ACLS Study Guide Key guidelines recommendations for healthcare professionals:
|
|
|
- Lindsey Atkinson
- 6 years ago
- Views:
Transcription

1 1
2 ACLS Study Guide Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative waveform capnography the monitoring and measuring of carbon dioxide output to confirm intubation and monitor CPR quality. Therapeutic hypothermia, or cooling, should be part of an overall interdisciplinary system of care after resuscitation from cardiac arrest. Atropine is no longer recommended for routine use in managing and treating pulseless electrical activity (PEA) or asystole. Patient Assessment In ACLS, the specific treatment of a given dysrhythmia or condition depends on the patient s hemodynamic,status. In general, patients can be divided into four categories to determine treatment priorities: Asymptomatic, Symptomatic Stable, Symptomatic Unstable, or Pulseless. Asymptomatic patients do not receive treatment, but should be monitored for changes in condition. Any patientwith symptoms (even apparently mild symptoms such as palpitations) should be assessed to determine if they are Stable or Unstable. Determination of a patient s level of hemodynamic compromise can include several factors, including General Appearance, Level of Consciousness, and Vital Signs (especially systolic Blood Pressure). 2
3 General Appearance: The first indication of hemodynamic status comes from a patient s general appearance, including skin signs, level of activity, and work of breathing. If a patient shows signs of compensation (such as pale, cool, or diaphoretic skin) or acute distress, they are unstable. Level of Consciousness: Interaction with the patient allows the provider to evaluate the patient s level of consciousness, based on the patient s activity, awareness of their surroundings, and ability to provide information. If a patient shows any level of mental deficit, family or friends should be consulted to determine if this state differs from the patient s baseline. If the mental deficit is acute, the patient should be considered unstable. Vital Signs: Vital signs provide a diagnostic evaluation of the patient. Blood Pressure is the primary indicator. A systolic blood pressure above 90 mm usually indicates that the patient is stable (although the provider should be alert for changes in blood pressure that might indicate an unstable patient even if blood pressure is normal). Other vital signs may be useful, but should not be relied upon exclusively. Pulse Oximetry can be useful, especially if it rises or falls, but providers should remember that various conditions (such as CO2 poisoning) can mask changes in blood oxygen levels, and that a high O2 saturation may be present in unstable patients (such as those in shock). Additionally, heart rate is of no use in determining if a patient is stable or unstable a patient with a heart rate of 80 can be severely unstable, while a patient with a heart rate of 210 can be stable if they are still perfusing well. If a patient s General Appearance, Level of Consciousness, and Vital Signs are all normal, the patient is stable. If possible, treatment should be rendered starting with the least invasive that is appropriate for that patient s hemodynamic status. In ACLS, the preferential treatment for symptomatic but stable patients is generally Medications, while the preferential treatment for unstable patients is generally Electrical Therapy. Once treatment is rendered, the provider must reassess the patient. If the patient remains symptomatic, the appropriate treatment (medications or electricity) should be given again depending on the patient s heart rhythm and current hemodynamic status. (Thus, if a patient was stable before, but becomes unstable after administration of a drug, the patient should receive electrical therapy to continue treating the dysrhythmia rather than additional doses of a medication.) If a patient s General Appearance indicates that they may be unconscious, you should check for responsiveness. 3
4 If the patient is Unresponsive, get help (send someone to call 911 and bring back an AED, call a code, etc.). The BLS Algorithm should then be followed Chest compression, Airway, Breathing (C-A-B). New science indicates the following order: C-A-B 1. Check the patient for responsiveness. 2. Check for no breathing or no normal breathing. 3. Call for help. 4. Check the pulse for no longer than 10 seconds. 5. Give 30 compressions. 6. Open the airway and give 2 breaths. 7. Resume compressions. If the patient is apneic, and if the patient is pulseless, rescuers should begin CPR. Once you determine that a patient is Pulseless, an AED or EKG monitor should be attached as soon as possible. CPR should be continued with minimal interruptions. After each rhythm check, the patient should be Defibrillated if appropriate (for V-Fib and Pulseless V-Tach). Regardless of the heart rhythm, medications should be given as soon as possible after CPR is resumed (the specific medication determined by the patient s exact status and heart rhythm). 4
5 ACLS Algorithm Review Always start with the C-A-B & D survey! ACUTE CORONARY SYNDROMES Algorithm: Acute Coronary Syndromes Remember: Consider MONA for patients with suspected ACS (angina or AMI): Morphine Oxygen Nitroglycerine (contraindicated SBP <90 mm/hg, Inferior wall MI and RT ventricular infarction, and Recent Viagra use). Aspirin but in the order Oxygen, Aspirin, Nitro, Morphine. Acute Stoke Case The identification and initial management of patients with acute stroke fall within the scope of the ACLS provider. The goal of stroke care is to minimize brain injury and maximize the patient s recovery. Early recognition of acute ischemic stroke is important because IV fibrinolytic treatment should be provided as early as possible, generally within 3 hours of onset of symptoms, or within 4.5 hours of onset of symptoms for selected patients. The 8 D s of Stroke care highlight the major steps in diagnosis and treatment of suspected patient. Detection: Rapid recognition of stroke Dispatch: Early activation of EMS by 911 Delivery: Rapid EMS ID, management, and transport. Door: Appropriate triage to stroke center Data: Rapid triage, evaluation, and management with in the ED Decision: Stroke expertise and therapy selection Drug: Fibrinolytic therapy, intra-arterial strategies Disposition: Rapid admission to the stroke unit 5
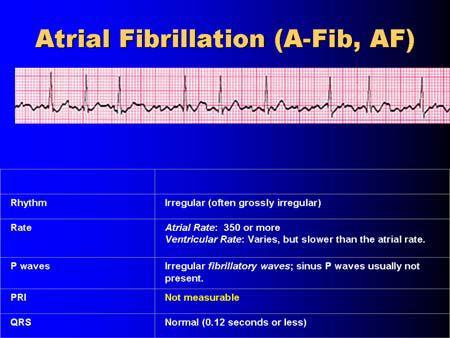
6 BRADYCARDIA Algorithm: Bradycardia Remember: All Trained Dogs Eat: Atropine 0.5 mg IVP for Sinus Bradycardia & 1, 2 Type I AV Block. Transcutaneous Pacing (preferred for 2 Type II and 3 HB); do not delay pacing in symptomatic patients (even those in Sinus Brady or lowdegree heart blocks) Dopamine 5-10 mcg/kg/min (if patient unresponsive to atropine/pacing) Epinephrine drip 2 to 10 mcg/min (if patient unresponsive to atropine/pacing) Note: Atropine is not indicated for 2 Type II & 3 heart blocks proceed directly to pacing if the patient is symptomatic, although Atropine can be considered if pacing is delayed TACHYCARDIA Algorithm: Tachycardia With Pulses Remember: If the patient is unstable, go directly to synchronized cardioversion. Otherwise: For Regular Narrow Complex Tachycardia (probable SVT) Obtain 12-lead ECG; consider expert consultation. Attempt vagal maneuvers. Adenosine 6 mg rapid IV push. If no conversion, give up to two more doses at 12 mg each. For Irregular Narrow Complex Tachycardia (probable A-Fib) Obtain 12-lead ECG; consider expert consultation. Control rate with Diltiazem or β-blockers. For Regular Wide Complex Tachycardia (probable V-Tach) Obtain 12-lead ECG; consider expert consultation. Adenosine 6 mg rapid IV push. If no conversion, give up to two more doses at 12 mg each. Convert rhythm using Amiodarone 150 mg over 10 minutes. Elective cardioversion. 6
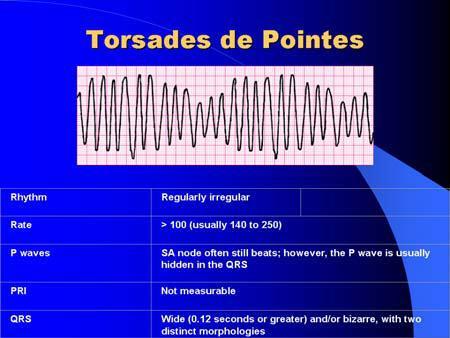
7 For Irregular Wide Complex Tachycardia Obtain 12-lead ECG; consider expert consultation. Consider antiarrhythmics. If Torsades de pointes, give Magnesium Sulfate 1 to 2 g over 5-60 minutes. VENTRICULAR FIBRILLATION / PULSELESS VENTRICULAR TACHYCARDIA Algorithm: Pulseless Arrest Shockable Remember: Good ACLS starts with good BLS: CPR start immediately. (C-A-B) Push hard and push fast. Shock analyze rhythm, and shock if in VF/pulseless VT. CPR resume CPR immediately after shock delivery. Continue for 5 cycles / 2 minutes. Vasopressor or Epi 1 mg q 3-5 min (can replace 1st or 2nd dose of Epi with 40 units Vasopressin).Give as soon as possible after resuming CPR, circulate with chest compressions. Shock analyze rhythm, and shock if in VF/pulseless VT. CPR resume CPR immediately after shock delivery. Continue for 5 cycles / 2 minutes. Antiarrhythmic Amiodarone 300 mg IV/IO or Lidocaine mg/kg up to 3 mg/kg. Give as soon as possible after resuming CPR, circulate with chest compressions. Shock analyze rhythm, and shock if in VF/pulseless VT. CPR resume CPR immediately after shock delivery. Continue for 5 cycles / 2 minutes. Note: Minimize interruptions to chest compressions do not check a pulse or evaluate the heart rhythm after a shock. After each shock, resume CPR immediately and continue for 5 cycles prior to rhythm analysis and possible pulse check. After a second dose of Epinephrine, a second antiarrhythmic dose (Amiodarone 150 mg or Lidocaine mg/kg) may given after the next rhythm check. 7
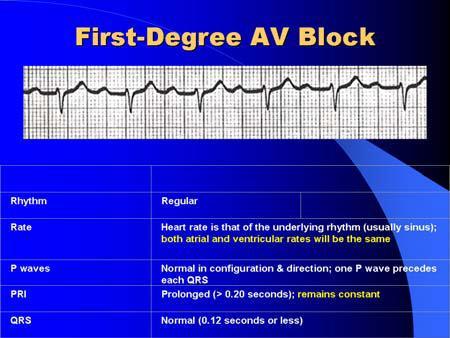
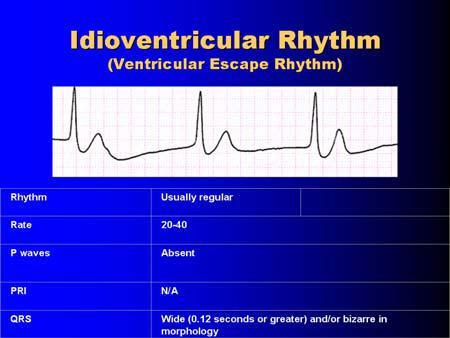
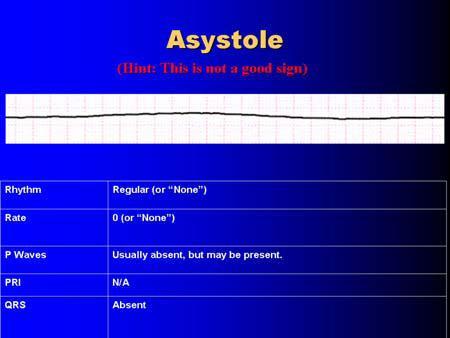
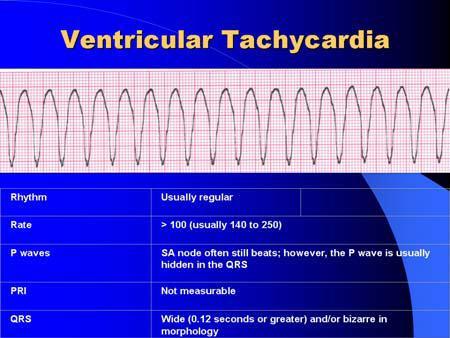
8 PULSELESS ELECTRICAL ACTIVITY Algorithm: Pulseless Arrest Not Shockable Remember: PEA: Possible causes (consider the 6 H s and 5 T s). Epinephrine 1 mg q 3-5 min (can replace 1st or 2nd dose of Epi with 40 units Vasopressin). Give as soon as possible after resuming CPR, circulate with chest compressions. Note: In PEA, the electrical system of the heart is functioning, but there is a problem with the pump, pipes, or volume a mechanical part of the system is not working. You can use the 5 H s and 5 T s to remember the most common reversible causes of PEA: Hypovolemia Hypoxia Hypo-/Hyperkalemia Hypothermia Hydrogen Ion (acidosis) Tamponade, cardiac Toxins Thrombosis coronary Tension Pneumothorax Thrombosis pulmonary ASYSTOLE Algorithm: Pulseless Arrest Not Shockable Remember: DEAD: Determine whether to initiate resuscitation. Epinephrine 1 mg q 3-5 min (can replace 1st or 2nd dose of Epi with 40 units Vasopressin). Give as soon as possible after resuming CPR, circulate with chest compressions. Differential Diagnosis or Discontinue resuscitation Are they still dead? Consider the 5 H s and 5 T s (see above) EKG and Electrical Therapy Review The EKG tracing represents electrical activity through the heart. The P wave represents depolarization of the atria; the QRS complex represents depolarization of the ventricles; and the T wave represents the latter stage of repolarization of the ventricles. The interval from the first deflection of the P wave to the beginning of the QRS complex is the P-R Interval (PRI), and should be between 0.12 and 0.20 seconds. A normal QRS complex has duration of
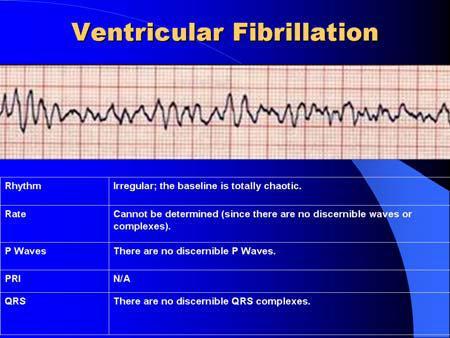
9 seconds or less; a longer duration (wide QRS) indicates delayed conduction through the ventricles, often as the result of a ventricular pacemaker focus. The horizontal axis of the EKG strip measures time. Each large box represents 0.20 seconds; each small box represents 0.04 seconds. To obtain a 3-lead EKG tracing, place the white (RA) electrode on the right chest just below the clavicle; the black electrode (LA) on the left chest just below the clavicle; and the Red electrode (LL) laterally on the lower left abdomen. Pacer pads go in the anterior/posterior positions. Defibrillation pads go on the upper right chest and lower left abdomen, although on children and other small patients the pads may need to be placed in the middle of the anterior and posterior chests. Rhythm Disturbances Treat the patient, not the dysrhythmia. Always assess your patient for pulses, perfusion, and level of consciousness Is the patient Stable, Unstable, or Pulseless? Next, assess the rhythm: Is it fast or slow? Is it life-threatening? As you treat the patient, try to discover the cause of the dysrhythmia for many patients, their only chance of survival is if you can identify and treat a reversible cause. There are many possible causes of rhythm disturbances or PEA. Common causes include sympathetic stimulation, stress, hypoxia, ischemia, drugs/toxins, and electrolyte disturbances. Although lab draws can be useful, a history of the patient and the current event obtained from a family member or caregiver is often more useful Defibrillation (Unsynchronized Shock) Fibrillation is a disorganized rhythm that, if present in the ventricles, is lifethreatening. Immediate CPR combined with early defibrillation is critical to survival from sudden cardiac arrest. Defibrillation terminates all electrical activity in the pulseless heart in the hopes that it will resume beating in a coordinated fashion. A shock should be delivered about once every 2 minutes if the patient remains in Ventricular Fibrillation. With a monophasic monitor, the recommendation is to deliver a single shock at 360 Joules. If a biphasic monitor is used, the recommended dosage is machine-dependent, and should appear on the front of the monitor. If optimal shock dosage is not known, the consensus is to defibrillate at 200 J. 9
10 Synchronized Cardioversion Synchronized cardioversion is the preferred treatment for unstable patients with a tachycardia such as Atrial Fibrillation, V-Tach with a pulse, or Supraventricular Tachycardia (SVT). The shock is timed by the monitor to be delivered in coordination with the QRS complex of the heart. If the patient is conscious, consider sedation prior to cardioversion; however, synchronized cardioversion should not be delayed while waiting for sedation in severely symptomatic patients. With a Monophasic monitor, the initial shock is delivered at 100 J; if the rhythm does not terminate, deliver additional shocks in stepwise fashion (200J, 300J, and 360J for subsequent shocks). With a Biphasic monitor, dosage and steps are device-dependent; if optimal doses are unknown, begin at 100 J and step up from there. Transcutaneous Pacing (TCP) External cardiac pacing is the recommended treatment for symptomatic bradycardias. If the patient is conscious, consider sedation; however, pacing should not be delayed while waiting for sedation. Begin pacing at zero milliamps, slowly increasing until capture is achieved. Then, set the rate at 20 beats per minute above the monitored heart rate, with a minimum rate of 50 bpm. Terminating Resuscitative Efforts In Hospital termination, the decision to terminate efforts will always rest with the treating physician in the hospital. In hospital setting if the rescuers cannot rapidly ID the reversible cause (H,T s) and the patients fails to respond to BLS and ACLS interventions termination efforts should be considered. Out of Hospital termination, has a different criteria needed to be meat by the rescuer. The returned of ROSC, reliable evidence of irreversible death (rigor mortis, brain matter or blood pooling present on the victim), a valid DNAR document at the scene, and if the rescuer cannot continue due to physical restrictions or an unsafe environment. EMS can also consider terminating resuscitative efforts after consulting with control. 10

11 Therapeutic Hypothermia Hypothermia is the only intervention proven to aid in the neurologic recovery in a patient with ROSC. The patient placed in hypothermia should be kept in this condition any were from 12Hr to 24Hr and the temperature can range from 32 C to 34 C. A contraindication for this treatment is if the patient is able to follow verbal commands. The core temperature should be closely monitored by the healthcare provider. Hypothermia can be used in conjunction with PCI without any adverse effects. Waveform Capnography The new 2010 American Heart Association Guidelines now endorse wave form capnography as a recommendation for ET tube verification, monitoring CPR quality and a recommendation for detecting return of spontaneous circulation. It is reasonable to consider using quantitative waveform capnography in intubated patients to monitor CPR quality and optimized chest compressions (PETCO2 <10 mm Hg in intubated patients indicates that cardiac output is inadequate to achieve ROSC),If PETCO2 abruptly increases to a normal value (35 to 40 mm Hg), it is reasonable to consider that this is an indicator of ROSC. A capnograph provides a picture of the patients cardio-respiratory system in the form of the CO 2 waveform which provides clinicians invaluable information. Viewing a numerical End Tidal CO 2 value 11

12 without the waveform is analogous to viewing the heart rate without the ECG trace. 12

13 13
14 14
15 15
16 16

17 17
18 18
19 19
20 20
21 ACLS Medications Review This information on medications meets the standard set by the 2010 American Heart Association for Advanced Cardiac Life Support. It does not supersede local protocols or medical control; consult with your medical director for the most upto-date guidelines on medication administration where you work. IV/IO medications should be administered in a peripheral line during CPR, as soon as possible after a rhythm check. It is recommended that you flush with 20 ml of fluid after each drug administration and elevate the extremity. Always use large bore catheters if possible. A Note on Endotracheal Administration of Medications: This route of medication administration is being de-emphasized by the AHA the IV or IO routes are preferred. However, the ET route can still be used if providers are unable to gain access by IV/IO. Use the mnemonic NAVEL to remember which drugs can be administered via this route: Narcan Atropine Vasopressin Epinephrine Lidocaine. If using the ET route, the drug dosage must be increased, typically times the IV/IO bolus dosage (although there is no consensus on Epinephrine or Vasopressin dosing via this route), followed by a 10 ml normal saline flush. ADENOSINE Class: Indicated for: IV Bolus Dosage (no IO): Endogenous nucleoside PSVT / Regular Narrow- 6 mg rapid IV push 1st dose; complex Tachycardia 12 mg rapid IV push 2nd dose 12 mg rapid IV push 3rd dose Notes: Doses are followed by a saline flush. Two subsequent doses of 12 mg each may be administered at 1 2 minute intervals. Use the port closest to cannulation. The AHA recommends that the dose be cut by half if administering through a central line, or in the presence of Dipyridamole or Carbamazepine. Larger doses may be required in the presence of caffeine or Theophylline. AMIODARONE Class: Indicated for: IV-IO Bolus Dosage: Antiarrhythmic V-Fib / Pulseless V-Tach 300 mg 1st dose; 150 mg 2nd dose Arrhythmias 360 mg over 6 hours (slow) 150 mg over 10 minutes (rapid) Infusion dose 540 mg IV/IO over 18 hours (.5 mg/min) Notes: Cumulative doses >2.2 g/24 hours are associated with significant hypotension. Do not administer with other drugs that prolong QT interval (i.e., Procainimide). Terminal elimination is extremely long half life lasts up to 40 days. During arrest, IV bolus should be delivered slowly, over 1 3 minutes. 21
22 ASPIRIN Class: Indicated for: PO Dosage (no IV-IO): NSAID (Non-Steroidal Chest pain / ACS 160 mg 325 mg Anti-Inflammatory Drug) Suppository Dose: 300 mg Notes: In suspected ACS, Aspirin can block platelet aggregation and arterial constriction. Also helps with pain control. May cause or exacerbate GI bleeding. ATROPINE Class: Indicated for: IV-IO Bolus Dosage: Parasympathetic Blocker Bradycardia 0.5 mg every 3-5 minutes as needed Notes: Used only in symptomatic bradycardia with heart rate < 60. (Not indicated in Second Degree Type II or Third Degree heart block.) Doses < 0.5 mg may result in paradoxical slowing of the heart. ET route discouraged, but can be used if IV/IO access not available. DEXTROSE/GLUCOSE Class: Indicated for: IV-IO Bolus Dosage: Carbohydrate Hypoglycemia 25 g (50 ml) of D50W Notes: Used to reverse documented hypoglycemia in patients with symptomatic bradycardia or during cardiac arrest. Should not be used routinely during cardiac arrest. DILTIAZEM Class: Indicated for: IV Dosage: Calcium Channel Blocker A-Fib / A-Flutter mg over 2 minutes Notes: May cause hypotension. Do not use in wide-qrs tachycardias of uncertain origin. DOPAMINE Class: Indicated for: IV Infusion: Catecholamine Symptomatic Bradycardia 2-10 μg/kg/min cardiac dose Hypotension μg/kg/min vasopressor dose Notes: Titrate to patient response. Correct hypovolemia with volume replacement before initiating Dopamine. May cause tachyarrhythmias. Do not mix with Sodium Bicarbonate. 22
23 EPINEPHRINE Class: Indicated for: IV-IO Bolus Dosage: Catecholamine Pulseless Arrest 1 mg (1:10,000) every 3-5 minutes Symptomatic Bradycardia Infusion: 1 mg in 500ml of D5W or NaCl at 1 μg/min titrated to effect. Notes: First line drug in all pulseless rhythms. Increases myocardial oxygen demand, and may cause myocardial ischemia or angina. ET route is discouraged, but if used give mg of a 1:1000 solution diluted in 10 ml normal saline. FLUID ADMINISTRATION (e.g., Normal Saline / NaCl) Class: Indicated for: IV/IO Bolus Dosage: Fluid Volume Hypovolemia cc bolus (repeat as needed) Notes: Use to treat specific reversible causes, such as hypovolemia. Routine administration of fluids during a resuscitation is not indicated, as it can reduce coronary perfusion pressure. HEPARIN (Unfractionated) Class: Indicated for: IV/IO Bolus Dosage: Anticoagulant STEMI (AMI) Initial Dose: 60 IU/kg (max IU) Infusion: 12 IU/kg/hr (max IU/hr) Notes: Do not use in patients with active bleeding or bleeding disorders; severe hypertension; or recent surgery. Monitor aptt and platelet count while administering. LIDOCAINE Class: Indicated for: IV / IO Bolus Dosage: Antiarrhythmic V-Fib/Pulseless V-Tach mg/kg (1st dose) Stable V-Tach Infusion: 1-4 mg/min (30-50 μg/kg/min) Notes: May repeat at mg/kg every 5-10 minutes to a max. dose of 3 mg/kg. Use with caution in presence of impaired liver; discontinue if signs of toxicity develop. Prophylactic usein AMI is contraindicated. ET route discouraged, but can be used if IV/IO access not available. MAGNESIUM SULFATE Class: Indicated for: IV/IO Bolus Dosage: Electrolyte Torsades de pointes or 1-2 g in 10 ml D5W over 5-20 minutes Hypomagnesemia Notes: A fall in blood pressure may be noted with rapid administration. Dose is given over 5-20 minutes during cardiac arrest, 5-60 minutes in living patients. Use with caution in renal failure. 23
24 MORPHINE SULFATE Class: Indicated for: IV/IO Bolus Dosage: Opiate / Analgesic Chest pain 2-4 mg every 5-30 minutes Pulmonary edema Notes: Administer slowly and titrate to effect; may cause hypotension. May cause respiratory depression be prepared to support ventilations. Naloxone is the reversal agent. NALOXONE HYDROCHLORIDE (NARCAN) Class: Indicated for: IV/IO Bolus Dosage: Opiate Antagonist Narcotic overdose mg (up to 10 mg in 10 min.) Notes: Monitor for recurrence of respiratory depression. May cause opiate withdrawal. ET route discouraged, but can be used if IV/IO access not available. NITROGLYCERIN Class: Indicated for: IV Bolus Dosage: Vasodilator Chest pain/acs μg in D5W or NaCl Sublingual Dose: mg Notes: Most commonly given sublingually as tablet or spray repeat up to 3 doses at 5 minute intervals. Hypotension may occur. Do not use with Viagra (Question Females as well as Males) or other phosphodiasteraseinhibitors; with severe bradycardia or tachycardia; or in presence of RV infarction or inferior MI. Do not mix with other drugs. OXYGEN Class: Indicated for: Flow Rate: Atmospheric Gas Any cardiopulmonary Stable Patient: 2-6 lpm via NC emergency Unstable Patient: lpm via NRB Suspected stroke Notes: Pulse oximetry provides a useful method of titrating oxygen administration; however, it may be inaccurate in low cardiac output states or in patients with specific toxicities (such ascarbon Monoxide exposure). SODIUM BICARBONATE Class: Indicated for: IV Bolus Dosage: Buffer Acidosis, hyperkalemia 1 meq/kg Notes: Not recommended for routine use in cardiac arrest patients. If available, use arterial blood gas analysis to guide bicarbonate therapy. 24
25 VASOPRESSIN Class: Indicated for: IV - IO Bolus Dosage: Hormone Pulseless arrest 40 U IV - IO Notes: Only given one time to replace the first or second dose of Epinephrine; Epinephrine dosing can continue 3 to 5 minutes after Vasopressin is administered. Vasopressin should not replace antiarrhythmics (such as Amiodarone). May cause cardiac ischemia and angina. Not recommended for responsive patients with coronary artery disease. ET route discouraged, but can be used if IV/IO access not available. VERAPAMIL Class: Indicated for: IV Bolus Dosage: Calcium Channel Blocker A-Fib/A-Flutter, PSVT mg over 2-5 minutes Notes: Alternative drug after Adenosine to terminate PSVT with adequate blood pressure and preserved LV function. Can cause peripheral vasodilation and hypotension. Use with extreme caution in patients receiving oral β-blockers. 25
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Advanced Cardiac Life Support ACLS
 Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Michigan Adult Cardiac Protocols TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket
 BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
BLS BASICS: Scene Safety First always first, your safety is above everything else, hands only CPR (use pocket facemask or AMBU bag) Adults call it in, start CPR, get AED Child CPR First, Phone call second
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
ADULT TREATMENT GUIDELINES
 A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
Shifts 28, 29, 30 Quizzes
 Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Shifts 28, 29, 30 Quizzes Name: Score: Date: 1. You are on the scene of a 4 year old in cardiac arrest. CPR is initiated and an E.T. tube has been placed, an I.V. has been established. What is the correct
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
 Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University
 Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation
Utah EMS Protocol Guidelines: Cardiac
 Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
ADULT CARDIAC EMERGENCIES
 ADULT CARDIAC EMERGENCIES Last Revised: September 2018 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate
ADULT CARDIAC EMERGENCIES Last Revised: September 2018 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Chain of Survival. Highlights of 2010 American Heart Guidelines CPR
 Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION
 RECERTIFICATION EXAMINATION") ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
Advanced Cardiac Life Support G 2010
 Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
ADULT CARDIAC EMERGENCIES
 ADULT CARDIAC EMERGENCIES Last Revised: July 2017 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate of
ADULT CARDIAC EMERGENCIES Last Revised: July 2017 Cardiac Emergencies Section A 1 CARDIOPULMONARY ARREST NOTE: High quality CPR includes: 1. Chest Compressions at a depth of at least 2 inches 2. Rate of
Pediatric Resuscitation
 Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Pediatric Resuscitation Section 24 Pediatric Cardiac Arrest Protocol The successful resuscitation of a child in cardiac arrest is dependent of a systematic approach of initiating life-saving CPR, recognition
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
ACLS. Advanced Cardiac Life Support Practice Test Questions. 1. The following is included in the ACLS Survey?
 1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
ACLS Emergency Cardiac Drug Therapy (bolded = changes based on 2005 AHA ACLS Guidelines) revised 01/18/07
 revised 01/18/07") Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Johnson County Emergency Medical Services Page 23
 Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
Non-resuscitation Situations: Resuscitation should not be initiated in the following situations: Prolonged arrest as evidenced by lividity in dependent parts, rigor mortis, tissue decomposition, or generalized
table of contents adult treatment guidelines
 table of contents adult treatment guidelines A1 ADULT PATIENT CARE... 3 A2 CHEST PAIN SUSPECTED ACUTE CORONARY SYNDROME/STEMI...4 5 A3 CARDIAC ARREST INITIAL CARE AND CPR...6 7 A4 VENTRICULAR FIBRILLATION
table of contents adult treatment guidelines A1 ADULT PATIENT CARE... 3 A2 CHEST PAIN SUSPECTED ACUTE CORONARY SYNDROME/STEMI...4 5 A3 CARDIAC ARREST INITIAL CARE AND CPR...6 7 A4 VENTRICULAR FIBRILLATION
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Asystole / PEA (PEDIATRIC)
") FRRCKSBURG MS Asystole / A (ATRC) 1 Check for Responsiveness Check for Breathing Check for Carotid ulse nitiate CR o As soon as a mechanical external compression device (i.e. Lucas 2) (rocedure 11) becomes
FRRCKSBURG MS Asystole / A (ATRC) 1 Check for Responsiveness Check for Breathing Check for Carotid ulse nitiate CR o As soon as a mechanical external compression device (i.e. Lucas 2) (rocedure 11) becomes
ACLS: 2015 Update. What s new? Or:
 ACLS: 2015 Update Or: What s new? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery CME Faculty Disclosure Dr. Shulman has no affiliation
ACLS: 2015 Update Or: What s new? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery CME Faculty Disclosure Dr. Shulman has no affiliation
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
HigHligHts of the 2018 Focused In 2015 Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life
 Highlights of the 2018 Focused Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life Support and Pediatric Advanced Life Support - Heart and Stroke Foundation
Highlights of the 2018 Focused Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life Support and Pediatric Advanced Life Support - Heart and Stroke Foundation
JUST SAY NO TO DRUGS?
 JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
CARDIAC ARREST GENERAL CONSIDERATION
 CARDIAC ARREST GENERAL CONSIDERATION A. Age delineation: Infant CPR guidelines apply to victims less than one year of age; Child CPR guidelines apply to victims one year of age to the onset of adolescence
CARDIAC ARREST GENERAL CONSIDERATION A. Age delineation: Infant CPR guidelines apply to victims less than one year of age; Child CPR guidelines apply to victims one year of age to the onset of adolescence
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES Page 1 Chapter 3 ACLS AND SPECIAL SITUATIONS CHAPTER The International Liaison Committee on Resuscitation (ILCOR)
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES Page 1 Chapter 3 ACLS AND SPECIAL SITUATIONS CHAPTER The International Liaison Committee on Resuscitation (ILCOR)
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
table of contents pediatric treatment guidelines
 table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
table of contents pediatric treatment guidelines P1 PEDIATRIC PATIENT CARE...70 P2 APPARENT LIFE-THREATENING EVENT (ALTE)...71 P3 CARDIAC ARREST INITIAL CARE AND CPR...72 73 P4 NEONATAL CARE AND RESUSCITATION...74
Simulation 15: 51 Year-Old Woman Undergoing Resuscitation
 Simulation 15: 51 Year-Old Woman Undergoing Resuscitation Flow Chart Flow Chart Opening Scenario Section 1 Type: DM Arrive after 5-6 min in-progress resuscitation 51 YO female; no pulse or BP, just received
Simulation 15: 51 Year-Old Woman Undergoing Resuscitation Flow Chart Flow Chart Opening Scenario Section 1 Type: DM Arrive after 5-6 min in-progress resuscitation 51 YO female; no pulse or BP, just received
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
Portage County EMS Patient Care Guidelines. Cardiac Arrest
 Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Portage County EMS Patient Care Guidelines Cardiac Arrest Note: These guidelines are based on (or adapted from) the current American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
2
 1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
ACLS: 2015 Update. Anything New?
 ACLS: 2015 Update Anything New? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery Copyright 2017 by Sea Courses Inc. All rights
ACLS: 2015 Update Anything New? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery Copyright 2017 by Sea Courses Inc. All rights
Prior to taking ACLS, it is assumed that you are proficient and currently certified in Basic Life
 Table of Contents Overview of Advanced Cardiovascular Life Support... 2 Updates to ACLS in 2015... 3 Chain of Survival... 4 Adult BLS Chain of Survival... 4 BLS and ACLS Surveys... 5 The BLS Survey...
Table of Contents Overview of Advanced Cardiovascular Life Support... 2 Updates to ACLS in 2015... 3 Chain of Survival... 4 Adult BLS Chain of Survival... 4 BLS and ACLS Surveys... 5 The BLS Survey...
Cardiology Part 2. Practice Test A
 Cardiology Part 2 Practice Test A The following practice exam is comprised of all multiple-choice questions. Select the response that MOST appropriately answers the question. The questions are designed
Cardiology Part 2 Practice Test A The following practice exam is comprised of all multiple-choice questions. Select the response that MOST appropriately answers the question. The questions are designed
Blanchard Valley Hospital Pharmacy Code Blue Overview
 Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
TABLE OF CONTENTS. Page 2 of 52
 Page 1 of 52 TABLE OF CONTENTS Table of Contents...2 List of Figures...4 List of Tables...4 Unit One: ACLS Overview...5 Preparing for ACLS...5 Organization of the ACLS Course...5 2015 ACLS Guideline Changes...6
Page 1 of 52 TABLE OF CONTENTS Table of Contents...2 List of Figures...4 List of Tables...4 Unit One: ACLS Overview...5 Preparing for ACLS...5 Organization of the ACLS Course...5 2015 ACLS Guideline Changes...6
Management Of Medical Emergencies. Zakaria S. Messieha, DDS
 Management Of Medical Emergencies Zakaria S. Messieha, DDS Z.S. Messieha Associate Professor, Anesthesiology University Of Illinois At Chicago Necessity Of Emergency Protocol Aging patient population.
Management Of Medical Emergencies Zakaria S. Messieha, DDS Z.S. Messieha Associate Professor, Anesthesiology University Of Illinois At Chicago Necessity Of Emergency Protocol Aging patient population.
ACLS.exam. Number: ACLS Passing Score: 800 Time Limit: 120 min File Version: ACLS. Advanced Cardiac Life Support
 ACLS.exam Number: ACLS Passing Score: 800 Time Limit: 120 min File Version: 1.0 ACLS Advanced Cardiac Life Support Version 1.0 Exam A QUESTION 1 What is the effect of atropine on vagal reflexes? Correct
ACLS.exam Number: ACLS Passing Score: 800 Time Limit: 120 min File Version: 1.0 ACLS Advanced Cardiac Life Support Version 1.0 Exam A QUESTION 1 What is the effect of atropine on vagal reflexes? Correct