Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
|
|
|
- Valentine Barnett
- 6 years ago
- Views:
Transcription
1 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
2 Background Aortic stenosis (AS) is the most frequent valve disease among referred patients >75 Years Years < 70 Years AS AR MS MR Multiple Right It is frequently identified at an asymptomatic stage.
3 Prevalence of AS /age (Iung and Vahanian :Can J Cardiol ;2014;30:1073-9)
4 Echocardiographic criteria for the definition of severe valve stenosis: an integrative approach Aortic stenosis Mitral stenosis Tricuspid stenosis Valve area (cm²) < 1.0 < 1.0 Indexed valve area (cm²/m² BSA) < 0.6 Mean gradient (mmhg) > 40 > 10 5 Maximum jet velocity (m/s) > 4.0 Velocity ratio < 0.25 Adapted from Baumgartner, EAE/ASE recommendations. Eur J Echocardiogr 2010;10:1-25 European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).

5 Asymptomatic AS Sudden death Myocardial dysfunction Amato et al, Heart 2001 Operative risk Prosthesis complications Edwards et al, JACC, 2001 Identify subgroups of asymptomatic patients at high risk of complications that could benefit from prophylactic aortic valve replacement+++.
6 Natural history
:61-7) E.")
7 Natural History of Aortic Stenosis (Ross and Braunwald Circulation 1968;38(Suppl.V):61-7) E.Braunwald

8 Important Interindividual Variability in the progression of AS (Otto Circ 1997)
9 Natural history of asymptomatic AS Prospective series n AS Severity Mean FU Sudden V.max (m/s) AVA (cm²) (months) Death (n) Otto (1997) Rosenhek (2000) Amato (2001) Das (2005) Monin (2009) Rosenhek (2010) Lancellotti (2010) Kang (2010) Maréchaux (2010) Cueff (2013) Incidence of sudden death < 1 per 100 pts-year
10 Asymptomatic AS Do not operate before symptoms, but : Rapid symptom onset High inter-patient variability Symptoms are subjective, progressive and often under-reported Identify patients at high risk for early symptom onset
11 Asymptomatic AS 123 pts with V max 2.5 m/s (max. gradient 25 mmhg) Age 63 ± 16 yrs Annual exercise test Death or AVR ( symptoms) Predictive factor V max. 4m/s (Otto et al. Circulation 1997;95: )
12 Severe Asymptomatic AS 128 pts with V max. 4 m/s (max. gradient 64 mmhg) Valve area 0.8 cm², mean 0.68 cm² Age 60 ± 18 yrs Death or AVR ( symptoms) Predictive factors Progression of V max. Extent of calcification (Rosenhek et al. N Engl J Med 2000;343:611-7)
13 Severe asymptomatic AS and aortic velocity 116 asymptomatic patients with severe AS 6 cardiac deaths (1 sudden death) 90 AVRs (Rosenhek et al. Circulation 2010;121;151-6)
14 Asymptomatic AS and exercise ECG 125 asymptomatic patients with AS < 1.4 cm² 46 (37%) had symptoms at exercise ECG 29 (23%) had inadequate blood pressure response 36 (29%) became symptomatic at 1 yr Predictive factors Symptoms at exercise ECG (p<0.001) BP response (p=0.17) (Das et al. Eur Heart J 2005;26: )
15 Asymptomatic AS and exercise ECG 66 asymptomatic patients with AS < 1.0 cm² Death or symptoms Initial exercise ECG Positivity criteria: - Chest pain or near syncope - systolic BP < 20 mmhg - ST - Ventricular arrhythmia (Amato et al. Heart 2001;86:381-6)
16 Asymptomatic AS and exercise echo 69 patients with asymptomatic severe AS Predictors of cardiac events Increase in mean gradient 18 mmhg <0.015 Abnormal exercise test Aortic valve area < 0.75 cm² p (Lancellotti et al. Circulation 2005, 112(suppl.I):I377-82)
17 Asymptomatic AS and exercise echo 135 patients with asymptomatic moderate AS and normal standard exercise test (Maréchaux et al. Eur Heart J 2010;31:1295-7)

18 Asymptomatic AS and exercise ECG Meta-analysis (Rafique et al. Am J Cardiol 2009;104:972-7)
19 Method Retrospective, observational study Inclusion criteria : We enrolled all consecutive patients with asymptomatic AS of at least moderate degree (MPG 25 mmhg) who underwent an exercise echocardiography between January 2005 and December 2014 at our institution Exclusion criteria : LV dysfunction (LVEF <50%), Congenital stenosis except bicuspid valve, Rheumatic stenosis, Aortic regurgitation or other valvular disease with a grade > 2/4 Presence of significant aortic acceleration or aortic obstruction. (Goublaire,Submitted)
20 Method All patients underwent first a comprehensive TTE at rest followed by a symptomlimited exercise echocardiography. A positive exercise test was defined by : occurrence of symptoms (dyspnea, angina, syncope), fall in systolic BP or rise < 20 mmhg, ST segment depression ( 2 mm) ventricular arrhythmia A positive stress echocardiography was defined as : exercise-induced MPG increase > 20 mmhg SPAP increase above 60 mmhg at peak stress, impaired LVEF Apparition of wall motion abnormalities. Patients with a positive exercise test were considered for surgery as well as those who developed LV dysfunction or wall motion abnormalities during exercise. The remaining population was conservatively managed.

21 Results Primary endpoint : Occurrence of symptoms Congestive heart failure In the 2 years of follow-up 148 patients enrolled Positive exercise test N = 36 Negative exercise test N = patients considered for surgery Lost of follow-up N = 4 Conservatively managed N = 108 Aortic valve replacement N = 33 Medical treatment N = 3 Positive exercise echocardiography N = 38 Negative exercise echocardiography N = 70
22 Event free survival, % Event-free survival according to MPG at rest MPG baseline < 40 mmhg 40 mmhg Follow-up duration, months P =
23 Event free survival, % Follow-up duration, months Event free survival according to exercise-induced increase in MPG Exercise-induced increase in MPG < 20 mmhg 20 mmhg P =
24 Event free survival, % Event-free survival according to SPAP at peak exercise SPAP at peak exercise 60 mmhg > 60 mmhg P = Follow-up duration, months
25 Mid term outcome
26 AS and natriuretic peptides 130 patients 70 patients (VA < 1 cm² or V. max > 4 m/sec.) (VA < 1 cm² and EF > 50%) Survival (Berger-Klein et al. (Lim et al. Circulation 2004;109:2302-8) Eur Heart J 2004;25: )

27 Asymptomatic AS and natriuretic peptides 1953 patients with moderate AS 40% asymptomatic (Clavel et al. J Am Coll Cardiol 2014;63: )
28 Asymptomatic AS and natriuretic peptides 142 asymptomatic patients with mild AS (102 moderate AS). Mean FU 1.8 years Event-free survival and Nt-proBNP: 142 mild AS 102 moderate AS Nt-proBNP and event free-survival, adjusted on age, gender and AVA p=0.40 p=0.43 (Cueff et al. Heart 2013;99:461-7)
29 Asymptomatic AS: multifactorial approach 107 patients with asymptomatic moderate or severe AS Score = (2 x V.max)+ (1.5 x log BNP) if female gender Event-free survival (Monin et al. Circulation 2009;120:69-75)
30 Resting heart rate Other prognostic factors (Greve et al. Int J Cardiol 2015;180:122-8) Valvulo-arterial impedance (Banovic et al. J Heart valve Dis 2015;24:156-63) Left ventricular deformation (Nagata et al. J Am Coll Cardiol Img 2015;8:235-45) BNP at exercise (Capoulade et al. Heart 2014;100: ) Cardiopulmonary exercise testing (Levy et al. Arch Cardiovasc Dis 2014;107:519-23) Myocardial fibrosis in CMR (Lee et al. Radiology 2015;274:259-69)
31 Index aortic valve area and outcome (Tribouilloy Circ Cardiovasc Imaging 2016)
32
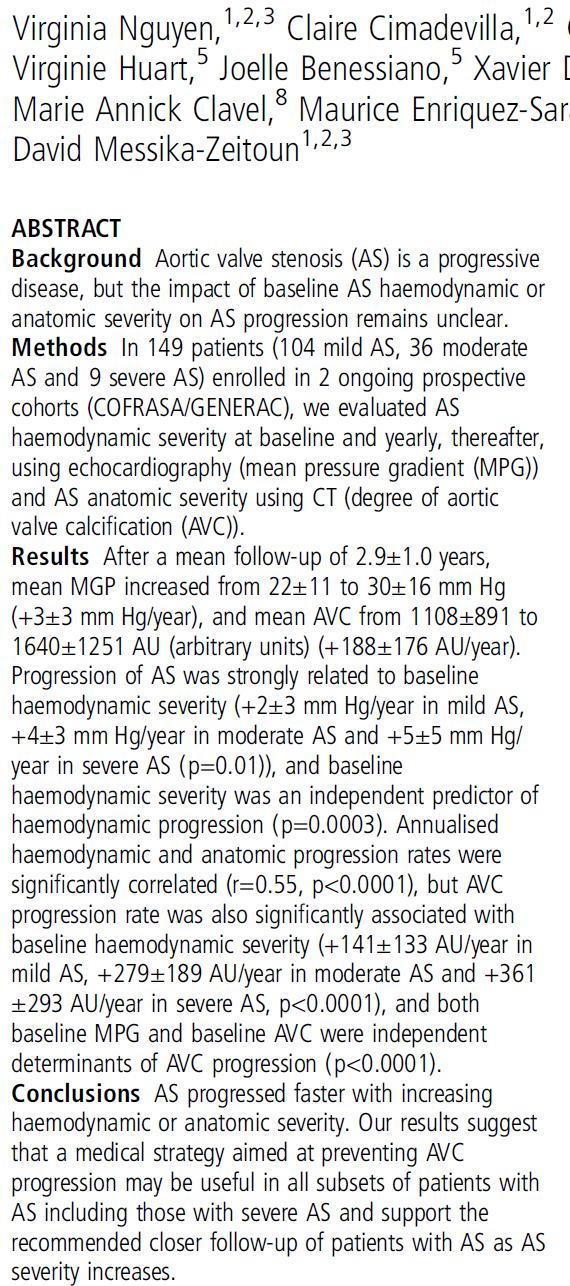
33 Progression of Aortic Valve Calcification in Aortic Stenosis - Impact of Severity. The COFRASA - GENERAC Study (N Guyen,Heart 2016)
34 Aortic valve replacement or cardiovascular death and cardiac troponin I concentrations (Chin C W L et al. Eur Heart J 2014;eurheartj.ehu189)
35 Predictors of Outcome in Asymptomatic AS Clinical: older age, presence of CV risk factors Echocardiography: higher peak velocity, severe calcification, rapid hemodynamic progression, reduced LVEF, excessive LVH, increase in gradient with exercise Exercise testing: symptoms on exercise (blood pressure fall) Biomarkers: markedly elevated natriuretic peptides (BNP, Nt-proBNP)
36 Natural history Medical therapy
37 Scottish Aortic Stenosis and Lipid Lowering Trial, Impact on Regression (SALTIRE) Investigators Double blinded randomized study: high-dose atorvastatine versus placebo (Cowell. N Engl J Med 2005;352:283-97)
38 Percentage of Patients SEAS Primary Endpoint 688 major cardiovascular events 355 Placebo / 333 Simvastatine + Ezetimibe Placebo EZ/Simva 10/40 mg 10 Hazard ratio: 0.96, P= Year
39 Natural history Medical therapy Surgery

40 Operative mortality STS Database 2013

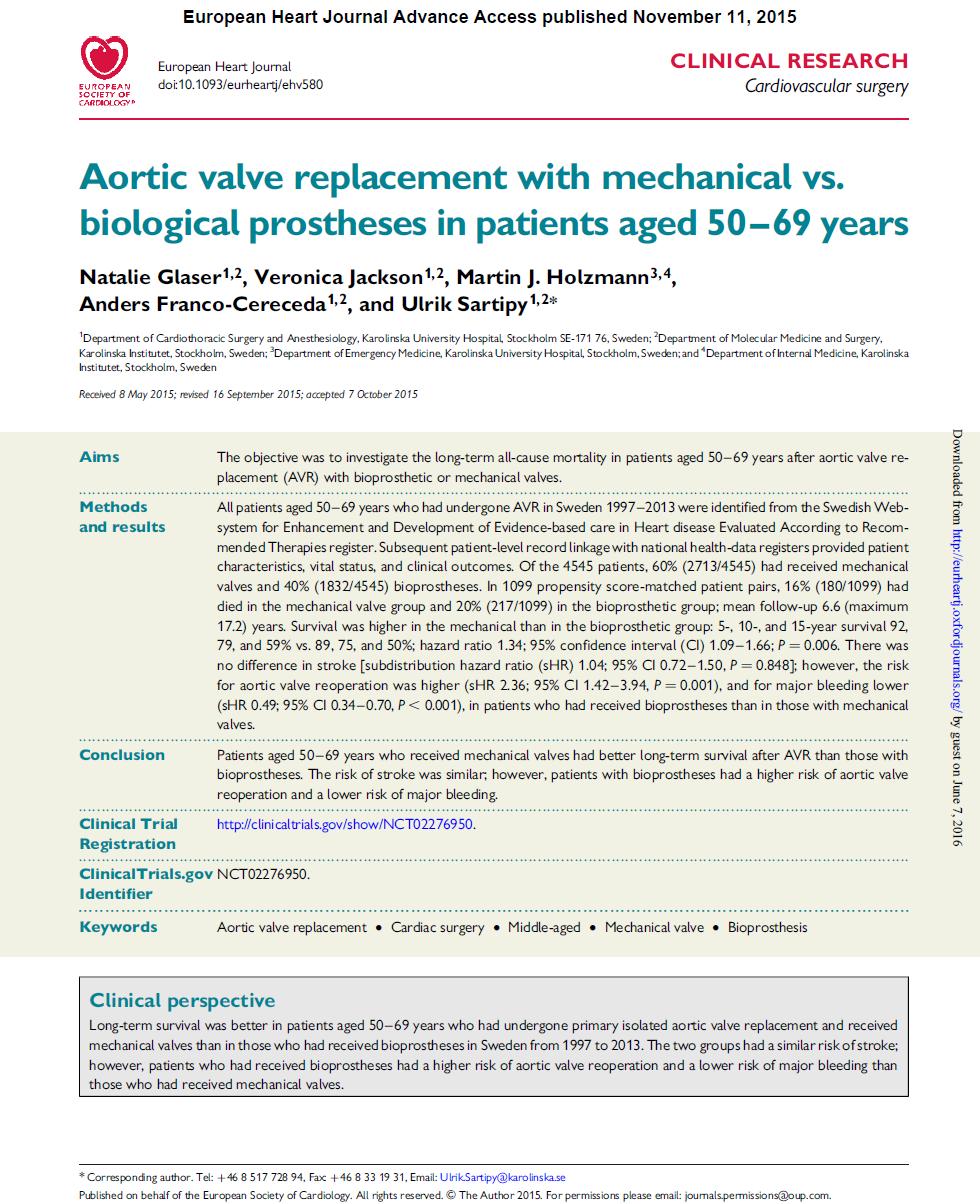
41 Long-term outcomes (Glaser Eur Heart J 2016)
42 ACC/AHA Guidelines
43 ESC/ EACTS Guidelines for the Management of Valvular Heart Disease «In the absence of a perfect quantitative score, the risk assessment should mostly rely on the clinical judgement of the heart team in addition to a combination of scores» European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
44 Early AVR vs conservative strategy 197 asymptomatic patients with AS AVA 0.75 cm² and v.max 4.5 m/s or mean gradient 50 mmhg Mean age 63 yrs, mean Euroscore 3.7 Early surgery in 102 patients 57 propensity matched pairs Follow-up in 95 patients (Kang et al. Circulation 2010;121;1502-9)

45 AVR vs Conservative strategy (Tanigushi ;J Am Coll Cardiol 2015)


46 AVR vs conservative strategy All cause death Heart failure hospitalization

47
48
49
50 Natural history Medical therapy Surgery Guidelines
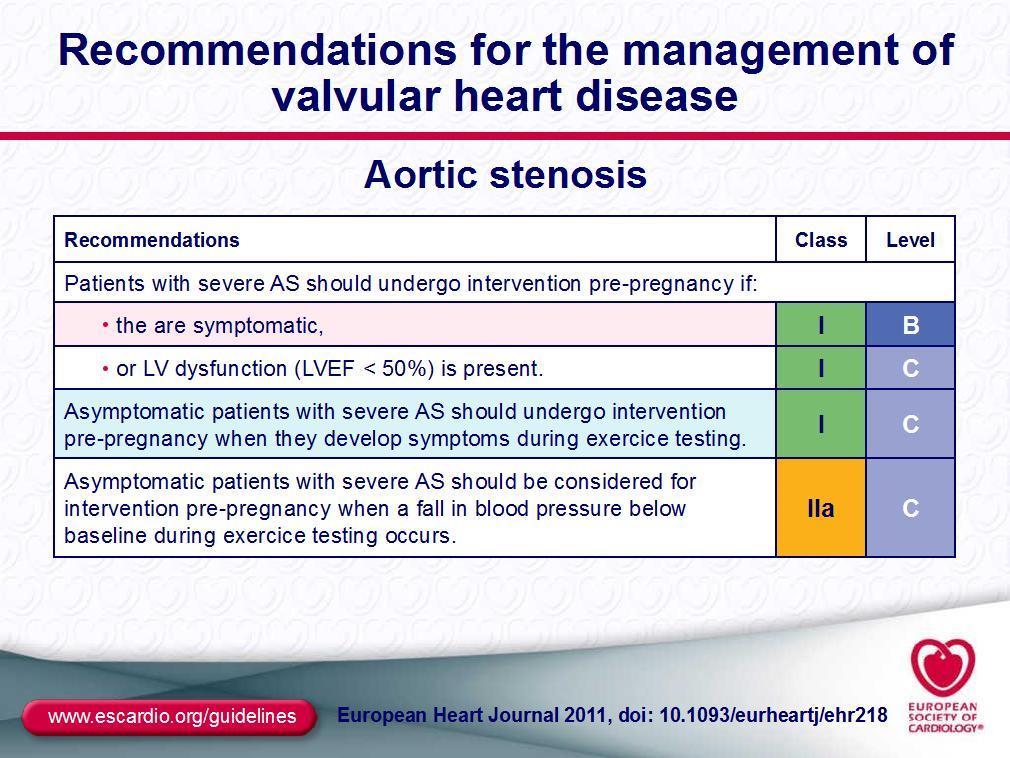
51 Indications for aortic valve replacement in asymptomatic aortic stenosis AVR is indicated in asymptomatic patients with severe AS and systolic LV dysfunction (LVEF < 50%) not due to another cause. AVR is indicated in asymptomatic patients with severe AS and abnormal exercise test showing symptoms on exercise clearly related to AS. AVR should be considered in asymptomatic patients with severe AS and abnormal excercise test showing fall in blood pressure below baseline. AVR should be considered in asymptomatic patients, with normal EF and none of the above mentioned exercise test abnormalities, if the surgical risk is low, and one or more of the following findings is present: very severe AS defined by a peak transvalvular velocity > 5.5 m/s, severe valve calcification and a rate of peak of transvalvular velocity progression 0.3 m/s per year. AVR may be considered in asymptomatic patients with severe AS, normal EF and none of the above mentioned exercise test abnormalities, if surgical risk is low, and one or more of the following findings is present: markedly elevated natriuretic peptide levels confirmed by repeated measurements without other explanations, increase of mean pressure gradient with exercise by > 20 mmhg, excessive LV hypertrophy in the absence of hypertension. Class I I IIa IIa IIb Level C C C C C European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
52 Management of severe aortic stenosis Severe AS Symptoms No Yes LVEF < 50% No Yes Contraindication for AVR No Physically active No Yes Exercise test Symptoms or fall in blood pressure below baseline Yes No High risk for AVR No Yes Yes Short life expectancy No Yes Presence of risk factors and low/intermediate individual surgical risk TAVI Med Rx No Yes AVR Re-evaluate in 6 months AVR or TAVI European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).

53 2012 ESC/EACTS v.s ACC/AHA Guidelines (Généreux et al. J Am Coll Cardiol 2016;67: )
54 ESC/EACTS Guidelines : Serial testing In the asymptomatic patient, the wide variability of the rate of progression of AS heightens the need for patients to be carefully educated about the importance of F.U. and reporting symptoms as soon as they develop. Stress tests should determine the recommended level of physical activity. Follow-up visits should include echocardiography with a focus on haemodynamic progression, LV function and hypertrophy, and the ascending aorta. Type and interval of follow-up should be determined on the basis of the index exam.. Asymptomatic severe AS should be re-evaluated at least every 6 months for the occurrence of symptoms, change in exercise tolerance (ideally using exercise testing if symptoms are doubtful), and change in echo parameters. Measurement of natriuretic peptides may be considered. In the presence of significant calcification, mild and moderate AS should be re-evaluated yearly.
55 Natural history Medical therapy Surgery Guidelines Specific situations
:doi:10.")
56 Management of patients with bicuspid valve disease European Heart Journal (2014):doi: /eurheartj/ehu281
57 Asymptomatic AS in the Elderly High prevalence Difficulties of watchful waiting AS is a progressive disease Impact of comorbidities, lifestyle Patient reluctancy Limitations of exercise testing Feasibility Lower predictive value (Das et al. Eur Heart J 2005;26: ) Possible need for non-cardiac surgery Higher risk of intervention
58 Management of severe aortic stenosis and elective non-cardiac surgery according to patient characteristics and the type of surgery Severe AS and need for elective non-cardiac surgery Symptoms No Yes Risk of non-cardiac surgery Low-moderate High Patient risk for AVR Patient risk for AVR High Low Low High Non-cardiac surgery Non-cardiac surgery under strict monitoring AVR before non-cardiac surgery Non-cardiac surgery under strict monigoring Consider BAV/TAVI European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
59
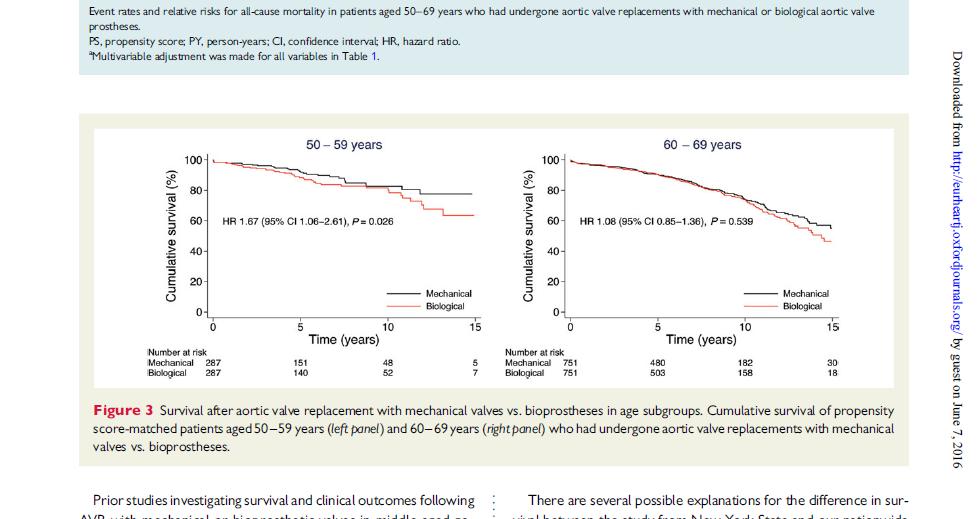
60 Perioperative course/symptoms Symptomatic AS Asymptomatic AS Control Total MACE (%) Death (%) Cardiac Non cardiac HF (%) (Tashiro T et al. Eur Heart J 2014;eurheartj.ehu044)
61
62

63 Indications for transcatheter aortic valve implantation TAVI should only be undertaken with a multidisciplinary heart team including cardiologists and cardiac surgeons and other specialists if necessary. TAVI should only be performed in hospitals with cardiac surgery onsite. TAVI is indicated in patients with severe symptomatic AS who are not suitable for AVR as assessed by a heart team and who are likely to gain improvement in their quality of life and to have a life expectancy of more than 1 year after consideration of their comorbidities. TAVI should be considered in high risk patients with severe symptomatic AS who may still be suitable for surgery, but in whom TAVI is favoured by a heart team based on the individual risk profile and anatomic suitability. Class I I I IIa Level C C B B European Heart Journal doi: /eurheartj/ehs109 & European Journal of Cardio-Thoracic Surgery doi: /ejcts/ezs455).
; p<0.0001 New AF(%) 5 28.3 5.9 29.2 New PM(%) 10.2 7.3 12.4 9.4 Valve area(cm²) 1.7±0.")
64 Comparison between Sapien 3 and surgery TAVI (963pts) Surgery (747pts) TAVI Surgery Death (%) Any stroke(%) Major vascular complication (%) AKI (%) days 1 Year TAVI is superior to AVR : Death,strokes,and moderate to severe AR H.R. -9.2%, 95%CI ( ); p< New AF(%) New PM(%) Valve area(cm²) 1.7± ± ± ±0.4 Moderate and severe AR (%) (Thourani,Lancet 2016)
65 More evidence to come on TAVI SURTAVI UK-TAVI PARTNER 3 Evolut R Low risk EARLY TAVR UNLOAD ACTIVATION POPULAR TAVI; GALILEO; ATLANTIS PORTICO IDE; SALUS; REPRISE III SOLVE TAVI; DIRECT; EASY TAVI
66 Conclusions Thanks to recent studies the prognosis of patients with asymptomatic AS can be better individualised. Exercise testing and the analysis of Vmax. are the main components of risk stratification. Guidelines are consistent for recommending surgery in selected patients with asymptomatic AS. Challenges remain: Low level of evidence Specific problems in the elderly Need for well designed randomized trials Evaluation of the role of TAVI
67 Thank you
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Transcatheter aortic valve implantation and pre-procedural risk assesment
 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Aortic Stenosis in the Elderly: Difficulties for the Clinician. Are Symptoms Due to Aortic Stenosis?
 Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic Stenosis in the Elderly: Difficulties for the Clinician Are Symptoms Due to Aortic Stenosis? Raphael Rosenhek Department of Cardiology Medical University of Vienna No disclosure European Society
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Severe Asymptomatic Aortic Stenosis
 Severe Asymptomatic Aortic Stenosis The Clinician s Perspective Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
Severe Asymptomatic Aortic Stenosis The Clinician s Perspective Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII
 Bichat hospital University Paris VII") When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
When is it too late to perform transcatheter mitral valve repair? Alec Vahanian, FESC,FRCP(Edin.) Bichat hospital University Paris VII I, (Alec Vahanian) DO have a financial interest/arrangement or affiliation
New Imaging for Aortic Valve Disease. Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego
 New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
New Imaging for Aortic Valve Disease Anthony DeMaria Judy and Jack White Chair Director, Sulpizio CV Center University of California, San Diego Imaging in Aortic Stenosis Valve morphology calcification
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
A new option for the Diagnosis and Management of Valvular Heart Disease. Oregon Comprehensive Valve Center
 A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
A new option for the Diagnosis and Management of Valvular Heart Disease Oregon Comprehensive Valve Center I have no disclosures Oregon Comprehensive Valve Center Weekly multidisciplinary case conferences
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
RANDOMISED TRIALS TAVI WITH SAVR STEPHAN WINDECKER AORTIC VALVE DISEASE COMPARING
 AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
AORTIC VALVE DISEASE RANDOMISED TRIALS COMPARING TAVI WITH SAVR STEPHAN WINDECKER DEPARTMENT OF CARDIOLOGY SWISS CARDIOVASCULAR CENTER AND CLINICAL TRIALS UNIT BERN BERN UNIVERSITY HOSPITAL, SWITZERLAND
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons
 Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Outcome of elderly patients with severe but asymptomatic aortic stenosis
 Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial
 in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial") Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Five-Year Outcomes of Transcatheter Aortic Valve Replacement (TAVR) in Inoperable Patients With Severe Aortic Stenosis: The PARTNER Trial Samir R. Kapadia, MD On behalf of The PARTNER Trial Investigators
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
TAVR in patients with. End-Stage CKD or in Renal Replacement Therapy:
 TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
TAVR in patients with End-Stage CKD or in Renal Replacement Therapy: Special Considerations and Prevention of early Valve Failure Antonios Chalapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens,
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
ESSENTIAL MESSAGES FROM
 ESSENTIAL MESSAGES FROM ESC GUIDELINES Committee for Practice Guidelines To improve the quality of clinical practice and patient care in Europe VHD ESC/EACTS Guidelines ON the Management OF VALVULAR HEART
ESSENTIAL MESSAGES FROM ESC GUIDELINES Committee for Practice Guidelines To improve the quality of clinical practice and patient care in Europe VHD ESC/EACTS Guidelines ON the Management OF VALVULAR HEART
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
2017 ESC/EACTS Guidelines for the management of valvular heart disease
 2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes
 Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Aortic Valve Stenosis: Flow and Gradient stratification and association with TAVR outcomes Kostis Raisakis General Hospital of Athens «G. Gennimatas» Severe Aortic Stenosis Peak Velocity 4 m/s Up to 40%
Cardiac catheterisation in AS
 AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Optimal Imaging Technique Prior to TAVI -Echocardiography-
 2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
2014 KSC meeting Optimal Imaging Technique Prior to TAVI -Echocardiography- Geu-Ru Hong, M.D. Ph D Associate Professor of Medicine Division of Cardiology, Severance Cardiovascular Hospital Yonsei University
Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc. (Hon.)
") Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc. (Hon.) DISCLOSURE As Editor, Current Problems in Cardiology Elsevier Honoraria for educational lectures from: American College of Cardiology Foundation;
Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc. (Hon.) DISCLOSURE As Editor, Current Problems in Cardiology Elsevier Honoraria for educational lectures from: American College of Cardiology Foundation;
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con
 TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
TAVR 2018: TAVR has high clinical efficacy according to baseline patient risk! ii. Con Dimitrios C. Angouras, MD, FETCS Associate Professor of Cardiac Surgery National and Kapodistrian University of Athens,
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
What the Cardiologist needs to know from Medical Images
 What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
What the Cardiologist needs to know from Medical Images Gerald Maurer Department of Cardiology Medical University of Vienna What kinds of Cardiologists Plumbers Electricians Photographers And then there
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
CIPG Transcatheter Aortic Valve Replacement- When Is Less, More?
 CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
CIPG 2013 Transcatheter Aortic Valve Replacement- When Is Less, More? James D. Rossen, M.D. Professor of Medicine and Neurosurgery Director, Cardiac Catheterization Laboratory and Interventional Cardiology
Improving Quality of Care for Patients with Heart Valve Disease
 Improving Quality of Care for Patients with Heart Valve Disease The Heart Team The Heart Valve Clinic Raphael Rosenhek Department of Cardiology Medical University of Vienna Eurovalve 2016 Brussels, March
Improving Quality of Care for Patients with Heart Valve Disease The Heart Team The Heart Valve Clinic Raphael Rosenhek Department of Cardiology Medical University of Vienna Eurovalve 2016 Brussels, March
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Suivi à long terme du TAVI: quelles leçons en 8rer? Dr Claire Boule, 17 Janvier 2015
 Suivi à long terme du TAVI: quelles leçons en 8rer? Dr Claire Boule, 17 Janvier 2015 Disclosures Research grants from: SFC, FFC, FRM, Servier Lectures: Novar,s, Daichii Sankyo Follow-up after TAVI Randomized
Suivi à long terme du TAVI: quelles leçons en 8rer? Dr Claire Boule, 17 Janvier 2015 Disclosures Research grants from: SFC, FFC, FRM, Servier Lectures: Novar,s, Daichii Sankyo Follow-up after TAVI Randomized
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines. Christophe Tribouilloy Amiens, France
 Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
DICE Session. The endocarditis team. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVR: Intermediate Risk Patients
 TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
TAVR: Intermediate Risk Patients Oscar A. Mendiz.MD.FACC.FSCAI Director Cardiology & Cardiovascular Institute (ICyCC) Chief Interventional Cardiology Department Board of Directors Hospital & Favaloro University
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes
 Original Article Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes Andrea Colli, Eleonora Bizzotto, Laura Besola, Dario Gregori, Francesca Toto, Erica Manzan,
Original Article Risk stratification of severe aortic stenosis according to new guidelines: long term outcomes Andrea Colli, Eleonora Bizzotto, Laura Besola, Dario Gregori, Francesca Toto, Erica Manzan,
Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy
 Mædica - a Journal of Clinical Medicine STATE TE-OF OF-THE THE-AR ART Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy Roxana Cristina SISU MD, Fellow in cardiology;
Mædica - a Journal of Clinical Medicine STATE TE-OF OF-THE THE-AR ART Timing for surgery in asymptomatic aortic valvular diseases a matter of controversy Roxana Cristina SISU MD, Fellow in cardiology;
Outcome of Patients With Aortic Stenosis, Small Valve Area, and Low-Flow, Low-Gradient Despite Preserved Left Ventricular Ejection Fraction
 Journal of the American College of Cardiology Vol. 60, No. 14, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.12.054
Journal of the American College of Cardiology Vol. 60, No. 14, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2011.12.054
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
TAVR IN INTERMEDIATE-RISK PATIENTS
 TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
TAVR IN INTERMEDIATE-RISK PATIENTS K. Lampropoulos MD, PhD, FESC, MEAPCI Interventional Cardiologist Evangelismos General Hospital The Burden of Valve Disease Prevalence Survival NATURAL HISTORY OF AS
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center
Program at Southcoast Health. Adam J. Saltzman, MD Cardiovascular Care Center") The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
The Transcatheter Aortic Valve Replacement (TAVR)Program at Southcoast Health Adam J. Saltzman, MD Cardiovascular Care Center Southcoast Health Disclosures Edwards Lifesciences: speaking honorarium Outline
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Transcatheter Aortic Valve Replacement TAVR
 Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
Transcatheter Aortic Valve Replacement TAVR Paul Gordon, MD Associate Prof of Medicine, Brown University Director, Cardiac Catheterization Laboratory The Miriam Hospital Disclosures: none 100 Symptomatic
B-type Natriuretic Peptide in VHD: a Non-imaging Helper for the Cardiologist. Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM
 B-type Natriuretic Peptide in VHD: a Non-imaging Helper for the Cardiologist Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None BNP Molecular Forms and Processing Brain
B-type Natriuretic Peptide in VHD: a Non-imaging Helper for the Cardiologist Dr. Julien Magne, PhD Sart Tilman Liège, BELGIUM Conflict of Interest Disclosure None BNP Molecular Forms and Processing Brain
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Balloon mitral valvuloplasty
 Echo for selecting and monitoring procedures in mitral valve diseases Balloon mitral valvuloplasty Eric Brochet,MD Cardiology Department Hôpital Bichat. Paris France Conflict of interest : none Balloon
Echo for selecting and monitoring procedures in mitral valve diseases Balloon mitral valvuloplasty Eric Brochet,MD Cardiology Department Hôpital Bichat. Paris France Conflict of interest : none Balloon
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Should early elective surgery be performed in patients with severe but asymptomatic aortic stenosis?
 European Heart Journal (2002) 23, 1417 1421 doi:10.1053/euhj.2002.3163, available online at http://www.idealibrary.com on Clinical Perspective Should early elective surgery be performed in patients with
European Heart Journal (2002) 23, 1417 1421 doi:10.1053/euhj.2002.3163, available online at http://www.idealibrary.com on Clinical Perspective Should early elective surgery be performed in patients with
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results
 Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Short Communication Bicuspid aortic root spared during ascending aorta surgery: an update of long-term results Marco Russo, Guglielmo Saitto, Paolo Nardi, Fabio Bertoldo, Carlo Bassano, Antonio Scafuri,
Aortic Stenosis: Background
 Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
Transcatheter Aortic Valve Replacement in Low Surgical Risk Patients Barry George, MD The Ohio State University Structural Heart Disease Course May 19 th, 2017 Aortic Stenosis: Background Severe Symptomatic
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Reverse left atrium and left ventricle remodeling after aortic valve interventions
 Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de