 3.5 ( ) ( ) to 12 months after index PCI 1 (0.5) 5 (2.5) 0.1 N12 months after index PCI 1 (0.5) 2 (1.0) 0.6 TVR, n (%) a Patient with any event 17 (8.5) 23 (11.3) 1.4 ( ) ( ) to 12 months after index PCI 16 (8.0) 14 (6.9) 0.7 N12 months after index PCI 1 (0.5) 9 (4.4) 0.01 TLR, n (%) Patient with any event 11 (5.5) 19 (9.3) 1.8 ( ) ( ) to 12 months after index PCI 10 (5.0) 10 (4.9) 1.0 N12 months after index PCI 1 (0.5) 9 (4.4) 0.01 MACE, n (%) Patient with any event 28 (13.9) 48 (23.5) 1.8 ( ) ( ) to 12 months after index PCI 22 (10.9) 28 (13.7) 0.4 N12 months after index PCI 6 (3.0) 20 (9.8) Stent thrombosis, n (%) Patient with any event 0 (0) 15 (7.4) b0.001 b 0 to 12 months after index PCI 0 (0) 7 (3.4) N12 months after index PCI 0 (0) 8 (3.9) MI or cardiac death, n (%) 15 (7.5) 42 (20.6) 3.0 ( ) b ( ) b0.001 All cause death, n (%) 11 (5.5) 13 (6.4) 1.2 ( ) ( ) 0.7 MI = myocardial infarction. PCI = percutaneous coronary intervention. TVR = target vessel revascularization. TLR = target lesion revascularization. a Including patients with TLR. b Fisher's exact test. Please cite this article as: Karjalainen PP, et al, Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population, Int J Cardiol (2009), doi: /j.ijcard
49 ARTICLE IN PRESS P.P. Karjalainen et al. / International Journal of Cardiology xxx (2009) xxx xxx 3 sided p valueb0.05 was required for statistical significance. All cause death, TVR, MI and MACE were analyzed by means of Kaplan Meier survival curves during the 3 years of follow-up and the differences between groups were compared using log-rank test. All data were analyzed with the use of SPSS version 11 [14] and SAS system for Windows version 9.1 (SAS Institute Inc., Cary, NC, USA). 3. Results 3.1. Clinical follow-up of the original study population Between May 2003 and November 2004, 201 patients (218 lesions/221 stents) were treated with BAS, and 204 patients (244 lesions/247 stents) with PES. The baseline clinical characteristics of the study population and the main procedural characteristics have been described in detail previously [9]. Briefly, the BAS patients were older, and they had more often hypercholesterolemia and hypertension in their medical history. In addition, BAS patients had more often acute MI as their presenting symptom and more complex B and C-type lesions treated. The total stent length was, however, significantly longer (pb0.001) in the PES group. Outcome events during the 3 year follow-up are listed in Table 1. Complete follow-up was obtained in all 405 patients. MACE-free survival at 3 years was 86.1% in the BAS group, as compared with 76.5% in the PES group (p=0.02, Table 1, Fig. 1). The rate of recurrent MI or cardiac death was significantly lower in the BAS group compared with the PES group (pb0.001). In addition, a total of 15 patients (7.4%) suffered ST in the PES group, of which 8 cases occurred after 1 year from the index procedure (very late ST). There was no ST observed in the BAS group. Clinically driven control angiography was done in 28% of the patients in BAS group and 29% of the patients in PES group during the 3 year follow-up. The c-statistic 0.82 for the propensity score model indicated good discrimination. Several baseline and procedural variables were imbalanced before adjusting for propensity score, but afterwards the differences between BAS and PES groups were non-significant, and the balance was achieved. After adjustment for propensity score, the differences in MACE (p=0.008) and in MI or cardiac death (pb0.001) between groups remained significant. In multivariable analysis, MACE at 3 years was predicted by older age (HR 1.03, 95% CI , p=0.02), previous MI (HR 1.7, 95% CI , p=0.03), non-st-elevation MI as presenting symptom (HR 1.8, 95% CI , p=0.01) and the use of PES (HR 2.0, 95% CI , p=0.006). MI or cardiac death was predicted by older age (HR 1.05, 95% CI , pb0.001), previous PCI (HR 2.1, 95% CI , p=0.009) and the use of PES (HR 3.2, 95% CI , pb0.001). After multivariable models were adjusted for propensity score the differences in MACE (HR 2.2, 95% CI , p=0.007) and MI or cardiac death (HR 4.1, 95% CI , pb0.001) between groups remained significant Clinical follow-up of the patients receiving BMS or undergoing CABG A total of 184 patients underwent PCI with BMS implantation during the same study period. Baseline and procedural characteristics in BMS group compared to original study population were comparable except that PES patients had more PCI's in their medical history (24% Fig. 1. The event-free survival during the 3 year follow-up period estimated with the Kaplan Meier method. The significance of differences between treatment groups was assessed by the log-rank test. (A) Myocardial infarction, (B) all cause death, (C) target vessel revascularization, and (D) MACE. Please cite this article as: Karjalainen PP, et al, Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population, Int J Cardiol (2009), doi: /j.ijcard
50 ARTICLE IN PRESS 4 P.P. Karjalainen et al. / International Journal of Cardiology xxx (2009) xxx xxx in PES group vs. 7% in BMS group), and PES patients also received longer stents than BMS patients (21.2 mm vs mm, respectively). In BMS group, patients had more often acute non-st-elevation MI as their presenting symptom before the procedure compared with PES group (39% in BMS group vs. 24% in PES group). When comparing to BAS group, BMS patients had less often previous MI in their medical history (44% in BAS group vs. 32% in BMS group) and also less complex C-type lesions treated (25% vs. 4%, respectively). CABG was done in 124 patients during the study period (mean age 64 years [range 38 85], 86% male). Diabetes was present in 26%, hypercholesterolemia in 92% and hypertension in 62% of patients, and 18% of patients were current smokers. A total of 14 patients (11%) had revascularization (11 patients PCI and 3 CABG) and 33 patients (27%) MI in their medical history. Ten patients (8%) had single vessel disease, and 41 patients (9 patients had ST-elevation MI, 28 non-st-elevation MI and 4 unstable angina) presented with acute coronary syndrome before the index angiography and subsequent CABG. The overall rate of MACE in CABG patients during 3 years of followup was 4% including 3 events of sudden cardiac death (2.4%), 3 events of acute MI (2.4%) and 1 event of TVR (0.8%). Only 1 patient died during the index hospitalisation, and this event occurred 2 days after the CABG. In addition, 2 patients died for non-cardiac cause during the follow-up. Fig. 1 illustrates the 3 year outcome events (MI, all cause death, TVR and MACE) in patients who received either BAS, PES or BMS, and in patients who underwent CABG. During the 3 year follow-up, perprotocol defined ST occurred in 2.7% of patients in BMS group (p=0.4 vs. BAS group; p=0.03 vs. PES group) Late follow-up after the clopidogrel discontinuation A consecutive series of 589 non-selected patients underwent PCI with stenting during the study period and 519 of them remained MACE free at the time of clopidogrel discontinuation (184 patients in BAS,183 in PES and 152 in BMS groups). During the 12 month follow-up after the clopidogrel withdrawal, there was no difference in the incidence of MACE between the three groups, but the incidence of MI was higher in PES group compared with the other two stent groups (Fig. 2). After the clopidogrel discontinuation, ST occurred more frequently in the PES group compared with the BAS group (3.8% vs. 0%, p=0.009). 4. Discussion 4.1. Major findings This study is the first long-term comparison of BAS with PES in routine clinical practice. The major finding of this study is that the unrestricted use of BAS in de novo lesions leads to a favourable longterm outcome compared with PES even in high-risk patients with complex coronary lesions. Secondly, although the overall risk of ST was fairly low, it was concentrated on the use of PES in the setting of acute MI. In addition, between 1 to 3 years, the use of PES resulted in significantly higher incidence of recurrent MI, ST and subsequent MACE compared with the use of BAS. The present study also showed that after clopidogrel discontinuation the rate of recurrent MI and very late ST was more common in PES group compared with other stent groups. In patients undergoing CABG, we observed lower rates of MACE and repeated revascularization compared to other study groups. On the other hand, the similar incidence of all cause death was observed in CABG and PES patients Safety of DES At present, the use of DES is the most effective way to reduce ISR according to randomized controlled trials in selected patient groups [1 3]. However, there is no evidence that DES or BMS could influence Fig. 2. Outcome events during the 12 month follow-up after the discontinuation of clopidogrel. TLR= target lesion revascularization; MI = myocardial infarction. BAS versus PES, p=0.01; BMS versus PES, p=0.01. BAS versus PES, p= mortality or MI after stent implantation [2,3]. The benefit of the 1st generation and pioneer DES's (Cypher and Taxus ) is related to more powerful inhibition of neointimal hyperplasia compared with BMS but these devices may have some side effects as well, some of which only arose recently [4,15]. There have been some concerns that some patients develop ST, a life threatening complication, unusually late after the implantation of DES [4]. The overall rate of ST in PES group was higher in the present study than in previous studies and registries of DES [2,4,5,15-17]. The higher rate may have been due to the inclusion of patients with more complex conditions and lesions and a higher prevalence of acute coronary syndromes. Total stent length was significantly longer in the PES group compared with the other stent groups which may partly explain our findings. It has been suggested that late ST has emerged as a distinct clinical entity with DES compared with BMS. Greater delay in arterial healing as manifested by poor endothelialization and persistence peristrut fibrin deposition associated with the implantation of DES may extend the risk of ST far beyond 30 days. Late ST is potentially due to a mismatch between the stent and the vessel and may be related to stent malapposition, overlapping stent placement, penetration of necrotic core, excessive stent length, bifurcation lesions, hypersensitivity to drug or polymer, or thrombogenic surface [18,19]. Premature discontinuation of antiplatelet therapy is recently recognised as the most important predisposing factor for late ST [20]. In the present study, 6 patients in the PES group and 4 patients in the BMS group suffered ST after the clopidogrel discontinuation. Most of the patients received dual antiplatelet treatment less than 12 months, and therefore the findings of the present work also underline the importance of proper and long-enough dual antiplatelet treatment. Historically, diagnosis of ST has been based of angiographic and clinical criteria, but any measurements of ST were complicated by the lack of a standardized definition. The recently proposed Academic Research Consortium has developed definitions of ST for use in future trials [21]. For on-label use of DES, identical rates of ST were observed in both selected DES and BMS patients up to 4 years according to Please cite this article as: Karjalainen PP, et al, Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population, Int J Cardiol (2009), doi: /j.ijcard
51 ARTICLE IN PRESS P.P. Karjalainen et al. / International Journal of Cardiology xxx (2009) xxx xxx 5 pooled analyses of randomized DES trials [4,5]. Recently presented data with the unrestricted use of first generation DES in routine clinical practice demonstrated that late ST occurred at a steady rate of 0.6% per year up to 4 years of follow-up [15]. In addition, despite the different incidence of ISR and ST, long-term death and MI rates appeared to be similar in pivotal DES trials in patients receiving either BMS or DES, including only relatively lowrisk patients. The incidence of all cause death in our study was similar between the study groups whilst the rate of recurrent MI appeared to be higher in the PES group. Although DES's seem to be safe and effective in on-label use, the long-term safety of off-label indications has not yet been properly evaluated Titanium-nitride-oxide-coating The rate of TLR was moderately low in both BAS and PES groups. Surprisingly there was no ST in the BAS group. Stent coating may contribute to these findings, since in vitro study has suggested that titanium-nitride-oxide reduces platelet adhesion and fibrinogen binding compared with stainless steel [6]. Titanium, a material commonly used for medical implants, features superior biocompatibility when compared with stainless steel, gold, or other surface coatings. Metallic sheaths coated with titanium nitride or titanium oxide exhibited higher cell density values on their surface compared to those without coating, supporting the view that deployment of stents with these coatings may achieve earlier complete endothelial coverage [7]. The safety of BAS has been confirmed by several clinical studies in both unselected populations as well as in the most complex indications such as diabetics, small vessels and acute MI [8 11] Outcome of patients receiving BMS or undergoing CABG At 3 years, the MACE rate in BMS group was higher compared to other stent groups and also to CABG group. This was mainly driven by a moderately high incidence of recurrent MI, TLR and cardiac death in the BMS group. It seems evident that when BMS are compared to DES [4,5] and also newer generation coated stents [11], the rate of TLR is high. In addition, the present study showed a favourable long-term outcome (MACE, MI and TVR) in patients undergoing CABG compared with patients undergoing PCI imitating the results of ARTS I and II trials [22,23]. The small sample size in CABG group may, however, limit the interpretation of these results Limitation The strength of our single-center registry is the fact that Satakunta Central Hospital is the only centre with coronary angiography capacity in the referral area. In this rural area, population is stationary enabling complete and long-enough follow-up of an all-inclusive unrestricted patient population undergoing coronary revascularization in daily clinical practice. In addition, all patients during the study period undergoing PCI or CABG were included in these analyses reflecting the actual outcome of patients with coronary heart disease needing revascularization. One of the limitations of our study is the limited size of the patient groups for subgroup analysis. This study carries the general problems of registry based observational studies with nonblinded outcome assessment. Low patient number registry may also give rise to unrecognised selection and performance bias. Angiographic control was performed in a minority of patients, and we may have underestimated the incidence of angiographic ISR and silent ST. On the other hand, by relying on clinical follow-up only, we avoided the chance of unnecessary TLR due to the oculostenotic reflex or patient's unjustified anxiety. 5. Conclusions In conclusion, BAS resulted in favourable clinical outcome during the 3 year follow-up with a reduced incidence of recurrent MI, MACE and ST compared with PES. The present findings suggest that there is a place for these new-generation bare-metal, bio-active -stents with proper vascular healing in the present day interventional cardiology. Acknowledgement The authors of this manuscript have certified that they comply with the Principles of Ethical Publishing in the International Journal of Cardiology [24]. References [1] Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349: [2] Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med 2004;350: [3] Babapulle MN, Joseph L, Belisle P, Brophy JM, Eisenberg MJ. A hierarchical bayesian meta-analysis of randomized clinical trials of drug-eluting stents. Lancet 2004;364: [4] Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and paclitaxeleluting coronary stents. N Engl J Med 2007;356: [5] Mauri L, Hsieh W, Massaro JM, Ho KK, D'Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med 2007;356: [6] Steinemann SG. Metal implants and surface reactions. Injury 1996;27(suppl 3): SC [7] Hung-I Y, Shao-Kou L, Tin-Yi T, Ray-Ching H, Wun-Hsing L, Cheng-Ho T. Comparison of endothelial cells grown on different stent materials. J Biomed Mater Res A 2006;76: [8] Karjalainen PP, Ylitalo A, Airaksinen KE. Real world experience with the TITAN stent: a 9-month follow-up report from the Titan PORI registry. Eurointerv 2006;2: [9] Karjalainen PP, Ylitalo A, Airaksinen JK. Titanium and nitride oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol 2006;18: [10] Mosseri M, Miller H, Tamari I, et al. The titanium-no stent: results of a multicenter registry. Eurointerv 2006;2: [11] Giraud-Sauveur Y. Titan 2 bio-active stent (BAS) with titanium-no. Eurointerv 2007;3: [12] Belotti D, Vergani V, Drudis T, et al. The microtubule-affecting drug paclitaxel has antiangiogenic activity. Clin Cancer Res 1996;2: [13] Giannakakou P, Robey R, Fojo T, Blagosklonny MV. Low concentrations of paclitaxel induce cell type-dependent p53, p21 and G1/G2 arrest instead of mitotic arrest: molecular determinants of paclitaxel-induced cytotoxicity. Oncogene 2001;20: [14] Buehl A, Zoefel P. SPSS 11: introduction in modern data analysis. 8th ed. Munich, Germany: Addison-Wesley; [15] Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study. Lancet 2007;369: [16] Daemen J, Tanimoto S, Garcia-Garcia H, et al. Comparison of three-year clinical outcome of sirolimus- and paclitaxel-eluting stents versus bare metal stents in patients with ST-segment elevation myocardial infarction (from the RESEARCH and T-Search Registries). Am J Cardiol 2007;99: [17] Wenaweser P, Daemen J, Zwahlen M, et al. Incidence and correlates of drug-eluting stent thrombosis in routine clinical practice. J Am Coll Cardiol 2008;52: [18] Virmani R, Guagliumi G, Farb A, et al. Localized hypersensitivity and late coronary thrombosissecondaryto a sirolimus-elutingstent: shouldwebecautious? Circulation 2004;109: [19] Finn AV, Nakazawa G, Joner M, et al. Vascular responses to drug eluting stents. Importance of delayed healing. Arterioscler Thromb Vasc Biol 2007;27: [20] Daemen J, Serruys PW. Drug-eluting stent update 2007: part II: unsettled issues. Circulation 2007;116: [21] Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials. Circulation 2007;115: [22] Serruys PW, Ong AT, van Herwerden LA, et al. Five-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease: the final analysis of the Arterial Revascularization Therapies study (ARTS) randomized trial. J Am Coll Cardiol 2005;46: [23] Serruys PW, Ong AT, Morice M-C, et al. Arterial revascularization therapies study part II sirolimus-eluting stents for the treatment of patients with multivessel de novo coronary artery lesions. Eurointerv 2005;1: [24] Coats AJ. Ethical authorship and publishing. Int J Cardiol 2009;131: Please cite this article as: Karjalainen PP, et al, Long-term clinical outcome with titanium-nitride-oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population, Int J Cardiol (2009), doi: /j.ijcard
52 Catheterization and Cardiovascular Interventions 00: (2010) Original Studies The EXTREME Registry: Titanium-Nitride-Oxide Coated Stents in Small Coronary Arteries Raúl Valdesuso, 1 MD, Pasi Karjalainen, 2 MD, Joan García, 3 MD, José Díaz, 4 MD, Javier Fernández Portales, 5 MD, Mónica Masotti, 6 MD, Francisco Picó, 7 MD, Antonio Serra, 8 MD, José Moreu Burgos, 9 MD, Luis Insa, 10 MD, Fina Mauri, 11 MD, Javier Rodriguez Collado, 12 MD, and Wail Nammas, 13 * MD Objectives: We sought to explore the immediate results of Titan2 VR stent implantation in small coronary arteries, as well as the incidence of major adverse cardiac events (MACE) at six months follow-up. Background: The safety of Titan2 VR stent has been confirmed in several studies in real-life unselected populations. Methods: We enrolled 311 consecutive patients admitted for percutaneous intervention for at least one significant (50%) de novo lesion in a native small coronary artery ( mm). All lesions were treated with Titan2 VR stent implantation. Patients were prospectively followed up for at least six months. The primary endpoint was MACE at six months follow-up [death, myocardial infarction (MI), or target vessel revascularization (TVR)]. Secondary endpoints included angiographic and clinical procedural success, in-hospital MACE, target lesion revascularization (TLR) during follow-up, and stent thrombosis. Results: The mean age was years (65.9% males). A total of 356 Titan2 VR stents were implanted in 353 lesions. Angiographic and clinical procedural success was achieved in 344 (97.5%) patients. No case of in-hospital MACE or acute stent thrombosis was reported. Clinical follow-up was completed for an average of months. Two patients (0.7%) died, and 6 (2.1%) developed MI. TLR was performed in 12 (4.2%) and TVR in 16 (5.5%) patients, all were clinically driven. Cumulative MACE occurred in 20 (6.9%) patients. One patient suffered subacute stent thrombosis, but no late stent thrombosis. Conclusions: Titan2 VR stent implantation in small coronary arteries achieves excellent immediate outcome, with a low incidence of MACE at mid-term follow-up. VC 2010 Wiley-Liss, Inc. Key words: bioactive stents; small coronary arteries; outcome 1 Cardiology Department, Hospital Universitario Virgen de la Arrixaca, Murcia, Spain 2 Cardiology Department, Satakunta Central Hospital, Pori, Finland 3 Cardiology Department, Hospital de Sant Pau, Barcelona, Spain 4 Cardiology Department, Hospital Juan Ramon Jimenez, Huelva, Spain 5 Cardiology Department, Hospital San Pedro de Alcántara, Cáceres, Spain 6 Cardiology Department, Hospital Clinic, Barcelona, Spain 7 Cardiology Department, Hospital Santa Maria del Rosell, Cartagena, Spain 8 Cardiology Department, Hospital del Mar, Barcelona, Spain 9 Cardiology Department, Hospital Virgen de la Salud, Toledo, Spain 10 Cardiology Department, Hospital Clinico, Valencia, Spain 11 Cardiology Department, Hospital Universitario Germans Trias y Pujol, Badalona, Spain 12 Cardiology Department, Hospital Clinico, Salamanca, Spain 13 Cardiology Department, Ain Shams University Hospital, Cairo, Egypt Conflict of interest: Nothing to report. *Correspondence to: Wail Nammas, Cardiology Department, Ain Shams University Hospitals, Faculty of Medicine, Ain Shams University. Abbassia, Cairo, Egypt. P.O wnammas@hotmail.com Received 21 December 2009; Revision accepted 15 January 2010 DOI /ccd Published online 00 Month 2010 in Wiley InterScience (www. interscience.wiley.com) VC 2010 Wiley-Liss, Inc.
53 2 Valdesuso et al. INTRODUCTION Percutaneous coronary stent implantation has notably improved procedural safety and promoted a better outcome of percutaneous coronary interventions (PCI) as compared with balloon angioplasty alone [1,2]. However, since the introduction of coronary stents, restenosis-the result of neointimal hyperplasia-has always been the Achilles Heel of this technique, often culminating in repeat revascularization with increased healthcare cost [3,4]. The incidence of restenosis after uncoated stents may approach 30% in several subgroups of patients, including diabetics, patients with small coronary vessels or long lesions [5,6]. The recent introduction of drug-eluting stents (DES) has revolutionized the practice of coronary angioplasty, since it has reduced the occurrence of restenosis by 50 70% [7,8]. Nevertheless, data from meta-analyses and registries have questioned the long-term safety of drug-eluting stents, raising concerns about a higher risk of late stent thrombosis, a potentially life-threatening complication [9 11]. Ultimately, the invention of bioactive stents (BAS) has been a form of natural evolution of stent technology. The safety of titanium-nitride-oxide-coated stents (Titan2 VR, Hexacath, Paris, France) has been confirmed in several studies in real-life unselected populations [12 16]. Interestingly, several randomized studies have demonstrated an even better outcome with BAS in comparison with Paclitaxel-eluting stents in the realworld setting of high-risk patients and complex (type B and C) coronary lesions [17,18], as well as in patients with acute myocardial infarction (MI) [19,20]. However, available data are limited regarding the use of BAS in patients with small coronary arteries. The purpose of this registry is to explore the immediate clinical and angiographic outcome of Titan2 VR stent implantation in small coronary vessels, as well as the incidence of major adverse cardiac events (MACE) during follow-up for at least six months. MATERIALS AND METHODS Study Design and Patient Selection EXTREME Registry (Titanium-nitride-oxide coated stents in small coronary arteries) is a prospective nonrandomized, multicenter registry with the chief aim to evaluate the use of Titan2 VR stent in small and extrasmall coronary arteries. From June 2004 through December 2005, we enrolled a total of 311 consecutive (as possible) patients with symptomatic ischemic heart disease admitted to undergo PCI. We considered patients as eligible for enrollment if they were above 18 years, had at least one significant de novo lesion Catheterization and Cardiovascular Interventions DOI /ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI). (defined as at least 50% diameter stenosis by visual estimation) in a native small coronary artery (defined by a reference diameter of mm at lesion site). Lesions with a diameter between 2.0 and 2.25 mm were included only if their length was below 13 mm (since Titan2 VR stent is available in these diameters, only in lengths of 7, 10, and 13mm). Treatment of more than one vessel was permissible, but only Titan2 VR stent was allowed, as dictated by the registry protocol. The stenting indication was determined by operator s discretion. We excluded patients with chronic renal insufficiency (serum creatinine above 3.0 mg/dl), pregnancy, bleeding risk (for example: active peptic ulcer), known hypersensitivity to aspirin or heparin, patients stented with two stents of different types, those with chronic total occlusion of the target vessel and those currently enrolled in another study. Before inclusion, an informed written consent was obtained from each patient and the study protocol was approved by the local institutional human research committee in each individual center as it conforms to the ethical guidelines of the 1964 Declaration of Helsinki, as revised in Device Used A commercially available stent (Titan2 VR, Hexacath, Paris, France), with a unique patent helicoidal design, was used in this study. It is a tubular thin-strut ( mm) balloon expandable stent made of stainlesssteel and coated with titanium-nitride-oxide which completely prevents discharge of nickel, chromium and molybdenum ions. The stent is available in lengths of 7, 10, 13, 16, 19, 22, and 28 mm for stents with diameter 2.50 and 2.75 mm. For stents with diameter 2 and 2.25 mm (Titan2 X-Small VR ), only the lengths 7, 10, and 13 mm were available. Adjunctive Pharmacological Therapy All included patients were already pretreated with aspirin (100 mg daily). Oral clopidogrel was initiated with a loading dose of 300 mg at least 6 hr before the procedure and continued thereafter in a daily dose of 75 mg for at least one month. For patients with allergy to clopidogrel, oral ticlopidine was administered in a dose of 250 mg twice daily orally, started one day before the procedure and continued thereafter for at least one month. During the procedure, intravenous heparin was given to maintain an activated clotting time between 200 and 300 sec. Use of peri-procedural glycoprotein IIb/IIIa inhibitors was left entirely to the operator s discretion. The medical treatment of coronary artery disease was optimized according to the contemporary guidelines.
54 Quantitative Coronary Analysis Coronary angiograms were obtained in multiple views after intracoronary injection of nitrates. Quantitative analysis of angiographic data before the procedure was performed in each participating center according to the standards of care, using validated edge detection techniques. A contrast filled non-tapered catheter was used for calibration. Interpolated reference vessel diameter, minimal lumen diameter, percent diameter stenosis, and lesion length were measured before the procedure as well as residual stenosis following stent implantation. Angioplasty Procedures Predilatation was left to operator s discretion. The operator decided the appropriate diameter to be implanted aiming at a stent: vessel ratio of 1.1:1 prior to stent placement (using nominal pressure). After stent deployment, post-dilatation was allowed as necessary (at operator s discretion) to ensure that residual stenosis was <20% (by visual estimation) with a TIMI grade 3 distal flow. An additional Titan2 VR stent could be deployed in case of edge dissection, incomplete lesion coverage or otherwise suboptimal result (always left to operator s discretion). The procedures conformed to the European guidelines for PCI. Follow-Up All patients were observed during hospital stay for the occurrence of the clinical end-points prespecified by the study protocol (as described below). Patients were prospectively followed up for at least six months by means of clinical visits or telephone contact by the attendant cardiologists. Follow-up coronary angiography was performed for patients developing recurrent symptoms during the follow-up period. The decision to perform further revascularization for the target lesion at follow-up coronary angiography was based on clinical justification (as described below). All patients data available from hospital records, institutional electronic database, or referring physicians, were entered into electronic case report forms in the participating centers, provided by an independent data coordinator service (Kika Medical). Titanox Coated Stent in Small Coronary Arteries 3 Study Endpoints and Definitions The primary endpoint of the study was the occurrence of MACE during follow-up for at least six months. Secondary endpoints included angiographic and clinical procedural success, in-hospital MACE, target lesion revascularization (TLR) during follow-up, and stent thrombosis. MACE were defined as a composite of cardiac death, non-fatal MI including Q wave and non-q wave MI, or target vessel revascularization (TVR). MI was diagnosed by persistent ischemic-type chest pain with a rise in the creatine kinase-mb fraction of more than three times the upper limit of normal lab reference, according to the ACC /AHA/ SCAI guidelines update for PCI [21]. Q wave MI was distinguished by the development of new abnormal Q waves, while their absence identified non-q wave MI. TLR was defined as re-intervention (surgical or percutaneous) to treat significant luminal stenosis within the stent or in the 5-mm distal or proximal segments adjacent to the stent. TVR was defined as reintervention to treat any lesion located in the index epicardial vessel. Revascularization was regarded as clinically-driven if it was motivated by anginal symptoms and/or myocardial ischemia in the target vessel territory proven by non-invasive testing. Angiographic procedural success was defined as successful implantation of the assigned study stent into the target lesion with residual stenosis <20% and a TIMI 3 flow at the conclusion of the procedure, in the absence of dissection or thrombosis. Clinical procedural success was defined as angiographic success in the absence of in-hospital MACE. Stent thrombosis was diagnosed by the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent, according to the definite category definition of the Academic Research Consortium [22]. We classified stent thrombosis into: acute (occurring within 24 hr of the index procedure), subacute (occurring after 24 hr but within 30 days), and late (occurring after 30 days). Angiographic restenosis was defined as 50% diameter stenosis (by visual estimation) within the stent or in the 5-mm distal or proximal segments adjacent to the stent, at follow-up coronary angiography. Statistical Analysis As EXTREME was an observational registry, there was no formal statistical hypothesis. No formal power calculation was performed. Continuous variables were presented as mean SD. Categorical variables were described with absolute and relative (percentage) frequencies. Analyses were performed with Eventa Software (Kika Medical) version RESULTS Baseline Clinical and Angiographic Characteristics A total of 311 patients-who received at least one Titan2 VR stent in small coronary arteries (as defined Catheterization and Cardiovascular Interventions DOI /ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).
55 4 Valdesuso et al. TABLE I. Baseline Clinical Characteristics of the Study Population Variable N ¼ 311 Age (years) Male gender 205 (65.9) Diabetes Mellitus 113 (36.3) Type 1 3 (0.96) Type (35.4) Hypertension 214 (68.8) Dislipidemia 182 (58.5) Current smoking 99 (31.8) Family history of IHD 53 (17) Acute coronary syndrome 154 (49.5) Acute MI 57 (18.3) Unstable angina 97 (31.2) Prior MI 108 (34.7) Prior PCI 56 (18%) Prior CABG 34 (11%) Three vessel disease 48 (17.5) Ejection fraction (%) Aspirin 311 (100) Clopidogrel 309 (99.4) Ticlopidine 2 (0.6) Heparin 311 (100) Glycoprotein IIb IIIa inhibitor 39 (12.5) Continuous variables are presented as mean SD, while categorical variables are presented as frequency (percentage). IHD, ischemic heart disease; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting. TABLE II. Baseline Angiographic Characteristics of the Study Population Variable N ¼ 353 Lesion type A 16 (4.5) B1 116 (32.9) B2 171 (48.4) C 50 (14.2) Thrombus 62 (17.6) Ulcerated plaque 63 (17.8) Calcification grade (51.6) (37.7) 2 38 (10.8) Eccentric lesion 269 (76.2) Bifurcation lesion 31 (8.8) Reference diameter (mm) MLD (mm) Lesion length (mm) Initial stenosis (%) Continuous variables are presented as mean SD, while categorical variables are presented as frequency (percentage). MLD, minimal lumen diameter. before) were included in the EXTREME registry. Baseline clinical characteristics of the study population are shown in Table I. Baseline angiographic characteristics are summarized in Table II. Catheterization and Cardiovascular Interventions DOI /ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI). TABLE III. Procedural Characteristics of the Study Population Variable N ¼ 353 Balloon predilatation 207 (58.6) Balloon diameter (mm) Balloon length (mm) Inflation pressure (bar) Post-balloon dissection 18 (5.1) Direct stenting 146 (41.4) Titan stent implantation 353 (100) Angiographic success 344 (97.5) Stent diameter (mm) Stent length (mm) Deployment pressure (bar) Post-stent dissection 6 (1.7) TIMI flow grade 2 1 (0.3) (99.7) Residual stenosis (%) Continuous variables are presented as mean SD, while categorical variables are presented as frequency (percentage). TIMI, Thrombolysis in myocardial infarction. TABLE IV. Follow-Up Data at Months N ¼ 289 Total MACE 20 (6.9) Death 2 (0.7) Myocardial infarction 6 (2.1) TVR 16 (5.5) TLR 12 (4.2) CABG 1 (0.34) All variables are presented as frequency (percentage). MACE, major adverse cardiac events; TVR, target vessel revascularization; TLR, target lesion revascularization; CABG, coronary artery bypass grafting. Procedural Data A total of 356 Titan2 VR stents were implanted in 353 lesions during index procedures. In 42 patients (out of 311), two small vessels were treated with Titan2 VR stents. Three vessels received two stents each (to seal edge dissection observed following deployment of the first stent). Table III summarizes procedural data. Poststent dissection occurred in six (1.7%) lesions, three of which were sealed by another stent and the other three were nonflow-limiting and were left for observation. Angiographic and clinical procedural success was achieved in 344 (97.5%) patients (no in-hospital MACE). No case of acute stent thrombosis was reported during hospital stay. Follow-Up Data Clinical follow-up for at least six months was completed in 289 (92.9%) patients, with an average followup period of 8 2 months. Of the patients who completed follow-up, 251 (86.9%) were symptom-free at the end of follow-up. Table IV demonstrates clinical
56 follow-up data at 8 2 months. Two patients (0.7%) died of a cardiac cause, and 6 (2.1%) developed nonfatal MI. TLR was performed in 12 (4.2%) and TVR in 16 (5.5%) patients, all were clinically driven. TLR included 11 (3.8%) cases of percutaneous and one case (0.34%) of surgical revascularization. Cumulative MACE at the end of follow-up occurred in 20 (6.9%) patients. One patient suffered subacute stent thrombosis, but no one suffered late stent thrombosis during follow-up, according to the perprotocol definition. DISCUSSION Current Strategy for Reduction of Restenosis Currently, the use of DES is the state-of-the-art means of reducing in-stent restenosis (ISR) in randomized clinical trials involving selected populations [7,8,23]. Several randomized controlled trials comparing bare metal stents with FDA-approved DES demonstrated significant reduction in coronary restenosis with DES, that was translated into lower TVR and TLR rates [7,8,24]. Nevertheless, after years of real-life experience with DES, the improvement of restenosis rate was not converted into reduction of the most powerful hard endpoints: death and MI. Additionally, recent worrisome data showed a significant increase of such serious events following the use of DES in predetermined clinical scenarios and/or lesion or procedural characteristics, chiefly, due to late and very late stent thrombosis [9 11,25,26]. Since the dawn of PCI, it is known that ISR is a less serious event; otherwise, it would have been impossible for PCI to be a feasible alternative to surgical revascularization. Therefore, in our search for a therapeutic option that effectively reduces ISR, we cannot accept any increase (even if minimal) in hard endpoints as a price paid to achieve such a target. Titanium-Nitride-Oxide BAS Titanium exhibits a better biocompatibility as compared with stainless steel, gold, or other surface coating materials [27]. Metallic sheaths coated with titanium nitride or titanium oxide demonstrated higher endothelial cell density values on their surfaces in comparison with those without such coatings, suggesting that the use of stents covered with these coatings may accomplish earlier complete endothelialization [28]. The safety of the titanium-nitride-oxide-coated Titan2 VR BAS has been validated in several clinical trials, both in unselected populations and in the most complex ones such as diabetic patients and those presenting with acute MI [13 16]. Yet, PCI in small coronary arteries still represents an obvious challenge to the Titanox Coated Stent in Small Coronary Arteries 5 interventional cardiologist. At present, PCI in small vessels of less than 3 mm accounts for almost 50% of all revascularization procedures and leads to a higher incidence of restenosis and adverse cardiac events [29]. BAS Outcome in Small Coronary Arteries The EXTREME registry has demonstrated an excellent immediate outcome of the Titan2 VR stent in small coronary arteries, with both angiographic and clinical success rates at 97.5%, a figure that is quite comparable with previous registries of Titan2 VR stent performed in unselected populations [13,14]. Failure to achieve angiographic (and hence clinical) success was primarily due to edge dissection, a fairly common event during small vessel PCI. Although the study population was a high-risk one (49.5% with acute coronary syndrome) with rather complex lesion characteristics (95.5% type B and C), no in-hospital MACE were encountered, and no definite stent thrombosis occurred during hospital stay. At 8 2 months follow-up, the rate of overall MACE (6.9%), as well as its individual components (death, nonfatal MI, and TVR) were again rather similar to previous registries of the stent in unselected populations [13,14]. Outcome was also comparable to the application of the stent in diabetic patients in the TIBET registry [30]; however, the population of the TIBET registry was a rather stable one with less complex lesion characteristics. Moreover, the low incidence of MACE in the current registry is comparable with many registries and randomized trials performed on DES [7,8,31,32]. It is well known that most randomized trials on DES were performed under the restraint of comprehensive lists of exclusion criteria, as for example: recent MI, visible thrombus, bifurcation lesion, etc. In contrast, the current registry was permissive to all these situations and involved a rather high-risk population, with quite complex lesion characteristics merely in small coronary arteries. Ultimately, several randomized trials showed a better outcome with Titan2 VR stent versus Paclitaxel-eluting stents in high-risk patients with complex (type B and C) lesions [17,18], and in patients presenting with acute MI [19]. Clinical Implications A cost-effectiveness analysis of DES based on the BASKET trial justified the use of DES only in highrisk groups [33]. Currently, it seems that small vessel size and ISR are the sole primary cost-effective indications of DES. Achievement of the goal of reducing TLR following PCI, even in the setting of small coronary arteries, without risking to develop the life-threatening hard endpoints of late and very late stent Catheterization and Cardiovascular Interventions DOI /ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).
57 6 Valdesuso et al. thrombosis, and at an almost similar cost, would be an appealing strategy in combating ISR. Furthermore, unlike DES which need maintenance clopidogrel therapy for at least 12 months (sometimes even for more extended periods), this therapy is required for no more than one month with the Titan2 VR stent. In the modern era of escalating healthcare costs, physicians will do both the patients and the Health System a great favor by resorting to safer and less costly means of maintaining coronary patency. In this context, BAS seem to open a new horizon for revascularization of coronary atherosclerosis. Study Limitations The EXTREME registry was not randomized, and hence it is liable for selection bias. Additionally, it bears an inherent limitation of any registry, namely, nonblinded outcome assessment. Furthermore, whether the outcome of the registry population can be extrapolated to the full spectrum of patients and lesion complexity, remains to be determined. Even longer-term follow-up is still needed before we can reach adequate conclusions on the long-term safety of this novel approach. In addition, the initial estimation of stenosis was visual-not quantitative-and it is well known that visual estimation may not correlate well with functional assessment. Finally, TLR was clinically-driven, and this might underestimate the actual incidence of restenosis, however, it would avoid unnecessary interventions in borderline lesions due to the oculostenotic reflex and undue patient anxiety. CONCLUSIONS Titan2 VR stent implantation in small coronary arteries achieves excellent immediate clinical and angiographic outcome, with a low incidence of MACE at mid-term follow-up. ACKNOWLEDGMENTS The abstract of this series was presented as a poster abstract in the Transcatheter Cardioascular Therapeutics (TCT) Scientific Sessions on Coronary Stent Design and Clinical Trial Insights, 27 October 2006, Washington DC, USA. REFERENCES 1. Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J, Moses J, Shaknovich A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S. A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331: Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P, Belardi J, Sigwart U, Colombo A, Goy JJ, van den Heuvel P, Delcan J, Morel M. A comparison of balloon-expandable stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331: Peterson ED, Cowper PA, DeLong ER, Zidar JP, Stack RS, Mark DB. Acute and long-term cost implications of coronary stenting. J Am Coll Cardiol 1999;33: Al Suwaidi J, Berger PB, Holmes DR Jr, Coronary artery stents. JAMA 2000;284: Abizaid A, Kornowski R, Mintz GS, Hong MK, Abizaid AS, Mehran R, Pichard AD, Kent KM, Satler LF, Wu H, Popma JJ, Leon MB. The influnce of diabetes mellitus on acute and late clinical outcomes following coronary stent implantation. J Am Coll Cardiol 1998;32: Kastrati A, Hall D, Schömig A. Long-term outcome after coronary stenting. Curr Control Trials Cardiovasc Med 2000;1: Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS, Jaeger JL, Kuntz RE. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349: Stone GW, Ellis SG, Cox DA, Hermiller J, O Shaughnessy C, Mann JT, Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med 2004; 350: Nordmann AJ, Briel M, Bucher HC. Mortality in randomized controlled trials comparing drug-eluting vs. bare metal stents in coronary artery disease: A meta-analysis. Eur Heart J 2006;27: Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first generation drug-eluting stents: A cause for concern. Circulation 2007;115: Lagerqvist B, James SK, Stenestrand U, Lindback J, Nilsson T, Wallentin L;SCAAR Study Group. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N Engl J Med 2007;356: Windecker S, Simon R, Lins M, Klauss V, Eberli FR, Roffi M, Pedrazzini G, Moccetti T, Wenaweser P, Togni M, Tüller D, Zbinden R, Seiler C, Mehilli J, Kastrati A, Meier B, Hess OM. Randomized comparison of a titanium-nitride oxide-coated stent with a stainless steel stent for coronary revascularization. The TINOX trial. Circulation 2005;111: Karjalainen PP, Ylitalo A, Airaksinen KE. Real world experience with the TITAN stent: A 9-month follow-up report from the Titan PORI registry. EuroInterv 2006;2: Mosseri M, Miller H, Tamari I, Plich M, Hasin Y, Brizines M, Frimerman A, Jefary J, Guetta V, Solomon M, Lotan C. The titanium-no stent: Results of a multicenter registry. EuroInterv 2006;2: Mosseri M, Tamari I, Plich M, Hasin Y, Brizines M, Frimerman A, Miller H, Jafari J, Guetta V, Solomon M, Lotan C. Short and long term outcome of the Titanium-NO stent registry. Cardiovasc Revasc Med 2005;6: Giraud-Sauveur Y. Titan 2 bio-active stent (BAS) with titanium-no. EuroInterv 2007;3: Karjalainen PP, Ylitalo A, Airaksinen JK. Titanium and nitride oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol 2006;18: Catheterization and Cardiovascular Interventions DOI /ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).
58 Titanox Coated Stent in Small Coronary Arteries Karjalainen PP, Annala AP, Ylitalo A, Vahlberg T, Airaksinen KE. Long-term clinical outcome with titanium-nitride-oxidecoated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. Int J Cardiol [Epub ahead of print] doi: /j.ijcard Karjalainen PP, Ylitalo A, Niemelä M, Kervinen K, Mäkikallio T, Pietili M, Sia J, Tuomainen P, Nyman K, Airaksinen KE. Titanium-nitride-oxide coated stents versus paclitaxel-eluting stents in acute myocardial infarction: A 12-months follow-up report from the TITAX AMI trial. EuroInterv 2008;4: Karjalainen PP, Ylitalo A, Niemela M, Kervinen K, Makikallio T, Pietila M, Sia J, Tuomainen P, Nyman K, Airaksinen KE. Two-year follow-up after percutaneous coronary intervention with titanium-nitride-oxide-coated stents versus paclitaxel-eluting stents in acute myocardial infarction. Ann Med 2009;21: Smith SC Jr, Feldman TE, Hirshfeld JW Jr, Jacobs AK, Kern MJ, King SB III, Morrison DA, O Neill WW, Schaff HV, Whitlow PL, Williams DO, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B; American College of Cardiology/American Heart Association Task Force on Practice Guidelines; ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). J Am Coll Cardiol 2006;47:e1 e Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es GA, Steg PG, Morel MA, Mauri L, Vranckx P, McFadden E, Lansky A, Hamon M, Krucoff MW, Serruys PW;Academic Research Consortium. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007;115: Babapulle MN, Joseph L, Belisle P, Brophy JM, Eisenberg MJ. A hierarchical Bayesian meta-analysis of randomized clinical trials of drug-eluting stents. Lancet 2004;364: Morice MC, Serruys PW, Sousa JE, Fajadet J, Ban Hayashi E, Perin M, Colombo A, Schuler G, Barragan P, Guagliumi G, Molnàr F, Falotico R;RAVEL Study Group. Randomized study with the sirolimus-coated bx velocity balloon-expandable stent in the treatment of patients with de novo native coronary artery lesions. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346: Spertus JA, Kettelkamp R, Vance C, Decker C, Jones PG, Rumsfeld JS, Messenger JC, Khanal S, Peterson ED, Bach RG, Krumholz HM, Cohen DJ. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement: results from the PREMIER registry. Circulation 2006;113: Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G, Airoldi F, Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N, Briguori C, Gerckens U, Grube E, Colombo A. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293: Steinemann SG. Metal implants and surface reactions. Injury 1996;27:SC16 SC Hung-I Y, Shao-Kou L, Tin-Yi T, Ray-Ching H, Wun-Hsing L, Cheng-Ho T. Comparison of endothelial cells grown on different stent materials. J Biomed Mater Res A 2006;76: Wong P, Lau KW, Lim YL, Oesterle SN. Stent placement for non-stress/benestent lesions: A critical review. Catheter Cardiovasc Interv 2000;51: Valdes M, Fernandez J, Bethencourt A, Perez E, Calvo I, Servet M, Lopez JR, Martinez A, Valdesuso R. The TIBET Registry. Clinical and angiographic events in diabetes patients treated with the TITAN stent. Am J Cardiol 2004;94:47E. 31. Ong AT, Serruys PW, Aoki J, Hoye A, van Mieghem C, Rodriguez-Granillo GA, Valgimigli M, Sonnenschein K, Regar E, van der Ent M, de Jaegere P, McFadden EP, Sianos G, van der Giessen WJ, de Feyter PJ, van Domburg RT. The unrestricted use of paclitaxel-versus sirolimus-eluting stents for coronary artery disease in an unselected population: One-year results of the Taxus-Stent Evaluated at Rotterdam Cardiology Hospital (T- SEARCH) registry. J Am Coll Cardiol 2005;45: Zahn R, Hamm CW, Schneider S, Zeymer U, Nienaber CA, Richardt G, Kelm M, Levenson B, Bonzel T, Tebbe U, Sabin G, Senges J. Incidence and predictors of target vessel revascularisation and clinical event rates of the sirolimus-eluting coronary stent (results from the prospective multicenter German Cypher Stent Registry). Am J Cardiol 2005;95: Kaiser C, Brunner-La Rocca HP, Buser PT, Bonetti PO, Osswald S, Linka A, Bernheim A, Zutter A, Zellweger M, Grize L, Pfisterer ME;BASKET Investigators. Incremental cost-effectiveness of drug-eluting stents compared with a third-generation bare-metal stent in a real-world setting: Randomised Basel Stent Kosten Effektivitäts Trial (BASKET). Lancet 2005;366: Catheterization and Cardiovascular Interventions DOI /ccd. Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).
59 Original Contribution Titanium and Nitride Oxide-Coated Stents and Paclitaxel-Eluting Stents for Coronary Revascularization in an Unselected Population Pasi P. Karjalainen, MD, Antti Ylitalo, MD, PhD, Juhani K.E. Airaksinen, MD, FESC ABSTRACT: The aim of this study was to compare clinical outcome of a stainless-steel stent coated with titanium nitride oxide (TITANOX) and a paclitaxel-eluting stent (PES) in routine clinical practice represented by two prospective registries including all patients with de novo coronary artery disease treated exclusively with a TITANOX stent (n = 201) or with a PES (n = 204) between May 2003 and November 2004 (63% of all PCI patients). The primary endpoint of the study was major adverse cardiac events (MACE) at 30 days and 12 months. The TITANOX stent patients were more frequently (p = 0.011) treated for acute myocardial infarction and had more complex B- and C-type lesions (p = 0.004). The PES patients had longer (p < 0.001) total stent length. At 30 days, the rate of MACE was 0% and 4.9% for the TITANOX stent and PES groups, respectively (p = 0.001). A significant difference in target vessel revascularization (TVR) was seen in favor of the TITANOX stent (0% vs. 2.9% for PES; p = 0.014). This was mainly driven by stent thrombosis (n = 7). At 12 months, the difference in MACE was no longer significant (10.9% vs. 13.7%; p = 0.40), but the rate of myocardial infarction was lower in the TITANOX stent group (4.5% vs. 10.3%; p = 0.025). The rate of TVR (8% vs. 6.9%; p = 0.67) was similar between the two groups. In conclusion, both the TITANOX-coated stent and PES resulted in good clinical outcome with infrequent need for repeat interventions in the real-world setting of high-risk patients and complex coronary lesions. J INVASIVE CARDIOL 2006;18: Coronary stents have reduced the risk of periprocedural complications and restenosis compared to balloon angioplasty alone. 1,2 In spite of this progress, restenosis is still a clinical problem of bare metal stents, particularly in certain high-risk patient subsets. 3,4 Widespread use of drug-eluting stents (DES) is the most effective way to reduce restenosis according to randomized, controlled trials in selected patient groups 5 9 and in everyday clinical practice Paclitaxel, a lipophilic molecule derived from the Pacific yew tree Taxus brevifolia, is capable of inhibiting cellular division, motility, activation, secretory processes and signal transduction. 13,14 A polymer-based, paclitaxel-eluting stent (PES) consistently reduced the rate of restenosis and the need for repeated revascularization procedures, as compared with bare metal stents. 6,7,15 Modifications in stent geometry, 16 strut thickness 17 and surface material 18 have been shown to influence the From Satakunta Central Hospital, Pori, Finland. The authors report no conflicts of interest regarding the content herein. Manuscript submitted March 23, 2006, provisional acceptance given May 2, 2006, manuscript accepted June 12, Address for correspondence: Pasi P. Karjalainen, MD, Satakunta Central Hospital, Sairaalatie 3, Pori, 28100, Finland. pasi.karjalainen@satshp.fi restenosis rate after bare metal stent implantation. Recently, patients with nickel allergy have been reported to be at an increased risk for restenosis after bare metal stent implantation. 19 Attempts to reduce restenosis after angioplasty with the use of various stent coatings have been largely unsuccessful. 20,21 Some studies have suggested that titanium features superior biocompatibility compared with stainless steel, gold or other surface coatings. 22,23 In vitro titanium nitride oxide shows diminished platelet adhesion and fibrinogen binding compared with stainless steel. 24 The Titan stent (Hexacath, France) is a thin-strut ( mm), balloon-expandable stent made of stainless steel and coated with titanium and nitride oxide (TITANOX) that completely prevents discharge of nickel, chromium and molybdenum. Stents coated with titanium nitride oxide reduced angiographic and ultrasonic measures of restenosis compared with stainless steel control stents in a prospective, randomized, multicenter trial (The TiNOX Trial). 25 The aim of this study was to report one-year clinical outcome of unrestricted use of TITANOX stents and PES. Methods Patients and study design. The Titan PORI Registry is a prospective, single-center registry with the main purpose of evaluating the safety and efficacy of TITANOX stent implantation for consecutive unselected patients treated in daily practice. Since May 2003, PES (Taxus ; Boston Scientific, Calway, Ireland) have been used in our hospital as the default stent for all patients selected for DES implantation. The Taxus PORI Registry is a prospective, single-center registry designed with the purpose of evaluating the safety and efficacy of PES implantation for patients treated in daily practice. Between May 2003 and November 2004, all consecutive patients with symptoms or signs of myocardial ischemia and de novo coronary lesion(s) scheduled for stent implantation were considered for these registries. A total of 405 patients fulfilled the criteria and entered this study. A total of 201 patients received only 1 or more TITANOX stents, and 204 received only 1 or more PES. The study material comprised 63% of all patients who underwent percutaneous coronary intervention (PCI) during the study period. The choice of a particular stent was at the discretion of the operator, with no exclusion criteria. The study was conducted according to the declaration of Helsinki, and written informed consent was obtained from all patients. This protocol was approved by the Ethics Committee of Satakunta Central Hospital. 462 The Journal of Invasive Cardiology
60 Table 1. Baseline clinical characteristics. Age (years) 67 ± ± Men, n (%) 143 (71) 147 (72) 0.85 Diabetes, n (%) 34 (17) 37 (18) 0.78 Current smoking, n (%) 58 (29) 53 (26) 0.31 Hypercholesterolemia, n (%) 181 (90) 167 (82) Hypertension, n (%) 133 (66) 110 (54) Medical treatment, n (%) Acetylsalicylic acid 189 (94) 190 (93) 0.72 ß-blockers 152 (76) 160 (78) 0.50 ACE inhibitor 33 (16) 36 (18) 0.74 Lipid-lowering agents 177 (88) 164 (80) Previous MI, n (%) 89 (44) 65 (32) Previous PCI, n (%) 29 (14) 49 (24) Previous CABG, n (%) 25 (12) 20 (10) 0.40 Multivessel disease, n (%) 133 (66) 137 (67) 0.94 Acute STEMI, n (%) 62 (31) 41 (20) Primary angioplasty, n (%) 22 (11) 10 (5) Rescue angioplasty, n (%) 40 (20) 31 (15) 0.21 Acute NSTEMI, n (%) 52 (26) 49 (24) 0.67 Unstable angina, n (%) 20 (10) 20 (10) 0.96 Data are mean (SD) or percentage. PES = paclitaxel-eluting stent; MI = myocardial infarction; PCI = percutaneous coronary intervention; CABG = coronary artery bypass graft surgery; STEMI = ST-elevation myocardial infarction; NSTEMI = non-st-elevation myocardial infarction. Table 2. Procedural and lesion characteristics. TITANOX Stent PES p-value (201 patients) (204 patients) TITANOX Stent PES p-value (218 lesions/ 221 stents) (244 lesions/ 247 stents) Target vessel, n (%) LAD 100 (46) 124 (51) 0.29 LCX 48 (22) 37 (15) RCA 54 (25) 68 (28) 0.45 Left main 7 (3) 7 (3) 0.83 Bypass graft (venous) 9 (4) 8 (3) 0.63 Lesion type, n (%) A 26 (12) 54 (22) B1/ B2 137 (63) 171 (70) 0.10 C 55 (25) 19 (8) < Thrombus present, n (%) 35 (16) 34 (14) 0.63 Diameter of reference vessel (mm) 2.95 ± ± Lesion length (mm) 13.1 ± ± Stent diameter (range, mm) 2.98 (2 3.5) ± ( ) ± Stent length used (range,mm) 15.6 (7-28) ± (8-32) ± 6.7 < Total stent length per lesion (mm) 16.0 ± ± 6.8 < Direct stenting, n (%) 48 (22) 46 (19) 0.40 GP IIb/IIIa inhibitor, n (%) 54 (27) 49 (24) 0.38 Clopidogrel prescription (months) 7.7 ± ± Data are mean (SD) or percentage. GP = glycoprotein; LAD = left anterior descending coronary artery; LCX = left circumflex coronary artery; RCA = right coronary artery. TITANOX Stent Compared to PES Coronary stent procedure. All patients were pretreated with aspirin (100 mg daily) and received intravenous enoxaparin (1 mg/kg) during the procedure. Oral clopidogrel was administered as a loading dose of 300 mg before or immediately after the procedure. Patients treated with PES were prescribed clopidogrel (75 mg/day) for a minimum of 6 months, based on data from randomized, controlled trials. 6 For patients treated with a TITANOX stent, clopidogrel was prescribed for a minimum of 3 months. Lesions were treated according to current standard interventional techniques, with the final strategy (direct stenting, post-dilatation, periprocedural glycoprotein IIb/IIIa inhibitor, intravascular ultrasound) left entirely to the operator s discretion. Angiographic success was defined as a residual stenosis < 30 % by visual analysis in the presence of Thrombolysis In Myocardial Infarction (TIMI) flow grade 3. TITANOX stents were available in lengths of 7, 10, 13, 16, 19, 22 and 28 mm, and in diameters of 2, 2.25, 2.50, 2.75, 3.0 and 3.5 mm. PES were available in lengths of 8, 12, 16, 20, 24, 28 and 32 mm, and in diameters of 2.25, 2.50, 2.75, 3.0 and 3.5 mm. Endpoint definitions and clinical follow up. The primary endpoint was major adverse cardiac events (MACE), defined as the occurrence of any of the following within 12 months after the index procedure: death from cardiac causes, Q-wave or non-q-wave myocardial infarction, or revascularization of the target vessel (emergency or elective coronary artery bypass grafting or repeated coronary angioplasty). Q-wave myocardial infarction was defined as either (1) the presence of chest pain or other acute symptoms consistent with myocardial ischemia and new pathologic Q-waves in 2 continuous electrocardiographic leads, or (2) elevated cardiac enzyme levels > 2 times the upper limit of normal associated with any elevation above the upper limit of normal in creatine kinase-mb levels in the presence of new pathologic Q-waves. Non-Q-wave myocardial infarction was defined as an elevated creatine kinase > 2 times the upper limit of normal associated with any elevation above the upper limit of normal in creatine kinase-mb levels. Target lesion revascularization (TLR) was defined as a repeat intervention to Vol. 18, No. 10, October
61 KARJALAINEN, et al. Probability of Event-Free Survival 1.0 p = PES TITANOX Stent Probability of Event-Free Survival 1.0 p = PES TITANOX Stent Figure 1. Kaplan-Meier Survival Curves for target lesion revascularization (TLR). Figure 2. Kaplan-Meier Survival Curves for major adverse cardiac events (MACE). treat a stenosis within the stent or in the segments 5 mm distal or proximal to the stent. Target vessel revascularization (TVR) was defined as a reintervention driven by any lesion located in the stented vessel. Stent thrombosis was diagnosed in the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent, or in autopsy. All MACE were reviewed by two cardiologists (P.K, A.Y). All patients underwent clinical follow up. Adverse events were monitored at hospital discharge and by office visits or telephone interviews by the cardiologist at 1, 6 and 12 months. In addition, all data available from hospital records, the institutional electronic clinical database and the referring physicians were checked at the end of the follow-up period (February 2006) and entered into the computer database. In both groups, follow-up coronary angiography was clinically driven by symptoms or signs suggestive of myocardial ischemia. Indication for repeat revascularization was a significant luminal stenosis (> 50% diameter stenosis) in the presence of anginal symptoms and/or proven myocardial ischemia in the target vessel territory. Statistical analysis. Continuous variables are presented as mean (SD) and were compared by Student s unpaired t-test. Categorical variables are presented as counts and percentages and were compared by the chi square or Fisher s exact test. The associations between variables were evaluated by univariate technique (Spearman s correlation coefficient). After the univariate analyses (p < 0.1), a logistic multivariable regression analysis was performed to identify independent predictors for MACE and stent thrombosis. The regression analysis was made for the whole population and separately in both registries. A two-sided Table 3. Clinical events during follow up. TITANOX Stent PES p-value (201 patients) (204 patients) 0 1 Month Death, n (%) 0 (0) 3 (1.5) 0.09 Death from cardiac causes, n (%) 0 (0) 3 (1.5) 0.09 Myocardial infarction, n (%) 0 (0) 8 (3.9) TVR, n (%) 0 (0) 6 (2.9) TLR, n (%) 0 (0) 5 (2.5) TVR (non-tlr), n (%) 0 (0) 1 (0.5) 0.32 MACE, n (%) 0 (0) 10 (4.9) Stent thrombosis, n (%) 0 (0) 7 (3.4) Months Death, n (%) 5 (2.5) 8 (3.9) 0.41 Death from cardiac causes, n (%) 1 (0.5) 5 (2.5) Myocardial infarction, n (%) 9 (4.5) a 21 (10.3) b TVR, n (%) 16 (8.0) 14 (6.9) 0.67 TLR, n (%) 10 (5.0) 10 (4.9) 0.97 TVR (non-tlr), n (%) 6 (3.0) 4 (2.0) 0.51 MACE, n (%) 22 (10.9) 28 (13.7) 0.40 Stent thrombosis, n (%) 0 (0) 7 (3.4) TLR = target lesion revascularization; TVR = target vessel revascularization; MACE = major adverse cardiac events. a = 9 of 9 underwent control angiography; b = 16 of 21 underwent control angiography. p-value < 0.05 was required for statistical significance. Target lesion revascularization (TLR) and MACE were analyzed by means of Kaplan-Meier survival curves. All data were analyzed with the use of SPSS software, version Results Baseline and procedural characteristics. Between May 2003 and November 2004, 405 patients (462 lesions/468 stents) were enrolled; 201 patients (218 lesions/21 stents) were 464 The Journal of Invasive Cardiology
62 TITANOX Stent Compared to PES Table 4. Characteristics of individual cases of PES stent thrombosis. Patient Age, Sex Indication Lesion Type Target Vessel Nominal Stent Total Stent GP IIb/IIIa Number for PCI Diameter (mm) Length (mm) Inhibitor < 30 Days 1 60, Male STEMI A LCX , Male UAP B1 SVG , Male STEMI B2 RCA , Male STEMI B2 LAD , Male STEMI B1 RCA , Female STEMI A LAD , Male STEMI B2 LAD LAST 1 54, Male STEMI C LAD , Male UAP B1 RCA , Male NSTEMI B1 LAD , Male STEMI B1 LAD , Male UAP B1 LAD , Male NSTEMI A RCA LAST = late angiographic stent thrombosis; PCI = percutaneous coronary intervention; NSTEMI = non-st-elevation myocardial infarction; STEMI = ST-elevation myocardial infarction; UAP = unstable angina pectoris; LCX = left circumflex coronary artery; SVG = saphenous vein graft; RCA = right coronary artery; LAD = left anterior descending coronary artery. treated with TITANOX coated stent(s), and 204 patients (244 lesions/247 stents) with PES. Table 1 shows the baseline clinical characteristics of the study population. The procedural characteristics are shown in Table 2. The TITANOX stent patients (p = 0.011) had acute myocardial infarction more often as their presenting symptom and more (p = 0.004) complex B- and C- type lesions treated. The total stent length was longer (p < 0.001) in PES patients. The other deployment and implantation variables were similar in the two groups. One- and twelve-month follow up. MACE during follow up are listed in Table 3. Complete follow up at 12 months was achieved in all 405 patients. At 30 days, the rate of MACE was 0% and 4.9% for the TITANOX stent and PES groups, respectively (p = 0.001). A significant difference in TVR was also seen in favor of the TITANOX stent patients (0% vs. 2.9%; p = 0.014). This was mainly driven by stent thrombosis (n = 7). At 12 months, the rate of myocardial infarction was higher in the PES group (p = 0.025), but the TLR rate was similar in both groups (Figure 1). The rate of clinical restenosis was 5% for TITANOX and 2.5% for PES (p = 0.18). At 1 year, 2.5% of patients in the TITANOX stent group and 3.9% in the PES group had died (p = 0.41). Event-free survival was 89.1% in the TITANOX stent group, as compared with 86.3% in the PES group (Figure 2). Clinically-driven control angiography was performed in 20% of the patients in the TITANOX stent group and 19% of the patients in the PES group during the 12- month follow-up period. Late follow up. At the end of follow-up period (February 2006), the mean follow up based on hospital records was 17 ± 4 months (median 20) for the TITANOX stent patients, and 20 ± 6 months (median 25) for the PES patients. The main finding in the late follow-up data was that there were 6 cases of late (after 1 year) stent thrombosis documented angiographically, and all of them were in the PES group. Characteristics of individual cases of PES stent thrombosis are shown in Table 4. In addition, there were 4 myocardial infarctions, 2 noncardiac deaths and 1 cardiovascular death in the PES group, and 1 myocardial infarction and 1 noncardiac death in the TITANOX stent group. Predictors of stent thrombosis and MACE. In the PES group, the patients with stent thrombosis had myocardial infarction more often as their presenting symptom before the index procedure (11% vs. 3%; p = 0.02), but there were no other significant predictors of stent thrombosis. MACE at 12 months was predicted by older age (70 vs. 63 years; p = 0.001), previous PCI (p = 0.002), previous CABG (p = 0.006) and multivessel disease (p = 0.020). Multivariate analysis showed that patient age (p = 0.014,) and previous PCI (p = 0.012) were the only independent predictors of MACE. In the TITANOX group, we found no significant predictors of MACE. When both registries were taken together, multivariate analysis revealed that total stent length (p = 0.042) was the only independent predictor of subacute, late and cumulative stent thrombosis. Discussion To our knowledge this is the first prospective comparison of titanium nitride oxide-coated stent with paclitaxel-eluting stent in routine clinical practice. The major finding of this study was that the unrestricted use of TITANOX stents and PES in de novo lesions leads to favorable and comparable outcomes after clinical decision making, even in high-risk patients with complex coronary lesions. Secondly, although the overall risk of Vol. 18, No. 10, October
63 KARJALAINEN, et al. Table 4 (cont.). Characteristics of individual cases of PES stent thrombosis. Patient Number Time to Notes Clinical Angiographic Finding Clinical Outcome Number of Stents Thrombosis Presentation and Therapy at Discharge < 30 Days days 0 NSTEMI New AMI after discharge, Dead Thrombus within stent, PCI, Cardiac death days 0 STEMI New AMI, Alive Thrombus within stent, PCI days 0 NSTEMI AMI, Cardiac death, Dead Autopsy: Totally occluded vessel days 0 STEMI New AMI after discharge, Alive Thrombus within stent, PCI days 0 STEMI New AMI after discharge, Alive Thrombus within stent, PCI day 0 STEMI ST-elevation in ECG, Alive Totally occluded vessel, PCI days 0 STEMI AMI, Totally occluded vessel, Alive Thrombus within stent, PCI LAST months Clopidogrel stopped STEMI ST- elevation in ECG, Alive 1 month prior a Thrombolysis, Thrombus within stent, PCI months Clopidogrel stopped STEMI ST- elevation in ECG, Alive 3 months prior a Totally occluded vessel, PCI months Clopidogrel stopped STEMI ST- elevation in ECG, Alive 4 months prior a Thrombus within stent, PCI months Clopidogrel stopped STEMI ST- elevation in ECG, Alive 5 months prior a Thrombus within stent, PCI months Clopidogrel stopped STEMI ST- elevation in ECG, Alive 11 months prior a Thrombus within stent, PCI months Clopidogrel stopped STEMI ST-elevation in ECG, Alive 13 months prior a Thrombus within stent, PCI LAST = late angiographic stent thrombosis; NSTEMI = non ST-elevation myocardial infarction; STEMI = ST-elevation myocardial infarction; AMI = acute myocardial infarction; PCI = percutaneous coronary intervention; ECG = electrocardiogram; a = acetylsalicylic acid monotherapy. stent thrombosis was low, it was concentrated in the use of PES in the setting of acute myocardial infarction. Currently, the use of DES is considered to be the most effective tool to prevent restenosis. 5 9 There is no evidence that DES could influence mortality or prevent myocardial infarction after stent implantation. PES have been shown to reduce the risk of restenosis in a broad range of lesions and patients undergoing PCI. 6,7 In the present study, the rates of clinical restenosis were low for both stent groups, substantiating the results of previous DES studies. 5 7 The three principal determinants of restenosis after coronary stent implantation are diabetes, vessel size and lesion length. 3 7 In the present 466 The Journal of Invasive Cardiology
64 TITANOX Stent Compared to PES study, there was no difference in the vessel size or prevalence of diabetes between the TITANOX stent- and PEStreated patients (Tables 1 and 2). The total stent length was, however, significantly longer in the PES group, although the actual stenosis length was comparable between the two groups. Clinically, the most alarming and unexpected finding was the high rate of stent thrombosis in the PES group. The overall rate of stent thrombosis in the PES group was higher in the present study than in previous DES studies The higher rate may have been due to the inclusion of patients with more complex conditions and lesions and a higher prevalence of acute coronary syndromes, since acute myocardial infarction and stent length were the significant predictors of stent thrombosis. In everyday clinical practice, late stent thrombosis may be an underestimated problem for DES, and the operators may not become aware of all late complications. Secondly, our findings underscore the importance of long-term follow up, particularly in the DES studies. The mechanisms of late stent thrombosis are unknown, but may be related to malapposition, inadequate endothelial coverage of DES, thrombogenic surface, 31 polymer coatings 32 and drugs in high doses. 33 In the present study all cases of late stent thrombosis occurred quite shortly (range 1 13 months) after clopidogrel withdrawal, stressing the importance of adequate long-term antiplatelet therapy after PES implantation. 28 Earlier studies 28,31,34 have shown that longer stented segments may predispose patients to stent thrombosis after DES implantation. In our patient cohort, stent length was a significant predictor only when both registries were taken together. The rate of restenosis was acceptable and there were no cases of stent thrombosis in the TITANOX group. Our current practice is to try to cover the entire plaque area with the PES, compared with a spotlike approach with bare metal stents in similar lesions. This difference in approach may reduce the risk of restenosis and thrombotic events in the TITANOX group. 28,31,35 Stent coating may also contribute to the findings, since an in vitro study has suggested that titanium nitride oxide reduces platelet adhesion and fibrinogen binding compared with stainless steel. 24 Similarly, a recent study compared the behavior of endothelial cells cultured on different stent materials. Metallic sheaths coated with titanium nitride (TiN) or titanium oxide (TiO2) exhibited higher cell density values on their surface compared to those without coating, supporting the view that deployment of stents coated with TiN or TiO2 may achieve earlier complete endothelial coverage. 36 Study strengths and limitations. The strength of our single-center registry is the fact that Satakunta Central Hospital is the only center with coronary angiography capacity in the referral area. In this rural area, the population is stationary, enabling complete and sufficiently long follow up of an all-inclusive, unrestricted PCI population reflecting daily clinical practice. One of the limitations of our study is the limited size of the patient groups for subgroup analysis. This study also carries the general problems of registry-based observational studies with nonblinded outcome assessment. The fact that this is a singlecenter, low-patient-number registry may also give rise to unrecognized selection and performance bias. Angiographic control was performed in a minority of patients, and we may have underestimated the incidence of angiographic restenosis and silent stent thrombosis. However, there is no evidence that they were more frequent in either of the groups because the clinical outcomes were similar. On the other hand, by relying on clinical follow up only, we avoided the chance of unnecessary target lesion revascularization procedures due to the oculostenotic reflex or the patient s unjustified anxiety. In addition to the characteristics listed in the Tables, the patients in the registries may have other unrecognized differences, e.g., we observed a less frequent use of PES in the setting of acute myocardial infarction during the latter part of the study period, and it is conceivable that patients at the highest risk of restenosis were more likely to be treated with PES. Conclusions In conclusion, both TITANOX coated stent and PES resulted in good clinical outcomes with infrequent need for repeat interventions in the real-world setting of high-risk patients and complex coronary lesions. Secondly, although the overall risk of stent thrombosis was low, it was concentrated in the use of PES in the setting of acute myocardial infarction. Further studies are warranted to randomly compare the TITANOX stent (to other passive and active coated stents) as an alternative to current DES, particularly in patients with acute myocardial infarction. References 1. Serruys PW, de Jaegere P, Kiemeneij F, et al. A comparison of balloon-expandablestent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331: Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronarystent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331: Kastrati A, Schomig A, Elezi S, et al. Predictive factors of restenosis after coronary stent placement. J Am Coll Cardiol 1997;30: Elezi S, Kastrati A, Pache J, et al. Diabetes mellitus and the clinical and angiographic outcome after coronary stent placement. J Am Coll Cardiol 1998;32: Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349: Colombo A, Drzewiecki J, Banning A, et al. Randomized study to assess the effectiveness of slow- and moderate-release polymer-based paclitaxel-eluting stents for coronary artery lesions. Circulation 2003;108: Stone GW, Ellis SG, Cox DA, et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med 2004;350: Babapulle MN, Joseph L, Belisle P, et al. A hierarchical bayesian meta-analysis of randomized clinical trials of drug-eluting stents. Lancet 2004;364: Pache J, Dibra A, Mehilli J, et al. Drug-eluting stents compared with thin-strut bare stents for the reduction of restenosis: A prospective, randomized trial. Eur Heart J 2005;26: Lemos PA, Serruys PW, van Domburg RT, et al. Unrestricted utilization of sirolimus-eluting stents compared with conventional bare stent implantation in the real world : The Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) registry. Circulation 2004;109: Ong AT, Serruys PW, Aoki J, et al. The unrestricted use of paclitaxel- versus sirolimus-eluting stents for coronary artery disease in an unselected population: Oneyear results of the Taxus-Stent Evaluated At Rotterdam Cardiology Hospital (T- SEARCH) registry. J Am Coll Cardiol 2005;45: Goy JJ, Stauffer JC, Siegenthaler M, et al. A prospective randomized comparison between paclitaxel and sirolimus stents in the real world of interventional cardiology: The TAXi trial. J Am Coll Cardiol 2005;45: Belotti D, Vergani V, Drudis T, et al. The microtubule-affecting drug paclitaxel has antiangiogenic activity. Clin Cancer Res 1996;2: Vol. 18, No. 10, October
