Antibody Mediated Rejection in Heart Transplantation
|
|
|
- Hugo Kelley
- 6 years ago
- Views:
Transcription
1 Antibody Mediated Rejection in Heart Transplantation 2012 Teresa De Marco, MD, FACC Professor of Medicine & Surgery Director Heart Failure and Pulmonary Hypertension Program Medical Director, Heart Transplantation The image cannot be displayed. Your computer may not have enough memory to open the image, or the image may have been corrupted. Restart your computer, and then open the file
2 Disclosures I will discuss off label use and/or investigational use of the following drugs in my presentation: Rituximab, Bortezomib, Everolimus I have no relevant relationships to disclose

3 Rejection

4 CARDIAC TRANSPLANTATION Rejection 0.5 to 1 episode per patient in year one
 % experiencing rejection within 1 year 60 Cyclosporine + MMF, Treatment Cyclosporine + MMF, No Treatment Tacrolimus + MMF, Treatment Tacrolimus + MMF, No Treatment 50 40 30 20 10 0 Overall")

5 PERCENTAGE OF ADULT HEART TRANSPLANT RECIPIENTS EXPERIENCING REJECTION BETWEEN TRANSPLANT DISCHARGE AND 1-YEAR FOLLOW-UP Stratified by Maintenance Immunosuppression (Follow-ups: July 1, June 30, 2008) % experiencing rejection within 1 year 60 Cyclosporine + MMF, Treatment Cyclosporine + MMF, No Treatment Tacrolimus + MMF, Treatment Tacrolimus + MMF, No Treatment Overall Overall: p < : p < : p < Female: p = Male: p < Female Male Cyclosporine + MMF: N = 2,360 Tacrolimus + MMF: N = 3,065 NOTE: There were 149 patients with cyclosporine+aza and 41 with tacrolimus+aza. These groups were excluded due to small numbers. ISHLT 2009 Analysis is limited to patients who were alive at the time of the follow-up Treated rejection = Recipient was reported to (1) have at least one acute rejection episode that was treated with an antirejection agent; or (2) have been hospitalized for rejection. No rejection = Recipient had (i) no acute rejection episodes and (ii) was reported either as not hospitalized for rejection or did not receive anti-rejection agents.


6 Types of Rejection Hyperacute rejection Preformed alloantibodies vs. HLA class 1 antigens Acute rejection Most common Cell mediated Antibody mediated - rare <10% Chronic rejection Slow progressive loss of graft function Occurs months to years post-transplantation
7 Basic Transplant Immunology Two forms of acute rejection Cellular rejection (CR) CD4 and CD8 T cells target donor human leukocyte antigens (HLA) à cytotoxic T cells à cell damage Antibody-mediated rejection (AMR) B cells activate à plasma cells à antibodies against HLA* à complement-dependent cytotoxicity

8 HC I, II Antigens Corticosteroids Cyclosporin, tacrolimus Antigen Macrophage presenting cell AZA, MMF Daclizumab Cyclosporin,tacrolimus Plasma Cells

9 Antithymocyte/antilymphocyte Antithymocity globulin OKT3 globulin monoclonal antibody



10 Clinical signs of allograft rejection None/asymptomatic/subclinical (surveillance RV bx and DSA monitoring) Non-specific Fever Elevated central venous pressure New S3 gallop New dysrrhythmias Unexpected relative hypotension Abnormal ventricular function Cardiogenic shock
 5% 5")


11 Right Ventricular Endomyocardial Biopsy 3 specimen: False (-) 5% 5 specimen: False (-) 3% Complications Mortality: 0.05% Cardiac perforation: % PTX: 1% Thromboembolism, air embolism, arrhythmia, BBB





12 Grades of Acute Cellular Rejection ISHLT { { Grade 0 No rejection 1A 1B Nomenclature Focal (perivascular or interstitial) infiltrate without necrosis Diffuse but sparse infiltrate without necrosis 2 One focus with aggressive infiltration and/or focal myocyte damage 3A 3B Multifocal aggressive infiltrates and/or myocyte damage Diffuse inflammatory process with necrosis 4 Diffuse aggressive polymorphous infiltrate + edema, + hemorrhage, + vasculitis, with necrosis 1= mild cellular rejection; 2 = moderate CR; 3 = severe CR






13 Grade 2R = MODERATE CR RX! IV steroid pulse or oral prednisone pulse - multifocal/diffuse lymphocytic infiltrate with myocyte necrosis
14 Challenges of Antibody-Mediated Rejection Diagnosis Are symptoms required? Clinical versus pathological? Prevention How do we identify patients at high risk for AMR? Can high-risk patients be treated prior to transplant? Treatment How should AMR be treated? If the initial therapy fails, what next?
 Hemodynamic compromise common 47% of all cases 68% of early cases Michaels PJ et al.")
15 Clinical Characteristics of Antibody-Mediated Rejection 44 patients with AMR More often female 52% female (compared with 26% overall transplant population) Hemodynamic compromise common 47% of all cases 68% of early cases Michaels PJ et al. Heart Lung Transplant 2003; 22: 58-69
16 Older Diagnostic Criteria: Antibody-Mediated Rejection Histologic evidence of acute capillary injury : A and B required A. Endothelial swelling or denudation B. Macrophages in capillaries C. Neutrophils in capillaries D. Interstitial edema, congestion, or hemorrhage Immunopathologic evidence for antibody action A. Ig (G,M, and/or A) + C3d and / or C4d or C1q B. Fibrin in vessels (optional) Serologic evidence of donor-specific anti-hla Ab Cardiac dysfunction required ACUTE CELLULAR REJECTION - Grade 1 R, mild: Interstitial and/or perivascular infiltrate with up to 1 focus of myocyte injury. ANTIBODY-MEDIATED REJECTION (AMR/ HUMORAL REJECTION) - AMR 1: Positive for antibodymediated rejection " Edema grade (0-3) 1+ Hemorrhage grade (0-3) 1+ Capillary swelling (0-3) 2+ GENERAL IMMUNOHISTOCHEMISTRY REPORT C4d Positive CD20 Negative CD3 Negative CD31 Positive, highlights dilated vessels CD68 Positive, highlights numerous intracapillary macrophages " Takemoto et al. Am J Transplant 2004;4:
 22 symptomatic (EF 40%) (TxAMR) 9 hemodynamic compromise Endothelial cell injury!")
17 Asymptomatic/Subclinical AMR: Increased risk of Cardiac Allograft Vasculopathy (CAV) transplants 43 with AMR 86 controls matched for age, sex, time from tx 21 asymptomatic and untreated (AsAMR) 22 symptomatic (EF 40%) (TxAMR) 9 hemodynamic compromise Endothelial cell injury! Wu et al, J Heart and Lung Transplant 2009; 28:417-22
18 Asymptomatic/Subclinical AMR: Increases Mortality transplants Excluded patients with hemodynamic compromise rejection Predominant pattern of rejection in first 3m post transplant 118 AMR ( 3 AMR episodes) All asymptomatic and untreated 490 CR (< 3 AMR episodes) All treated 193 mixed ( 3 mixed episodes) All treated Mortality over 7 yr avg f/u: CR: 12 % MR: 18 % AMR: 21 % Kfoury et al, J Heart and Lung Transplant 2009; 28:781-4
19 Asymptomatic AMR: Lessons Learned Asymptomatic AMR if untreated: Increased incidence of CAV compared to patients with no AMR and patients with treated, symptomatic AMR Increased mortality compared to patients with treated cellular or mixed rejection Conclusion The diagnosis of AMR should be pathological, not clinical Asymptomatic AMR should be treated
20 New Diagnostic Criteria: AMR Histology Endothelial activation : intravascular macrophages, capillary destruction Edema/hemorrhage less specific; not required Immunopathology Immunofluorescence: C3d, C4d, HLA deposition Immunoperoxidase: C4d, CD68 deposition IMMUNOFLUORESCENCE RESULTS: IgG: 1+ interstitial IgM: Negative IgA: Negative C'3: Negative C1q: Negative *HLA-Dr: 1+ vascular C4D: 3+ vascular C3D: Negative Fibrinogen: 1+ interstitial IMMUNOPEROXIDASE RESULTS: CD68: Stromal macrophages present CD31: Vascular endothelial cells highlighted C4D: Diffuse capillary staining C3D: Diffuse capillary staining RESULTS SUMMARY: X Immunologic positive Histology positive Findings of severe rejection ANTIBODY-MEDIATED REJECTION CLASSIFICATION: AMR 0: None. Negative immunologic stain(s) and negative histology. X AMR 1: Suspicious. Positive immunologic stain(s) or histology (but not both). AMR 2: Definite. Positive immunologic stain(s) and positive histology. AMR 3: Severe. Positive immunologic stain(s) and positive histology with hemorrhage, edema, neutrophils, vasculitis. Kobashigawa et al, J Heart and Lung Transplant 2011;30(3):
21 pamr 0: both histological and immunopathological studies are negative pamr 1(H+):suspicious for pathologic AMR histopathological alone pamr 1 (I+): suspicious for pathologic AMR immunopathological alone pamr 2: both histological and immunopathological pamr 3: Diagnostic Criteria: Antibody Mediated Rejection New pathologic diagnostic criteria studies are positive severe AMR; interstitial hemorrahge, capillary fragmentation, mixed inflammatory infiltrates, endothelial cell pyknosis, and /or karyorrhexis, marked edema Serologic evidence of donor specific anti-hla Ab and non-hla antibodies Berry, G et al. J Heart Lung Transplant ( 6):601-11






22 Antibody-Mediated Rejection H & E A I m m u n o p e C r o x i d a s e E Intravascular cells; no lymphocytes B CD68 CD3 Prominent macrophages Rare T lymphocytes D C4d CD34 EC;Intravascuar macrophages F Complement in capillaries Courtesy Michelle Kittleston from Wu, G et al J Heart Lung Transpl 2009;28:417-22



23 EC swelling; Macrophages C4D stain Surrounds EC Gonzales-Stawinski GV et al J Heart Lung Transplant 2008;27:375-61


24 C4D labeling with cardiac dysfunction Focal C4D labeling without cardiac dysfunction Positive DSA MFI = 8,000 Bruneval, P ISHLT Newsletter
25 Recommended Frequency for Routine Monitoring Endomyocardial Biopsy Histologic evaluation of every protocol biopsy for AMR Immunoperoxidase/immunofluorescent staining (C4d): Post-transplant: 2 weeks and 1, 3, 6, 12 months, and AMR suspected Interval testing for C4d AMR suspected on histologic, serologic, or clinical findings Routine C4d staining on subsequent biopsy specimens after a positive result until clearance Kobashigawa et al, J Heart and Lung Transplant 2011;30(3):
26 Recommended Frequency for Routine Monitoring Circulating Antibody Use of solid-phase assay and/or cell-based assays to: Assess for DSA (& quantification if Ab present) Post-transplant: 2 weeks and 1, 3, 6, 12 months, and annually, and AMR clinically suspected Kobashigawa et al, J Heart and Lung Transplant 2011;30(3):
27 Challenges of Antibody-Mediated Rejection Diagnosis Are symptoms required? No Clinical versus pathological? Pathological Prevention How do we identify patients at high risk for AMR? Can high-risk patients be treated prior to transplant? Treatment How should AMR be treated? If the initial therapy fails, what next?
28 Antibody-Mediated Rejection: Prevention Targets of the antibody response Human leukocyte antigens (HLA) Endothelial cell antigens Risk factors: sensitization Blood transfusions Pregnancy Previous transplant VAD Goal: identify sensitized patients Anti-HLA Ab aka Panel Reactive Antibodies (PRA) Non-HLA Ab (experimental)
29 Assessing Panel Reactive Antibodies: Screening for the Presence of Antibodies Screening Low Risk: PRA < 10% Moderate Risk: PRA 10-25% High Risk: PRA > 25% Specification Identification of anti-hla Ab Quantification Are they cytotoxic? Survival % Nwakanma LU Annals Thoracic Surg :
30 Antibody Detection Methods Membrane-Based Peripheral Leukocytes or Cell Lines Solid Phase ELISA Complement Dependent Cytotoxicity (CDC) Lacks sensitivity for all HLAs Cannot detect HLA Class II reliably Cannot distinguish IgM from IgG Fluorescent Bead Assays Luminex Flow PRA Specification of single HLA Class I and II IgG Ab - Quantification of HLA Ab (indication of cytotoxicity) - Rapid turn-around time

31 Assessing Panel Reactive Antibodies: Identification by Fluorescent Bead Assays Screening Low = PRA < 10% Moderate = PRA 10-25% High = PRA > 25% Specification Identification of anti-hla Ab Quantification Are they cytotoxic? Laser Freq Fluorescence







")
32 Assessing Panel Reactive Antibodies: Quantification by Fluorescent Bead Assays Screening Low = PRA < 10% Moderate = PRA 10-25% High = PRA > 25% Specification Identity of anti-hla Ab Quantification Are they cytotoxic? Mean Fluorescent Intensity (MFI) Weak < 5,000 Moderate 5,000-10,000 Strong (Cytotoxic) > 10,000
33 What matters clinically: Calculated PRA How easy will it be to find a donor for my patient awaiting transplant? cpra defines the frequency of the unacceptable HLA in the donor population Step 1: Define unacceptable HLA Potentially cytotoxic : MFI > 5000 Patient has anti-hla Ab with MFI > 5000 à unacceptable HLA - PANEL REACTIVE ANTIBODY SCREEN - ANTIBODY CLASS II % PRA 75 - ANTIBODY CLASS I % PRA 78 - SINGLE ANTIBODY ID CLASS I - - MFI B78: B51: 6537 B37: B75: 3996 B35: B53: 2748 B76: B52: 2455 A66: A26: 2164 A25: 2125 " - - SINGLE ANTIBODY ID CLASS II - MFI - - DR7: DQ7: DQ9: DQ8: DR12: 4403 DR103: DR53: 3268"

34 What matters clinically: How easy will it be to find a donor for my patient awaiting transplant? cpra defines the frequency of the unacceptable HLA in the donor population Step 2: Determine frequency of those HLA in the population Link on UNOS website Calculated PRA

35 What matters clinically: The Calculated PRA How easy will it be to find a donor for my patient awaiting transplant? cpra defines the frequency of the unacceptable HLA in the donor population Step 3: Assess cpra cpra 10% = 90% of donors would be a match cpra 80% = only 20% of donors would be a match cpra 53% = only 47% donors would be a match
36 Pre-transplant Protocol: Management of Sensitized Patients Check PRA < 10% Recheck Q 6 m 2w post sensitizing event Infection Transfusion Prospective vs Virtual Xmatch > 10% Specification (anti-hla Ab) Quantification (MFI) Calculated PRA Desensitization if cpra > 50% Kobashigawa JA J Heart and Lung Transplant 2009; 28:213-25
37 Desensitization Protocols Adapted from renal transplantation experience Indications Pre-transplant cpra > 50% to prevent AMR Post-transplant Positive Xmatch (induction) Refractory AMR Components Remove preformed Ab: Plasmapheresis Block Ab function: IV IgG B cell destruction: Monoclonal Ab against CD20 on B cells Rituximab Plasma cell destruction: Proteasome inhibitor targeting plasma cells Bortezomib FDA approved for multiple myeloma
 Refractory AMR Vo AA NEJM 2008")
38 Desensitization Protocols Indications Pre-transplant cpra > 50% Post-transplant Positive Xmatch (induction) Refractory AMR Vo AA NEJM :
39 Desensitization Protocol: Managing Refractory Antibodies Some patients have a persistently elevated PRA despite plasmapheresis, IV Ig and rituximab Median fluorescent intensity Drop after 1 st round of PP, IV Ig, ritux Rebound after 2 nd round of IV Ig, ritux 1/4/09 3/3/09 3/26/09 4/22/09 DR7 DQ7 DQ9 B78 B51 Drop after bortezomib
40 Refractory Antibodies: Role of Bortezomib Cedar Sinai experience 6 patients with cpra 50% despite PP/IV Ig/ritux Side effects UTI, pneumonia, catheter infection, C difficile Neuropathy: responded to reduction in dose Outcomes cpra ê from 62% to 35% 5 with fall in cpra and successfully transplanted 1 with no Δ in cpra and died from sepsis after cycle #2 1 died post-oht from sepsis cpra 50% after IV Ig/ritux protocol Days 1, 4, 8, 11 Day 25 Repeat 2-wk cycle if cpra 50% Plasmapheresis Bortezomib 1.3 mg/m 2 Check PRA Patel et al J Heart and Lung Transp 2011; 30:1320
41 Prospective Crossmatch Purpose Avoid donors with HLA to which the recipient has cytotoxic anti- HLA antibodies Prevent hyperacute rejection Process Test recipient serum against donor cells Geographic constraints to limit the donor pool Indications Pre-transplant, if multiple low-level anti-hla Ab (MFI ) Post-transplant surveillance T CELL FLOW CROSSMATCH POSITIVE " T CELL MCS 51 " " T cell MCS Reference range:" Heart : Negative < 50 MCS " B CELL FLOW CROSSMATCH NEGATIVE B CELL MCS 65 " " B cell MCS Reference range: Heart: Negative <121 MCS "
42 Virtual Crossmatch Purpose Avoid donors with HLA for which the recipient has strong anti-hla Ab Prevent hyperacute rejection Advantages Does not require donor cells + recipient serum No geographic constraints Process Step 1: define cytotoxic HLA Ab by MFI threshold (> ) Step 2: avoid donors with these HLA Higher MFI threshold More donor offers Greater chance of rejection Reserved for unstable patients with projected long wait time - PANEL REACTIVE ANTIBODY SCREEN - ANTIBODY CLASS II % PRA 75 - ANTIBODY CLASS I % PRA 78 - SINGLE ANTIGEN ID CLASS I - - MFI B78: B51: 6537 B37: B75: 3996 B35: B53: 2748 B76: B52: 2455 A66: A26: 2164 A25: 2125 " - - SINGLE ANTIGEN ID CLASS II - MFI - DR7: DQ7: DQ9: DQ8: DR12: DR103: DR53: 3268"
 Incompatible (+) Compatible (-) 89 23 12 133 89/112 PPV 79% 133/145 NPV 92% PPV 79% à 21% false-incompatible")

43 Prospective vs Virtual Crossmatch 257 samples from highly sensistized pts Prospective Xmatch Virtual Xmatch Incompatible (+) Compatible (-) Incompatible (+) Compatible (-) /112 PPV 79% 133/145 NPV 92% PPV 79% à 21% false-incompatible rate à yet donor pool is still expanded by lack of geographical constraints NPV 92% à 8% of patients will have incompatible matches à use retrospective Xmatch post transplant to guide therapy Stehlik et al. J Heart and Lung Transplant 2009;28:
44 Prognostic Value of Post-transplant PRA Study Smith JD Transplantation 1992 George JF JHLT 1995 Przybylowski P Transplantation 1999 Tambur AR Transplantation 2000 Ho EK Human Immunology 2009 Post-tx PRA Anti-HLA DSA Anti-HLA DSA Anti-HLA DSA Anti-HLA DSA Anti-HLA DSA Outcome 6-month rejection 1-year survival 1-year rejection (50% vs 16%) 1-year survival (86% vs 92%) 1-year rejection 10-year survival (63% vs 79%)
45 Challenges of Antibody-Mediated Rejection Diagnosis Are symptoms required? Clinical versus pathological? Prevention How do we identify patients at high risk for AMR? Can high-risk patients be treated prior to transplant? Treatment How should AMR be treated? If the initial therapy fails, what next?

46 Mechanisms Underlying Treatment of AMR IV immune globulin Rituximab Plasmapheresis Photopheresis Anti-thymocyte globulin Bortezomib Anti-thymocyte globulin Rituximab Proliferation signal inhibitors Adapted from Singh et al, Transplantation Reviews, 2009;23:34-46
 IV immune globulin IV pulse steroids Cytolytic therapy (ATG) Plasmapheresis (")
47 Treatment of Rejection Asymptomatic/ Subclinical Reduced EF Heart Failure/Shock Cellular Antibody-Mediated Target higher CNI levels Oral steroid bolus + taper Sirolimus To treat or not to treat? Oral steroid bolus/ taper or IV pulse steroids IV pulse steroids or Cytolytic therapy Plasmapheresis (before ATG dose) IV immune globulin IV pulse steroids Cytolytic therapy (ATG) Plasmapheresis ( before ATG dose) IV immune globulin Inotropic therapy IV heparin Inotropes, IABP or ECMO support

 IV immune globulin Inotropic therapy IV")
48 Treatment of Rejection Asymptomatic/ Subclinical Reduced EF Heart Failure/Shock Cellular Target higher CNI levels Oral steroid bolus + taper Sirolimus Oral steroid bolus/ taper or IV pulse steroids IV pulse steroids Cytolytic therapy (ATG) Plasmapheresis (before ATG dose) Antibody-Mediated To treat or not to treat? IV pulse steroids or Cytolytic therapy Plasmapheresis (before ATG dose) IV immune globulin Inotropic therapy IV heparin IABP or ECMO support IV immune globulin
49 After the dust settles... AMR Maintenance Protocol Acute therapy determined by clinical picture MMF à PSI Repeat echo, EMBx, PRAs 1-2w post rx Normal EF/hemos, no DSA, no rejection Persistent low EF, abnormal hemos, or DSA EMBx/echos per protocol PRA q 6m Photopheresis? IV Ig, rituximab, bortezomib











50 Evidence for AMR therapies Study Organ Therapy #pts Results Crespo-Leiro MG Am J Transplant 2005 Heart PP 7-19d 12 pts 11/12 had resolution of AMR Jordan SC Pediatr Transplant 2005 Kidney IV Ig +/- PP 20 pts 15/20 had resolution of AMR Garrett HE JHLT 2005 Heart Rituximab 8 pts 8/8 had resolution of AMR
51 Proliferation signal inhibitors (PSIs) Ø Mechanism l Inhibit proliferation of T, B, smooth muscle, endothelial cells Ø In clinical trials l rejection, CAV l viral infections l renal insufficiency l Impaired wound healing Ø Indications for sirolimus/ everolimus l Rejection l CAV l Malignancy l Viral infections (CMV) l Renal dysfunction (i/o CNI) Incidence of treated rejection Kobashigawa et al. Am J Transplant 2006;6:
52 Refractory Antibodies: Role of Bortezomib Cedar Sinai experience 6 patients with cpra 50% despite PP/IV Ig/ritux Side effects UTI, pneumonia, catheter infection, C difficile Neuropathy: responded to reduction in dose Outcomes cpra ê from 62% to 35% 5 with fall in cpra and successfully transplanted 1 with no Δ in cpra and died from sepsis after cycle #2 1 died post-oht from sepsis cpra 50% after IV Ig/ritux protocol Days 1, 4, 8, 11 Day 25 Repeat 2-wk cycle if cpra 50% Plasmapheresis Bortezomib 1.3 mg/m 2 Check PRA Patel et al J Heart and Lung Transp 2011; 30:1320
 Marques")
53 Photopheresis Principle Immunomodulation Promote destruction of cytotoxic T cells against the donor heart Procedure Leukapheresis: remove white cells Photoactivation: mix cells with psoralen and expose to UV light à apoptosis Reinfusion Role in rejection Tested in primary prevention and recurrent rejection Reduction in rejection and coronary intimal medial thickness (marker for CAV) Marques MB J Clin Apheresis 2006:

54 Photopheresis 60 pts, standard therapy vs photopheris q wk for 6 months post- OHT - Decrease in acute rejection - Did not look at humoral rejection Barr ML NEJM 1998; 339: pts with recurrent rejection 3-12 mon photopheresis Risk of rejection or death reduced after 3 months Kirklin JK JHLT 2006; 25:
 1 year: 16% vs 5% 3 years: 36% vs 17% 5 years: 64% vs 30% Michaels P J Heart Lung Transplant 2003; 22:")
55 Clinical Characteristics of Antibody-Mediated Rejection 44 patients with AMR Higher incidence of CAV (stenosis > 30%) 1 year: 16% vs 5% 3 years: 36% vs 17% 5 years: 64% vs 30% Michaels P J Heart Lung Transplant 2003; 22: 58-69


56 Year 0 Year 1 Year 2

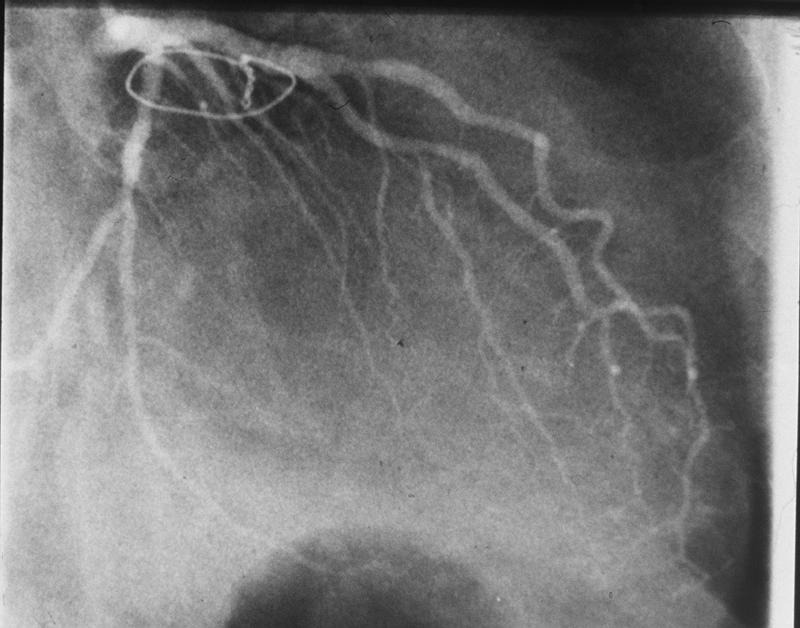
57 CASE STUDY 25 yr M 3 yrs S/P OHT noncompliant with IMS Admitted in cardiogenic shock EF <20%; Bx: Severe AMR; + DSA Treatment: Inotropes, IABP, cytolytic rx, plasmapheresis, IVIgG, augmented 3 drug rx Subsequent bx: neg; DSA low MFI Clinically improved with EF 50%; Pre-discharge coronary angiogram: no luminal abn 4 mon after successful rx of AMR pt died suddenly Autopsy: Severe CAV
58 Challenges of Antibody-Mediated Rejection Diagnosis Are symptoms required? Clinical versus pathological? Prevention How do we identify patients at high risk for AMR? Can high-risk patients be treated prior to transplant? Treatment How should AMR be treated? If the initial therapy fails, what next?
59 Antibody-Mediated Rejection: Summary Diagnosis Pathological findings only Prevention Assays for specification and quantification of HLA Ab cpra and virtual crossmatch Desensitization targeting B cells, plasma cells, and antibodies Treatment Subclinical AMR should be treated Long-term therapy: photopheresis vs densensitization Close monitoring for complications

60 AMR: Conclusion Difficult problem in heart transplantation-requires high index of suspicion Associated with increased morbidity and mortality Evidence based therapeutic strategies are limited
Solid Organ Transplant
 Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients
 in LUNG TRANSPLANT Recipients") Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
Antibody Mediated Rejection (AMR) in Heart Transplantation Session
 in Heart Transplantation Session") Page 1 Antibody Mediated Rejection (AMR) in Heart Transplantation Session Dear Colleagues: The Heart session at Banff this year will be solely focused on AMR and besides the fact that many of us attending
Page 1 Antibody Mediated Rejection (AMR) in Heart Transplantation Session Dear Colleagues: The Heart session at Banff this year will be solely focused on AMR and besides the fact that many of us attending
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
3/6/2017. Prevention of Complement Activation and Antibody Development: Results from the Duet Trial
 Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
3/6/2017. Treatment of Detected Antibodies. I have financial relationship(s) with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker
 with: Thoratec/St. Jude/Abbott Consultant CareDx Consultant/Speaker") Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Treatment of Detected Antibodies Sean Pinney, MD Director, Advanced Heart Failure & Transplantation Mount Sinai Hospital New York, NY Sean Pinney, MD Associate Professor of Medicine Icahn School of Medicine
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Desensitization in Kidney Transplant. James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver
 Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Antibody-Mediated Rejection in the Lung Allograft. Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305
 Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
AND My presentation does include discussion of off-label or investigational use (empiric therapy)
") Managing Sensitized Patients Pre-Heart Transplantation Patricia P. Chang, MD MHS Associate Professor of Medicine Director, UNC Heart Failure & Transplant Program Patricia P. Chang, MD MHS Associate Professor
Managing Sensitized Patients Pre-Heart Transplantation Patricia P. Chang, MD MHS Associate Professor of Medicine Director, UNC Heart Failure & Transplant Program Patricia P. Chang, MD MHS Associate Professor
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New. Ramsey Hachem, MD March 28, 2017
 Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Endothelitis in cardiac allograft biopsy specimens: Possible relationship to antibody-mediated rejection
 http://www.jhltonline.org ORIGINAL CLINICAL SCIENCE Endothelitis in cardiac allograft biopsy specimens: Possible relationship to antibody-mediated rejection Fabio Tavora, MD, a Raghava Munivenkatappa,
http://www.jhltonline.org ORIGINAL CLINICAL SCIENCE Endothelitis in cardiac allograft biopsy specimens: Possible relationship to antibody-mediated rejection Fabio Tavora, MD, a Raghava Munivenkatappa,
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
Heart Transplantation ACC Middle East Conference Dubai UAE October 21, 2017
 Heart Transplantation ACC Middle East Conference Dubai UAE October 21, 2017 Randall C Starling MD MPH FACC FAHA FESC FHFSA Professor of Medicine Kaufman Center for Heart Failure Department of Cardiovascular
Heart Transplantation ACC Middle East Conference Dubai UAE October 21, 2017 Randall C Starling MD MPH FACC FAHA FESC FHFSA Professor of Medicine Kaufman Center for Heart Failure Department of Cardiovascular
Heart Transplantation
 Heart Transplantation Abbas Ardehali, M.D., F.A.C.S. Professor of Surgery and Medicine, Division of Cardiac Surgery William E. Connor Chair in Cardiothoracic Transplantation Director, UCLA Heart, Lung,
Heart Transplantation Abbas Ardehali, M.D., F.A.C.S. Professor of Surgery and Medicine, Division of Cardiac Surgery William E. Connor Chair in Cardiothoracic Transplantation Director, UCLA Heart, Lung,
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS
 APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
2017 BANFF-SCT Joint Scientific Meeting. BARCELONA March 2017
 2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
Is it safe to transplant against HLA DSA in cardiothoracic patients? development and implementation of national Guidelines
 Is it safe to transplant against HLA DSA in cardiothoracic patients? development and implementation of national Guidelines Dr Martin Howell. Laboratory Director. Department of H&I, NHS Blood and Transplant,
Is it safe to transplant against HLA DSA in cardiothoracic patients? development and implementation of national Guidelines Dr Martin Howell. Laboratory Director. Department of H&I, NHS Blood and Transplant,
Treatment of Chronic Antibody Mediated Rejection
 Treatment of Chronic Antibody Mediated Rejection Robert A. Montgomery MD, DPhil Professor of Surgery Director of the NYU Langone Transplant Institute Disclosures: Served on Advisory Boards for Genentech
Treatment of Chronic Antibody Mediated Rejection Robert A. Montgomery MD, DPhil Professor of Surgery Director of the NYU Langone Transplant Institute Disclosures: Served on Advisory Boards for Genentech
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation
 Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
HLA Part II: My Patient Has DSA, Now What?
 2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
2017 CST-Astellas Canadian Transplant Fellows Symposium HLA Part II: My Patient Has DSA, Now What? James Lan, MD, FRCPC, D(ABHI) Dr. Lan completed his nephrology training at the University of British Columbia.
Transplant in Pediatric Heart Failure
 Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Heart Transplant: State of the Art. Dr Nick Banner
 Heart Transplant: State of the Art Dr Nick Banner Heart Transplantation What is achieved Current challenges Donor scarcity More complex recipients Long-term limitations Non-specific Pharmacological Immunosuppression
Heart Transplant: State of the Art Dr Nick Banner Heart Transplantation What is achieved Current challenges Donor scarcity More complex recipients Long-term limitations Non-specific Pharmacological Immunosuppression
2/28/2017. Adult Heart Transplants Donor and Recipient Characteristics UNOS, Retransplant VCM. Other /2015 (N = 24,474)
") 1 46% 2% 3% 4% 0% 2% 2% CHD HCM ICM NICM RCM 49% 3% 3% 3% 1% 3% 3% Retransplant VCM 42% Other 35% 1/1982 6/2015 1/2009 6/2015 2016 JHLT. 2016 Oct; 35(10): 1149-1205 UNOS, 2017 Adult Heart Transplants Donor
1 46% 2% 3% 4% 0% 2% 2% CHD HCM ICM NICM RCM 49% 3% 3% 3% 1% 3% 3% Retransplant VCM 42% Other 35% 1/1982 6/2015 1/2009 6/2015 2016 JHLT. 2016 Oct; 35(10): 1149-1205 UNOS, 2017 Adult Heart Transplants Donor
Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT. 4th April 2014
 Solid Organ Transplantation How the Lab Contributes to Improved Patient Outcomes Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT 4th April 2014 Solid Organ Transplantation
Solid Organ Transplantation How the Lab Contributes to Improved Patient Outcomes Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT 4th April 2014 Solid Organ Transplantation
Research Article The Natural History of Biopsy-Negative Rejection after Heart Transplantation
 Transplantation Volume 2013, Article ID 236720, 6 pages http://dx.doi.org/10.1155/2013/236720 Research Article The Natural History of Biopsy-Negative Rejection after Heart Transplantation Zhaoyi Tang,
Transplantation Volume 2013, Article ID 236720, 6 pages http://dx.doi.org/10.1155/2013/236720 Research Article The Natural History of Biopsy-Negative Rejection after Heart Transplantation Zhaoyi Tang,
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Transfusion support in Transplantation
 Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation
 AACC Professional Course BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation J. Ryan
AACC Professional Course BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation J. Ryan
Interstitial Inflammation
 Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Interstitial Inflammation Currently considered to be T cell-mediated process Plasma cell rich acute rejection often associated with AMR Preliminary data suggests that interstitial follicular helper T cells
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients
 Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Innovative Application of Immunologic Principles in Heart Transplantation
 The Ochsner Journal 10:231 235, 2010 f Academic Division of Ochsner Clinic Foundation Innovative Application of Immunologic Principles in Heart Transplantation Stacy A. Mandras, MD,* Joaquin Crespo, MD,{
The Ochsner Journal 10:231 235, 2010 f Academic Division of Ochsner Clinic Foundation Innovative Application of Immunologic Principles in Heart Transplantation Stacy A. Mandras, MD,* Joaquin Crespo, MD,{
Virtual Crossmatch in Kidney Transplantation
 Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
AMR in Liver Transplantation: Incidence
 AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
Med Path Rads Conference Gurpreet Sodhi M.D.
 Med Path Rads Conference 5.10.13 Gurpreet Sodhi M.D. Objectives -Define and understand noncompaction cardiomyopathy -Briefly review normal intracardiac hemodynamic pressures and interpret a patient s pressures
Med Path Rads Conference 5.10.13 Gurpreet Sodhi M.D. Objectives -Define and understand noncompaction cardiomyopathy -Briefly review normal intracardiac hemodynamic pressures and interpret a patient s pressures
DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY
 2016 DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY James H Lan, MD, FRCP(C), D(ABHI) Clinical Assistant Professor, University of British Columbia Nephrology & Kidney Transplantation, Vancouver General
2016 DE-MYSTIFYING THE BLACK BOX OF TRANSPLANT IMMUNOLOGY James H Lan, MD, FRCP(C), D(ABHI) Clinical Assistant Professor, University of British Columbia Nephrology & Kidney Transplantation, Vancouver General
Intravascular macrophages in cardiac allograft biopsies for diagnosis of early and late antibody-mediated rejection
 http://www.jhltonline.org Intravascular macrophages in cardiac allograft biopsies for diagnosis of early and late antibody-mediated rejection Marny Fedrigo, MD, PhD, a Giuseppe Feltrin, MD, PhD, a Francesca
http://www.jhltonline.org Intravascular macrophages in cardiac allograft biopsies for diagnosis of early and late antibody-mediated rejection Marny Fedrigo, MD, PhD, a Giuseppe Feltrin, MD, PhD, a Francesca
The multidisciplinary approach to AMR in lung transplantation: Reaching a consensus. Deborah Jo Levine Professor of Medicine University of Texas
 The multidisciplinary approach to AMR in lung transplantation: Reaching a consensus Deborah Jo Levine Professor of Medicine University of Texas Disclosures I have no financial relations with any relevant
The multidisciplinary approach to AMR in lung transplantation: Reaching a consensus Deborah Jo Levine Professor of Medicine University of Texas Disclosures I have no financial relations with any relevant
Marta Farrero Torres₁, Marcelo Pando₂, Dolly Tyan₂, Hannah Valantine₃, Spenser Smith₃, Kiran Khush₃
 Development of HLA donor specific antibodies after heart transplantation: importance of a new method to detect the first component of the complement cascade Marta Farrero Torres₁, Marcelo Pando₂, Dolly
Development of HLA donor specific antibodies after heart transplantation: importance of a new method to detect the first component of the complement cascade Marta Farrero Torres₁, Marcelo Pando₂, Dolly
Intruduction PSI MODE OF ACTION AND PHARMACOKINETICS
 Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
 Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Desensitization protocols for patients undergoing solid organ transplantation
 Desensitization protocols for patients undergoing solid organ transplantation Travail de Master en Médecine présenté à la Faculté de Biologie et de Médecine de l Université de Lausanne par Clara Guo Jury
Desensitization protocols for patients undergoing solid organ transplantation Travail de Master en Médecine présenté à la Faculté de Biologie et de Médecine de l Université de Lausanne par Clara Guo Jury
ABSTRACT AJCP /ORIGINAL ARTICLE. Downloaded from by guest on 07 January 2019
 Correlation of Circulating Complement-Fixing Donor-Specific Antibodies Identified by the C1q Assay and Presence of C4d in Endomyocardial Biopsy Specimens Renee Frank, MD, 1 Priti Lal, MD, 1 Jane Kearns,
Correlation of Circulating Complement-Fixing Donor-Specific Antibodies Identified by the C1q Assay and Presence of C4d in Endomyocardial Biopsy Specimens Renee Frank, MD, 1 Priti Lal, MD, 1 Jane Kearns,
Symposium. Post-operative Management Of Pediatric Heart Transplantation : A Brief Review
 DOI-10.21304/2018.0503.00394 Symposium Post-operative Management Of Pediatric Heart Transplantation : A Brief Review Balakrishnan KR*, Suresh KG**, Muralikrishna T***, Suresh Kumar R **** *Director, Cardiac
DOI-10.21304/2018.0503.00394 Symposium Post-operative Management Of Pediatric Heart Transplantation : A Brief Review Balakrishnan KR*, Suresh KG**, Muralikrishna T***, Suresh Kumar R **** *Director, Cardiac
Desensitization for solid organ and hematopoietic stem cell transplantation
 Andrea A. Zachary Mary S. Leffell Desensitization for solid organ and hematopoietic stem cell transplantation Authors address Andrea A. 1 Zachary, Mary S. Leffell 1 1 Department of Medicine, Division of
Andrea A. Zachary Mary S. Leffell Desensitization for solid organ and hematopoietic stem cell transplantation Authors address Andrea A. 1 Zachary, Mary S. Leffell 1 1 Department of Medicine, Division of
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Quantifying HLA-specific antibodies in patients undergoing desensitization Andrea Zachary a and Nancy L. Reinsmoen b
 Quantifying HLA-specific antibodies in patients undergoing desensitization Andrea Zachary a and Nancy L. Reinsmoen b a John Hopkins University, Immunogenetics Laboratory, Baltimore, Maryland and b Cedars-Sinai
Quantifying HLA-specific antibodies in patients undergoing desensitization Andrea Zachary a and Nancy L. Reinsmoen b a John Hopkins University, Immunogenetics Laboratory, Baltimore, Maryland and b Cedars-Sinai
Diagnosis and Management of Acute and Chronic Humoral Rejection. Lars Pape
 Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Diagnosis and Management of Acute and Chronic Humoral Rejection Lars Pape Immunosuppression Acute rejection Chronic rejection Side effects Infections Nephrotoxicity Adult population Nearly all late rejection-related
Tolerance Induction in Transplantation
 Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Objectives 3/6/2017. Impact of Non-HLA Antibodies in Lung Transplantation
 Impact of Non-HLA Antibodies in Lung Transplantation Nancy L. Reinsmoen, Ph.D., D(ABHI) Director, HLA and Immunogenetics Laboratory (Retired) Cedars Sinai Medical Center Los Angeles, CA Nancy L. Reinsmoen,
Impact of Non-HLA Antibodies in Lung Transplantation Nancy L. Reinsmoen, Ph.D., D(ABHI) Director, HLA and Immunogenetics Laboratory (Retired) Cedars Sinai Medical Center Los Angeles, CA Nancy L. Reinsmoen,
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
The Acceptable Mismatch program of Eurotransplant.
 The Acceptable Mismatch program of Eurotransplant. Frans Claas Leiden University Medical Center Eurotransplant Reference Laboratory Leiden, the Netherlands. Hinterzarten, December 7, 2013 Main problem
The Acceptable Mismatch program of Eurotransplant. Frans Claas Leiden University Medical Center Eurotransplant Reference Laboratory Leiden, the Netherlands. Hinterzarten, December 7, 2013 Main problem
6/19/2012. Who is in the room today? What is your level of understanding of Donor Antigens and Candidate Unacceptables in KPD?
 6/19/212 KPD Webinar Series: Part 3 Demystifying the OPTN Kidney Paired Donation Pilot Program Unacceptable HLA antigens: The key to finding a compatible donor for your patient M. Sue Leffell, Ph.D. J.
6/19/212 KPD Webinar Series: Part 3 Demystifying the OPTN Kidney Paired Donation Pilot Program Unacceptable HLA antigens: The key to finding a compatible donor for your patient M. Sue Leffell, Ph.D. J.
OBJECTIVES. Phases of Transplantation and Immunosuppression
 Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ
 Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ Art of Good Cooking Good Ingredient Good donor + OK recipient Good technique Good team Good timing Good
Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ Art of Good Cooking Good Ingredient Good donor + OK recipient Good technique Good team Good timing Good
Management of a Recipient with a Failed Kidney Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Disclosures Grant support: Bristol-Myers and Squibb Pharmaceuticals,
Management of a Recipient with a Failed Kidney Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Disclosures Grant support: Bristol-Myers and Squibb Pharmaceuticals,
Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly Sensitized Renal Transplanted Patients
 BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
Heart Transplantation
 Heart Transplantation Age and Outcome Mayo Clinic Richard Daly, MD Professor of Surgery Surgical Director Heart & Lung Transplantation 2014 MFMER 3346076-1 Rochester, Minnesota 2014 MFMER 3346076-2 The
Heart Transplantation Age and Outcome Mayo Clinic Richard Daly, MD Professor of Surgery Surgical Director Heart & Lung Transplantation 2014 MFMER 3346076-1 Rochester, Minnesota 2014 MFMER 3346076-2 The
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation. Doctoral Thesis. Dr. Petra Gombos
 Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Thesis Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Dr. Róbert Langer, Ph.D. Consultant:
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Thesis Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Dr. Róbert Langer, Ph.D. Consultant:
Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab
 ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
1. Discuss the basic pathophysiology of end-stage liver and kidney failure.
 TRANSPLANT SURGERY ROTATION (PGY1, 2) A. Medical Knowledge Goal: The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes. The resident will be exposed
TRANSPLANT SURGERY ROTATION (PGY1, 2) A. Medical Knowledge Goal: The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes. The resident will be exposed
Antihuman leukocyte antigen (HLA) antibodies can be
 antibodies can be") Antihuman Leukocyte Antigen Specific Antibody Strength Determined by Complement-Dependent or Solid-Phase Assays Can Predict Positive Donor-Specific Crossmatches Ibrahim Batal, MD; Adriana Zeevi, PhD; John
Antihuman Leukocyte Antigen Specific Antibody Strength Determined by Complement-Dependent or Solid-Phase Assays Can Predict Positive Donor-Specific Crossmatches Ibrahim Batal, MD; Adriana Zeevi, PhD; John
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Vascular Remodelling in Pancreas Transplantation
 Vascular Remodelling in Pancreas Transplantation Prof Steve White Consultant HPB/Transplant Surgeon The Freeman Hospital Newcastle President Elect EPITA European Pancreas Transplants Pancreas Transplants
Vascular Remodelling in Pancreas Transplantation Prof Steve White Consultant HPB/Transplant Surgeon The Freeman Hospital Newcastle President Elect EPITA European Pancreas Transplants Pancreas Transplants
IMMUNOBIOLOGY OF TRANSPLANTATION. Wasim Dar
 IMMUNOBIOLOGY OF TRANSPLANTATION Wasim Dar Immunobiology of Transplantation Overview Transplantation: A complex immunologic process Contributions Innate Immunity Adaptive immunity T Cells B Cells HLA Consequences
IMMUNOBIOLOGY OF TRANSPLANTATION Wasim Dar Immunobiology of Transplantation Overview Transplantation: A complex immunologic process Contributions Innate Immunity Adaptive immunity T Cells B Cells HLA Consequences
23/10/2017. Panel Reactive Antibodies and Crossmatch by Flow Cytometry. Antibodies against. Renal transplantation. Antibody mediated rejection (AMR)
") Renal transplantation Panel Reactive Antibodies and Crossmatch by Flow Cytometry Katherina Psarra Immunology Histocompatibility Dept Evangelismos Hospital Athens, Greece In spite of the enormous progress
Renal transplantation Panel Reactive Antibodies and Crossmatch by Flow Cytometry Katherina Psarra Immunology Histocompatibility Dept Evangelismos Hospital Athens, Greece In spite of the enormous progress
Nephrology Grand Rounds
 Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Figure 1. Actuarial survival of patients with ABO I, ABO compatible, and ABO identical grafts.
 New Insights into Antibody Mediated Graft Injury after Pediatric Liver Transplantation S.V. McDiarmid MD Professor of Pediatrics and Surgery David Geffen School of Medicine University of California, Los
New Insights into Antibody Mediated Graft Injury after Pediatric Liver Transplantation S.V. McDiarmid MD Professor of Pediatrics and Surgery David Geffen School of Medicine University of California, Los
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Transplant Success in Sensitized Patients Receiving a Standardized Desensitization Therapy: 3 Year Outcomes
 Transplant Success in Sensitized Patients Receiving a Standardized Desensitization Therapy: 3 Year Outcomes INTRODUCTION In patients awaiting a transplant, having antibodies reactive to HLA antigens present
Transplant Success in Sensitized Patients Receiving a Standardized Desensitization Therapy: 3 Year Outcomes INTRODUCTION In patients awaiting a transplant, having antibodies reactive to HLA antigens present
Anoxic insult Stroke/Cerebrovascular accident
 Page 1 of 5 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form 10: Death Print this Form t Started 1 Date of Death MM/DD/YYYY 2 Primary cause of death
Page 1 of 5 Patient Details Hidden Show Show/Hide Annotations Stickies: Toggle All Toggle Open Toggle Resolved Form 10: Death Print this Form t Started 1 Date of Death MM/DD/YYYY 2 Primary cause of death
FIT Board Review Corner March 2016
 FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
Review Article Antibody-Mediated Rejection in Heart Transplantation: Case Presentation with a Review of Current International Guidelines
 Transplantation Volume 2011, Article ID 351950, 7 pages doi:10.1155/2011/351950 Review Article Antibody-Mediated Rejection in Heart Transplantation: Case Presentation with a Review of Current International
Transplantation Volume 2011, Article ID 351950, 7 pages doi:10.1155/2011/351950 Review Article Antibody-Mediated Rejection in Heart Transplantation: Case Presentation with a Review of Current International
Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients
 Trends in Transplant. 2014;8:3-9 Gregor Bartel, Georg A. Böhmig: Alloantibodies and Graft Function Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients Gregor Bartel
Trends in Transplant. 2014;8:3-9 Gregor Bartel, Georg A. Böhmig: Alloantibodies and Graft Function Posttransplant Human Leukocyte Antigen Antibodies in Stable Kidney Transplant Recipients Gregor Bartel
Transplantation in Australia and New Zealand
 Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Acute Antibody-Mediated Rejection in Renal Transplantation: Current Clinical Management
 Curr Transpl Rep (2014) 1:78 85 DOI 10.1007/s40472-014-0012-y KIDNEY TRANSPLANTATION (ML HENRY, SECTION EDITOR) Acute Antibody-Mediated Rejection in Renal Transplantation: Current Clinical Management Carrie
Curr Transpl Rep (2014) 1:78 85 DOI 10.1007/s40472-014-0012-y KIDNEY TRANSPLANTATION (ML HENRY, SECTION EDITOR) Acute Antibody-Mediated Rejection in Renal Transplantation: Current Clinical Management Carrie
Transfusion Reactions. Directed by M-azad March 2012
 Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Transfusion Reactions Directed by M-azad March 2012 Transfusion Reactions are Adverse reactions associated with the transfusion of blood and its components Transfusion reactions Non-threatening to fatal
Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting Antibody-Mediated Rejection
 Clinical and Developmental Immunology Volume 2013, Article ID 460316, 6 pages http://dx.doi.org/10.1155/2013/460316 Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting
Clinical and Developmental Immunology Volume 2013, Article ID 460316, 6 pages http://dx.doi.org/10.1155/2013/460316 Research Article The Diagnostic Value of Transcription Factors T-bet/GATA3 Ratio in Predicting
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
The New Kidney Allocation System: What You Need to Know. Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health
 The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
HLA Antibody Complement Based Assays. Howard M. Gebel, PhD, D(ABHI) Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA
 Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA") HLA Antibody Complement Based Assays Howard M. Gebel, PhD, D(ABHI) Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA Disclosure Neither presenter has any financial relationships related
HLA Antibody Complement Based Assays Howard M. Gebel, PhD, D(ABHI) Robert A. Bray, PhD, D(ABHI) Emory University Hospital Atlanta, GA Disclosure Neither presenter has any financial relationships related
Sheena Surindran Grand Rounds 2/15/11
 Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Pediatric Kidney Transplantation
 Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
PCI in Patients with Transplant Coronary Artery Disease. Michael S. Lee, MD, FACC, FSCAI Assistant Professor UCLA School of Medicine
 PCI in Patients with Transplant Coronary Artery Disease Michael S. Lee, MD, FACC, FSCAI Assistant Professor UCLA School of Medicine Faculty Disclosure Honararia for Boston Scientific, BMS, Daiichi Sankyo,
PCI in Patients with Transplant Coronary Artery Disease Michael S. Lee, MD, FACC, FSCAI Assistant Professor UCLA School of Medicine Faculty Disclosure Honararia for Boston Scientific, BMS, Daiichi Sankyo,
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique. Mark D. Stegall Mayo Clinic, Rochester, MN
 Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
Clinical impact of de-novo HLA antibodies in pancreas and islet transplantation
 Clinical impact of de-novo HLA antibodies in pancreas and islet transplantation David Turner, PhD, FRCPath Lead for H&I Services, Scottish National Blood Transfusion Service Treatment of Type I DM Insulin
Clinical impact of de-novo HLA antibodies in pancreas and islet transplantation David Turner, PhD, FRCPath Lead for H&I Services, Scottish National Blood Transfusion Service Treatment of Type I DM Insulin
Approach to Kidney Transplant in Sensitized Potential Transplant Recipients
 RevIew Approach to Kidney Transplant in Sensitized Potential Transplant Recipients Antoine Barbari, Souodod Abbas, Mahassen Jaafar Abstract More than one-third of patients on waiting lists for kidney transplant
RevIew Approach to Kidney Transplant in Sensitized Potential Transplant Recipients Antoine Barbari, Souodod Abbas, Mahassen Jaafar Abstract More than one-third of patients on waiting lists for kidney transplant
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Utility of protocol kidney biopsies for de novo donor- specific antibodies
 Received: 6 June 2017 Revised: 24 July 2017 Accepted: 29 July 2017 DOI: 10.1111/ajt.14466 BRIEF COMMUNICATION Utility of protocol kidney biopsies for de novo donor- specific antibodies Sandesh Parajuli
Received: 6 June 2017 Revised: 24 July 2017 Accepted: 29 July 2017 DOI: 10.1111/ajt.14466 BRIEF COMMUNICATION Utility of protocol kidney biopsies for de novo donor- specific antibodies Sandesh Parajuli
Controversies in Renal Transplantation. The Controversial Questions. Patrick M. Klem, PharmD, BCPS University of Colorado Hospital
 Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial
: a randomised trial") Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Long-term efficacy and safety of conversion to tacrolimus in heart. transplant recipients with ongoing or recurrent acute cellular.
 Long-term efficacy and safety of conversion to tacrolimus in heart transplant recipients with ongoing or recurrent acute cellular rejection Blanka Skalická, Ivan Málek, Miloš Kubánek, Jevgenija Vymětalová,
Long-term efficacy and safety of conversion to tacrolimus in heart transplant recipients with ongoing or recurrent acute cellular rejection Blanka Skalická, Ivan Málek, Miloš Kubánek, Jevgenija Vymětalová,