Emerging Trends in Critical Card Nursing Symposium GSLC AACCN March 17, Marye J. Gleva M.D. F.A.C.C. F.H.R.S. Professor of Medicine
|
|
|
- Mitchell Goodwin
- 6 years ago
- Views:
Transcription
1 Understanding the ECG in Arrhythmias and Pacemakers: A Case Based Approach Emerging Trends in Critical Card Nursing Symposium GSLC AACCN March 17, 2017 Marye J. Gleva M.D. F.A.C.C. F.H.R.S. Professor of Medicine 1
2 Disclosures None relevant to today s topic Clinical Trial Endpoint Committees BIOTRONIK Protego Lead Boston Scientific CAPTIVATE KESTRA-- WCD Medtronic MRI; IMPROVE SCA NIH CABANA Research Grants BIOTRONIK to ACC/NCDR 2
3 Objectives Recognize the common causes of narrow complex tachycardia Recognize the common causes of a wide complex tachycardia Understand the basics of implantable pacemakers 3
4 Approaching an ECG of a Tachycardia Rate (bpm or CL) Atrial Ventricular Same or different QRS narrow or wide? What is the QRS morphology RBBB, LBBB, LAD, RAD etc? QRS regular or irregular? 4
5 Objectives Recognize the common causes of narrow complex tachycardia Recognize the common causes of a wide complex tachycardia Understand the basics of implantable pacemakers 5

6 Common SVTs AT= atrial tachycardia AVNRT = AV node reentry tachycardia AP = Accessory pathway mediated tachycardia General concepts to remember: The AV node can conduct forward and backwards antegrade and retrograde An AP can also conduct antegrade and retrograde Antegrade = preexcitation 6
 ORT: The circuit is the AVN antegrade and the accessory pathway retrograde; so the QRS is narrow ART (wide complex): The circuit is an accessory pathway antegrade")
7 Regular Narrow Complex Tachycardias 1. AVNRT= AV node reentry tachycardia The circuit is in the AV node and perinodal region; can extend to the os of the coronary sinus 2. AVRT = AV reentry tachycardia (WPW) ORT: The circuit is the AVN antegrade and the accessory pathway retrograde; so the QRS is narrow ART (wide complex): The circuit is an accessory pathway antegrade and either the AVN or another accessory pathway retrograde; the QRS is wide 3. Atrial Flutter The circuit is in the atrium 4. Atrial tachycardia Usually not reeentrant; a focal mechanism ( irritable site ) 5. Sinus tachycardia Associated with fever, illness, PE, volume depletion, tamponade etc 7
8 Another Classification of SVT The RP interval Measured from the onset of the QRS to the retrograde p wave Short RP (<½ of the R-R interval) tachycardia AVNRT ORT Long RP (>½ R-R interval)tachycardia Atypical AVNRT Atrial tachycardia PJRT the permanent form of junctional reciprocating tachycadia A decremental accessory pathway 8
9 Irregular Supraventricular Tachycardia 1. Atrial fibrillation No clear p waves; variable QRS or RR intervals 2. Atrial tachycardia Multifocal atrial tachycardia Three different p waves and PR intervals Some ATs can have rate variability based on variable autonomic tone 9

10 Multifocal Atrial Tachycardia 10
11 Atrial Fibrillation 11
12 Objectives Recognize the common causes of narrow complex tachycardia Recognize the common causes of a wide complex tachycardia Understand the basics of implantable pacemakers and ICDs 12
13 Wide Complex Tachycardia SVT with aberration Preexcited SVT Mahaim PPM mediated tachycardia VT Myocardial/scar Fascicular RVOT BBRT 13
14 VENTRICULAR TACHYCARDIA 14
15 Preexcited Atrial Fibrillation 15
 Bidirectional VT Brugada et al (more Brugadas) Circulation 1991")
16 WCT: Brugada Criteria Wide Complex Tachycardia Regular VT SVT with RBBB or LBBB aberration Irregular Caveats» Preexcited tachycardia» Mahaim tachycardia» Pacemaker mediated tachycardia Atrial fibrillation with aberration Polymorphic VT (PMVT) Bidirectional VT Brugada et al (more Brugadas) Circulation
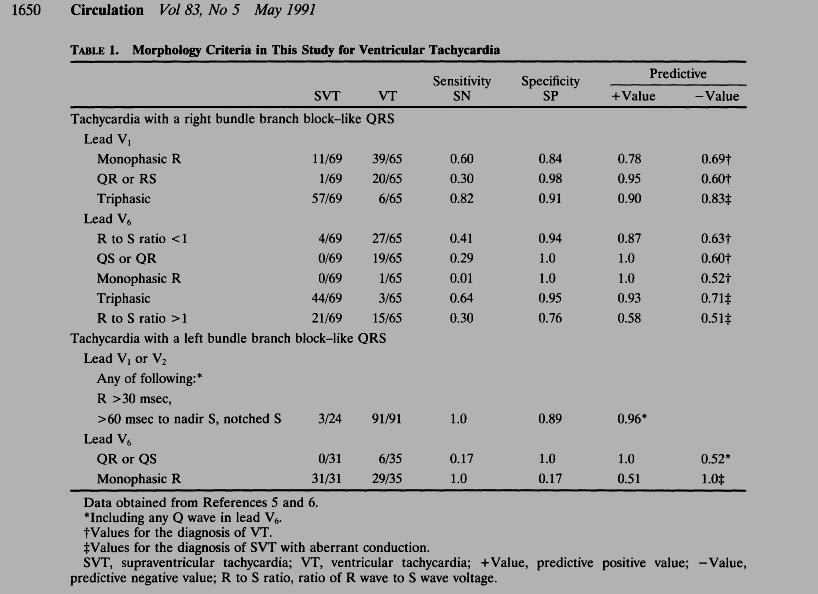
17 WCT: Brugada Criteria 1. Absence of RS across precordium 2. R to S > 100 msec in precordial lead 3. AV dissociation 4. Morphology criteria Brugada et al Circulation 1991; 83 (5) 17
18 WCT Brugada Criteria/Morphology 18
19 WCT: Wellens Criteria Original paper Am J Med 1978: 64: $40 to get from journal website Not available through Becker Updated version published in 2001 Same guy who described pre infarction anterior TW inversions 19

20 WCT: Wellens Criteria Do not panic when confronted with a wide QRS tachycardia QRS width >160 msec Concordance All Qs or all Rs in precordial leads Axis AV Dissociation Use of Lewis lead 20

21 avr Criteria for WCT 21
22 avr Criteria Presence of an initial R wave in avr? yes no VT Presence of initial q wave or r wave > 40 msec no Presence of a notch on descending limb of a predominately negative onset and predominately negative QRS no yes yes VT VT v i /v t 1 yes no VT SVT Vereckei A et al HR 2008; 5:

23 avr Criteria for VT 23
24 Objectives Recognize the common causes of narrow complex tachycardia Recognize the common causes of a wide complex tachycardia Understand the basics of implantable pacemakers 24
25 Why do Patients Have Pacemakers? Symptoms from a slow heart beat Sinus node dysfunction AV node dysfunction Complete heart block Heart Failure indications NYHA Class II-IV LBBB LVEF <35% 25
26 Indications for permanent pacing Class I Symptomatic sinus bradycardia, chronotropic incompetence, or bradycardia due to required drug therapy Symptomatic second-degree AVB (Mobitz I or II) and thirddegree AVB Asymptomatic Mobitz II Asymptomatic third-degree AVB with escape > 40 bpm with cardiomegaly Alternating bundle branch block Transient AVB with associated bundle branch block after STEMI Recurrent syncope with carotid pressure and asystole of > 3 seconds Heart Rhythm 2008;5:934 26
27 Indications for permanent pacing Class II Class IIa Sinus brady < 40, symptoms, but no clear correlation between the two HV 100 ms during EPS Syncope with bifascicular block when other causes are excluded Syncope of unclear cause, and asystole > 3sec with carotid pressure Class IIb Minimal symptoms with sinus brady at < 40 bpm while awake Syncope with significant bradycardia documented on tilt table testing 27
28 Indications for permanent pacing Class III A PPM is NOT indicated in these situations: Asymptomatic sinus node dysfunction Asymptomatic first-degree AVB Bifascicular block ± first-degree AVB without symptoms or AVB Situational vasovagal syncope when behavior modification is preferred 28
29 The Basics of PPMs To have a device interrogated, you need to know Manufacturer Medtronic Boston Scientific (Guidant) St. Jude Biotronik ELA Don t know? Ask the patient! Should have ID card Look at CXR 29

30 Pacemaker MODE 30
31 Important concepts in pacing: it s all about TIMING Lower rate limit (LRL) Upper rate limit (URL) Atrioventricular delay (AVD) ~ PR interval HR (bpm) CL (ms) Bpm=60,000/CL 31
32 Commonly seen PPM Modes VVI Paces Ventricle only Senses Ventricle only Response to an event sensed in the ventricle = Inhibit pacing output 32
33 DDD Paces - atrium and ventricle (Dual) Senses atrium and ventricle (Dual) Response: of atrial lead to a sensed event in the atrium = inhibit pacing output in the atrium of ventricular lead to a sensed event in the ventricle = inhibit pacing output in the ventricle of ventricular lead to a sensed event in the atrium = track Therefore, response is both inhibit and track (Dual) 33
34 Lower rate limit (LRL) VVI 60 bpm 1000 ms Sensed event: Timer resets 1000 ms 34
35 DDD bpm, AVD=200 ms URL 500 ms AVD URL is inviolable If URL is 120 bpm, then ventricular paced beats cannot be more than 120 bpm 35
36 PPM Response to Atrial Arrhythmias: Mode switch Avoids tracking of atrial fibrillation Only possible in dual chamber pacemakers Programmable On/ Off/ Detection rate For example, if mode switch rate is at 150 bpm, the device will automatically switch from DDD to VVI mode when > the atrial rate is > 150 bpm Mode switch episodes in general can correlate to episodes of atrial fibrillation 36
37 How to Look at a PPM ECG Scan the tracing for the following: What is the rhythm? How many types of pacing spikes seen? Is there capture in each chamber? Is there sensing in each chamber? Is the paced morphology appropriate? Are there appropriate periods of non paced timing? Pauses Other algorithms functioning (ie EP fellowship) Consider a peek at the CXR,,,, 37
38 Now for the Case Based Approach Narrow complex tachycardias Wide complex tachycardias PPM cases An overview of arrhythmia management 38
39 Narrow Complex Tachycardia Case #1: SS 70 y/o female with LE edema for 3 days Presented to ED and developed elevated HR PMHx: HTN Remote CVA 39

40 Narrow Complex Tachycardia Case 1 Rate 180 bpm Narrow QRS, no clear p waves Short RP tachycardia; likely AVNRT Treated with adenosine; added oral BB Outpt follow-up for ablation 40

41 SVT Case 1: After Adenosine 41
42 Narrow Complex Tachycardia Case #2: KB 27 y/o male with palpitations Presented to ED with elevated heart rate for 3 days Admitted to inpatient service PMHx: Repaired congenital heart disease dtga; s/p Mustard 42

43 SVT Case #2 HR 150s, almost RBB and RAD. Given CHD, likely SVT Adenosine 6 mg IV then 12 mg IV 43

44 SVT Case #2: After Adenosine Now can see the flutter waves Heparin drip started, BB for rate control TEE to r/o LAA clot and then CV Taken to EP lab and underwent ablation of the atrial isthmus between the TV and the IVC 44
45 SVT Case #3: VZ Young female with racing heart beats Persistent after walking across campus To ED, seen in consult in ED after adenosine given PMHx: None 45

46 46 SVT Case #3: VZ

47 47 SVT Case #3: NSR

48 SVT Case #3: NSR Again. 48
49 Wide Complex Tachycardia: Case 1 83 y/o male Ischemic CM with EF 20% ICD present S/P VT RFA Presents with palpitations 49



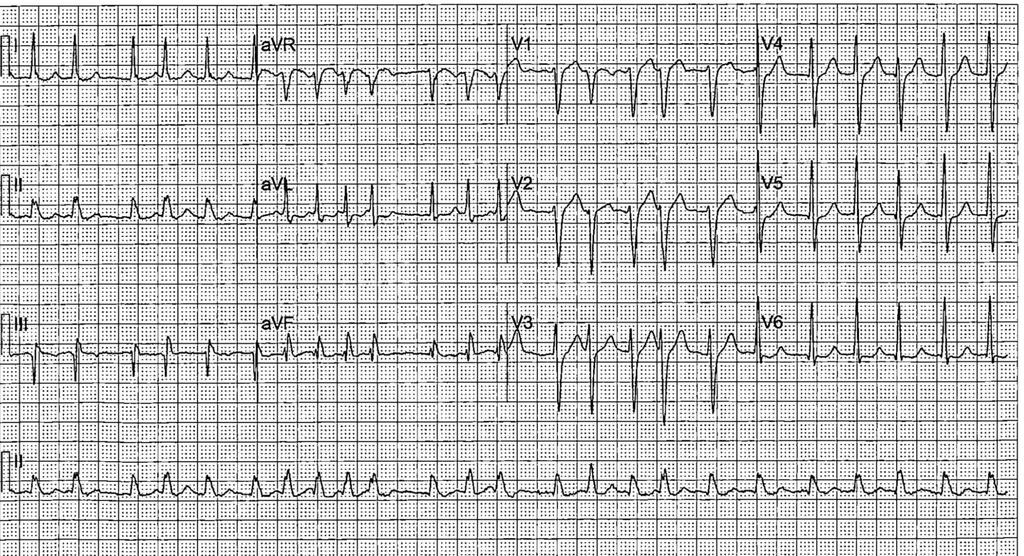
50 WCT Case #1 WG AVR criteria = VT Brugada Step 2 = VT RBBB LAD WCT Rate 100 bpm ECG consistent with VT by two algorithms Acute Management Amiodarone 150 mg IV, then drip Attempted ATP 50
51 WCT Case #2: JI 49 y/o male Presents with worsening CHF Hypercoagulable state with mutiple prior embolic events R ICD Allergy to amiodarone 51


52 WCT Case #2: JI LBBB LAD WCT tachycardia Rate 140 bpm VT by AVR criteria and Brugada; probable AV diss Lidocaine IV 100 mg then 1 mg/min 52
53 WCT Case #3 SC 70 y/o male S/P Aortic root repair for aneurysm Remote hx of AVR for bicuspid aortic valve Known LV dysfunction with EF 35% BIV ICD Arrhythmia noted on telemetry one night at BJH.. 53

54 WCT Case #3 SC RBBB RAD WCT Rate 170 msec Possible P wave in lead V2 preceeding each QRS. AVR with q wave suggests Hmmmm SVT or VT???? 54

55 WCT Case #3 SC ATP from ICD terminates VT 55
56 WCT Case #4 DC 43 y/o male with NICM EF 30% Prior history of VSD repair VHD with AI Admitted with frequent palpitations and associated SOB 56

57 WCT Case #4 DC RBBB RAD irregular WCT Average rate 150 bpm VT suggested by AVR criteria Slowed with beta blockers Recurred so taken to EP lab AT near CS os ablated 57

58 WCT Case #4: NSR 58
59 WCT Case #5 53 y/o male with recurrent angina and palpitations ECG recorded upon arrival in ED Tachycardia spontaneously terminated Not on digoxin 59
60 WCT Case #5 RBBB alternating axis WCT Rate 140 bpm Very bizarre axis leads II, III AVR criteria suggests VT 60
61 AVR Criteria Bidirectional VT CC with RCA and LAD disease; s/p PCI Abnormal MRI ICD implant with BB 61
62 PPM Case #1: What is shown on this ECG? 62
63 PPM Case #2: What is Happening Here? 63
64 PPM Case #3: Appropriate PPM Function? 64

65 PPM Case #4: Is this Appropriate Pacemaker Function? 65


66 PPM Case #4: Does this CXR Confirm Your Dx? 66

67 PPM Case #5 A new patient is admitted with syncope. She s getting dizzy again. The problem is: A. Failure to capture B. Failure to sense 67
 Asynchronous")
68 PPM Case #6 The problem is: A. Failure to capture B. Failure to sense C. Oversensing Solutions: Increase sensitivity (make less sensitive) Asynchronous pacing 68
69 Management of Arrhythmias Diagnosis Crucial as it guides therapy Management Rate control Adenosine Beta blockers Calcium channel blockers IV and/or PO diltiazem» Rare to use verapamil as it is a potent negative inotrope. Is used in HCM IV and/or PO amiodarone AVN ablation with PPM or ICD implant Rhythm control Adenosine/ Beta blockers/ Calcium channel blockers if triggered activity such as atrial tachycardia Digoxin (rarely) AA drugs Ablation 69
70 ACLS
71 Acute Management of Atrial Fibrillation Hemodynamically stable or unstable? If unstable, urgent synchronized cardioversion Anticoagulation: yes or no If anticoagulation contraindicated, rate control strategy Rate control vs. rhythm control Symptoms Concomitant cardiac conditions HCM CHD Factors affecting choices for pharmacologic rhythm control Liver renal or lung problems LVEF 71
:2246-2280. doi:10.1016/j.jacc.2014.03.")
72 From: 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society J Am Coll Cardiol. 2014;64(21): doi: /j.jacc Figure Legend: Strategies for rhythm control in patients with paroxysmal and persistent AF. *Catheter ablation is only recommended as first-line therapy for patients with paroxysmal AF (Class IIa recommendation). Drugs are listed alphabetically. Depending on patient preference when performed in experienced centers. Not recommended with severe LVH (wall thickness >1.5 cm). Should be used with caution in patients at risk for torsades de pointes ventricular tachycardia. Should be combined with AV nodal blocking agents. AF indicates atrial fibrillation; AV, atrioventricular; CAD, Date coronary of download: artery disease; HF, heart failure; Copyright and LVH, The left ventricular American hypertrophy. College of Cardiology. 4/28/2015 All rights reserved. 72
73 Common Drugs for Intravenous Rate Control Drug IV Dose Metoprolol 1.25 to 5 mg q6-12 hours Propranolol Diltiazem 1mg IV; repeat q5 min up to 5 mg 0.25mg/kg bolus over 2 minutes (15-20 mg) then mg/hr Amiodarone 150 mg IV; then mg/min Digoxin 0.25 mg IV 73
74 Common Drugs for Intravenous Rhythm Control Drug IV Dose Amiodarone 150 mg IV bolus; 1 mg/min for 6 hours then 0.5 mg/min Lidocaine 1 Procainamide 1,2 1 mg/kg bolus, then 1-3 mg/min mg/kg bolus then 1-4 mg/min ECG and continuous telemetry for all anti-arrhythmic drugs 1 Monitor levels 2 Caution if renal dysfunction 74



75 Other Rate Control Strategies AVN ablation with pacemaker implant The ultimate in rate control 75
76 Ventricular Arrhythmias: Treatment ICDs are the mainstay of treatment for patients with mmvt, PMVT or VF [secondary prevention] Beta blockers Maximize doses AA drugs (Class III) and ablation are adjuvant treatments Amiodarone, sotalol, mexilitene ICDs provide a mortality benefits Ablation to reduce shocks or events 76
77 Conclusions A straightforward approach can be used for diagnosis of tachycardias based on the ECG Regular vs irregular If regular, one of 5 diagnoses likely If irregular, one of 2 diagnoses likely Do not panic with any WCT; remember AVR Management is ACLS Consider expert consultation 77
78 Selected References American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Circulation. 2015;132:S315-S367, originally published October 14, AHA/ACC/HRS AF 2014 Guidelines J Am Coll Cardiol. 2014;64(21): doi: /j.jacc avr Criteria Vereckei A et al HR 2008; 5:
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group Disclosures No financial relationships to disclose Objectives At the conclusion of this activity,
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천
 The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
The Efficient and Smart Methods for Diagnosis of SVT 대구파티마병원순환기내과정병천 Differentiation Supraventricular Origin from Ventricular Origin on ECG. QRS-Complex Width. 1. Narrow QRS-Complex Tachycardia (
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
Return to Basics. Normal Intervals & Axes. ECG Rate and Rhythm
 Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Return to Basics Management of the Hospitalized Patient October 15, 2010 ECG Refresher and Update 2010 Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none
 ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none TEST EXAMPLE What is the colour of this rectangle? 1. Blue? 2. Red? 3. Purple? 4. Green? 5. Yellow? 6. 1 and 3? 7. Any of
ECG QUIZ Luc DE ROY Brussels Belgium Disclosure in relation to this topic: none TEST EXAMPLE What is the colour of this rectangle? 1. Blue? 2. Red? 3. Purple? 4. Green? 5. Yellow? 6. 1 and 3? 7. Any of
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
BHRS Prep course Pub style Quiz NOT A
 BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
How To Think About Rhythms and Conduction
 How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
How To Think About Rhythms and Conduction Frank Yanowitz, MD Professor of Medicine (Cardiology) University of Utah School of Medicine Medical Director, IHC ECG Services Intermountain Healthcare http://ecg.utah.edu
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst
 Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst 1. Patient K.P., male, 68 years Fatigue Exercise intolerance for
Cardiology update Clinical Decision Seminar: Difficult ECG Interpretations February 13th, 2013 Lars Eckardt Firat Duru Corinna Brunckhorst 1. Patient K.P., male, 68 years Fatigue Exercise intolerance for
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Arrhythmias (II) Ventricular Arrhythmias. Disclosures
 Ventricular Arrhythmias. Disclosures") Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Arrhythmias (II) Ventricular Arrhythmias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Rhythms and Mortality Implantable loop recorder post-mi
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019
 THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
THE ELECTROCARDIOGRAM A UBIQUITOUS AND COST-EFFECTIVE DIAGNOSTIC TOOL FOR THE FAMILY MEDICINE REFRESHER COURSE MARCH 8, 2019 Major Clinical Disorders Pulmonary Embolism 69 y/o woman with dyspnea and an
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology
 EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
Bundle Branch & Fascicular Blocks. Reading Assignment (p53-58 in Outline )
") Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
Bundle Branch & Fascicular Blocks Reading Assignment (p53-58 in Outline ) Objectives 1. QRS analysis of Right and Left BBB 2. Uncomplicated vs complicated BBB 3. Diagnosis of RBBB with LAFB and LPFB 4.
INTERESTING ECGS. Wide-complex tachycardias 11/13/ yr male with acute ant wall MI, S/P primary PTCA
 INTERESTING ECGS V S Prakash Prof, & Head Dept. of Cardiology M S Ramaiah Hospitals 50 yr male with acute ant wall MI, S/P primary PTCA Pt. underwent successful PAMI An hour later,in the CCU Ventricular
INTERESTING ECGS V S Prakash Prof, & Head Dept. of Cardiology M S Ramaiah Hospitals 50 yr male with acute ant wall MI, S/P primary PTCA Pt. underwent successful PAMI An hour later,in the CCU Ventricular
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Dr.Binoy Skaria 13/07/15
 Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
Dr.Binoy Skaria binoyskaria@hotmail.com binoy.skaria@heartofengland.nhs.uk 13/07/15 Acknowledgement Medtronic, Google images & Elsevier for slides Natalie Ryan, Events Manager, HEFT- for organising the
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017
 Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017 Normal EKG EKG boxes Heart Rate 1 big box = 200ms 1 small box = 40ms Big Boxes Between QRS complexes Heart
Fast & Slow Tachy & Brady Arrhythmias DAVID STULTZ, MD, FACC KPN HEART & VASCULAR AUGUST 7, 2017 Normal EKG EKG boxes Heart Rate 1 big box = 200ms 1 small box = 40ms Big Boxes Between QRS complexes Heart
Supraventricular Arrhythmias. Reading Assignment. Chapter 5 (p17-30)
") Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
Supraventricular Arrhythmias Reading Assignment Chapter 5 (p17-30) The Supraventricular Rhythms In Our Lives Site of Origin Single Events Slow Rates Intermediate Rates Fast Rates (>100 bpm) Sinus Sinus
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Unknown ECGs for the Clinician
 Unknown ECGs for the Clinician 2016 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board for Medtronic
Unknown ECGs for the Clinician 2016 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board for Medtronic
Ventricular arrhythmias
 Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
Ventricular arrhythmias Assoc.Prof. Lucie Riedlbauchová, MD, PhD Department of Cardiology University HospitalMotol and2nd FacultyofMedicine, Charles University in Prague Definition and classification Ventricular
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm
 Discharges ICD Storm") Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
Recurrent Implantable Defibrillator Discharges (ICD) Discharges ICD Storm Guy Amit, MD, MPH Soroka University Medical Center Ben-Gurion University of the Negev Beer-Sheva, Israel Disclosures Consultant:
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Episode 112 Tachydysrhythmias
 Wide & regular tachydysrhythmias Ventricular Tachycardia (VT) vs SVT with aberrancy: Assume VT Episode 112 Tachydysrhythmias With Amal Mattu & Paul Dorion Prepared by Shaun Mehta, July 2018 General Approach
Wide & regular tachydysrhythmias Ventricular Tachycardia (VT) vs SVT with aberrancy: Assume VT Episode 112 Tachydysrhythmias With Amal Mattu & Paul Dorion Prepared by Shaun Mehta, July 2018 General Approach
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ
 Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Seek and Ye Shall Find: Surprising Findings When Using the ILR-LINQ Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System www.arrhythmia.org; @drsuneet October 31, 2015
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh
 Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Arrhythmias and Heart Failure Dr Chris Lang Consultant Cardiologist and Electrophysiologist Royal Infirmary of Edinburgh Arrhythmias and Heart Failure Ventricular Supraventricular VT/VF Primary prevention
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC
, FACC") Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Hatim Al Lawati. MD, FRCPC, DABIM(CV), FACC Consultant Interventional Cardiology & Structural Heart Disease Department of Medicine Sultan Qaboos University Hospital hatim.al.lawati@gmail.com April 2017
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions
 InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
InterQual Care Planning SIM plus Criteria 2014 Clinical Revisions The Clinical Revisions provide details of changes to InterQual Clinical Criteria. They do not provide information on changes made to CareEnhance
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Tachycardia Devices Indications and Basic Trouble Shooting
 Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Tachycardia Devices Indications and Basic Trouble Shooting Peter A. Brady, MD., FRCP Cardiology Review Course London, March 6 th, 2014 2011 MFMER 3134946-1 Tachycardia Devices ICD Indications Primary and
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Sustained tachycardia with wide QRS
 Sustained tachycardia with wide QRS Courtesy from Prof. Antonio Américo Friedmann. Electrocardiology Service of University of Faculty of São Paulo. Opinions from colleagues Greetings to everyone, In a
Sustained tachycardia with wide QRS Courtesy from Prof. Antonio Américo Friedmann. Electrocardiology Service of University of Faculty of São Paulo. Opinions from colleagues Greetings to everyone, In a
Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
 Journal of Geriatric Cardiology (2018) 15: 193 198 2018 JGC All rights reserved; www.jgc301.com Case Report Open Access Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
Journal of Geriatric Cardiology (2018) 15: 193 198 2018 JGC All rights reserved; www.jgc301.com Case Report Open Access Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016
 CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016 + OBJECTIVES Diagnosis and management of ACS When to liaise with tertiary centre Complications of ACS Tachyarrhythmias Bradyarrhythmias
CARDIOLOGY EMERGENCIES ON CALL DR. ALI ROOMI CARDIOLOGY ST3 23RD JULY 2016 + OBJECTIVES Diagnosis and management of ACS When to liaise with tertiary centre Complications of ACS Tachyarrhythmias Bradyarrhythmias
Programming of Bradycardic Parameters. C. W. Israel, M.D. Dept. of Cardiology Evangelical Hospital Bielefeld Germany
 Programming of Bradycardic Parameters C. W. Israel, M.D. Dept. of Cardiology Evangelical Hospital Bielefeld Germany Carsten.Israel@evkb.de Programming of ICD Brady Parameters Conflict of Interest Biotronik
Programming of Bradycardic Parameters C. W. Israel, M.D. Dept. of Cardiology Evangelical Hospital Bielefeld Germany Carsten.Israel@evkb.de Programming of ICD Brady Parameters Conflict of Interest Biotronik
FLB s What Are Those Funny-Looking Beats?
 FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
FLB s What Are Those Funny-Looking Beats? Reading Assignment (pages 27-45 in Outline ) The 5-Step Method ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis=
PAEDIATRIC ECG Dimosthenis Avramidis, MD.
 PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
PAEDIATRIC ECG Dimosthenis Avramidis, MD. Consultant Mitera Children s Hospital Athens Greece S. Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece 5 y/o with sinus tach Background ECG changes
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation?
 How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
How Do I Balance Bradycardia with Rate Control in Atrial Fibrillation? Thang Nguyen MD FRCPC Assistant Professor Section of Cardiology Department of Internal Medicine University of Manitoba Objectives
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Mitchell Cohen MD FACC FHRS Co-Director of the Heart Center Section Chief, Pediatric Cardiology Phoenix Children s Hospital Professor of Child Health
 10 Annoying Reasons an Electrophysiologist Gets Called to the Cardiac ICU Mitchell Cohen MD FACC FHRS Co-Director of the Heart Center Section Chief, Pediatric Cardiology Phoenix Children s Hospital Professor
10 Annoying Reasons an Electrophysiologist Gets Called to the Cardiac ICU Mitchell Cohen MD FACC FHRS Co-Director of the Heart Center Section Chief, Pediatric Cardiology Phoenix Children s Hospital Professor
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists
 PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
PERMANENT PACEMAKERS AND IMPLANTABLE DEFIBRILLATORS Considerations for intensivists Craig A. McPherson, MD, FACC Associate Professor of Medicine Constantine Manthous, MD, FACP, FCCP Associate Clinical
Advances in Ablation Therapy for Ventricular Tachycardia
 Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Advances in Ablation Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS Director, Cardiac Electrophysiology Training Program University of California, San Francisco For those of you who
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Tachy. Induction tachycardia lead ECG during Tachy /25/2009. Sinus Rhythm Single His
 12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
Bryan Heart. Unknown ECGs for the Clinician. Disclaimer 9/2/2015
 Bryan Heart Unknown ECGs for the Clinician 2015 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board
Bryan Heart Unknown ECGs for the Clinician 2015 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Cardiac rhythm detailed monitoring by an implanted pacemaker: The iecg solution
 Cardiac rhythm detailed monitoring by an implanted pacemaker: The iecg solution Francesco Zanon, MD, FESC, FHRS Arrhythmia and Electrophysiology Unit, Cardiology Dept. Santa Maria della Misericordia General
Cardiac rhythm detailed monitoring by an implanted pacemaker: The iecg solution Francesco Zanon, MD, FESC, FHRS Arrhythmia and Electrophysiology Unit, Cardiology Dept. Santa Maria della Misericordia General
(living in the fast lane)
") (living in the fast lane) Presented by M.D. Cardiology IT S A group of ECG and Electrophysiological abnormalities in which The atrial impulses are conducted partly or completely, PREMATURELY, to the ventricles
(living in the fast lane) Presented by M.D. Cardiology IT S A group of ECG and Electrophysiological abnormalities in which The atrial impulses are conducted partly or completely, PREMATURELY, to the ventricles