ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
|
|
|
- Elmer Sherman
- 6 years ago
- Views:
Transcription
1 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
2 Outline Definition of ARDS Epidemiology of ARDS Pathophysiology of ARDS Ventilator management strategies Low tidal volume ventilation Permissive hypercapnia Open lung ventilation Recruitment maneuvers Prone ventilation High frequency ventilation Non ventilatory and novel therapies
3 Introduction Condition first described in 1960s Described by military clinicians in Vietnam as shock lung Simultaneously described as adult respiratory distress syndrome Terminology changed when it was discovered that persons of any age could be affected acute respiratory distress syndrome
4 Definitions Acute onset of bilateral pulmonary infiltrates consistent with pulmonary edema Without evidence of elevated left atrial pressure PCWP 18 mmhg ALI (acute lung injury) and ARDS are differentiated by degree of hypoxemia ALI P/F ratio of 201 to 300 mmhg ARDS P/F ratio of 200 mmhg
5 P/F Ratio PaO2 requires ABG analysis to determine Can be difficult to obtain in some patients SpO2 is a reasonable substitute (Rice, 2007) SpO2/FiO2 235 predicted P/F 200 SpO2/FiO2 315 predicted P/F 300 ALI/ARDS is an arbitrary definition
6 Oxyhemoglobin Dissociation Curve
7 Epidemiology Incidence (Rubenfeld, 2012) ALI 86 per 100k person years ARDS 64 per 100k person years Increases dramatically with patient age 16/100k person years (15 19y/o) 306/100k person years (75 84y/o) Approximately 190,000 cases of ALI in the U.S each year
8 Epidemiology 10 15% of ICU patients meet criteria for ALI or ARDS 20% of those mechanically ventilated Incidence appears to be decreasing (Li, 2010) Decline in hospital acquired ARDS Those with ARDS tend to be much sicker than they used to be
9 Epidemiology Previously had a mortality rate greater than 50% (Ashbaugh, 1967) Mortality decreased to 29 38% during the 1990s Mortality appears to be continuing to decline, now approaching 25% A minority of patients with ARDS die exclusively from respiratory failure Most patients succumb to secondary complications or their primary illness

10 Pathophysiology ARDS is characterized by accumulation of fluid and protienaceous debris in the alveoli and interstitium of the lung Normal lung function requires dry, patent alveoli to be closely approximated to perfused capillaries
11 Pathophysiology Fluid crosses pulmonary capillary membranes under control of hydrostatic and oncotic forces Serum protein remains intravascular Small quantities of fluid are normally allowed into the interstitium Three mechanisms normally prevent alveolar edema Retained intravascular protein Interstitial lymphatic return Capillary epithelial tight junctions
12 Pathophysiology ALI/ARDS are consequences of alveolar injury leading to diffuse alveolar damage Lung injury leads to release of pro inflammatory cytokines Neutrophils are recruited to the lungs Toxic mediators are released damaging capillary and alveolar endothelium Protein escapes from the vascular space Fluid overwhelms lymphatics and fills air spaces Alveolar collapse ensues
13 Consequences of Injury Impairment of gas exchange V/Q mismatching Shunting leads to hypoxemia Increased dead space impairs CO 2 elimination Decreased lung compliance Stiffness of nonaerated lung Smaller tidal volumes can lead to markedly elevated airway pressures Pulmonary hypertension
14 Three Stages of ARDS Exudative stage Diffuse alveolar damage Proliferative stage Resolution of pulmonary edema Proliferation of type II pneumocytes Squamous metaplasia Interstitial infiltration Collagen deposition Fibrotic stage Obliteration of lung architecture Cyst formation Fibrosis
15 Etiologies Many different potential etiologies More than 60 possible causes have been identified Sepsis Most common cause of ALI/ARDS Concurrent alcoholism markedly increases risk 70% vs. 30% Aspiration ALI/ARDS develops in approximately 33% of hospitalized patients with witnessed aspiration
16 Etiologies Pneumonia CAP is most common cause of out of hospital development of ALI/ARDS 1 Nosocomial pneumonia well recognized to progress to ALI/ARDS Severe trauma Bilateral lung contusion Fat embolism following long bone fractures Delayed onset 12 to 48 hours following trauma Many patients predisposed to sepsis Trauma related ALI/ARDS carries more favorable prognosis than ALI/ARDS from other causes 2 1. Baumann WR. Incidence and mortality of adult respiratory distress syndrome: a prospective analysis from a large metropolitan hospital. Crit Care Med 1986;14(1): Calfee CS, Eisner MD, Ware LB, et al. Trauma associated lung injury differs clinically and biologically from acute lung injury due to other clinical disorders. Crit Care Med 2007;35(10):
17 Etiologies Massive transfusion >15 units of PRBC is a risk factor for the development of ALI/ARDS 1 Selection bias? TRALI Development within 6 hours of transfusion Lung and HSCT Primary graft failure in lung transplant recipients Poor preservation of donor organ DAH, engraftment syndrome, infections in HSCT recipients 1. Hudson LD. Clinical risks for development of the acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine 1995;151(2):
18 Etiologies Overdose and toxicity (Reed, et al.) Aspirin, cocaine, opioids, phenothiazines, tricyclic antidepressants Protamine, nitrofurantoin, systemic chemotherapy (at therapeutic dosages)
19 Initial Course Pulmonary abnormalities develop within 48 to 72 hours following the inciting event Rapid worsening of clinical status common ABG generally indicates respiratory alkalosis, hypoxemia Hypoxemia due to physiologic shunting

20 ARDS Initial CXR
21 Subsequent Course Following the initial acute phase of disease, patients may take one of two courses: Improvement in ventilatory requirements accompanied by radiographic improvement Entrance into the organizing/fibrotic phase of ARDS with persistent ventilator dependence and radiographic abnormality
22 Complications ALI/ARDS is associated with many complications generally seen in states of critical illness Complications specific to ALI/ARDS Barotrauma Sedation/paralysis
23 Barotrauma A result of pulmonary parenchymal tissue breakdown and a generally uniform need for positive pressure ventilation Incidence appears to be 13% among patients using low tidal volume ventilation strategies Highest levels of barotrauma found among patients receiving high PEEP Mean airway pressure, plateau pressure, and driving pressure did not predict barotrauma 1. Eisner M, Thompson B, Schoenfeld D, Anzueto A, Matthay M, Network TARDS. Airway Pressures and Early Barotrauma in Patients with Acute Lung Injury and Acute Respiratory Distress Syndrome. AJRCCM 2002;165(7):
24 Consequences of Sedation and Paralysis Prolonged depression of mental status Persistent neuromuscular weakness Critical illness myopathy Most prominent when neuromuscular blocking agents are used in conjunction with corticosteroids
25 Ventilatory Strategies Low Tidal Volume Ventilation Permissive hypercapnia Open lung ventilation Recruitment maneuvers Prone ventilation High frequency ventilation
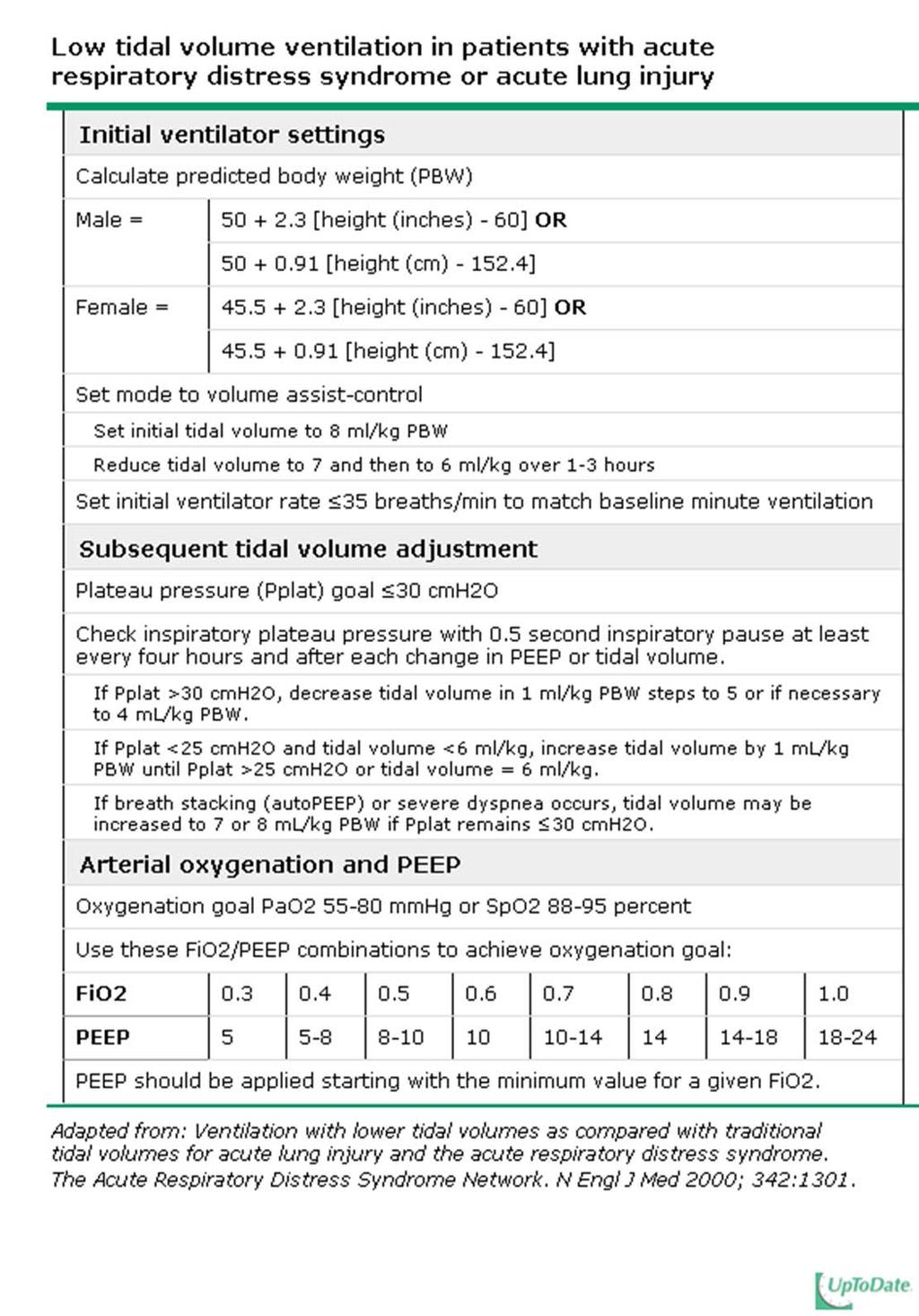
26 Low Tidal Volume Ventilation
27 Low Tidal Volume Ventilation Randomized 861 patients with ALI/ARDS to traditional ventilation versus lower tidal volume ventilation Traditional ventilation: initial V t 12 ml/kg; plateau pressure 50 cm H 2 O Lower tidal volume ventilation: initial V t 6 ml/kg; plateau pressure 30 cm H 2 O Study aborted because mortality was significantly lower in the lower tidal volume group (31.0% vs. 39.8%) Number of days without ventilator increased in lowertidal volume group (12 vs. 10)
28 Low Tidal Volume Ventilation Preponderance of quality evidence has shown LTVV improves mortality and other outcomes in ARDS Reduction in mortality and increases in ventilator free days
29 Potential Harm of LTVV Was not associated with any clinically important adverse outcomes in the ARMA trial Auto PEEP Higher respiratory rates are required for LTVV to maintain the same minute ventilation May lead to hemodynamic instability Sedation WOB and ventilator asynchrony may increase with LTVV Initial need for increased sedation when ventilation initiated, but does not appear to persist Post hoc analysis of ARMA trial did not find any differences in sedation duration among patient groups
30 Breath Stacking Can occur despite sedation Causes episodic delivery of higher V t which may undermine benefits of LTVV Can be ameliorated by delivering slightly higher V t P plat should remain 30 cm H 2 O
31 Breath Stacking 1. J. Pediatr. (Rio J.) vol.83 no.2 suppl.0 Porto Alegre May 2007
32
33 Application of LTVV A threshold P plat below which safety is certain is not known Goal of 30 is derived from ARMA trial Plateau pressure should be kept as low as possible Oxygenation goal PaO 2 between mmhg SpO 2 between 88 95%
34 Permissive Hypercapnia The understanding that protective lung ventilation strategies will occasionally limit alveolar ventilation Low tidal volume ventilation will sometimes lead to hypercapnia, which has been shown to be generally well tolerated in trials Safe for most patients Some patients exist in whom permissive hypercapnia may be harmful
35 Contraindications to Permissive Hypercapnia Cerebral disease Mass lesions, trauma, cerebral edema Seizure disorder Hypercapnia is associated with cerebral vasodilitation Increases cerebral blood flow May cause increased ICP and potentially reduce CPP May lower seizure threshold Associated with intraventricular hemorrhage in neonates 1. Feihl F. Permissive hypercapnia. How permissive should we be? American Journal of Respiratory and Critical Care Medicine 1994;150(6):
36 Hypercapnia may be Harmful Patients with significant heart disease Increased sympathetic tone Patients taking beta blockers Negative inotropic effects Hypovolemia Systemic vasodilation Leads to hypotension
37 Open Lung Ventilation Combines low tidal volume ventilation with higher PEEP Maximizes alveolar recruitment Low tidal volume ventilation mitigates alveolar overdistention Elevated PEEP seeks to minimize cyclic atalectasis
38 Open Lung Ventilation Has been shown to provide survival benefit in two trials Trials have severe methodologic limitations Unclear if survival benefits translate into real practice at this point May require permissive hypercapnia

39
40 Amato, et al. 53 patients randomized Conventional ventilation Lowest possible PEEP with V t 12 ml/kg Protective ventilation PEEP above the lower inflection point on a static pressure volume curve V t of <6 ml/kg Driving pressure <20 cm above PEEP value Preferential use of pressure limited ventilatory modes
41 Amato, et al. Protective strategy improved survival at 28 days Higher rate of weaning from mechanical ventilation Lower rate of barotrauma among patients with ARDS Not associated with a higher rate of survival to hospital discharge
42 Application of Open Lung Ventilation No universally accepted protocol Applied PEEP is set at least 2 cm above the lower inflection point of the pressure volume curve 16 cm PEEP is generally used if the lower inflection point is uncertain
43 High PEEP Ventilation Type of open lung ventilation that does not require a pressure volume curve Less need for neuromuscular blockade Applied PEEP should open collapsed alveoli Decreases alveolar overdistention Each breath is more evenly spread over the lung Cyclic atelectasis is reduced

44 High PEEP Ventilation 1. Briel, M., Meade, M., Mercat, A., Brower, R. G., Talmor, D., Walter, S. D., Slutsky, A. S., et al. (2010). Higher vs Lower Positive End Expiratory Pressure in Patients With Acute Lung Injury and Acute Respiratory Distress Syndrome: Systematic Review and Meta analysis. JAMA: The Journal of the American Medical Association, 303(9), doi: /jama
45 Briel, et al. Meta analysis of 2299 patients in 3 trials All patients received LTVV Treatment with higher vs lower levels of PEEP was not associated with improved hospital survival among all comers Among the subgroup of patients with ARDS, higher levels of PEEP were associated with improved survival
46 Recruitment Maneuvers Brief application of high level of CPAP (35 40cmH2O) for 40 seconds Clinical impact is uncertain Meta analysis found recruitment maneuvers do not affect mortality, LOS, barotrauma Improve oxygenation Complications can include hypotension and transient desaturation
47 Prone Ventilation Mechanical ventilation taking place with the patient lying the prone position Improves oxygenation in many patients with ARDS Uncertain clinical benefits
48 Physiologic Effects Optimization of V/Q matching How prone positioning may improve ventilation: Improves differences between dorsal and ventral pleural pressures More homogenous lung recruitment Unloads the weight of the heart which normally compresses lung beneath it in the supine position Displaces diaphragm, decreasing posterior caudal compression of the lung
49 Physiologic Effects How prone ventilation may improve perfusion: V/Q matching is improved when prone as blood flow is relocated to ventilated portions of lung More aerated lung is perfused as a percentage of total overall blood flow through the lung Shunting is minimized No evidence to suggest real clinical benefit
50 Clinical Outcomes of Prone Ventilation Increases arterial PaO2 in most patients with ARDS (uncontrolled trials) Predictors of sustained response Improved oxygenation during a brief trial Diffuse pulmonary edema and dependent atalectasis Extrapulmonary causes of ARDS Elevated intra abdominal pressure
51 Mortality Benefit of Prone Ventilation Prone ventilation does not confer a mortality benefit (randomized trials/meta analyses) Exception may be made for those patients with the greatest severity of illness Two trials demonstrated mortality benefits among severely hypoxemic patients P/F ratio < 100 Meta analysis demonstrated 53% vs 63% mortality reduction among 555 patients 1. Sud S, Friedrich JO, Taccone P, et al. Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia: systematic review and meta analysis. Intensive Care Medicine 2010;36(4):
52 In the End Prone ventilation is warranted in select patients (most critically ill) Prone ventilation should not be used as routine management in all patients with ARDS Duration of effective prone ventilation is unknown No good data to justify its use Best reserved as a rescue therapy
53 High Frequency Ventilation Provides tidal volumes below that of anatomic dead space at frequencies of greater than 60 breaths/minute May decrease VILI and reduce barotrauma in patients with ARDS May improve V/Q matching and reduce risk of hemodynamic compromise
54 Potential Complications of HFV Desiccation of mucus Airway damage due to high gas velocities Air trapping High shear forces Between areas of lung with different impedances
55 HFV in Practice Poor data to support routine use in patients with ALI/ARDS May improve oxygenation compared to conventional ventilation, but benefits are not sustained over time Should be reserved as salvage therapy for patients failing conventional ventilation Significant expertise and resources are necessary to safely and effectively perform HFV
56 Types of HFV High frequency jet ventilation (HFJV) High frequency oscillatory ventilation (HFOV) High frequency percussive ventilation (HFPV) High frequency positive pressure ventilation (HFPPV)
57 Novel Therapies Surfactant No evidence to support routine use More study is needed in formulation and delivery systems Inhaled vasodilators (NO, prostacyclin) Have not been shown to reduce morbidity or mortality in patients with ARDS Liquid ventilation May cause undue harm in ARDS patients Cannot be recommended for use in ARDS at this time ECMO Poor base of evidence to support use Resource intensive Antiinflammatory agents
58 In Conclusion ARDS is reasonably common, but the incidence is declining Complications related to ARDS are generally related to concurrent critical illness, although barotrauma is common a significant iatrogenic complication Low tidal volume ventilation has been consistently shown to improve morbidity and mortality in ARDS The use of high levels of PEEP is probably beneficial Other ventilatory strategies are best used as salvage therapy for severely hypoxemic individuals A number of novel nonventilatory therapies are being studied in ARDS but are not yet proven to provide benefit
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015
: Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015") Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
Pediatric Acute Respiratory Distress Syndrome (PARDS): Do we have consensus? Doug Willson, MD Children s Hospital of Richmond at VCU April 20, 2015 Conflicts to Disclose! I am a consultant for Discovery
3/5/14. Disclosures. Background. None. No discussion of non FDA approved products
 Disclosures None No discussion of non FDA approved products Background Who are the patients at risk for severe hypoxemic respiratory failure? ú Acute Lung Injury (ALI) PaO 2 /FIO 2 300 ú Acute Respiratory
Disclosures None No discussion of non FDA approved products Background Who are the patients at risk for severe hypoxemic respiratory failure? ú Acute Lung Injury (ALI) PaO 2 /FIO 2 300 ú Acute Respiratory
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Ventilation in ARDS. 13 February C Evans CONTENTS. Definition Introduction Diagnostic Criteria for ARDS Pathogenesis...
 13 February 2009 CONTENTS Ventilation in ARDS Definition... 3 Introduction... 3 Diagnostic Criteria for ARDS... 4 C Evans Commentator: G Allopi Moderator: NT Brouckaert Pathogenesis... 4 Risk Factors...
13 February 2009 CONTENTS Ventilation in ARDS Definition... 3 Introduction... 3 Diagnostic Criteria for ARDS... 4 C Evans Commentator: G Allopi Moderator: NT Brouckaert Pathogenesis... 4 Risk Factors...
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
INTRODUCTION. Acute respiratory distress syndrome (ARDS) is a common complication of critical illness
 is a common complication of critical illness") Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Breanna Keller NDFS 356 Acute Respiratory Distress Syndrome INTRODUCTION Acute respiratory distress syndrome (ARDS) is a common complication of critical illness and results in the sudden failure of the
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS
 Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Non- conventional forms of respiratory support
 Non- conventional forms of respiratory support Dr Liesel Bosenberg Specialist Physician & Fellow in Critical Care Medicine Kalafong & Steve Biko Academic Hospitals Points we will ponder: ECMO Liquid Ventilation
Non- conventional forms of respiratory support Dr Liesel Bosenberg Specialist Physician & Fellow in Critical Care Medicine Kalafong & Steve Biko Academic Hospitals Points we will ponder: ECMO Liquid Ventilation
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management
:Evidence Based Management") Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management John C. Klick, M.D., F.C.C.P. Assistant Professor Department of Anesthesiology and Perioperative Medicine University Hospitals Case
Acute Respiratory Distress Syndrome (ARDS):Evidence Based Management John C. Klick, M.D., F.C.C.P. Assistant Professor Department of Anesthesiology and Perioperative Medicine University Hospitals Case
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Introduction Definition Etiology Epidemiology Lung injury prediction score. Pathophysiology Diagnosis Clinical presentation Management Conclusion
 Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
Fluid restriction is superior in acute lung injury and ARDS
 TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
Asthma Management in ICU. by DrGary Au From KWH
 Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Asthma Management in ICU by DrGary Au From KWH Overview of Asthma Pathophysiology Therapeutic options Medical treatment NPPV Mechanical ventilation Salvage therapy ~ 235 million people worldwide were affected
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation
 https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio: