Jonathan D. Marmur, MD, FACC Professor of Medicine Director, Cardiac Catheterization and Interventional Cardiology. State University of New York
|
|
|
- Justina Ball
- 6 years ago
- Views:
Transcription

1 STEMI Management 2007 Jonathan D. Marmur, MD, FACC Professor of Medicine i Director, Cardiac Catheterization and Interventional Cardiology Health Science Center at Brooklyn State University of New York








2 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 06MM 0.6 ST-segment elevation MI 14MM 1.4 Non-ST-segment elevation ACS




3 The EKG is based on the string galvanometer invented in 1901 in Leiden, The Netherlands Willem Einthoven In 1924, Einthoven was awarded the Nobel Prize in Medicine Einthoven W. Un nouveau galvanometre. Arch Neerl Sc Ex Nat 1901;6:625 ARCHIVES NEERLANDAISES DES SCIENCES EXACTES ET NATURELLES

4 NSTEMI vs STEMI
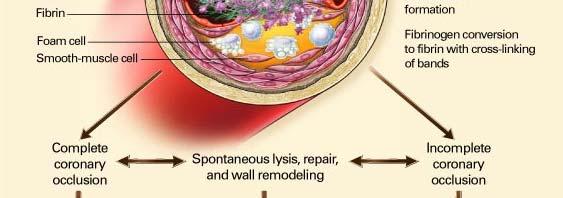
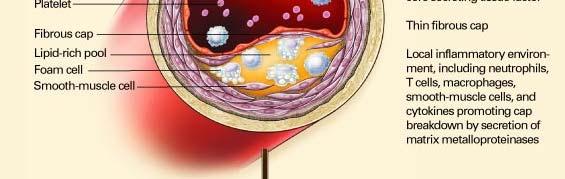
5 1980;303: Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction MA DeWood, J Spores, R Notske, LT Mouser, R Burroughs, MS Golden, and HT Lang To define the prevalence of total coronary occlusion in the hours after transmural myocardial infarction, we used coronary arteriography to study the degree of coronary obstruction in 322 patients admitted within 24 hours of infarction. Total coronary occlusion is frequent during the early hours of transmural infarction and decreases in frequency during the initial 24 hours, suggesting that coronary spasm or thrombus formation with subsequent recanalization or both may be important in the evolution of infarction.
6 ASA vs Placebo in ISIS-II: II: Odds of Vascular Death Astrological Gemini/Libra (n=1442) Birthsign All Others (n=7157) Odds ratio and 95% CI Play of chance Unrecognized randomization error True effect Prior MI Yes No Diabetic Yes No Sex Male Female Age < Systolic BP < Heart Rate < EKG BBB IMI AMI ST ALL PATIENTS (9.4 vs 11.8% mortality) 23% When in a trial with a clearly positive result many subgroups are considered, false negative results in some particular subgroups must be expected It is clear that the best estimate of the real effect is given by the overall results derived from all subgroups combined. Modified from: ISIS-2 Lancet 1988 Aug 13;2(8607): ASA better 1 Placebo better 1.5



7 Oral Anti-platelet Agents Sites of Action
8 Mo ortality (% %) COMMIT: Effect of Clopidogrel on Death in Hospital Placebo + ASA: 1846 deaths (8.1%) Clopidogrel + ASA: 1728 deaths (7.5%) 7% (SE3) relative risk reduction (2P=.03) Time (d Since Randomization [ 28 d) Adapted with permission from COMMIT Collaborative Group. Lancet. 2005;366:
9 CLARITY TIMI TIMI 28: Primary Endpoint Occluded Artery (or Death/MI Through Angio/HD) rtery or Death/MI (% %) % 21.7 Odds Reduction 15.0 Odds Ratio: 0.64 (95% CI, ) P=.001 Oc ccluded A 5 0 n=1752 n=1739 Clopidogrel Placebo Clopidogrel Better Placebo Better Sabatine MS et al N Engl J Med 2005;352:
10 ST Elevation Myocardial Infarction (STEMI) 8 6 Relationship Between Time to Reperfusion and Mortality: GUSTO-IIb 6.4 p= day mortality (%) < > 91 N: Time to PTCA (minutes) Berger et al. Circulation 1999;100:14
11 Wavefront Theory of Myocardial Loss min 3h 6h 24h 96h 0 3h 6h 24h Duration of occlusion Time post-occlusion Reimer et al Circulation 1977;56:786-94
12 19 Randomized Trials of PCI vs Lysis N = 5,066 12% 10% 10.0% Lysis PCI vent rate E 8% 6% 4% 2% 0% p= % 7.6% 6.7% p= % 72% 7.2% p< % Death Death (excl shock) Reinfarction Keeley, Grines; Lancet 2003
13 19 Randomized Trials of PCI vs Lysis N = 5,066 3% Lysis PCI 2.2% vent rate E 2% 1% 1.3% P< p= % 0% 008% 0.08% Hemorrhagic stroke Total stroke Keeley, Grines; in press
14 DANAMI-2: Patient Flow ST- elevation MI (n=1,900) Randomize 100 mg accelerated t-pa PCI (+ stent)
