RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in
|
|
|
- Bethany Holt
- 6 years ago
- Views:
Transcription
1 RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in Christopher P. Cannon Deepak L Bhatt, patients Jonas Oldgren, Gregory with YH Lip, atrial Stephen G Ellis, fibrillation Takeshi Kimura, Michael Maeng, Bela Merkely, Uwe Zeymer, Savion Gropper, Matias Nordaby, Eva Kleine, Ruth Harper, Jenny Manassie, James L Januzzi, Jurrien M ten Berg, Philippe Gabriel Steg and Stefan H Hohnloser On behalf of the steering committee and RE-DUAL PCI investigators
2 Antithrombotic therapy for atrial fibrillation and PCI NVAF PCI NVAF and PCI Anticoagulant therapy Anticoagulation superior to antiplatelet therapy ASA, acetylsalicylic acid; PCI, percutaneous coronary intervention Antiplatelet therapy Dual antiplatelet therapy superior to ASA alone BOTH anticoagulant and dual antiplatelet therapy = triple therapy High bleeding risk
3 Study Design: Multicenter, randomized, open-label trial following a PROBE design Patients with AF undergoing PCI with stenting N=2725 Randomization 120 hours post-pci* R Dabigatran 150 mg BID + P2Y12 inhibitor Dabigatran 110 mg BID + P2Y12 inhibitor Warfarin (INR ) + P2Y12 inhibitor + ASA 6-month minimum treatment duration with visits every 3 months for the first year, then visits and telephone contact alternating every 3 months and a 1-month post-treatment visit Mean duration of follow-up: ~14 months Dabigatran (110 or 150 mg) P2Y12 inhibitor Warfarin P2Y12 inhibitor 1 month of ASA (BMS) 3 months of ASA (DES) *Study drug should be administered 6 hours after sheath removal and no later than 120 hrs post-pci ( 72 hrs is preferable). PROBE, prospective, randomized, open, blinded endpoint; R, randomization; BMS, bare metal stent; DES, drug-eluting stent. ClinicalTrials.gov: NCT ; Cannon et al. Clin Cardiol 2016
4 Study objective and design RE-DUAL PCI tests the safety and efficacy of two regimens of dual therapy with dabigatran without aspirin vs triple therapy with warfarin The primary endpoint was time to first ISTH major or clinically relevant non-major bleeding Formally tested and powered endpoints included: Non-inferiority of 110 mg and 150 mg dual therapy groups on time to first ISTH major or clinically relevant non-major bleeding event. Non-inferiority of both dual therapy groups combined on time to first event of death, thromboembolic event (MI, stroke, systemic embolism) or unplanned revascularization Superiority testing of the bleeding endpoints 100% of outcome events were independently adjudicated by blinded external committee ISTH, International Society of Thrombosis and Haemostasis; MI, myocardial infarction Non-inferiority testing (margin 1.38)
5 Baseline characteristics Dabigatran 110 mg dual therapy (n=981) Warfarin triple therapy (n=981) Dabigatran 150 mg dual therapy (n=763) Corresponding Warfarin triple therapy (n=764) Age, years, mean (US, ROW), 70 (Japan), % <80 (US, ROW), <70 (Japan), % Male, % Baseline CrCl, ml/min, mean Diabetes mellitus, % CHA 2 DS 2 VASc score (mean) Modified HAS-BLED score at baseline (mean) ACS indication for PCI, % DES only, % ROW, rest of world
 Non-inferiority P<0.0001 P=0.")
6 Primary Endpoint: Time to first ISTH major or clinically relevant non-major bleeding event HR: 0.52 (95% CI: ) Non-inferiority P< P< Warfarin triple therapy HR: 0.72 (95% CI: ) Non-inferiority P< P=0.002 Warfarin triple therapy Probability of event (%) Dabigatran 110 mg dual therapy Dabigatran 150 mg dual therapy Time to first event (days) Time to first event (days) Full analysis set presented. HRs and Wald CIs from Cox proportional-hazard model. For the dabigatran 110 mg vs warfarin comparison, the model is stratified by age, non-elderly vs elderly (<70 or 70 in Japan and <80 or 80 years old elsewhere). For the dabigatran 150 mg vs warfarin comparison, an unstratified model is used, elderly patients outside the USA are excluded. Non-inferiority P value is one sided (alpha=0.025). Wald two-sided P value from (stratified) Cox proportional-hazard model (alpha=0.05)
7 Primary endpoint: ISTH major or clinically relevant non-major bleeding event Patients with outcome event (%) HR: 0.52 (95% CI: ) P< ARR: 11.5% 15.4% Dabigatran 110 mg dual therapy (n=981) 26.9% Warfarin triple therapy (n=981) HR: 0.72 (95% CI: ) P=0.002 ARR: 5.5% 20.2% Dabigatran 150 mg dual therapy (n=763) 25.7% Warfarin triple therapy (n=764) Wald two-sided P value from (stratified) Cox proportional-hazard model (alpha=0.05). ARR, absolute risk reduction
8 Rates of ISTH major bleeding Patients with outcome event (%) HR: 0.52 (95% CI: ) P= ARR: 4.2% 5.0% Dabigatran 110 mg dual therapy (n=981) 9.2% Warfarin triple therapy (n=981) HR: 0.64 (95% CI: ) P=0.022 ARR: 2.8% 5.6% Dabigatran 150 mg dual therapy (n=763) 8.4% Warfarin triple therapy (n=764) Wald two-sided P value from (stratified) Cox proportional-hazard model (alpha=0.05). ISTH major bleeding definition: fatal, critical organ (including intracranial haemorrhage), clinically overt bleeding with fall in Hb 2 g/dl. Hb, haemoglobin
9 Rate of intracranial haemorrhage 1,5 Patients with outcome event (%) 1 0,5 0 HR: 0.30 (95% CI: ) P=0.064 ARR: 0.7% 0.3% Dabigatran 110 mg dual therapy (n=981) 1.0% Warfarin triple therapy (n=981) HR: 0.12 (95% CI: ) P=0.047 ARR: 0.9% 0.1% Dabigatran 150 mg dual therapy (n=763) 1.0% Warfarin triple therapy (n=764) Wald two-sided P value from (stratified) Cox proportional-hazard model (alpha=0.05)
10 Time to death or thromboembolic event, or unplanned revascularization Patients with outcome event (%) HR: 1.04 (95% CI: ) Non-inferiority P= % 13.4% Dabigatran (combined dose) dual therapy Warfarin triple therapy Probability of event (%) Time to first event (days) Dabigatran (combined doses) dual therapy Warfarin triple therapy Non-inferiority P value is one sided (alpha=0.025). Results presented are Step 3 of hierarchical testing procedure, testing non-inferiority of dabigatran dual therapy (combined doses) to warfarin triple therapy in death or thromboembolic event and unplanned revascularization
11 Additional individual thromboembolic endpoints Dabigatran 110 mg dual therapy (n=981) n (%) Warfarin triple therapy (n=981) n (%) D110 DT vs warfarin TT Dabigatran Warfarin D150 DT vs warfarin TT 150 mg dual triple therapy therapy (n=764) (n=763) HR (95% CI) P value n (%) HR (95% CI) P value n (%) All-cause death 55 (5.6) 48 (4.9) 1.12 ( ) (3.9) 35 (4.6) 0.83 ( ) 0.44 Stroke 17 (1.7) 13 (1.3) 1.30 ( ) (1.2) 8 (1.0) 1.09 ( ) 0.85 Unplanned revascularization 76 (7.7) 69 (7.0) 1.09 ( ) (6.7) 52 (6.8) 0.96 ( ) 0.83 MI 44 (4.5) 29 (3.0) 1.51 ( ) (3.4) 22 (2.9) 1.16 ( ) 0.61 Stent thrombosis 15 (1.5) 8 (0.8) 1.86 ( ) (0.9) 7 (0.9) 0.99 ( ) 0.98 Results presented are times to event. Stent thrombosis is time to definite stent thrombosis
12 Additional individual thromboembolic endpoints Dabigatran 110 mg dual therapy (n=981) n (%) Warfarin triple therapy (n=981) n (%) D110 DT vs warfarin TT Dabigatran Warfarin D150 DT vs warfarin TT 150 mg dual triple therapy therapy (n=764) (n=763) HR (95% CI) P value n (%) HR (95% CI) P value n (%) All-cause death 55 (5.6) 48 (4.9) 1.12 ( ) (3.9) 35 (4.6) 0.83 ( ) 0.44 Stroke 17 (1.7) 13 (1.3) 1.30 ( ) (1.2) 8 (1.0) 1.09 ( ) 0.85 Unplanned revascularization 76 (7.7) 69 (7.0) 1.09 ( ) (6.7) 52 (6.8) 0.96 ( ) 0.83 MI 44 (4.5) 29 (3.0) 1.51 ( ) (3.4) 22 (2.9) 1.16 ( ) 0.61 Stent thrombosis 15 (1.5) 8 (0.8) 1.86 ( ) (0.9) 7 (0.9) 0.99 ( ) 0.98 Results presented are times to event. Stent thrombosis is time to definite stent thrombosis
13 Conclusions In patients with AF who have undergone PCI: Dual therapy with dabigatran and a P2Y12 antagonist significantly reduced the risk of bleeding versus warfarin triple therapy, with non-inferiority for overall thromboembolic events Absolute risk reductions with dabigatran dual therapy were 11.5% and 5.5% in ISTH major or clinically relevant non-major bleeding at the 110 mg and 150 mg doses, respectively, compared with warfarin triple therapy These dabigatran dual therapy regimens, using doses approved worldwide for stroke prevention, offer clinicians two additional options for managing Afib patients post-pci
14
15 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology Chairpersons: Borja Ibanez (Spain), Stefan James (Sweden). Authors/Task Force Members: Stefan Agewall (Norway), Manuel J. Antunes (Portugal), Chiara Bucciarelli-Ducci (UK), Héctor Bueno (Spain), Alida L. P. Caforio (Italy), Filippo Crea (Italy), John A. Goudevenos (Greece), Sigrun Halvorsen (Norway), Gerhard Hindricks (Germany), Adnan Kastrati (Germany), Mattie J. Lenzen (The Netherlands), Eva Prescott (Denmark), Marco Roffi (Switzerland), Marco Valgimigli (Switzerland), Christoph Varenhorst (Sweden), Pascal Vranckx (Belgium), Petr Widimský (Czech Republic). 15




16 Level of evidence A B C 21% Data derived from multiple randomized clinical trials or meta-analyses. Data derived from a single randomized clinical trial or large non-randomized studies. Consensus of opinion of the experts and/or small studies, retrospective studies, registries. 159 recommendations based on 477 references C 78 49% 37 23% 44 28% B A 16





17 Class I Classes of recommendations Classes Definition Evidence and/or general agreement that a given treatment or procedure is beneficial, useful, effective. Suggested wording Recommended/ is indicated. 159 recommendations 13 IIb 8% III 16 10% Class III Class IIa Class IIb Weight of evidence/opinion is in favour of usefulness/efficacy. Usefulness/efficacy is less well established by evidence/opinion. Evidence or general agreement that the given treatment or procedure is not useful/effective, and in some cases may be harmful. Should be considered. May be considered. Not recommended. IIa 38 24% 92 58% I
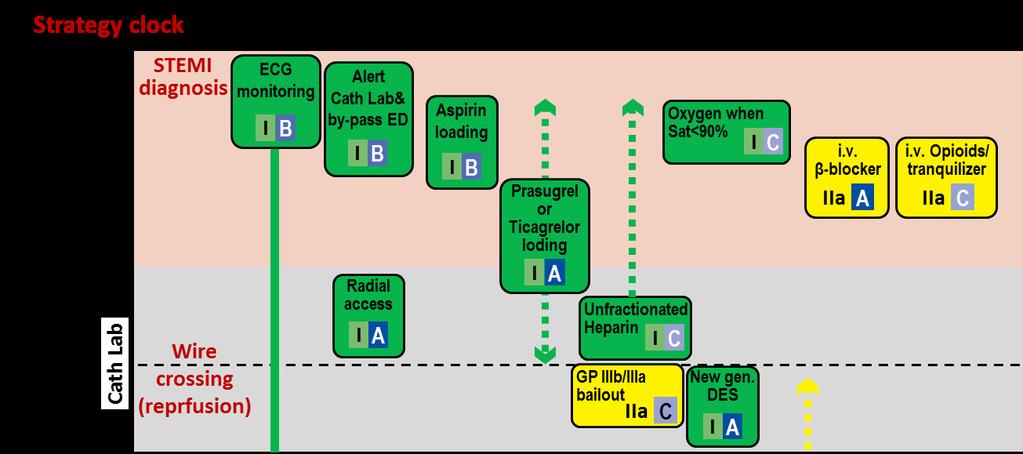
. Definition of time 0 to choose reperfusion strategy (i.e. the strategy clock starts at the time of STEMI diagnosis ).")
; 12-48h (Class IIa); >48h (Class III).")
18 What is new in 2017 Guidelines on AMI-STEMI MINOCA AND QUALITY INDICATORS: New chapters dedicated to these topics NEW / REVISED CONCEPTS STRATEGY SELECTION AND TIME DELAYS: Clear definition of first medical contact (FMC). Definition of time 0 to choose reperfusion strategy (i.e. the strategy clock starts at the time of STEMI diagnosis ). Selection of PCI over fibrinolysis: when anticipated delay from STEMI diagnosis to wire crossing is 120 min. Maximum delay time from STEMI diagnosis to bolus of fibrinolysis agent is set in 10 min. Door-to-Balloon term eliminated from guidelines. TIME LIMITS FOR ROUTINE OPENING OF AN IRA: 0-12h (Class I); 12-48h (Class IIa); >48h (Class III). ELECTROCARDIOGRAM AT PRESENTATION: Left and right bundle branch block considered equal for recommending urgent angiography if ischaemic symptoms. TIME TO ANGIOGRAPHY AFTER FIBRINOLYSIS: Timeframe is set in 2-24h after successful fibrinolysis. PATIENTS TAKING ANTICOAGULANTS: Acute and chronic management presented. 18

19 Reperfusion strategies in the infarct-related artery according to time from symptoms onset 19
20 Modes of patient presentation, components of ischaemic time and flowchart for reperfusion strategy selection Patient delay EMS delay Total ischaemic time System delay STEMI diagnosis FMC: EMS <10 <10 FMC: Non-PCI centre Time to PCI? 120 min >120 min Primary PCI strategy Fibrinolysis strategy <90 <10 Reperfusion (Wire crossing) Reperfusion (Lytic bolus) Patient delay Primary <10 PCI STEMI strategy FMC: PCI centre diagnosis System delay Total ischaemic time Reperfusion (Wire crossing) <60 20


21 Modes of patient presentation, components of ischaemic time and flowchart for reperfusion strategy selection Patient delay EMS delay Total ischaemic time System delay STEMI diagnosis FMC: EMS <10 <10 FMC: Non-PCI centre Time to PCI? 120 min >120 min Primary PCI strategy Fibrinolysis strategy <90 <10 Reperfusion (Wire crossing) Reperfusion (Lytic bolus) Patient delay Primary <10 PCI STEMI strategy FMC: PCI centre diagnosis System delay Total ischaemic time Reperfusion (Wire crossing) <60 21
22 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Radial access DES over BMS Complete Revascularization Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge MATRIX EXAMINATION, COMFORTABLE-AMI, NORSTENT PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Oxygen when SaO2 <95% Same dose i.v in all patients OXYGEN TNK-tPA Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM 22
23 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Oxygen when SaO2 <95% Same dose i.v in all patients Radial access DES over BMS Complete Revascularization Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge OXYGEN TNK-tPA EXAMINATION, COMFORTABLE-AMI, NORSTENT Sabate et al. Lancet 2012;380: PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM MATRIX 23
24 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Oxygen when SaO2 <95% Same dose i.v in all patients Radial access DES over BMS Complete Revascularization Engstrom et al, Lancet 2015 Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge OXYGEN TNK-tPA EXAMINATION, COMFORTABLE-AMI, NORSTENT PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM MATRIX 24
25 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Frobert et al, NEJM 2013 Radial access DES over BMS Complete Revascularization Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge MATRIX EXAMINATION, COMFORTABLE-AMI, NORSTENT PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Jolly et al, NEJM 2015 Oxygen when SaO2 <95% Same dose i.v in all patients OXYGEN TNK-tPA Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM 25
26 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Oxygen when SaO2 <95% Same dose i.v in all patients Radial access DES over BMS Complete Revascularization Valgimigli et al, NEJM 2015 PRAMI, DANAMI-3-PRIMULTI, Shazad et al, Lancet 2014 CVLPRIT, Compare-Acute Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge OXYGEN TNK-tPA EXAMINATION, COMFORTABLE-AMI, NORSTENT TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM MATRIX 26
27 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Radial access DES over BMS Complete Revascularization Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge MATRIX EXAMINATION, COMFORTABLE-AMI, NORSTENT PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Oxygen when SaO2 <95% Same dose i.v in all patients OXYGEN TNK-tPA Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM 27
28 What is new in 2017 Guidelines on AMI-STEMI CHANGE IN RECOMMENDATIONS Radial access DES over BMS Complete Revascularization Thrombus Aspiration Bivalirudin Enoxaparin Early Hospital Discharge MATRIX EXAMINATION, COMFORTABLE-AMI, NORSTENT PRAMI, DANAMI-3-PRIMULTI, CVLPRIT, Compare-Acute TOTAL, TASTE MATRIX, HEAT-PPCI ATOLL, Meta-analysis Small trials & observational data Hofman et al. NEJM 2017 Oxygen when SaO2 <95% Same dose i.v in all patients OXYGEN TNK-tPA Oxygen when SaO2 <90% AVOID, DETO2X Half dose i.v. in Pts 75 years STREAM 28
29 What is new in 2017 Guidelines on AMI-STEMI Additional lipid lowering therapy if LDL >1.8 mmol/l (70 mg/dl) despite on maximum tolerated statins. IMPROVE-IT, FOURIER 2017 NEW RECOMMENDATIONS Complete revascularization during index primary PCI in STEMI patients in shock. Expert opinion Cangrelor if P2Y 12 inhibitors have not been given. CHAMPION Switch to potent P2Y 12 inhibitors 48 hours after fibrinolysis. Expert opinion Extend Ticagrelor up to 36 months in high-risk patients. PEGASUS-TIMI 54 Use of polypill to increase adherence. FOCUS Routine use of deferred stenting. DANAMI 3-DEFER I IIa IIb III 29
30 Routine therapies in the acute, subacute and FOURIER long-term phases IMPROVE- (continued) IT Recommendations Class Level Lipid lowering therapies It is recommended to start high-intensity statin therapy as early as possible, unless contra-indicated, and maintain it long term. An LDL-C goal of < 1.8 mmol/l (70 mg/dl) or a reduction of at least 50% if the baseline LDL-C is between 1.8 and 3.5 mmol/l (70 and 135 mg/dl) is recommended. It is recommended to obtain a lipid profile in all STEMI patients as soon as possible after presentation. In patients with LDL-C 1.8 mmol/l ( 70 mg/dl) despite a maximally tolerated statin dose who remain at high risk, further therapy to reduce LDL-C should be considered. NEJM, March NEJM, June 18, 2015 I I I IIa A B C A same updated no longer fasting new 30
31 Bonaca et al, NEJM 2015 What is new in 2017 Guidelines on AMI-STEMI Additional lipid lowering therapy if LDL >1.8 mmol/l (70 mg/dl) despite on maximum tolerated statins. IMPROVE-IT, FOURIER 2017 NEW RECOMMENDATIONS Complete revascularization during index primary PCI in STEMI patients in shock. Expert opinion Cangrelor if P2Y 12 inhibitors have not been given. CHAMPION Switch to potent P2Y 12 inhibitors 48 hours after fibrinolysis. Expert opinion Extend Ticagrelor up to 36 months in high-risk patients. PEGASUS-TIMI 54 Use of polypill to increase adherence. FOCUS Routine use of deferred stenting. DANAMI 3-DEFER I IIa IIb III 31

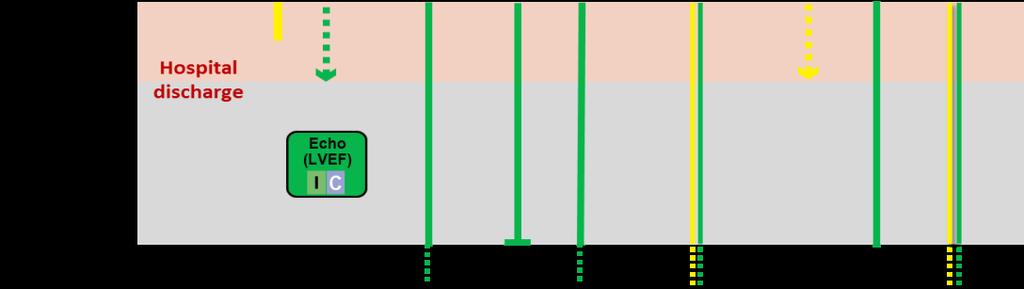
32 Do not forget interventions in STEMI patients undergoing a primary PCI strategy 32
 to choose primary PCI strategy over fibrinolysis (ifthis target time cannot be met, consider fibrinolysis).")
33 Summary of important time targets Intervals Maximum time from FMC to ECG and diagnosis. Maximum expected delay from STEMI diagnosis to primary PCI (wire crossing) to choose primary PCI strategy over fibrinolysis (ifthis target time cannot be met, consider fibrinolysis). Maximum time from STEMI diagnosis to wire crossing in patients presenting at primary PCI hospitals. Maximum time from STEMI diagnosis to wire crossing in transferred patients. Time targets 10 min 120 min 60 min 90 min NEW: The strategy clock starts at the time of STEMI diagnosis (not FMC) 33
34 34
Study design: multicenter, randomized, open-label trial following a PROBE design
 Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
2017 ESC Guidelines for the management of acute myocardial infarcnon in panents presennng with ST-segment elevanon
 2017 ESC Guidelines for the management of acute myocardial infarcnon in panents presennng with ST-segment elevanon The Task Force for the management of acute myocardial infarc6on in pa6ents presen6ng with
2017 ESC Guidelines for the management of acute myocardial infarcnon in panents presennng with ST-segment elevanon The Task Force for the management of acute myocardial infarc6on in pa6ents presen6ng with
2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation
 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Prof. Marco Roffi Geneva University Hospitals Geneva, Switzerland Declaration of interests:
2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Prof. Marco Roffi Geneva University Hospitals Geneva, Switzerland Declaration of interests:
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in patients with atrial fibrillation
 RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in patients with atrial fibrillation Christopher P. Cannon Deepak L Bhatt, Jonas Oldgren, Gregory YH Lip,
RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in patients with atrial fibrillation Christopher P. Cannon Deepak L Bhatt, Jonas Oldgren, Gregory YH Lip,
Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου
, FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου") Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018 Disclosures: None Primary efficacy outcome* (%/year) Antiplatelet Therapy
Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018 Disclosures: None Primary efficacy outcome* (%/year) Antiplatelet Therapy
Essential Messages from ESC Guidelines
 Essential Messages from ESC Guidelines Committee for Practice Guidelines AMI-STEMI 2017 Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation Essential
Essential Messages from ESC Guidelines Committee for Practice Guidelines AMI-STEMI 2017 Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation Essential
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ Χρήστος Δ.Καλλιάνος Α Καρδιολογικό τμήμα και Ηλεκτροφυσιολογικό Εργαστήριο ΓΝΑ «Ο Ευαγγελισμός»
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ Χρήστος Δ.Καλλιάνος Α Καρδιολογικό τμήμα και Ηλεκτροφυσιολογικό Εργαστήριο ΓΝΑ «Ο Ευαγγελισμός»
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
Additional Contributor: Glenn Levine (USA).
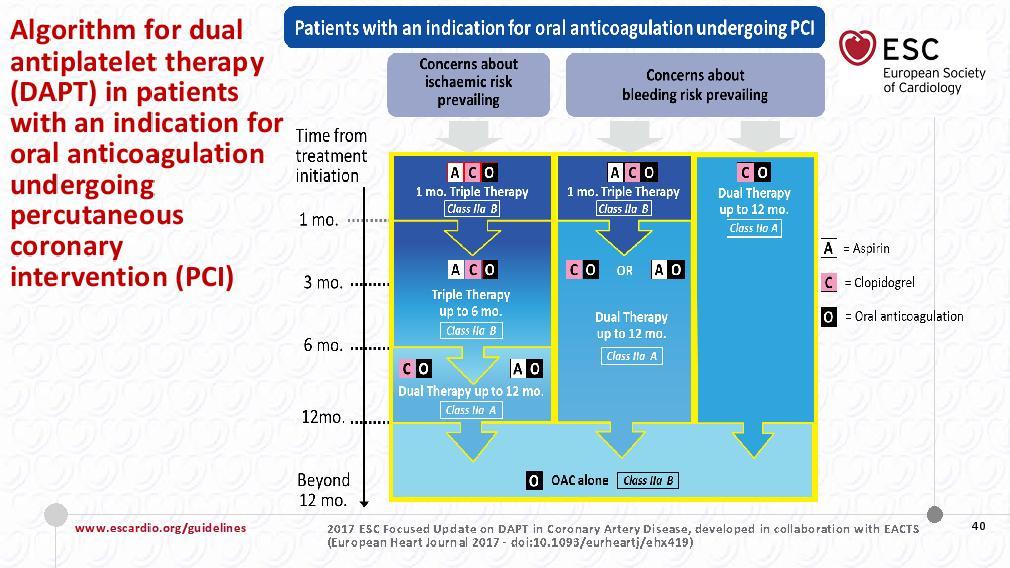
.") 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the Management
2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the Management
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Disclosure. Financial disclosure: National Advisory Board & Research Grant from Boehringer-Ingelheim
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting
 How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
How to approach non-infarct related artery disease in patients with STEMI in a limited resource setting Ahmed A A Suliman, MBBS, FACP, FESC Associate Professor, University of Khartoum Interventional Cardiologist,
Stable CAD, Elective Stenting and AFib
 Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές
 4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
After acute coronary syndromes patients continue to have recurrent ischemic events despite revascularization and dual antiplatelet therapy
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained
 Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
STEMI Linee guida ESC Maddalena Lettino, Italy
 STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
STEMI Linee guida ESC 2017 Maddalena Lettino, Italy Disclosure Speaker fee: Aspen, Astra Zeneca, BMS, Boehringer, Eli Lilly, DaichiiSankio, Bayer, Pfizer, Sanofi Advisory board member: Astra Zeneca, Eli
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom?
 Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom? Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Patients (%) Patients
Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom? Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Patients (%) Patients
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION. STREAM 1Y AHA 2013 P Sinnaeve
 STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
STREAM - ONE YEAR MORTALITY STRATEGIC REPERFUSION EARLY AFTER MYOCARDIAL INFARCTION PCI Hospital Ambulance/ER STREAM design STEMI
Meet the Guidelines Le principali novità che modificheranno la nostra pratica clinica: STEMI
 Meet the Guidelines 2017. Le principali novità che modificheranno la nostra pratica clinica: STEMI Guido Parodi Cardiologia Interventistica AOU Sassari Scuola di Specializzazione in Malattie dell Apparato
Meet the Guidelines 2017. Le principali novità che modificheranno la nostra pratica clinica: STEMI Guido Parodi Cardiologia Interventistica AOU Sassari Scuola di Specializzazione in Malattie dell Apparato
AF & CAD. Management and prognosis
 AF & CAD Management and prognosis Maria Agelaki Cons. Cardiologist Red Cross GN Hosp. AF and CAD share in common Most common arrhythmia and cardiovascular disease respectively High prevalence in general
AF & CAD Management and prognosis Maria Agelaki Cons. Cardiologist Red Cross GN Hosp. AF and CAD share in common Most common arrhythmia and cardiovascular disease respectively High prevalence in general
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
North Wales Cardiac Network Guidelines on oral antiplatelet therapy in cardiovascular disease
 Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원
 Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Acute coronary syndromes A European viewpoint. Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT
 Acute coronary syndromes A European viewpoint Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT Potential conflicts of interest In the past 2 years Felicita
Acute coronary syndromes A European viewpoint Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT Potential conflicts of interest In the past 2 years Felicita
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction
 Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Culprit PCI vs MultiVessel PCI for Acute Myocardial Infarction Dipti Itchhaporia, MD, FACC, FESC Trustee, American College of Cardiology Director of Disease Management, Hoag Hospital Robert and Georgia
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology
 Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
Thrombolysis in Cardiology to whom? Professor Steen D. Kristensen, MD, DMSc, FESC Department of Cardiology UNIVERSITY OF AARHUS 1 COI Speakers fee: Aspen, AZ, Bayer, BMS/Pfizer Departmental research grant:
DAPT Essential Messages from ESC Guidelines. Committee for Practice Guidelines
 2017 Essential Messages from ESC Guidelines Committee for Practice Guidelines DAPT Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease Essential Messages 2017 ESC focused update on dual
2017 Essential Messages from ESC Guidelines Committee for Practice Guidelines DAPT Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease Essential Messages 2017 ESC focused update on dual
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin
 Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin Marc S. Sabatine, MD, MPH on behalf of the PEGASUS-TIMI 54 Executive
Prevention of Cardiovascular Events in Patients With Prior Heart Attack Using Ticagrelor Compared to Placebo on a Background of Aspirin Marc S. Sabatine, MD, MPH on behalf of the PEGASUS-TIMI 54 Executive
Bivalirudin Clinical Trials Update Evidence and Future Perspectives
 Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction
 Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
STEMI AND MULTIVESSEL CORONARY DISEASE
 STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
STEMI AND MULTIVESSEL CORONARY DISEASE ΤΣΙΑΦΟΥΤΗΣ Ν. ΙΩΑΝΝΗΣ ΕΠΕΜΒΑΤΙΚΟΣ ΚΑΡΔΙΟΛΟΓΟΣ Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΝΟΣ ΕΡΥΘΡΟΥ ΣΤΑΥΡΟΥ IRA 30-50% of STEMI patients have additional stenoses other than the infarct related
Primary Prevention of Stroke
 Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Primary Prevention of Stroke Dr Chris Ellis Cardiologist Green Lane CVS Service, Auckland City Hospital & Auckland Heart Group, Mercy Hospital, Auckland 67 Pages Long, 735 References 29 Sub-Headings for
Antiplatelet Therapy in Patients on Anticoagulation
 Antiplatelet Therapy in Patients on Anticoagulation Ziad A Ali MD DPhil Cardiovascular Research Foundation Columbia University New York, Medical NY Center Cardiovascular Research Foundation Disclosure
Antiplatelet Therapy in Patients on Anticoagulation Ziad A Ali MD DPhil Cardiovascular Research Foundation Columbia University New York, Medical NY Center Cardiovascular Research Foundation Disclosure
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο)
") Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events
 Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
TRIAL UPDATE 1. ISAR TRIPLE SECURITY Trial. Dr Deven Patel Royal Free Hospital
 TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach
 Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Current Advances and Best Practices in Acute STEMI Management A pharmacoinvasive approach Frans Van de Werf, MD, PhD University Hospitals, Leuven, Belgium Frans Van de Werf: Disclosures Research grants
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia
 Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
ANTIPLATELET REGIMENS:
 ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Triple antithrombotic therapy following an acute coronary syndrome
 Triple antithrombotic therapy following an acute coronary syndrome prevalence, outcomes and prognostic utility of the HAS- BLED score Presented by: Nouf alanazi Supervised by: Dr.Khalid Alhabib Scenario
Triple antithrombotic therapy following an acute coronary syndrome prevalence, outcomes and prognostic utility of the HAS- BLED score Presented by: Nouf alanazi Supervised by: Dr.Khalid Alhabib Scenario
Robert C. Welsh, MD, FRCPC Professor of Medicine, University of Alberta Zone Clinical Department Head, Cardiac Sciences
 Managing Atrial Fibrillation and ACS/PCI Applying New Evidence to Clinical Practice Dual Anti-Thrombotic Therapy in Acute Coronary Syndromes (ACS) and Afib + PCI/ACS Patients Robert C. Welsh, MD, FRCPC
Managing Atrial Fibrillation and ACS/PCI Applying New Evidence to Clinical Practice Dual Anti-Thrombotic Therapy in Acute Coronary Syndromes (ACS) and Afib + PCI/ACS Patients Robert C. Welsh, MD, FRCPC
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction
 Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction The Bavarian Reperfusion Alternatives Evaluation (BRAVE) 4
Randomized Comparison of Prasugrel and Bivalirudin versus Clopidogrel and Heparin in Patients with ST-Segment Elevation Myocardial Infarction The Bavarian Reperfusion Alternatives Evaluation (BRAVE) 4
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome
 State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
Disclosures. Updates in Acute Coronary Syndromes 10/21/17. No Conflicts of Interest. Updates in Acute Coronary Syndromes. Krishan Soni, MD, MBA, FACC
 Disclosures Updates in Acute Coronary Syndromes No Conflicts of Interest Krishan Soni, MD, MBA, FACC Assistant Professor of Medicine Division of Cardiology Krishan.soni@ucsf.edu Updates in Acute Coronary
Disclosures Updates in Acute Coronary Syndromes No Conflicts of Interest Krishan Soni, MD, MBA, FACC Assistant Professor of Medicine Division of Cardiology Krishan.soni@ucsf.edu Updates in Acute Coronary
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial)
") UCR Uppsala Clinical Research Center Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial) Main results at 30 days Ole Fröbert, MD, PhD - on behalf of the TASTE investigators
UCR Uppsala Clinical Research Center Thrombus Aspiration in ST- Elevation myocardial infarction in Scandinavia (TASTE trial) Main results at 30 days Ole Fröbert, MD, PhD - on behalf of the TASTE investigators
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Controversies In STEMI Management
 Controversies In STEMI Management Professor Mohamed Sobhy, MD, FACC, FESC Professor of Cardiology Department, Alexandria University - Egypt Past President of the Egyptian Society of Cardiology President
Controversies In STEMI Management Professor Mohamed Sobhy, MD, FACC, FESC Professor of Cardiology Department, Alexandria University - Egypt Past President of the Egyptian Society of Cardiology President
Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved
 . Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
. Følgende dias er fremlagt ved DCS / DTS Fællesmøde 13. januar 2011 og alle rettigheder tilhører foredragsholderen. Gengivelse må kun foretages ved tilladelse Antithrombotic therapy in Atrial Fibrillation
Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation
 Original Article Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation Christopher P. Cannon, M.D., Deepak L. Bhatt, M.D., M.P.H., Jonas Oldgren, M.D., Ph.D., Gregory Y.H. Lip, M.D.,
Original Article Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation Christopher P. Cannon, M.D., Deepak L. Bhatt, M.D., M.P.H., Jonas Oldgren, M.D., Ph.D., Gregory Y.H. Lip, M.D.,
Days
 Post ACS Care 2013 Clinical dilemmas Christopher Granger, MD Professor of Medicine Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic
Post ACS Care 2013 Clinical dilemmas Christopher Granger, MD Professor of Medicine Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic
Pathophysiology of ACS
 Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Pathophysiology of ACS ~ 2.0 MM patients admitted to CCU or telemetry annually 0.6 MM ST-segment elevation MI 1.4 MM Non-ST-segment elevation ACS NSTEMI vs STEMI VANQWISH Boden et al N Engl J Med 1998;338:1785-1792
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Trial Update- TOTAL. Jonathan Byrne
 Trial Update- TOTAL Jonathan Byrne No conflicts of interest Background- rationale for thrombectomy Major Limitation of primary PCI: distal embolisation and reduced flow Stonel JACC 2002;39:591-7 Henriques
Trial Update- TOTAL Jonathan Byrne No conflicts of interest Background- rationale for thrombectomy Major Limitation of primary PCI: distal embolisation and reduced flow Stonel JACC 2002;39:591-7 Henriques
Subsequent management and therapies
 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY
ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation Subsequent management and therapies Marco Valgimigli, MD, PhD University of Ferrara ITALY