65 KARJALAINEN, et al. 14. Giannakakou P, Robey R, Fojo T, et al. Low concentrations of paclitaxel induce cell type-dependent p53, p21 and G1/G2 arrest instead of mitotic arrest: Molecular determinants of paclitaxel-induced cytotoxicity. Oncogene 2001;20: Grube E, Silber S, Hauptmann KE, et al. TAXUS I: Six- and twelve- month results from a randomized, double-blind trial on a slow-release paclitaxel-eluting stent for de novo coronary lesions. Circulation 2003;107: Garasic JM, Edelman ER, Squire JC, et al. Stent and artery geometry determine intimal thickening independent of arterial injury. Circulation 2000;101: Kastrati A, Mehilli J, Dirschinger J, et al. Intracoronary stenting and angiographic results: Strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation 2001;103: Babapulle MN, Eisenberg MJ. Coated stents for the prevention of restenosis: Part II. Circulation 2002;106: Koster R, Vieluf D, Kiehn M, et al. Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet 2000;356: Vom Dahl J, Haager PK, Grube E, et al. Effects of gold coating of coronary stents on neointimal proliferation following stent implantation. Am J Cardiol 2002;89: Park SJ, Lee CW, Hong MK, et al. Comparison of gold-coated NIR stents with uncoated NIR stents in patients with coronary artery disease. Am J Cardiol 2002;89: Steinemann SG. Titanium: The material of choice? Periodontol ;17: Steinemann SG. Metal implants and surface reactions. Injury 1996;27(Suppl 3):SC16 SC Windecker S, Mayer I, De Pasquale G, et al. Stent coating with titanium-nitride oxide for reduction of neointimal hyperplasia. Circulation 2001;104: Windecker S, Simon R, Lins M, et al. Randomized comparison of a titanium-nitride oxide-coated stent with a stainless steel stent for coronary revascularization. The TINOX trial. Circulation 2005;111: Buehl A, Zoefel P. SPSS 11: Introduction in Modern Data Analysis. 8th ed. Munich, Germany: Addison-Wesley, Hofma SH, Ong AT, Aoki J, et al. One year clinical follow up of paclitaxel-eluting stents for acute myocardial infarction compared with sirolimus-eluting stents. Heart 2005;91: Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293: Ong AT, Hoye A, Aoki J, et al. Thirty-day incidence and six-month clinical outcome of thrombotic stent occlusion after bare-metal, sirolimus, or paclitaxel stent implantation. J Am Coll Cardiol 2005;45: Ong AT, McFadden EP, Regar E, et al. Late angiographic stent thrombosis (LAST) events with drug-eluting stents. J Am Coll Cardiol 2005;45: McFadden EP, Stabile E, Regar E, et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004;364:1519 ß Virmani R, Guagliumi G, Farb A, et al. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimus-eluting stent: Should we be cautious? Circulation 2004;109: Walpoth BH, Pavlicek M, Celik B, et al. Prevention of neointimal proliferation by immunosupression in synthetic vascular grafts. Eur J Cardiothorac Surg 2001;19: Cutlip DE, Baim DS, Ho KK, et al. Stent thrombosis in the modern era: A pooled analysis of multicenter coronary stent clinical trials. Circulation 2001;103: Dietz U, Holz N, Dauer C, et al. Shortening the stent length reduces restenosis with bare metal stents: Matched pair comparison of short stenting and conventional stenting. Heart 2006;92: Hung-I Y, Shao-Kou L, Tin-Yi T, et al. Comparison of endothelial cells grown on different stent materials. J Biomed Mater Res A 2006;76: The Journal of Invasive Cardiology
66 Volume 2 - Number 2 - August 2006 Reprint Real world experience with the TITAN stent: a 9-month follow-up report from The Titan PORI Registry Pasi P Karjalainen, Antti S Ylitalo, K.E. Juhani Airaksinen
67 Clinical research Real world experience with the TITAN stent: a 9-month follow-up report from The Titan PORI Registry Pasi P Karjalainen 1 *, MD; Antti S Ylitalo 1, MD, PhD; K.E. Juhani Airaksinen 2, MD, FESC 1. Satakunta Central Hospital, Division of Cardiology, Pori, Finland; 2. Turku University Hospital, Internal Medicine, Turku, Finland. The authors have no conflict of interest to declare. KEYWORDS Stent, titanium, angioplasty, restenosis. Abstract Aims: The aim of the Titan PORI Registry was to evaluate the safety and efficacy of a stainless steel stent coated with titanium nitride oxide (Titan, Hexacath, France) in routine clinical practice. Methods and results: We report a prospective single-centre experience in treating patients with the Titan stent. All consecutive patients receiving Titan stent(s) were enrolled. The choice of a stent was at the discretion of the operator with no exclusion criteria. The primary end point of the registry was Major Adverse Cardiac Events (MACE) at 6 and 9 months. A total of 210 lesions were treated in 193 enrolled patients (mean age 67±10; men 71%; diabetes 17%). Lesions were of type B in 64% and type C in 23%. The indications for PCI were unstable angina or non-q-wave MI in 36% and acute STEMI in 30% of the patients. Mean reference diameter was 2.9±0.3 mm and mean lesion length 12.9±3.0 mm. Mean stent size was 2.98 mm (range mm) and length 15.5 mm (range 7-28 mm). Stent delivery was successful in all cases (23% direct stenting). Complete follow-up of all 193 patients was obtained up to 9 months. There were no in-hospital or 30-day MACE observed. At 270 days, the MACE rate was 10.4% (MI 4.1%, cardiac death 0%, TVR 8.3%). There were no cases with stent thrombosis. Conclusion: These medium term data confirm good safety profile of Titan stent even in high risk patients and complex coronary lesions in routine clinical use. * Corresponding author: Satakunta Central Hospital, Sairaalatie 3, 28100, Pori, Finland. pasi.karjalainen@satshp.fi Europa Edition All rights reserved. EuroInterv.2006;2:
68 The Titan PORI Registry Introduction The implantation of bare metal coronary stents reduces the risk of periprocedural complications and restenosis compared to plain balloon angioplasty 1,2. Despite the use of coronary stents, the frequency of restenosis may be up to 30 percent in several subgroups of patients, including diabetics and patients with small coronary vessels or long lesions 3,4. Modifications in stent geometry 5, strut thickness 6, and surface material 7 have been shown to influence the restenosis rate after bare metal stent implantation. Recently, patients with nickel allergy have been reported to be at an increased risk for restenosis after bare metal stent implantation 8. Attempts to reduce restenosis after angioplasty with the use of various stent coatings have been largely unsuccessful 9,10. Titanium features superior biocompatibility compared with stainless steel, gold, or other surface coatings 11,12. In vitro examination titanium nitride oxide showed diminished platelet adhesion and fibrinogen binding compared with stainless steel 13. Titan stent (Hexacath, France) is a thin strut balloon expandable stent made of stainless steel and coated with titanium nitride oxide. Stent coating with titanium nitride oxide reduced angiographic and ultrasonic measures of restenosis compared with stainless steel control stents in a prospective, randomised, multicentre trial (The TiNOX Trial) 14. However, there is only limited data available on unrestricted use of Titan stents in unselected populations 15,16. The aim of this study was to evaluate the safety and efficacy of a stainless steel stent coated with titanium nitride oxide (Titan ) in unrestricted routine clinical practice. Methods Study design and patient population The Titan PORI Registry is a prospective single centre registry with the main purpose of evaluating the safety and efficacy of Titan stent implantation for consecutive unselected patients treated in daily practice. Between June, 2003 and November, 2004, all consecutive patients with symptoms or signs of myocardial ischaemia and de novo coronary lesion(s) scheduled for stent implantation were considered for study enrolment. The choice of a stent was at the discretion of the operator with no exclusion criteria. During the study period a total of 193 patients were treated with the Titan stent(s) comprising 32% of all patients with de novo disease who underwent percutaneous coronary intervention (PCI) in our centre. Stents A commercially available stainless steel stent with the unique helicoidal design was used in this study. Titan stent is a thin strut ( mm) balloon expandable stent made of stainless steel and coated with titanium nitride oxide which completely prevents discharge of nickel, chromium and molybdenum. Coating of stainless steel stents is performed by plasma enhanced vapour deposition of titanium in a pre-specified gas mixture of nitrogen and oxygen in a vacuum chamber. Stents were available in lengths of 7, 10, 13, 16, 19, 22 and 28 mm and in diameters of 2, 2.25, 2.50, 2.75, 3.0 and 3.5 mm. Coronary-stent procedure All patients were pre-treated with aspirin (100 mg daily) and received intravenous enoxaparine (1 mg/kg) during the procedure. Oral clopidogrel was administered as a loading dose of 300 mg before or immediately after the procedure and clopidogrel was continued at a daily dose of 75 mg for at least 3 months. Lesions were treated according to current standard interventional techniques, with the final strategy (including direct stenting, post-dilatation, periprocedural glycoprotein IIb/IIIa inhibitor, and the use of intravascular ultrasound) left entirely up to the operator s discretion. Angiographic success was defined as a residual stenosis < 30% by visual analysis in the presence of Thrombolysis In Myocardial Infarction (TIMI) flow grade 3. The medical treatment of coronary artery disease was optimised according to the contemporary guidelines. End point definitions and clinical follow-up The primary end point of the Titan PORI registry was major adverse cardiac events (MACE), defined as the occurrence of any of the following within 270 days after the index procedure: death from cardiac causes, Q-wave or non-q-wave myocardial infarction, or revascularisation of the target vessel (emergency or elective coronaryartery bypass grafting or repeated coronary angioplasty). Q-wave myocardial infarction was defined as either (1) the presence of chest pain or other acute symptoms consistent with myocardial ischaemia and new pathologic Q waves in > 2 continuous electrocardiographic leads, or (2) elevated cardiac enzyme levels > 2 times the upper limit of normal associated with any elevation above the upper limit of normal in creatine kinase-mb levels in the presence of new pathologic Q waves. Non-Q-wave myocardial infarction was defined as an elevated creatine kinase > 2 times the upper limit of normal associated with any elevation above the upper limit of normal in creatine kinase-mb levels. Target lesion revascularisation (TLR) was defined as a repeat intervention to treat a stenosis within the stent or in the segments 5mm distal or proximal to the stent. Target vessel revascularisation (TVR) was defined as a reintervention driven by any lesion located in the stented vessel. Stent thrombosis was diagnosed in the presence of an acute coronary syndrome with angiographic evidence of either vessel occlusion or thrombus within the study stent. All MACE were reviewed by two of the cardiologists. All patients underwent clinical follow-up. Adverse events were monitored at hospital discharge and by office visits or telephone interviews by the cardiologist at 6 months and after a follow-up of at least 9 months. All data available from hospital records, the institutional electronic clinical database, or the referring physicians were entered into a computer database. Follow-up coronary angiography was clinically driven by symptoms or signs suggestive of myocardial ischaemia. Indication for repeat revascularisation was a significant luminal stenosis (> 50% diameter stenosis) in the presence of anginal symptoms and/or proven myocardial ischaemia in the target vessel territory. Statistical analysis Continuous variables are presented as mean±standard deviation and categorical variables as counts and percentages. The event free
69 Clinical research survival curve was calculated according to the Kaplan-Meier method. Logistic regression analysis was performed to identify independent predictors of MACE. All data were analysed with the use of SPSS version Results Baseline and procedural characteristics A total of 193 patients who received > 1 Titan stent(s) during the index PCI were included in the Titan PORI Registry. The baseline clinical characteristics of the population are shown in Table 1. Most of the patients (66%) were treated for acute ST-elevation myocardial infarction, non-q-wave myocardial infarction or unstable angina. Diabetes was present in 17% of the patients. The angiographic and procedural characteristics are summarised in Table 2. A total of 212 stents were implanted in 210 lesions in 193 patients. Lesions were of type B in 64% and type C in 23%, and 25% were bifurcation lesions and 4% chronic total occlusions. Direct stenting was performed in 48 lesions (23%). A glycoprotein IIb/IIIa inhibitor was used in 52 patients (27%). Procedural success was reached in all cases. Clinical outcome Complete follow-up was obtained in all 193 (100%) patients. The mean duration of the clopidogrel treatment was 7.7±3.3 months. The coronary angiography was done in 37 (19%) patients. Clinical events during 6 and 9 months follow-up are shown in Table 3. Table 1. Baseline clinical characteristics Patients (n=193) Mean age (range, years) 67(39-94)±10 Male sex (%) 71 Diabetes (%) 17 Hypercholesterolaemia (%) 89 Hypertension (%) 66 Current smoking (%) 30 Medical treatment (%) Acetylsalicylic acid 94 ß-Blockers 76 ACE inhibitor 16 Lipid-lowering agents 88 Previous MI (%) 46 Previous angioplasty (%) 15 Previous CABG (%) 13 Multivessel disease (%) 66 Acute STEMI (%) 30 Primary angioplasty 11 Rescue angioplasty 19 Acute NSTEMI (%) 27 Unstable angina (%) 9 MI: myocardial infarction; CABG: coronary artery bypass graft surgery; STEMI: ST-elevation myocardial infarction; NSTEMI: non ST-elevation myocardial infarction. Table 2. Procedural and lesion characteristics Lesions (n=210) Treated vessel LAD (%) 45.6 LCX (%) 22.8 RCA (%) 25.4 LM (%) 2.1 SVG (%) 4.1 Lesion type Type A (%) 12.4 Type B (%) 64.2 Type C (%) 23.4 Reference vessel diameter (mm) 2.93±0.3 Lesion length (mm) 12.93±3.0 Stent diameter (range, mm) 2.98 (2-3.5)±0.3 Stent length (range, mm) (7-28)±3.4 Bifurcation stenting (%) 25 Direct stenting (%) 23 Multivessel treatment (%) 8 Glycoprotein IIb/IIIa inhibitor (%) 27 Clopidogrel prescription (months) 7.7±3.3 LAD: left anterior descending coronary artery, LCX: left circumflex coronary artery, RCA: right coronary artery, LM: left main coronary artery, SVG: saphenous vein graft. Table 3. Major adverse cardiac events during 6 and 9 months of follow-up 6 months 9 months (n=193) (n=193) Death, n (%) 2 (1) 4 (2.1) Cardiac death, n (%) 0 0 Nonfatal myocardial infarction, n (%) 4 (2.1) 8 (4.1) TVR, n (%) 12 (6.2) 16 (8.3) TLR, n (%) 7 (3.6) 10 (5.2) TVR (non-tlr), n (%) 5 (2.6) 6 (3.1) Stent thrombosis, n (%) 0 0 MACE, n (%) 13 (6.7) 20 (10.4) TVR: target vessel revascularisation, TLR: target lesion revascularisation, MACE: major adverse cardiac events. There were no in-hospital MACE observed. At 270 days follow-up, there were no cardiac deaths. Four patients died during the follow-up: two patients from malignant tumours, one patient from progressive renal failure and one patient from an infection after an orthopaedic operation. Seven patients had new non-q-wave myocardial infarction and one patient had Q-wave myocardial infarction. The incidence of Target Vessel Revascularisation (TVR) and Target Lesion Revascularisation (TLR) were 8.3% and 5.2%, respectively. The overall MACE rate at 9 months was 10.4%. The event free survival curve is illustrated in Figure 1. Multivariate analysis revealed no independent predictors for MACE. There were no cases of subacute or late stent thrombosis
70 The Titan PORI Registry % % Time (months) Figure 1. Event free survival at 9 months. Discussion Currently, drug-eluting stents (DES) are considered to be the most effective tool to prevent restenosis. However, there is no evidence that DES could influence mortality or prevent myocardial infarction after stent implantation. A pressing question concerns the potential risk of stent thrombosis in clinical practice 18,19. In this prospective, single-centre study, unrestricted use of Titan stent was safe and effective even in high risk patients with complex coronary lesions. Of note, no cases of stent thrombosis were observed. Our results are in agreement with earlier small registry studies on Titan stents 15,16 extending their results to a more complex patient population. The TIBET registry demonstrated an acceptable rate of angiographic restenosis in diabetic patients treated with Titan stent compared to bare metal stent 15. Similarly, the Titan Israeli Registry reported a good safety profile and a low clinical TLR rate 16. Recent registries on bare metal stents have also demonstrated comparable low rates of MACE and TLR 20,21. In both of these registries, however, the included patients had stable angina and the stented vessels were larger than in our study. The relatively low incidence of MACE in the present registry is comparable to recently published randomised DES trials 22,23 and DES registries 24,25. Most randomised DES trials have been performed in patient populations with comprehensive lists of exclusion criteria, including recent myocardial infarction, left main coronary artery, ostial or bifurcated lesions, chronic total occlusions, visible thrombus, depressed left ventricular function or saphenous vein grafts 22,23. In our study, there were no exclusion criteria and all the above patient and lesion characteristics were allowed and were common. One strength of our study is the fact that Satakunta Central Hospital is the only centre with coronary angiography capacity in the referral area. In this rural area, the population is stationary enabling a complete and sufficiently long-term follow-up of an all-inclusive unrestricted PCI population reflecting daily clinical practice. Our study carries with it all the general problems related to registry based observational studies with non-blinded outcome assessment. The fact that this is a single-centre, low patient number registry may give rise to an unrecognised selection and performance bias. The surprisingly low rate of mortality may be attributable to a play of chance in a relatively small patient population with single vessel PCI. Angiographic control was performed on clinical grounds, and only in a minority of patients. So, our results probably underestimate the incidence of angiographic restenosis. On the other hand, by relying on clinical follow-up alone, we avoided the chance of unnecessary TVRs due to the occulo-stenotic reflex or patient s unjustified anxiety. In a recent meta-analysis of PCI trials with a follow-up > 6 months, the incidence of clinical restenosis and need for revascularisation increased with the duration of follow-up 26. Our data support the view that we need a follow-up longer then 6 months to disclose all the angioplasty related clinical events, since one-third of the MACE occurred after 6 months, even though we had no cases of late thrombosis. Conclusions These medium-term data confirm good safety profile of titanium nitride oxide coated stent (Titan ) even in high-risk patients and complex coronary lesions in routine clinical use. The clinical restenosis rate was low and so the Titan stent may be an attractive alternative to DES especially in patients with high-risk features for stent thrombosis. Further investigation is however warranted to randomly compare the Titan stent to other passive and active coated stents as an alternative to current drug-eluting stents in various subsets of patients. References 1. Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P, Belardi J, Sigwart U, Colombo A, Goy JJ, van den Heuvel P, Delcan J, Morel M. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331: Fischman DL, Leon MB, Baim DS, Schatz RA, Savage MP, Penn I, Detre K, Veltri L, Ricci D, Nobuyoshi M, Cleman M, Heuser R, Almond D, Teirstein PS, Fish RD, Colombo A, Brinker J, Moses J, Shaknovich A, Hirshfeld J, Bailey S, Ellis S, Rake R, Goldberg S. A randomised comparison of coronary-stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331: Abizaid A, Kornowski R, Mintz GS, Hong MK, Abizaid AS, Mehran R, Pichard AD, Kent KM, Satler LF, Wu H, Popma JJ, Leon MB. The influnce of diabetes mellitus on acute and late clinical outcomes following coronary stent implantation. J Am Coll Cardiol 1998;32: Kastrati A, Hall D, Schömig A. Long-term outcome after coronary stenting. Curr Control Trials Cardiovasc Med 2000;1: Garasic JM, Edelman ER, Squire JC, Seifert P, Williams MS, Rogers C. Stent and artery geometry determine intimal thickening independent of arterial injury. Circulation 2000;101: Kastrati A, Mehilli J, Dirschinger J, Dotzer F, Schuhlen H, Neumann FJ, Fleckenstein M, Pfafferott C, Seyfarth M, Schömig A. Intracoronary stenting and angiographic results: strut thickness effect on restenosis outcome (ISAR-STEREO) trial. Circulation 2001;103: Babapulle MN, Eisenberg MJ. Coated stents for the prevention of restenosis: part II. Circulation 2002;106: Koster R, Vieluf D, Kiehn M, Sommerauer M, Kahler J, Baldus S, Meinertz T, Hamm CW. Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet 2000;356:
71 Clinical research 9. vom Dahl J, Haager PK, Grube E, Gross M, Beythien C, Kromer EP, Cattelaens N, Hamm CW, Hoffmann R, Reineke T, Klues HG. Effects of gold coating of coronary stents on neointimal proliferation following stent implantation. Am J Cardiol 2002;89: Park SC, Lee CW, Hong MK, Kim JJ, Park SW, Tahk SJ, Jang YS, Seung KB, Yang JY, Jeong MH. Comparison of gold-coated NIR stents with uncoated NIR stents in patients with coronary artery disease. Am J Cardiol 2002;89: Steinemann SG. Metal implants and surface reactions. Injury 1996;27(suppl 3):SC16-SC Steinemann SG. Titanium: the material of choice? Periodontol ;17: Windecker S, Mayer I, De Pasquale G, Maier W, Dirsch O, De Groot P, Wu YP, Noll G, Leskosek B, Meier B, Hess OM. Stent coating with titanium-nitride oxide for reduction of neointimal hyperplasia. Circulation 2001;104: Windecker S, Simon R, Lins M, Klauss V, Eberli FR, Roffi M, Pedrazzini G, Moccetti T, Wenaweser P, Togni M, Tuller D, Zbinden R, Seiler C, Mehilli J, Kastrati A, Meier B, Hess OM. randomised comparison of a titanium-nitride oxide-coated stent with a stainless steel stent for coronary revascularisation. The TINOX trial. Circulation 2005;111: Valdes M, Fernandez J, Bethencourt A, Perez E, Calvo I, Servet M, Lopez JR, Martinez A, Valdesuso R. The TIBET Registry. Clinical and angiographic events in diabetes patients treated with the TITAN stent. Am J Cardiol 2004;94(suppl 6A):47E. 16. Mosseri M, Tamari I, Plich M, Hasin Y, Brizines M, Frimerman A, Miller H, Jafari J, Guetta V, Solomon M, Lotan C. Short- and long-term outcomes of the titanium-no stent registry. Cardiovasc Revasc Med 2005;6: Buehl A, Zoefel P. SPSS 11: Introduction in Modern Data Analysis. 8th ed. Munich, Germany: Addison-Wesley; McFadden EP, Stabile E, Regar E, Cheneau E, Ong AT, Kinnaird T, Suddath WO, Weissman NJ, Torguson R, Kent KM, Pichard AD, Satler LF, Waksman R, Serruys PW. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004;364: Ong AT, McFadden EP, Regar E, de Jaegere PT, van Domburg RT, Serruys PW. Late angiographic stent thrombosis (LAST) events with drugeluting stents. J Am Coll Cardiol 2005;45: Sketch MH, Ball M, Rutherford B, Popma JJ, Russell C, Kereiakes DJ. Evaluation of the Medtronic (Driver) cobalt-chromium alloy coronary stent system. Am J Cardiol 2005;95: Kereiakes DJ, Cox DA, Hermiller JB, Midei MG, Bachinsky WB, Nukta ED, Leon MB, Fink S, Marin L, Lansky AJ. Usefulness of a cobalt chromium coronary stent alloy. Am J Cardiol 2003;92: Moses JW, Leon MB, Popma JJ, Fitzgerald PJ, Holmes DR, O Shaughnessy C, Caputo RP, Kereiakes DJ, Williams DO, Teirstein PS, Jaeger JL, Kuntz RE. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349: Stone GW, Ellis SG, Cox DA, Hermiller J, O Shaughnessy C, Tift Mann J, Turco M, Caputo R, Bergin P, Greenberg J, Popma JJ, Russell ME. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N Engl J Med 2004;350: Ong AT, Serruys PW, Aoki J, Hoye A, van Mieghem C, Rodriguez- Granillo GA, Valgimigli M, Sonnenschein K, Regar E, van der Ent M, de Jaegere P, McFadden EP, Sianos G, van der Giessen WJ, de Feyter PJ, van Domburg RT. The unrestricted use of paclitaxel- versus sirolimuseluting stents for coronary artery disease in an unselected population. One-year results of the Taxus-stent evaluated at Rotterdam Cardiology Hospital (T-SEARCH) registry. J Am Coll Cardiol 2005;45: Zahn R, Hamm CW, Schneider S, Zeymer U, Nienaber CA, Richardt G, Kelm M, Levenson B, Bonzel T, Tebbe U, Sabin G, Senges J. Incidence and predictors of target vessel revascularisation and clinical event rates of the sirolimus-eluting coronary stent (results from the prospective multicenter German Cypher Stent Registry). Am J Cardiol 2005;95: Cutlip DE, Chauhan MS, Baim DS, Ho KK, Popma JJ, Carrozza JP, Cohen DJ, Kuntz RE. Clinical restenosis after coronary stenting: perspectives from multicenter clinical trials. J Am Coll Cardiol 2002;40:
72 Volume 2 - Number 2 - August 2006 Reprint The Titanium-NO Stent: results of a multicenter registry Morris Mosseri, Hilton Miller, Israel Tamari, Michael Plich, Yonathan Hasin, Mark Brizines, Aharon Frimerman, Jamal Jefary, Victor Guetta, Mivi Solomon, Chaim Lotan
73 Clinical research The Titanium-NO Stent: results of a multicenter registry Morris Mosseri 1 *, Hilton Miller 2, Israel Tamari 3, Michael Plich 4, Yonathan Hasin 5, Mark Brizines 6, Aharon Frimerman 7, Jamal Jefary 8, Victor Guetta 9, Mivi Solomon 10, Chaim Lotan 1 1. Hadassah Hebrew University Medical Center, Jerusalem; 2. Tel-Aviv Hospital, Tel-Aviv; 3. Wolfson Hospital Hulon; 4. Ziv Hospital, Zefat; 5. Poriah Hospital, Tiberias; 6. Nahariah Hospital, Nahariah; 7. Hilel-Jaffe Hospital, Hadera; 8. Barzilai Hospital, Ashkelon; 9. Shiba Hospital, Tel-Aviv; 10. The Israeli Working Group for Interventional Cardiology, Israel Morris Mosseri became a consultant for the Hexacath Company, France after completing the Titan study. None of the other co-authors have a conflict of interest to declare. KEYWORDS Allergy, angioplasty, atherosclerosis, coronary artery, restenosis Abstract Background: Contemporary stents discharge nickel, chromium and molybdenum which might contribute to restenosis. The Titan stent is coated with titanium nitride-oxide that prevents completely discharge of metal elements. Aims: To assess short and long term outcome of the Titan in a multi-centre registry. Methods: Included were all patients except those in cardiogenic shock. Titan stents were mm in diameter and 7-28 mm in length. Clinical follow-up was performed at 30 days and 6 months. Results: Total of 333 Titan stents were implanted in 296 patients (age 68.8±11.8 years, 81% men). Risk factors included hypercholesterolaemia (61.3%), hypertension (51.3%), diabetes mellitus (DM) (36.6%) and current smoking (27.6%). Eighty-one percent of patients had Acute Coronary Syndrome (ACS). Sixty two percent of treated lesions were B2/C type. Lesion length was 17.5±14.8 mm and stent diameter was 3.0±2.12 mm. Procedural success was 99.7%. At 180 days, 6.3% of patients had a total of 7.6% MACE including 5.4% TLR, 0.7% MI, 0.7% stent thrombosis and 0.7% death. Conclusion: The Titan stent has a remarkable safety profile. Notwithstanding the highly complicated lesion and case mix, the short- and long-term results of this registry approach those of drug-eluting stents. * Corresponding author: Hadassah Hebrew University Medical Center, P.O.Box 12,000, Jerusalem 91,120 Israel mosseri@cc.huji.ac.il Europa Edition All rights reserved. EuroInterv.2006;2:
74 Titanium-NO Stent Registry Introduction Inflammation is an imperative factor in the pathogenesis of restenosis. Contemporary stents are made of stainless steel or cobalt/chromium alloys, all of which comprise significant amounts of nickel, cobalt and chromium and some contain also molybdenum. Up to 15% of the population have an allergy to nickel, chromium or molybdenum, triggered by reaction of inflammatory cells to metals charged with ions. Such allergies might therefore contribute to restenosis. The Titan stent (Hexacath Company, France) is a balloon expandable stainless steel stent coated with titanium nitride-oxide which prevents completely discharge of nickel, chromium and molybdenum. Windecker et al have shown that Titanium-Nitride-Oxide (TiNOX) coating diminishes cell and tissue reaction in a pig model 1. We have found exceptionally good outcomes after implantation of a Titanium-Nitride-Oxide (Titan) stent in a small group of patients 2. Recently, a small multi-centre randomised clinical study has demonstrated reduction in restenosis by the TiNOX stent compared to stainless steel stents 3. To assess short and long term outcome of the Titan stent we performed a multi-centre registry of Titan stent implantation. Methods Patients This multi-centre (9 hospitals) registry was performed between April 1, 2003 and January 31 of The first 100 patients were recruited as a part of the requirements of the Israeli Ministry of Health for approval of new stents. The registry was then extended by recruiting another 196 patients in 2 medical centres (Hadassah, Jerusalem and Tel-Aviv hospital, Tel-Aviv). Included were all patients who were candidates for stent implantation. Since most operators excluded patients in cardiogenic shock from national new stent registries, we excluded such patients from this paper. Lesions Lesions treated with the Titan stent included de-novo and restenotic lesions of native coronary arteries and Saphenous Vein Grafts (SVG). Stents Titan stent diameter was and length was 7-28 mm. Data analysis Clinical data included gender, age, risk factors, cardiac history and clinical presentation. PCI data included lesion location, type and characteristics, delivery data and deployment pressure. Vessel diameters and lesion length were estimated by the operators. Thirty day and 6 month phone-call follow-up was performed by an independent research nurse. Outcome data included immediate technical and clinical success and complications, and major adverse cardiac events (MACE) including sub-acute thrombosis, MI, target lesion revascularisation (TLR), target vessel revascularisation (TVR) and death, at 30 days and 6 months. Results Patients demographics A total of 333 Titan stents were implanted in 296 patients. Six month follow-up was completed in 295 patients (one tourist patient was lost to follow-up). Patients age was 68.8±11.8 (33-87) years and 246 (81%) of them were men. Risk factors for coronary artery disease, previous cardiac history and indications for PCI are presented in Table 1. Table 1. Patients demographics % Risk factors Hypercholesterolaemia 61.3 Hypertension 51.3 DM 36.6 Current Smoking 27.6 Past Smoking 18.0 Family history 17.0 Cardiac history Prior MI 26.3 Prior PCI 40.3 Prior CABG 11.6 Indications for PCI Silent ischaemia 9.4 Stable AP 9.6 Acute MI 36.0 Unstable AP 45.0 Coronary anatomy and lesion demographics Thirty-three percent of the patients had single vessel, 30% had double vessel and 37% had triple vessel disease. The vessels treated, lesion location, lesion type and indications for stenting are presented in Table 2. Stent diameter was 3.0±2.12 mm and lesion length was 17.5±14.8 mm. Fifty-one percent of the lesions were less than 15 mm in length, 36% were and 13% were mm in length. Stent deployment and peri-procedural medical treatment In 91% of the patients dilation of the lesion with a balloon catheter was performed prior to stent implantation and in 9% direct stenting was performed. This reflects the practice of the operators during the registry period. The pressure used for deployment was < 12 bar in 21% and > 12 bars in 79% of the patients. All patients were treated during PCI with heparin, and 28% were treated with IIb-IIIa antagonists. All patients were treated with clopidogrel 75 mg for one month and aspirin 100 mg for life. Angiographic and clinical outcome Procedural success was 99.7%. At 30 days 1% of patients (3 patients) had total of 1.6% MACE, including 0.6% TVR (Table 3)
75 Clinical research Table 2. Lesions demographics Vessels treated LM 0.3 LAD 34 Diagonal 2 Cx 7 Marginal 13 RCA 33 PDA 9 SVG 2 Lesion location Ostial 3 Proximal 45 Mid 36 Distal 16 Lesion type A 9.5 B B C 18.6 Indication for stenting Dissection 6.9 Residual stenosis > 30% 9.9 Acute MI 23.7 In-stent restenosis 3.9 Restenosis prevention 55.4 Table 3. MACE at 30 days and 6 months follow up MACE At 30 days At 6 months % (patients) % (patients) TVR 0.6% (2) 5.7% (17) (TLR-5.4%) PCI 0.6% (2) 5.1% (15) CABG 0 0.6% (2) QWMI 0 0.3% (1) NQWMI 0.3% (1) 0.3% (1) Subacute-thrombosis 0.3% (1) Acute Thrombosis 0.3% (1) 0.3% (1) Death 0.3% (1) 0.7% (2) Total MACE 1.6% (5) 7.6% (21) At 180 days 6.3% of patients had total of 7.6% MACE including TVR 5.7% (5.4% of them TLR), 5.1% of which were PCI and 0.6% CABG (Table 3). One patient underwent Non-Q MI due to acute thrombosis and another patient Q-wave MI due to sub-acute thrombosis (total of 0.7%). Two patients (0.7%) died; the first, a 74 year old lady, had a Titan stent implanted to Cx and a non-titan stent to SVG to PL. Because of no-flow in the PL she was treated with IIb- IIIa antagonists and IABP. The next day she underwent resection of the small intestine due to superior mesenteric artery occlusion. % Three weeks later she suffered from dyspnea, hypotension and VF, underwent a failed CPR and died. The second patient was a 79 years old post CABG man who suffered from amyloidosis. He underwent PCI and successful implantation of 2 Titan stents to a long lesion in the 1st marginal. Six weeks later he was hospitalised due to severe right heart failure, sinus bradycardia, paroxysmal atrial flutter and renal failure. He was scheduled for atrial flutter ablation and pace-maker implantation but deteriorated to severe dyspnea and desaturation and underwent a failed CPR. Another 24 patients (8%) underwent angiography for chest pain and their coronary arteries stented with Titan were patent. At 180 days 83% of the patients had class 1 angina, 15% had class 2, 1% had class 3 and 1% had class 4 angina. Discussion The results of this multi-centre registry with the Titan, a Titanium- Nitride-Oxide coated stent are remarkably good. At 6 months there were only 5.7% TVR (of them 5.4% TLR), 0.7% MI and 0.7% death. The inflammation burden and restenosis In-stent restenosis occurs in 20-30% of patients undergoing stent implantation and is caused entirely by neointimal proliferation 4,5. Inflammation is an imperative factor in the restenosis process. The inflammation burden prior and after angioplasty depends on the individual s systemic and local (arterial) factors. Diabetes mellitus, vessel morphology (e.g. vessel diameter, lesion length, amount of residual plaque burden) 6,7 and procedural factors (e.g. vessel wall trauma and basement membrane disruption) may all amplify instent restenosis. The role of metallic implants in restenosis Stent implantation adds iatrogenic factor by enhancing neo-intimal hyperplasia, a so called response to foreign material. Metallic implants can induce electron exchange (redox reaction), proton exchange (hydrolysis), and complex formation (metal ion-organic molecule binding) in living tissues 8. The resultant protein (e.g. fibrinogen) activation, cell toxicity, fibroblast growth stimulation, platelet, monocyte/ macrophage and endothelial cells adhesion, and endothelial cell migration 8 may all contribute to restenosis. Stainless steel used to produce stents (316L) is made of iron fortified with carbon and contains significant amounts of Nickel (12%), Chromium (as chromate) (17%) and Molybdenum (2%). Ions of these elements elute from the stents and might induce the above mentioned reactions 8. Nickel has been shown to cause skin contact allergic dermatitis in 5% of the male, and 15% of the female population 9, and inflammatory and allergic reactions that form new tissue around metallic alloys containing nickel are well known in patients with dental and orthopaedic implants 10. It is conceivable that stents which contain nickel and other elements would enhance neointimal hyperplasia formation. In a study performed by Koster et al, 131 patients were studied prior to angiography for suspected coronary in-stent restenosis of a stainless-steel stent 9. All patients underwent allergy patch testing for nickel, chromate, molybdenum, manganese and stainless steel. Eighty-nine patients had restenosis and 10 of them (11%) had positive patch test results and under
76 Titanium-NO Stent Registry went repeat angioplasty. Forty-two patients did not have restenosis and none of them had positive patch test (p=0.03). Thus, all 10 patients with positive patch test had in-stent restenosis. Another study failed to show correlation between nickel sensitivity and restenosis in a group of 20 post-angioplasty and 7 pre-angioplasty patients, but these groups were far too small to yield a measurable restenosis rate or draw any conclusion 11. Stent coatings Several stent coatings such as heparin 12,13, silicon carbide 14 and gold 15 have been constructed to create a biologically inert barrier between the stent surface and circulating blood but none of them decreased and some even increased 15 restenosis rate. Although drug eluting stents (DES) decrease restenosis, they have not abolished it. An investigation of 8 different biodegradable and nondegradable polymers showed marked inflammatory reactions with subsequent neointimal hyperplasia 16, and it has been proposed that this inflammatory process contributes to residual restenosis and possibly late thrombosis. Thus, there is still a need to improve bare metal stents features both as stand alone and platform for carrying neointimal hyperplasia inhibiting drugs. The Titanium Nitride-Oxide stent Titanium is biologically inert due to its low electrochemical surface potential. It has an excellent biocompatibility because it has neither redox or hydrolysis reaction nor complex formation and biologically it had no fibroblast growth, protein or platelet adhesion 1,3,8,10. Titanium-nitride-oxide (TiNOX) is a titanium alloy suitable for coating of stainless steel stents preventing completely release of Nickel, Chromium, Molybdenum or other metals. In-vitro experiments have shown reduced platelet adhesion and fibrinogen binding to TiNOX coated stents during incubation in human plasma for 48 hours 1. Invivo experiments with the pig model have proved decreased cell and tissue reaction 1. In a recent small multi-centre randomised study, Windecker et al have shown reduction in angiographic and IVUS parameters of restenosis among patients treated with a non-commercial, custom made TiNOX stent compared to stainless steel stents, and this was translated into a lower MACE rate 3. The lesions treated in that study were however undemanding and clinically complicated patients were excluded. In the present study we used a commercial TiNOX stent (Hexacath, France). Experience with this stent has been presented recently. Karjalainen et al has performed a single-centre registry in Finland in 195 unselected patients (214 stents). At 9 months clinical follow up, MACE rate, cardiac death, MI and TLR were 10.3%, 0%, 4.1% and 5.1%, respectively 17. Valdes et al have performed a multi-centre (9 hospitals) registry in Spain in 156 diabetic patients (197 stents). At 6 months clinical follow up, MACE rate, cardiac death, QMI and TLR were 10.3%, 1.95%, 1.29% and 7.09%, respectively. The authors considered these results to be the best ever encountered with bare-metal stents, and close to some drug eluting stents in diabetic patients 18. In this study we included elderly patients (68.8±11.8, years old) with high risk profile; 36.6% were diabetics, 81% had ACS (36% hospitalised with acute MI) and 67% had multi-vessel disease. The lesions were mid or distal in >50% of cases, 62% were type B2 or C, and lesion length was 17.5±14.8 mm. Notwithstanding this highly complicated lesion and case mix, the results were excellent with only 5.4% TLR and 1.3% composite of death or MI. Post-mortem examination was not performed in the two patients who died and therefore stent thrombosis (non-titan or Titan) can not be excluded. Non-coronary death is however more likely in the amyloid patient. Possible contributors to these favourable results are TiNOX s low electrochemical surface potential and the avoidance of nickel and chromium discharge. The role of NO attached to titanium is not known and has to be elucidated. Interestingly, pooled data of 15 Israeli national BMS registries (100 stents in each) showed 10.6% TVR and 1.3% death rate. In comparison, the Israeli Cypher registry had 2.2% TVR and 0.7% death rate at 6 months. Thus, the Titan results are situated in between other BMS and Cypher results. Also of interest, a recent meta-analysis of 3,669 patients treated with sirolimus- or paclitaxel-eluting stents, demonstrated TLR of 5.1% and 7.8%, death rate of 1.4% and 1.6%, and composite of death or MI of 4.9% and 5.8% within 6-13 months, respectively 19. Since DES are not devoid of drawbacks including high cost, it is hoped that further developing of inert or bioactive stents such as the TiNOX might compete favourably with DES or serve as better platform for carrying neointimal hyperplasia inhibiting drugs. Study limitations Our study involves an inherent limitation of any registry, namely the non-blinded outcome assessment. Since not all hospitalised patients were treated with a Titan stent during the registry period, there might be a selection bias. This registry has a low/patient number experience. TLR was clinically driven and silent restenosis might have been overlooked. These limitations are partially counterbalanced by registries advantages over randomised trials; population selection and clinical relevance resemble real-life better, and unnecessary interventions in borderline lesions (that affect study results) are avoided. In conclusion, the Titan is stent coated with titanium-nitride-oxide, which has an excellent biocompatibility and eliminates the discharge of elements such as nickel, chromium and molybdenum. This multi-centre registry demonstrated excellent short and long term outcome with very low clinical TLR, MI and death rates. References 1. Windecker, S, Mayer I, De Pasquale G, Maier W, Dirsch O, De Groot P, Wu Y, Noll G, Leskosek B, Meier B, Hess O. Stent coating with Titanium- Nitide-Oxide for reduction of neointimal hyperplasia. Circulation 2001; 104: Mosseri M, Tamari I, Plich M, Hasin Y, Brizines M, Frimerman A, Miller H, Jafari J, Guetta V, Solomon M, Lotan C. Short and long term outcome of the Titanium-NO stent registry. Cardiovasc Revasc Med 6(1); 2-6, Windecker S, Simon R, Lins M, Klauss V, Eberli FR,, Roffi M, Pedrazzini G, Moccetti T, Wenaweser P, Togni M, Tüller D, Zbinden R, Seiler C, Mehilli J, Kastrati A, Meier B, Hess OM. Randomized
77 Clinical research Comparison of a Titanium-Nitride-Oxide-Coated Stent With a Stainless Steel Stent for Coronary Revascularization. The TiNOX Trial. Circulation 2005;111: Dussaillant GR, Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ, Wong SC, Leon MB. Small stent size and intimal hyperplasia contribute to restenosis: a volumetric intravascular ultrasound analysis. J Am Coll Cardiol. 1995; 26: Hoffmann R, Mintz GS, Dussaillant GR, Popma JJ, Pichard AD, Satler LF, Kent KM, Griffin J, Leon MB. Patterns and mechanisms of instent restenosis: a serial intravascular ultrasound study. Circulation. 1996; 94: Serruys PW, Kay IP, Disco C, Deshpande NV, de Feyter PJ. Periprocedural quantitative coronary angiography after Palmaz-Schatz stent implantation predicts the restenosis rate at six months: results of a metaanalysis of the BElgian NEtherlands Stent study (BENESTENT) I, BENES- TENT II Pilot, BENESTENT II and MUSIC trials: Multicenter Ultrasound Stent In Coronaries. J Am Coll Cardiol 1999; 34: Prati F, Di Mario C, Moussa I, Reimers B, Mallus MT, Parma A, Lioy E, Colombo A. In-stent neointimal proliferation correlates with the amount of residual plaque burden outside the stent: an intravascular ultrasound study. Circulation 1999; 99: Steinemann SG. Metal implants and surface reactions. Injury. 1996; 27 (suppl 3): SC16-SC Koster R, Vieluf D, Kiehn M, Sommerauer M, Kahler J, Baldus S, Meinertz T, Hamm CW. Nickel and Molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet 2000; 356: Steinemann SG. Titanium: the material of choice? Periodontology 2000; 17: Hillen U, Haude M, Erbel R, Goos M. Evaluation of metal allergies in patients with coronary arteries. Contact Dermatitis 2002; 47: Hardhammar PA, vanbeusekom HMM, Emanuelsson HU, Hofma SH, Albertsson PA, Verdouw PD, Boersma E, Serruys PW. Van der Giessen WJ. Reduction in thrombotic events with heparin-coated Palmaz- Schatz stents in normal porcine coronary arteries. Circulation. 1996; 93: Serruys PW, van Hout B, Bonnier H, Legrand V, Garcia E, Macaya C, Sousa E, van der Giessen W, Colombo A, Seabra-Gomes R, Kiemeneij F, Ruygrok P, Ormiston J, Emanuelsson H, Fajadet J, Haude M, Klugmann S, Morel MA. Randomised comparison of implantation of heparin-coated stents with balloon angioplasty in selected patients with coronary artery disease (Benestent II). Lancet. 1998; 352: Heublein B, Pethig K, Elsayed AM. Silicon carbide coating: a semiconducting hybrid design of coronary stents: a feasibility study. J Invasive Cardiol. 1998; 10: Kastrati A, Schomig A, Dirschinger J, Mehilli J, von Welser N, Pache J, Schuhlen H, Schilling T, Schmitt C, Neumann FJ. Increased risk of restenosis after placement of gold-coated stents: results of a randomized trial comparing gold-coated with uncoated steel stents in patients with coronary artery disease. Circulation. 2000; 101: van der Giessen WJ, Lincoff AM, Schwartz RS, van beusekom HM, Serruys PW, Holmes DR, Ellis SG, Topol EJ. Marked inflammatory sequelae to implantation of biodegradable and nonbiodegradable polymers in porcine coronary arteries. Circulation. 1996; 94: Karjalainen P, Ylitalo A, Airaksinen J. Coated stent in clinical practice; The Titan Pori Registry. TCT Meeting, Washington DC, October 20, M. Valdés, J. Fernández, A. Bethencourt, E. Pérez, I. Calvo, JR López, A. Martínez, R Valdesuso, J Moreu. Clinical and Angiographic results Events in Diabetic Patients Treated with the TITAN Stent. TCT Meeting, Washington DC, September 30, Kastrati A, Dibra A, Eberle S, Stat D, Mehilli J, de Lezo JS, Goy JJ, Ulm K, Schömig A. Sirolimus-eluting stents vs Paclitaxel-eluting stents in patients with coronary artery disease, meta-analysis of randomized trials. JAMA 2005; 294:

78 Cardiovascular Revascularization Medicine 6 (2005) 2 6 Short- and long-term outcomes of the titanium-no stent registry Morris Mosseri a, T, Israel Tamari b, Michael Plich c, Yonathan Hasin d, Mark Brizines e, Aaron Frimerman f, Hilton Miller g, Jamal Jafari h, Victor Guetta i, Mivi Solomon j, Chaim Lotan a a Hadassah Hebrew University Medical Center, Jerusalem, Israel b Wolfson Hospital, Hulon, Israel c Ziv Hospital, Zefat, Israel d Poriah Hospital, Tiberias, Israel e Nahariah Hospital, Nahariah, Israel f Hilel-Jaffe Hospital, Hadera, Israel g Ichilov Hospital, Tel-Aviv, Israel h Barzilai Hospital, Ashkelon, Israel i Shiba Hospital, Tel-Aviv, Israel j The Israeli Working Group for Interventional Cardiology, Israel Received 18 April 2005; accepted 18 April 2005 Abstract Keywords: Background: Five to 15% of the population have allergy to nickel, chromium, or molybdenum, which is a potential cause for in-stent restenosis. The Titan stent is made of stainless steel and is coated with titanium-nitride oxide (TiNOX), which completely prevents the discharge of metal elements. We performed a real-life multicenter registry to assess the short- and long-term characteristics of the Titan stent. Methods and results: A total of 103 Titan stents was implanted in 100 patients. Patients were 61.4F12.6 years old (81 men). Risk factors included hypercholesterolemia (63%), hypertension (53%), diabetes mellitus (DM; 35%), and current smoking (23%). Indications for PCI (percutaneous coronary intervention) were acute coronary syndromes (ACS) in 68% [acute ST elevation myocardial infarction (MI) in 8%], stable AP (angina pectoris) in 25%, and silent ischemia in 7% of the patients. Fifty-two percent of the treated lesions were of Type B2 or C. Lesion length was 14.3F2.9 mm and stent diameter was 3.06F0.36 mm. Indications for stenting were prevention of restenosis in 66%, residual stenosis in 33%, dissection in 13%, acute MI in 13%, and in-stent restenosis in 7% of the patients. Procedural success was 100%, with no complications. At 30 days, there were no major adverse cardiac events (MACE), including death, MI, and revascularization. At 180 days, only three patients had TVR (target vessel revascularization); two had TLR (target lesion revascularization) (one PCI and one CABG [coronary artery bypass grafting]), and one patient had a new narrowing proximal to the stent and underwent CABG due to multivessel disease. Conclusions: The Titan stent has a remarkable safety profile in high-risk patients and complex coronary lesions and excellent short- and long-term outcome with a very low clinical TLR rate. D 2005 Elsevier Inc. All rights reserved. Allergy; Angioplasty; Atherosclerosis; Coronary artery; Restenosis 1. Introduction T Corresponding author. Hadassah Hebrew University Medical Center, P.O. Box 12,000, Jerusalem 91, 120 Israel. Tel.: /4; fax: address: mosseri@cc.huji.ac.il (M. Mosseri). Most stents have been made from stainless steel, which is known to be contaminated from other elements and agents during foundry production. Recently, the use of other alloys, /05/$ see front matter D 2005 Elsevier Inc. All rights reserved. doi: /j.carrev
79 M. Mosseri et al. / Cardiovascular Revascularization Medicine 6 (2005) such as cobalt chromium, enabled the construction of more flexible stents with thinner struts. Inflammation plays a major role in restenosis. Inflammatory cells react differently to different chemical domains and metals and are often stimulated by ionic charges. Five to 15% of the population have an allergy to nickel, chromium, or molybdenum, which has been held responsible for inducing restenosis. The Titan stent is a balloon expandable stent made of stainless steel and coated with titanium-nitride oxide (TiNOX), which completely prevents discharge of nickel, chromium and molybdenum. Windeck er et al. [ 1] have shown that TiNOX coating decreases tissue reaction and diminishes cell reaction in a pig model. In vitro experiments implied that the electromechanical properties of TiNOX were more important for the prevention of neointimal hyperplasia than was the difference in platelet adhesion or fibrinogen binding [1]. We report here the results of a multicenter registry that was performed to assess the short- and long-term characteristics of the Titan stent in patients. 2. Methods This multicenter (nine hospitals) registry was performed as a part of the requirements of the Israeli Ministry of Health for the approval of new stents Patients and lesions Included were all patients who were candidates for stent implantation. Choosing the Titan stent was at the operator discretion, with no exclusion criteria. Treated lesions included de novo and restenotic lesions of native coronary arteries and SVGs. Thirty-day and 6-month phone call follow-up was performed by an independent research nurse Stents Titan stents were available in diameters of 2.5, 3.0, and 3.5 mm and lengths of 10, 13, 16, and 19 mm Data analysis and statistics Clinical data included gender, age, risk factors, cardiac history, and clinical presentation. PCI data included lesion location, type and characteristics, delivery data, stent size, and deployment pressure. Outcome data included immediate technical and clinical success and complications and major adverse cardiac events (MACE), including subacute thrombosis, myocardial infarction (MI), TLR, TVR, and death, at 30 days and 6 months. The v 2 test was used to compare the TVR and death rate of the Titan stent with previous Israeli national stent registries (pooled data of 15 bare stents and 1 drug-eluting stent). 3. Results 3.1. Patients The mean patient age was 61.4F12.6 (42 86) years, and 81% of them were men. Risk factors for ischemic heart disease included hypercholesterolemia in 63%, hypertension in 53%, diabetes mellitus (DM) in 35%, current smoking in 23%, past smoking in 19%, and family history in 12% of the patients. Fifty-seven of the patients had single vessel, 19% had double vessel, and 24% had triple vessel disease. Previous cardiac history included MI in 21%, PCI in 14%, and CABG in 7% of the patients. The indications for PCI were acute coronary syndromes (ACS) in 68%, including acute ST elevation MI in 8% (six were treated with primary angioplasty and two with thrombolysis), non-st elevation MI in 26%, and unstable AP in 34% of the patients. Other indications for PCI were stable AP in 25% and silent ischemia in 7% of the patients. During PCI, all patients were treated with heparin, and 20% were treated with IIb IIIa antagonists. All patients were treated with Aspirin 100 mg for life and Clopidogrel 75 mg for 1 month Lesion anatomy and morphology A total of 103 Titan stents was implanted in 100 patients. Stented arteries included 34 LAD coronary arteries, 29 RCA, 20 Cx, 15 marginal branches, 12 diagonal branches, 2 LM coronary arteries, and 1 SVG. The stented segment was proximal in 37, mid in 46, distal in 10, and ostial in 7 of the lesions. Sixteen percent of the treated lesions was of Type A, 32% of Type B1, 38% Type B2, and 14% Type C. Stent diameter was 3.06F0.36 mm (2.5 mm in 22%, 3 mm in 46%, and 3.5 mm in 35% of the stents). Stent length was 14.31F2.90 mm. Forty seven of 100 patients had a lesion length of z15 mm. Fourteen lesions had a bend of N458, and 35 were calcified. The indication for stenting as recorded by the operators was prevention of restenosis in 66% of the patients, residual stenosis in 33%, dissection in 13%, and acute MI in 13%. Table 1 The 180-day follow-up results of 15 stent registries in Israel Bare stent Titan Cypher Total number TVR (CABG) 124 (29) 3 (2) 5 (5) Death The data are given in absolute numbers. See Results and Fig. 1 for percent data and statistics.
80 4 M. Mosseri et al. / Cardiovascular Revascularization Medicine 6 (2005) % Notably, in 7% of the patients, a Titan stent was implanted within an in-stent restenosis Stent deployment In 71% of the patients, dilation of the lesion with a balloon catheter was performed prior to stent implantation, and in 29%, direct stenting was performed. The pressure used for deployment was b12 bar in 42% and z12 bars in 58% of the patients. Twenty patients underwent an implantation of additional 26 non-titan stents to other lesions (3 of them Cypher stents) Outcome Procedural success was 100%, with no complications. At 30 days, there was no MACE. At 180 days, 95% of the patients had angina class grade I. Eight patients underwent repeat angiography for chest pain and five of them had patent stents. Only three patients (3%) had TVR; two had TLR (one PCI and one CABG), and one had a new narrowing proximal to the stent and underwent CABG due to multivessel disease. A comparison of 180-day TVR rate of the Titan stent with pooled data of 15 Israeli national bare-stent registries (which had 8.6% TVR, Table 1 and Fig. 1) showed that the Titan stent was superior ( Pb.05). A comparison of 180-day TVR of the Titan stent with The Israeli Cypher registry (which had 1.2% TVR, Table 1 and Fig. 1) showed that the Titan stent was not statistically inferior to the Cypher. The number of deaths in all three groups was small and with no statistical difference. 4. Discussion P<0.05 P=NS P=NS 6 months TVR 6 months Death Bare stent Titan Cypher Fig. 1. One hundred eighty-days follow-up results of 17 stent (including Titan and Cypher) registries in Israel. In-stent restenosis is observed in 20 30% of patients undergoing stent implantation and is caused by neointimal proliferation [2,3]. Drug-eluting stents have not abolished restenosis and still have 8 9% angiographic restenosis and 1 2% TVR. Factors such as diabetes mellitus, vessel morphology (e.g., vessel diameter, lesion length, and amount of residual plaque burden; [4,5]), stent characteristics (the use of multiple stents and their length), and extent of arterial trauma during angioplasty may all contribute to the increased rate of in-stent restenosis. In this manuscript, we present, for the first time, clinical experience with the Titan, a TiNOX-coated stent. The results of this real-life multicenter registry of high-risk patients with complex coronary lesions were exceptionally good. There were no immediate complications and only 3% 6-month TVR (2% TLR), with no other MACE Biologic interactions of metallic implants Metallic implants can interact with living tissues in three ways: electron exchange (redox reaction), proton exchange (hydrolysis), and complex formation (metal ion-organic molecule binding). These reactions are responsible for protein (e.g., fibrinogen) activation, cell toxicity, fibroblast growth stimulation, platelet, monocyte/macrophage and endothelial cells adhesion, and endothelial cell migration. Stainless steel is made of iron fortified with carbon. Stainless steel used to produce stents (316L) contains significant amounts of other elements, mainly nickel (12%), chromium (as chromate; 17%), and molybdenum (2%). This combination renders the alloy even more resistant to corrosion (rust) while in contact with blood, but ions of these elements are eluted from the stents. Iron and carbon are major constituents of cell structure and metabolism and are unlikely to cause any hypersensitivity reaction. The biological behavior of stainless steel is dominated principally by its nickel component, which induces all three reactions mentioned above [6]. Clinically, nickel has been shown to cause skin contact allergic reaction in 5% of male and 15% of female population. Inflammatory and allergic reactions associated with the formation of new tissue around metallic alloys that include nickel are well known in patients with orthopedic and dental implants [7]. To date, there are only two clinical studies that examined the association between metal allergy and coronary in-stent restenosis. Koster et al. [7] studied 131 patients prior to angiography for suspected coronary in-stent restenosis of a stainless-steel stent. All patients underwent allergy patch testing for nickel, chromate, molybdenum, manganese, and stainless steel. Eighty-nine patients had restenosis (N50% angiographic narrowing), and 10 of them (11%) had positive patch test results (4 to molybdenum and 7 to nickel) and underwent repeat angioplasty. Forty-two patients did not have restenosis and none of them had a positive patch test ( P=.03). Thus, all 10 patients with a positive patch test had in-stent restenosis. There was no positive reaction to chromate, manganese, or 316L. Following this publication, Hillen et al. [8] performed a patch test in a small group of 20 patients after angioplasty and another 7 patients before angioplasty (another 7 patients in the prospective group did not get a stent or were lost to follow up). Nickel sensitivity did not correlate with
81 M. Mosseri et al. / Cardiovascular Revascularization Medicine 6 (2005) restenosis, but these groups were far too small to expect a measurable restenosis rate or draw any conclusion Stent coatings for the prevention of thrombosis and restenosis Stent coatings are made to create a biologically inert barrier between the stent surface and circulating blood. Heparin-coated stents have been shown to reduce subacute stent thrombosis [9,10], but no reduction in neointimal proliferation was observed in animal models or in clinical studies. Silicon carbide, a semiconductor ceramic, deposited on the surface of coronary artery stents reduces the electrochemical surface potential of stainless-steel stents. However, stent thrombosis and in-stent restenosis rates in one clinical study were 2% and 27%, respectively [11], similar to uncoated stents. Gold-coated stents have been used in two coronary artery stents (InFlow and NIR Royal, Boston Scientific). A randomized clinical trial demonstrated a significantly increased (50%) in-stent restenosis in the gold-coated inflow stents compared with 38% restenosis in identical uncoated stainless-steel stents [12]. Several polymers have been investigated as a platform for drug-eluting stents. An investigation of eight different biodegradable and nondegradable polymers showed marked inflammatory reactions with subsequent neointimal hyperplasia [13]. Nevertheless, the polymers included in the drug-eluting stents presently in use (Cypher and Taxus) did not impede with the favorable results of these stents. Titanium, with its low electrochemical surface potential, is biologically inert and has excellent biocompatibility, exemplified by the lack of a redox and hydrolysis reaction, as well as an absent complex formation. Biologically, this is translated to no fibroblast growth, protein, or platelet adhesion observed with titanium [14]. TiNOX is a titanium alloy suitable for the coating of stainless-steel stents. TiNOX does not release nickel, chromium, molybdenum, or other metals. Windecker et al. [1] have shown that, in a pig model, stents coated with TiNOX had decreased tissue reaction and diminished cell reaction. In vitro experiments showed reduced platelet adhesion and fibrinogen binding after the incubation of TiNOX-coated stents with human plasma for 48 h [1]. The results of these experiments implied that the electromechanical properties of TiNOX were more important than the reduced platelet and fibrinogen effects for the prevention of neointimal hyperplasia. It is important to emphasize that nitride oxide was used as a part of the TiNOX coating in the Titan stent because it rendered titanium suitable for coating stainless steel stents. The TiNOX does not release NO, and it is not known whether it obtains biological characteristics similar to those of free NO molecules released from endothelial cells. Inflammation is an important factor in restenosis. The inflammation burden prior and after angioplasty depends on individual systemic and local (arterial) factors and on procedural factors such as the degree of trauma to the vessel wall and disruption of the basement membrane. Bare stents add iatrogenic contribution by enhancing neointimal hyperplasia a so-called bresponse to foreign materialq. It is imperative to diminish any inflammatory stimulus that may exist before, during, or after percutaneous vascular intervention. Our study is the first to summarize clinical experience with the TiNOX-coated stent. While keeping in mind that it is a registry and not a randomized study, the results are remarkably good, especially when compared with our database stent registries performed in the same fashion. We propose that this outcome is due to the prevention of discharge of elements such as nickel and chromium, thereby eliminating one important cause for inflammation and restenosis. The possible contribution of the low electrochemical surface potential of titanium and of nitride oxide to the outstanding results in this study has to be elucidated. In summary, nickel and other elements eluted from stainless steel stents may provoke inflammatory reaction. The Titan stent is coated with TiNOX, which eliminates the discharge of such elements. In this real-life multicenter registry, the Titan stent had a remarkable safety profile in high-risk patients with complex coronary lesions, as well as excellent short- and long-term outcome with a very low clinical TLR rate. References [1] Windecker S, Mayer I, De Pasquale G, Maier W, Dirsch O, De Groot P, Wu Y, Noll G, Leskosek B, Meier B, Hess O. Stent coating with titanium-nitride-oxide for reduction of neointimal hyperplasia. Circulation 2001;104: [2] Dussaillant GR, Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ, Wong SC, Leon MB. Small stent size and intimal hyperplasia contribute to restenosis: a volumetric intravascular ultrasound analysis. J Am Coll Cardiol 1995;26: [3] Hoffmann R, Mintz GS, Dussaillant GR, Popma JJ, Pichard AD, Satler LF, Kent KM, Griffin J, Leon MB. Patterns and mechanisms of in-stent restenosis: a serial intravascular ultrasound study. Circulation 1996;94: [4] Serruys PW, Kay IP, Disco C, Deshpande NV, de Feyter PJ. Periprocedural quantitative coronary angiography after Palmaz-Schatz stent implantation predicts the restenosis rate at six months: results of a meta-analysis of the BElgian NEtherlands Stent study (BENE- STENT) I, BENESTENT II Pilot, BENESTENT II and MUSIC trials: multicenter ultrasound stent in coronaries. J Am Coll Cardiol 1999;34: [5] Prati F, Di Mario C, Moussa I, Reimers B, Mallus MT, Parma A, Lioy E, Colombo A. In-stent neointimal proliferation correlates with the amount of residual plaque burden outside the stent: an intravascular ultrasound study. Circulation 1999;99: [6] Steinemann SG. Metal implants and surface reactions. Injury 1996;27(Suppl 3):SC16 SC22. [7] Koster R, Vieluf D, Kiehn M, Sommerauer M, Kahler J, Baldus S, Meinertz T, Hamm CW. Nickel and molybdenum contact allergies in patients with coronary in-stent restenosis. Lancet 2000;356: [8] Hillen U, Haude M, Erbel R, Goos M. Evaluation of metal allergies in patients with coronary arteries. Contact Dermatitis 2002;47: [9] Hardhammar PA, vanbeusekom HMM, Emanuelsson HU, Hofma SH, Albertsson PA, Verdouw PD, Boersma E, Serruys PW, Van der
82 6 M. Mosseri et al. / Cardiovascular Revascularization Medicine 6 (2005) 2 6 Giessen WJ. Reduction in thrombotic events with heparin-coated Palmaz-Schatz stents in normal porcine coronary arteries. Circulation 1996;93: [10] Serruys PW, van Hout B, Bonnier H, Legrand V, Garcia E, Macaya C, Sousa E, van der Giessen W, Colombo A, Seabra-Gomes R, Kiemeneij F, Ruygrok P, Ormiston J, Emanuelsson H, Fajadet J, Haude M, Klugmann S, Morel MA. Randomised comparison of implantation of heparin-coated stents with balloon angioplasty in selected patients with coronary artery disease (Benestent II). Lancet 1998;352: [11] Heublein B, Pethig K, Elsayed AM. Silicon carbide coating: a semiconducting hybrid design of coronary stents: a feasibility study. J Invasive Cardiol 1998;10: [12] Kastrati A, Schomig A, Dirschinger J, Mehilli J, von Welser N, Pache J, Schuhlen H, Schilling T, Schmitt C, Neumann FJ. Increased risk of restenosis after placement of gold-coated stents: results of a randomized trial comparing gold-coated with uncoated steel stents in patients with coronary artery disease. Circulation 2000;101: [13] van der Giessen WJ, Lincoff AM, Schwartz RS, van Beusekom HM, Serruys PW, Holmes DR, Ellis SG, Topol EJ. Marked inflammatory sequelae to implantation of biodegradable and nonbiodegradable polymers in porcine coronary arteries. Circulation 1996;94: [14] Steinemann SG. Titanium: the material of choice? Periodontology 2000;17:7 21.
83 , LLC July 2010 Volume 22/Number 7 The Official Journal of the International Andreas Gruentzig Society Pooled Analysis of Trials Comparing Titanium-Nitride-Oxide-Coated Stents with Paclitaxel-Eluting Stents in Patients Undergoing Coronary Stenting...P.P. KARJALAINEN, ET AL.
84 Original Contribution Pooled Analysis of Trials Comparing Titanium-Nitride-Oxide- Coated Stents with Paclitaxel-Eluting Stents in Patients Undergoing Coronary Stenting Pasi P. Karjalainen, MD, PhD a, Fausto Biancari, MD, PhD b, Antti Ylitalo, MD, PhD a, Lorentz Raeber, MD c, Michael Billinger, MD c, Otto Hess, MD, PhD c, K. E. Juhani Airaksinen, MD, PhD d ABSTRACT: We performed a pooled analysis of three trials comparing titanium-nitride-oxide-coated bioactive stents (BAS) with paclitaxeleluting stents (PES) in 1,774 patients. All patients were followed for 12 months. The primary outcomes of interest were recurrent myocardial infarction (MI), death and target lesion revascularization (TLR). Secondary endpoints were stent thrombosis (ST) and major adverse cardiac events (MACE) including MI, death and TLR. There were 922 patients in the BAS group and 852 in the PES group. BAS significantly reduced the risk of recurrent MI (2.7% vs. 5.6%; risk ratio 0.50, 95% CI ; p = 0.004) and MACE (8.9% vs. 12.6%; risk ratio 0.71, 95% CI ; p = 0.02) during the 12 months of follow up. In contrast, the differences between BAS and PES were not statistically significant with respect to TLR (risk ratio 0.98, 95% CI ), death (risk ratio 0.96, 95% CI ) and definite ST (risk ratio 0.28, 95% CI ). In conclusion, the results of this analysis suggest that BAS is effective in reducing TLR and improves clinical outcomes by reducing MI and MACE compared with PES. J INVASIVE CARDIOL 2010;22: Standalone balloon angioplasty has been replaced with the use of coronary stents because of the near-elimination of abrupt closure and emergency coronary artery bypass graft surgery (CABG). 1,2 Drug-eluting stents (DES), including paclitaxeleluting stents (PES), have been shown to improve early and late outcomes as compared with bare-metal stents (BMS), predominantly as a result of a reduction in in-stent restenosis (ISR) and subsequent target lesion revascularization (TLR). 3,4 Recently, there have been concerns about the safety of DES, e.g., most notably late or very late stent thrombosis (ST). 5,6 On the other hand, stent coatings with compounds like titanium-nitrideoxide seem to decrease acute surface thrombogenicity 7 11 and reduce ISR when compared with conventional stainless-steel stents. 8 Results from several trials comparing titanium-nitrideoxide coated bioactive stent (BAS) and PES have been previously reported. 9,12 14 BAS have been shown to result in comparable From the a Department of Cardiology, Satakunta Central Hospital, Pori, Finland, b Division of Cardiothoracic and Vascular Surgery, Department of Surgery, Oulu, Finland, c Department of Cardiology, University Hospital Bern, Bern, Switzerland, and d Department of Medicine, Turku University Hospital, Turku, Finland. The authors report no conflicts of interest regarding the content herein. Manuscript submitted March 4, 2010, provisional acceptance given March 29, 2010, final version accepted April 12, Address for correspondence: Pasi P. Karjalainen, MD, PhD, Satakunta Central Hospital, Sairaalantie 3, Pori, 28500, Finland. pasi.karjalainen@satshp.fi clinical outcomes compared with PES in the real-world clinical practice involving high-risk patients and patients presenting with acute myocardial infarction (MI). Since these studies had insufficient power to assess the incidence of rare outcome events such us ST, we decided to perform a pooled analysis based on data from studies comparing BAS and PES. Methods Search strategy. The reference search was performed through PubMed, Science Direct, and the Cochrane Library up to November 2009 for studies comparing BAS versus PES in myocardial revascularization and reporting on at least 1-year outcomes. Tangential electronic exploration of related articles and hand searches of bibliographies and related journals were also performed. The key words employed in the search were: titanium, paclitaxel, eluting, titanium-nitride-oxide-coated, Titan, BAS, PES and stent. Studies evaluating any other coronary stents other than BAS and PES were not included in this study. Two review authors (PPK, FB) independently assessed the titles and abstracts of references identified by the search strategy according to the selection criteria. Full versions of the identified articles were obtained if, from the initial assessment, they appeared to satisfy the inclusion criteria. Full papers were checked independently to identify those that matched the inclusion criteria. Any disagreement was resolved by consensus. Reference lists of all retrieved studies were screened to identify further studies which were then retrieved. Studies were included if they met each of the following criteria: prospective studies with randomization as well as with control groups comparing BAS with PES in coronary revascularization reporting at least two pertinent clinical outcome endpoints among the following: death, MI, revascularization of the target vessel (CABG or repeat percutaneous coronary intervention [PCI] to treat ISR or a stenosis immediately adjacent to the stent). Clinical endpoints are reported as originally defined by the authors. Statistical analysis. This analysis was performed using Review Manager (RevMan) Version 5.0 for Windows (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008). The outcome endpoints were analyzed as dichotomous and continuous variables. Continuous outcome endpoints were expressed as weighted mean difference with a 95% confidence interval (95% CI). Dichotomous outcome endpoints were expressed as risk ratio (RR) with 95% CI. Heterogeneity was explored by calculating the 322 The Journal of Invasive Cardiology
85 Pooled-Analysis Comparing BES with PES in PCI Table 1. Characteristics of three prospective studies included in the present pooled analysis comparing titanium-nitride-oxide bioactive stents (BAS) and paclitaxeleluting stents (PES) in coronary revascularization. Age Bern Registry Pori Registry TITAX AMI Trial Male Bern Registry Pori Registry TITAX AMI Trial Diabetes Bern Registry Pori Registry TITAX AMI Trial Hypertension Bern Registry Pori Registry TITAX AMI Trial Hypercholesterolemia Bern Registry Pori Registry TITAX AMI Trial Smoking Bern Registry Pori Registry TITAX AMI Trial History of MI Bern Registry Pori Registry TITAX AMI Trial Previous PCI Bern Registry Pori Registry TITAX AMI Trial Previous CABG Bern Registry Pori Registry TITAX AMI Trial Acute STEMI Bern Registry Pori Registry TITAX AMI Trial Acute NSTEMI Bern Registry Pori Registry TITAX AMI Trial GP IIb/IIIa inhibitor Bern Registry Pori Registry TITAX AMI Trial BAS, 922 Patients (%) 67 ± ± ± (75.9%) (21.6%) (68.2%) (60.7%) (43.8%) (20.4%) (12.1%) (9.4%) (33.8%) (28.6%) (25.6%) PES, 852 Patients (%) 65 ± ± ± (74.6%) (20.1%) (56.7%) (64.0%) (37.1%) (16.7%) (14.6%) (8.5%) (34.2%) (27.3%) (18.5%) p-value, Risk Ratio (95% CI) 0.03, 1.73* ( ) 0.58, 1.02 ( ) 0.49, 1.07 ( ) < , 1.20 ( ) 0.77, 0.98 ( ) 0.005, 1.18 ( ) 0.07, 1.27 ( ) 0.82, 0.94 ( ) 0.46, 1.12 ( ) 0.82, 1.03 ( ) 0.28, 1.08 ( ) 0.10, 1.69 ( ) Data are mean (SD) or numbers (%). MI = myocardial infarction; PCI = percutaneous coronary intervention; CABG = coronary artery bypass grafting; STEMI = ST-elevation myocardial infarction; NSTEMI = non-st-elevation myocardial infarction; GP = glycoprotein. * Mean difference and 95% confidence interval I 2 statistic to quantify the degree of heterogeneity across the trials that could not be attributed to chance alone. If there was a significant heterogeneity (I 2 < 40%), a random-effect model was chosen, otherwise a fixed-effect model was used. Results We identified seven studies comparing BAS with either BMS or DES. Three of those studies compared exclusively BAS with BMS and were therefore excluded from the analysis. 8,15,16 The study by Grenadier et al has been excluded for the analysis because they reported unpublished results on the use of BAS compared with PES or sirolimus-eluting stents. 17 Altogether, three trials with 1,774 patients were included in the present analysis: two prospective, nonrandomized reports (Pori registry, Bern registry) and one prospective, randomized multicenter trial (TITAX-AMI). 9,13,18 Baseline clinical characteristics of these reports are summarized in Table 1. A total of 922 patients (Pori, n = 201; Bern, n = 507; TITAX- AMI, n = 214) were treated with BAS, and 852 patients (Pori, n = 204; Bern, n = 437; TITAX- AMI, n = 211) with PES. The patients in the BAS group were older and were more likely to undergo treatment for hypertension. Lesion and procedural characteristics are listed in Table 2. Lesion and stent lengths, as well as diameters, were comparable between the study groups. All trials reported results from 12-month clinical follow up. The mean length of clopidogrel therapy in BAS and PES groups was 7.7 and 8.2 months in the Pori registry and 7.6 and 10.0 months in the TITAX-AMI trial, respectively. In the Bern registry, clopidogrel was prescribed for 1 month in the BAS group and for 12 months in the PES group. Figure 1 shows forest plots on the absolute rate of MI and MACE during the 12-month clinical follow up in the BAS versus PES groups, with the risk ratio for each of these trials. Across the trials, no evidence of heterogeneity was observed (I 2 = 0%). With respect to recurrent MI, the use of BAS was associated with a risk ratio of 0.50 (95% CI ; p = 0.004) compared with PES. Similarly, BAS were associated with a risk ratio of 0.71 (95% CI ; p = 0.02) for MACE. Twelve-month probability of MACE was 8.9% in the BAS group and 12.6% in the PES group (p = 0.014). The number of patients who suffered TLR, death and definite ST are shown in Figure 2. Overall, the use of BAS was associated with a Vol. 22, No. 7, July
86 KARJALAINEN, et al. Table 2. Procedural characteristics of three prospective studies included in the present pooled analysis comparing titanium-nitride-oxide bioactive stents (BAS) and paclitaxel-eluting stents (PES) in coronary revascularization. Target vessel LAD Bern Registry Pori Registry TITAX AMI Trial LCX Bern Registry Pori Registry TITAX AMI Trial RCA Bern Registry Pori Registry TITAX AMI Trial Left main Bern Registry Pori Registry TITAX AMI Trial SVG Bern Registry Pori Registry TITAX AMI Trial RVD Bern Registry Pori Registry TITAX AMI Trial Lesion length Bern Registry Pori Registry TITAX AMI Trial Stent diameter Bern Registry Pori Registry TITAX AMI Trial Stent length Bern Registry Pori Registry TITAX AMI Trial BAS 1,148 Stents (%) 473 (41.2%) (21.9%) (32.5%) (1.1%) (3.0%) ± ± ± ± ± ± ± ± ± ± ± ± 6.4 PES 1,061 Stents (%) 480 (45.2%) (19.0%) (30.3%) (1.8%) (3.2%) ± ± ± ± ± ± ± ± ± ± ± ± 7.2 risk ratio of 0.98 (95% CI ; p = 0.90) for TLR, 0.96 (95% CI ; p = 0.85) for death, and 0.28 (95% CI ; p = 0.13) for definite ST when compared with PES. Discussion To our knowledge, this is the first pooled analysis comparing BAS with PES in patients undergoing PCI. With respect to stent efficacy as measured by the device-specific, ischemia-driven TLR, we found no significant difference between patients treated with either BAS or PES. On the other hand, the safety data of the present analysis showed that treatment with BAS was associated with a 52% decrease in the risk of MI and a 29% decrease in MACE compared with PES. However, no significant difference was found in the risk of definite ST or death between the study groups. Previous studies and meta-analysis have demonstrated a drastic reduction of neointimal hyperplasia and subsequent TLR with DES when compared with BMS in patients with various clinical and angiographic characteristics. 3 5,19 The data from the present analysis is intriguing because it includes MI patients (TITAX-AMI) and all-comers (Pori, Bern), and therefore this cohort of patients reflects our everyday clinical practice. Although the present pooled analysis shows imprecise estimates of TLR, the findings are of a similar magnitude as presented with the use of DES in previous randomized trials. 5,19 21 Interestingly, the rate of TLR was moderately low in both BAS and PES groups. The safety of DES has been scrutinized in depth and there have been concerns that some patients develop ST, a life-threatening complication, unusually late after stent implantation. 5,6 However, in randomized trials and large-scale registries, mortality and MI rates were found to be similar or even lower with use of DES. 5,22 In our analysis, the incidence of definite ST was comparable among patients treated with BAS or PES (0.7% vs. 2.2%), which substantiates the safety of these devices. Nevertheless, the MI rate was found to be significantly higher with the use of PES compared with BAS. The literature is rich with data regarding the advantages of titanium (-oxides) used for implantable medical devices. 23,24 In our analysis, the incidence of MI and MACE was lower in patients receiving BAS. Titanium-nitrideoxide coating may contribute to these findings, since in vitro examinations showed that titanium oxides were able to inhibit platelet aggregation and fibrin growth. 7 In addition, a recent report demonstrated that titanium-nitrideoxide was able to promote and accelerate endothelial cell growth when compared with other materials such as stainless steel or nitinol, supporting the hypothesis that a stent with titanium-nitride-oxide coating could achieve earlier reendothelialization compared with BMS or DES. 25 Our analysis included trials with follow up of 12 months. Recently, longer-term follow-up data were published from the Pori registry (36 months) 12 and the TITAX-AMI trial (24 months). 14 Both of these trials exhibited an increase in ST, cardiac death and MI in the PES group between 12- to 24-month follow up, which was mainly seen after clopidogrel discontinuation. An alternative p-value, Risk Ratio (95% CI) 0.08, 0.92 ( ) 0.31, 1.13 ( ) 0.35, 1.06 ( ) 0.24, 0.67 ( ) 0.51, 0.95 ( ) 0.51, *-0.01 ( ) 0.05, *-0.45 ( ) 0.71, *-0.02 ( ) 0.40, *-1.78 ( ) Data are mean (SD) or numbers (%) LAD = left anterior descending artery; LCX = left circumflex artery; RCA = right coronary artery; SVG = saphenous vein graft; RVD = reference vessel diameter * Mean difference and 95% confidence interval 324 The Journal of Invasive Cardiology
87 Pooled-Analysis Comparing BES with PES in PCI MACE Favors BAS Favors PES Myocardial Infarction Favors BAS Favors PES Figure1. Risk of MACE and myocardial infarction during 12-month clinical follow up in the BAS versus PES groups. MACE = major adverse coronary events. BAS = bioactive stents; PES = paclitaxel-eluting stents. explanation for the lower incidence of late ST and MIs with BAS is the stent coating and its ability to enhance vascular healing at the site of stent implantation. In addition, polymers used on current DES may trigger an immune reaction and induce chronic inflammation, explaining some of the late events after PES use. Study limitations. The findings of our pooled analysis should be interpreted with caution. Regardless of the benefit of a pooled analysis to increase the statistical power, the rare occurrence of adverse events might limit the capacity of our analysis to detect differences between the treatment strategies. One limitation of the present study is that only three trials were available for the analysis. Two of them were prospective registries, hence our analysis is liable to reflect a selection bias. Conclusions In conclusion, we observed comparable efficacy with BAS and PES in patients undergoing PCI during 12 months of clinical follow up. On the other hand, the use of BAS reduced the risk of recurrent MI and MACE compared with PES. References 1. De Muinck ED, den Heijer P, van Dijk RB, et al. Autoperfusion balloon versus stent for acute or threatened closure during percutaneous transluminal coronary angioplasty. Am J Cardiol 1994;74: Altmann DB, Racz M, Battleman DS, et al. Reduction in angioplasty complications after the introduction of coronary stents: Results from a consecutive series of 2242 patients. Am Heart J 1996;132: Moses JW, Leon MB, Popma JJ, et al. Sirolimus eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med 2003;349: Stone GW, Ellis SG, Cox DA, et al. One-year clinical results with the slow-release, polymer-based, paclitaxel-eluting TAXUS stent: The TAXUS-IV trial. Circulation 2004;109: Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus- and paclitaxeleluting coronary stents. N Engl J Med 2007;356: Mauri L, Hsieh W, Massaro JM, et al. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med 2007;356: Zhang F, Zheng Z, Chen Y, et al. In vivo investigation of blood compatibility of titanium oxide films. J Biomed Mater Res 1998;42: Windecker S, Simon R, Lins M, et al. Randomized comparison of a titanium-nitride oxide coated stent with a stainless steel stent for coronary revascularization. The TINOX trial. Circulation 2005;111: Karjalainen PP, Ylitalo A, Airaksinen KEJ. Titanium and nitride oxide coated stents and paclitaxel eluting stents for coronary revascularization in an unselected population. J Invasive Cardiol 2006;18: Karjalainen P, Ylitalo A, Airaksinen KEJ. Real world experience with TITAN stent: A 9-month follow-up report from the Titan PORI registry. Eurointerv 2006;2: Mosseri M, Miller H, Tamari I, et al. The Titanium-NO Stent: Results of a multicenter registry. Eurointerv 2006;2: Karjalainen PP, Annala AP, Ylitalo A, et al. Long-term clinical outcome with titaniumnitride oxide-coated stents and paclitaxel-eluting stents for coronary revascularization in an unselected population. Int J Cardiol 2009; Apr 27. (Epub ahead of print). 13. Karjalainen PP, Ylitalo A, Niemelä M, et al. Titanium-nitride-oxide coated stents versus paclitaxel eluting stents in acute myocardial infarction: A 12-months follow-up report from the TITAX AMI trial. Eurointerv 2008;4: Karjalainen PP, Ylitalo A, Niemelä M, et al. Two-year follow-up after percutaneous coronary intervention with titanium-nitride-oxide-coated stents versus paclitaxeleluting stents in acute myocardial infarction. Ann Med 2009;41: Sansa M, Cernigliaro C, Bongo SA, et al. Titanium-NO coated stent versus BMS in ACS: Early and late thrombosis and restenosis. TCT 2006 (W181). 16. Sant Anna FM, Batista LA, Brito M, et al. Randomized comparison of percutaneous coronary intervention with titanium-nitride-oxide-coated stents versus stainless steel stents in patients with coronary artery disease: RIO Trial. Revista Cardiologia Invasiva 2009;17: Vol. 22, No. 7, July
88 KARJALAINEN, et al. TARGET LESION REVASCULARIZATION Favors BAS Favors PES ALL-CAUSE DEATH Favors BAS Favors PES DEFINITE STENT THROMBOSIS Favors BAS Favors PES Figure 2. Risk of target lesion revascularization, cardiac death and definite stent thrombosis during 12-month clinical follow up in the BAS versus PES groups. BAS = bioactive stents; PES = paclitaxel-eluting stents. 17. Grenadier E, Mosseri M, Lotan C, et al. Comparative prospective non randomized analysis of BAS versus DES in true small vessel stenting. Taiwan Transcatheter Therapeutics (TTT), Lauterburg A, Loetscher S, Raeber L, et al. Clinical outcome following PCI using titanium nitride oxide coated stents in complex patients, compared with Cypher- and Taxus-stents in a clinical registry. TCT Submitted for publication Kirtane AJ, Gupta A, Iyengar S, et al. Safety and efficacy of drug-eluting and bare metal stents: Comprehensive meta-analysis of randomized trials and observational studies. Circulation 2009;119: Kastrati A, Dibra A, Spaulding C, et al. Meta-analysis of randomized trials on drugeluting stents vs. bare-metal stents in patients with acute myocardial infarction. Eur Heart J 2007;28: Stone GW, Lansky AJ, Pocock SJ, et al; HORIZONS-AMI Trial Investigators. Paclitaxel-eluting stents versus bare-metal stents in acute myocardial infarction. N Engl J Med 2009;360: Nienaber CA, Akin I, Schneider S, et al. Clinical outcomes after sirolimus-eluting, paclitaxel eluting, and bare metal stents (from the first phase of the prospective multicenter German DES Registry). Am J Cardiol 2009;104: Steineman SG. Metal implants and surface reactions. Injury 1996;27:SC Gotman I. Characteristics of metal used in implants. J Endourol 1997;11: Yeh HI, Lu SK, Tian TY, et al. Comparison of endothelial cells grown on different stent materials. J Biomed Mater Res A 2006;76: The Journal of Invasive Cardiology
89
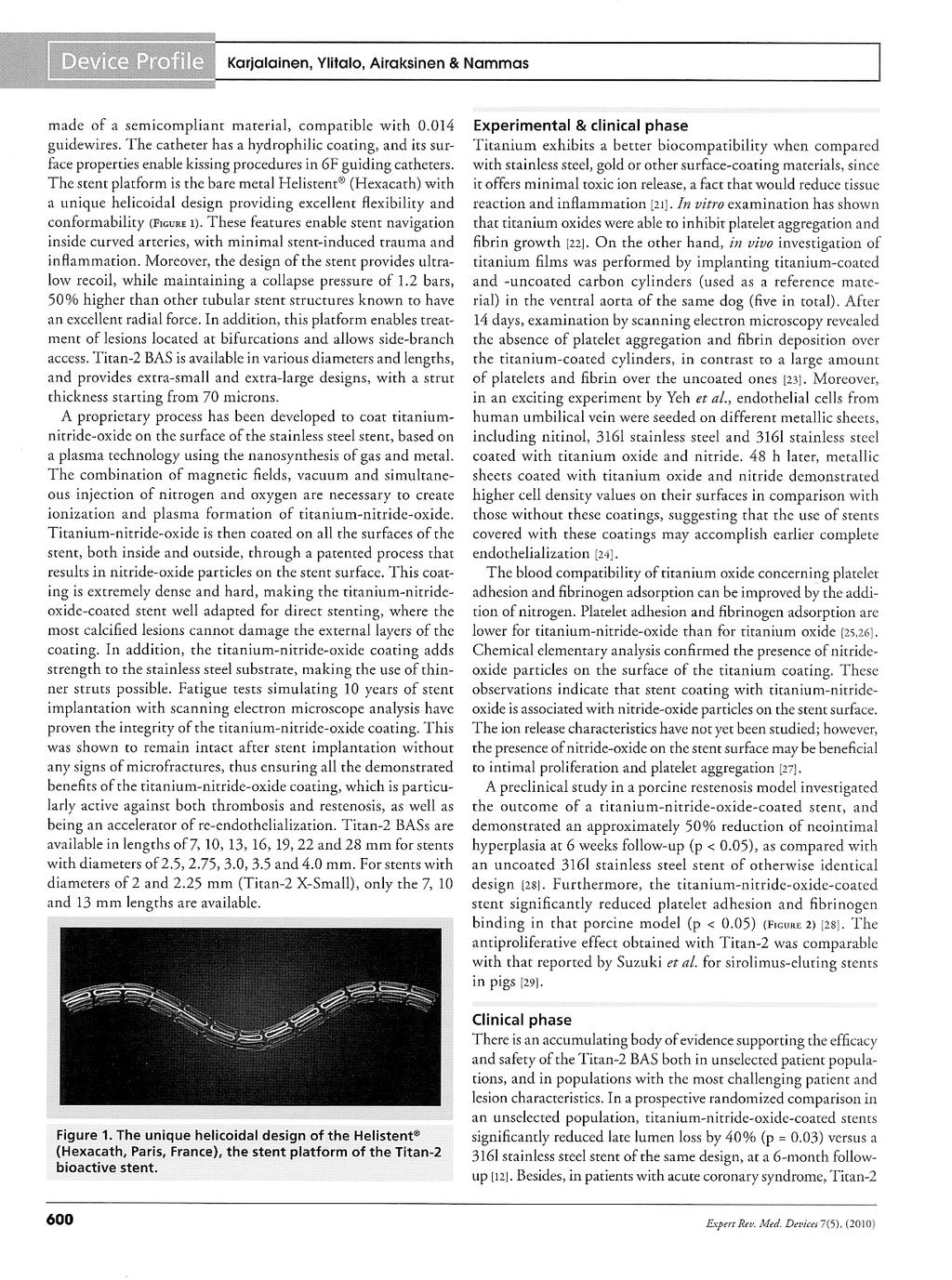
90
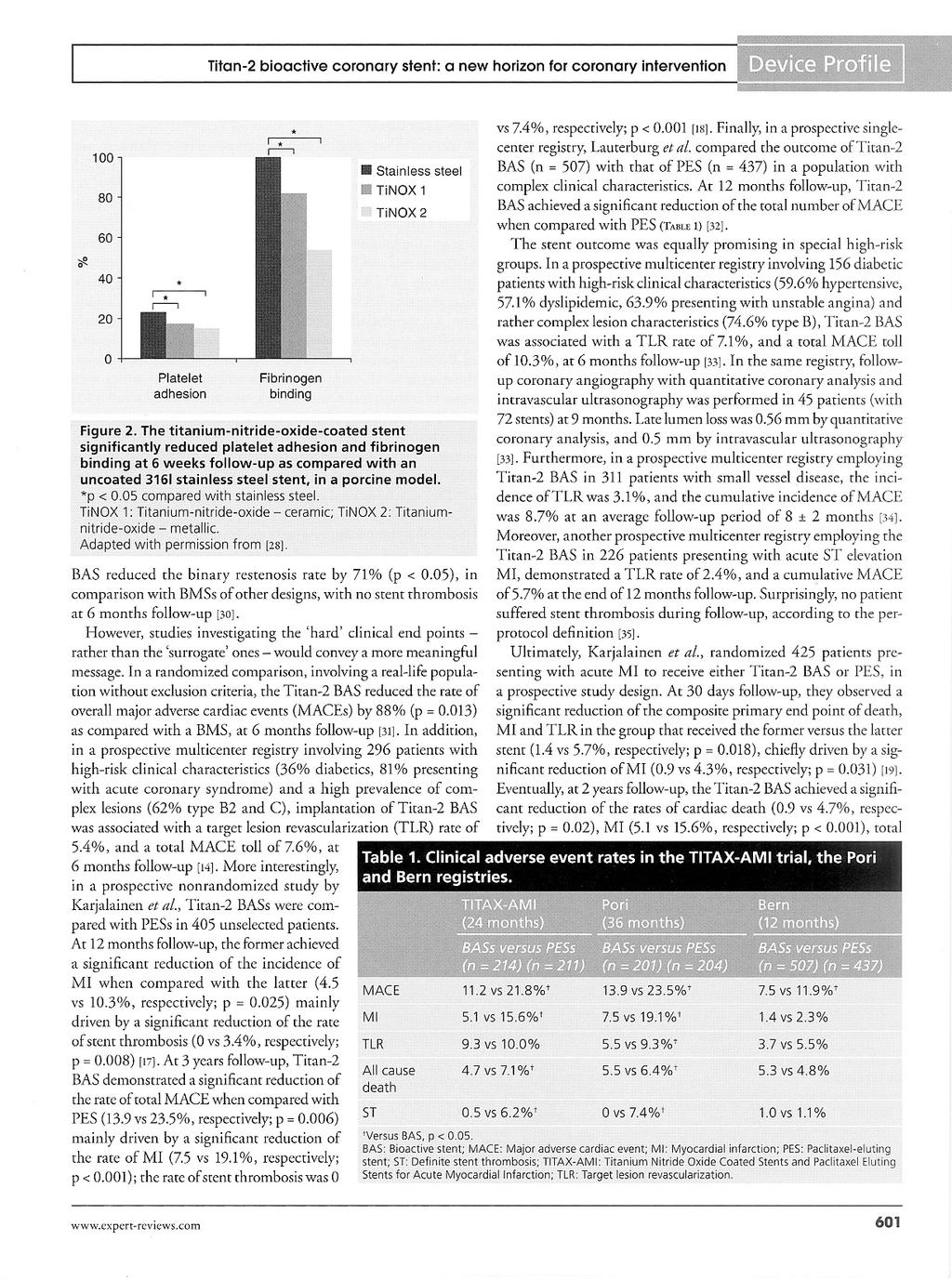
91

92
For Personal Use. Copyright HMP 2012
 Original Contribution Gender-Based Analysis of the 3-Year Outcome of Bioactive Stents Versus Paclitaxel-Eluting Stents in Patients with Acute Myocardial Infarction: An Insight from the TITAX-AMI Trial
Original Contribution Gender-Based Analysis of the 3-Year Outcome of Bioactive Stents Versus Paclitaxel-Eluting Stents in Patients with Acute Myocardial Infarction: An Insight from the TITAX-AMI Trial
Stent strut coverage of titanium-nitride-oxide coated stent compared to paclitaxel-eluting stent in acute myocardial infarction: TITAX-OCT study
 DOI 10.1007/s10554-012-0032-6 ORIGINAL PAPER Stent strut coverage of titanium-nitride-oxide coated stent compared to paclitaxel-eluting stent in acute myocardial infarction: TITAX-OCT study Tuomas Lehtinen
DOI 10.1007/s10554-012-0032-6 ORIGINAL PAPER Stent strut coverage of titanium-nitride-oxide coated stent compared to paclitaxel-eluting stent in acute myocardial infarction: TITAX-OCT study Tuomas Lehtinen
The titanium nitride oxide stent an alternative to DES. Adam de Belder MD FRCP Sussex Cardiac Centre BSUH on behalf of Hexacath
 The titanium nitride oxide stent an alternative to DES Adam de Belder MD FRCP Sussex Cardiac Centre BSUH on behalf of Hexacath Advanced Angioplasty 2008 Declaration of interest I have received an honorarium
The titanium nitride oxide stent an alternative to DES Adam de Belder MD FRCP Sussex Cardiac Centre BSUH on behalf of Hexacath Advanced Angioplasty 2008 Declaration of interest I have received an honorarium
Titan versus TAXUS Stents at 1 Year Clinical Outcome
 Original Article Titan versus TAXUS Stents at 1 Year Clinical Outcome Acta Cardiol Sin 2011;27:94 100 Interventional Cardiology One-Year Follow-Up after Percutaneous Coronary Intervention with Titanium-Nitride-Oxide-Coated
Original Article Titan versus TAXUS Stents at 1 Year Clinical Outcome Acta Cardiol Sin 2011;27:94 100 Interventional Cardiology One-Year Follow-Up after Percutaneous Coronary Intervention with Titanium-Nitride-Oxide-Coated
Titanium and Nitride Oxide-Coated Stents and Paclitaxel-Eluting Stents for Coronary Revascularization in an Unselected Population
 Original Contribution Titanium and Nitride Oxide-Coated Stents and Paclitaxel-Eluting Stents for Coronary Revascularization in an Unselected Population Pasi P. Karjalainen, MD, Antti Ylitalo, MD, PhD,
Original Contribution Titanium and Nitride Oxide-Coated Stents and Paclitaxel-Eluting Stents for Coronary Revascularization in an Unselected Population Pasi P. Karjalainen, MD, Antti Ylitalo, MD, PhD,
Maintenance of Long-Term Clinical Benefit With Sirolimus-Eluting Stents in Patients With ST-Segment Elevation Myocardial Infarction
 Journal of the American College of Cardiology Vol. 55, No. 8, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.09.046
Journal of the American College of Cardiology Vol. 55, No. 8, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.09.046
INDEX 1 INTRODUCTION DEVICE DESCRIPTION CLINICAL PROGRAM FIRST-IN-MAN CLINICAL INVESTIGATION OF THE AMAZONIA SIR STENT...
 May 2017 INDEX 1 INTRODUCTION... 2 2 DEVICE DESCRIPTION... 3 ANTI-PROLIFERATIVE DRUG - SIROLIMUS... 3 BIODEGRADABLE POLYMERS... 3 SIROLIMUS CONTROLLED ELUTION... 4 STENT PLATFORM... 4 3 CLINICAL PROGRAM...
May 2017 INDEX 1 INTRODUCTION... 2 2 DEVICE DESCRIPTION... 3 ANTI-PROLIFERATIVE DRUG - SIROLIMUS... 3 BIODEGRADABLE POLYMERS... 3 SIROLIMUS CONTROLLED ELUTION... 4 STENT PLATFORM... 4 3 CLINICAL PROGRAM...
A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI
 HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
HORIZONS-AMI: A Large Prospective Randomized Trial of DES vs BMS in Patients with STEMI Gregg W. Stone MD Columbia University Medical Center Cardiovascular Research Foundation Disclosures Gregg W. Stone
Clinical Investigations
 Clinical Investigations Clinical Outcomes for Single Stent and Multiple Stents in Contemporary Practice Qiao Shu Bin, MD; Liu Sheng Wen, MD; Xu Bo, BS; Chen Jue, MD; Liu Hai Bo, MD; Yang Yue Jin, MD; Chen
Clinical Investigations Clinical Outcomes for Single Stent and Multiple Stents in Contemporary Practice Qiao Shu Bin, MD; Liu Sheng Wen, MD; Xu Bo, BS; Chen Jue, MD; Liu Hai Bo, MD; Yang Yue Jin, MD; Chen
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis Alaide Chieffo
 Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Drug Eluting Stents Sometimes Fail ESC Stockholm 29 Set 2010 Stent Thrombosis 11.45-12.07 Alaide Chieffo San Raffaele Scientific Institute, Milan, Italy Historical Perspective 25 20 15 10 5 0 Serruys 1991
Béla MERKELY MD, PhD, DSc, FESC. Stent thrombosis: patophysiology, predisposing factors, definition, classification, prevention and treatment
 Semmelweis University Heart Center Budapest, Hungary Béla MERKELY MD, PhD, DSc, FESC Stent thrombosis: patophysiology, predisposing factors, definition, classification, prevention and treatment 10th Interventional
Semmelweis University Heart Center Budapest, Hungary Béla MERKELY MD, PhD, DSc, FESC Stent thrombosis: patophysiology, predisposing factors, definition, classification, prevention and treatment 10th Interventional
TIDES-ACS trial. Comparison of TItanium-nitride-oxide coated bioactive stent to the Drug (everolimus)-eluting Stent in Acute Coronary Syndrome
-eluting Stent in Acute Coronary Syndrome") TIDES-ACS trial Comparison of TItanium-nitride-oxide coated bioactive stent to the Drug (everolimus)-eluting Stent in Acute Coronary Syndrome Pasi P Karjalainen Potential conflicts of interest Speaker's
TIDES-ACS trial Comparison of TItanium-nitride-oxide coated bioactive stent to the Drug (everolimus)-eluting Stent in Acute Coronary Syndrome Pasi P Karjalainen Potential conflicts of interest Speaker's
Nine-year clinical outcomes of drug-eluting stents vs. bare metal stents for large coronary vessel lesions
 Journal of Geriatric Cardiology (2017) 14: 35 41 2017 JGC All rights reserved; www.jgc301.com Research Article Open Access Nine-year clinical outcomes of drug-eluting stents vs. bare metal stents for large
Journal of Geriatric Cardiology (2017) 14: 35 41 2017 JGC All rights reserved; www.jgc301.com Research Article Open Access Nine-year clinical outcomes of drug-eluting stents vs. bare metal stents for large
1. Whether the risks of stent thrombosis (ST) and major adverse cardiovascular and cerebrovascular events (MACCE) differ from BMS and DES
 and major adverse cardiovascular and cerebrovascular events (MACCE) differ from BMS and DES") 1 Comparison of Ischemic and Bleeding Events After Drug- Eluting Stents or Bare Metal Stents in Subjects Receiving Dual Antiplatelet Therapy: Results from the Randomized Dual Antiplatelet Therapy (DAPT)
1 Comparison of Ischemic and Bleeding Events After Drug- Eluting Stents or Bare Metal Stents in Subjects Receiving Dual Antiplatelet Therapy: Results from the Randomized Dual Antiplatelet Therapy (DAPT)
PROMUS Element Experience In AMC
 Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Promus Element Luncheon Symposium: PROMUS Element Experience In AMC Jung-Min Ahn, MD. University of Ulsan College of Medicine, Heart Institute, Asan Medical Center, Seoul, Korea PROMUS Element Clinical
Abstract Background: Methods: Results: Conclusions:
 Two-Year Clinical and Angiographic Outcomes of Overlapping Sirolimusversus Paclitaxel- Eluting Stents in the Treatment of Diffuse Long Coronary Lesions Kang-Yin Chen 1,2, Seung-Woon Rha 1, Yong-Jian Li
Two-Year Clinical and Angiographic Outcomes of Overlapping Sirolimusversus Paclitaxel- Eluting Stents in the Treatment of Diffuse Long Coronary Lesions Kang-Yin Chen 1,2, Seung-Woon Rha 1, Yong-Jian Li
Journal of the American College of Cardiology Vol. 47, No. 7, by the American College of Cardiology Foundation ISSN /06/$32.
 Journal of the American College of Cardiology Vol. 47, No. 7, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.05.102
Journal of the American College of Cardiology Vol. 47, No. 7, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2005.05.102
ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions
 Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Julinda Mehilli, MD Deutsches Herzzentrum Technische Universität Munich Germany ISAR-LEFT MAIN: A Randomized Clinical Trial on Drug-Eluting Stents for Unprotected Left Main Lesions Background Left main
Lessons learned From The National PCI Registry
 Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
Lessons learned From The National PCI Registry w a v e On Behalf of The Publication Committee of the National PCI Registry Objectives & Anticipated Achievements To determine the epidemiology of patients
SKG Congress, 2015 EVOLVE II. Stephan Windecker
 SKG Congress, 2015 EVOLVE II Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland BIODEGRADABLE POLYMER DES Stefanini,
SKG Congress, 2015 EVOLVE II Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland BIODEGRADABLE POLYMER DES Stefanini,
Bern-Rotterdam Cohort Study
 Bern-Rotterdam Cohort Study Newer generation everolimus-eluting stents eliminate the risk of very late stent thrombosis compared with early generation sirolimus-eluting and paclitaxel-eluting stents Lorenz
Bern-Rotterdam Cohort Study Newer generation everolimus-eluting stents eliminate the risk of very late stent thrombosis compared with early generation sirolimus-eluting and paclitaxel-eluting stents Lorenz
Adults With Diagnosed Diabetes
 Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Adults With Diagnosed Diabetes 1990 No data available Less than 4% 4%-6% Above 6% Mokdad AH, et al. Diabetes Care. 2000;23(9):1278-1283. Adults With Diagnosed Diabetes 2000 4%-6% Above 6% Mokdad AH, et
Paclitaxel-Eluting Coronary Stents in Patients With Diabetes Mellitus
 Journal of the American College of Cardiology Vol. 51, No. 7, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.10.035
Journal of the American College of Cardiology Vol. 51, No. 7, 2008 2008 by the American College of Cardiology Foundation ISSN 0735-1097/08/$34.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.10.035
Stent Thrombosis in Bifurcation Stenting
 Summit TCT Asia Pacific 2009 Stent Thrombosis in Bifurcation Stenting Associate Professor Tan Huay Cheem MBBS, M Med(Int Med), MRCP, FRCP(UK), FAMS, FACC, FSCAI Director, National University Heart Centre,
Summit TCT Asia Pacific 2009 Stent Thrombosis in Bifurcation Stenting Associate Professor Tan Huay Cheem MBBS, M Med(Int Med), MRCP, FRCP(UK), FAMS, FACC, FSCAI Director, National University Heart Centre,
Clinical Study Age Differences in Long Term Outcomes of Coronary Patients Treated with Drug Eluting Stents at a Tertiary Medical Center
 Aging Research Volume 2013, Article ID 471026, 4 pages http://dx.doi.org/10.1155/2013/471026 Clinical Study Age Differences in Long Term Outcomes of Coronary Patients Treated with Drug Eluting Stents at
Aging Research Volume 2013, Article ID 471026, 4 pages http://dx.doi.org/10.1155/2013/471026 Clinical Study Age Differences in Long Term Outcomes of Coronary Patients Treated with Drug Eluting Stents at
The PASEO (PaclitAxel or Sirolimus-Eluting Stent Versus Bare Metal Stent in Primary Angioplasty) Randomized Trial
 Randomized Trial") JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 6, 2009 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/09/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2009.03.012 The PASEO
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 6, 2009 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/09/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2009.03.012 The PASEO
DES in Diabetic Patients
 DES in Diabetic Patients Charles Chan, M.D., FACC Gleneagles Hospital Singapore TCT ASIA PACIFIC 2007 Why do diabetics have worse outcome after PCI? More extensive atherosclerosis and diffuse disease Increase
DES in Diabetic Patients Charles Chan, M.D., FACC Gleneagles Hospital Singapore TCT ASIA PACIFIC 2007 Why do diabetics have worse outcome after PCI? More extensive atherosclerosis and diffuse disease Increase
Stent Thrombosis: Patient, Procedural, and Stent Factors. Eugene Mc Fadden Cork, Ireland
 Stent Thrombosis: Patient, Procedural, and Stent Factors Eugene Mc Fadden Cork, Ireland Definitions Early 1 yr TAXUS >6months CYPHER Incidence and Timing BMS Registry data
Stent Thrombosis: Patient, Procedural, and Stent Factors Eugene Mc Fadden Cork, Ireland Definitions Early 1 yr TAXUS >6months CYPHER Incidence and Timing BMS Registry data
Paclitaxel-Eluting versus Uncoated Stents in Primary Percutaneous Coronary Intervention
 original article Paclitaxel-Eluting versus Uncoated Stents in Primary Percutaneous Coronary Intervention Gerrit J. Laarman, M.D., Ph.D., Maarten J. Suttorp, M.D., Ph.D., Maurits T. Dirksen, M.D., Loek
original article Paclitaxel-Eluting versus Uncoated Stents in Primary Percutaneous Coronary Intervention Gerrit J. Laarman, M.D., Ph.D., Maarten J. Suttorp, M.D., Ph.D., Maurits T. Dirksen, M.D., Loek
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company
 SMC No. (638/10) The Medicines Company") bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
bivalirudin 250mg powder for concentrate for solution for injection or infusion (Angiox) SMC No. (638/10) The Medicines Company 06 August 2010 The Scottish Medicines Consortium (SMC) has completed its
MULTIcentre evaluation of Single high-dose. acute myocardial infarction study
 MULTIcentre evaluation of Single high-dose Tirofiban bolus TiRofiban vs. versus with sirolimus eluting stent or barein metal stent in during primary PCI STEMI acute myocardial infarction study M. Valgimigli,
MULTIcentre evaluation of Single high-dose Tirofiban bolus TiRofiban vs. versus with sirolimus eluting stent or barein metal stent in during primary PCI STEMI acute myocardial infarction study M. Valgimigli,
2-Year Follow-Up of a Randomized Controlled Trial of Everolimus- and Paclitaxel-Eluting Stents for Coronary Revascularization in Daily Practice
 Journal of the American College of Cardiology Vol. 58, No. 1, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.02.023
Journal of the American College of Cardiology Vol. 58, No. 1, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.02.023
SeQuent Please World Wide Registry
 Journal of the American College of Cardiology Vol. 6, No. 18, 212 212 by the American College of Cardiology Foundation ISSN 735-197/$36. Published by Elsevier Inc. http://dx.doi.org/1.116/j.jacc.212.7.4
Journal of the American College of Cardiology Vol. 6, No. 18, 212 212 by the American College of Cardiology Foundation ISSN 735-197/$36. Published by Elsevier Inc. http://dx.doi.org/1.116/j.jacc.212.7.4
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation?
 What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
What is the Optimal Triple Anti-platelet Therapy Duration in Patients with Acute Myocardial Infarction Undergoing Drug-eluting Stents Implantation? Keun-Ho Park, Myung Ho Jeong, Min Goo Lee, Jum Suk Ko,
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion
 Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol
Periprocedural Myocardial Infarction and Clinical Outcome In Bifurcation Lesion Hyeon-Cheol Gwon Cardiac and Vascular Center Samsung Medical Center Sungkyunkwan University School of Medicine Dr. Hyeon-Cheol
Clinical Study Everolimus-Eluting versus Paclitaxel-Eluting Stents in Percutaneous Coronary Intervention: Meta-Analysis of Randomized Trials
 Thrombosis Volume 2012, Article ID 126369, 8 pages doi:10.1155/2012/126369 Clinical Study Everolimus-Eluting versus Paclitaxel-Eluting Stents in Percutaneous Coronary Intervention: Meta-Analysis of Randomized
Thrombosis Volume 2012, Article ID 126369, 8 pages doi:10.1155/2012/126369 Clinical Study Everolimus-Eluting versus Paclitaxel-Eluting Stents in Percutaneous Coronary Intervention: Meta-Analysis of Randomized
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Case Report Primary Percutaneous Coronary Intervention in an Acute Myocardial Infarction Due to the Occlusion of the Left Main Coronary Artery
 Hellenic J Cardiol 48: 368-372, 2007 Case Report Primary Percutaneous Coronary Intervention in an Acute Myocardial Infarction Due to the Occlusion of the Left Main Coronary Artery STELIOS PARASKEVAIDIS,
Hellenic J Cardiol 48: 368-372, 2007 Case Report Primary Percutaneous Coronary Intervention in an Acute Myocardial Infarction Due to the Occlusion of the Left Main Coronary Artery STELIOS PARASKEVAIDIS,
Coronary Stent Choice in Patients With Diabetes Mellitus
 Rome Cardiology Forum 2014 Coronary Stent Choice in Patients With Diabetes Mellitus Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University
Rome Cardiology Forum 2014 Coronary Stent Choice in Patients With Diabetes Mellitus Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University
Coronary drug-eluting stents (DES) were first approved
 were first approved") Thrombosis in Coronary Drug-Eluting Stents Report From the Meeting of the Circulatory System Medical Devices Advisory Panel of the Food and Drug Administration Center for Devices and Radiologic Health,
Thrombosis in Coronary Drug-Eluting Stents Report From the Meeting of the Circulatory System Medical Devices Advisory Panel of the Food and Drug Administration Center for Devices and Radiologic Health,
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial
 Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
Effect of Intravascular Ultrasound- Guided vs. Angiography-Guided Everolimus-Eluting Stent Implantation: the IVUS-XPL Randomized Clinical Trial Myeong-Ki Hong, MD. PhD on behalf of the IVUS-XPL trial investigators
PCI for In-Stent Restenosis. CardioVascular Research Foundation
 PCI for In-Stent Restenosis ISR of BMS Patterns of In-Stent Restenosis Pattern I : Focal Type IA: Articulation / Gap Type IB: Marginal Type IC: Focal body Type ID: Multifocal Pattern II,III,IV : Diffuse
PCI for In-Stent Restenosis ISR of BMS Patterns of In-Stent Restenosis Pattern I : Focal Type IA: Articulation / Gap Type IB: Marginal Type IC: Focal body Type ID: Multifocal Pattern II,III,IV : Diffuse
COMPARE Trial Elvin Kedhi Maasstad Ziekenhuis Rotterdam The Netherlands
 COMPARE Trial Elvin Kedhi Maasstad Ziekenhuis Rotterdam The Netherlands TCTAP 2010 Seoul, Korea Disclosures Research Foundation of the Cardiology Department has received unrestricted research grants from:
COMPARE Trial Elvin Kedhi Maasstad Ziekenhuis Rotterdam The Netherlands TCTAP 2010 Seoul, Korea Disclosures Research Foundation of the Cardiology Department has received unrestricted research grants from:
Stent Thrombosis in Randomized Clinical Trials of Drug-Eluting Stents
 T h e n e w e ng l a nd j o u r na l o f m e dic i n e original article Thrombosis in Randomized Clinical Trials of Drug-Eluting s Laura Mauri, M.D., Wen-hua Hsieh, Ph.D., Joseph M. Massaro, Ph.D., Kalon
T h e n e w e ng l a nd j o u r na l o f m e dic i n e original article Thrombosis in Randomized Clinical Trials of Drug-Eluting s Laura Mauri, M.D., Wen-hua Hsieh, Ph.D., Joseph M. Massaro, Ph.D., Kalon
Outcomes With the Paclitaxel-Eluting Stent in Patients With Acute Coronary Syndromes Analysis From the TAXUS-IV Trial
 Journal of the American College of Cardiology Vol. 45, No. 8, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.10.074
Journal of the American College of Cardiology Vol. 45, No. 8, 2005 2005 by the American College of Cardiology Foundation ISSN 0735-1097/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2004.10.074
Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents
 Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents Prof. Dr. med. Julinda Mehilli Medizinische Klinik und Poliklinik I Klinikum der Universität München Campus Großhadern Key Factors
Komplexe Koronarintervention heute: Von Syntax zu bioresorbierbaren Stents Prof. Dr. med. Julinda Mehilli Medizinische Klinik und Poliklinik I Klinikum der Universität München Campus Großhadern Key Factors
One-Year Clinical Outcomes after Sirolimus-Eluting Coronary Stent Implantation for Acute Myocardial Infarction in the Worldwide e-select Registry
 C 2012, Wiley Periodicals, Inc. DOI: 10.1111/j.1540-8183.2011.00705.x One-Year Clinical Outcomes after Sirolimus-Eluting Coronary Stent Implantation for Acute Myocardial Infarction in the Worldwide e-select
C 2012, Wiley Periodicals, Inc. DOI: 10.1111/j.1540-8183.2011.00705.x One-Year Clinical Outcomes after Sirolimus-Eluting Coronary Stent Implantation for Acute Myocardial Infarction in the Worldwide e-select
Influence of Planned Six-Month Follow-Up Angiography on Late Outcome After Percutaneous Coronary Intervention A Randomized Study
 Journal of the American College of Cardiology Vol. 38, No. 4, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01476-0 Influence
Journal of the American College of Cardiology Vol. 38, No. 4, 2001 2001 by the American College of Cardiology ISSN 0735-1097/01/$20.00 Published by Elsevier Science Inc. PII S0735-1097(01)01476-0 Influence
Journal of the American College of Cardiology Vol. 55, No. 9, by the American College of Cardiology Foundation ISSN /10/$36.
 Journal of the American College of Cardiology Vol. 55, No. 9, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.09.052
Journal of the American College of Cardiology Vol. 55, No. 9, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/10/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.09.052
Oral Antiplatelet Therapy in PCI/ACS. Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine
 Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Impact of Chronic Kidney Disease on Long-Term Outcome in Coronary Bypass Candidates Treated with Percutaneous Coronary Intervention
 Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Impact of Chronic Kidney Disease on Long-Term Outcome in Coronary Bypass Candidates Treated with Percutaneous Coronary
Original Article Print ISSN 1738-5520 On-line ISSN 1738-5555 Korean Circulation Journal Impact of Chronic Kidney Disease on Long-Term Outcome in Coronary Bypass Candidates Treated with Percutaneous Coronary
Are Asian Patients Different? - Updates Of Biomatrix Experience In Regional Settings: BEACON II (3 Yr F up) &
 &") Are Asian Patients Different? - Updates Of Biomatrix Experience In Regional Settings: BEACON II (3 Yr F up) & Biomatrix TM Single Center Experience (Indonesia)(Final 5 Yr F up) T. Santoso University of
Are Asian Patients Different? - Updates Of Biomatrix Experience In Regional Settings: BEACON II (3 Yr F up) & Biomatrix TM Single Center Experience (Indonesia)(Final 5 Yr F up) T. Santoso University of
Reduction in Stent Thrombosis better tablets or better stents?
 Reduction in Stent Thrombosis better tablets or better stents? Dr James Cotton MD FRCP Heart and Lung Centre Wolverhampton MY CONFLICTS OF INTEREST ARE Speaker Fees/Honoraria/Travel Support Lilly/Daiichi
Reduction in Stent Thrombosis better tablets or better stents? Dr James Cotton MD FRCP Heart and Lung Centre Wolverhampton MY CONFLICTS OF INTEREST ARE Speaker Fees/Honoraria/Travel Support Lilly/Daiichi
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Supplementary Material to Mayer et al. A comparative cohort study on personalised
 Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Suppl. Table : Baseline characteristics of the patients. Characteristic Modified cohort Non-modified cohort P value (n=00) Age years 68. ±. 69.5 ±. 0. Female sex no. (%) 60 (0.0) 88 (.7) 0.0 Body Mass
Angiographic Stent Thrombosis at Coronary Bifurcations
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 1, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2011.09.015 Angiographic
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 1, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2011.09.015 Angiographic
Evaluation of a novel stent technology: the Genous EPC capturing stent Klomp, M.
 UvA-DARE (Digital Academic Repository) Evaluation of a novel stent technology: the Genous EPC capturing stent Klomp, M. Link to publication Citation for published version (APA): Klomp, M. (2012). Evaluation
UvA-DARE (Digital Academic Repository) Evaluation of a novel stent technology: the Genous EPC capturing stent Klomp, M. Link to publication Citation for published version (APA): Klomp, M. (2012). Evaluation
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Gender-Based Outcomes in Percutaneous Coronary Intervention with Drug-Eluting Stents (from the National Heart, Lung, and Blood Institute Dynamic
 Gender-Based Outcomes in Percutaneous Coronary Intervention with Drug-Eluting Stents (from the National Heart, Lung, and Blood Institute Dynamic Registry) J. D. Abbott, et al. Am J Cardiol (2007) 99;626-31
Gender-Based Outcomes in Percutaneous Coronary Intervention with Drug-Eluting Stents (from the National Heart, Lung, and Blood Institute Dynamic Registry) J. D. Abbott, et al. Am J Cardiol (2007) 99;626-31
Long-Term Comparison of Everolimus-Eluting and Sirolimus-Eluting Stents for Coronary Revascularization
 Journal of the American College of Cardiology Vol. 57, No. 21, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.01.023
Journal of the American College of Cardiology Vol. 57, No. 21, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.01.023
Diabetic Patients: Current Evidence of Revascularization
 Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Diabetic Patients: Current Evidence of Revascularization Alexandra J. Lansky, MD Yale University School of Medicine University College of London The Problem with Diabetic Patients Endothelial dysfunction
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Nobori Clinical Studies Up-dates. Gian Battista DANZI, M.D. Ospedale Maggiore Policlinico University of Milan, Italy
 Nobori Clinical Studies Up-dates Gian Battista DANZI, M.D. Ospedale Maggiore Policlinico University of Milan, Italy Drug Eluting Stents High benefit in preventing restenosis and improving quality of life
Nobori Clinical Studies Up-dates Gian Battista DANZI, M.D. Ospedale Maggiore Policlinico University of Milan, Italy Drug Eluting Stents High benefit in preventing restenosis and improving quality of life
Prevention of Coronary Stent Thrombosis and Restenosis
 Prevention of Coronary Stent Thrombosis and Restenosis Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea 9/12/03 Coronary
Prevention of Coronary Stent Thrombosis and Restenosis Seong-Wook Park, MD, PhD, FACC Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea 9/12/03 Coronary
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Antiplatelet therapy in myocardial infarction and coronary stent thrombosis Heestermans, Antonius Adrianus Cornelius Maria
 University of Groningen Antiplatelet therapy in myocardial infarction and coronary stent thrombosis Heestermans, Antonius Adrianus Cornelius Maria IMPORTANT NOTE: You are advised to consult the publisher's
University of Groningen Antiplatelet therapy in myocardial infarction and coronary stent thrombosis Heestermans, Antonius Adrianus Cornelius Maria IMPORTANT NOTE: You are advised to consult the publisher's
Formation of and countermeasures for subacute coronary stent thrombosis in elderly diabetic patients
 Formation of and countermeasures for subacute coronary stent thrombosis in elderly diabetic patients Z.-F. Li 1, Y.-P. Zhang 2, Z.-Q. Qin 2, X.-L. Li 1, C.-H. Gao 1, S. Yang 1 and Z.-J. Chen 1 1 Department
Formation of and countermeasures for subacute coronary stent thrombosis in elderly diabetic patients Z.-F. Li 1, Y.-P. Zhang 2, Z.-Q. Qin 2, X.-L. Li 1, C.-H. Gao 1, S. Yang 1 and Z.-J. Chen 1 1 Department
Rationale for Percutaneous Revascularization ESC 2011
 Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
Rationale for Percutaneous Revascularization Marie Claude Morice, Massy FR MD, FESC, FACC ESC 2011 Paris Villepinte - 27-31 August, 2011 Massy, France Potential conflicts of interest I have the following
Comparison of Bare metal Vs Drug eluting stents for in-stent Restenosis among Diabetics
 Original Article Comparison of Bare metal Vs Drug eluting stents for in-stent Restenosis among Diabetics Mynuddin Ahmed Nawaz 1, Ia Avaliani 1, Irakli Davitashvili 1, Georgi Getmansky 1 Khatuna Jalabadze
Original Article Comparison of Bare metal Vs Drug eluting stents for in-stent Restenosis among Diabetics Mynuddin Ahmed Nawaz 1, Ia Avaliani 1, Irakli Davitashvili 1, Georgi Getmansky 1 Khatuna Jalabadze
Culprit Lesion Remodeling and Long-term (> 5years) Prognosis in Patients with Acute Coronary Syndrome
 Prognosis in Patients with Acute Coronary Syndrome") Culprit Lesion Remodeling and Long-term (> 5years) Prognosis in Patients with Acute Coronary Syndrome Hiroyuki Okura*, MD; Nobuya Matsushita**,MD Kenji Shimeno**, MD; Hiroyuki Yamaghishi**, MD Iku Toda**,
Culprit Lesion Remodeling and Long-term (> 5years) Prognosis in Patients with Acute Coronary Syndrome Hiroyuki Okura*, MD; Nobuya Matsushita**,MD Kenji Shimeno**, MD; Hiroyuki Yamaghishi**, MD Iku Toda**,
Supplementary Table S1: Proportion of missing values presents in the original dataset
 Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Supplementary Table S1: Proportion of missing values presents in the original dataset Variable Included (%) Missing (%) Age 89067 (100.0) 0 (0.0) Gender 89067 (100.0) 0 (0.0) Smoking status 80706 (90.6)
Treatment of Left Main Coronary Trifurcation Lesions with the Paclitaxel Drug-Eluting Stent: Mid-Term Outcomes from a Tertiary Medical Center
 Original Contribution Treatment of Left Main Coronary Trifurcation Lesions with the Paclitaxel Drug-Eluting Stent: Mid-Term Outcomes from a Tertiary Medical Center Nicolas W. Shammas, MD, MS, Gail A. Shammas,
Original Contribution Treatment of Left Main Coronary Trifurcation Lesions with the Paclitaxel Drug-Eluting Stent: Mid-Term Outcomes from a Tertiary Medical Center Nicolas W. Shammas, MD, MS, Gail A. Shammas,
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Few areas of medicine have evolved as rapidly as coronary
 Perspective Annals of Internal Medicine Balancing Efficacy and Safety of Drug-Eluting in Patients Undergoing Percutaneous Coronary Intervention Allen Jeremias, MD, MSc, and Ajay Kirtane, MD, SM Drug-eluting
Perspective Annals of Internal Medicine Balancing Efficacy and Safety of Drug-Eluting in Patients Undergoing Percutaneous Coronary Intervention Allen Jeremias, MD, MSc, and Ajay Kirtane, MD, SM Drug-eluting
Unprotected LM intervention
 Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Unprotected LM intervention Guideline for COMBAT Seung-Jung Park, MD, PhD Professor of Internal Medicine, Seoul, Korea Current Recommendation for unprotected LMCA Stenosis Class IIb C in ESC guideline
Pathology of percutaneous interventions (PCI) in coronary arteries. Allard van der Wal, MD.PhD; Pathologie AMC, Amsterdam, NL
 in coronary arteries. Allard van der Wal, MD.PhD; Pathologie AMC, Amsterdam, NL") Pathology of percutaneous interventions (PCI) in coronary arteries Allard van der Wal, MD.PhD; Pathologie AMC, Amsterdam, NL Percutaneous Coronary Intervention (PCI) Definition: transcatheter opening of
Pathology of percutaneous interventions (PCI) in coronary arteries Allard van der Wal, MD.PhD; Pathologie AMC, Amsterdam, NL Percutaneous Coronary Intervention (PCI) Definition: transcatheter opening of
New Generation Drug- Eluting Stent in Korea
 New Generation Drug- Eluting Stent in Korea Young-Hak Kim, MD, PhD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Purpose To briefly introduce the
New Generation Drug- Eluting Stent in Korea Young-Hak Kim, MD, PhD Department of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea Purpose To briefly introduce the
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI
 Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Target vessel only revascularization versus complet revascularization in non culprit lesions in acute myocardial infarction treated by primary PCI Gamal Abdelhady, Emad Mahmoud Department of interventional
Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice (COMPARE): a randomised trial
: a randomised trial") Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice (COMPARE): a randomised trial Elvin Kedhi, Kaiyum Sheik Joesoef, Eugene McFadden, Jochem Wassing, Carlos van Mieghem,
Second-generation everolimus-eluting and paclitaxel-eluting stents in real-life practice (COMPARE): a randomised trial Elvin Kedhi, Kaiyum Sheik Joesoef, Eugene McFadden, Jochem Wassing, Carlos van Mieghem,
Clinical outcomes between different stent designs with the same polymer and drug: comparison between the Taxus Express and Taxus Liberte stents
 ORIGINAL ARTICLE Korean J Intern Med 2013;28:72-80 Clinical outcomes between different stent designs with the same polymer and drug: comparison between the Taxus Express and Taxus Liberte stents Jang-Won
ORIGINAL ARTICLE Korean J Intern Med 2013;28:72-80 Clinical outcomes between different stent designs with the same polymer and drug: comparison between the Taxus Express and Taxus Liberte stents Jang-Won
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
3-Year Clinical Outcomes in the Randomized SORT OUT III Superiority Trial Comparing Zotarolimus- and Sirolimus-Eluting Coronary Stents
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 8, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.04.008
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 5, NO. 8, 2012 2012 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jcin.2012.04.008
PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study
 ESC, Hotline III, Paris, August, 30, 2011 PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study M. Valgimigli, MD, PhD University of Ferrara, ITALY On behalf of the
ESC, Hotline III, Paris, August, 30, 2011 PROlonging Dual antiplatelet treatment after Grading stent-induced Intimal hyperplasia study M. Valgimigli, MD, PhD University of Ferrara, ITALY On behalf of the
HCS Working Group Seminars Macedonia Pallas Hotel, Friday 21 st February Drug-eluting stents Are they all equal?
 HCS Working Group Seminars Macedonia Pallas Hotel, Friday 21 st February 2014 Drug-eluting stents Are they all equal? Vassilis Spanos Interventional Cardiologist, As. Director 3 rd Cardiology Clinic Euroclinic
HCS Working Group Seminars Macedonia Pallas Hotel, Friday 21 st February 2014 Drug-eluting stents Are they all equal? Vassilis Spanos Interventional Cardiologist, As. Director 3 rd Cardiology Clinic Euroclinic
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
C L I N I C A L R E S E A R C H
 C L I N I C A L R E S E A R C H Clinical long-term outcome after implantation of titanium nitride-oxide coated stents compared with paclitaxel- or sirolimus-eluting stents: propensity-score matched analysis
C L I N I C A L R E S E A R C H Clinical long-term outcome after implantation of titanium nitride-oxide coated stents compared with paclitaxel- or sirolimus-eluting stents: propensity-score matched analysis
TCTAP Upendra Kaul MD,DM,FACC,FSCAI,FAMS,FCSI
 Indian TUXEDO Trial In Medically Treated Diabetics Upendra Kaul MD,DM,FACC,FSCAI,FAMS,FCSI Executive Director and Dean Escorts Heart Institute & Medical Research Center and Fortis Hospitals, New Delhi
Indian TUXEDO Trial In Medically Treated Diabetics Upendra Kaul MD,DM,FACC,FSCAI,FAMS,FCSI Executive Director and Dean Escorts Heart Institute & Medical Research Center and Fortis Hospitals, New Delhi
Drug eluting stents From revolution to evolution. Current limitations
 Drug eluting stents From revolution to evolution Current limitations Eric Eeckhout Centre Hospitalier Universitaire Vaudois Lausanne - Switzerland eric.eeckhout@chuv.ch Overview Historical perspective
Drug eluting stents From revolution to evolution Current limitations Eric Eeckhout Centre Hospitalier Universitaire Vaudois Lausanne - Switzerland eric.eeckhout@chuv.ch Overview Historical perspective
Bivalirudin Clinical Trials Update Evidence and Future Perspectives
 Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Drug Eluting Stents: an update Abbott Vascular. All rights reserved.
 Drug Eluting Stents: an update DES: Science and Education for Better Practice--Introduction The clinical benefits of DES in reducing the risk of restenosis are well established. Recently the safety profile
Drug Eluting Stents: an update DES: Science and Education for Better Practice--Introduction The clinical benefits of DES in reducing the risk of restenosis are well established. Recently the safety profile
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017
 EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
EXCEL vs. NOBLE: How to Treat Left Main Disease in 2017 AATS International Cardiovascular Symposium December 8-9, 2017 Igor F. Palacios, MD Director of Interventional Cardiology Professor of Medicine Massachusetts
The Risk of Stent Thrombosis in Patients With Acute Coronary Syndromes Treated With Bare-Metal and Drug-Eluting Stents
 JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 6, 2009 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/09/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2009.04.003 The Risk
JACC: CARDIOVASCULAR INTERVENTIONS VOL. 2, NO. 6, 2009 2009 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 1936-8798/09/$36.00 PUBLISHED BY ELSEVIER INC. DOI: 10.1016/j.jcin.2009.04.003 The Risk
Final Clinical and Angiographic Results From a Nationwide Registry of FIREBIRD Sirolimus- Eluting Stent: Firebird In China (FIC) Registry (PI R. Gao)
 Registry (PI R. Gao)") The Microport FIREBIRD Polymer-based Sirolimus- Eluting Stent Clinical Trial Program Update: The FIC and FIREMAN Registries Junbo Ge, MD, FACC, FESC, FSCAI On behalf of Runlin Gao (FIC PI) and Haichang
The Microport FIREBIRD Polymer-based Sirolimus- Eluting Stent Clinical Trial Program Update: The FIC and FIREMAN Registries Junbo Ge, MD, FACC, FESC, FSCAI On behalf of Runlin Gao (FIC PI) and Haichang
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Original Research Clinical Outcomes of Drug-Eluting Stents Compared with Bare Metal Stents in Our Routine Clinical Practice
 Hellenic J Cardiol 2008; 49: 132-138 Original Research Clinical Outcomes of Drug-Eluting Stents Compared with Bare Metal Stents in Our Routine Clinical Practice MOHAMMAD ALIDOOSTI, MOJTABA SALARIFAR, ALI
Hellenic J Cardiol 2008; 49: 132-138 Original Research Clinical Outcomes of Drug-Eluting Stents Compared with Bare Metal Stents in Our Routine Clinical Practice MOHAMMAD ALIDOOSTI, MOJTABA SALARIFAR, ALI
Summary HTA. Drug-eluting stents vs. coronary artery bypass-grafting. HTA-Report Summary. Gorenoi V, Dintsios CM, Schönermark MP, Hagen A
 Summary HTA HTA-Report Summary Drug-eluting stents vs. coronary artery bypass-grafting in coronary heart disease Gorenoi V, Dintsios CM, Schönermark MP, Hagen A Scientific background The coronary heart
Summary HTA HTA-Report Summary Drug-eluting stents vs. coronary artery bypass-grafting in coronary heart disease Gorenoi V, Dintsios CM, Schönermark MP, Hagen A Scientific background The coronary heart