P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
|
|
|
- Loren Booker
- 6 years ago
- Views:
Transcription


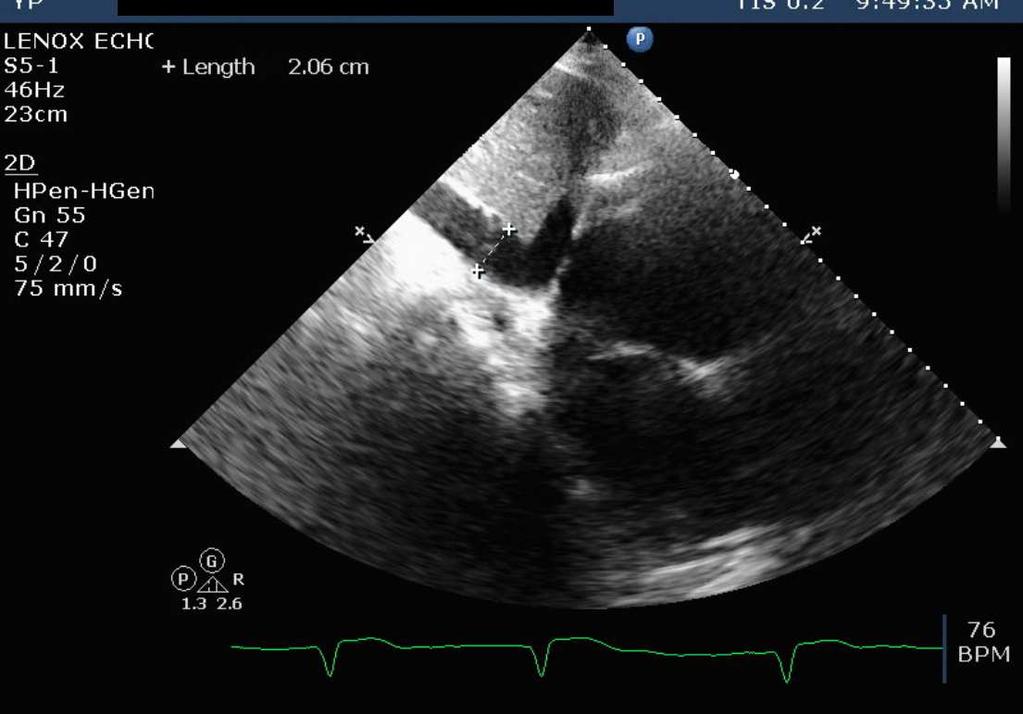
1 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli Equation P = 4V 2 P = pressure (mm Hg) V = velocity (m / sec) Liv Hatle Very New Criteria IVC Dimensions IVC diameter 2.1 cm which collapses >50% with a sniff suggests RA pressure 0-5 mmhg IVC diameter > 2.1 cm which collapses <50% with a sniff suggests RA pressure -20 mmhg Scenarios where IVC diameter & collapse do not fit this paradigm, an intermediate value of 5- mmhg should be used. 1




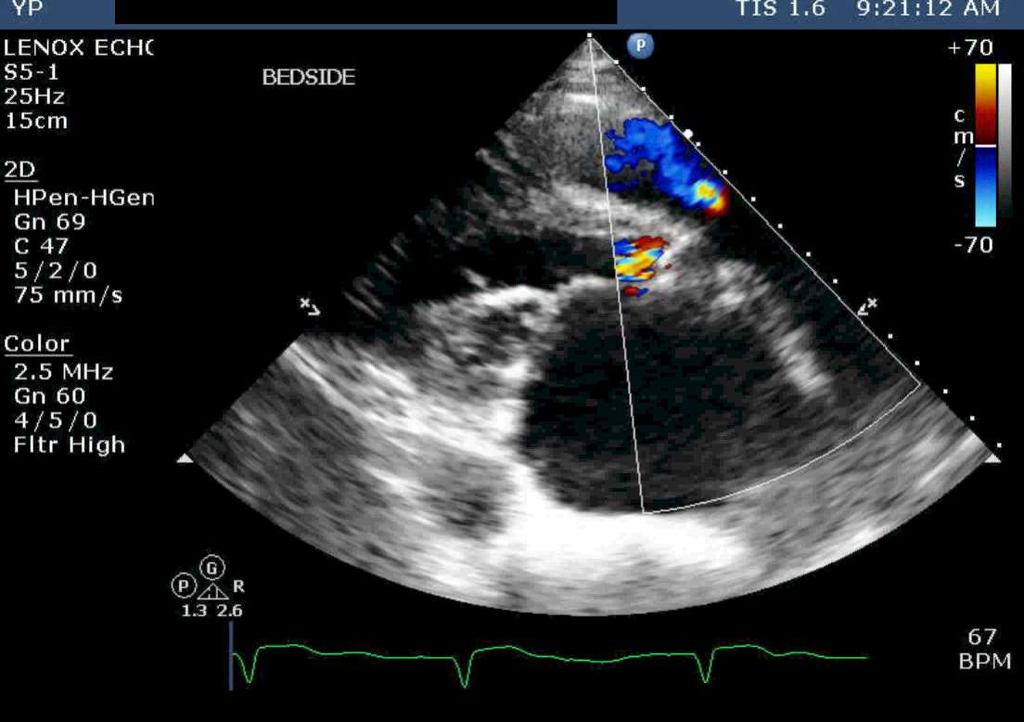
2 RA Pressure = 5 mmhg Markedly elevated RA pressure (> 15 mm Hg) 2.8 cm Note: 1. Dilated IVC 2. Lack of respiratory variation Tricuspid Regurg. 2.5x2.5x4 =25mmHg 4x2.5x2.5=25mmHg 2.5m/sec RV Syst Pressure = TR Gradient +RAP PVC TVC RV PA RA 2
 way of estimating RV systolic pressure AoVC MVC")
3 Evaluation of RV Systolic Pressure RV systolic pressure = TR gradient + RA pressure Evaluation of PA Systolic Pressure In the absence of PS PA systolic pressure = RV systolic pressure = TR gradient + RA pressure In the presence of PS PA systolic pressure = = RV systolic pressure - PS gradient Pressure Gradients in VSD An alternative (non-tr based) way of estimating RV systolic pressure AoVC MVC LV Ao RV 3

4 Post MI VSD BP 175/70mmHg 6m/sec 1.7 LV-RV systolic gradient = 4x6x6=144mmHg RV systolic pressure = systolic BP - VSD gradient = 31 mmhg Evaluation of RV Diastolic Pressure In the absence of TS RV diastolic pressure = RA pressure In the presence of TS RV diastolic pressure = RA pressure - TS gradient CW of Pulmonic Valve Flow 2.5 m/sec The study suggests: 1. Severe PS 2. Right heart failure 3. Pulmonary hypertension 4. Constrictive Pericarditis 4
