BGS Spring Conference 2015
|
|
|
- Duane Porter
- 6 years ago
- Views:
Transcription
1 Neuroradiology in hyperacute stroke: what is the UK position? Dr Shelley Renowden Bristol
2 NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows that efficacy is unproven.suitability for thrombolysis can be guided by criteria used in the PISTE trial. 1.1 Patients with acute ischaemic stroke for whom thrombolysis is unsuitable/failed;.only performed with special arrangements for clinical governance, consent, audit, research 1.2 Patients with acute ischaemic stroke for whom thrombolysis is suitable:..used only in the context of research, which should in be RCTs comparing mechanical clot retrieval or the current methods of management and should report details of patient selection, timing of the intervention after onset of symptoms, the devices and techniques used, complications and functional outcomes NICE encourages clinicians to enter patients into RTs such as PISTE we have been doing thrombectomy in selected patients.
3 ischaemic stroke patient age co-morbidites (age, diabetes) NIHSS site, extent of occlusion collateral circulation extent of recanalisation time from ictus to recanalisation SICH leukoariosis
4 NIHSS NIHSS > % chance of good outcome at 1yr cf 60-70% in those with NIHSS <10 see Balami et al, Brain, 2013, 136, )
5 IV TPA / NIHSS: STOPSTROKE good poor outcome NIHSS 0-5 n=352 no iv tpa 81% 19% iv tpa 70% 30% p=0.31 NIHSS 6-10 n= 109 no iv tpa 52% 48% iv tpa 74% 26% p=0.038 NIHSS n=79 no IV tpa 35% 65% iv tpa 50% 50% p=0.15 NIHSS >=16 n= 109 no iv tpa 12% 88% iv tpa 27.5% 72.5% p=0.034 Gonzalez et al, Stroke, 2013, 44,
6 NIHSS and LVO? median NIHSS in M1 occlusion is 14 NIHSS % PPV LVO 48% sensitivity 55% of pts with NIHSS 10 - had LVO LVO in 90% NIHSS 16+ LVO in 100% NIHSS 27+ Maas et al, Stroke, 2009, 40,
7 Effect of IV TPA and occlusion site prox MCA distal MCA ICA/MCA TICA BA n NIHSS 18 (6-32) 13 (3-29) 19(6-29) 20(11-28) 27 TIMI 3 30% 44% 27% 6% 35% <2hr p=0.007 early 16% 33% 24% 0% 25% Improvement p= day 25% 52% 21% 18% 25% mrs<=1 p<0.001 mortal 24% 17% 14% 45% 75% 90 day p= Saqqur et al Stroke 2009 (Clotbust)
8 location of thrombus, outcome, anterior circulation stroke IVT, within 3 hours impact of thrombus location on CTP, % salvaged brain ICA M1p M1d M2-3 age` NIHSS onset to TPA ASPECTS infarct vol ml (mean) mrs % 82% 86% 90 days Sillanpaa et al, AJNR, 2013
9 final infarct volumes: EVT cf IVT in LVO 203 pts; LVO; mean age 66; median NIHSS 19; median infarct volume smaller for EVT (42cm3) cf IVT (109cm3) no Rx group (110cm3) EVT IV TICA occ M1 MCA M NIHSS Rangaraju et al, JAMA Neurology, 2013, 70,

10 clot length occlusion location is the strongest predictor of clot length (Kamaliam et al, Stroke 2013, 44, ) clot length 8+mm in 94% TICA, 73% M1 and 22% M2 occlusions IVT has no potential to recanalise occluded vessels if thrombus length > 8mm (Riedel et al, Stroke 2011, 42, )

11 7+ - predicts independent outcome


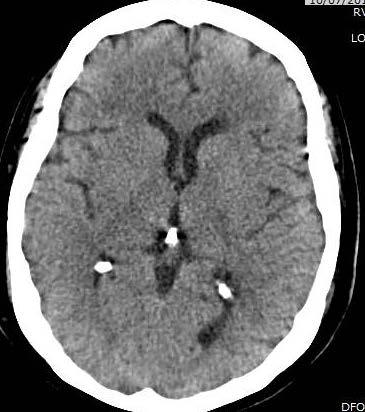
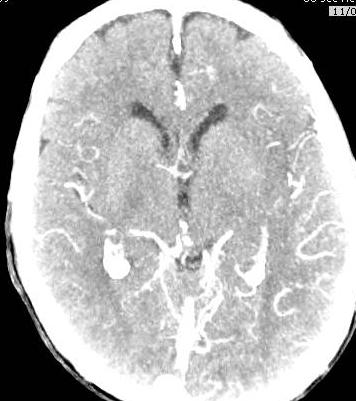
12 57F, AF, 3.5 hours after ictus left facial weakness, dense right hemiparesis (0/5) extensor R plantar left VFD severe expressive dysphasia NIHSS 20 ASPECTS 7



13
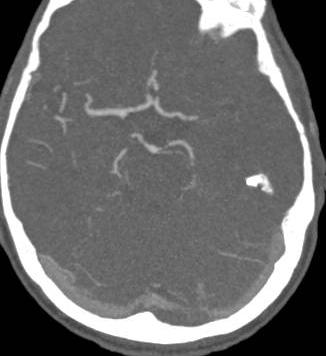

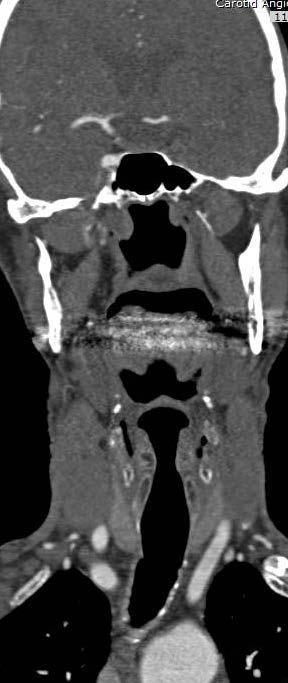
14


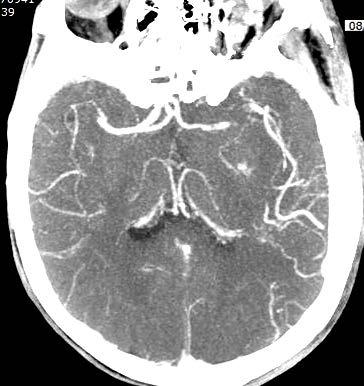
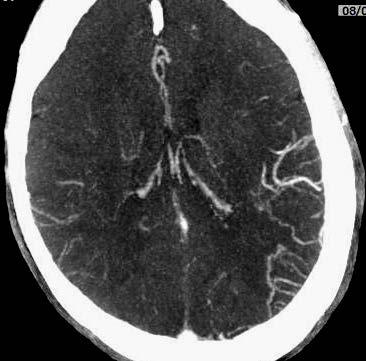
15 CTA normal parenchyma 71 F, NIHSS sec CT Brain
16 Recanalise Recanalisation using combined intravenous altepase and neurointerventional algorithm for acute ischaemic stroke n 90/7 favourable early neuro improvement outcome TIMI % 14% TIMI % 44% TIMI % 73% p < Mazighi et al, Stroke, 2009
17 IV TPA- recanalisation rates CTA database Calgary Stroke programme 216 pts- IV TPA; 103 went on to IA TPA M1-32.3%(43.1%); TICA 4% (39.1%); M2 31%(61.5%); BA 4% (52%) 60.5% who recanalised had good outcomes cf 24.3% who did notstrongest predictor of good outcome early recanalisation is associated with a better outcome than late Bhatia et al, Stroke, 2010, 41,
18 time from ictus to recanalisation IMS III - every 30 min delay in reperfusion is associated with 10% relative reduction in probability of a good outcome MRCLEAN OR for good outcome decreasing from 3.0 at 3.5 hours post ictus to reperfusion to 1.5 at 6 hours for each hour delay from ictus to TICI 2b/3 odds of good clinical outcome decreased by 38% - Menon et al, Stroke 2014 for every minute of arterial occlusion 1.9 million neurons and 14 billion synapses are lost
19 Recanalise n 90/7 favourable early neuro improvement outcome >260 mins 16 37% 37% mins 15 67% 73% ( 0.07) <210 mins 15 93% 93% (0.01) Mazighi et al, Stroke, 2009


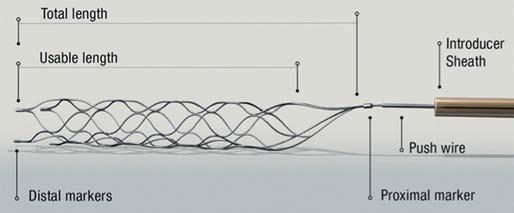
20 stent retriever



21 71F, NIHSS ictus 9.30am
22 SPEED SWIFT,TREVO - 2 RCTS USA median time to Rx 4.6 and 4.7 hours mrs % 40% STAR, TREVO EU median time to Rx 3.2 and 3.4 hours mrs % 55%
23 STAR prospective, 14 centres, 202 consecutive pts mean age 72, mean NIHSS 17, anterior circulation occlusion, Solitaire TICA 18%; M1 67%; M2 14% 59% IV TPA treated within 8 hours; median time from ictus to groin puncture 238 mins procedure time 29+/-27 mins balloon guide catheter, flow reversal mandatory TICI 2b/3 79% mrs % mortality 7% SICH 1.5% good collaterals correlate with good outcome p=0.034 Perreira et al, Stroke 2013, 44,




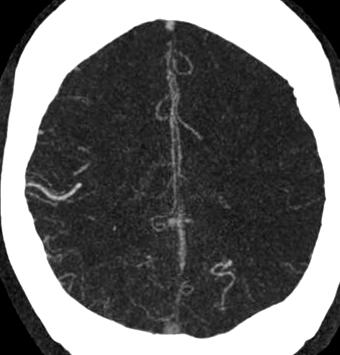
24 74M ictus NIHSS 21
25
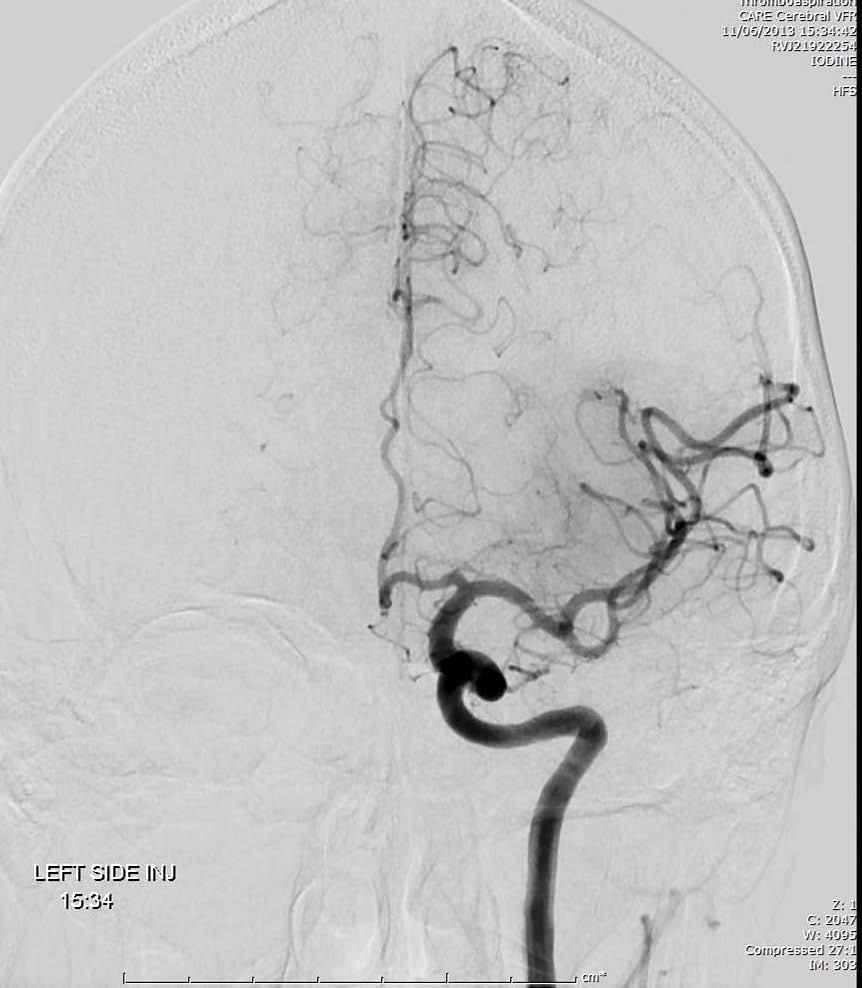
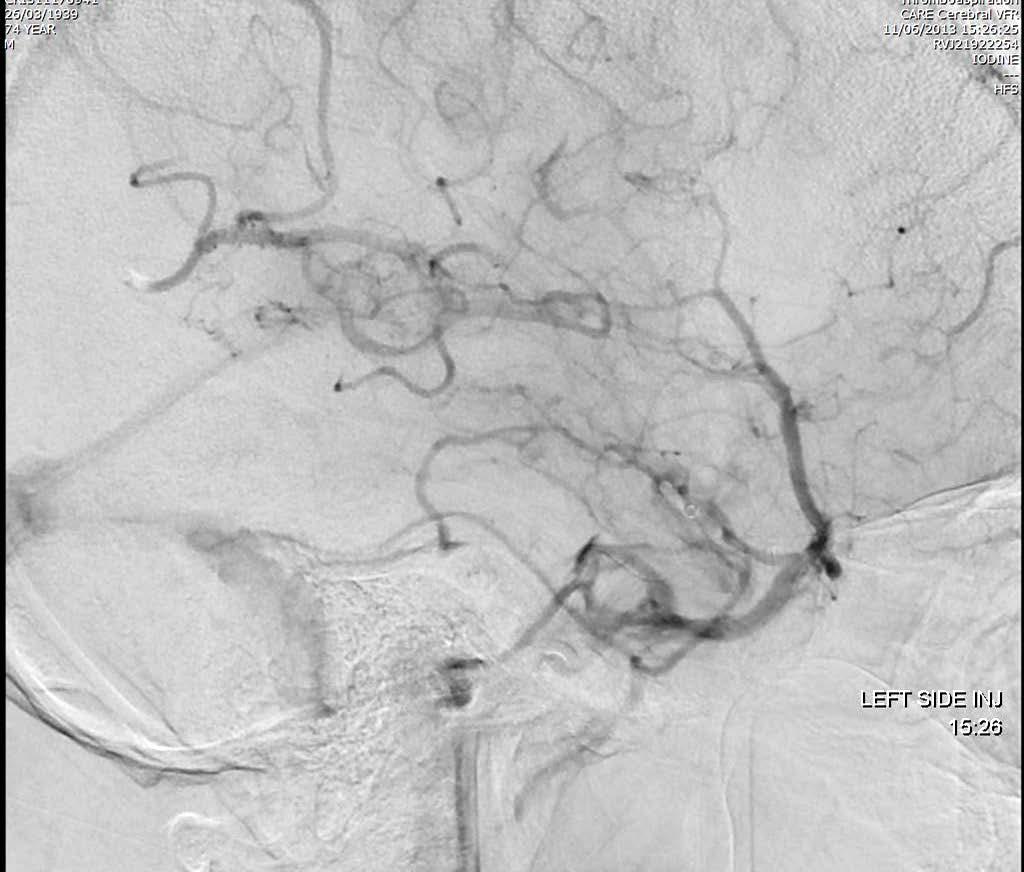
26 15.34


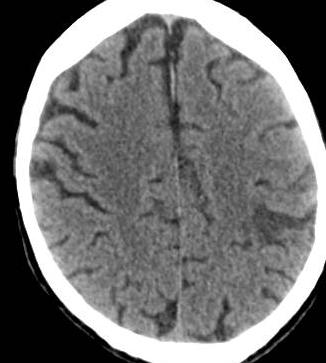
27
28 ADAPT - a direct aspiration first pass technique 37 consecutive pts (39-90 years old) (4 month study period) mean NIHSS 16.3 (5-30) M1 17; TICA 7; basilar 7; M2 5; M3 1; ADAPT alone successful in 75% flexible large bore catheter to thrombus. Aspiration with 20 or 60 ml syringe or Penumbra aspiration pump. Engage catheter in thrombus, then slowly withdraw with suction 9 required addition of stent retriever mean time from groin puncture to TICI 2b/3 28mins TICI 2b/3 in 100% TICI 3 in 65% 1 procedural complication (asymptomatic small SAH) 2 SICH mean NIHSS 4.2 at discharge (24pts (65%) 5 or below) 5 deaths Turk et al, JNIS 2014,



29 S BG rin g Sp 65M, NIHSS 22 on f C ce er en 15 20

30 Souza et al AJNR, 2012, 33, % bad outcome
31 105 consecutive pts, IV TPA within 3 hours median NIHSS 13 28% 18% 20% 29% 2% Saarinen et al AJNR, 2014

32 distal clot distal M1, M2, M3 good collaterals Souza 2-4


33 72M, NIHSS ictus 10.30am normal parenchyma



34 rin g C on f er en ce IV TPA running S Sp BG TICI pm

35 NIHSS 1





36 67M ;NIHSS 23 ictus 7am 8.37am 8.37am


37 80 sec head


38 9.30 am 10.28am

39
40 MRCLEAN NEJM, 2015, centres, Netherlands, Dec March pts, proximal anterior circulation occlusion (CTA/MRA)IAT cf usual Rx - 267pts- IVTPA; 233 EVT within 6 hours NIHSS 2 -: average 17, 18; ASPECTS 9 (median) in each group. 233 IAT (38% GA), acute carotid stenting 13% Mean age 65yrs: range yrs 445 pts IV TPA before randomization.time ictus to random mins Stentretrievers in 97% Independence in 32.6% cf 19.1% ; infarct vol at 7 days 49 cf 80ml No difference in mortality (7days: 12% each gp; 19% at 30) or SICH (18%: 17%) IAT usual ICA/M1 25% 28% M1 66% 62% M2 8% 8% A1/A2 32% 26% Time ictus to groin puncture 260 minutes (median) TICI 2b/3 in 59% FU CTA /MRA 24 hours - no occlusion in 75% cf 33%
41 EXTEND IA NEJM 2015 IV TPA within 4.5 hours cf EVT stent retriever 70 pts enrolled; 35 each arm; stopped prematurely ICA or MCA occlusion CTP ischaemic core <70 ml. EVT within 6 hours Ischaemic core at presentation / ml Perfusion volume at presentation 116 +/- 48ml IV TPA Median NIHSS /- 18.5ml 103 +/- 39ml IV +EVT ICA 31% 31% M1 51% 57% M2 17% 11% Median time ictus to groin puncture Median time ictus to TICI 2b/3 TICI 2b/3 in 86% 210 mins 248 mins 90 day mrs % 71% p=0.01 No significant difference in mortality and SICH; 12% GA. NNT 3
42 SWIFT PRIME, NEJM 2015 Stopped prematurely after 196 pts, 39 centres All had IV TPA within 4.5 hours, NIHSS 8-29 (11O 17+) YEARS OLD LVO anterior circulation ASPECTS > 6; CT EIC < 1/3 MCA territory EVT within 6 hours; 88% complete reperfusion mrs 0-2 at 90 days 60.2% EVT cf 35.5% IVT p<0.001 NNT 4 SICH 0% cf 3% (IV) Mortality at 90 days 9.2% cf 12.4% (IV) Ictus to arterial puncture was min (IQR) Ictus to first deployment of Solitaire min (IQR)
43 REVASCAT NEJM pts within 8 hours, 4 centres in Spain, halted early because of other trials years old, NIHSS 6+ (IQR ; median 17) ASPECTS < 7 excluded Later years ASPECTS 8+ IV TPA cf IV TPA and Solitaire, anterior circulation LVO 6.7% GA Wait 30 mins for IVTPA mrs 0-2 at 90 days 44% cf 28% OR day mortality 18.4% cf 15.5% SICH 2% each arm Median time from ictus to groin puncture 269mins ( ) Median time from ictus to revascularisation 355 mins ( )
44 ESCAPE NEJM 2015 LVO anterior circulation, within 12 hours, ASPECTS 6-10; poor collaterals excluded Standard care cf thrombectomy; enrolment up to 12 hours Stopped early 49 (15.5%) randomized after 6 hours 22 centres, 316 pts; 238 received IV TPA (120 in EVT group) Median time from CT to reperfusion was 84 mins and from ictus to reperfusion, 241 mins EVT IVT Median NIHSS ASPECTS 9 (8-10) 9(8-10) ICA + M1 27.6% 26.5% M1 or all M2 68.1% 71.4% M2 single 3.7% 2.0% 90 day mrs % 29.3% p<0.001 Mortality 10.4% 19% SICH 3.6% 2.7% GA 9%
45 MRCLEAN OR for good outcome decreasing from 3.0 at 3.5 hours ictus to reperfusion to 1.5 at 6 hours treatment effect not statistically significant if reperfusion after 6 hours 19 mins ESCAPE- 15.5% pts were treated successfully after 6 hours collaterals extending time window based on imaging

46 MRCLEAN 16% were 80+ years old significant benefit from EVT- similar to entire EV cohort : OR 3.24 ESCAPE, SWIFT PRIME also showed benefit for those 80+ (oldest in ESCAPE was 93!) MRCLEAN EVT beneficial with ASPECTS 5+ not 4 and below
47 ESO-Karolinska Stroke Update with ESMINT, ESNR mechanical thrombectomy with IV TPA within 4.5 hours, LVO, anterior circulation up to 6 hours after ictus (level of evidence A/1a) decision jointly by multidisciplinary team including stroke physician and INR, experienced centre thrombectomy by trained experienced INR large infarcts excluded
48 NICE HIS July, 2013 The current evidence on mechanical clot retrieval for treating acute ischaemic stroke shows that efficacy is unproven.suitability for thrombolysis can be guided by criteria used in the PISTE trial. 1.1 Patients with acute ischaemic stroke for whom thrombolysis is unsuitable/failed;.only performed with special arrangements for clinical governance, consent, audit, research 1.2 Patients with acute ischaemic stroke for whom thrombolysis is suitable:..used only in the context of research, which should in be RCTs comparing mechanical clot retrieval or the current methods of management and should report details of patient selection, timing of the intervention after onset of symptoms, the devices and techniques used, complications and functional outcomes NICE encourages clinicians to enter patients into RTs such as PISTE
49 ?
50

51 PISTE 18 years+, eligible IV TPA within 4.5 hours LVO, NIHSS 6+ EVT must be started within 90 mins of the IV TPA; groin puncture no more than 5.5 hours post ictus; angio within 6 hours 90 day mrs 0-2 mrs 0-1, mortality, eni 8+ NIHSS or NIHSS 0,1 at 72 hours, angio patency, immediate revascularisation rate, home time, sich etc
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016
 Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
Mechanical Thrombectomy: Where Are We Now? T. Adam Oliver, MD Tallahassee Neurological Clinic Tallahassee, Florida TMH Neurosymposium June 11, 2016 none DISCLOSURES Where did we come from? Spiotta, et
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Endovascular Stroke Therapy
 Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Endovascular Stroke Therapy Update with Emphasis on Practical Clinical and Imaging Considerations Sachin Kishore Pandey, MD, FRCPC Disclosures I have no relevant financial disclosures or conflict of interest
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Neuro-vascular Intervention in Stroke. Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust
 Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Neuro-vascular Intervention in Stroke Will Adams Consultant Neuroradiologist Plymouth Hospitals NHS Trust Stroke before the mid 1990s Swelling Stroke extension Haemorrhagic transformation Intravenous thrombolysis
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke P A C I F I C N E U R O. O R G
 Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Latest Advances in the Neurointerventional Treatment of Ischemic Stroke Neurointerventional Management of Ischemic Stroke 1. Thrombectomy for acute ischemic stroke 2. Carotid artery stenting 3. Management
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke. Kenneth V Snyder MD PhD SUNY Buffalo, NY
 Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Evidence for Mechanical ThrombectomyFor Acute Ischemic Stroke Kenneth V Snyder MD PhD SUNY Buffalo, NY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Honorarium
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Strokecenter Key lessons of MR CLEAN study
 Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Strokecenter Key lessons of MR CLEAN study Diederik Dippel Disclosures Funded by the Dutch Heart Foundation Nominal, unrestricted grants from AngioCare BV Medtronic/Covidien/EV3 MEDAC Gmbh/LAMEPRO Penumbra
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Endovascular Clot Retrieval. Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital
 Christchurch Hospital") Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Endovascular Clot Retrieval Teddy Wu Neurologist (and Stroke enthusiast) Christchurch Hospital Something you can do tomorrow Melbourne half marathon 2016 In 2009 Simple approach to stroke - blocked artery,
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials
 Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Figures for Draft Response to IMS III, MR RESCUE, and SYNTHSESIS Trials Figure 1: Lay Press Judgment May Belie a Deeper Examination of the Data. Truman ultimately defeated Dewey for the Presidency Subject
Acute Stroke Management What is State of the Art?
 Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
Acute Stroke Management What is State of the Art? Karl-Titus Hoffmann Department of Neuroradiologie University of Leipzig / University Hospital Leipzig Disclosure Speaker name: Karl-Titus Hoffmann I have
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Further Pragmatic Trials of Thrombectomy are Needed
 Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Further Pragmatic Trials of Thrombectomy are Needed Prof Keith W Muir Institute of Neuroscience & Psychology University of Glasgow Institute of Neurological Sciences Queen Elizabeth University Hospital
Endovascular stroke research after MRCLEAN. W. van Zwam
 1 Endovascular stroke research after MRCLEAN W. van Zwam 2 Layout 1. What do we know by now 2. Next research questions Anesthesia Aspiration 3. Ongoing and future research Dutch initiatives 3 4 N=70 Intervention
1 Endovascular stroke research after MRCLEAN W. van Zwam 2 Layout 1. What do we know by now 2. Next research questions Anesthesia Aspiration 3. Ongoing and future research Dutch initiatives 3 4 N=70 Intervention
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Pr Roman Sztajzel Service de Neurologie HUG
 Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
Pr Roman Sztajzel Service de Neurologie HUG Conflict of interest: none IV THROMBOLYSIS AND ENDOVASCULAR THROMBECTOMY approved treatments of acute stroke main criteria time (delay) IV thrombolysis radiological
ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE HHS Stroke Annual Review March 7 and March 8, 2018 Objectives To review the stroke endovascular mechanical thrombectomy evidence
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials
 Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
Published online: March 13, 2015 1664 9737/15/0034 0115$39.50/0 Review Endovascular Treatment for Acute Ischemic Stroke: Considerations from Recent Randomized Trials Manabu Shirakawa a Shinichi Yoshimura
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Sentinel Stroke National Audit Programme (SSNAP) Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017
 Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017") Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
What is the best imaging protocol for LVO screening when outside of 0-6h window?
 Klinik und Poliklinik für Neuroradiologische Diagnostik und Intervention Zentrum für Radiologie und Endoskopie WLNC, Los Angeles/CA, USA, May 15-17, 2017 What is the best imaging protocol for LVO screening
Klinik und Poliklinik für Neuroradiologische Diagnostik und Intervention Zentrum für Radiologie und Endoskopie WLNC, Los Angeles/CA, USA, May 15-17, 2017 What is the best imaging protocol for LVO screening
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 IN PATIENTS WITH ACUTE ISCHEMIC STROKE") A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE Hocine REDJEM Raphaël BLANC Bertrand LAPERGUE Gabriele CICCIO Stanislas SMAJDA Mikael MAZIGHI Georges RODESCH Michel
A DIRECT ASPIRATION FIRST PASS TECHNIQUE (ADAPT) IN PATIENTS WITH ACUTE ISCHEMIC STROKE Hocine REDJEM Raphaël BLANC Bertrand LAPERGUE Gabriele CICCIO Stanislas SMAJDA Mikael MAZIGHI Georges RODESCH Michel
Endovascular Therapy: Beyond the Guidelines
 Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Endovascular Therapy: Beyond the Guidelines Ashutosh P. Jadhav, MD PhD Assistant Professor, Neurology and Neurological Surgery Center for Neuro-endovascular Therapy UPMC Stroke Institute Pittsburgh, PA
Acute Management of Stroke due to Intracranial Steno-occlusion. Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital
 Acute Management of Stroke due to Intracranial Steno-occlusion Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital None Disclosure Contents Current status of acute management
Acute Management of Stroke due to Intracranial Steno-occlusion Joon-Tae Kim, MD, PhD Department of Neurology Chonnam National University Hospital None Disclosure Contents Current status of acute management
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times
 ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
ESCAPE Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times Michael D Hill, Mayank Goyal on behalf of the ESCAPE Trial
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention
 Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Stroke Cart Improves Efficiency in Acute Ischemic Stroke Intervention MR Amans, F Settecase, R Darflinger, M Alexander, A Nicholson, DL Cooke, SW Hetts, CF Dowd, RT Higashida, VV Halbach Interventional
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit. Hans Henkes, Wiebke Kurre Stuttgart, Germany
 Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit Hans Henkes, Wiebke Kurre Stuttgart, Germany 1 Thrombectomy... with stent-retrievers is an evidence based therapy for intracranial
Distal Mechanical Thrombectomy in Acute Ischemic Stroke Method and Benefit Hans Henkes, Wiebke Kurre Stuttgart, Germany 1 Thrombectomy... with stent-retrievers is an evidence based therapy for intracranial
TCD Monitoring of reperfusion therapies in acute ischemic stroke patients with proximal intracranial occlusion
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 5 Advanced neurosonology - Level 3 TCD Monitoring of reperfusion therapies in acute ischemic
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 5 Advanced neurosonology - Level 3 TCD Monitoring of reperfusion therapies in acute ischemic
Volume 13 - Issue 3, Interventions
 Volume 13 - Issue 3, 2013 - Interventions Interventional Radiology And Stroke Therapy Authors Dr. Leo Lawler Dr. Matt Crockett Dr. Eoin Kavanagh Prof. Sean Murphy Stroke Physician Mater Misericordiae University
Volume 13 - Issue 3, 2013 - Interventions Interventional Radiology And Stroke Therapy Authors Dr. Leo Lawler Dr. Matt Crockett Dr. Eoin Kavanagh Prof. Sean Murphy Stroke Physician Mater Misericordiae University
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Lessons Learned from IMS III: Implications for the Future
 Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Interventional Revolution in Treatment of Stroke
 TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
TCT RUSSIA 2018 XX Moscow s International Course on Endovascular Therapies Moscow, Russia, May 18-20, 2018 Interventional Revolution in Treatment of Stroke Horst Sievert, Ilona Hofmann, Laura Vaskelyte,
AHA/ASA Guideline. Downloaded from by on November 7, 2018
 AHA/ASA Guideline 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular
AHA/ASA Guideline 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular
Acute Ischemic Stroke Imaging Innovations
 Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
Acute Ischemic Stroke Imaging Innovations Guilherme Dabus, MD, FAHA Director, Fellowship NeuroInterventional Surgery Miami Cardiac & Vascular Institute Baptist Neuroscience Center Baptist Neuroscience
Endovascular Therapy for Acute Ischaemic Stroke in Northern Ireland. Ian Rennie Interventional Neurologist On behalf of the Belfast trust stroke team
 Endovascular Therapy for Acute Ischaemic Stroke in Northern Ireland Ian Rennie Interventional Neurologist On behalf of the Belfast trust stroke team Belfast Team Evidence base we rely on ESCAPE trial Acute
Endovascular Therapy for Acute Ischaemic Stroke in Northern Ireland Ian Rennie Interventional Neurologist On behalf of the Belfast trust stroke team Belfast Team Evidence base we rely on ESCAPE trial Acute
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Better identification of patients who may benefit from therapy
 Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Jon Jui MD, MPH Large Vessel Occlusion Low rates of re-canalization after tpa Only 25 % of large vessel strokes re-canalization after tpa Newer invasive techniques Solitaire vs Merci Better identification
Benjamin Fox, MD Medical Director: Neurointerventional Radiology (NIR) DRMC Medical Director: Neurosurgery & Neurovascular, Intermountain Healthcare
 DRMC Medical Director: Neurosurgery & Neurovascular, Intermountain Healthcare") Update on neurointerventional (NIR) services at Dixie Regional Medical Center and in the Southwest Region Benjamin Fox, MD Medical Director: Neurointerventional Radiology (NIR) DRMC Medical Director: Neurosurgery
Update on neurointerventional (NIR) services at Dixie Regional Medical Center and in the Southwest Region Benjamin Fox, MD Medical Director: Neurointerventional Radiology (NIR) DRMC Medical Director: Neurosurgery
12/4/2017. Disclosures. Study organization. Stryker Medtronic Penumbra Viz Route 92. Data safety monitoring board Tudor G.
 12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
12/4/2017 Update on Stroke Trials:Extending the Window DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo NP001713
1/19/2018. Endovascular Therapy for Stroke
 Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
Endovascular Therapy for Stroke 1 PROACT II (1999, IA urokinase)first to demonstrate benefit of EST Newer trials (including MERCI in 2005) demonstrated vessel recanalization but no clinical benefit 2 Based
IV tpa and mechanical thrombectomy case selection
 IV tpa and mechanical thrombectomy case selection 22 April 2017, 9.50-10.30 Deidre De Silva SGH campus, NNI, Singapore OUTLINE Reperfusion concept Case Selection factors IV tpa & Mechanical Thrombectomy
IV tpa and mechanical thrombectomy case selection 22 April 2017, 9.50-10.30 Deidre De Silva SGH campus, NNI, Singapore OUTLINE Reperfusion concept Case Selection factors IV tpa & Mechanical Thrombectomy
Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke.
 Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke. Poster No.: C-1669 Congress: ECR 2014 Type: Scientific Exhibit
Extra- and intracranial tandem occlusions in the anterior circulation - clinical outcome of endovascular treatment in acute major stroke. Poster No.: C-1669 Congress: ECR 2014 Type: Scientific Exhibit
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
WHY TIMELINESS MATTERS. W&M Wren Association Lecture Series
 WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
WHY TIMELINESS MATTERS April 10, 2018 W&M Wren Association Lecture Series Pankajavalli Ramakrishnan, M.D., Ph.D. Stroke Neurologist and Neurointerventionalist Riverside Regional Medical Center Comprehensive
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Disclosures. Current Management of Acute Ischemic Stroke. Overview. Focal brain ischemia. Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015
 Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
Disclosures Current Management of Acute Ischemic Nerissa U. Ko, MD, MAS Professor of Neurology May 8, 2015 Nothing to disclose Research Funding: American Heart Association NIH/NINDS Selected slides courtesy
ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS
 Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
Associate Professor of Neurology Director of Neurointerventional Services University of Louisville School of Medicine ACUTE STROKE INTERVENTION: THE ROLE OF THROMBECTOMY AND IA LYSIS Conflict of Interest
NHS England. Evidence review: Mechanical thrombectomy for acute ischaemic stroke in the anterior cerebral circulation
 NHS England Evidence review: Mechanical thrombectomy for acute ischaemic stroke in the anterior cerebral circulation 1 NHS England Evidence review: Mechanical thrombectomy for acute ischaemic stroke in
NHS England Evidence review: Mechanical thrombectomy for acute ischaemic stroke in the anterior cerebral circulation 1 NHS England Evidence review: Mechanical thrombectomy for acute ischaemic stroke in
Thrombectomy with the preset stent-retriever. Insights from the ARTESp* trial
 Thrombectomy with the preset stent-retriever Insights from the ARTESp* trial Wiebke Kurre, MD Klinikum Stuttgart - Germany * Acute Recanalization of Thrombo-Embolic Ischemic Stroke with preset (ARTESp)
Thrombectomy with the preset stent-retriever Insights from the ARTESp* trial Wiebke Kurre, MD Klinikum Stuttgart - Germany * Acute Recanalization of Thrombo-Embolic Ischemic Stroke with preset (ARTESp)
Trial and Cost Effectiveness Evaluation of Intra arterial Thrombectomy in Acute Ischemic Stroke
 Trial and Cost Effectiveness Evaluation of Intra arterial Thrombectomy in Acute Ischemic Stroke S. Bracard, F. Guillemin, X. Ducrocq for the THRACE investigators Disclosure Personal: No disclosure Study
Trial and Cost Effectiveness Evaluation of Intra arterial Thrombectomy in Acute Ischemic Stroke S. Bracard, F. Guillemin, X. Ducrocq for the THRACE investigators Disclosure Personal: No disclosure Study
Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion 14 Hours after Stroke Onset
 Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 9289218, 4 pages https://doi.org/10.1155/2017/9289218 Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion
Hindawi Case Reports in Neurological Medicine Volume 2017, Article ID 9289218, 4 pages https://doi.org/10.1155/2017/9289218 Case Report Successful Mechanical Thrombectomy of a Middle Cerebral Artery Occlusion
UNIVERSITY HOSPITAL UDINE/ITALY A SINGLE CENTRE EXPERIENCE IN STROKE TREATMET WITH EMBOTRAP II. TECHNOLOGY BASE ON CLOT RESEARCH
 UNIVERSITY HOSPITAL UDINE/ITALY A SINGLE CENTRE EXPERIENCE IN STROKE TREATMET WITH EMBOTRAP II. TECHNOLOGY BASE ON CLOT RESEARCH Massimo Sponza, Vladimir Gavrilović RIPERFUSION THERAPY Intraovenous thrombolysis
UNIVERSITY HOSPITAL UDINE/ITALY A SINGLE CENTRE EXPERIENCE IN STROKE TREATMET WITH EMBOTRAP II. TECHNOLOGY BASE ON CLOT RESEARCH Massimo Sponza, Vladimir Gavrilović RIPERFUSION THERAPY Intraovenous thrombolysis
Supplementary Online Content
 Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
Supplementary Online Content Badhiwala JH, Nassiri F, Alhazzani W, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis. JAMA. doi:10.1001/jama.2015.13767. etable 1. The modified
DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
What Have We Learned: Selection for Endovascular Stroke Therapy
 What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director,
What Have We Learned: Selection for Endovascular Stroke Therapy Raul G Nogueira, MD Associate Professor in Neurology, Neurosurgery, and Radiology Emory University Director, Neuroendovascular Service Director,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of mechanical clot retrieval for treating acute ischaemic stroke An ischaemic stroke
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of mechanical clot retrieval for treating acute ischaemic stroke An ischaemic stroke
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Patient selection for i.v. thrombolysis and thrombectomy
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 8 Acute treatment and early secondary prevention of stroke Level 2 Patient selection for
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
Historical. Medical Policy
 Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Medical Policy Subject: Mechanical Embolectomy for Treatment of Acute Stroke Policy #: SURG.00098 Current Effective Date: 01/01/2016 Status: Revised Last Review Date: 08/06/2015 Description/Scope This
Intra-arterial Stroke Therapy: 2018 Update
 Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
Intra-arterial Stroke Therapy: 2018 Update Expanding the Treatment Window Parita Bhuva, M.D. Medical Director Enrolling investigator Stryker Neurovascular (DAWN trial) Disclosures Most common large vessel
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
Developing the DAISI (Devices for Acute Ischemic Stroke Intervention) Coordinated Registry Network: A NEST Development Project
 Coordinated Registry Network: A NEST Development Project") Travelling through the NETs of the NEST: Toward Collective, Collaborative Intelligence via Continuum of Evidence Generation Developing the DAISI (Devices for Acute Ischemic Stroke Intervention) Coordinated
Travelling through the NETs of the NEST: Toward Collective, Collaborative Intelligence via Continuum of Evidence Generation Developing the DAISI (Devices for Acute Ischemic Stroke Intervention) Coordinated
Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time
 DOI: 10.5797/jnet.oa.2016-0140 Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time Yoichi Morofuji, 1,2 Nobutaka Horie, 1,2 Yohei Tateishi, 2,3 Minoru Morikawa, 4 Eisaku Sadakata,
DOI: 10.5797/jnet.oa.2016-0140 Endovascular Therapy for Acute Ischemic Stroke: Reducing Door-to-puncture Time Yoichi Morofuji, 1,2 Nobutaka Horie, 1,2 Yohei Tateishi, 2,3 Minoru Morikawa, 4 Eisaku Sadakata,