15 DANAMI-2 DENMARK 5.4 mill. inhabitants t 5 PCI centers 24 referral hospitals 62% of the Danish population Transport distance up to 95 US miles (mean 35 miles) 100 US miles
16 DANAMI-2: Primary Results (%) Death / MI / Stroke 16% 12% 8% 4% 14% Combined P= RRR 45% 8% Transfer Sites P= % 16% 14% 12% 8% 4% RRR 40% 9% 12% 8% 4% Non-Transfer Sites P= % RRR 45% 7% 0% 0% 0% Lytic Primary PCI Lytic Primary PCI Lytic Pi Primary PCI
, is presented.")
17 2007;99: Mortality with PCI with different delays to therapy compared with immediate thrombolytic therapy. A patient s baseline mortality risk, assuming treatment with thrombolytic therapy at 30 minutes (x axis), is presented. A 70-year-old patient s expected mortality with PCI at different ECG-to-needle times for a given baseline risk (multiple solid lines) is displayed, with prediction intervals (gray areas). Patients at low risk (baseline mortality risk 5%) have similar mortality outcomes regardless of delay. When delay to therapy is short (e.g., ECG-to-needle time 90 minutes), the degree of benefit increases with increasing baseline risk. However, when delay to therapy is longer (e.g., ECG-to-needle time 150 minutes), increasing baseline risk is associated with a higher probability of harm. At an ECG-to-needle time of 130 minutes (representing a PCI-related delay of 100 minutes compared with thrombolysis), mortality outcomes are expected to be roughly similar with either form of reperfusion across the spectrum of baseline risk.
18 Monday, November 13, 2006, 12:01 a.m. CT The American College of Cardiology and Partners Launch National Alliance To Reduce Door-to-Balloon (D2B) Times D2B alliance aims to save time and lives CHICAGO - The American College of Cardiology (ACC), together with the American Heart Association (AHA) and other key national healthcare organizations, announces the launch of its latest quality campaign, Door to Balloon (D2B): An Alliance for Quality. A Guidelines Applied in Practice (GAP) Program, the D2B campaign is aimed at improving the timeliness of lifesaving therapy for patients with heart attacks at the nation s hospitals that perform emergency angioplasty. Previously published guidelines developed by the ACC and the AHA recommend that hospitals treating STEMI patients with percutaneous coronary intervention (PCI) should reliably achieve a door-to-balloon time of 90 minutes or less. However, accomplishing this level of performance is an organizational challenge and many patients are not treated within the guideline recommendation

19 Six Evidence-Based Strategies Adopted at SUNY Downstate Having ED physicians activate cath lab. Using a single call to activate the cath lab. Having the cath-lab team arrive and be ready within 20 to 30 minutes. Providing real-time data feedback Having commitment from management. Using a team-based approach spanning multiple departments. Percent of C ases Door to Balloon Time Within Guidelines Y 2004 Y 2005 Y 2006 Y 2007 <90 min as of 3rd Q 2006




20 Treatment Delays Prehospital assessment ED care Those associated with the cath lab Transport
21 2007;99: We developed a protocol empowering paramedics to identify and directly triage patients with STEMI to a prealerted PCI hospital. This study assessed time to PCI and in-hospital mortality using this protocol compared with other patterns of arrival. Paramedics were educated in EKG criteria for STEMI. Medtronic LIFEPAK 12 defibrillators were used to obtain an initial EKG on all field patients with suspected MI. Paramedic identified patients with STEMI were transported directly to a PCI hospital ED, often bypassing closer, referring hospitals. The PCI ED triage personnel, upon receipt of the paramedic alert, activated t the cath lab team.
22 2007;99:
23 Inclusion ST-segment elevation Myocardial infarction (MI), with any mention of location or combinations of locations (e.g., anterior, apical, basal, inferior, lateral, posterior, or combination), IF DESCRIBED AS ACUTE/EVOLVING (e.g., posteriorami ) Q wave AMI Q wave MI, IF DESCRIBED AS ACUTE/EVOLVING ST ST abnormality consistent with injury, infarct, or acute/evolving MI ST changes consistent t with injury, infarct, or acute/evolving MI ST consistent with injury, infarct, or acute/evolving MI ST-elevation (STE) ST-elevation myocardial infarction (STEMI) ST-segment noted as.10mv ST-segment noted as 1 mm Transmural AMI Transmural MI, IF DESCRIBED AS ACUTE/EVOLVING Left bundle branch block (LBBB) Intraventricular conduction delay of LBBB type Variable LBBB Exclusion ST-segment elevation Non Q wave MI (NQWMI) Non ST-elevation MI (NSTEMI) ST clearly described as confined to ONE lead ST described as minimal, <.10mV, <1 mm, non-diagnostic, or non-specific inall leads noted to have ST-elevation ST-elevation clearly described as confined to ONE lead ST-elevation described as minimal, <.10mV, < 1 mm, nondiagnostic, or nonspecific in ALL leads noted to have STelevation ST-elevation due to early repolarization ST-elevation due to left ventricular hypertrophy (LVH) ST-elevation due to normal variant ST-elevation with mention of pericarditis ST-elevation with mention of Pit Printzmetal/Printzmetal's tl/pit tl' variant ST-segment elevation, or any of the other ST-segment elevation inclusion terms, described using one of the negative modifiers or qualifiers listed in Appendix H, Table 2.6, Qualifiers and Modifiers Table ST-elevation elevation, or any of the other STsegment elevation inclusion terms, with mention of pacemaker/pacing (unless atrial only) Left bundle branch block (LBBB) Incomplete left bundle branch block (LBBB) Intraventricular conduction block Intraventricular conduction delay(ivcd) Left bundle branch block (LBBB), or any of the other left bundle branch block inclusion terms, described using one of the negative modifiers or qualifiers listed in Appendix H, Table 2.6, Qualifiers and Modifiers Table Left bundle branch block (LBBB), or any of the other left bundle branch block inclusion terms, with mention of pacemaker/pacing (unless atrial only)
24 Definitions Definition: A percutaneous coronary intervention (PCI) is considered non-primary when it is used for reasons that are not emergent in nature. Non-primary PCIs include elective, rescue, and salvage PCIs. In contrast, a primary PCI is the use of a percutaneous reperfusion procedure in the acute phase of ST-segment elevation MI (usually within 12 hours or less from the onset of ischemic symptoms) with the goal of restoring blood flow to the affected myocardium, thereby improving outcomes including reduced mortality rates.
25 Reasons for Delay System reasons for delay are not acceptable, regardless of any linkage to the timing of PCI/reperfusion. ο Equipment-related (e.g., unavailability, malfunction) ο Staff-related (e.g., waiting for cath lab staff) ο Participation in clinical trial (e.g., waiting for trials coordinator) ο Consultation with other clinician ο Cath lab unavailability (e.g., no open cath lab) The linkage between a non-system reason and the timing/delay of PCI/reperfusion/cath/transfer to cath lab must be made clear somewhere in the medical record. Abstractors should NOT make inferences from documentation of a sequence of events alone or otherwise attempt to interpret from documentation. Clinical judgment should not be used in abstraction.
26 Reasons for Delay Examples of ACCEPTABLE documentation: H Hold on PCI. Will do TEE to r/o aortic dissection. Patient waiting for family and clergy to arrive wishes to consult with them before PCI. Pt. presented to ER in full cardiac arrest. ACLS protocol instituted. Unable to do PCI until patient stable. He had to be defibrillated several times prior to transfer to cath lab. SVG Angiojet cath did not cross lesion. XMI catheter successfully crossed the stenosis. Flow reestablished after 30 min. delay. PCI delayed due to intermittent hypotensive episodes when crossing lesion. o Note: Initial patient/family refusal of PCI/reperfusion/cath/transfer to cath lab is an acceptable reason for delay and does NOT need to be linked to the timing/delay in PCI.
27 Reasons for Delay Examples of UNACCEPTABLE documentation: Patient is discussing PCI with family. (Effect on timing/delay of PCI not documented) Patient developed v fib and cardiorespiratory arrest. Defib x 2, intubated. To cath lab for PCI. (Linkage to timing/delay of PCI not clear Abstractor should not infer from sequence of events) ST-elevation on initial ECG resolved. Chest pain now recurring. To cath lab for PCI. (Linkage to timing/delay of PCI not clear requires clinical judgment) Cath contraindicated too high risk. (Effect on timing/delay of PCI not documented) d) PCI not indicated. (Effect on timing/delay of PCI not documented) During the Angiojet thrombectomy, the patient had bradycardia which required pacing. (Effect on timing/delay i of PCI not documented) d) If unable to determine whether a documented reason is system in nature, or if physician/apn/pa documentation does not establish a linkage between event(s)/condition(s) and the timing/delay in PCI/reperfusion/cath/transfer to cath lab, select No.
28 False Positive STEMI
29
30
31
32
33
34
35 True Positive STEMI
36
37
38 Reciprocal Changes Wall Affected Leads Showing ST Segment Elevation Leads Showing Reciprocal ST Segment Depression Septal V1, V2 None LAD Anterior V3, V4 None LAD Anteroseptal eosepa V1, V2, V3, V4 None LAD Anterolateral Extensive anterior (Sometimes called Anteroseptal with Lateral extension) V3, V4, V5, V6, I, avl V1,V2,V3, V2 V3 V4, V5, V6, I, avl II, III, avf II, III, avf Suspected Culprit Artery LAD, or CIRC Left Main Inferior II, III, avf I, avl RCA or CIRC Lateral I, avl, V5, V6 II, III, avf CIRC Posterior (Usually associated with Inferior or Lateral but can be isolated) Right Ventricular (Usually associated with Inferior) V7, V8, V9 V1,V2,V3, V4 PDA II, III, avf, V1, V4R I, avl RCA
39
40 IMI due to OM1 (old total RCA); patent LAD
41 IMI due to proximal RCA occlusion; patent LAD
42 Algorithm for EKG Identification of the Infarct Related Artery in Anterior MI Zimetbaum et al NEJM 2003;348:
43 Algorithm for EKG Identification of the Infarct Related Artery in IMI Zimetbaum et al NEJM 2003;348:
44
45 The Evolution of Optimal Myocardial Infarction Therapy Eisenhower Year: Cheney Therapy: Morphine Angioplasty/Stent Heparin Heparin Warfarin Aspirin Atropine Abciximab Clopidogrel pd β-blocker Statin Bd Bed Rest: 7 Weeks < 2 Days Expected Mortality: 30% < 5%
Pathophysiology of ACS
 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Improving STEMI outcomes in Denmark. Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark
 Improving STEMI outcomes in Denmark Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark Presenter Disclosure Information Study funded by Fondation Leducq Michael Rahbek Schmidt The
Improving STEMI outcomes in Denmark Michael Rahbek Schmidt, MD, PhD. Aarhus University Hospital Skejby Denmark Presenter Disclosure Information Study funded by Fondation Leducq Michael Rahbek Schmidt The
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki. 2013, American Heart Association
 NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
NEBRASKA STEMI CONFERENCE 2015 Dr. Doug Kosmicki 2013, American Heart Association 1 Dr. Doug Kosmicki Reperfusion Strategies Disclosure Information Report any disclosure information of conflicts of interest.
Patient Transfer. Mark de Belder The James Cook University Hospital Middlesbrough
 Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Patient Transfer Mark de Belder The James Cook University Hospital Middlesbrough Current Management Strategies for ACS ACS No ST Elevation ST ST Elevation Elevation Early Invasive Early Conservative Fibrinolysis
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
APPENDIX F: CASE REPORT FORM
 APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
APPENDIX F: CASE REPORT FORM Instruction: Complete this form to notify all ACS admissions at your centre to National Cardiovascular Disease Registry. Where check boxes are provided, check ( ) one or more
OUTCOME OF THROMBOLYTIC AND NON- THROMBOLYTIC THERAPY IN ACUTE MYOCARDIAL INFARCTION
 OUTCOME OF THROMBOLYTIC AND NON- THROMBOLYTIC THERAPY IN ACUTE MYOCARDIAL INFARCTION FEROZ MEMON*, LIAQUAT CHEEMA**, NAND LAL RATHI***, RAJ KUMAR***, NAZIR AHMED MEMON**** OBJECTIVE: To compare morbidity,
OUTCOME OF THROMBOLYTIC AND NON- THROMBOLYTIC THERAPY IN ACUTE MYOCARDIAL INFARCTION FEROZ MEMON*, LIAQUAT CHEEMA**, NAND LAL RATHI***, RAJ KUMAR***, NAZIR AHMED MEMON**** OBJECTIVE: To compare morbidity,
Sanford Chest Pain Network: Improving Rural STEMI Outcomes
 Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
Sanford Chest Pain Network: Improving Rural STEMI Outcomes Naveen Rajpurohit, MD Cardiovascular Fellow Sanford Cardiovascular Institute Sanford Heart Hospital The University of South Dakota Sioux Falls,
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
Thrombus Aspiration before PCI: Routine Mandatory. Professor Clinical Cardiology Academic Medical Center University of Amsterdam
 Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
Seoul, 27 April TCT AP 2010 Thrombus Aspiration before PCI: Routine Mandatory Robbert J de Winter MD PhD FESC Professor Clinical Cardiology Academic Medical Center University of Amsterdam AMC Amsterdam
12 Lead Electrocardiogram (ECG) PFN: SOMACL17. Terminal Learning Objective. References
 PFN: SOMACL17. Terminal Learning Objective. References") 12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network:
 The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28 STEMI = Acute Coronary Thrombosis STEMI
The Role of DHMC as an ST Elevation Myocardial Infarction Receiving Center in a Regional STEMI Care Network: Nathaniel Niles, MD CREST Symposium November 7th, 28 STEMI = Acute Coronary Thrombosis STEMI
Myocardial Infarction In Dr.Yahya Kiwan
 Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
Myocardial Infarction In 2007 Dr.Yahya Kiwan New Definition Of Acute Myocardial Infarction The term of myocardial infarction should be used when there is evidence of myocardial necrosis in a clinical setting
The First 12 Hours. ST-Segment Elevation AMI: Introduction. Definitions
 ST-Segment Elevation AMI: The First 12 Hours Acute myocardial infarction (AMI) accounts for half of the deaths due to ischemic heart disease and is associated with significant use of resources. Because
ST-Segment Elevation AMI: The First 12 Hours Acute myocardial infarction (AMI) accounts for half of the deaths due to ischemic heart disease and is associated with significant use of resources. Because
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Eagles 2007 Focused Quality in EMS The Five Required Actions
 Eagles 2007 Focused Quality in EMS The Five Required Actions Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Prior
Eagles 2007 Focused Quality in EMS The Five Required Actions Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Prior
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Management of STEMI in era of Reperfusion. Eagles Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police
 Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Management of STEMI in era of Reperfusion Eagles 2007 Peter Moyer, MD, MPH Medical Director Boston EMS, Fire and Police STEMI in US ST Segment Elevation Myocardial Infarction (STEMI) ~500 K per year Thrombolysis
Controversies on Primary angioplasty in STEMI
 Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
Controversies on Primary angioplasty in STEMI 원주의대이승환 Case ( 51/M) CC C.C: ongoing squeezing chest pain D : for 2 hours Risk factors Current smoker ( 40 PYs) Hypercholesterolemia (+) Case ( 51/M) Physical
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
REFERRAL HOSPITAL. The Importance of Door In Door Out Time DIDO
 REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
REFERRAL HOSPITAL The Importance of Door In Door Out Time DIDO Jean Skonhovd,RN,BSN,MSAS Emergency Department Director Avera Heart Hospital of South Dakota Time to Treatment is critical for STEMI patients
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Frans Van de Werf, MD, PhD Leuven, Belgium
 STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
STEMI Cases and the ESC STEMI Guidelines Frans Van de Werf, MD, PhD Leuven, Belgium The Easy Case 2/21/2011 History and Risk Factors 50-year old male patient Past medical history: Teratoma right testis
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
Marcin Dada, MD December 03, 2013
 STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
12/18/2009 Resting and Maxi Resting and Max mal Coronary Blood Flow 2
 Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Ischemia and Infarction 103.10.07 Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Ischemia and Infarction 103.10.07 Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Critical Review Form Therapy Objectives: Methods:
 Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
Critical Review Form Therapy Clinical Trial Comparing Primary Coronary Angioplasty with Tissue-Plasminogen Activator for Acute Myocardial Infarction (GUSTO-IIb), NEJM 1997; 336: 1621-1628 Objectives: To
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
PPCI in STEMI. ESC at the 22nd Annual Conference of the Saudi Heart Association February 21th, 2011
 PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
PPCI in STEMI Dr Hassan Mhish Interventional Cardiology Consultant Cardiology Fellowship Program Director Prince Salman Heart Center King Fahd Medical City Riyadh, KSA ESC at the 22nd Annual Conference
Chapter 3 for 12 Lead Training -Precourse-
 ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
Coronary Interventions Indications, Treatment Options and Outcomes
 Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
Coronary Interventions Indications, Treatment Options and Outcomes A talk should be like a woman s skirt long enough to cover the subject, but short enough to keep it interesting. Coronary anatomy Physiology
The Strategic Reperfusion Early After STEMI study Implications for clinical practice
 The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
The Strategic Reperfusion Early After STEMI study Implications for clinical practice Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization and Interventional
Recurrent Thrombosis in a Case of Coronary Ectasia with Large Thrombus Burden Successfully Treated by Adjunctive Warfarin Therapy
 Case Report Acta Cardiol Sin 2013;29:462 466 Recurrent Thrombosis in a Case of Coronary Ectasia with Large Thrombus Burden Successfully Treated by Adjunctive Warfarin Therapy Hung-Hao Lee, 1 Tsung-Hsien
Case Report Acta Cardiol Sin 2013;29:462 466 Recurrent Thrombosis in a Case of Coronary Ectasia with Large Thrombus Burden Successfully Treated by Adjunctive Warfarin Therapy Hung-Hao Lee, 1 Tsung-Hsien
ECG in coronary artery disease. By Sura Boonrat Central Chest Institute
 ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
Ischemic Postconditioning During Primary Percutaneous Coronary Intervention Mechanisms and Clinical Application Jian Liu, MD FACC FESC FSCAI Chief Phy
 Ischemic Postconditioning During Primary Percutaneous Coronary Intervention Mechanisms and Clinical Application Jian Liu, MD FACC FESC FSCAI Chief Physician, Professor of Medicine Department of Cardiology,
Ischemic Postconditioning During Primary Percutaneous Coronary Intervention Mechanisms and Clinical Application Jian Liu, MD FACC FESC FSCAI Chief Physician, Professor of Medicine Department of Cardiology,
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Cardiac Ischemia ECG Workshop
 Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
STEMI in the State of Jefferson ASSET - 5 Years Later. Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center
 STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
STEMI in the State of Jefferson ASSET - 5 Years Later Brian W. Gross, MD, FACC Mary Barnum, RN, BSN Karen Bales, RN, BSN Rogue Valley Medical Center Sept 22, 2008 Percent # Procedures Performed Coronary
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Update on the management of STEMI. Elliot Rapaport, M.D. San Francisco, CA December 14, 2007
 Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Update on the management of STEMI Elliot Rapaport, M.D. San Francisco, CA December 14, 2007 Universal MI Definition Committee 2007 Recommendations Type 1 Spontaneous MI associated with ischemia and due
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies
 Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Recommendations for criteria for STEMI systems of care: A focus on pharmacoinvasive strategies Mohammad Zubaid, MB, ChB, FRCPC, FACC Professor of Medicine, Kuwait University Chairman, Faculty of Cardiology,
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI
 Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Effect of upstream clopidogrel treatment in patients with ST-segment elevation myocardial infarction undergoing primary PCI Dr Sasha Koul, MD Dept of Cardiology, Lund University Hospital, Lund, Sweden
Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks
 Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks Mark I. Langdorf, MD, MHPE, FACEP, FAAEM, RDMS Professor and Chair Associate Residency Director Department of Emergency Medicine University
Diagnosis of Myocardial Infarction/Ischemia with Bundle Branch Blocks Mark I. Langdorf, MD, MHPE, FACEP, FAAEM, RDMS Professor and Chair Associate Residency Director Department of Emergency Medicine University
Name Authentication Date (Position or Committee) Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee
 Quality & Patient Safety Steering. Meeting Minutes & 08/14 Committee") Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
Title: Document Number: Document Type: Affected Departments: Review Bodies: Revision/(Review) Dates: (Dates that included only a review, but no content 07/14 revision, are in parentheses) Effective Date:
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Electrocardiography. Hilal Al Saffar College of Medicine,Baghdad University
 Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ
 William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ PROBLEM: blood supply to the heart has been compromised and heart
William D. Salerno, M.D. Director, Coronary Care Unit Hackensack University Medical Center Clinical Associate Professor of Medicine, UMDNJ PROBLEM: blood supply to the heart has been compromised and heart
Thrombolysis in Acute Myocardial Infarction
 CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
CHAPTER 70 Thrombolysis in Acute Myocardial Infarction J. S. Hiremath Introduction Reperfusion of the occluded coronary artery at the earliest is the most important aim of management of STEMI. Once a flow
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI?
 SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
SHOULD A REGIONAL STEMI CENTRE ONLY OFFER PRIMARY PCI? Kurt Huber, MD 3 Department of Internal Medicine, Cardiology and Intensive Care Medicine, Wilhelminenhospital, Vienna, Austria Disclosures DISCLOSURE
Know the Quality of our Care at Every Step. Kansas City ACS Summit BI-State Cardiovascular Education Consortium
 Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
Know the Quality of our Care at Every Step Kansas City ACS Summit BI-State Cardiovascular Education Consortium Welcome to the Kansas City ACS Summit Objectives: Follow the flow and care of an ACS patient
1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11
 Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11") May 2011 1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11 Yes b) If confirmed please provide details on the number of
May 2011 1 a) Please confirm or deny whether your Trust has admitted patients for acute myocardial infarction in 2008/09, 2009/10 or 2010/11 Yes b) If confirmed please provide details on the number of
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Level One STEMI Connecting the Dots changing Points of Care into Systems of Care
 Level One STEMI Connecting the Dots changing Points of Care into Systems of Care Myron Bloom MD MMM Medical Director Rural Healthcare Quality Network RHQN.org drmbloom@msn.com The Eastern Washington Level
Level One STEMI Connecting the Dots changing Points of Care into Systems of Care Myron Bloom MD MMM Medical Director Rural Healthcare Quality Network RHQN.org drmbloom@msn.com The Eastern Washington Level
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
JAWDA Quarterly Waiting Time Guidelines for (Specialized and General Hospitals)
") JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
JAWDA Waiting Time Guidelines for (Specialized and General Hospitals) January 2019 Page 1 of 22 Table of Contents Executive Summary... 3 About this Guidance... 4 Performance Indicators... 5 APPENDIX -
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Critics of Thrombolytics: Is Pre-Hospital Clot-busting Actually a Bad Thing? David Persse, MD Houston Fire Department EMS
 Critics of Thrombolytics: Is Pre-Hospital Clot-busting Actually a Bad Thing? David Persse, MD Houston Fire Department EMS STEMI Stuff New or Recurrent MI s in U.S.: 865,000 Acute STEMI s: 500,000 Sooner
Critics of Thrombolytics: Is Pre-Hospital Clot-busting Actually a Bad Thing? David Persse, MD Houston Fire Department EMS STEMI Stuff New or Recurrent MI s in U.S.: 865,000 Acute STEMI s: 500,000 Sooner
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Treatment of ST-elevation myocardial infarction in China: Where are we?
 Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Treatment of ST-elevation myocardial infarction in China: Where are we? Associate Professor, Yihong Sun, MD Peking University People s Hospital Beijing, China Disclosure conflict of Interest The Challenges
Alphabetical Data Element List
 Alphabetical Data Element List Element Name Page # Collected For: Arrival Time 3 All Records Aspirin Received 6 OP-4 Birthdate 8 All Records Discharge Code 9 E/M Code 11 ECG 12 OP-5 ECG Date 13 OP-5 ECG
Alphabetical Data Element List Element Name Page # Collected For: Arrival Time 3 All Records Aspirin Received 6 OP-4 Birthdate 8 All Records Discharge Code 9 E/M Code 11 ECG 12 OP-5 ECG Date 13 OP-5 ECG
2018 Acute Coronary Syndrome. Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute
 2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
Clinical Lessons from BMC2-PCI
 Clinical Lessons from BMC2-PCI The Blue Cross Blue Shield of Michigan Cardiovascular Consortium Hitinder Gurm, M.D. University of Michigan Overview 32 papers since inception 10 papers published this year
Clinical Lessons from BMC2-PCI The Blue Cross Blue Shield of Michigan Cardiovascular Consortium Hitinder Gurm, M.D. University of Michigan Overview 32 papers since inception 10 papers published this year
Disclosures 1/25/2018. Mission: Quality Can Mission Lifeline Help Your Performance Improvement Program? None
 Mission: Quality Can Mission Lifeline Help Your Performance Improvement Program? Jeremy T Cushman, MD MS EMT-P FACEP FAEMS Associate Professor of Emergency Medicine and Public Health Sciences Chief, Division
Mission: Quality Can Mission Lifeline Help Your Performance Improvement Program? Jeremy T Cushman, MD MS EMT-P FACEP FAEMS Associate Professor of Emergency Medicine and Public Health Sciences Chief, Division
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
Cardiac Arrhythmias in Acute Coronary Syndrome. Roj Rojjarekampai, MD Thammasart Hospital 26/5/59
 Cardiac Arrhythmias in Acute Coronary Syndrome Roj Rojjarekampai, MD Thammasart Hospital 26/5/59 OUTLINE Management of tachy and brady-arrhytmia related ACS : AF : VA [ sustained VT /VF] : conduction disturbance
Cardiac Arrhythmias in Acute Coronary Syndrome Roj Rojjarekampai, MD Thammasart Hospital 26/5/59 OUTLINE Management of tachy and brady-arrhytmia related ACS : AF : VA [ sustained VT /VF] : conduction disturbance
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI
 INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Mission: Lifeline Addressing the System of STEMI Care
 Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
Mission: Lifeline Addressing the System of STEMI Care Alice K. Jacobs, M.D. Boston University Medical Center Boston, MA, USA ACC West Virginia Chapter, April 2017 Disclosure Information FINANCIAL DISCLOSURE:
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department
: Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department") ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
ST-segment Elevation Myocardial Infarction (STEMI): Optimal Antiplatelet and Anti-thrombotic Therapy in the Emergency Department decision-making. They have become the cornerstone of many ED protocols for
GWTG-CAD: Mission: Lifeline Focus July 2017 PMT FORM SELECTION. Pre-Hospital/Arrival
 GWTG-CAD: Mission: Lifeline Focus July 2017 PMT FORM SELECTION Page 1 Legend: BOLD = Required ^ = MLL Data Element Admin (Tab) ^Patient ID: Physician/Provider NPI: DOB: / / ^Arrival Date/Time: Race: Hispanic
GWTG-CAD: Mission: Lifeline Focus July 2017 PMT FORM SELECTION Page 1 Legend: BOLD = Required ^ = MLL Data Element Admin (Tab) ^Patient ID: Physician/Provider NPI: DOB: / / ^Arrival Date/Time: Race: Hispanic
Objectives 1/10/2013. Hospital Outpatient Quality Reporting Specifications Manual Updates January 1, 2013
 Hospital Outpatient Quality Reporting Specifications Manual Updates January 1, 2013 Wanda Johnson, OFMQ Casey Thompson, OFMQ Kari Johnston, OFMQ Hospital Outpatient Quality Reporting Program Announcements
Hospital Outpatient Quality Reporting Specifications Manual Updates January 1, 2013 Wanda Johnson, OFMQ Casey Thompson, OFMQ Kari Johnston, OFMQ Hospital Outpatient Quality Reporting Program Announcements
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical