Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
|
|
|
- Roger Garrison
- 6 years ago
- Views:
Transcription


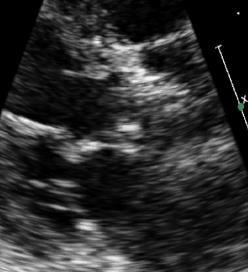
1 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal Long Axis View 1

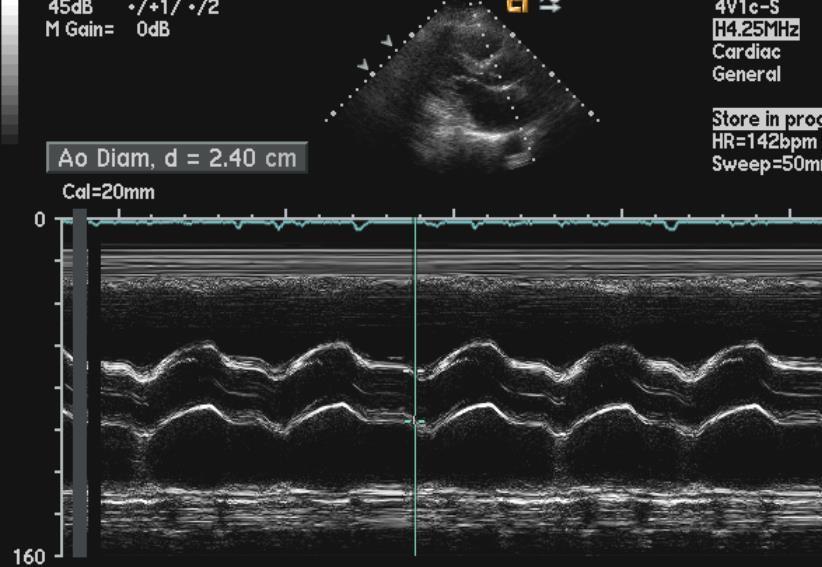
2 Normal AV M-Mode coaptation in center of aortic root 2


3 Normal AV orientation and opening Diastole Systole N R L Aortic Stenosis Etiology Senile/Degenerative Calcific Calcification resembles ectopic bone Risk factors similar to those for atherosclerosis Renal dysfunction may accelerate Premature Calcific Bicuspid / Congenital Rheumatic Less common in the United States Less common Type 2 Hyperlipidemia, SLE, Irradiation, Paget s Dz 3



4 Calcific Aortic Stenosis: Progressive reduction in leaflet motion Spectral Doppler of the AV Apical Five Chamber AS jet AR jet 4

 Associated")
5 Bicuspid Aortic Valve Most common congenital anomaly (1-2%) Commissure may be horizontal or vertical Horizontal: Anterior and Posterior leaflets Vertical: Right and Left (coronary) leaflets Accel. Calcification premature stenosis Proximal aortopathy (even in normals) Associated abnormalities - coarctation Bicuspid Aortic Valve PLAX View Doming Diastole Systole 5



6 Bicuspid Aortic Valve PSAX view morphology Diastole Systole raphe raphe Systolic ellipsoid orifice identifies as Rheumatic Aortic Stenosis: Less calcification, More commissural fusion 6

 Late: Cardinal Symptoms Chest Pressure, Syncope, Congestive Heart")
7 Aortic Valve: Other Anomalies associated with AS Unicuspid AoV Quadracuspid AoV Aortic Stenosis: Physiologic Sequelae Chronic LV pressure overload Myocardial Hypertrophy Progressive, Concentric LA dilatation Progressive diastolic & systolic dysfunction END STAGE: Limited Cardiac Output After long latency SYMPTOMS: Early: Dyspnea and Fatigue (often subtle) Late: Cardinal Symptoms Chest Pressure, Syncope, Congestive Heart Failure 7

8 Evaluation of AS: Echo Essentials Valve Anatomy - establish etiology Exclude other forms of LVOT obstruction Severity of stenosis Physiologic sequelae LV hypertrophy, diastolic fxn, systolic fxn LA dilatation, Pulmonary hypertension Evaluate concurrent disease Proximal aorta and arch Aortic Valve Regurgitation, Mitral Disease Aortic Stenosis: Assessing Severity Peak AV Jet Velocity Mean AV Gradient Valve Area by continuity equation Velocity Ratio ( Dynamic Index ) Planimetry }ASE / EAE Recommend 8

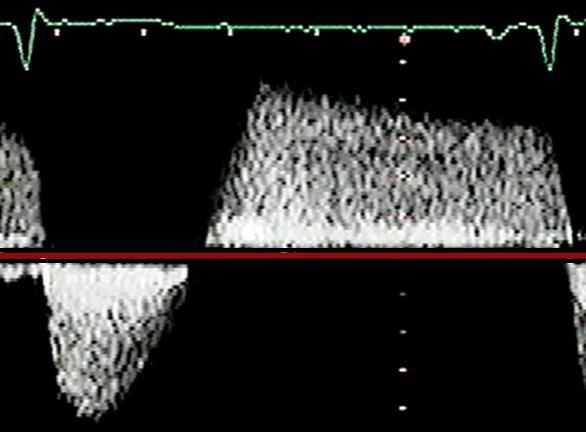
 95:2262 Aortic Stenosis: Peak Velocity Continuous Wave (CW) Doppler in Apical 5 Chamber View Must be parallel to the")
9 Aortic Stenosis: Prognosis of Velocity Variable Rate of Progression Avg ~0.3 m/sec/year High rate of events, even for asymptomatic AS Peak Jet Velocity, Rate of velocity change, Functional status: predict clinical outcome Otto C, et al. Circulation (1997) 95:2262 Aortic Stenosis: Peak Velocity Continuous Wave (CW) Doppler in Apical 5 Chamber View Must be parallel to the ejection jet Confirm Right Parasternal Suprasternal also possible Use highest velocity Avoid feathery signals at tip Piedoff non-imaging probe Decrease gains & adjust baseline 18 9
10 Aortic stenosis Assessment by Peak Velocity Mild stenosis: Moderate stenosis: Severe stenosis: Very Severe or Critical stenosis: m/s m/s > 4.0 m/s > 5.0 m/s Aortic Stenosis: Peak Gradient Peak Gradient = 4 (VAV) 2 Peak Instantaneous Gradient 10
11 Instantaneous vs. Peak to Peak Echo a more physiologic measurement Doppler peak gradient always higher Doppler Cath Mean gradient and AVA should correlate Gradients are flow dependent Aortic Stenosis: Mean Gradient Mean Gradient Integration of velocity over time Estimate 0.7 * Peak Grad. Correlates with cath Peak-to-Peak gradient 11
12 Aortic stenosis Assessment by Mean Gradient Mild stenosis: < 20 mmhg Moderate stenosis: mmhg Severe stenosis: 40 mmhg Velocity and Gradient pitfall: Influence of Cardiac Output High CO = High gradient Aortic regurgitation Hyperdynamic function Low CO = Low gradient Reduced ejection fraction Small ventricular cavity/lvh High systemic vascular resistance/impedance Significant mitral regurgitation 12
13 Aortic stenosis Assessment of Valve Area Normal valve area: = 3-4 cm 2 Mild stenosis: > 1.5 cm 2 Moderate stenosis: cm 2 Severe stenosis: < 1.0 cm 2 Critical stenosis: < 0.7 cm 2 Calculation of AV Area: Continuity Equation Based on conservation of mass Flow within LVOT = Flow across AV LVOT area * VTI LVOT = AVA * VTI AV [π * (LVOT radius ) 2 ] * VTI LVOT = AVA * VTI AV [π * (LVOT radius ) 2 ] * VTI LVOT = AVA VTI AV 13


 flow through")
14 LVOT diameter 2.1 cm Flow through LVOT Pulse Wave Doppler Spectral Envelope With sample volume in LVOT Velocity Time Integral (VTI) flow through a single point VTI = 19 cm 14

 2 x 3.14 x 19 cm 85 cm AVA = 0.")
15 Flow Across the Aortic Valve: Continuous Wave Doppler VTI = 85 cm Calculating Aortic Valve Area AVA = (Diameter LVOT / 2) 2 x π x VTI LVOT VTI AV AVA = (2.1 cm / 2) 2 x 3.14 x 19 cm 85 cm AVA = 0.7 cm 2 15

16 Continuity Equation: Pitfalls LVOT measurement Diameter is squared Can propagate large error LVOT velocity AV velocity Missing the Peak: Use multiple sites / Piedoff / highest velocity Beware MR! Doppler Velocity Index Eliminates errors of LVOT measurement DVI = VTILVOT / VTIAV Criteria for Severe AS: DVI < 0.25 Relatively flow-independent measure of stenosis 16


17 Planimetry of the Aortic Valve AVA = 1.1 cm 2 Planimetry Correlates with invasively obtained areas Flow dependent Difficult to distinguish decreased opening due to LV failure TEE superior - use of color flow area Dense calcification reduces accuracy 17
 22:1-23 So My patient has")

18 Summary Baumgartner H, et al. JASE (2009) 22:1-23 So My patient has severe aortic stenosis! What do I do? Does echo help me? WHEN SHOULD I OPERATE? 18
19 The Good Old Days: The Symptomatic Cliff Braunwald E, et al. Circulation (1968) 38:61-67 Stages of Disease Stage A: At risk for disease Stage B: Progressive disease Stage C: Severe disease (asymptomatic) Stage D: Severe disease (symptomatic) 19
20 Stage C can be subdivided: Stage A: At risk for disease Stage B: Progressive disease Stage C1: Severe (asymptomatic) Compensated LV Stage C2: Severe (asymptomatic) Decompensated LV Stage D: Severe disease (symptomatic) O bs e r v e O b s e r v e??? I ntervene I n t e r v e n e Guidelines Assist in Decision-Making Calcified/Thickened leaflets Reduced Systolic Opening Asymptomatic Vmax 5 m/s + low AVR risk Vmax 4 m/s EF <50% EF 50% Undergoing other CV Surgery ETT BP / ex capacity Rapid progression + low AVR risk AVR (IIa) AVR (I) AVR (I) AVR (IIa) AVR (IIb) 20


21 Low Gradient Aortic Stenosis Peak Velocity 2.74 m/sec Mean Gradient 15 mmhg Calculated AVA 0.5 cm 2 Low Output Low Gradient AS Low Ejection Fraction AVA of 0.5 cm 2, but MG of 15mmHg? WHY? Because low SV (low flow) leads to low gradients Real AS 1 o Prob: Severe obstruction to flow 2 o Prob: Depressed LVEF Improves Pseudo-AS 1 o Prob: Depressed LVEF 2 o Prob: Mild/Mod obstruction is made to look severe by SV with AVR 21
22 Low Output Low Gradient AS Dobutamine Stress Testing Increase LV contractility -> Increase Stroke Volume Increase Stroke Volume by 20% -> Real AS Peak vel/mean gradient significantly AVA stays unchanged or slightly Pseudo AS Peak vel/mean gradient minimal AVA What if LV contractility / SV don t increase? Low Gradient - Normal EF EF 50%, AVA <1 cm 2, mean grad <40mmHg Whah???... Still a stroke volume problem!! SVindex 35 ml/m 2 despite EF Typical patient: Older, h/o hypertension, women Concentric LVH, small cavity, impaired filling Markedly increased vascular impedance Pibarot P, Dumesnil JG. Heart (2010) 96:

 AVR (IIa) AVR (IIa) Rule")
23 Guidelines Assist in Decision-Making Suspected Low Flow AS Symptoms No Symptoms V max 4 m/s V max <4 m/s EF <50% EF 50% AVR NOT Indicated DSE MG 40mmHg or Pk Vel 4 m/s AVA index 0.6 cm 2 /m 2 and SV index <35 ml/m 2 AVR (I) AVR (IIa) AVR (IIa) Rule Out other causes for Sx!! Thank You! 23
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Affecting the elderly Requiring new approaches. Echocardiographic Evaluation of Hemodynamic Severity. Increasing prevalence Mostly degenerative
 Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Workshop Facing the challenge of TAVI 2016
 Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
Workshop Facing the challenge of TAVI 2016 Congrès annuel de la SSC Lausanne 15 Juin 2016 Pitfalls in the severity assessment of aortic stenosis by echocardiography Hajo Müller, unité d échocardiographie,
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
G. AORTIC STENOSIS (AS)
") G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Normal TTE/TEE Examinations
 Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Assessment of LV systolic function
 Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Different Variants Amr E Abbas, MD, FACC, FSCAI, FASE, FSVM Director, Interventional Cardiology Research Beaumont Health Associate Professor of Medicine, OU/WB School of Medicine ASCeXAM/ReASCeXAM 2018
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons
 Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Early Surgery in Asymptomatic Severe Aortic Stenosis Pros and Cons Duk-Hyun Kang, M.D. Division of Cardiology Asan Medical Center Seoul, Korea Background Dilemma of balancing the risks versus benefits
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
TAVR TTE INTERROGATION BY ALAN MATTHEWS
 TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
Imaging Guide Echocardiography
 Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Martin G. Keane, MD, FASE Temple University School of Medicine
 Martin G. Keane, MD, FASE Temple University School of Medicine Measurement of end-diastolic LV internal diameter (LVIDd) made by properly-oriented M-Mode techniques in the Parasternal Long Axis View (PLAX):
Martin G. Keane, MD, FASE Temple University School of Medicine Measurement of end-diastolic LV internal diameter (LVIDd) made by properly-oriented M-Mode techniques in the Parasternal Long Axis View (PLAX):
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
Low gradient severe aortic stenosis with preserved left ventricular ejection fraction
 Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD
 Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
Evaluation of Left Ventricular Function and Hypertrophy Gerard P. Aurigemma MD Board Review Course 2017 43 year old health assistant Severe resistant HTN LT BSA 2 Height 64 1 Here is the M mode echocardiogram
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Vevo 2100 System Cardio Measurements. Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc.
 Vevo 2100 System Cardio Measurements Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc. dfuchs@visualsonics.com Instructions This document is a guideline on how to assess cardiac function in rodents imaged
Vevo 2100 System Cardio Measurements Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc. dfuchs@visualsonics.com Instructions This document is a guideline on how to assess cardiac function in rodents imaged
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
NEW GUIDELINES PAGE 9
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Stenosis, Including Recommendations for Echocardiography in Relation to Transcatheter Aortic Valve Implantation From the British Society
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Stenosis, Including Recommendations for Echocardiography in Relation to Transcatheter Aortic Valve Implantation From the British Society
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona
, FASE Mayo Clinic, Arizona") Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Right Ventricle Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona 1. In which scenario will applying the simplified Bernoulli equation to the peak tricuspid regurgitation velocity and adding
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Ref 1. Ref 2. Ref 3. Ref 4. See graph
 Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Aortic Stenosis.
 Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Aortic Stenosis www.cardiconcept.com Common causes Normal Rheumatic (Rim or Commissures) Calcific Degenerative Bicuspid Adapted from C. Otto, Principles of Echocardiography, 2007 Rare causes Congenital
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment
 Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Aortic Valve Stenosis: When stress TTE and/or TEE is required to make the diagnosis and guide treatment Stefanos Karagiannis MD PhD Cardiologist Director Echocardiology Dpt Athens Medical Center ESC 2017
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ;
 Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Ελληνική Καρδιολογική Εταιρεία Σεμινάρια ομάδων εργασίας Θεσσαλονίκη, 8-10 Φεβρουαρίου 2018 Ομάδα εργασίας Ηχωκαρδιολογίας Δυναμική υπερηχοκαρδιογραφία στις μυοκαρδιοπάθειες : έχει θέση και ποια ; ΑΓΑΘΗ-ΡΟΖΑ
Aortic valve Stenosis: Insights in the evaluation of LV function. Erwan DONAL Cardiologie CHU Rennes
 Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Aortic valve Stenosis: Insights in the evaluation of LV function Erwan DONAL Cardiologie CHU Rennes erwan.donal@chu-rennes.fr Preload Afterload Myocardial Fiber Shortening Circumferential Longitudinal
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading