AKI in Hospitalized Patients ACOI 2017
|
|
|
- Gloria White
- 6 years ago
- Views:
Transcription
1 AKI in Hospitalized Patients ACOI 2017
2 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI
3 AKI Case 67 yo woman admitted with community acquired pneumonia. She has a history of DM II, CKD Stage 3 and HTN. Her medical treatment consists of metformin and lisinopril. She has a MAP < 65 on presentation with a lactate level of 3.3 and qsofa of 2. She is treated with 30 ml/kg isotonic fluid and appropriate antibiotics and admitted to the ICU
4 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI 6. Cases
5 Diagnostic criteria Acute Kidney Injury An abrupt (within 48 hours) reduction in kidney function currently defined as an absolute increase in serum creatinine of more than or equal to 0.3 mg/dl ( 26.4 μmol/l), a percentage increase in serum creatinine of more than or equal to 50% (1.5-fold from baseline), or a reduction in urine output (documented oliguria of less than 0.5 ml/kg per hour for more than six hours). Sustained prerenal resolves over 72 hours
6 Definition of Acute Renal Failure Acute Renal Failure is a decline in renal function (UO and solute clearance) which is abrupt and sustained Abrupt over 48 hours Sustained for > 24 hours Severity AKI Staging
7
8
9 ARF AKI Staging The presence of AKI ( even Stage 1) predicts increased mortality, LOS, hospital costs, and need for RRT The AKI definition is both sensitive and specific to diagnose ARF (ascertainment bias) The worse the stage, the worse the prognosis of the patient, longer hospital LOS, ICU LOS, higher cost and higher mortality
10 AKI Case LABS: 2.8 BC grow Strep pneumonia Creatinine: baseline 1.4 admission 1.8 day 1 Urine output 1000/24 hrs (< 0.5 ml/kg)
11 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI
12 AKI Incidence 20% of hospitalized patients have AKI 50% of ICU patients have AKI Incidence is increasing Mortality is static at 33% for all and 50% ICU
13
14 AKI Complications - Immediate Short term mortality 33% all and 50% ICU Higher the AKI Stage the higher the mortality Longer the course the higher the mortality Patients with AKI are: more likely to die of sepsis, develop respiratory failure and require long term and short term nursing care

15 ARF and Mortality Chertow 2005

16
17 AKI Complications Long Term There are long term effects from AKI Higher total and CV mortality Faster progression of CKD Higher rates of ESRD
18 Association between AKI and cardiovascular mortality and cardiovascular events. Ayodele Odutayo et al. JASN 2017;28:
19 One-year survival after percutaneous coronary intervention in patients with or without CKD and with or without CIN (4). Rudnick M, Feldman H CJASN 2008;3:
20
21 AKI Case Patient developed respiratory failure requiring mechanical ventilation for 7 days and NSTEMI Her renal function worsened but she never required dialysis She was discharge to rehabilitation and then home. Her GFR is 20 ml/min after 90 days
22 Kaplan-Meier survival estimates by septic acute kidney injury Bagshaw, S. M. et al. Clin J Am Soc Nephrol 2007;2:
23 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI 6. Cases
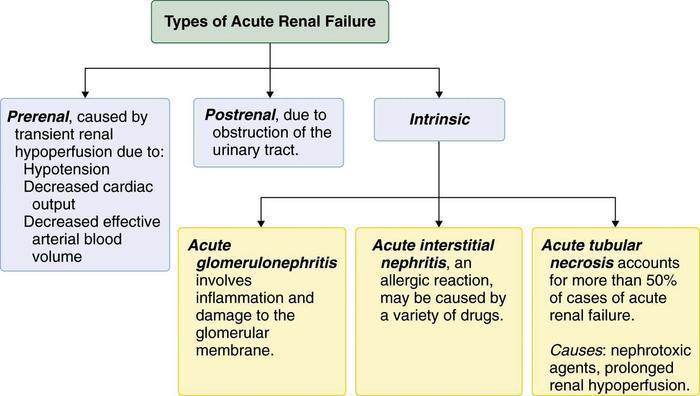
24 Etiology of AKI Outpatient Inpatient Prerenal Intrarenal Obstruct Idiopath
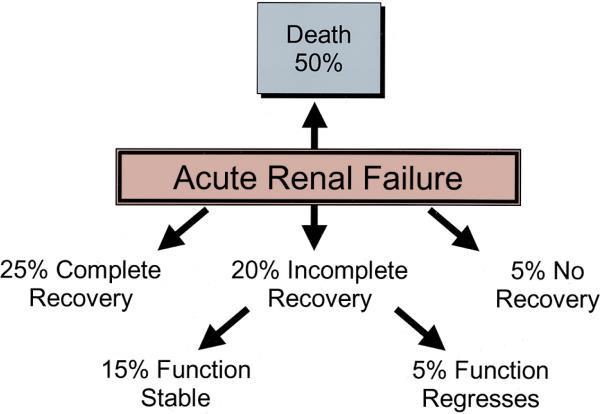
25 Main Categories of Acute Renal Failure Thadhani, R. et al. N Engl J Med 1996;334:
26
27

28
29
30
31
32
33 Furosemide Stress Test Furosemide 1 mg/kg for naïve patients or 1.5 mg/kg in furosemide is given IV + test - UO is < 200 ml over subsequent 2 hours + test predicts AKI progression, need for RRT and mortality

34
35
36 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI 6. Cases
37 Primary prevention of AKI Baseline risks Acute clinical conditions Nephrotoxic agents Advanced age Sepsis Contrast media Diabetes mellitus Hypotension/shock Antimicrobial agents CKD Volume depletion Chemotherapeutic agents Heart failure Rhabdomyolysis NSAIDs Liver failure Male gender Race & genetic variation Hypoalbuminemia Cardiac/vascular surgery Non-renal solid organ transplantation Abdominal compartment syndrome Mechanical ventilation Arterial vascular disease
38 Forest plot for risk of peripheral edema and AKI per subgroup. Kenneth P. Chen et al. CJASN 2016;11:
39
40 Contrast Induced Nephropathy Traditionally IV contrast has been thought to cause AKI Incidence unclear but seemed to be based on pre contrast risks (GFR etc), dose and route of administration(iv VS IA) Recent observational data suggests much less common than thought Prophylaxis and discretion still recommended for now
41 The variable relationship between contrast administration and AKI across the examined disease states. Emilee Wilhelm-Leen et al. JASN 2017;28:
42 Remote Ischemic Preconditioning Transient ischemia protects cells from later ischemic events locally (heart, brain, kidney) Transient local ischemia also has remote protective effects Inducing brachial (local) ischemia has been shown to prevent CIN. Data for CV surgery is mixed
43
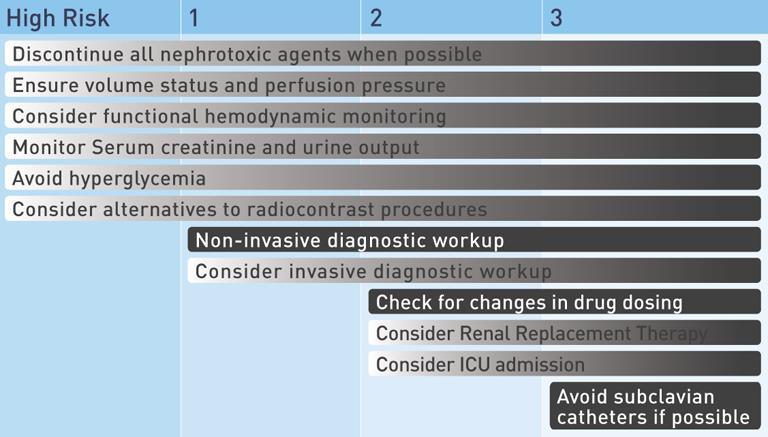
44 AKI Prevention Identification of patients at risk Protocolized comprehensive management plans for sepsis, CV and vascular surgery etc (ASA postop CPB) Avoidance of nephrotoxins or potentially nephrotoxic events
45
46 From: Association Between a Chloride-Liberal vs Chloride-Restrictive Intravenous Fluid Administration Strategy and Kidney Injury in Critically Ill Adults JAMA. 2012;308(15): doi: /jama Figure Legend: Stage 2 or 3 defined according to the Kidney Disease: Improving Global Outcomes clinical practice guideline. Date of download: 10/6/2014 Copyright 2014 American Medical Association. All rights reserved.
47 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI 6. Cases
48
49 Management of AKI 1. Remove or treat offending agent 2. Dx US, UA, Urinary indices 3. Improve hemodynamics if wet dry, if not wet wet 4. Make non-oliguric. Fix electrolytes 5. Avoid nephrotoxins 6. Adjust meds for egfr 7. RRT
50
51 Fig 2. Odd ratios and 95% confidence interval of death for AKI episodes which had AKI Care Bundle completed within 24 hours. Kolhe NV, Staples D, Reilly T, Merrison D, Mcintyre CW, et al. (2015) Impact of Compliance with a Care Bundle on Acute Kidney Injury Outcomes: A Prospective Observational Study. PLOS ONE 10(7): e
52 Fig 3. Adjusted survival curve stratified by timing of completion of AKI Care Bundle. Kolhe NV, Staples D, Reilly T, Merrison D, Mcintyre CW, et al. (2015) Impact of Compliance with a Care Bundle on Acute Kidney Injury Outcomes: A Prospective Observational Study. PLOS ONE 10(7): e
53 Assessment of Volume Bedside 50% of ICU patients are volume responsive. Dynamic vs. Static Static CVP and PAOP Dynamic IVC collapse Pulse pressure and SBP variation Passive straight leg raise Lactate clearance
54 Assessment of Volume Responsiveness Our clinical exam predicts volume responsiveness 50% of the time Adding CVP measurements -50% Adding IVC assessment 60% Dynamic measurements PPV, PSLR or stroke volume variation predictive value > 80% To avoid volume overload use dynamic measurements
55
56
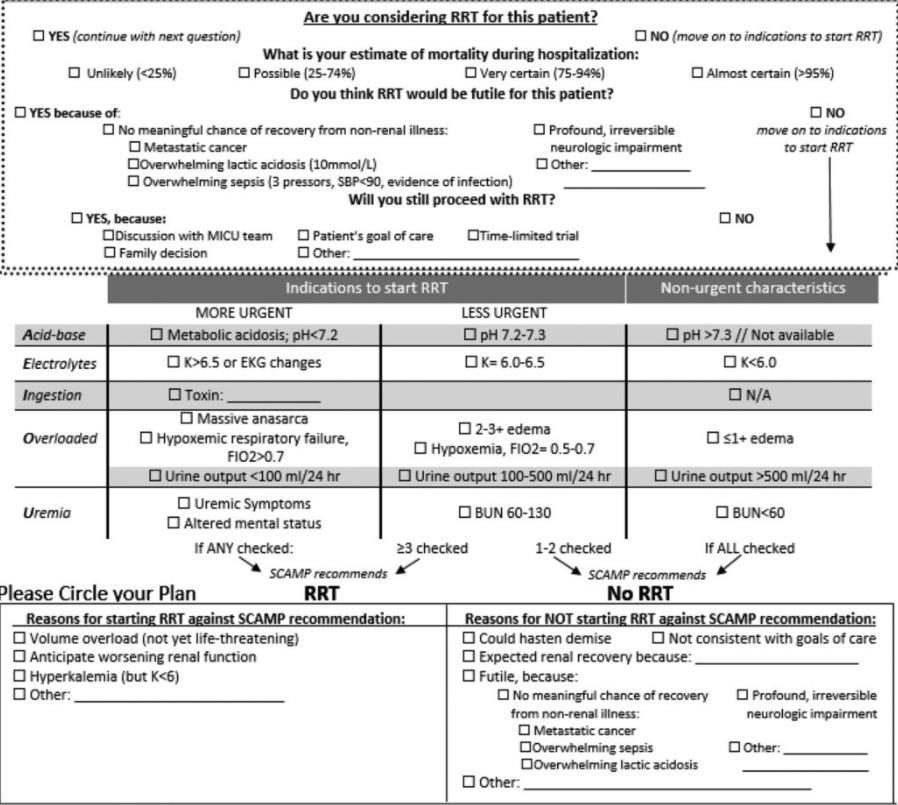
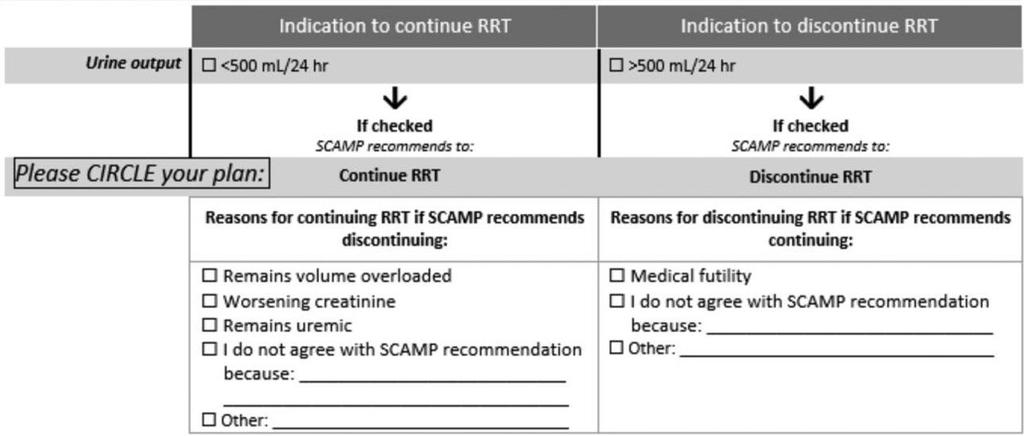
57 Indications for RRT in AKI Volume overload unresponsive to diuretics Metabolic acidosis refractory to medical management Intoxication with dialyzable drug or toxin Uremic symptoms Encephalopathy Pericarditis Uremic bleeding Progressive azotemia in the absence of specific symptoms
58 Indications are open to interpretations How volume overloaded? What should potassium level be? How severe for metabolic acidosis? What is the definition of diuretic resistance?

59 Types of Renal Replacement Therapy
60
61
62
63 AKI Treatment Summary Perfusion IVF, diuretics, inotropes Underlying cause remove, reverse, treat Monitor volume status, electrolytes, urine Prevent complications volume overload, electrolytes, medication adjustment
64 Objectives 1. Define AKI KDIGO Classification 2. Incidence and consequences of AKI 3. Causes of AKI and workup 4. Prevention of AKI 5. Treatment of AKI 6. Cases
65 Case Cardio-Renal Syndrome 65 yo gentleman with long standing HTN admitted for ADHFpEF and 10 kg weight gain. Creatinine 1.8 and egfr 49. He is treated with high dose loop diuretics with a loss of 5 kg and stable egfr. On day 4 his creatinine was noted to be 2.5 and diuretics were discontinued. The next day his creatinine was 3.0
66 Cardiorenal Syndromes Definition Negative effects of heart or kidney dysfunction on the other organ CRS 1 - rapid worsening of cardiac function leading to AKI CRS 2 chronic cardiac dysfunction leads to CKD CRS 3 AKI leads to cardiac dysfunction CRS 4 CKD and cardiovascular disease CRS 5 Systemic illness affecting heart and kidney

67 House A A CJASN 2013;8: Dual hemodynamic pathways for acute cardiorenal syndrome.
68 Case CRS High percentage of CKD with ADHF (30-40%) AKI is called worsening renal function (WRF) in CHF literature and uses same KDIGO criteria and associated with increased mortality Most patients with ADHF are under diuresed

69 Change in body weight at discharge based on Acute Decompensated Heart Failure National Registry database. Kazory A CJASN 2013;8:
70 CRS Patterns of AKI 1. AKI on admission improving with treatment 2. AKI which worsens daily from admission Flash pulmonary edema 3. Stable GFR which worsens as diuresis progresses
71 CRS Case Our patient has pattern 3. 75% of these patient have high RAP and may also have low MAP The venous congestion leads to AKI and treatment is decongestion (diuresis) Typically egfr improves as patient is diuresed
72 Case HRS 31 yo man with a hx of psychiatric disease is admitted for recent onset of jaundice, weakness and swelling Hx of heavy ETOH use over the past several years. + peripheral edema. Liver large and tender. No abdominal tenderness Last drink 1 week ago
73 Case HRS Labs: ALT and AST 5X nl ALT/AST ratio 2, bilirubin 49, albumin 2.5, and INR 1.4. WBC 20K Creatinine 1.4 on admission rising to 3 over several days. UA negative except bilirubin He makes < 0.3 ml/kg/hr urine US ABD minimal ascites, no hydronephrosis
74 Journal of Hepatology , DOI: ( /j.jhep ) Copyright 2015 BMJ Publishing Group Ltd, British Society of Gastroenterology and European Association for the Study of the Liver
75
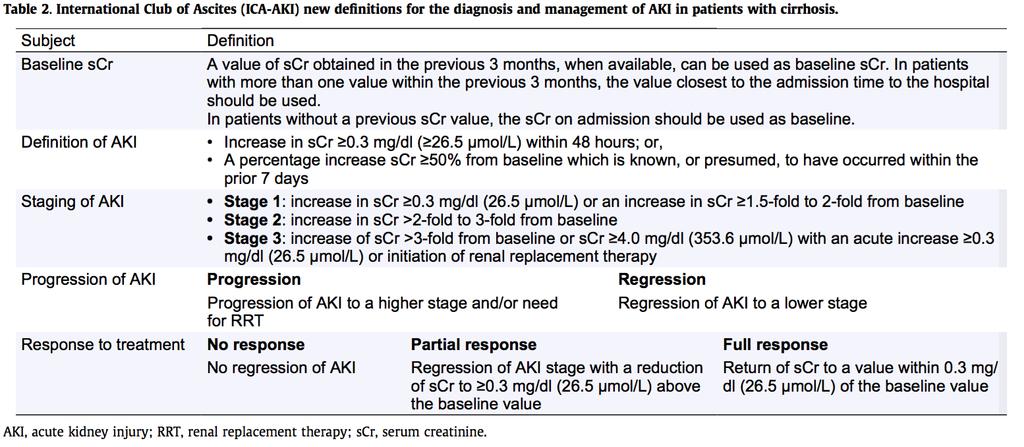
76 Assessing kidney function in pts with cirrhosis Serum creatinine levels should be used to estimate GFR in cirrhosis with the following conditions: There is decreased muscle and hepatic production of creatinine. Malnutrition The edematous state that complicates endstage liver disease leads to large distribution of Cr in the body and lower serum Cr concentration Formula that use creatinine to estimate GFR will overestimate Cystatin C has same problems Proulx et al. Nephrology Dialysis Transplantation 2005
77
78 Munoz S. Medical Clinics of North America July 2008
79 Causes & Outcomes of Renal Failure Martin-Llahi et al, Gastroenterology 2011
80 Causes & Outcomes of Renal Failure Martin-Llahi et al, Gastroenterology 2011

81 Fig. 1 Journal of Hepatology , DOI: ( /j.jhep )
82 Acute Kidney Injury in Cirrhosis Nearly 50% of patients with cirrhosis develop AKI Causes Pre-renal Renal Post-renal
83 Causes & Outcomes of Renal Failure Martin-Llahi et al, Gastroenterology 2011

84 Wong F. Nat Rev. Gastoenterol 2012
85 Cirrhosis Intrahepatic resistance Portal (sinusoidal) hypertension Splanchnic/systemic vasodilatation Arterial BP Activation of neurohumoral systems Renal vasoconstriction HEPATORENAL SYNDROME
86 Cirrhosis Intrahepatic resistance Portal (sinusoidal) hypertension Splanchnic/systemic vasodilatation Arterial BP Albumin Activation of neurohumoral systems Renal vasoconstriction HEPATORENAL SYNDROME
87 Cirrhosis Intrahepatic resistance Portal (sinusoidal) hypertension Splanchnic/systemic vasodilatation Threat to arterial BP Vasoconstricto rs Albumin Activation of neurohumoral systems Renal vasoconstriction HEPATORENAL SYNDROME
88 ICU Management of HRS 1. Norepinephrine titrated to raise MAP >15 2. Octreotide and albumin used as adjuncts 3. Vasopressin has been used but in doses 10X septic shock doses. (Associated with complications)
89 Floor Management of HRS 1. Midodrine 7.5 mg PO TID, up to 15 mg PO TID 2. Octreotide 100 μg SC TID, up to 200 μg SC TID 3. Rapidly titrate to obtain increase in MAP 15 mmhg 4. Albumin (maintenance) 1 gm/kg/d X 48 hrs then g/day Discontinue if serum albumin >4.0 g/dl
90 Management of HRS 1. Stop treatment if no reduction in scre after 3 days or not <50% by day 7 of highest dose?norepinephrine infusion if floor protocol fails 2. If response, continue until Cr <1.5 mg/dl or 14 days
91 HRS Prevention Avoidance of nephrotoxins IV diuretics only with peripheral edema + ascites High volume paracentesis with SPA (8gm/liter removed) Prophylactic antibiotics (quinolone) in high risk (low Na, increased creatinine, increased bilirubin with ascites albumin of < 1.5 gm/dl Treatment of SBP
92 Summary HRS1 is a disease that has a high mortality If a liver transplant candidate, treatment is warranted (does not worsen outcomes) If not a transplant candidate, evaluate for reversible liver disease If no reversible liver disease, shared decision making regarding level of care Therapy is directed toward the pathophysiology of the syndrome
93 Case Our patient developed progressive AKI He was not a liver transplant candidate due to lack of abstinence no RRT He did not have acute hepatitis B no RRT He did have acute alcoholic hepatitis with a chance of reversibility trial of RRT
94 Summary HRS1 is a disease that has a high mortality If a liver transplant candidate, treatment is warranted (does not worsen outcomes) If not a transplant candidate, evaluate for reversible liver disease If no reversible liver disease, shared decision making regarding level of care Therapy is directed toward the pathophysiology of the syndrome
95 AKI Summary Using a standard definition improves recognition AKI leads to worse short term and long term outcomes AKI is a predictor of severity of illness
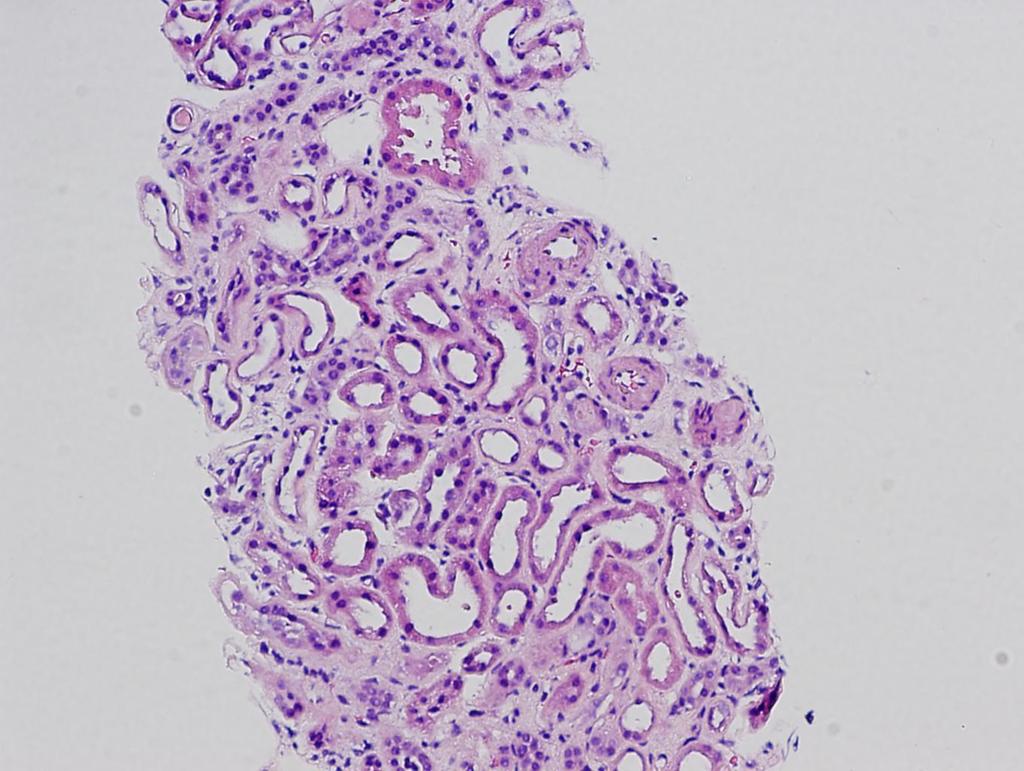
96 ATN, H&E.
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Recognizing and Treating Patients with the Cardio-Renal Syndrome
 Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Recognizing and Treating Patients with the Cardio-Renal Syndrome Joachim H. Ix, MD, MAS, FASN Professor of Medicine Chief; Division of Nephrology-Hypertension University of California San Diego 1 Conflicts
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Kidney Injury Care in the Chronic Unit
 Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Heart Failure and Renal Disease Cardiorenal Syndrome
 Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Advanced Heart Failure: Clinical Challenges Heart Failure and Renal Disease Cardiorenal Syndrome 17 th Apr 2015 Ju-Hee Lee, M.D Cardiovascular Center, Chungbuk National University Hospital Chungbuk National
Acute Kidney Injury. Amandeep Khurana, MD Southwest Kidney Institute
 Acute Kidney Injury Amandeep Khurana, MD Southwest Kidney Institute 66 yr white male w/ DM, HTN, CAD admitted to an OSH w/ E Coli UTI on 7/24/16, developed E Coli bacteremia and Shock (on vaso + levo)
Acute Kidney Injury Amandeep Khurana, MD Southwest Kidney Institute 66 yr white male w/ DM, HTN, CAD admitted to an OSH w/ E Coli UTI on 7/24/16, developed E Coli bacteremia and Shock (on vaso + levo)
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
The Triple Threat. Cardiac Care in the NT Annual Workshop 2017 is proudly supported by:
 The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
The Triple Threat DR KELUM PRIYADARSHANA FRACP CONSULTANT NEPHROLOGIST ROYAL DARWIN HOSPITAL Cardiac Care in the NT Annual Workshop 2017 is proudly supported by: Pathogenesis Diabetes CKD CVD Diabetic
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
ACUTE KIDNEY INJURY. Stuart Linas U. Colorado SOM
 ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
ACUTE KIDNEY INJURY Stuart Linas U. Colorado SOM Marked increases in incidence of dialysis-requiring AKI in last decade JASN 24 37 2013 Question 1 Of patients who recover from an episode of AKI, what percentage
Acute Kidney Injury IM Resident Lecture. Yongen Chang, MD, PhD Nephrology July 2018
 Acute Kidney Injury IM Resident Lecture Yongen Chang, MD, PhD Nephrology July 2018 Objectives Epidemiology Definition and Staging Etiology and Diagnostic Approach Specific syndromes of AKI Treatment Biomarkers
Acute Kidney Injury IM Resident Lecture Yongen Chang, MD, PhD Nephrology July 2018 Objectives Epidemiology Definition and Staging Etiology and Diagnostic Approach Specific syndromes of AKI Treatment Biomarkers
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Contrast Induced Nephropathy
 Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Contrast Induced Nephropathy O CIAKI refers to an abrupt deterioration in renal function associated with the administration of iodinated contrast media O CIAKI is characterized by an acute (within 48 hours)
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen
 When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
Acute Kidney Injury for the General Surgeon
 Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Acute Kidney Injury for the General Surgeon UCSF Postgraduate Course in General Surgery Maui, HI March 20, 2011 Epidemiology & Definition Pathophysiology Clinical Studies Management Summary Hobart W. Harris,
Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology. Biomarkers of Renal Injury and Dysfunction
 CRRT 2011 San Diego, CA 22-25 February 2011 Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology Biomarkers of Renal Injury and Dysfunction Dinna Cruz, M.D., M.P.H. Department of Nephrology San Bortolo
CRRT 2011 San Diego, CA 22-25 February 2011 Heart Failure and Cardio-Renal Syndrome 1: Pathophysiology Biomarkers of Renal Injury and Dysfunction Dinna Cruz, M.D., M.P.H. Department of Nephrology San Bortolo
Overcoming the Cardiorenal Syndrome
 Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Overcoming the Cardiorenal Syndrome October 29, 2016 Randall C Starling MD MPH FACC FESC FHFSA FHFA Professor of Medicine Heart & Vascular Institute Cleveland Clinic Lerner College of Medicine Cleveland
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
How and why to measure renal function in patients with liver disease?
 ow and why to measure renal function in patients with liver disease? P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology
ow and why to measure renal function in patients with liver disease? P. Angeli, Dept. of Medicine, Unit of Internal Medicine and epatology (), University of Padova (Italy) pangeli@unipd.it 10th Paris epatology
Pivotal Role of Renal Function in Acute Heart failure
 Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Pivotal Role of Renal Function in Acute Heart failure Doron Aronson MD, FESC Department of Cardiology RAMBAM Health Care Campus Haifa, Israel Classification and definitions of cardiorenal syndromes CRS
Elevated Creatinine in a Patient With Cirrhosis
 REVIEW Elevated Creatinine in a Patient With Cirrhosis Heather L. Klavan, M.D., and Brett E. Fortune, M.D., M.S. Elevation in serum creatinine is a common laboratory finding for patients with cirrhosis
REVIEW Elevated Creatinine in a Patient With Cirrhosis Heather L. Klavan, M.D., and Brett E. Fortune, M.D., M.S. Elevation in serum creatinine is a common laboratory finding for patients with cirrhosis
Cardiorenal syndrome. Sofie Gevaert. Ghent University Hospital, Belgium
 Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Cardiorenal syndrome Sofie Gevaert Ghent University Hospital, Belgium Disclosures Consultancy Astra Zeneca Boegringer MSD Novartis 68 y old man, ADHF ICMP, ejection fraction 35 %: progressive dyspnea,
Management of Advanced Systolic Heart Failure. Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University
 Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
Management of Advanced Systolic Heart Failure Robert W. Hull MD FACC Associate Professor of Medicine West Virginia University American College of Cardiology Foundation (ACCF) American Heart Association
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Las dos caras de la cretinina sérica The two sides of serum creatinine
 Las dos caras de la cretinina sérica The two sides of serum creatinine ASOCIACION COSTARRICENSE DE MEDICINA INTERNA San José, Costa Rica June 2017 Kianoush B. Kashani, MD, MSc, FASN, FCCP 2013 MFMER 3322132-1
Las dos caras de la cretinina sérica The two sides of serum creatinine ASOCIACION COSTARRICENSE DE MEDICINA INTERNA San José, Costa Rica June 2017 Kianoush B. Kashani, MD, MSc, FASN, FCCP 2013 MFMER 3322132-1
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
The Cardiorenal Syndrome in Heart Failure
 The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
The Cardiorenal Syndrome in Heart Failure Van N Selby, MD Assistant Professor of Medicine Advanced Heart Failure Program, UCSF October 9, 2015 Disclosures None 1 Cardiorenal Syndrome (CRS) A pathophysiologic
Ricky Bell Renal/ICM Registrar
 Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
Practical Points in Cardiorenal Syndrome
 Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Practical Points in Cardiorenal Syndrome Vichai Senthong, MD. Cardiovascular Unit, Faculty of Medicine Khon Kaen university HFCT Annual Scientific Meeting June 16, 2017, Eastin Grand Sathorn Hotel, Bangkok
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Acute Kidney Injury in the Hospitalized Patient
 Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Acute Kidney Injury in the Hospitalized Patient Biff F. Palmer, M.D. Professor of Internal Medicine University of Texas Southwestern Medical Center, Dallas Texas Classification of Acute Kidney Injury 1
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Vasoconstrictor Therapy in Hepatorenal Syndrome: When to Use it and How
 KidneyCon Little Rock, AR, April 7 th, 2018 Vasoconstrictor Therapy in Hepatorenal Syndrome: When to Use it and How Juan Carlos Q. Velez, MD Associate Professor of Medicine, Ochsner Clinical School / The
KidneyCon Little Rock, AR, April 7 th, 2018 Vasoconstrictor Therapy in Hepatorenal Syndrome: When to Use it and How Juan Carlos Q. Velez, MD Associate Professor of Medicine, Ochsner Clinical School / The
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Update in. Acute Kidney Injury. Mark Devonald Consultant Nephrologist. Nottingham AKI Research Group
 Update in Acute Kidney Injury Mark Devonald Consultant Nephrologist If you stay awake you might hear about Why AKI is important Some cases to illustrate some specific points A couple of updates on AKI
Update in Acute Kidney Injury Mark Devonald Consultant Nephrologist If you stay awake you might hear about Why AKI is important Some cases to illustrate some specific points A couple of updates on AKI
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
Prevention of Acute Renal Failure Role of vasoactive drugs and diuretic agents
 of Acute Renal Failure Role of vasoactive drugs and diuretic agents Armand R.J. Girbes Prof.dr. A.R.J. Girbes Chairman department of Intensive Care VU University Medical Center Netherlands (Failure of)
of Acute Renal Failure Role of vasoactive drugs and diuretic agents Armand R.J. Girbes Prof.dr. A.R.J. Girbes Chairman department of Intensive Care VU University Medical Center Netherlands (Failure of)
Minimizing the Renal Toxicity of Iodinated Contrast
 Minimizing the Renal Toxicity of Iodinated Contrast Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Chief Academic and Scientific Officer St. John Providence Health System Detroit, MI USA Outline
Minimizing the Renal Toxicity of Iodinated Contrast Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Chief Academic and Scientific Officer St. John Providence Health System Detroit, MI USA Outline
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
RRT in Advanced Heart Failure and Liver Failure When to start and when to stop?
 Critical Care Medicine Apollo Hospitals RRT in Advanced Heart Failure and Liver Failure When to start and when to stop? Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine
Critical Care Medicine Apollo Hospitals RRT in Advanced Heart Failure and Liver Failure When to start and when to stop? Ramesh Venkataraman, AB (Int. Med), AB (CCM) Senior Consultant, Critical Care Medicine
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Adding Insult to Injury. Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London
 Acute Kidney Injury Adding Insult to Injury Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London Content 1. Brief review of AKI and its impact 2. Comments on the
Acute Kidney Injury Adding Insult to Injury Marlies Ostermann Consultant in Nephrology & Critical Care Guy s & St Thomas Hospital, London Content 1. Brief review of AKI and its impact 2. Comments on the
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
THE KIDNEY IN HYPOTENSIVE STATES. Benita S. Padilla, M.D.
 THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
THE KIDNEY IN HYPOTENSIVE STATES Benita S. Padilla, M.D. Objectives To discuss what happens when the kidney encounters low perfusion To discuss new developments and clinical application points in two scenarios
Hand-Carried Ultrasound Performed by a Hospitalist to Assist with Clinical Decisions in Medicine Inpatients: a Case Series
 Hand-Carried Ultrasound Performed by a Hospitalist to Assist with Clinical Decisions in Medicine Inpatients: a Case Series Stefan Tchernodrinski, MD Cook County Hospital Chicago, Illinois Introduction
Hand-Carried Ultrasound Performed by a Hospitalist to Assist with Clinical Decisions in Medicine Inpatients: a Case Series Stefan Tchernodrinski, MD Cook County Hospital Chicago, Illinois Introduction
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Failure of the circulation to maintain Tissue cellular. Tissue hypoperfusion Cellular hypoxia SHOCK. Perfusion
 Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Shock SHOCK Failure of the circulation to maintain Tissue cellular Perfusion Organs Syndrome RR
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
OBJECTVES OF LEARNING
 OBJECTVES OF LEARNING ACUTE RENAL FAILURE AND RENAL REPLACEMENT THERAPY DR.TAI CHENG SHENG RECOGNITION OF DEFINITION OF ARF RECOGNITION OF CAUSE OF ARF RECOGNITION OF PATHOGENESIS OF ARF RECOGNITION OF
OBJECTVES OF LEARNING ACUTE RENAL FAILURE AND RENAL REPLACEMENT THERAPY DR.TAI CHENG SHENG RECOGNITION OF DEFINITION OF ARF RECOGNITION OF CAUSE OF ARF RECOGNITION OF PATHOGENESIS OF ARF RECOGNITION OF
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Cardiorenal Syndrome
 SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
SOCIEDAD ARGENTINA DE CARDIOLOGIA Cardiorenal Syndrome Joint session ESC-SAC ESC Congress 2012, Munich César A. Belziti Hospital Italiano de Buenos Aires I have no conflicts of interest to declare Cardiorenal
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
Case Presentation. This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Worsening Renal Function in Heart Failure Patients Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs. Florence Wong University of Toronto. Falk Symposium October 14, 2007
 From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
AKI: definitions, detection & pitfalls. Jon Murray
 AKI: definitions, detection & pitfalls Jon Murray Previous conventional definition Acute renal failure (ARF) An abrupt and sustained decline in renal excretory function due to a reduction in glomerular
AKI: definitions, detection & pitfalls Jon Murray Previous conventional definition Acute renal failure (ARF) An abrupt and sustained decline in renal excretory function due to a reduction in glomerular
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
A patient with acute heart failure and renal impairment ACCA Masterclass 2017
 A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
A patient with acute heart failure and renal impairment Dr Sofie Gevaert Mister P. J.M., 67-years-old Cardiac risk factors: Ex-smoker, AHT, Type 2 diabetes, BMI 43, Hyperlipidaemia Medical history: 2009:
SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity
 SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity Dr. Vijay Kunadian MBBS, MD, MRCP Senior Lecturer and Consultant Interventional Cardiologist Institute of Cellular Medicine, Faculty of Medical
SAFETY IN THE CATH LAB How to Minimise Contrast Toxicity Dr. Vijay Kunadian MBBS, MD, MRCP Senior Lecturer and Consultant Interventional Cardiologist Institute of Cellular Medicine, Faculty of Medical
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome. Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium
 Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic