Talking about blood pressure
|
|
|
- Kory Stewart
- 6 years ago
- Views:
Transcription
1 Talking about blood pressure
 HbA1c 43 She has been promising to do more exercise and eat more")

2 Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight has gone up. She gets side effects with most meds and isn t keen to take any tablets. She feels fine thank you
3
4
5
6
 Ambulatory (24hrs) Lying/sitting/standing Size of cuff Position of arm")
7 Measuring Blood Pressure Clinic (Doctor) manual vs automated Clinic (non-doctor) Home readings (1week) Ambulatory (24hrs) Lying/sitting/standing Size of cuff Position of arm Which arm?
8 Causes of Hypertension Unknown or essential Hyperaldosteronism 5-10% Renal disease Cushings syndrome Thyroid disease Phaechromocytoma %
9 The Lancet , DOI: ( /S (14) ) Copyright 2014 Rapsomaniki et al. Open Access article distributed under the terms of CC BY Terms and Conditions Figure 1 Is high blood pressure bad for you? HR per 20/10mm Hg
10 Figure 5 The Lancet , DOI: ( /S (14) ) Copyright 2014 Rapsomaniki et al. Open Access article distributed under the terms of CC BY Terms and Conditions
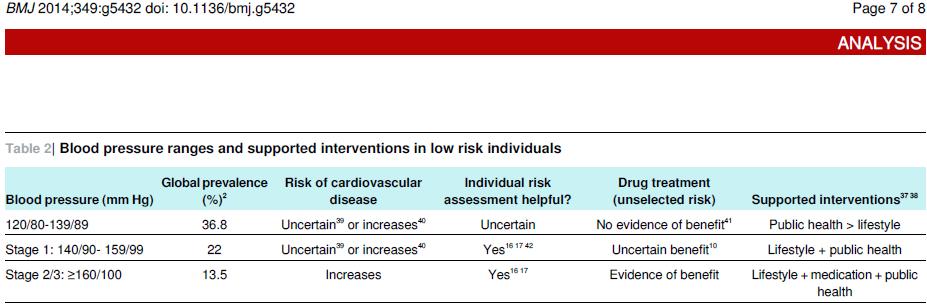
11 What systolic blood pressure is bad for you? It depends on how you look at it
12

13 What does weight loss achieve? Evidence is of poor quality 4kg weight loss overall produced 4.5/3.2 mm Hg reduction No data on mortality or morbidity


14 moderate reduction (3gram/day) may achieve up to 3-5/ mmhg reduction No data on morbidity/mortality Switch to low alcohol beer resulted in a 3/1.5 mm Hg reduction No data on morbidity/mortality
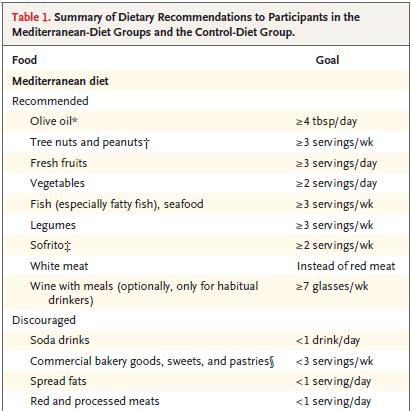
15 Dietary Approaches to Stop Hypertension 1997 NEJM 459 adults av. Age 44 BP 132/85 Food prepared in lab kitchen Control Fruit and Vegetables Diet Combination Diet
16
17


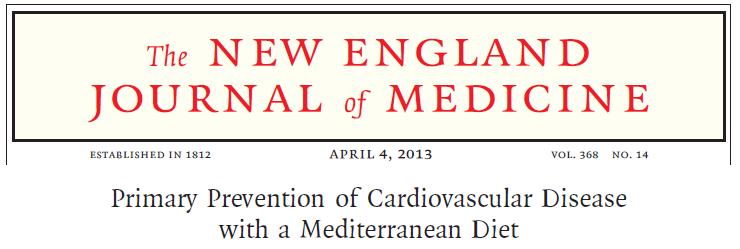
18
19 4.5yrs
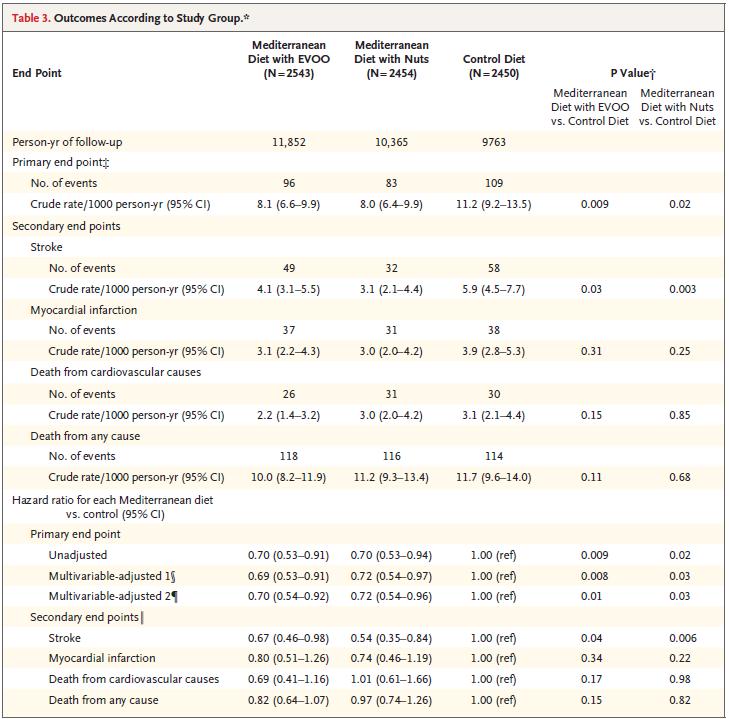
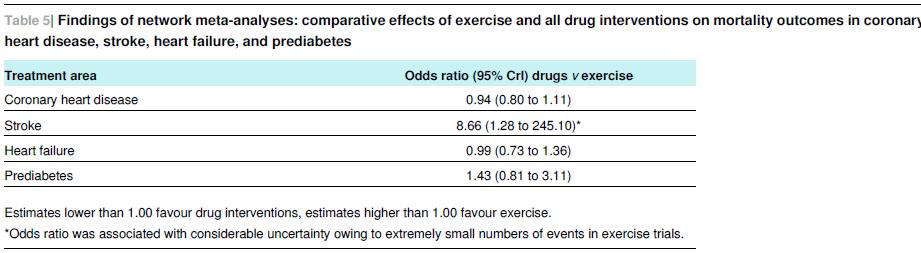
20 What about exercise?
21
22 16 MAs, 305 RCTs with participants
23
24
25

26 Perspectives on Drugs to lower mild BP

27 Use of blood pressure lowering drugs in the prevention of cardiovascular disease: metaanalysis of 147 randomised trials in the context of expectations from prospective epidemiological studies M R Law, professor of epidemiology J K Morris, professor of medical statistics N J Wald, professor of environmental and preventive medicine BMJ 2009;338:b1665


28 Cochrane 2012

29
30

31 What about different medications?
32 The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial ALLHAT study overview Double-blind, randomized trial to determine whether the occurrence of fatal CHD or nonfatal MI is lower for high-risk hypertensive patients treated with newer agents (amlodipine, lisinopril, or doxazosin) compared with a diuretic (chlorthalidone) Cohort 42,418 patients ( 55 years old) from 623 sites in North America Stage 1 or 2 hypertension 1 additional risk factor for CHD Comparisons between chlorthalidone and amlodipine and chlorthalidone and lisinopril have been reported together, excluding the doxazosin arm (n=9,062), which was terminated early CHD=coronary heart disease; MI=myocardial infarction ALLHAT Research Group. JAMA. 2002;288: org
 stopped drug Lisinopril n=9,054 n=8,158 1,842 (22.6%) stopped drug YEAR 5 n=6,210 1,873 (30.2%) stopped drug n=3,769 1,052 (27.9%) stopped drug n=3,605 1,399 (38.8%) stopped drug n=9,054 218 (2.")
33 Doxazosin n=9,062 ALLHAT Study Design Discontinued early at 3.3 yrs Randomized n=42,418 YEAR 1 Chlorthalidone n=15,255 n=13,854 2,235 (16.1%) stopped drug Amlodipin e n=9,048 n=8,215 1,357 (16.5%) stopped drug Lisinopril n=9,054 n=8,158 1,842 (22.6%) stopped drug YEAR 5 n=6,210 1,873 (30.2%) stopped drug n=3,769 1,052 (27.9%) stopped drug n=3,605 1,399 (38.8%) stopped drug n=9, (2.4%) lost to followup 58 (0.6%) refused follow-up ntent-to- Treat Analysis n=15, (2.2%) lost to followup 80 (0.5%) refused follow-up n=9, (2.2%) lost to follow-up 58 (0.6%) refused follow-up ALLHAT Research Group. JAMA. 2002;288: org
34 ALLHAT Endpoints Primary endpoint Composite of fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI) Other predefined endpoints all-cause mortality stroke combined CHD nonfatal MI, CHD death, coronary revascularization, hospitalized angina combined cardiovascular disease combined CHD, stroke, lower extremity revascularization, treated angina, fatal/ hospitalized/treated congestive heart failure, hospitalized or outpatient peripheral arterial disease other renal ALLHAT Research Group. JAMA. 2002;288: org
35 ALLHAT Baseline Characteristics Chlorthalidon e n=15,255 systoli c diastoli c Amlodipine n=9,048 systolic diastoli c Lisinopril n=9,054 systoli c diastoli c Mean BP (mmhg) Treated (90%) Untreated (10%) Mean age (yrs) Black (%) Women (%) Current smoking (%) History of CHD (%) BP=blood pressure CHD=coronary heart disease Type 2 diabetes (%) ALLHAT Research Group. JAMA. 2002;288: org
36 Systolic BP (mmhg) Diastolic BP (mmhg) ALLHAT Mean Systolic and Diastolic Blood Pressure During Follow-up Chlorthalidone Chlorthalidone 150 Amlodipine Lisinopril 90 Amlodipine Lisinopril Compared to chlorthalidone: SBP significantly higher in amlodipine (~1 mmhg) and lisinopril (~2 mmhg) groups Compared to chlorthalidone: DBP significantly lower in amlodipine group (~1 mmhg) Follow-up, yrs SBP=systolic blood pressure ALLHAT Research Group. JAMA. 2002;288: pressure Copyright 2002, American Medical Association. DBP=diastolic blood org
37 % Patients with BP <140/90 mmhg ALLHAT BP Controlled to <140/90 mmhg Chlorthalidone * * Amlodipine Lisinopril Baseline Year 1 Year 2 Year 3 Year 4 Year 5 *P<0.001 for amlodipine vs chlorthalidone P<0.001 for lisinopril vs chlorthalidone ALLHAT Research Group. JAMA. 2002;288: org
38 Patients (%) ALLHAT Treatment and Blood Pressure Control Drug 2 Drugs 3 Drugs Average # of drugs 0 6 mos 1 yr 3 yr 5 yr Blood pressure controlled <140/90 mmhg 49.8% 55.2% 62.3% 65.6% Cushman WC, et al. J Clin Hypertens. 2002;4: org 0
39 Cumulative Fatal CHD and Nonfatal MI event rate (%) ALLHAT Primary Outcome by Treatment Group Chlorthalidone Amlodipine Lisinopril 8 4 No. at Risk Chlorthalidone Amlodipine Lisinopril Time to event, yrs ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association org
 lisinopril chlorthalidone 0.98 (0.90-1.07) 0.99 (0.85-1.16) 0.97 (0.88-1.08) 0.98 (0.87-1.09) 0.99 (0.85-1.15) 1.01 (0.86-1.18) 0.97 (0.87-1.08) 0.99 (0.87-1.13) 0.97 (0.86-1.09) 0.99 (0.91-1.")
40 ALLHAT CHD Death and Nonfatal MI TOTAL Age <65 Age 65 Men Women Black Nonblack Diabetic Nondiabeti c Relative Risk Favors Favors Relative Risk Favors Favors (95% CI) amlodipine chlorthalidone (95% CI) lisinopril chlorthalidone 0.98 ( ) 0.99 ( ) 0.97 ( ) 0.98 ( ) 0.99 ( ) 1.01 ( ) 0.97 ( ) 0.99 ( ) 0.97 ( ) 0.99 ( ) 0.95 ( ) 1.01 ( ) 0.94 ( ) 1.06 ( ) 1.10 ( ) 0.94 ( ) 1.00 ( ) 0.99 ( ) ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association. org
 0.96 (0.83-1.10) 0.96 (0.88-1.03) 0.95 (0.87-1.04) 0.96 (0.86-1.07) 0.97 (0.87-1.09) 0.94 (0.87-1.03) 0.96 (0.87-1.07) 0.95 (0.87-1.04) 1.00 (0.94-1.08) 0.")
41 TOTAL Age <65 Age 65 Men Women Black Nonblack Diabetic Nondiabeti c ALLHAT All-Cause Mortality Relative Risk Favors Favors Relative Risk Favors Favors (95% CI) amlodipine chlorthalidone (95% CI) lisinopril chlorthalidone 0.96 ( ) 0.96 ( ) 0.96 ( ) 0.95 ( ) 0.96 ( ) 0.97 ( ) 0.94 ( ) 0.96 ( ) 0.95 ( ) 1.00 ( ) 0.93 ( ) 1.03 ( ) 0.99 ( ) 1.02 ( ) 1.06 ( ) 0.97 ( ) 1.02 ( ) 1.00 ( ) ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association. org
 1.03 (0.94-1.12) 1.05 (0.99-1.12) 1.04 (0.98-1.11) 1.04 (0.96-1.13) 1.06 (0.96-1.16) 1.04 (0.97-1.10) 1.06 (0.98-1.15) 1.02 (0.96-1.09) 1.10 (1.05-1.16) 1.05 (0.97-1.15) 1.13 (1.")
42 TOTAL Age <65 Age 65 Men Women Black Nonblack Diabetic Nondiabeti c ALLHAT Combined CV Disease Relative Risk Favors Favors Relative Risk Favors Favors (95% CI) amlodipine chlorthalidone (95% CI) lisinopril chlorthalidone 1.04 ( ) 1.03 ( ) 1.05 ( ) 1.04 ( ) 1.04 ( ) 1.06 ( ) 1.04 ( ) 1.06 ( ) 1.02 ( ) 1.10 ( ) 1.05 ( ) 1.13 ( ) 1.08 ( ) 1.12 ( ) 1.19 ( ) 1.06 ( ) 1.08 ( ) 1.12 ( ) ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association. org
43 Cumulative event rate (%) ALLHAT Stroke by Treatment Group Chlorthalidone Amlodipine Lisinopril 4 2 No. at Risk Chlorthalidone Amlodipine Lisinopril Time to event, yrs ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association org
 0.93 (0.73-1.19) 0.93 (0.81-1.08) 1.00 (0.85-1.18) 0.84 (0.69-1.03) 0.93 (0.76-1.14) 0.93 (0.79-1.10) 0.90 (0.75-1.08) 0.96 (0.81-1.14) 1.15 (1.02-1.30) 1.21 (0.97-1.")
44 ALLHAT Stroke Relative Risk Favors Favors Relative Risk (95% CI) amlodipine chlorthalidone (95% CI) Favors Favors lisinopril chlorthalidone TOTAL Age <65 Age 65 Men Women Black Nonblack Diabetic Nondiabeti c 0.93 ( ) 0.93 ( ) 0.93 ( ) 1.00 ( ) 0.84 ( ) 0.93 ( ) 0.93 ( ) 0.90 ( ) 0.96 ( ) 1.15 ( ) 1.21 ( ) 1.13 ( ) 1.10 ( ) 1.22 ( ) 1.40 ( ) 1.00 ( ) 1.07 ( ) 1.23 ( ) ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association. org

45 Cumulative event rate (%) ALLHAT Heart Failure by Treatment Group Chlorthalidone Amlodipine Lisinopril P<0.001 for chlorthalidone vs amlodipine and chlorthalidone vs lisinopril 6 3 No. at Risk Chlorthalidone Amlodipine Lisinopril Time to event, yrs ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association org
46 TOTAL Age <65 Age 65 Men Women Black Nonblack Diabetic Nondiabeti c ALLHAT Heart Failure Relative Risk Favors Favors Relative Risk Favors Favors (95% CI) amlodipine chlorthalidone (95% CI) lisinopril chlorthalidone 1.38 ( ) 1.51 ( ) 1.33 ( ) 1.41 ( ) 1.33 ( ) 1.47 ( ) 1.33 ( ) 1.42 ( ) 1.33 ( ) 1.20 ( ) 1.23 ( ) 1.20 ( ) 1.19 ( ) 1.23 ( ) 1.32 ( ) 1.15 ( ) 1.22 ( ) 1.20 ( ) ALLHAT Research Group. JAMA. 2002;288: Copyright 2002, American Medical Association. org
47 ALLHAT Conclusions Better control of systolic BP was achieved with chlorthalidone than with amlodipine or lisinopril There were no differences in risk for CHD death/nonfatal MI between chlorthalidone and amlodipine or lisinopril In secondary endpoints, chlorthalidone was associated with lower risk for stroke, combined CVD, and HF compared with lisinopril HF compared with amlodipine MI=myocardial infarction CHD=coronary heart disease HF=heart failure ALLHAT Research Group. JAMA. 2002;288: org


, N.")
, G. Beevers, M.")

48 A randomised controlled trial of the prevention of CHD and other vascular events by BP and cholesterol lowering in a factorial study design B.Dahlof (Co-chair), P.Sever (Co-chair), N. Poulter (Secretary) H. Wedel (Statistician), G. Beevers, M. Caulfield, R. Collins S. Kjeldsen, A. Kristinsson, J. Mehlsen, G. McInnes, M. Nieminen E. O Brien, J. Östergren, on behalf of the ASCOT Investigators
49 ASCOT- BPLA Primary Objective To compare the effect on non-fatal myocardial infarction (MI) and fatal CHD of the standard antihypertensive regimen ( -blocker ± diuretic) with a more contemporary regimen (CCB ± ACE inhibitor)
50 Study design 19,257 hypertensive patients ASCOT-BPLA atenolol ± bendroflumethiazide PROBE design amlodipine ± perindopril 10,305 patients TC 6.5 mmol/l (250 mg/dl) ASCOT-LLA atorvastatin 10 mg Double-blind placebo Investigator-led, multinational randomised controlled trial
51 Patient inclusion criteria Screening and baseline BP 160/100 mm Hg untreated 140/90 mm Hg following treatment with 1 or more drugs Age years No previous MI or current clinical CHD 3 or more CV risk factors
52 Treatment algorithm to BP targets < 140/90 mm Hg or < 130/80 mm Hg in patients with diabetes amlodipine 5-10 mg add perindopril 4-8 mg atenolol mg add bendroflumethiazide-k mg add doxazosin GITS 4-8 mg add additional drugs, eg, moxonidine/spironolactone
53 Baseline characteristics amlodipine perindopril atenolol thiazide Demographics and clinical characteristics n = 9639 n = 9618 Woman 2258 (23.4%) 2257 (23.5%) White 9187 (95.3%) 9170 (95.3%) Current smoker 3168 (32.9%) 3110 (32.3%) Age (years) 63.0 (8.5) 63.0 (8.5) SBP (mm Hg) (18.1) (18.0) DBP (mm Hg) 94.8 (10.4) 94.5 (10.4) Heart rate (bpm) 71.9 (12.7) 71.8 (12.6) BMI (kg/m 2 ) 28.7 (4.6) 28.7 (4.5) Drug therapy Previous antihypertensive treatments (19.1%) 1825 (19.0%) (44.4%) 4283 (44.5%) (36.5%) 3510 (36.5%) Lipid-lowering therapy 1046 (10.9%) 1004 (10.4%) Aspirin 1851 (19.2%) 1837 (19.1%) Values are number of patients, (%) or mean (SD)
54 mm Hg Systolic and diastolic blood pressure SBP Mean difference 2.7 atenolol thiazide amlodipine perindopril DBP Mean difference Baseline Time (years) Last visit
55 Summary of all end points Primary Non-fatal MI (incl silent) + fatal CHD Secondary Non-fatal MI (exc. Silent) +fatal CHD Total coronary end point Total CV event and procedures All-cause mortality Cardiovascular mortality Fatal and non-fatal stroke Fatal and non-fatal heart failure Tertiary Silent MI Unstable angina Chronic stable angina Peripheral arterial disease Life-threatening arrhythmias New-onset diabetes mellitus New-onset renal impairment Amlodipine perindopril better Atenolol thiazide better Post hoc Primary end point + coronary revasc procs The area of the blue square is proportional to the amount of statistical information Unadjusted Hazard ratio (95% CI) 0.90 ( ) 0.87 ( ) 0.87 ( ) 0.84 ( ) 0.89 ( ) 0.76 ( ) 0.77 ( ) 0.84 ( ) 1.27 ( ) 0.68 ( ) 0.98 ( ) 0.65 ( ) 1.07 ( ) 0.70 ( ) 0.85 ( ) 0.86 ( )
56 Variables which differed significantly (baseline - final visit) between treatment regimens Mean differences (Amlodipine perindopril - Atenolol thiazide) Changes baseline to final visit p-value Systolic BP (mm Hg) < Diastolic BP (mm Hg) < Heart rate (bpm) < Weight (kg) < HDL-cholesterol (mmol/l) 0.11 < Triglycerides (mmol/l) < Glucose (mmol/l) < Creatinine (µmol/l) < Potassium (mmol/l) 0.05 <0.0001
57 Impact on the treatment effect on coronary events after adjustment for BP and all variables that differed Hazard ratio 95% CI Unadjusted SBP SBP + covariates SBP + DBP + covariates MBP** + covariates PP + covariates Amlodipine perindopril better Atenolol thiazide better p-value Hazard ratio ** MBP = (SBP+DBP)/2
58 Impact on the treatment effect on stroke events after adjustment for BP and all variables that differed Hazard Hazard ratio ratio 95% CI 95% CI Unadjusted Mean BP SBP + covariates SBP + DBP + covariates MBP** + covariates PP + covariates Amlodipine perindopril better Atenolol thiazide better p-value Hazard ratio ** MBP = (SBP+DBP)/2

59 What about B-blockers?
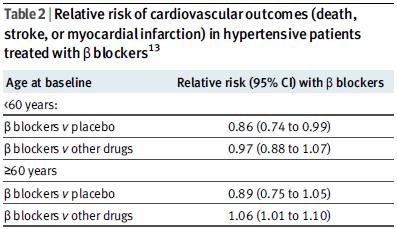
60

61 What about the Elderly?
62 Systolic Hypertension in the Elderly JAMA 1991 Randomized, double-blind, placebo controlled 4736 people aged 60yrs+ BP /<90 Average BP 170/77, average age 72 Step 1 Chlorthalidone 12.5mg or placebo Step 2 Atenolol 25mg/placebo Atenolol 50mg/placebo
63 SHEP 1991 Follow up 4.5yrs Average BP 143/68 treatment group, 155/72 placebo 5.2% total stroke (treatment) vs 8.2% (placebo) 3% absolute risk reduction Coronary death and non fatal MI RR 0.73 All cause mortality RR 0.87
64 Indapamide 1.5mg MR then Perindopril 2mg/4mg

65 HYVET 2008
66 HYVET 2008

67 HYVET 2008

68 What about Diabetics?
69
70

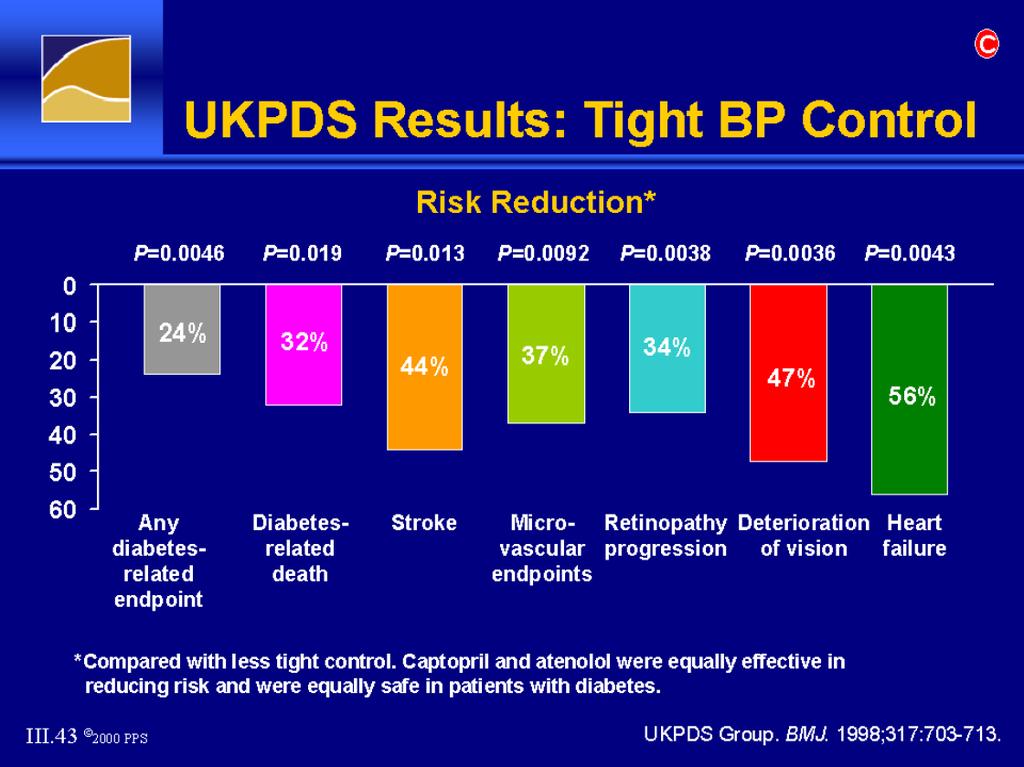
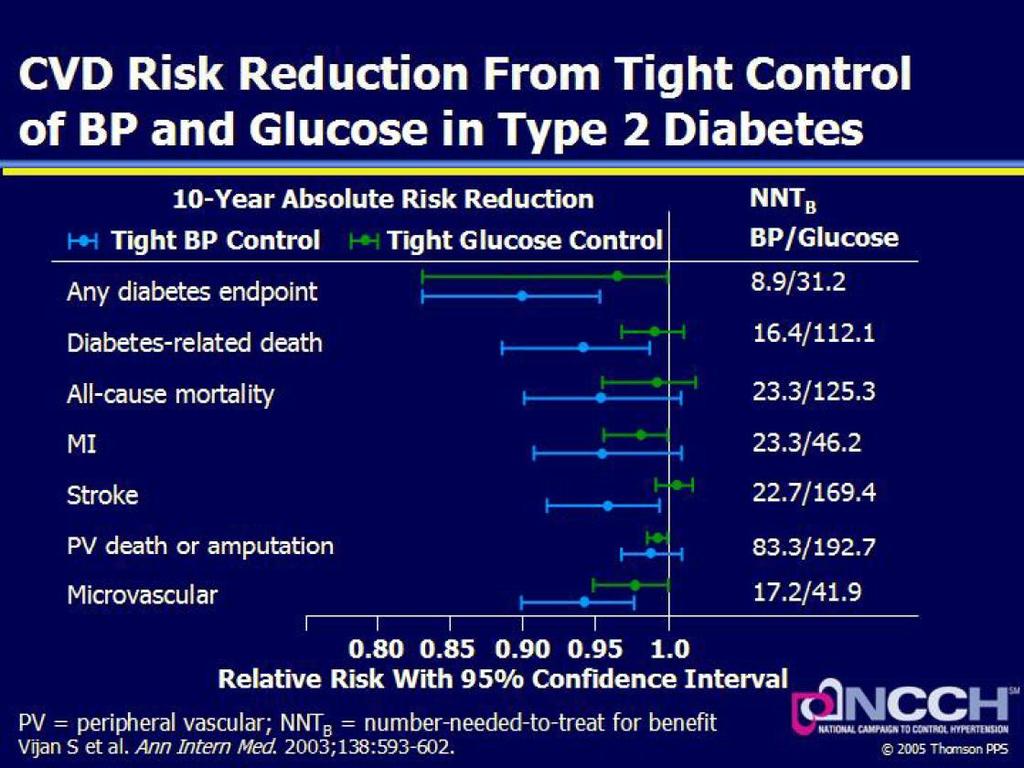
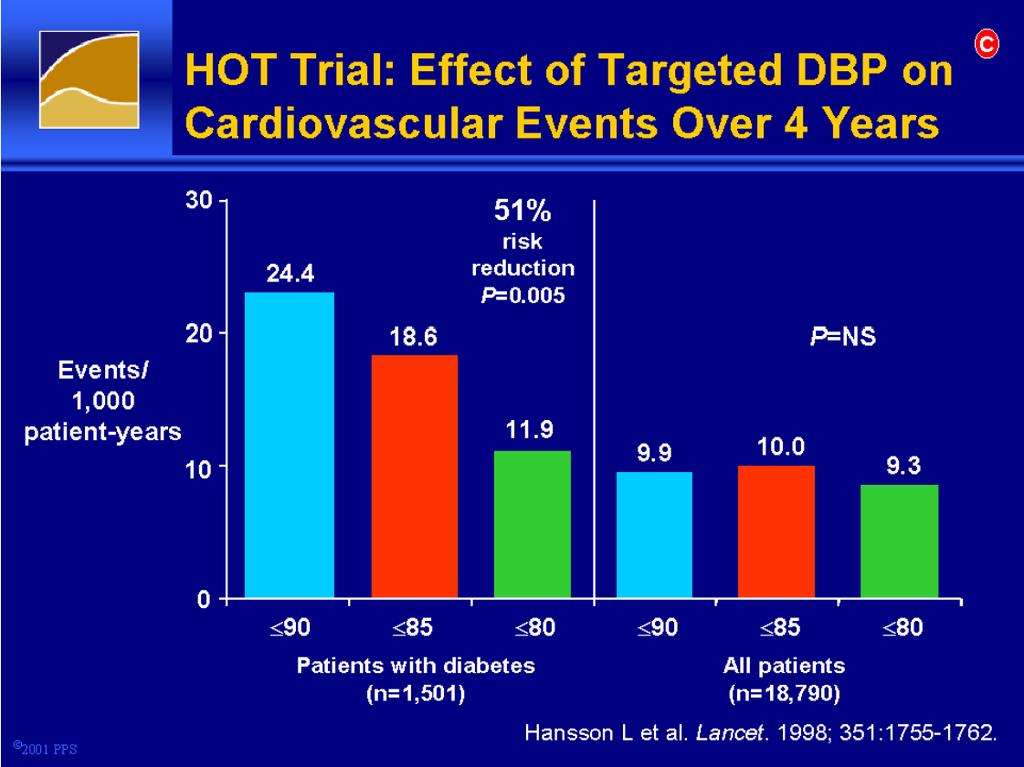
71 Hypertension Optimal Treatment

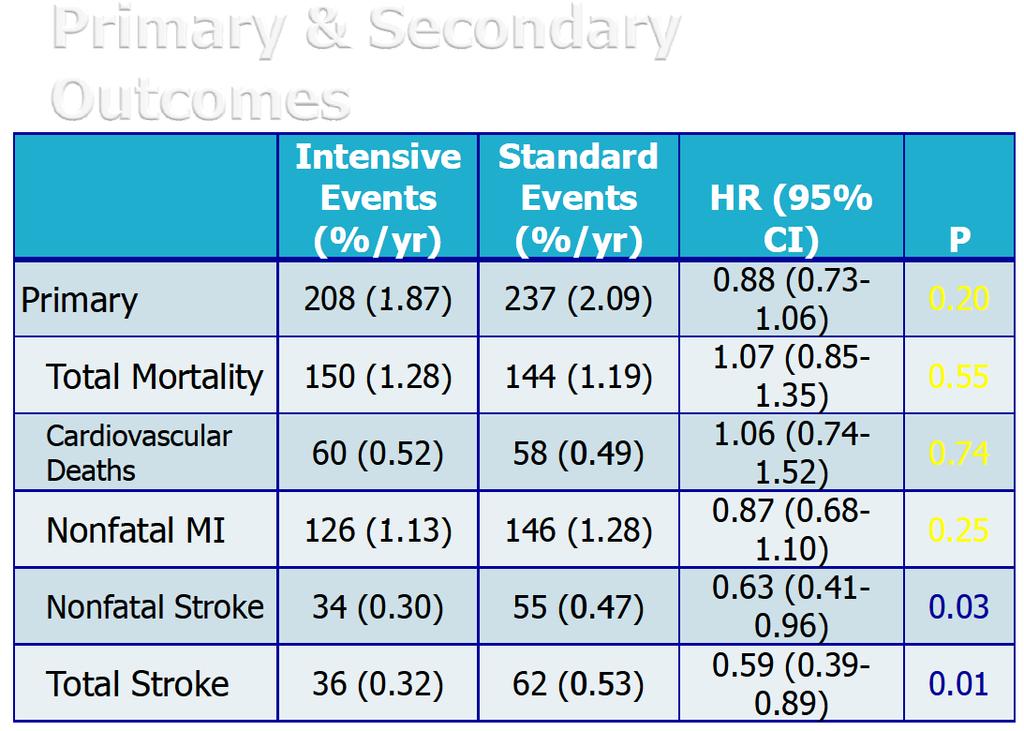
72 HOT trial Non diabetics

73 HOT trial Diabetics
74
75
76
77
78
79
80

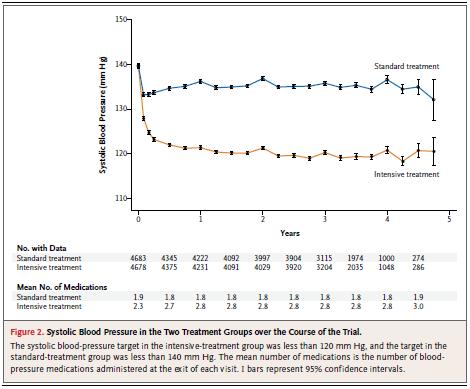
81 Randomised open label study 9361 average BP 140/78 at start Intensive 120/- or Standard 140/- Stopped early after 3.2yrs
82
83
84
85 Conclusions? How I see it anyway Good evidence for lowering BP in stage 2 BP reducing mortality and morbidity (SHEP) Some evidence for tighter targets for diabetic patients reducing cardiovascular mortality but not total mortality but from starting BP (HOT) Some emerging evidence for tighter BP targets in one recent study (SPRINT). Little difference between different drug groups (ASCOT, ALLHAT)
86 Conclusions 2 Medications for mild hypertension not demonstrated (apart from SPRINT) Tighter BP targets in CKD is based on observation of association not RCTs Some evidence that ACEI less good in black ethnic groups

87 Hypertension Implementing NICE guidance 2 nd Edition March 2013 NICE clinical guideline 127
88 High Blood Pressure: Background Major risk factor for stroke, myocardial infarction, heart failure, chronic kidney disease, cognitive decline and premature death. Untreated hypertension can cause vascular and renal damage leading to a treatment-resistant state. Each 2 mmhg rise in systolic blood pressure associated with increased risk of mortality: 7% from heart disease 10% from stroke.
89 Epidemiology Hypertension is common in the UK population. Prevalence influenced by age and lifestyle factors. 25% of the adult population in the UK have hypertension. 50% of those over 60 years have hypertension. With an ageing population, the prevalence of hypertension and requirement for treatment will continue to increase.
90 Definitions Stage 1 hypertension: Clinic blood pressure (BP) is 140/90 mmhg or higher and ABPM or HBPM average is 135/85 mmhg or higher. Stage 2 hypertension: Clinic BP 160/100 mmhg is or higher and ABPM or HBPM daytime average is 150/95 mmhg or higher. Severe hypertension: Clinic BP is 180 mmhg or higher or Clinic diastolic BP is 110 mmhg or higher.
91 Diagnosis (1) If the clinic blood pressure is 140/90 mmhg or higher, offer ambulatory blood pressure monitoring (ABPM) to confirm the diagnosis of hypertension.
92 Diagnosis (2) When using the following to confirm diagnosis, ensure: ABPM: at least two measurements per hour during the person s usual waking hours, average of at least 14 measurements to confirm diagnosis HBPM: two consecutive seated measurements, at least 1 minute apart blood pressure is recorded twice a day for at least 4 days and preferably for a week measurements on the first day are discarded average value of all remaining is used.
93 Initiating drug treatment Offer antihypertensive drug treatment to people: who have stage 1 hypertension, are aged under 80 and meet identified criteria who have stage 2 hypertension at any age. If aged under 40 with stage 1 hypertension and without evidence of target organ damage, cardiovascular disease, renal disease or diabetes, consider: specialist evaluation of secondary causes of hypertension further assessment of potential target organ damage.
94 Monitoring drug treatment (1) Use clinic blood pressure measurements to monitor response to treatment. Aim for target blood pressure below: 140/90 mmhg in people aged under /90 mmhg in people aged 80 and over
95 Type 2 Diabetes BP targets
96 Monitoring drug treatment (2) For people identified as having a white-coat effect consider ABPM or HBPM as an adjunct to clinic blood pressure measurements to monitor response to treatment. Aim for ABPM/HBPM target average of: below 135/85 mmhg in people aged under 80 below 145/85 mmhg in people aged 80 and over. White-coat effect: a discrepancy of more than 20/10 mmhg between clinic and average daytime ABPM or average HBPM blood pressure measurements at the time of diagnosis.
97 CBPM 140/90 mmhg & ABPM/HBPM 135/85 mmhg Stage 1 hypertension CBPM 160/100 mmhg & ABPM/HBPM 150/95 mmhg Stage 2 hypertension Care pathway If target organ damage present or 10-year cardiovascular risk > 20% Offer antihypertensive drug treatment If younger than 40 years Consider specialist referral Offer lifestyle interventions Offer patient education and interventions to support adherence to treatment Offer annual review of care to monitor blood pressure, provide support and discuss lifestyle, symptoms and medication

98 Aged under 55 years A Aged over 55 years or black person of African or Caribbean family origin of any age C 2 Step 1 Summary of antihypertensive drug treatment A + C 2 A + C + D Resistant hypertension A + C + D + consider further diuretic 3, 4 or alpha- or beta-blocker 5 Consider seeking expert advice Step 2 Step 3 Step 4 Key A ACE inhibitor or low-cost angiotensin II receptor blocker (ARB) 1 C Calcium-channel blocker (CCB) D Thiazide-like diuretic See slide notes for details of footnotes 1-5

99 Choosing antihypertensive drug treatment Offer people aged 80 and over the same antihypertensive drug treatment as people aged over 55, taking into account any comorbidities. Drug treatment

100 * See notes Measuring blood pressure: updated recommendations Standardise the environment and provide a relaxed, temperate setting with the person quiet and seated. When using an automated device: palpate the radial or brachial pulse before measuring blood pressure. If pulse if irregular measure blood pressure manually ensure that the device is validated* and an appropriate cuff size for the person s arm is used.
101 Assessing cardiovascular risk and target organ damage: updated recommendations Use a formal estimation of cardiovascular risk to discuss prognosis and healthcare options with people with hypertension. For all people with hypertension offer to: test urine for presence of protein take blood to measure glucose, electrolytes, creatinine, estimated glomerular filtration rate and cholesterol examine fundi for hypertensive retinopathy arrange a 12-lead ECG.
102 Additional recommendations Lifestyle interventions Offer guidance and advice about: diet (including sodium and caffeine intake) and exercise alcohol consumption smoking. Patient education and adherence Provide: information about benefits of drugs and side effects details of patient organisations an annual review of care.
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Hypertension Clinical case scenarios for primary care
 Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Hypertension Clinical case scenarios for primary care Implementing NICE guidance August 2011 NICE clinical guideline 127 What this presentation covers Five clinical case scenarios, including: presentation
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127
 Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension in adults: diagnosis and management Clinical guideline Published: 24 August 2011 nice.org.uk/guidance/cg127 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
CVD Risk of Hypertension. Regina Giblin CVD Clinical Development Coordinator
 CVD Risk of Hypertension Regina Giblin CVD Clinical Development Coordinator CVD Clinical Development Coordinator In-house education for your team: Regina Giblin giblinr@bhf.org.uk Often interactive with
CVD Risk of Hypertension Regina Giblin CVD Clinical Development Coordinator CVD Clinical Development Coordinator In-house education for your team: Regina Giblin giblinr@bhf.org.uk Often interactive with
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
NICE BHS Hypertension guidelines 2011 update
 NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
NICE BHS Hypertension guidelines 2011 update Review for clinicians Sept 2011 Mark Thomas West Midlands Hypertension Centre Heart of England NHS Trust www.wmhc.co.uk mark.thomas@heartofengland.nhs.uk Full
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Impact of Recent Hypertension Guidelines on Clinical Practice
 C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
C H A P T E R 144 Impact of Recent Hypertension Guidelines on Clinical Practice NK Soni, VB Jindal The movement towards evidence-based healthcare has been gaining ground quickly over the past few years,
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Acre Surgery Diviash Thakrar
 Blood Pressure Acre Surgery Diviash Thakrar Why Are We Doing This? 1. Improve education for patients within the practice 2. Allow us use this for general health promotion Raise money for charity 3. Raise
Blood Pressure Acre Surgery Diviash Thakrar Why Are We Doing This? 1. Improve education for patients within the practice 2. Allow us use this for general health promotion Raise money for charity 3. Raise
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Primary hypertension in adults
 Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
The State of Hypertension in NZ in 2010 personal view
 The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011)
") Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Volume 6; Number 1 January 2012 NICE CLINICAL GUIDELINE 127: HYPERTENSION CLINICAL MANAGEMENT OF PRIMARY HYPERTENSION IN ADULTS (AUGUST 2011) What s new in hypertension? NICE has issued an updated Clinical
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Traitements associés chez l hypertendu: Statines, Aspirine
 Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
h i g h b l o o d p r e s s u r e
 h i g h b l o o d p r e s s u r e where are we at? The recent literature has raised doubts about the role of ßblockers for lowering blood pressure and the New Zealand Guidelines Group is updating the Assessment
h i g h b l o o d p r e s s u r e where are we at? The recent literature has raised doubts about the role of ßblockers for lowering blood pressure and the New Zealand Guidelines Group is updating the Assessment
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
North of Tyne and Gateshead Guidelines for Management and Diagnosis of Hypertension Reviewed August 2017
 North of Tyne and Gateshead Guidelines for Management and Diagnosis of Hypertension Reviewed August 2017 An electronic version of this document can also be viewed / downloaded from the North of Tyne and
North of Tyne and Gateshead Guidelines for Management and Diagnosis of Hypertension Reviewed August 2017 An electronic version of this document can also be viewed / downloaded from the North of Tyne and
Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation
 TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
TrialResults-center.org www.trialresultscenter.org Cholesterol lowering intervention for cardiovascular prevention in high risk patients with or without LDL cholesterol elevation A systematic review and
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Outcomes in Hypertensive Black and Nonblack Patients Treated With Chlorthalidone, Amlodipine, and Lisinopril JAMA. 2005;293:
 ORIGINAL CONTRIBUTION Outcomes in Hypertensive and Patients Treated With, Amlodipine, and Lisinopril Jackson T. Wright, Jr, MD, PhD J. Kay Dunn, PhD Jeffrey A. Cutler, MD Barry R. Davis, MD, PhD William
ORIGINAL CONTRIBUTION Outcomes in Hypertensive and Patients Treated With, Amlodipine, and Lisinopril Jackson T. Wright, Jr, MD, PhD J. Kay Dunn, PhD Jeffrey A. Cutler, MD Barry R. Davis, MD, PhD William
TREATMENT AND COMPLICAtions
 ORIGINAL CONTRIBUTION JAMA-EXPRESS Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic The Antihypertensive and
ORIGINAL CONTRIBUTION JAMA-EXPRESS Major Outcomes in High-Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic The Antihypertensive and
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Abbreviations Cardiology I
 Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Cardiology I and Clinical Controversies Joseph J. Saseen, Pharm.D., FCCP, BCPS (AQ Cardiology) Reviewed by Stuart T. Haines, Pharm.D., FCCP, BCPS; and Michelle M. Richardson, Pharm.D., FCCP, BCPS Learning
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure