Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med
|
|
|
- Brittney Lambert
- 6 years ago
- Views:
Transcription


1 Stuart Beldner, MD, FHRS Assistant Professor NSLIJ Hofstra School of Med
2 None

3 There s no reason to panic. While it is true that one of the crew members is ill, slightly.
4
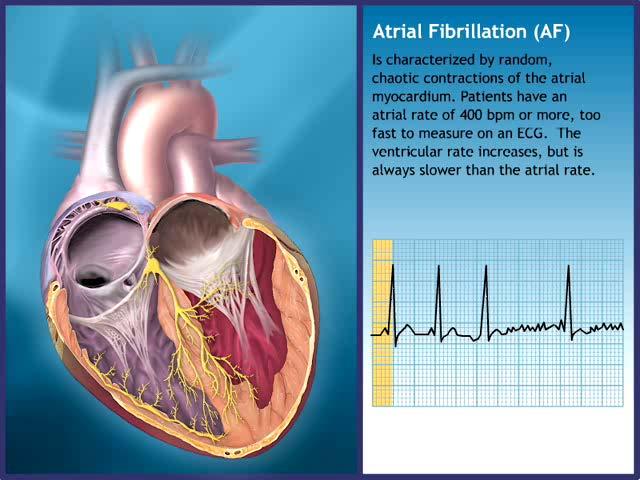
5 Absence of discrete P waves Chaotic atrial activity Ventricular rate irregularity

6 Mechanisms of AF. AF indicates atrial fibrillation; Ca++, ionized calcium; and RAAS, reninangiotensin-aldosterone system. January C T et al. Circulation. 2014;130:e199-e267 Copyright American Heart Association, Inc. All rights reserved.
7 Term Paroxysmal AF Definition AF that terminates spontaneously or with intervention within 7 d of onset. Episodes may recur with variable frequency. Persistent AF Continuous AF that is sustained >7 d. Longstanding persistent AF Permanent AF Nonvalvular AF Continuous AF >12 mo in duration. The term permanent AF is used when the patient and clinician make a joint decision to stop further attempts to restore and/or maintain sinus rhythm. Acceptance of AF represents a therapeutic attitude on the part of the patient and clinician rather than an inherent pathophysiological attribute of AF. Acceptance of AF may change as symptoms, efficacy of therapeutic interventions, and patient and clinician preferences evolve. AF in the absence of rheumatic mitral stenosis, a mechanical or bioprosthetic heart valve, or mitral valve repair.
8
9
10 Rate versus Rhythm Trials Trial Year n PIAF Primary End Point Improvement AF symptoms HR (Rate vs Rhythm Control) P AFFIRM Overall mortality RACE Composite STAF Composite HOT CAFE Composite 1.98 >0.71 AF-CHF Cardiovascular mortality PABA- CHF Composite Multiple <0.001
11 Trials such as AFFIRM and RACE, did NOT prove that rate-controlled and anticoagulated AF is as good as NSR. They show that a rhythm control strategy using an ITT analysis, suggests equivalence in at least some populations. These trials do NOT disprove that sinus rhythm would be better than AF in regard to QOL if one were to actually attain and maintain it with a safe and effective therapy.
12 Patients in Sinus Rhythm, % Rate Arm Rhythm Arm R 2 Mo 4 Mo 1 Yr 2 Yr 3 Yr 4 Yr 5 Yr Time The AFFIRM Investigators. NEJM: 2002; 347:
13 5 fold increase in risk for stroke * AF strokes are usually more severe than nonaf strokes 3 fold risk of heart failure ** 2 fold risk of dementia *** and mortality * *Kannel et al. Am J of Coll **Wang et al. Circu *** Ott et al. Stroke 1997.
14 Time dependant, on treatment, Multivariate Analysis of Survival HR (99%) 1.06 ( ) 1.56 ( ) 1.57 ( ) 1.56 ( ) 1.78 ( ) 1.70 ( ) 0.74 ( ) 1.36 ( ) 0.50 ( ) 1.42 ( ) 0.53 ( ) 1.49 ( ) Factor Age (per year) CAD CHF Diabetes Smoking Stroke/TIA Normal LVEF Mitral Regurg Warfarin Digoxin Sinus Rhythm AA drug Better Worse
15 Singh BN, et al, NEJM 2005; 352: SF-36 Change in One Year Physical Fx General Health Social Fx Vitality NSR AF HR Rest Exercise Duration HR Peak
16 Class I: Class IC: propafenone (also very weak β-blocker), flecainide (no β-blockade effects) Sustained-release propafenone (Rythmol SR) and flecainide are bid; Propafenone appears to be less proarrhythmic Class IA: disopyramide, quinidine, procainamide No longer included in the ACC/AHA/ESC algorithm Disopyramide may be useful in vagally induced AF Class III: Sotalol (class III plus β-blocker) Dofetilide (pure class III) Amiodarone (class III plus class I, II, IV); highly overused Dronedarone (similar to amiodarone with different pharmacokinetics and markedly reduced organ toxic potential)
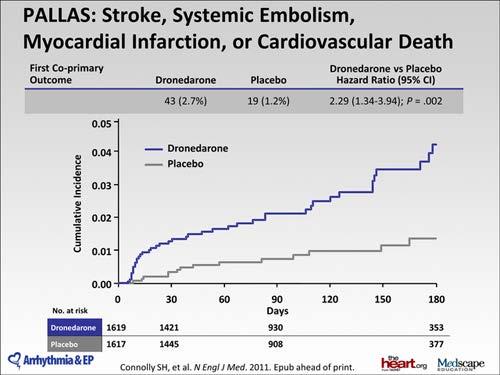
17 Trial Study Design Dronedarone Effects ERATO Dronedarone vs placebo Significant decrease in ventricular rates (24-hr Holter and maximal exercise) DAFNE Dronedarone vs placebo Efficacy vs placebo in time to first AF recurrence with 400 mg bid dose EURIDIS and ADONIS ANDROMEDA DIONYSOS ATHENA PALLAS Dronedarone vs placebo in 1237 patients with AF/AFL Dronedarone vs placebo in 627 patients with severe HF Dronedarone vs amiodarone in 504 patients with persistent AF Dronedarone vs placebo in 4628 high-risk AF patients Dronedarone vs placebo in 3236 patient with permanent AF Significant and consistent reduction in first recurrence of AF/AFL; comparable safety vs placebo Excess mortality risk vs placebo (n=25 vs n=12; HR, 2.13; P=.03); trial stopped early Mixed observations Efficacy against AF Reduction in CV mortality and hospitalization Reduction in additional end points a 2.29-fold increase in the coprimary end point of stroke, MI, embolism, or cardiovascular death events, compared to placebo, and led to a halt in a planned 10,800-patient international randomized trial
18 Results show dronedarone significantly prolongs the time to AF recurrence compared with placebo No significant difference was found between placebo and dronedarone in all-cause mortality Dronedarone reduced CV mortality, CV hospitalizations, ACS, arrhythmic deaths, and stroke Adverse events occurring significantly more frequently with dronedarone than with placebo included bradycardia, QTinterval prolongation, diarrhea, nausea, rash, and an increase in the serum creatinine level Total discontinuation rates for dronedarone and placebo were identical, no pulmonary or thyroid toxicity was evident, and there were no TDP/VF deaths in the high-risk AF population in dronedarone-treated patients Hohnloser SH, et al. N Engl J Med. 2009;360(7):
19
20 Efficacy of Antiarrhythmic Drug Therapy for A Fib Gold Standard for Judging Ablative Therapy % Patients Free of Symptomatic AF 100 Arm Overestimate AF control 80 with drug (No Sxs) Increased Mortality? (The prevalence of sinus rhythm in the rhythmcontrol group at follow-up was 82.4 percent, 73.3 percent, and 62.6 percent at one, three, and RATE VS RHYTHM CONTROL 60 AFFIRM * Roy et al NEJM, 2000 **Antman et al, JACC 1990 ***Crijns et al, AJC 1991 #Natale et al JACC 2001 AFFIRM TRIAL Rhythm Control five years, respectively.) Propafenone** Months Amiodarone* Sotalol** Hx of Two Failed Drugs*** # Atrial Flutter
21 Ranalozine (Ranexa) Has a greater effect on the late sodium current (late > peak) which should make it more effective in ischemic patients. Vernakalat Ikur Blocker
22 Approved for the treatment of chronic stable angina An atrially effective compound, substantially inhibiting peak Na + current mainly in the atria and has been shown to decrease the incidence of atrial fibrillation in an in vitro model. MERLIN TIMI 36 1 (Metabolic Efficiency with Ranolazine for Less Ischemia in Non-ST Elevation Acute Coronary Syndromes) 6,560 patients with prior chronic angina A neutral effect on overall mortality Suggested (P= 0.08) a 26% reduction in new onset atrial fibrillation. The incidence of significant arrhythmias was screened with holter monitoring P= (2.3%) 55 (1.7%) Placebo Ranolazine JACC 2009;53:1510-6

23 Burashnikov A et al. JACC 2010
24 A Phase 2, Proof of Concept, Randomized, Placebo- Controlled, Parallel Group Study to Evaluate the Effect of Ranolazine and Dronedarone When Given Alone and in Combination on Atrial Fibrillation Burden in Subjects With Paroxysmal Atrial Fibrillation Primary endpoint The effect of ranolazine and of low dose dronedarone when given alone and in combination at different dose levels on atrial fibrillation burden (AFB) over 12 weeks of treatment the combination of ranolazine (Ranexa, Gilead Sciences) and dronedarone (Multaq, Sanofi) appeared to lower the burden of atrial fibrillation (AF) by >70% over three months in 45% to 60% of patients with the paroxysmal form of the arrhythmia Kowey et al. Presented at HRS 2014
25 A 59-year-old woman is referred to you for management of permanent atrial fibrillation that she has had for three years. The referring physician reports that recently performed echocardiography revealed normal findings. The patient's current medications are dabigatran and metoprolol, 50 mg daily. During your initial evaluation, the patient says she feels well and has no symptoms. A 12-lead electrocardiogram shows a resting heart rate of 100 beats per minute (bpm). (A) Continue the current drug regimen and schedule follow-up evaluation (B) Increase metoprolol dosage and obtain a 24-hour ambulatory electrocardiographic recording; adjust metoprolol dosage to achieve a heart rate of less than 70 bpm during rest and less than 120 bpm during moderate exercise (C) Increase metoprolol dosage and obtain a 24-hour ambulatory electrocardiographic recording; adjust metoprolol dosage to achieve a heart rate of less than 80 bpm during rest and less than 110 bpm during moderate exercise (D) Increase metoprolol dosage and obtain a 24-hour ambulatory electrocardiographic recording; adjust metoprolol dosage to achieve a heart rate of less than 80 bpm during rest and less than 130 bpm during moderate exercise
26 2006 guidelines for AF recommended target heart rates of 60 to 80 bpm at rest and 90 to 115 bpm during moderate exercise AFFIRM no higher than 80 bpm at rest and no higher than 110 bpm during a 6-minute walk test, and an average heart rate no higher than 100 bpm over 18+ hours of Holter monitoring with no rates >100% of maximal age-predicted heart rate, as well RACE Resting heart rate < 100 bpm
![Trial design: Patients with permanent AF were randomized to lenient (resting heart rate [HR] <110 bpm) or strict rate control (resting HR <80 bpm). Patient follow-up was 3 years. % 3 0 2 0 (p = 0.](/docs-images/72/67504621/images/27-2.jpg "001)* 12.9 14.9 % 30 2 0 (p = NS) Results Primary outcome was similar in lenient and strict control arms (12.9% vs. 14.9%) Stroke with lenient control (1.6% vs. 3.9%, p< 0.05) CHF (3.8% vs. 4.")
27 Trial design: Patients with permanent AF were randomized to lenient (resting heart rate [HR] <110 bpm) or strict rate control (resting HR <80 bpm). Patient follow-up was 3 years. % (p = 0.001)* % (p = NS) Results Primary outcome was similar in lenient and strict control arms (12.9% vs. 14.9%) Stroke with lenient control (1.6% vs. 3.9%, p< 0.05) CHF (3.8% vs. 4.1%), CV death, PPM implantation (0.8% vs. 1.4%) were similar Conclusions Primary endpoint Lenient control (n = 311) * For noninferiority CV mortality Strict control (n = 303) Lenient rate control easier to achieve than strict control, and noninferior for clinical outcomes Most patients had lower CHADS 2 score. Safety and efficacy in patients with higher CHADS 2 score will need to be explored Needs to be tested in patients with significant LV dysfunction Van Gelder IC, et al. N Engl J Med 2010;Mar 15:[Epub]
 2.8 (2.0-3.8) 4.0 (3.1 5.1) 8.5 (6.3-11.1) 12.5 (8.2-17.5) 18.2 (10.5-27.")
28 CHADS 2 Risk Criteria Score Prior stroke or TIA 2 Age > 75 1 Hypertension 1 Diabetes Mellitus 1 Heart Failure 1 Patients Adjusted Stroke Risk CHADS 2 Score ( ) 2.8 ( ) 4.0 ( ) 8.5 ( ) 12.5 ( ) 18.2 (
29 CHA 2 DS 2 -VASc Risk Factor Score C ongestive heart failure/lv dysfunction 1 H ypertension 1 A ge > 75 y 2 D iabetes mellitus 1 S troke/tia/te 2 V ascular disease 1 A ge y 1 S ex category (ie female gender) 1

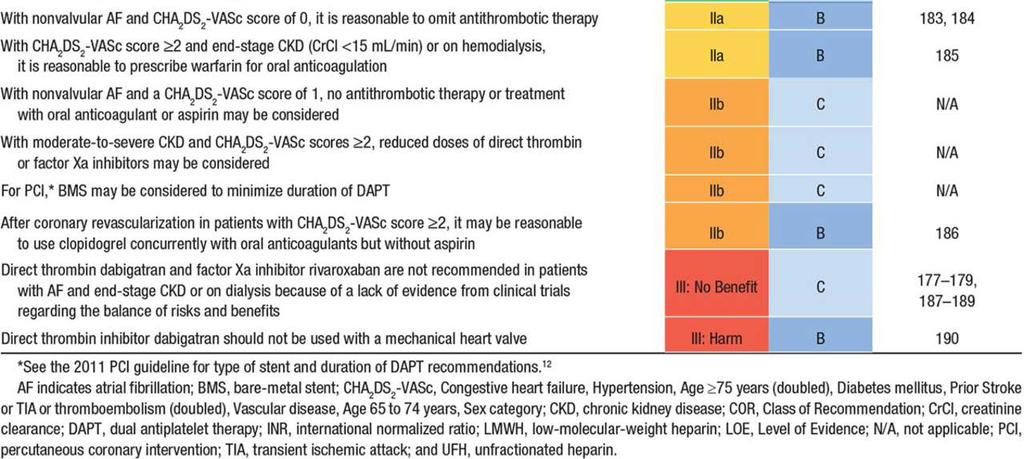
30 Summary of Recommendations for Risk-Based Antithrombotic Therapy. January C T et al. Circulation. 2014;130:e199-e267 Copyright American Heart Association, Inc. All rights reserved.
31
32 Primary Endpoint stroke or systemic embolism INR D150 VKA (RELY) Rivaroxaban VKA (ROCKET AF) Apixaban VKA (ARISTOLE) Quartlie % 1.7% (HR= 0.61) (HR= 0.48) (HR= 0.73) % 2.2% (HR- 0.48) (HR= 0.61) (HR=0.94) % 1.4% (HR= 0.76) (HR= 0.66) (HR= 0.64) % 1.4% (HR= 0.88) (HR= 0.58) (HR= 0.88) Major bleeding INR D150 VKA (RELY) Rivaroxaban* VKA (ROCKET AF)* Apixaban VKA (ARISTOLE) Quartlie % 3.3% (HR= 0.74) (HR= 0.80) (HR= 0.5) % 3.9% (HR= 0.84) (HR= 0.81) (HR= 0.64) % 3.2% (HR= 1.12) (HR= 1.03) (HR= 0.85) % 3% (HR= 1.08) (HR= 1.25) (HR=0.75) * Event rate (100 pt years)
33 There is evidence from meta-analyses of RCTs that home monitoring of VKA therapy reduces thromboembolic events by 42% compared with usual monitoring. THIS IS SIMILAR TO THE 33% relative risk reduction with dabigatran 150 mg Bid!!!
34 Dose adjusted VKA therapy + ASA is not recommended in stable coronary artery disease SPORTIF Associated with a nearly 2 fold increase in bleeding with NO significant reduction in stroke or MI. RE-LY Major bleeding was twice as high in patients on aspirin AND either dabigatran or wafarin
35 No increase in death Nonfatal stroke CHADS 2 = 0 2 fewer strokes/1000 CHADS 2 = 1 6 fewer strokes/1000 CHADS 2 = 2 11 fewer strokes/1000 CHADS 2 = fewer strokes/1000 Nonfatal MI 21 fewer/1000 Nonfatal Major Extracranial Bleed 26 more bleeds/1000 (RR= 2.37) CHEST February 2012
36 WOEST Primary Endpoint: Total number of TIMI bleeding events Cumulative incidence of bleeding 50 % 40 % 30 % 20 % Triple therapy group Double therapy group 44.9% 19.5% 10 % 0 % p<0.001 HR= %CI[ ] Days n at risk:
37 WOEST Secondary Endpoint (Death, MI,TVR, Stroke, ST) 20 % Triple therapy group Double therapy group 17.7% Cumulative incidence 15 % 10 % 11.3% 5 % 0 % p=0.025 HR= %CI[ ] Days n at risk:
38 The primary purpose of this study is to evaluate the safety for 2 different rivaroxaban treatment strategies and one Vitamin K Antagonist (VKA) treatment strategy utilizing various combinations of dual antiplatelet therapy (DAPT) or low-dose aspirin (ASA) or clopidogrel (or prasugrel or ticagrelor).
39 Thank you
Are Drugs Better? Dr Mauro Lencioni. Drugs or ablation as first line treatment for AF? Consultant Cardiologist & Electrophysiologist
 Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
Are Drugs Better? Drugs or ablation as first line treatment for AF? Dr Mauro Lencioni Consultant Cardiologist & Electrophysiologist The Philosophical Issue What do we mean by Better? Outcome measures Measurement
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Saudi Heart Association February 22, 2011
 Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Atrial Fibrillation and the NOAC s. John Raymond MS, PA-C, MHP February 10, 2018
 Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Atrial Fibrillation and the NOAC s John Raymond MS, PA-C, MHP February 10, 2018 Pathogenesis EPIDEMIOLOGY Arrhythmia-related hospitalisations in the US Ventricular fibrillation 2% Atrial fibrillation 34%
Out with the old, in with The 2010 Atrial Fibrillation Guidelines
 Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Out with the old, in with The 2010 Atrial Fibrillation Guidelines Kseniya Chernushkin B.Sc.(Pharm.), VCH/PHC Pharmacy Resident Mary Elliot B.Sc.(Pharm.), VCH/PHC Pharmacy Resident March 22, 2011 Outline
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Half Moon Bay Treatment of Atrial Fibrillation. Dr. Roger A. Winkle MD. Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital
 Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Half Moon Bay 2018 Treatment of Atrial Fibrillation Dr. Roger A. Winkle MD Silicon Valley Cardiology, PAMF, Sutter Health Sequoia Hospital Disclosures: Investor Farapulse Things a Primary Care Doctor Should
Dronedarone: Need to Perform a CV Outcome Safety Study
 Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Dronedarone: Need to Perform a CV Outcome Safety Study Gerald V. Naccarelli M.D. Consultant: Glaxo-Smith-Kline, Pfizer, Sanofi, Boehringer-Ingelheim, Daiichi-Sankyo, Bristol Myers Squibb, Otsuka, Janssen
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Atrial Fibrillation. Ivan Anderson, MD RIHVH Cardiology
 Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
Atrial Fibrillation Ivan Anderson, MD RIHVH Cardiology Outline Definition and Pathophysiology Rate versus rhythm control Rate control thresholds (how much is enough) Anti-coagulation CHADS2VASc score HASBLED
» A new drug s trial
 » A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
» A new drug s trial A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause
ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ. ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C
 ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C Definitions of AF: A Simplified Scheme Term Definition Paroxysmal AF AF that terminates
ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΦΑΡΜΑΚΕΥΤΙΚΗ ΗΛΕΚΤΡΙΚΗ ΑΝΑΤΑΞΗ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ Καρδιολόγος, Ε/Α, Γ.Ν.Κατερίνης. F.E.S.C Definitions of AF: A Simplified Scheme Term Definition Paroxysmal AF AF that terminates
Update in the Management of Atrial Fibrillation
 Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Update in the Management of Atrial Fibrillation Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research: Gilead, Medtronic,
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
What s New in the AF Guidelines
 Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Impact on New AF Guidelines on Heart Failure Management Gothenburg - May 22 nd 2011 Europace (2010) 12, 1360-420 http://europace.oxfordjournals.org JACC (2011) 57, 223-42 http://www.cardiosource.org What
Polypharmacy - arrhythmic risks in patients with heart failure
 Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Influencing sudden cardiac death by pharmacotherapy Polypharmacy - arrhythmic risks in patients with heart failure Professor Dan Atar Head, Dept. of Cardiology Oslo University Hospital Ullevål Norway 27.8.2012
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Samer Nasr, M.D. Mount Lebanon Hospital.
 Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Samer Nasr, M.D. Mount Lebanon Hospital. Lone atrial fibrillation: Younger than 60 years old. No clinical or echo evidence of cardiopulmonary disease. Favorable prognosis. Thromboembolism usually not
Dronedarone For Atrial Fibrillation: Unbridled Enthusiasm Or Just Another Small Step Forward?
 Dronedarone For Atrial Fibrillation: Unbridled Enthusiasm Or Just Another Small Step Forward? James A. Reiffel, M.D. Introduction In July 2009, the federal Food and Drug Administration (FDA) approved the
Dronedarone For Atrial Fibrillation: Unbridled Enthusiasm Or Just Another Small Step Forward? James A. Reiffel, M.D. Introduction In July 2009, the federal Food and Drug Administration (FDA) approved the
Atrial Fibrillation and Common Supraventricular Tachycardias. Sunil Kapur MD
 Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Atrial Fibrillation 2009
 Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Atrial Fibrillation 2009 Michael Glikson, MD Director of Pacing & Electrophysiology Leviev Heart Center Sheba medical Center Sheba Medical Center Tel Hashomer The Leviev Heart Center Rhythm vs rate control
Management of atrial fibrillation a holistic view - Prof. Dr. Martin Borggrefe Mannheim
 a holistic view - Prof. Dr. Martin Borggrefe Mannheim Patients with atrial fibrillation (millions) 16 14 12 10 8 6 4 2 0 Management of atrial fibrillation Expected prevalence of apparent AF 5,1 5,1 5,9
a holistic view - Prof. Dr. Martin Borggrefe Mannheim Patients with atrial fibrillation (millions) 16 14 12 10 8 6 4 2 0 Management of atrial fibrillation Expected prevalence of apparent AF 5,1 5,1 5,9
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital
 Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Use of Antiarrhythmic Drugs for AF Who, What and How? Dr. Marc Cheng Queen Elizabeth Hospital Content i. Rhythm versus Rate control ii. Anti-arrhythmic for Rhythm Control iii. Anti-arrhythmic for Rate
Practical Rate and Rhythm Management of Atrial Fibrillation
 Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Practical Rate and Rhythm Management of Atrial Fibrillation pocket guide UPDATED FEBRUARY 2013 Adapted from the ACCF/AHA/HRS 2011 Focused Updates Incorporated into the ACC/AHA/ESC Guidelines for the Management
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
dronedarone, 400mg, film-coated tablets (Multaq ) SMC No. (636/10) Sanofi-aventis Ltd
 SMC No. (636/10) Sanofi-aventis Ltd") dronedarone, 400mg, film-coated tablets (Multaq ) SMC No. (636/10) Sanofi-aventis Ltd 6 August 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
dronedarone, 400mg, film-coated tablets (Multaq ) SMC No. (636/10) Sanofi-aventis Ltd 6 August 2010 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
Fred Kusumoto Professor of Medicine
 Fred Kusumoto Professor of Medicine Faculty photo will be placed here Kusumoto.Fred@mayo.edu 2015 MFMER 3543652-1 Atrial Fibrillation Presentation Subtitle Here Mayo School of Continuous Professional Development
Fred Kusumoto Professor of Medicine Faculty photo will be placed here Kusumoto.Fred@mayo.edu 2015 MFMER 3543652-1 Atrial Fibrillation Presentation Subtitle Here Mayo School of Continuous Professional Development
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Fibs and Flutters: The Heart of the Matter
 Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Invasive and Medical Treatments for Atrial Fibrillation. Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic
 Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
Invasive and Medical Treatments for Thomas J Dresing, MD Section of Electrophysiology and Pacing Cleveland Clinic Disclosures Fellow s advisory panel for St Jude Medical Speaking honoraria from: Boston
National Horizon Scanning Centre. Dronedarone (Multaq) for atrial fibrillation and atrial flutter. December 2007
 for atrial fibrillation and atrial flutter. December 2007") Dronedarone (Multaq) for atrial fibrillation and atrial flutter December 2007 This technology summary is based on information available at the time of research and a limited literature search. It is not
Dronedarone (Multaq) for atrial fibrillation and atrial flutter December 2007 This technology summary is based on information available at the time of research and a limited literature search. It is not
Primary Care Update in Medicine January 31 February 1, 2013 New Management Options for Patients with Atrial Fibrillation
 Primary Care Update in Medicine January 31 February 1, 2013 New Management Options for Patients with Atrial Fibrillation Anne B. Curtis, MD, FACC, FHRS, FACP, FAHA Charles and Mary Bauer Professor, Chair,
Primary Care Update in Medicine January 31 February 1, 2013 New Management Options for Patients with Atrial Fibrillation Anne B. Curtis, MD, FACC, FHRS, FACP, FAHA Charles and Mary Bauer Professor, Chair,
AF#in#pa(ents#with#CAD# Is#dronedarone#a#good#choice?!
 AF#in#pa(ents#with#CAD# Is#dronedarone#a#good#choice?! DRUG#PROPHYLAXIS#OF#AF:# FOCUS#ON#DRONEDARONE# Friday#16C10C2015# Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research
AF#in#pa(ents#with#CAD# Is#dronedarone#a#good#choice?! DRUG#PROPHYLAXIS#OF#AF:# FOCUS#ON#DRONEDARONE# Friday#16C10C2015# Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research
Treatment strategy decision tree
 strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
strategy decision tree strategy decision tree Confirmed diagnosis of AF Further investigations and clinical assessment including risk stratification for stroke/thromboembolism Paroxysmal AF Persistent
ATHENA - A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular
 1 ATHENA - A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patients
1 ATHENA - A placebo-controlled, double-blind, parallel arm Trial to assess the efficacy of dronedarone 400 mg bid for the prevention of cardiovascular Hospitalization or death from any cause in patients
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Objectives for Technicians. Objectives for Pharmacists. Pathophysiology. Conflict of Interest. Atrial Fibrillation
 Warfar IN or Warfar-OUT? And Other Updates in the Management of Atrial Fibrillation Kimberly Ackerbauer, PharmD, BCPS Clinical Pharmacy Specialist Rush University Medical Center Conflict of Interest I
Warfar IN or Warfar-OUT? And Other Updates in the Management of Atrial Fibrillation Kimberly Ackerbauer, PharmD, BCPS Clinical Pharmacy Specialist Rush University Medical Center Conflict of Interest I
Relevant Advances in Atrial Fibrillation
 Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisco Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Antiarrhythmic Drug
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Dronedarone in the Post-Pallas Era. Jorge E. Schliamser, MD Carmel Medical Center Haifa
 Dronedarone in the Post-Pallas Era Jorge E. Schliamser, MD Carmel Medical Center Haifa Disclosures None Dronedarone is a multichannel blocker Dronedarone possesses electrophysiologic characteristics of
Dronedarone in the Post-Pallas Era Jorge E. Schliamser, MD Carmel Medical Center Haifa Disclosures None Dronedarone is a multichannel blocker Dronedarone possesses electrophysiologic characteristics of
Debate PRO. Dronedarone is an important drug in the management of paroxysmal atrial fibrillation. John Camm
 ESC ICM - Internationales Congress Center München 2012 Atrial Fibrillation Controversies in Medical Treatment Debate Dronedarone is an important drug in the management of paroxysmal atrial fibrillation
ESC ICM - Internationales Congress Center München 2012 Atrial Fibrillation Controversies in Medical Treatment Debate Dronedarone is an important drug in the management of paroxysmal atrial fibrillation
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Defining Sub-Clinical Atrial Fibrillation and its management
 Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Defining Sub-Clinical Atrial Fibrillation and its management Jeff Healey MD, MSc, FRCP, FHRS PHRI Chair in Cardiology Research Population Health Research Institute McMaster University, Canada Sub-Clinical
Atrial fibrillation workshop: rate- versus rhythm-control
 Atrial fibrillation workshop: rate- versus rhythm-control Rocky Mountain Internal Medicine Conference Nov, 2011 Dr F. Russell Quinn Cardiac Electrophysiologist, Foothills Medical Centre, Calgary Disclosures
Atrial fibrillation workshop: rate- versus rhythm-control Rocky Mountain Internal Medicine Conference Nov, 2011 Dr F. Russell Quinn Cardiac Electrophysiologist, Foothills Medical Centre, Calgary Disclosures
Antiarrhythmic agents in 2014
 7 AP-HRS Scientific Session, New Dehli, India - Oct 29 to Nov 1, 2014 Antiarrhythmic agents in 2014 Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation - Venice, Italy
7 AP-HRS Scientific Session, New Dehli, India - Oct 29 to Nov 1, 2014 Antiarrhythmic agents in 2014 Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation - Venice, Italy
Rate Control versus Rhythm Control in NSTEMI
 Rate Control versus Rhythm Control in NSTEMI Gulmira Kudaiberdieva, MD, FESC Adana, Turkey Conflict of interest: None to declare Istanbul - 2012 OUTLINE Significance of AF in ACS Prognostic value of AF
Rate Control versus Rhythm Control in NSTEMI Gulmira Kudaiberdieva, MD, FESC Adana, Turkey Conflict of interest: None to declare Istanbul - 2012 OUTLINE Significance of AF in ACS Prognostic value of AF
Atrial Fibrillation Ablation in Patients with Heart Failure
 Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Update on Dronedarone and Cardiovascular Outcomes
 Update on and Cardiovascular Outcomes Dr. Stuart Connolly MD McMaster University Hamilton Ontario Disclosure: Research grants, speaker fees and consulting honoraria from sanofi aventis has key structural
Update on and Cardiovascular Outcomes Dr. Stuart Connolly MD McMaster University Hamilton Ontario Disclosure: Research grants, speaker fees and consulting honoraria from sanofi aventis has key structural
UC SF. Division of General Internal Medicine UNIVERSITY OF CALIFORNIA SAN FRANCISCO, DIVISION OF HOSPITAL MEDICINE
 Updates in the Management of Atrial Fibrillation Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic UC SF Division of
Updates in the Management of Atrial Fibrillation Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic UC SF Division of
Hypertension and Atrial Fibrillation in 2017
 Boma Inn, Eldoret, 24th 25thFebruary 2017 Hypertension and Atrial Fibrillation in 2017 Dr Mzee Ngunga Consultant Cardiologist Aga Khan University Hospital, Nairobi Objectives 1. Understand the relationship
Boma Inn, Eldoret, 24th 25thFebruary 2017 Hypertension and Atrial Fibrillation in 2017 Dr Mzee Ngunga Consultant Cardiologist Aga Khan University Hospital, Nairobi Objectives 1. Understand the relationship
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Newer Anti-Anginal Agents and Anticoagulants
 Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017
 MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017 1 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart
MANAGING ATRIAL FIBRILLATION: BEYOND ANTICOAGULATION December 9, 2017 1 Faculty Disclosure Faculty: Peter Leong-Sit MSc, MD, FRCPC, FHRS Associate Professor, Western University Cardiologist, London Heart
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Subclinical AF: Implications of device based episodes
 Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
Subclinical AF: Implications of device based episodes Michael R Gold, MD, PhD Medical University of South Carolina Charleston, SC Disclosures: Clinical Trials and Consulting: Medtronic, Boston Scientific
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Dronedarone for the treatment of non-permanent atrial fibrillation
 Dronedarone for the treatment of non-permanent atrial Issued: August 2010 last modified: December 2012 guidance.nice.org.uk/ta197 NICE has accredited the process used by the Centre for Health Technology
Dronedarone for the treatment of non-permanent atrial Issued: August 2010 last modified: December 2012 guidance.nice.org.uk/ta197 NICE has accredited the process used by the Centre for Health Technology
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely
 Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
ESC Stockholm Arrhythmias & pacing
 ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
ESC Stockholm 2010 Take Home Messages for Practitioners Arrhythmias & pacing Prof. Panos E. Vardas Professor of Cardiology Heraklion University Hospital Crete, Greece Disclosures Small teaching fees from
5/5/2010. World incidence 720, 000 new cases / year. World prevalence 5.55 million AF prevalence increasing with aging of population
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Atrial fibrillation and advanced age
 Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial fibrillation and advanced age Prof. Fiorenzo Gaita Director of the Cardiology School University of Turin, Italy Prevalence of AF in the general population Prevalence and age distribution in patients
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
Innovations in AF Management
 Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Innovations in AF Management Barry Boilson MD PhD FRCPI boilson.barry@mayo.edu Disclosures Relevant None financial relationship(s) with industry None Off Label Usage None Overview Mechanisms of AF AF as
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation
 Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Ablation Should Not Be Used as Primary Therapy for Treatment of Patients with Atrial Fibrillation 25 October 2008 Update in Electrocardiography and Arrhythmias Zian H. Tseng, M.D., M.A.S. Assistant Professor
Recent observations have focused attention on the PVs as a source of ectopic activity i determining i AF
 Atrial Fibrillation in 2010 Panos Vardas Professor of Cardiology President of EHRA Atrial Fibrillation Pathophysiology of AF Triggers Recent observations have focused attention on the PVs as a source of
Atrial Fibrillation in 2010 Panos Vardas Professor of Cardiology President of EHRA Atrial Fibrillation Pathophysiology of AF Triggers Recent observations have focused attention on the PVs as a source of
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT
 AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
Conflicts of Interests
 Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
Advances in the Management of Atrial Fibrillation State of the Art in 2013 Overview of AF Stroke risk and anticoagulation Rate control Antiarrhythmic Drug Therapy Catheter ablation Conclusion Hugh Calkins
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham
 New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
New Guidelines for SPAF Professor DA Fitzmaurice Primary Care Clinical Sciences University of Birmingham Stroke prevention and atrial fibrillation Epidemiology of atrial fibrillation How common is it?
DECLARATION OF CONFLICT OF INTEREST. Consultant Sanofi Biosense Webster Honorarium Boehringer Ingelheim St Jude Medical
 DECLARATION OF CONFLICT OF INTEREST Consultant Sanofi Biosense Webster Honorarium Boehringer Ingelheim St Jude Medical ESC Congress Paris, France August 27-31, 2011 Risk & Complications of AADs for Rhythm
DECLARATION OF CONFLICT OF INTEREST Consultant Sanofi Biosense Webster Honorarium Boehringer Ingelheim St Jude Medical ESC Congress Paris, France August 27-31, 2011 Risk & Complications of AADs for Rhythm
Engage AF-TIMI 48. Edoxaban in AF: What can we expect? Cardiology Update John Camm. St. George s University of London United Kingdom
 Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Dronedarone( What%is%the%future?!
 Dronedarone( What%is%the%future?! DRUG(PROPHYLAXIS(OF(AF:( FOCUS(ON(DRONEDARONE( Friday(16>10>2015( Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research grants, consulting
Dronedarone( What%is%the%future?! DRUG(PROPHYLAXIS(OF(AF:( FOCUS(ON(DRONEDARONE( Friday(16>10>2015( Harry%JGM%Crijns% Maastricht,%The%Netherlands% Disclosures Harry Crijns - research grants, consulting
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
ΑΣΥΜΠΤΩΜΑΤΙΚΗ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ
 ΑΣΥΜΠΤΩΜΑΤΙΚΗ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΓΕΩΡΓΙΟΣ ΣΤΑΥΡΟΠΟΥΛΟΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΠΓΝΘ ΙΠΠΟΚΡΑΤΕΙΟ 9 Ο Βορειοελλα ATRIAL FIBRILATION Atrial fibrillation (AF) is the most common clinically significant heart
ΑΣΥΜΠΤΩΜΑΤΙΚΗ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ ΓΕΩΡΓΙΟΣ ΣΤΑΥΡΟΠΟΥΛΟΣ Β ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΠΓΝΘ ΙΠΠΟΚΡΑΤΕΙΟ 9 Ο Βορειοελλα ATRIAL FIBRILATION Atrial fibrillation (AF) is the most common clinically significant heart
Management of Atrial Fibrillation in the Hospitalized Patient
 Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
Management of Atrial Fibrillation in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisco Disclosures Research:
ESC. Update of the ESC Guidelines on Medical Therapy. John Camm. ICM Internationales Congress Center München
 ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
ESC 2012 ICM Internationales Congress Center München Update on Consensus Statements on Management of Atrial Fibrillation European Heart Rhythm Association Update of the ESC Guidelines on Medical Therapy
Atrial Fibrillation Ablation in Patients with Heart Failure
 Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
Atrial Fibrillation Ablation in Patients with Heart Failure Eleftherios M. Kallergis, MD, PhD, FESC Cardiology Department, Heraklion University Hospital Since auricular fibrillation so often complicates
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Atrial Fibrillation Etiologies and Treatment. Shawn Liu Learner Centered Learning Goal
 Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
Atrial Fibrillation Etiologies and Treatment Shawn Liu Learner Centered Learning Goal Pathophysiology Defined by the absence of coordinated atrial systole Results from multiple reentrant electrical waves
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Atrial Fibrillation: Beyond the AFFIRM trial
 Atrial Fibrillation: Beyond the AFFIRM trial Daniel J. Cantillon MD FACC FHRS Cardiac Electrophysiology and Pacing Assistant Professor, Lerner College of Medicine Cleveland Clinic, Heart & Vascular Institute
Atrial Fibrillation: Beyond the AFFIRM trial Daniel J. Cantillon MD FACC FHRS Cardiac Electrophysiology and Pacing Assistant Professor, Lerner College of Medicine Cleveland Clinic, Heart & Vascular Institute
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination