Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy
|
|
|
- Frederica Townsend
- 6 years ago
- Views:
Transcription
1 Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System 01/06/2017 1
2 Objectives Provide an overview of the epidemiology, etiology, and pathophysiology of CAD Briefly review the evidence for benefit of aspirin therapy for patients with stable CAD Analyze the literature in order to provide a clinical recommendation on the use of aspirin + DOAC combination therapy for AF patients post MI/TIA with stable CAD 2
3 Abbreviations ACCP American College of Chest Physicians AF atrial fibrillation APT antiplatelet therapy ASA acetylsalicylic acid OR aspirin AWP average wholesale price BID twice daily administration CABG Coronary artery bypass graft CAD coronary artery disease CHD coronary heart disease CI confidence interval CRNM clinically relevant nonmajor DE drug exposure DOAC direct oral anticoagulant HDER higher dose edoxaban regimen HR hazard ratio INR international normalized ratio LDER lower dose edoxaban regimen MI myocardial infarction PCI percutaneous coronary intervention RCT randomized controlled trial SAPT single antiplatelet therapy SEE systemic embolic event SSE stroke and systemic embolism TIA transient ischemic attack VKAs vitamin K antagonists 3
4 CAD Epidemiology, Etiology, and Pathophysiology 4
5 CAD Definition One or more of the following Stable angina pectoris History of unstable angina pectoris History of PCI CABG Previous MI Stable disease 12 months since event 5 CHEST 2012; 141(2)(Suppl):e637S e668s
6 Epidemiology Major cause of death and disability in developed countries Responsible for 1/3 or more of all deaths in people over 35 years old The Global Burden of Disease Study in 2013 Estimated that deaths related to cardiovascular disease has increased 41% since
7 CAD in the US CAD in Middle aged Men CAD in Middle aged Women ~50% ~33% 7
8 CAD and AF On average, 30% of patients with AF have concomitant CAD 10 15% of patients with stable CAD have an indication for long term oral anticoagulation Little is known about AF prognosis in stable CAD outpatients AF + CHADS2 score of 3: 4.6% annual risk of stroke Schurtz G, Bauters C, Ducrocq G, et al. Panminerva Medica 2016 December;58(4):
9 Audience Response Question Which of the following is NOT a risk factor for CAD? 1. Hypertension 2. Depression 3. Obesity 4. Diabetes 5. All of the above are risk factors for CAD 9
10 Risk Factors Non Modifiable Increasing Age: Men >45yrs Post menopausal Women Male Sex Family History Race African Americans Mexican Americans American Indians Hawaiian Asian Americans Modifiable Hyperlipidemia Low HDL High LDL High Triglycerides Tobacco Smoke Hypertension Physical Inactivity Overweight / Obesity Diabetes Mellitus Excessive Alcohol Depression / Stress 10
11 Bleeding Risk Clinical characteristic* Points Hypertension (ie, uncontrolled blood H pressure) 1 Abnormal renal and liver function (1 point A each) 1 or 2 S Stroke 1 B Bleeding tendency or predisposition 1 L Labile INRs (for patients taking warfarin) 1 E Elderly (age greater than 65 years) 1 Drugs (concomitant aspirin or NSAIDs) or D excess alcohol use (1 point each) 1 or 2 HAS BLED Score Total Bleeds per 100 patientyears to 9 Insufficient data Other contributing factors Anemia Hx of GI bleed Recent bleed Diabetes mellitus Inherited disorders 11

12 Etiology 12 Image from:

13 Etiology 13 Image from:

14 Etiology 14 Image from:

15 Etiology 15 Image from:

16 Etiology 16 Image from:

17 Pathophysiology Rupture of the vulnerable plaque Complex inflammatory and coagulation cascade Image from: 1 Illustration of the blood clotting process showing the four mainsteps of.png 17

18 Primary Hemostasis Clopidogrel Prasugrel Ticlopidine (irreversible) Ticagrelor (reversible) Aspirin Image from: 1 Illustration of the blood clotting process showing the four mainsteps of.png 18
19 Clotting Cascade Kininogen Kallikrein Trauma Trauma 19 Cross linked Fibrin Clot
20 Clotting Cascade Kininogen Kallikrein Trauma Warfarin Warfarin Rivaroxaban Apixaban Edoxaban Dabigatran Trauma 20 Cross linked Fibrin Clot
21 ASPIRIN FOR SECONDARY PREVENTION OF CAD Per ACCP Guidelines 21

22 CHEST Guideline Evidence Aspirin Table 3 22
23 The number of vascular events and total deaths prevented is far greater than the number of bleeding events that resulted from aspirin. 23


24 CHEST Guideline Evidence Clopidogrel Table 4 24
25 After a mean follow up of 1.9 years, clopidogrel was associated with a possible reduction in nonfatal MI and nonfatal extracranial bleeding and little or no effect on total mortality. 25
26 CHEST Guidelines Recommendation Long term single APT with aspirin (75 100mg) OR clopidogrel 75mg daily for patients with stable CAD Considering difference in cost and mortality benefits, many patients are placed on daily aspirin 81mg Clopidogrel reasonable alternative for patients with ASA allergy ASA 81mg, EC CLOPIDOGREL 75mg AWP (120 tabs) $6.40 (90 tabs) $ VA price (120 tabs) $0.60 (90 tabs) $
27 DOACS AND ASPIRIN Evaluating Their Role in Patients with Both AF and CAD 27
28 CHEST Guidelines on DOACs and ASA Mostly discusses ASA + VKAs RE LY trial Rates of major bleeding were roughly 2x higher for patients receiving aspirin in conjunction with either warfarin (INR 2 3) or dabigatran Recommendation For patients with AF and stable CAD who choose oral anticoagulation, we suggest VKA therapy alone (INR 2 3) rather than combination of VKA therapy and aspirin. 28
29 Trials Evaluating DOACs and Antiplatelet Use Apixaban ARISTOTLE Dabigatran RE LY Edoxaban ENGAGE Rivaroxaban ROCKET AF 29
30 Apixaban vs. Warfarin with Concomitant Aspirin in Patients with Atrial Fibrillation: Insights from the ARISTOTLE Trial Alexander JH, et al. Eur Heart J. 2014;35(4):
31 Insights from the ARISTOTLE Trial Objectives Describe the use over time and dose of concomitant aspirin in patients with AF overall and in the subgroups of patients with and without arterial vascular disease Evaluate the efficacy and safety of apixaban compared with warfarin in patients receiving and not receiving aspirin overall and in the subgroups of patients with and without arterial vascular disease 31
32 Insights from the ARISTOTLE Trial Design Treatment Groups Double blind, double dummy RCT of patients with AF and at least one additional risk factor for stroke or systemic embolism >=75yrs, HTN, diabetes, HF, or reduced ventricular systolic function, and prior stroke or systemic embolism Apixaban 5mg BID + warfarin placebo (N=9120) Dose adjusted to 2.5mg BID where appropriate Apixaban placebo + warfarin (N=9081) with INR of 2 3 Defined as those using aspirin on Day 1 Considered to be taking aspirin in a particular week if they received aspirin for at least 50% of the days of the week Aspirin Users 32
33 Subgroup Breakdown ASA added No ASA Apixaban Warfarin N= 2233 N= 2201 N= 6852 N=
34 Baseline Characteristics Baseline Characteristics Aspirin Users (n=4434) Non user (n=13699) P value Age, median (25th, 75th) 70 (64,76) 70 (62,75) Male Sex (%) 3029 (68.3) 8709 (63.6) < Diabetes (%) 1282 (28.9) 3249 (23.7) < HTN (%) 3940 (88.9) (87.0) Hx of CAD (%) 2264 (51.1) 4354 (31.8) < Hx of MI (%) 1046 (23.6) 1529 (11.2) < Hx of PCI (%) 744 (16.8) 903 (6.6) < >12 months from most recent PCI 618 (83.4) 706 (78.5) Proportion with Stent Placed (%) 518 (70.7) 562 (63.4) Hx of CABG (%) 582 (13.1) 620 (4.5) < Hx of Stroke (%) 501 (11.3) 1624 (11.9) CHADS2 Score (31.4) 4763 (34.8) (36.4) 4882 (35.6) < (32.2) 4054 (29.2) Aspirin users were more likely to be male, have diabetes, HTN, have a Hx of CAD, MI, PCI, CABG and have higher CHADS2 scores 34
35 Results Reduction in Ischemic Events: Apixaban vs. Warfarin Stroke or Systemic Embolism ASA Status HR CI ASA without ASA Interaction P value Ischemic Stroke ASA without ASA MI ASA without ASA Death ASA without ASA Patients on ASA had statistically significant improvements in SSE 35
36 Results (cont.) Reductions in Bleeding: Apixaban vs. Warfarin Major Bleeding Hemorrhagic Stroke Major or CRNM Bleeding Any Bleeding ASA Status HR CI ASA without ASA ASA without ASA ASA without ASA ASA without ASA Statistically Significant Interaction P value Compared to non users, ASA users had similar rates of bleeding 36
37 Authors Conclusions If there is a strong indication for combination aspirin and oral anticoagulation, apixaban seems to be safer than warfarin in patients with AF irrespective of ASA use In ARISTOTLE, concomitant aspirin was used in 20 25% of patients with AF treated with an anticoagulant (apixaban or warfarin) and was associated with a higher risk of bleeding 37
38 Authors Conclusions (cont.) Similar effects of apixaban, compared with warfarin, on stroke or systemic embolism, major bleeding, or mortality irrespective of concomitant aspirin use Adequately powered RCT are needed to better define optimal antithrombotic regimen and its duration in patients with both AF and atherosclerotic CAD, especially those with ACS or recent stenting 38
39 Critical Appraisal Strengths One of very few trials looking at the effects of concomitant aspirin and DOAC use Large sample size Conclusions matched data presented Clinically useful Limitations Patients receiving ASA were different, with higher risk for both ischemic and bleeding events Though adjustments for confounders were made, more likely exist Aspirin use was not blinded Subgroup analysis limited power Generalizability Bristol Myers Squibb and Pfizer participated in trial design and data collection Conclusion: Apixaban + ASA still carries improved bleeding risk over warfarin +/ ASA and may have benefits on SSE 39
40 Concomitant Use of Antiplatelet Therapy with Dabigatran or Warfarin in the Randomized Evaluation of Long Term Anticoagulation Therapy (RE LY) Trial Dans AL, et al. Circulation. 2013;127(5):
41 Insights from the RE LY Trial Objective Determine the efficacy and safety of two doses of dabigatran versus warfarin in relation to whether concomitant antiplatelet treatment was used during the RE LY study 41
42 Insights from the RE LY Trial Design Treatment Groups Antiplatelet Users 18,113 patients with AF and additional risk factors for stroke recruited to receive one of two blinded doses of dabigatran (110mg BID or 150mg BID) or open label warfarin (INR 2 3) Main efficacy outcome = stroke or systemic embolism Safety outcome = major bleeding Dabigatran 110mg BID Dabigatran 150mg BID Warfarin (INR2 3) +/ antiplatelet agent Use of anti platelet agents was allowed at the discretion of the attending physicians and recorded at every visit Aspirin or clopidogrel 42
43 Subgroup Breakdown Antiplatelet Therapy No Antiplatelet Agent Dabigatran 110mg BID Dabigatran 150mg BID Warfarin (INR 2 3) N=2322 N=2304 N=2326 N=3693 N=3772 N=
44 Antiplatelet Use Only 27% of patients were on concomitant antiplatelet therapy at any one time during the study ASA Dose N % <100mg % Antiplatelet Use in RE LY No APT 62% Aspirin 32% Clopidogrel 2% mg % 300mg % Both Aspirin and Clopidogrel 4% 44
45 Baseline Characteristics ASA users and non users were seemingly well balanced. No p values provided for statistically significant differences 45
46 Results }Benefits attenuated with ASA use 46
47 Results (cont.) CHEST: Rates of major bleeding were roughly 2x higher for patients receiving aspirin in conjunction with either warfarin (INR 2 3) or dabigatran 47
48 Authors Conclusions Concomitant antiplatelet drugs appeared to increase the risk for major bleeding in RE LY without affecting the advantages of dabigatran over warfarin Dabigatran 150mg BID reduced the primary outcome of stroke and systemic embolism compared to warfarin However, this effect seemed attenuated among patients who used anti platelets (HR 0.80, 95% CI ) in comparison to those who did not (HR 0.52, 95% CI ) 48
49 Critical Appraisal Strengths One of very few trials looking at the effects of concomitant aspirin and DOAC use Large sample size Conclusions matched data presented Aspirin doses defined Mean duration of use was 66% of total study duration similar to real adherence rates Limitations Patients receiving APT were different, with higher risk for both ischemic and bleeding events Though adjustments for confounders were made, more likely exist Aspirin and Clopidogrel used, not randomized Only 16% of Aspirin users used 81mg Subgroup analysis limited power Generalizability Conclusion: Dabigatran + ASA increases major bleeding risk similar to warfarin + ASA but may NOT exhibit benefits on SSE 49
50 Concomitant Use of Single Antiplatelet Therapy with Edoxaban or Warfarin in Patients With Atrial Fibrillation: Analysis From the ENGAGE AF TIMI48 Trial Xu H, Ruff CT, Giugliano RP, et al. J Am Heart Assoc. 2016;5(2) 50
51 Insights from the ENGAGE Trial Objective Study the concomitant use of SAPT on the efficacy and safety of the anti Xa agent edoxaban in patients with atrial fibrillation 51
52 Insights from the ENGAGE trial Design Treatment Groups Antiplatelet Users Multinational, double blind, RCT comparing two dosing regimens of edoxaban with warfarin 21,105 patients with AF and a CHADS2 score 2 enrolled Exclusion Criteria: CrCl <30 ml/min, high bleeding risk, receiving or anticipated DAPT, Hx of stroke, ACS or coronary revascularization within 30 days of randomization Primary efficacy endpoint: SSE Primary safety endpoint: major bleeding Net clinical outcome: composite of SSE, all cause death, or major bleeding HDER: Edoxaban 60mg/day Edoxaban 30mg/day, if expected increased DE LDER: Edoxaban 30mg/day Edoxaban 15mg/day, if expected increased DE Warfarin (INR2 3) +/ ASA beginning 3 months after randomization Physician discretion Aspirin 100mg daily strongly encouraged Clopidogrel used in small subset of patients 52
53 Subgroup Breakdown Antiplatelet Therapy at 3 Months No Antiplatelet Agent at 3 Months HDER LDER Warfarin (INR 2 3) N=1642 N=1625 N=1645 N=4953 N=5046 N=
54 Antiplatelet Use 24.6% of patients were on concomitant antiplatelet therapy during the study, after the 3 month point 25% of patients on APT at randomization discontinued within 3 months 1196 subjects with death/sse/major bleed prior to 3 months OR missing APT data at 3 months were excluded No APT 75% Antiplatelet Use in ENGAGE Aspirin 23% Clopidogrel 2% 54
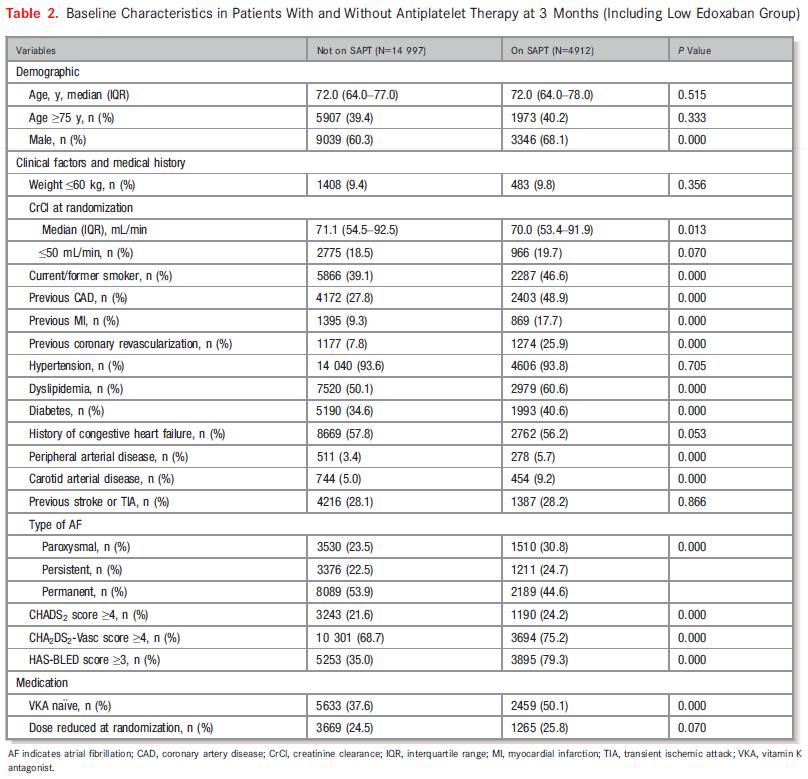
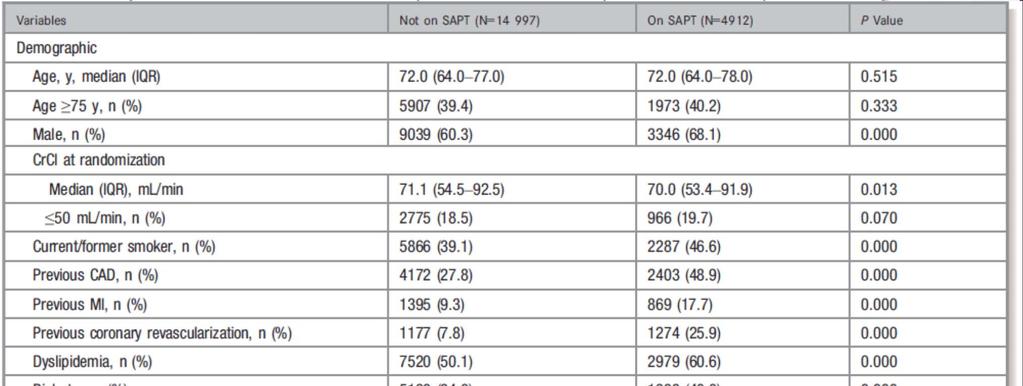

55 Baseline Characteristics 55
56 Results HDER 56
57 Results HDER (cont.) 57
58 Authors Conclusions Patients with AF who were selected by their physicians to receive APT in addition to an anticoagulant had similar risk of stroke/see and higher rates of bleeding than those not receiving SAPT Edoxaban exhibited similar relative efficacy and reduced bleeding compared to warfarin, with or without concomitant SAPT Patients with AF who are deemed to require the addition of a SAPT should receive a Xa inhibitor for anticoagulation whenever possible 58
59 Critical Appraisal Strengths Limitations One of very few trials looking at the effects of concomitant aspirin and DOAC use Large sample size Consistent 24 25% of patients were on APT throughout the study Very little other APT used other than ASA 100mg Patients receiving APT were different, with higher risk for both ischemic and bleeding events Though adjustments for confounders were made, more likely exist APT use not randomized 25% of patients on APT at study randomization discontinued within first 3 months Subgroup analysis limited power Generalizability Daiichi Sankyo funded the trial, provided the study drug, and some authors are Daiichi Sankyo employees Conclusion: Edoxaban + ASA has favorable bleeding risk over warfarin +/ ASA and may exhibit benefits on SSE 59
60 Use of Concomitant Aspirin In Patients With Atrial Fibrillation: Findings From the ROCKET AF Trial Shah R, Hellkamp A, Lokhnygina Y, et al. Am Heart J. 2016;179:
61 Insights from the ROCKET AF Trial Objective Understand the relationship between aspirin use and clinical outcomes in patients enrolled in Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET AF), in particular, those with known CAD. 61
62 Insights from the ROCKET AF Trial Design Treatment Groups Antiplatelet Users Multicenter, double blind, double dummy, eventdriven trial to assess non inferiority of rivaroxaban vs. warfarin Exclusion Criteria: CrCl <30 ml/min, bleeding risk, recent stroke or SEE, prosthetic heart valves, or had significant mitral stenosis Primary efficacy endpoint: stroke or non central nervous system embolism Secondary efficacy endpoints: MI, vascular death, and all cause death Primary safety endpoint: major or non major clinically relevant bleeding Secondary safety endpoints of major fatal bleeding, intracranial hemorrhage and hemorrhagic stroke Rivaroxaban 20mg daily (15mg daily if CrCl 30 49mL/min) Warfarin (INR 2 3) +/ ASA at baseline Analysis performed using baseline aspirin use 62
63 Antiplatelet Use 63 Mean baseline daily dose of aspirin was 99.2mg

64 Baseline Characteristics ASA patients were more likely to be Female Slightly younger Paroxysmal AF Mean CHADS2 score of 3.5 CAD HTN Prior MI CHF and COPD Prior VKA use ACE/ARB at baseline Digoxin at baseline 64
65 Statistical Methods Chi square test for categorical variables Presented using percentage (count) Wilcoxon rank sum test for continuous variables Presented using median (2th 75 th percentiles) Cox proportional hazard method used to calculate hazard ratios All endpoints were generated as events per 100 patient years and total events 65

66 Results 66

67 Results (cont.) 67

68 Results (cont.) 68
69 Authors Conclusions Aspirin use at baseline was associated with an increased risk of bleeding and all cause death in ROCKET AF, a risk most pronounced in patients without known CAD No significant differences in treatment effect for rivaroxaban or warfarin were detected between patients with and without baseline aspirin use for any of the efficacy outcomes or the safety outcomes Baseline ASA + Rivaroxaban vs Baseline ASA + Warfarin was significant for reducing all cause death and less intracranial and fatal bleeds 69

70 Critical Appraisal Strengths One of very few trials looking at the effects of concomitant aspirin and DOAC use Large sample size Limitations Post hoc analysis Study not powered to show a difference Author s conclusions ASA not randomized, started and stopped during the trial Generalizability high baseline CHADS2 score almost 3.5 Jansen grant funded the study Conclusion: Rivaroxaban + ASA may have favorable benefits for CAD secondary prevention and may have less bleeding events than warfarin + ASA. More data needed. 70
71 Summary Apixaban Apixaban + ASA still carries improved bleeding risk over warfarin +/ ASA and may have benefits on SSE Dabigatran Dabigatran + ASA increases major bleeding risk similar to warfarin + ASA but may NOT exhibit benefits on SSE Edoxaban Edoxaban + ASA has favorable bleeding risk over warfarin +/ ASA and may exhibit benefits on SSE Rivaroxaban Conclusion: Rivaroxaban + ASA may have favorable benefits for CAD secondary prevention and may have less bleeding events than warfarin + ASA. More data needed. 71
72 Overall Conclusions ASA 81mg + DOAC therapy (apixaban, edoxaban) has so far been shown to be consistently safer in regards to bleeding events than warfarin therapy +/ ASA therapy Use of ASA with dabigatran 150mg BID may attenuate beneficial effects of ASA therapy while still carrying an increased risk of bleeding More data are needed to make recommendations on rivaroxaban s place in AF + CAD management 72
73 Clinical Recommendations Careful consideration should be made when recommending ASA + DOAC therapy Increases bleeding risk from baseline, regardless of DOAC chosen May have benefits on overall SSE Monotherapy with a DOAC is likely best for most patients CHEST Guideline recommendation If your patient has AF and a strong clinical indication for secondary CAD event prevention, recommend edoxaban or apixaban as preferred DOAC options Not enough data to conclude rivaroxaban s role Dabigatran may have attenuated SSE benefits with concomitant APT and still carries increased bleeding risk similar to warfarin + ASA 73
74 Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central Texas Veterans Healthcare System 01/06/
75 Acknowledgements Dr. Erin Pilcher would like to thank the following people for their assistance and guidance in this presentation: Dr. Christine Wicke, Pharm.D., BCACP, CDE Dr. Katerine Getchell, Pharm.D., BCACP My Co Residents: Dr. Sarah Cho Dr. Diana Loffgren Dr. Steven Braun 75

76 Questions 76
77 Resources 1) Aguilar E, Garcia Diaz AM, Sanchez Munoz Torrero JF, Alvarez LR, Piedecausa M, Arnedo G, et al. Clinical outcome of stable outpatients with coronary, cerebrovascular or peripheral artery disease, and atrial fibrillation. Thromb Res 2012;130: ) Alexander JH, Lopes RD, Thomas L, et al. Apixaban vs. warfarin with concomitant aspirin in patients with atrial fibrillation: insights from the ARISTOTLE trial. Eur Heart J. 2014;35(4): ) Behnes M, Fastner C, Ansari U and Akin I. New oral anticoagulants in coronary artery disease. Cardiovascular and Haematological Disorders Drug Targets. 2015(15) ) Dans AL, Connolly SJ, Wallentin L, et al. Concomitant use of antiplatelet therapy with dabigatran or warfarin in the Randomized Evaluation of Long Term Anticoagulation Therapy (RE LY) trial. Circulation. 2013;127(5): ) Wilson P, Douglas PS, et al. Epidemiology of coronary heart disease. UpToDate. Topic updated Jan 23, Updated Dec of coronary heart disease 6) Lamberts M, Gislason GH, Lip GY, et al. Antiplatelet therapy for stable coronary artery disease in atrial fibrillation patients taking an oral anticoagulant: a nationwide cohort study. Circulation. 2014;129(15): ) Schurtz G, Bauters C, Ducrocq G, et al. Effect of aspirin in addition to oral anticoagulants in stable coronary artery disease outpatients with an indication for anticoagulation. Panminerva Medica 2016 December;58(4): ) Shah R, Hellkamp A, Lokhnygina Y, et al. Use of concomitant aspirin in patients with atrial fibrillation: Findings from the ROCKET AF trial. Am Heart J. 2016;179:
78 Resources 9) Shireman TI, Mahnken JD, Howard PA, Kresowik TF, Hou Q, Ellerbeck EF. Development of a contemporary bleeding risk model for elderly warfarin recipients. Chest. 2006;130(5): ) Vandvik O., Lincoff AM., Gore JM., et al. Primary and secondary prevention of cardiovascular disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e637s e668s. 11) Xu H, Ruff CT, Giugliano RP, et al. Concomitant Use of Single Antiplatelet Therapy With Edoxaban or Warfarin in Patients With Atrial Fibrillation: Analysis From the ENGAGE AF TIMI48 Trial. J Am Heart Assoc. 2016;5(2) 12) You JJ, Singer DE, Howard PA, et al. Antithrombotic therapy for atrial fibrillation: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e531S 75S. 78
Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy
 Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central
Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central
Stable CAD, Elective Stenting and AFib
 Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Atrial Fibrillation. 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018
 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF
 Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Debate: New Generation Anti-Coagulation Agents are a Better Choice than Warfarin in the Management of AF Bradley P. Knight, MD Director of Cardiac Electrophysiology Bluhm Cardiovascular Institute Northwestern
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Study design: multicenter, randomized, open-label trial following a PROBE design
 Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis
 Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Anticoagulation: Novel Agents
 Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation
 Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation September 14, 2018 Nina Maguire, PharmD PGY1 Pharmacy Resident Seton Healthcare Family Christina.maguire@ascension.org ASCENSION TEXAS Direct
Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation September 14, 2018 Nina Maguire, PharmD PGY1 Pharmacy Resident Seton Healthcare Family Christina.maguire@ascension.org ASCENSION TEXAS Direct
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
Lessons from recent antithrombotic studies and trials in atrial fibrillation
 Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Edoxaban in Atrial Fibrillation
 Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Engage AF-TIMI 48. Edoxaban in AF: What can we expect? Cardiology Update John Camm. St. George s University of London United Kingdom
 Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
Cardiology Update 2013 N S N O N H O H N S1 pocket Aryl binding N site O O N H N Cl Engage AF-TIMI 48 Edoxaban in AF: What can we expect? John Camm St. George s University of London United Kingdom Advisor
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Analysing Apixaban: Potential Growth Driver for Pfizer and Bristol Myers Squibb. Tro Kalayjian Chief Medical Analyst Chimera Research Group
 Analysing Apixaban: Potential Growth Driver for Pfizer and Bristol Myers Squibb Tro Kalayjian Chief Medical Analyst Chimera Research Group Prevalence of AFib in the US is expected to increase upwards of
Analysing Apixaban: Potential Growth Driver for Pfizer and Bristol Myers Squibb Tro Kalayjian Chief Medical Analyst Chimera Research Group Prevalence of AFib in the US is expected to increase upwards of
Old and New Anticoagulants For Stroke Prevention Benefits and Risks
 Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Stepheny Sumrall, FNP, AGACNP Cardiovascular Clinic of Hattiesburg
 Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
Novel Oral Anticoagulants Analyzing Clinical Trial Findings of the Efficacy and Safety Profiles of Novel Anticoagulants for the Treatment of Atrial Fibrillation and Prevention of Stroke Stepheny Sumrall,
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
A Patient with Chest Pain and Atrial Fibrillation
 A Patient with Chest Pain and Atrial Fibrillation Kurt Huber, Vienna, Austria Declaration of Interest Lecturing & Consulting Activities: AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi
A Patient with Chest Pain and Atrial Fibrillation Kurt Huber, Vienna, Austria Declaration of Interest Lecturing & Consulting Activities: AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC DEBATE: DOAC vs Good Old Warfarin André Roussin MD, FRCP, CSPQ CHUM and ICM/MHI Associate professor University of Montreal A. Roussin
Scoring Systems in AF 8/10/2016. Strategies in the Prevention of Atrial Fibrillation-Related Strokes. Overview
 Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China
 AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China Case report 64-year-old Chinese man with history of hypertension,
AF in Asian: which NOAC to choose for particular patient and at what dose? DEJIA HUANG West China Hospital of Sichuan University, Chengdu, China Case report 64-year-old Chinese man with history of hypertension,
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely
 Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Apixaban for stroke prevention in atrial fibrillation. August 2010
 Apixaban for stroke prevention in atrial fibrillation August 2010 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Apixaban for stroke prevention in atrial fibrillation August 2010 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Xarelto (rivaroxaban)
") Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure?
 The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
Atrial Fibrillation. Alan Bell, MD, CCFP. Staff Physician, Humber River Regional Hospital. University of Toronto
 Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
FINAL CDEC RECOMMENDATION
 FINAL CDEC RECOMMENDATION APIXABAN (Eliquis Bristol-Myers Squibb Canada and Pfizer Canada Inc.) New Indication: Prevention of Stroke and Systemic Embolism in Patients with Atrial Fibrillation Recommendation:
FINAL CDEC RECOMMENDATION APIXABAN (Eliquis Bristol-Myers Squibb Canada and Pfizer Canada Inc.) New Indication: Prevention of Stroke and Systemic Embolism in Patients with Atrial Fibrillation Recommendation:
ESC Congress 2012, Munich
 ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
ESC Congress 2012, Munich Anticoagulation in Atrial Fibrillation 2012: Which Anticoagulant for Which Patient? Stefan H. Hohnloser J.W. Goethe University Frankfurt am Main S.H.H. has served as a consultant,
Thrombosis and Thromboembolsim October Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy
 Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
Thrombosis and Thromboembolsim October 2012 Stroke Prevention in Atrial Fibrillation Risk Stratification and Choice of Antithrombotic Therapy Christian T. Ruff, MD, MPH TIMI Study Group Brigham and Women
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease
 Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention
 Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
Utilizing Anticoagulants for Atrial Fibrillation Related Stroke Prevention Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania
A Patient Unsuitable for VKA Treatment
 Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Will Apixaban change practice in atrial fibrillation? A Patient Unsuitable for VKA Treatment Professor Yoseph Rozenman The E. Wolfson Medical Center Jerusalem June 2013 Disclosures I have the following
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy
 New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy Hans-Christoph Diener Department of Neurology and Stroke Center University Hospital Essen Germany Conflict of Interest
New Aspects in the Diagnosis and Treatment of Atrial Fibrillation: Antithrombotic Therapy Hans-Christoph Diener Department of Neurology and Stroke Center University Hospital Essen Germany Conflict of Interest
7 th Munich Vascular Conference
 7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
Conflict of interest statement
 Risk of stroke, systemic embolism or death according to heart failure and left ventricular function status in patients with atrial fibrillation: results of the ARISTOTLE trial J.J.V. McMurray 1, B. Lewis
Risk of stroke, systemic embolism or death according to heart failure and left ventricular function status in patients with atrial fibrillation: results of the ARISTOTLE trial J.J.V. McMurray 1, B. Lewis
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute
 Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Indications of Anticoagulants; Which Agent to Use for Your Patient? Marc Carrier MD MSc FRCPC Thrombosis Program Ottawa Hospital Research Institute Disclosures Research Support/P.I. Employee Leo Pharma
Evaluate Risk of Stroke & Bleeding in AF Patients
 XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
XV World Congress of Arrhythmias, Beijing, China - 17-20 September, 2015 Evaluate Risk of Stroke & Bleeding in AF Patients Antonio Raviele, MD, FESC, FHRS President ALFA Alliance to Fight Atrial fibrillation
Drug Class Monograph
 Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION
 FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION") RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
RETROSPECTIVE CLAIMS DATABASE STUDIES OF DIRECT ORAL ANTICOAGULANTS (DOACS) FOR STROKE PREVENTION IN NONVALVULAR ATRIAL FIBRILLATION Craig I. Coleman, PharmD Professor, University of Connecticut School
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Direct Oral Anticoagulants An Update
 Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
Oct. 26, 2017 Direct Oral Anticoagulants An Update Kathleen Heintz, DO, FACC Assistant Professor of Medicine Cooper Heart Institute Direct Oral Anticoagulants: DISCLAIMERS No Conflicts of Interest So what
NOAC trials for AF: A review
 NOAC trials for AF: A review Chern-En Chiang, MD, PhD, FACC, FESC General Clinical Research Center Division of Cardiology Taipei Veterans General Hospital National Yang-Ming University Taipei, Taiwan Presenter
NOAC trials for AF: A review Chern-En Chiang, MD, PhD, FACC, FESC General Clinical Research Center Division of Cardiology Taipei Veterans General Hospital National Yang-Ming University Taipei, Taiwan Presenter
Long-Term Care Updates
 Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter?
 Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter? Renato D. Lopes, MD, PhD, FACC on behalf of the ARISTOTLE Investigators
Digoxin And Mortality in Patients With Atrial Fibrillation With and Without Heart Failure: Does Serum Digoxin Concentration Matter? Renato D. Lopes, MD, PhD, FACC on behalf of the ARISTOTLE Investigators
Clinical issues which drug for which patient
 Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Anticoagulants - a matter of heart! Towards a bright future? Clinical issues which drug for which patient Sabine Eichinger Dept. of Medicine I Medical University of Vienna/Austria Conflicts of interest
Edoxaban. Direct Xa inhibitor Direct thrombin inhibitor Direct Xa inhibitor Direct Xa inhibitor
 This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
This table provides a summary of the pharmacotherapeutic properties, side effects, drug interactions and other important information on the four anticoagulant medications currently in use or under review
Peer Review Report #2. Novel oral anticoagulants. (1) Does the application adequately address the issue of the public health need for the medicine?
 Does the application adequately address the issue of the public health need for the medicine?") 20 th Expert Committee on Selection and Use of Essential Medicines Peer Review Report #2 vel oral anticoagulants (1) Does the application adequately address the issue of the public health need for the
20 th Expert Committee on Selection and Use of Essential Medicines Peer Review Report #2 vel oral anticoagulants (1) Does the application adequately address the issue of the public health need for the
Relationship between Center Time in Therapeutic Range and Comparative Treatment Effect of Rivaroxaban and Warfarin: Results from the ROCKET AF Trial
 Relationship between Center Time in Therapeutic Range and Comparative Treatment Effect of Rivaroxaban and Warfarin: Results from the ROCKET AF Trial Jonathan P. Piccini, Frank Harrell, Yulia Lokhnygina,
Relationship between Center Time in Therapeutic Range and Comparative Treatment Effect of Rivaroxaban and Warfarin: Results from the ROCKET AF Trial Jonathan P. Piccini, Frank Harrell, Yulia Lokhnygina,
Antithrombotics in the elderly. Robert Gabor Kiss FESC FACC Budapest
 Antithrombotics in the elderly Robert Gabor Kiss FESC FACC Budapest The patient in the elderly You are sitting in Your office prescribing drugs and observing outcome The black box from prescription to
Antithrombotics in the elderly Robert Gabor Kiss FESC FACC Budapest The patient in the elderly You are sitting in Your office prescribing drugs and observing outcome The black box from prescription to
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Is Apixaban Effective for the Prevention of Stroke in Patients With Non-Valvular Atrial Fibrillation?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 Is Apixaban Effective for the Prevention
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 Is Apixaban Effective for the Prevention
Events after discontinuation of randomized treatment at the end of the ARISTOTLE trial
 Events after discontinuation of randomized treatment at the end of the ARISTOTLE trial Christopher Granger, John Alexander, Michael Hanna, Jerry Wang, Puneet Mohan, Jack Lawrence, Elaine Hylek, Jack Ansell,
Events after discontinuation of randomized treatment at the end of the ARISTOTLE trial Christopher Granger, John Alexander, Michael Hanna, Jerry Wang, Puneet Mohan, Jack Lawrence, Elaine Hylek, Jack Ansell,
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016
 1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
1 Atrial fibrillation and anticoagulation JIR-PING BOEY, DEPARTMENT OF HAEMATOLOGY, FLINDERS MEDICAL CENTRE FEBRUARY 2016 Disclosures 2 No conflicts of interest Some questions 3 Should my patient with
Controversies in Anticoagulation : Optimizing Outcome in NOACs for GI Bleeding Risk
 Controversies in Anticoagulation : Optimizing Outcome in NOACs for GI Bleeding Risk Boyoung Joung, MD, PhD Professor, Division of Cardiology Director of Electrophysiology Laboratory Severance Cardiovascular
Controversies in Anticoagulation : Optimizing Outcome in NOACs for GI Bleeding Risk Boyoung Joung, MD, PhD Professor, Division of Cardiology Director of Electrophysiology Laboratory Severance Cardiovascular