Penetrating Neck Trauma. Herve J. LeBoeuf, MD Francis B. Quinn, MD
|
|
|
- Kimberly Welch
- 6 years ago
- Views:
Transcription


1 Penetrating Neck Trauma Herve J. LeBoeuf, MD Francis B. Quinn, MD
2 Introduction 5-10% of all trauma Overall mortality rate as high as 11% Major vessel injury fatal in 65%, including prehospital deaths Attending physician must have excellent knowledge of anatomy Otolaryngologist as part of major trauma team
3 Historical Perspective/ pre WW I Ligation of the major vessels described as early as 1522 by Ambrose Pare Ligation was the procedure of choice for vascular injury through WW 1 Associated mortality rates up to 60% Significant neurologic impairment in 30 %
4 Historical / post WW II Mandatory exploration of all penetrating neck wounds, through the platysma Fogelman and Stewart reported Parkland Memorial Hospital experience of early, mandatory exploration with mortality of 65 vs.. 35% for delayed exploration 40% to 60% rate of negative explorations with mandatory exploration Present mortality for civilian wounds is 4% to 6%
5
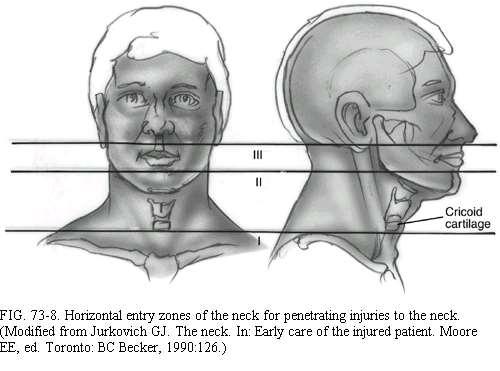
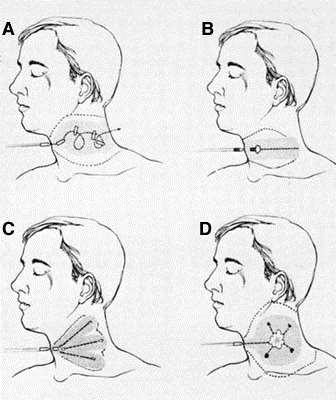
6 Anatomy/Zone I Bound superiorly by the cricoid and inferiorly by the sternum and clavicles Contains the subclavian arteries and veins, the dome of the pleura, esophagus, great vessels of the neck, recurrent nerve, trachea Signs of significant injury may be hidden from inspection in the mediastinum or chest
7 Anatomy/Zone II Bound inferiorly by the cricoid and superiorly by the angle of the mandible Contains the larynx, pharynx, base of tongue, carotid artery and jugular vein, phrenic, vagus, and hypoglossal nerves Injuries here are seldom occult Common site of carotid injury
8 Anatomy/Zone III Lies above the angle of the mandible Contains the internal and external carotid arteries, the vertebral artery, and several cranial nerves Vascular and cranial nerve injuries common
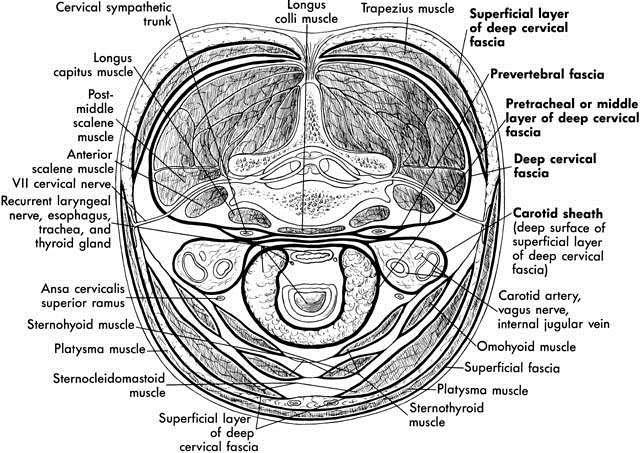
9 Fascial Layers Superficial cervical fascia - platysma Deep cervical fascia Investing: sternocleidomastoid muscle, trapezius muscle Pretracheal: larynx, trachea, thyroid gland, pericardium Prevertebral: prevertebral muscles, phrenic nerve, brachial plexus, axillary sheath Carotid sheath: carotid artery, internal jugular vein, vagus nerve
10
11
12
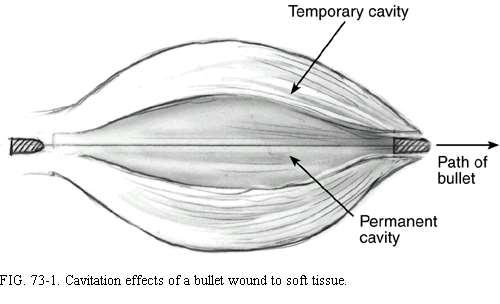
13 Ballistics Over 95% of penetrating neck wounds are from guns and knives, remainder from motor vehicle, household, and industrial accidents The amount of energy transferred to tissue is difference between the kinetic energy of the projectile when it enters the tissue, and the kinetic energy of any exiting fragments or projectiles The velocity of the projectile is the most significant aspect of energy transfer (K.E. = 1/2 mv^2
14 Ballistic cont... Muzzle velocity less than 1000 ft/s is considered low velocity.22 and.38 caliber handguns have a velocity of 800 ft/sec.357 magnum and.45 as high as 1500 ft/sec High power rifles: ft/sec Shotguns at less than 20 feet ft/sec
15 Ballistic cont. Injuries inflicted with high power rifles, shotguns at less than 20 feet, and.357 and.45 caliber handguns can cause extensive damage extending beyond the path of the projectile and should be explored Stab wounds do not have this effect Beware of the stab wound just over the clavicle -- the subclavian vein is at high risk
16
17
18 Stabilization/Airway Established Airway be prepared to obtain an airway emergently intubation or cricothyrotomy beware of cutting the neck in the region of the hematoma -- disruption there of may lead to massive bleeding must assume cervical spine injury until proven otherwise
19 Breathing Zone I injuries with concomitant thoracic injuries pneumothorax hemopneumothorax tension pneumothorax
20 Circulation Bleeding should be controlled by pressure Do not clamp blindly or probe the wound depths The absence of visible hemorrhage does not rule out Two large bore IVs Careful of IV in arm unilateral to subclavian injury
21 History Obtain from EMS witnesses, patient Mechanisms of injury - stab wounds, gunshot wound, high-energy, low-energy, trajectory of stab Estimate of blood loss at scene Any associated thoracic, abdominal, extremity injuries Neurologic history
22 Physical Examination Thorough head and neck exam using palpation and stethoscope to search for thrills and bruits Neuro exam: mental status, cranial nerves, and spinal column Examine the chest, abdomen, and extremities Be sure to examine the back of the patient as unsuspected stab or gunshot wounds have been missed here Don t blindly explore wound or clamp vessel
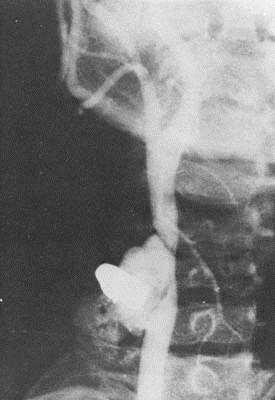
23 Radiographs CXR - inspiratory/expiratory films to assess for phrenic nerve injury, look for pneumothorax Cervical spine film to rule out fractures Soft tissue neck films AP and Lateral Arteriograms, contrast studies as indicated
24 Preoperative Preparation Surgeon and staff ready for emergent/urgent tracheotomy Gentle cleansing of wound, betadine paint only Prep vein donor site, and chest for possible thoracotomy Avoid NG tube until airway secure and patient anesthetized
25 Penetrating neck trauma Diagnosis Vascular injury Laryngotracheal injury Pharynx/esophagus injury Signs and symptoms Shock Hematoma Hemorrhage Pulse deficit Neurologic deficit Bruit or thrill in neck Subcutaneous emphysema Airway obstruction Sucking wound Hemoptysis Dyspnea Stridor Hoarseness or dysphonia Subcutaneous emphysema Hematemesis Dysphagia or odynophagia
26 Exploration vs. Observation Many experts have adopted a policy of selective exploration Decreased number of negative explorations, increased number of positive explorations Decreased cost of medical care, maybe No increase in mortality when adjunctive diagnostic studies and serial exams performed Patients taken to OR if clinical exam changes, around 2% in most studies
27
28 Site/Zone I Adequate exposure for exploration and repair may require sternotomy, clavicle resection, or thoracotomy High morbidity of exploration, thus suspicion must be great before taking the patient to OR Cardiothoracic surgery consultation a must Angiography is essential
29 Site/Zone II Few injuries will escape clinical examination Most carotid injuries occur here Adjunctive studies, except barium swallow and esophagoscopy where indicated, are not necessary Symptomatic zone II injuries can generally be safely managed by observation
30 Site/Zone III High rate of vascular injury, often multiple Often difficult to obtain proximal and distal vessel control Exploration has high rate of injury to cranial nerves Adequate exposure may require mandibular subluxation or mandibulotomy Angiography needed to delineate site of injury Embolization techniques of greatest value here
31 Clinical Setting Observation requires admission to an intensive care unit where serial examination can be performed by a surgeon Adjunctive studies must be available at all times and at a moments notice Absence of these dictates exploration of all patients - such as in a rural setting
32 Pharyngo Esophageal Gastrografin swallow followed by Barium if negative Flexible ± rigid esophagoscopy Invert the mucosal edges and close with two layers of absorable sutures JP drain and muscle flap
33

34
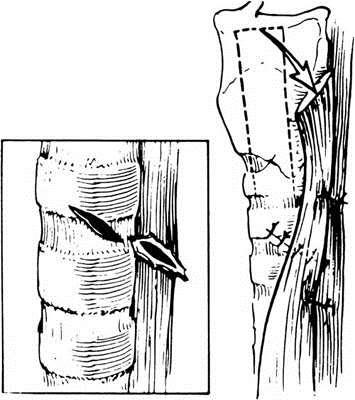
35 Airway DL where laryngeal injury is suspected Mucosal tears are closed with absorbable sutures Cover raw surfaces with nasal, buccal, or local mucosal flap A keel or soft stent is placed when denuded areas are opposed Tracheotomy one ring below injury when high tracheal injury Suprahyoid muscle release for primary closure of segmental defect
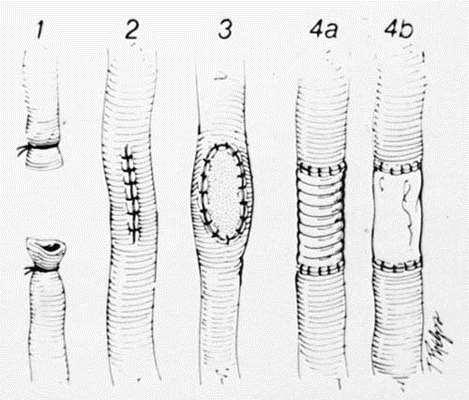
36 Vascular The subclavian and internal jugular veins can be ligated without adverse effect Major arteries should be repaired where possible except the vertebral which can be ligated Partial lacerations can be closed primarily -- vein patches will help prevent subsequent stenosis High velocity wounds produce a surrounding area of contusion which may be thrombogenic and which must be resected; then primary reanastamosis if possible
37
38
39 Vascular cont. When tension is required, vein grafts from the sphenous or internal jugular are interposed In central neurologic deficits: repair the artery when there are minimal deficits, with gross deficits restoration of flow can convert ischemic infarcts into hemorrhagic ones -- the artery should be ligated a deterioration in neurologic status dictates arteriography and reexploration EC-IC bypass when irreparable injury to ICA
40
41 Conclusions Maintain a healthy respect for apparently minor neck wounds because of potential fatal outcome for initially benign appearing injuries Do not try to infer trajectories of gunshot wounds from clinical or radiographic studies Careful history and complete physical exam with appropriate ancillary studies will avoid missed injuries Arteriography for zone I and zone III injuries Vascular injuries most immediately life-threatening, missed esophageal injury causes late mortality
42
Tips & Techniques in Operative Surgery II: Neck Exploration
 Tips & Techniques in Operative Surgery II: Neck Exploration ศ.ดร.นพ. พรช ย โอเจร ญร ตน สาขาว ชาศ ลยศาสตร ศ รษะ-คอ และเต านม ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Indications to Explore a Neck Removing
Tips & Techniques in Operative Surgery II: Neck Exploration ศ.ดร.นพ. พรช ย โอเจร ญร ตน สาขาว ชาศ ลยศาสตร ศ รษะ-คอ และเต านม ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล Indications to Explore a Neck Removing
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Tony Capizzani, MD, FACS
 Tony Capizzani, MD, FACS Trauma Medical Director Hillcrest Hospital Cleveland Clinic October 2, 2017 No disclosures Goals and Objectives Describe airway anatomy and innervation Recognize the association
Tony Capizzani, MD, FACS Trauma Medical Director Hillcrest Hospital Cleveland Clinic October 2, 2017 No disclosures Goals and Objectives Describe airway anatomy and innervation Recognize the association
Management of Penetrating Neck Trauma
 Management of Penetrating Neck Trauma Shashidhar S. Reddy, MD, MPH Faculty Advisor: Shawn D. Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Management of Penetrating Neck Trauma Shashidhar S. Reddy, MD, MPH Faculty Advisor: Shawn D. Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Penetrating Neck Trauma January 1999
 TITLE: Penetrating Neck Trauma SOURCE: Dept. of Otolaryngology, UTMB, Grand Rounds Presentation DATE: January 26, 1999 RESIDENT: Herve J. LeBoeuf, M.D. FACULTY: Francis B. Quinn, Jr., M.D. SERIES EDITOR:
TITLE: Penetrating Neck Trauma SOURCE: Dept. of Otolaryngology, UTMB, Grand Rounds Presentation DATE: January 26, 1999 RESIDENT: Herve J. LeBoeuf, M.D. FACULTY: Francis B. Quinn, Jr., M.D. SERIES EDITOR:
A CASE PRESENTATION AND DISCUSSION ON HEAD AND NECK TRAUMA
 A CASE PRESENTATION AND DISCUSSION ON HEAD AND NECK TRAUMA Nolan Ortega Aludino, M.D. Department of Surgery Ospital ng Maynila Medical Center General Data: B.R. 64 year old Male Tondo Manila Chief Complaint:
A CASE PRESENTATION AND DISCUSSION ON HEAD AND NECK TRAUMA Nolan Ortega Aludino, M.D. Department of Surgery Ospital ng Maynila Medical Center General Data: B.R. 64 year old Male Tondo Manila Chief Complaint:
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September ISSN
 International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
The Neck. BY: Lina Abdullah & Rahaf Jreisat
 The Neck BY: Lina Abdullah & Rahaf Jreisat Boundaries of the Neck: generally from base of the skull to root of the neck Superior margin :From superior nuchal line of occipital bone up to mastoid process
The Neck BY: Lina Abdullah & Rahaf Jreisat Boundaries of the Neck: generally from base of the skull to root of the neck Superior margin :From superior nuchal line of occipital bone up to mastoid process
Penetrating Trauma in Pediatric Patients. Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017
 Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Penetrating Trauma in Pediatric Patients Heidi P. Cordi, MD, MPH, MS, EMTP, FACEP, FAADM EMS WEEK 2017 Introduction Trauma is the leading cause of death between ages of 1-18 years Penetrating injury accounts
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function
 The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
How Do I Manage Penetrating Neck Trauma?
 Review Article ISSN 2508-5298 How Do I Manage Penetrating Neck Trauma? Hyun Min Cho Department of Trauma and Surgical Critical Care, Pusan National University Hospital, Busan, Korea Penetrating neck trauma
Review Article ISSN 2508-5298 How Do I Manage Penetrating Neck Trauma? Hyun Min Cho Department of Trauma and Surgical Critical Care, Pusan National University Hospital, Busan, Korea Penetrating neck trauma
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
Tracheo-innominate artery fistula (TIF) is an uncommon
 is an uncommon") Technique for Managing Tracheo-Innominate Artery Fistula Gorav Ailawadi, MD Tracheo-innominate artery fistula (TIF) is an uncommon complication (0.1-1%) following both open and percutaneous tracheostomy.
Technique for Managing Tracheo-Innominate Artery Fistula Gorav Ailawadi, MD Tracheo-innominate artery fistula (TIF) is an uncommon complication (0.1-1%) following both open and percutaneous tracheostomy.
Case Review: Airway Trauma Case 1: Tracheal Transection Pre-hospital:
 (Prepared by: A. Bacevice, MD) The following two cases were submitted for the case competition in 2016. They are presented to illustrate the theme of airway trauma. Case Review: Airway Trauma Case 1: Tracheal
(Prepared by: A. Bacevice, MD) The following two cases were submitted for the case competition in 2016. They are presented to illustrate the theme of airway trauma. Case Review: Airway Trauma Case 1: Tracheal
Anatomy of the Thyroid Gland
 Anatomy of the Thyroid Gland Introduction Nomenclature G, thyreos= shield, eidos= like Location Root of the neck ventrally (C5-T1) Function endocrine gland that secretes: Thyroxine (T4) T3 Calcitonin LWW,
Anatomy of the Thyroid Gland Introduction Nomenclature G, thyreos= shield, eidos= like Location Root of the neck ventrally (C5-T1) Function endocrine gland that secretes: Thyroxine (T4) T3 Calcitonin LWW,
Thyroid and Parathyroid Glands
 Thyroid and Parathyroid Glands Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/ explanation Objectives: By the end of the lecture,
Thyroid and Parathyroid Glands Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/ explanation Objectives: By the end of the lecture,
Management of Airway Trauma I:
 Management of Airway Trauma I: Tracheobronchial Injuries James P. Kelly, M.D., Watts R. Webb, M.D., Peter V. Moulder, M.D., Charles Everson, M.D., Buford H. Burch, M.D., and Edward S. Lindsey, M.D. ABSTRACT
Management of Airway Trauma I: Tracheobronchial Injuries James P. Kelly, M.D., Watts R. Webb, M.D., Peter V. Moulder, M.D., Charles Everson, M.D., Buford H. Burch, M.D., and Edward S. Lindsey, M.D. ABSTRACT
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Combat Extremity Vascular Trauma
 Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi
 Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Ballistic Trauma. L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016
 Ballistic Trauma L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016 Case Presentation Most cases at Kings County Hospital Case Presentation HPI: 22yo male presented as Level I Trauma
Ballistic Trauma L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016 Case Presentation Most cases at Kings County Hospital Case Presentation HPI: 22yo male presented as Level I Trauma
ISPUB.COM. Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots. B Phillips CASE REPORT THE OPERATING ROOM
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Tracheal Trauma: Management and Treatment. Kosmas Iliadis, MD, PhD, FECTS
 Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Tracheal Trauma: Management and Treatment Kosmas Iliadis, MD, PhD, FECTS Thoracic Surgeon Director of Thoracic Surgery Department Hygeia Hospital, Athens INTRODUCTION Heterogeneous group of injuries mechanism
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Skin Anatomy and Physiology
 Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Skin Anatomy and Physiology Body s largest organ Three layers: Epidermis Dermis Subcutaneous tissue 1 2 Skin Anatomy and Physiology Complex system, variety of functions Sensation Control of water loss
Prevertebral Region, Pharynx and Soft Palate
 Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Chapter 44 Neck Trauma
 Chapter 44 Neck Trauma Episode Overview: 1) Describe the landmarks and structures using the Zones of the neck & the Triangles of neck 2) List 6 hard and 6 soft signs of penetrating neck trauma. What are
Chapter 44 Neck Trauma Episode Overview: 1) Describe the landmarks and structures using the Zones of the neck & the Triangles of neck 2) List 6 hard and 6 soft signs of penetrating neck trauma. What are
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
Neck Ultrasound. Faculty Info: Amy Kule, MD
 Neck Ultrasound Date: Friday, October 19, 2018 Time: 11:00 AM Location: SMALL GROUP LABORATORY SSOM L71 Watch: Ø Neck Ultrasound Scanning Protocol (4:00): https://www.youtube.com/watch?v=zozd2x2ll4q Faculty
Neck Ultrasound Date: Friday, October 19, 2018 Time: 11:00 AM Location: SMALL GROUP LABORATORY SSOM L71 Watch: Ø Neck Ultrasound Scanning Protocol (4:00): https://www.youtube.com/watch?v=zozd2x2ll4q Faculty
THE DESCENDING THORACIC AORTA
 Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Anatomy: head and Neck (6 questions) 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli.
 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli.") Anatomy: head and Neck (6 questions) 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli. Rectus Capitis Anterior. Rectus Capitis Lateralis. Rectus Capitis
Anatomy: head and Neck (6 questions) 1. Prevertebral Flexor Musculature (lying in front of the vertebrae) include all, EXCEPT: Longus Colli. Rectus Capitis Anterior. Rectus Capitis Lateralis. Rectus Capitis
THYROID & PARATHYROID. By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy
 THYROID & PARATHYROID By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy 1 OBJECTIVES By the end of the lecture, the student should be able to: Describe the shape, position, relations and structure of
THYROID & PARATHYROID By Prof. Saeed Abuel Makarem & Dr. Sanaa Al-Sharawy 1 OBJECTIVES By the end of the lecture, the student should be able to: Describe the shape, position, relations and structure of
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
9/10/2012. Chapter 49. Learning Objectives. Learning Objectives (Cont d) Thoracic Trauma
 Thoracic Trauma") Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
Chapter 49 Thoracic Trauma 1 Learning Objectives Explain relevance of thoracic injuries as part of the overall mortality rate from major trauma List thoracic injuries that may result in early death if
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER
 GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
Tympanic Bulla Temporal Bone. Digastric Muscle. Masseter Muscle
 Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Anterior triangle of neck
 Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
11/3/16. Understanding and Addressing Strangulation. Jenifer Markowitz ND, RN, WHNP-BC, SANE-A, DF-IAFN. Copyright Notice
 Understanding and Addressing Strangulation Jenifer Markowitz ND, RN, WHNP-BC, SANE-A, DF-IAFN Copyright Notice This multimedia presentation contains the creative work of others and is used by permission,
Understanding and Addressing Strangulation Jenifer Markowitz ND, RN, WHNP-BC, SANE-A, DF-IAFN Copyright Notice This multimedia presentation contains the creative work of others and is used by permission,
10/14/2018 Dr. Shatarat
 2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
Esophageal injuries. 新光急診張志華醫師 Facebook.com/jack119
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Esophageal injuries. Pre-test /11/10. 新光急診張志華醫師 Facebook.com/jack119. O What is the most common cause of esophageal injuries?
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Surgery
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA Surgery
Chapter 16. Thoracic Injuries
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line.
 Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
ACDF. Anterior Cervical Discectomy and Fusion. An introduction to
 An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
Respiratory System. Clinical notes. Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz)
") Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Brain & Vascular Choke. Definition. The Choke Hold Don Muzzi MD & Larry Lovelace DO. Submission Breakdown UFC Events 4/27/17! 15% of Cardiac Output
 The Choke Hold Don Muzzi MD & Larry Lovelace DO Submission Breakdown UFC Events 25% of fights end in submission anaconda! d acre! 74% of submissions are result of choke hold Does not reflect opinions of
The Choke Hold Don Muzzi MD & Larry Lovelace DO Submission Breakdown UFC Events 25% of fights end in submission anaconda! d acre! 74% of submissions are result of choke hold Does not reflect opinions of
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions.
 Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Lecture 01. The Thyroid & Parathyroid Glands. By: Dr Farooq Khan PMC Date: 12 th March. 2018
 Lecture 01 The Thyroid & Parathyroid Glands By: Dr Farooq Khan PMC Date: 12 th March. 2018 INTRODUCTION LAYERS OF THE NECK The neck has four major compartments or layer which are enclosed by an outer musculofascial
Lecture 01 The Thyroid & Parathyroid Glands By: Dr Farooq Khan PMC Date: 12 th March. 2018 INTRODUCTION LAYERS OF THE NECK The neck has four major compartments or layer which are enclosed by an outer musculofascial
Emergency Approach to the Subclavian and Innominate Vessels
 Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Subclavian and Axillary Artery Aneurysms
 Subclavian and Axillary Artery Aneurysms April 2008 Francesco A Aiello, M.D. Assistant Professor of Surgery Division of Vascular Endovascular Surgery University of Massachusetts Medical School None DISCLOSURES
Subclavian and Axillary Artery Aneurysms April 2008 Francesco A Aiello, M.D. Assistant Professor of Surgery Division of Vascular Endovascular Surgery University of Massachusetts Medical School None DISCLOSURES
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Tracheostomy in a Gunshot Wound Neck: A Case Report S K Singh *, Maj Tarun Sood **, Maj Abhipsa Hota ***,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Tracheostomy in a Gunshot Wound Neck: A Case Report S K Singh *, Maj Tarun Sood **, Maj Abhipsa Hota ***,
Mediastinum and pericardium
 Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions. 4 May 2012
 SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
SCHOOL OF ANATOMICAL SCIENCES Mock Run Questions 4 May 2012 1. With regard to the muscles of the neck: a. the platysma muscle is supplied by the accessory nerve. b. the stylohyoid muscle is supplied by
Aortic arch pathology. Cerebral ischemia following carotid artery stenosis.
 Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Important: -Subclavian Steal Syndrome -Cerebral ischemia Aortic arch pathology. Cerebral ischemia following carotid artery stenosis. Mina Aubeed & Alba Hernández Pinilla Aortic arch pathology Common arch
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Lung & Pleura. The Topics :
 Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Anatomy notes-thorax.
 Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
ISPUB.COM. GSW To The Face: "Hunting Camp" C Perry, B Phillips CASE REPORT
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 2 Number 2 C Perry, B Phillips Citation C Perry, B Phillips.. The Internet Journal of Rescue and Disaster Medicine. 2000 Volume 2 Number
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 2 Number 2 C Perry, B Phillips Citation C Perry, B Phillips.. The Internet Journal of Rescue and Disaster Medicine. 2000 Volume 2 Number
Superior and Posterior Mediastinum. Assoc. Prof. Jenny Hayes
 Superior and Posterior Mediastinum Assoc. Prof. Jenny Hayes WARNING This material has been provided to you pursuant to section 49 of the Copyright Act 1968 (the Act) for the purposes of research or study.
Superior and Posterior Mediastinum Assoc. Prof. Jenny Hayes WARNING This material has been provided to you pursuant to section 49 of the Copyright Act 1968 (the Act) for the purposes of research or study.
1. Thyroxine (inactive form) also called T4 (90% of the secretion). 2. Triiodothyronine (active form) also called T3 (10% of the secretion).
 also called T4 (90% of the secretion). 2. Triiodothyronine (active form) also called T3 (10% of the secretion).") A Introduction The nomenclature of the thyroid gland comes from its close relation to the thyroid cartilage (the thyroid cartilage was named like this because thyroid means shield and it is shielding the
A Introduction The nomenclature of the thyroid gland comes from its close relation to the thyroid cartilage (the thyroid cartilage was named like this because thyroid means shield and it is shielding the
 55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
55-year-old male with 2nd and 3rd degree burns to face, chest, and arms on 25% of the body Respirations: 34 Pulse: 120 Mental Status: moans to painful stimulus Mucous membranes charred Stridor 10 cm scalp
Surgical Anatomy of the Neck. M. J. Jurkiewicz, John Bostwick. Surgical Clinics of North America, Vol 54, No 6, December 1974.
 Surgical Anatomy of the Neck M. J. Jurkiewicz, John Bostwick Surgical Clinics of North America, Vol 54, No 6, December 1974. The radical neck dissection is a safe, effective therapeutic procedure for eradication
Surgical Anatomy of the Neck M. J. Jurkiewicz, John Bostwick Surgical Clinics of North America, Vol 54, No 6, December 1974. The radical neck dissection is a safe, effective therapeutic procedure for eradication
Objectives. Thoracic Inlet. Thoracic Inlet Boundaries. Thoracic Inlet Sagittal View ANTERIOR SCALENE ANTERIOR SCALENE
 Objectives Thoracic Inlet Deborah L. Reede M.D. SUNY Downstate Medical Center Learn the anatomy of the thoracic inlet (TI) Review the clinical and radiographic findings of common lesions encountered in
Objectives Thoracic Inlet Deborah L. Reede M.D. SUNY Downstate Medical Center Learn the anatomy of the thoracic inlet (TI) Review the clinical and radiographic findings of common lesions encountered in
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Chapter 28. Objectives. Objectives 01/09/2013. Bleeding and Soft-Tissue Trauma
 Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous structures - Significant thoracic inj
 PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous
PEDIATRIC CHEST TRAUMA Children are not small adults Role of imaging Spectrum of injury Children are not small adults Children are Not Small Adults Anatomic considerations Pliable bony & cartilagenous