5 CW of Pulmonic Valve Flow Pulmonary hypertension Note the end-diastolic gradient of 2.5 m/sec, indicating an end diastolic gradient of 25 mmhg between the PA and RV Evaluation of PA Diastolic Pressure PA diastolic pressure = PR gradient + RA(V) pressure PVC PA RV RA Estimating RV & PA pressures when there is no TR (or PR) 1. M-Mode 2. 2D (septal flattening) 3. RVOT flow pattern 4. RV outflow velocity acceleration time 5




6 Severe PHT 1. No A wave 2. Systolic flying W 3. No diastolic posterior motion 2D in PHT - D shaped LV RVOT Acceleration time (Mahan s Formula) 125msec Mean PAP = 79 - (0.45 x AcT) Normal AcT > 120msec If AcT<90msec, peak PA systolic pressure is more than 60 mmhg Mean PAP = 79 (0.45 * 90) = = 39 mmhg 6
7 CW of MR Jet in a pt with a BP of 120 / 80. The MR velocity is 7.7 m / sec The most likely dx is: 1. Aortic Stenosis 2. Aortic Insufficiency 3. High Cardiac Output 4. Pulmonary Embolism CW of MR Jet in a pt with a BP of 120 / 80 Aortic Stenosis The velocity of the MR jet indicates a peak systolic LV-LA gradient of 237 mm Hg; Therefore the Aortic gradient is at least 120 mm Hg. MR Velocity in AS Peak systolic LVP Peak systolic BP Ao LA LV 7
8 CW of Aortic Valve Flow The BP is 150 / 80 LV Ao LA 4m/sec 4m/sec The LV pressure is: / / / /16 CW of Aortic Valve Flow The BP is 150 / 80 LV Ao LA ANSWER: /16 LV (sys)= Sys. BP (150) + 70%Ao gradient (45) = 195 LV (dias) = Dias. BP (80) - Ao dias. Gradient (64) = 16 Aortic Valve Gradient 1. Peak - to - Peak Gradient (P2P) 2. Maximum Instantaneous Gradient (MIG) 3. Mean Gradient MIG = (4 m/sec) 2 = 64 mm Hg P2P = 70% * MIG = 0.7 * 64 = 45 mm Hg Ao The P2P gradient is 70% of the MIG LV 8
9 Evaluation of LV Systolic Pressure In pts without aortic valve disease: LV systolic pressure = systolic BP In pts with AS or LVOT obstruction: LV systolic pressure = systolic BP + gradient Evaluation of LV Diastolic Pressure In pts with AR: LV end-diastolic pressure = diastolic BP - AR gradient In the absence of MS: LVDP = (approx.) LA pressure Calculation of LVEDP Systemic diastolic BP - End Diastolic Aortic Gradient Ao LV 9
+1.")
![9] Nagueh 1999 6cm/sec LAP = E/e + 4 120cm/sec LAP= 120/6 + 4 = 24 mmhg E/e = 8: LA pressure nl E/e = 15: LA pressure](/docs-images/71/66241654/images/10-1.jpg "high Estimating LA Pressure by E/e May Be Inaccurate in: Mitral Stenosis Mitral annular calcification Prosthetic MV")
10 Evaluation of LA Pressure from transmitral and PV flow A. Normal 6-12 mm Hg B. Abnormal Relax C. Pseudonormal D. Restrictive > 22 Calculation of LA pressure LAP= 1.24[(E/e )+1.9] Nagueh cm/sec LAP = E/e cm/sec LAP= 120/6 + 4 = 24 mmhg E/e = 8: LA pressure nl E/e = 15: LA pressure high Estimating LA Pressure by E/e May Be Inaccurate in: Mitral Stenosis Mitral annular calcification Prosthetic MV Mitral regurgitation Diffuse severe LV dysfunction
11 Evaluation of LA Pressure in pt with MS In MS, LA diastolic pressure = LVDP + transmitral gradient Mean MV gradient 16mmHg Mean MV gradient 4mmHg Noninvasive Hemodynamic Study 63-Year Year-Old female with Dyspnea BP 0/55 Bibasilar rales MS, AS, MR, TR murmurs 0/55 CP MMS + AS 11


12 MMR + AR M TR + PR Normal IVC Size 2.0 cm <50% Respiratory Variation 0/65 CP
 = mm Hg 0/55 3.")

 = 30 0/55 66/30 2.2m/sec 2.")
 AR gradient (36) = 19mmHg")
13 RV Pressures RV systolic = RA pressure () + TR gradient (56) = mm Hg 0/55 3.7m/sec 56mmHg 66/ In the absence of TS RV diastolic pressure = RA pressure PA Pressure Systolic = RV systolic (66) Diastolic = PR gradient (20) + RA pressure () = 30 0/55 66/30 2.2m/sec mmHG 20mmHg 66/ CP LVEDP = aortic diastolic pressure (55) AR gradient (36) = 19mmHg 0/55 66/30 55mmHg 36mmHg 3.7 3m/sec 66/ /19 CP
 + 70% of AV gradient (46) =")



14 LV systolic pressure = aortic systolic pressure (0) + 70% of AV gradient (46) = 146mmHg 0/55 66/30 66mmHg MIG P2P = 0.7 * 66 = 46 66/ 146/19 LA pressure = LV diastolic (19) + MV mean gradient (7) = 26mmHg /55 66/ /19 66/ 6 Calculation of Systemic Blood Flow SBF = VTI LVOT X Area LVOT X HR D = 2 cm VTI = 24 cm HR = 80 SBF= 6,000 cc 1 x 1 x 3.14 x 24 x 80 14


15 Calculation of Pulmonary Blood Flow C.O. = VTI RVOT X Area RVOT X HR Can also be calculated using RV inflow and TV VTI Calculation of Shunts (ASD, VSD) Shunt flow = 1. Pulmonary blood flow - systemic blood flow - or - 2. ASD or VSD orifice area x Shunt VTI x HR Calculation of ASD L-to-R Shunt RA LA ASD diameter = 1.2 cm Shunt Flow = Orifice Area x VTI of shunt x HR = 0.6 x 0.6 x 3.14 x 80 x 0 = 9L/min. 15


16 Real time, 3D TEE: Secundum ASD Pulmonary Vascular Resistance Normal =2 Wood s units PVR = (mean PAP- mean PCWP)/C.O. 4.9m/sec Another method VTI PVR= (Peak TR Velocity/RVOT VTI ) PVR=Wood s units TR Velocity = m/sec RVOT TVI = cm Conclusions Normal and abnormal hemodynamics can be evaluated non invasively by Doppler Echocardiography. Invasive evaluation may be needed for details not seen on Echo, or when the clinical impression is not consistent with the echo-doppler findings 16
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Swan Song: Echocardiography as a Pulmonary Artery Catheter? Interdepartmental Division of Critical Care Medicine
 Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
2/4/2011. Nathan Kerner, M.D.
 Nathan Kerner, M.D. Definition Elevated pressures - cut off usually >40 mmhg pulmonary artery systolic pressure (PASP) Usually associated with elevated pulmonary vascular resistance (PVR) measured in dynessec/cm
Nathan Kerner, M.D. Definition Elevated pressures - cut off usually >40 mmhg pulmonary artery systolic pressure (PASP) Usually associated with elevated pulmonary vascular resistance (PVR) measured in dynessec/cm
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Right Heart Hemodynamics: Echo-Cath Discrepancies
 Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care. Dr. Mark Tutschka Dr. Rob ArnAield
 Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Constriction vs Restriction Case-based Discussion
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Constriction vs Restriction Case-based Discussion Jae K. Oh, MD Samsung Professor
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Constriction vs Restriction Case-based Discussion Jae K. Oh, MD Samsung Professor
An Integrated Approach to Study LV Diastolic Function
 An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
An Integrated Approach to Study LV Diastolic Function Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania LV Diastolic Dysfunction impaired relaxation (early diastole)
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Doppler and Hemodynamics Muhamed Saric and Itzhak Kronzon
 LWBK739-C07_p77-119.qxd 9/1/10 11:50 PM Page 77 Aptara Doppler and Hemodynamics Muhamed Saric and Itzhak Kronzon CHAPTER 7 1. On echocardiography, the diameter of the inferior vena cava is measured at
LWBK739-C07_p77-119.qxd 9/1/10 11:50 PM Page 77 Aptara Doppler and Hemodynamics Muhamed Saric and Itzhak Kronzon CHAPTER 7 1. On echocardiography, the diameter of the inferior vena cava is measured at
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Echo in Pulmonary HTN
 Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Right Heart Catheterization. Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich
 Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
Right Heart Catheterization Franz R. Eberli MD Chief of Cardiology Stadtspital Triemli, Zurich Right Heart Catheterization Pressure measurements Oxygen saturation measurements Cardiac output, Vascular
Fig.1 Normal appearance of RV in SAX:
 Tutorial 7 - Assessment of the right heart Assessment of the Right heart The right heart assessment clinically and echocardiographically is not a very important part of mainstream cardiology. In the ICU,
Tutorial 7 - Assessment of the right heart Assessment of the Right heart The right heart assessment clinically and echocardiographically is not a very important part of mainstream cardiology. In the ICU,
Diastology Disclosures: None. Dias2011:1
 Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
Diastology 2011 James D. Thomas, M.D., F.A.C.C. Cardiovascular Imaging Center Department of Cardiology Cleveland Clinic Foundation Cleveland, Ohio, USA Disclosures: None Dias2011:1 Is EVERYBODY a member!?!
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
5 Working With Measurements
 5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Pericardial Disease: Case Examples. Echo Fiesta 2017
 Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation.
 Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Brief View of Calculation and Measurement of Cardiac Hemodynamics
 Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Cronicon OPEN ACCESS EC CARDIOLOGY Review Article Brief View of Calculation and Measurement of Cardiac Hemodynamics Samah Alasrawi* Pediatric Cardiologist, Al Jalila Children Heart Center, Dubai, UAE *
Disclosure. RV is not the innocent bystander 10/1/16. Assessment and Management of Pulmonary Heart Disease in the Female Patient
 Assessment and Management of Pulmonary Heart Disease in the Female Patient Oct 1, 2016 Deborah Women s Heart Center Susan E Wiegers, MD, FASE, FACC Professor of Medicine Senior Associate Dean of Faculty
Assessment and Management of Pulmonary Heart Disease in the Female Patient Oct 1, 2016 Deborah Women s Heart Center Susan E Wiegers, MD, FASE, FACC Professor of Medicine Senior Associate Dean of Faculty
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Pulmonary hypertension in clinical practice: are we focusing on the problem?
 Pulmonary hypertension in clinical practice: are we focusing on the problem? Odd Bech-Hanssen, MD, PhD Cardiology/Clinical Physiology Sahlgrenska University Hospital Gothenburg, Sweden Definition Mean
Pulmonary hypertension in clinical practice: are we focusing on the problem? Odd Bech-Hanssen, MD, PhD Cardiology/Clinical Physiology Sahlgrenska University Hospital Gothenburg, Sweden Definition Mean
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
10/1/2016. Constrictive Pericarditis Unique Hemodynamics. What s New in Pericardial Disease? Case-based Discussion
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification What s New in Pericardial Disease? Case-based Discussion Jae K. Oh, MD Samsung
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification What s New in Pericardial Disease? Case-based Discussion Jae K. Oh, MD Samsung
Outline. Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials
 Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials John R Schairer DO FACC Henry Ford Heart and Vascular Institute No Disclosures Outline Normal Anatomy and Physiology Pathophysiology
Echocardiographic Assessment of Pericardial Effusion/Tamponade: The Essentials John R Schairer DO FACC Henry Ford Heart and Vascular Institute No Disclosures Outline Normal Anatomy and Physiology Pathophysiology
Imaging in Heart Failure: A Multimodality Approach. Thomas Ryan, MD
 Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
Imaging in Heart Failure: A Multimodality Approach Thomas Ryan, MD Heart Failure HFrEF HFpEF EF50% Lifetime risk 20% Prevalence 6M Americans Societal costs - $30B 50% 5-year survival 1 Systolic
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Diastology State of The Art Assessment
 Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Diastology State of The Art Assessment Dr. Mohammad AlGhamdi Assistant professor, KSAU-HS Consultant Cardiologist King AbdulAziz Cardiac Center Ministry of National Guard Health Affairs Diagnostic Clinical
Pulmonary Hypertension: Echocardiographic Evaluation of Pulmonary Hypertension and Right Ventricular Function. Irmina Gradus-Pizlo, MD
 Pulmonary Hypertension: Echocardiographic Evaluation of Pulmonary Hypertension and Right Ventricular Function Irmina Gradus-Pizlo, MD Disclosures: Nothing to disclose Overview Is pulmonary hypertension
Pulmonary Hypertension: Echocardiographic Evaluation of Pulmonary Hypertension and Right Ventricular Function Irmina Gradus-Pizlo, MD Disclosures: Nothing to disclose Overview Is pulmonary hypertension
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Emergency Echo, Emergency Setting, ABCD Approach
 ECHO Alex Conference 2010 Emergency Echo, Emergency Setting, ABCD Approach Aleksandar N. Nešković Clinical Hospital Center Zemun Belgrade University School of Medicine Emergency Echocardiography Why ECHO
ECHO Alex Conference 2010 Emergency Echo, Emergency Setting, ABCD Approach Aleksandar N. Nešković Clinical Hospital Center Zemun Belgrade University School of Medicine Emergency Echocardiography Why ECHO
Clinical implication of exercise pulmonary hypertension: when should we measure it?
 Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Clinical implication of exercise pulmonary hypertension: when should we measure it? Jang-Young, Kim Wonju College of Medicine, Yonsei Univ. Exercise pulmonary hypertension (EPH) Introduction of pulmonary
Diastolic Heart Failure
 Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Chronic Heart Failure Prevalence overall = 2-3 % Diastolic Heart Failure Patrick Wouters University Hospital Ghent Belgium (Heart Failure + Asymptomatic Ventricular Dysfunction) Prevalence > 70 y = 10-20
Imaging Assessment of the Pulmonary Valve in Stenosis/Atresia and Regurgitation
 Imaging Assessment of the Pulmonary Valve in Stenosis/Atresia and Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children SCAI Fall Fellows Course 2014 Las
Imaging Assessment of the Pulmonary Valve in Stenosis/Atresia and Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children SCAI Fall Fellows Course 2014 Las
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
ΚΑΡΔΙΟΛΟΓΟΣ EUROPEAN ACCREDITATION IN TRANSTHORACIC AND TRANSESOPHAGEAL ECHOCARDIOGRAPHY
 1 ΚΑΡΔΙΟΛΟΓΟΣ EUROPEAN ACCREDITATION IN TRANSTHORACIC AND TRANSESOPHAGEAL ECHOCARDIOGRAPHY 2 Constrictive pericarditis (CP) is characterized by impaired ventricular filling due to a stiffened or noncompliant
1 ΚΑΡΔΙΟΛΟΓΟΣ EUROPEAN ACCREDITATION IN TRANSTHORACIC AND TRANSESOPHAGEAL ECHOCARDIOGRAPHY 2 Constrictive pericarditis (CP) is characterized by impaired ventricular filling due to a stiffened or noncompliant
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Transthoracic echocardiography in the evaluation of pediatric pulmonary hypertension and ventricular dysfunction
 REVIEW ARTICLE Transthoracic echocardiography in the evaluation of pediatric pulmonary hypertension and ventricular dysfunction Martin Koestenberger, 1 Mark K. Friedberg, 2 Eirik Nestaas, 3 Ina Michel-Behnke,
REVIEW ARTICLE Transthoracic echocardiography in the evaluation of pediatric pulmonary hypertension and ventricular dysfunction Martin Koestenberger, 1 Mark K. Friedberg, 2 Eirik Nestaas, 3 Ina Michel-Behnke,
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Pulmonary Hypertension. Echocardiography: Pearls & Pitfalls
 Pulmonary Hypertension Echocardiography: Pearls & Pitfalls Αθανάσιος Γ. Κουτσάκης Ειδικευόμενος Καρδιολογίας Α Καρδιολογική Κλινική ΑΠΘ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας Ιωάννινα,
Pulmonary Hypertension Echocardiography: Pearls & Pitfalls Αθανάσιος Γ. Κουτσάκης Ειδικευόμενος Καρδιολογίας Α Καρδιολογική Κλινική ΑΠΘ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας Ιωάννινα,
GENERAL PRINCIPLES FOR ECHO ASSESSMENT OF DIASTOLIC FUNCTION (For full recommendation refer to the Left Ventricular Diastolic Function Guideline)
") 1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
1 THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR THE EVALUATION OF LEFT VENTRICULAR DIASTOLIC FUNCTION BY ECHOCARDIOGRAPHY: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
ASCeXAM / ReASCE. Practice Board Exam Questions. Tuesday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
E/Ea is NOT an essential estimator of LV filling pressures
 Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
The Hemodynamics of PH Interpreting the numbers
 The Hemodynamics of PH Interpreting the numbers Todd M Bull MD Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
The Hemodynamics of PH Interpreting the numbers Todd M Bull MD Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The Patient with Atrial Fibrilation
 Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Assessment of Diastolic Function The Patient with Atrial Fibrilation Assoc. Prof. Adriana Ilieşiu, FESC University of Medicine Carol Davila Bucharest, Romania Associated Conditions with Atrial Fibrillation
Constrictive Pericarditis
 Constrictive Pericarditis Never Confused with Anything Else Jae K. Oh, MD 2018 MFMER 3712003-1 ARS #1 CP Which of following patients has constrictive pericarditis? 1 2 3 Medial e 13 cm/s Medial e 3 cm/s
Constrictive Pericarditis Never Confused with Anything Else Jae K. Oh, MD 2018 MFMER 3712003-1 ARS #1 CP Which of following patients has constrictive pericarditis? 1 2 3 Medial e 13 cm/s Medial e 3 cm/s
Echo Emergencies. Outline. Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures
 Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Ref 1. Ref 2. Ref 3. Ref 4. See graph
 Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018