Clinical Application of CRRT for Infants and Children
|
|
|
- Arleen Turner
- 6 years ago
- Views:
Transcription



1 Clinical Application of CRRT for Infants and Children Geoffrey Fleming Daryl Ingram Jordan Symons 22 nd International Conference on Advances in Critical Care Nephrology San Diego 2017
2 Introduction Pediatric CRRT is no longer a novel therapy Many years of experience Literature to support our approach Each patient presents unique challenges Adapting standards to clinical situations Adjusting approach to address complications Each program faces its own issues Technology, support, staffing, acuity, etc.
3 Format for the Session Present a clinical case or question Discuss as a group Review our perspective Case resolution Points illustrated Data/literature review where available Summarize at the end
4 Case #1 CRRT AND ECMO
5 Case # 1 Clinical Scenario 14 years old, previously healthy male with h/o URI for 4-5 days, sore throat and cough. Transferred from outside hospital to PICU with hypoxic respiratory failure, sepsis, necrotizing pneumonia Cannulated for VA-ECMO VA- ECMO with flows currently at 3.5 Liters/Min Pressures Pre-membrane 300 Post-membrane 310 Weight (actual) 61.2kg Intubated Vent settings R-18, 30/10,30% O2
6 Case # 1 Clinical Scenario (Continued) Urine output noted to go down Serum creatinine rising 0.7mg/dL à 1.3mg/dL Worsening edema on exam PICU team contacts you regarding AKI and possible need for RRT
7 Case # 1 Discussion How do you address the need for RRT when a patient is on ECMO? What technical challenges must you anticipate? How do you coordinate care between teams?
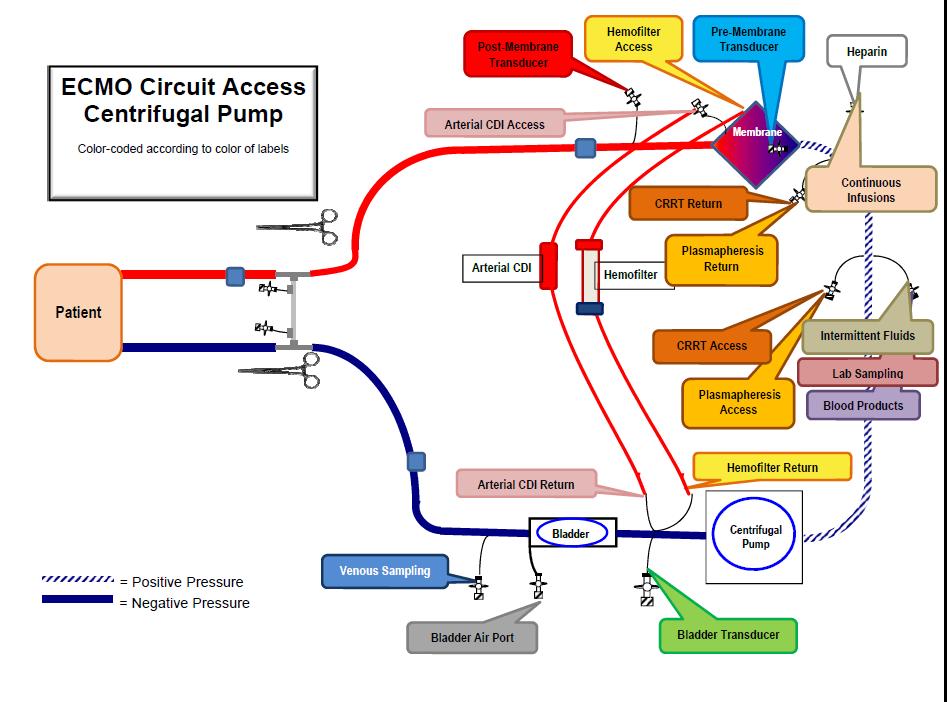
8 CRRT and ECMO: Blood Pathway Blood Flow ECMO Venous Pull line, Drain line ECMO Arterial Return line, Re-infuse line CRRT Arterial (Access) Pull line CRRT Venous (Return) Re-infuse line
9 Deoxygenated Blood Venous Oxygenated Blood Arterial Negative Pressure Bridge Oxygenator Pump Motor
10 CRRT and ECMO: Issues with the ECMO Circuit Negative Pressure with Centrifugal pumps CRRT circuit standard pressure mode Lower pressures, likely less pressure alarms Danger of AIR if disconnected
11 Deoxygenated Blood Venous Oxygenated Blood Arterial Bridge Oxygenator Positive Pressure Pump Motor
12 CRRT and ECMO: Issues with the ECMO Circuit Positive Pressure (roller head or centrifugal) CRRT circuit positive pressure mode High ECMO pressures will influence CRRT pressures, likely more pressure alarms Danger of Exsanguination if disconnected
13 CRRT and ECMO: Ideal Connection 1. Least risk for introducing air 2. Minimize pressure alarms on CRRT Connection location will determine Arterial pressure Stopcocks and/or restrictors Venous NO restrictors
14 Venous Arterial Deoxygenated Blood Venous Bridge Oxygenated Blood Arterial Oxygenator Pump Motor Arterial Ideal Connection Venous
15
16 Case # 1 Additional Discussion Do you perform ECMO and CRRT at your center? What challenges and issues have you needed to address when considering RRT for patients receiving ECMO?
17 Case # 1 Summary ECMO circuit determines CRRT pressures Ideal connection site: post pump/pre oxygenator Connections secure, frequent checks Standardized the process Options for high pressures
18 Case # 2 CRRT FOR NEONATES
19 Case # 2 Clinical Scenario 3 week old term female with perinatal asphyxia (abruption) and chorioamnionitis; looks septic Cr has been rising (1mg/dL à 3.2mg/dL) Weight increased (BW 3.2kg à 4.1kg); edematous Increased ventilator support; urine dwindling
20 Case # 2 Discussion Does this patient require renal replacement? What modality would be best for support? What issues and complications must we watch for if we go forward with renal replacement?
21 Renal Support Options Hemodialysis, Peritoneal Dialysis, CRRT Each has advantages & disadvantages Choice is guided by Patient Characteristics Disease/Symptoms Hemodynamic stability Goals of therapy Fluid removal Electrolyte correction Toxin removal Availability, expertise, cost Pediatr Nephrol (2009) 24:37 48
22 CRRT for Neonates: A Series of Challenges Small patient with small blood volume Equipment designed for bigger people No specific protocols Complications may be magnified No clear guidelines Limited outcome data
23 Prescribing CRRT: Special Neonatal Considerations Vascular access Blood Prime Blood flow rates Fluids/Modality (CVVH vs. CVVHD vs. CVVHDF) Ultrafiltration goals Anticoagulation Filter/membrane
24 Neonatal CRRT Access Access size is key to success Frequent clotting and circuit down time is time without therapy Vessel size French ~3x diameter of vessel in mm Bedside ultrasound nearly universally available SVC is bigger than femoral vein Low resistance Resistance ~8lη/2r 4 So, the biggest and shortest catheter should be best
25 Access Considerations Internal Jugular Very accessible Large caliber (SVC) Great flows Low recirculation rate Risk for pneumothorax Cardiac monitoring may take precedence Femoral Usually accessible Smaller than SVC Flows may be diminished by: Abdominal pressures Patient movement Risk for retroperitoneal hemorrhage Higher recirculation rate Subclavian: Many feel current double lumen vas cath are too stiff to make the turn into the SVC and I don t personally use them. Although they are used in some centers. Better for bigger kids likely.

26 In patients with cardiac lesions concerns re upper vessels needed for future heart transplant Femoral vessels may not be big enough for an 8F DLC Risk for clots Risk for future inability to perform catheterizations Reported on 6 babies PD failed All had 2 single lumen catheters Most ran for over 60 hours. Average circuit life 55.2 hr (double circuit life for infants < 5 kg in ppcrrt registry
27 Blood Prime for Pediatric CRRT Smaller patients (e.g. <10-15kg) require blood priming to prevent hypotension/hemodilution Circuit volume > 10-15% patient blood volume Example 5 kg infant : Blood Volume (BV) 400ml (80ml/kg) Extracorporeal circuit volume 100 ml (25% of BV) Technique: prime first with saline, then blood/albumin mix to Hct of ~35
28 Blood Prime Increases Risks Blood product exposure possibly repeated Biochemical imbalances HYPOCALCEMIA Citrate anticoagulant in PRBCs HYPERKALEMIA K+ release from RBCs more over time (older unit) ACIDEMIA Increases risk for bradykinin release syndrome
29 Bradykinin Release Syndrome Mucosal congestion, bronchospasm, hypotension at start of CRRT Resolves with discontinuation of CRRT Thought to be related to bradykinin release when patient s blood contacts hemofilter Exquisitely ph sensitive Associated with AN-69 membrane
30 Bypass System to Prevent Bradykinin Release Syndrome PRBC Waste Modified from Brophy, et al. AJKD, 2001
31 Recirculation System to Prevent Bradykinin Release Syndrome Normalize ph Recirculation Plan: D Qb 200ml/min Qd ~40ml/min Time 7.5 min Normalize K + Based on Pasko, et al. Ped Neph 18: , 2003 Waste
32 Neonatal Double CRRT Restart Cross prime from active circuit to new circuit No new units of blood from blood bank Blood in system already equilibrated to patient Need several more hands Only good for restarts when current circuit still functioning
33 Neonatal Double CRRT Restart NS
34 Simple Systems to Limit Likelihood of Bradykinin Release Syndrome Don t prime on with blood Don t use the AN-69 membrane






35 Device Limitations for Infant CRRT

")

36 Infant-Specific/Adapted Devices Cardio Renal Pediatric Dialysis Emergency Machine (CARPEDIEM) Newcastle Infant Dialysis and Ultrafiltration System (NIDUS) Aquadex FlexFlow
37 Case # 2 Additional Discussion Do you provide CRRT for infants at your center? What challenges and issues have you encountered with infant CRRT? Do you prefer other modalities for infants? How do you choose?
38 Case #2 Summary CRRT can be an effective therapy for even the smallest patients Multiple challenges remain on several fronts The possibility of a better devices for neonates may open further options
39 Case #3 CRRT FOR HYPERAMMONEMIA
40 Case #3 Clinical Scenario 4 day old infant male, initially well Presents with poor feeding, decreased muscle tone, obtundation Admitted to local hospital for evaluation 2.6kg Ammonia 1600 micromol/l Presumed inborn error of metabolism Did not respond to medical management Transferred to our center for further care
41 Case #3 Discussion Would you have accepted this patient? How would you approach overall care? What are your goals for ammonia removal? How would you organize and implement treatment for this patient?
42 Hyperammonemia and Inborn Errors of Metabolism Diagnoses include: Urea Cycle Defects Organic Acidemias Duration of hyperammonemia associated with neurodevelopmental outcome Goal is rapid detoxification Ammonia level below 200 micromol/l
43 Toxin (NH 3 ) Removal Procedures Current recommendations: Bring down ammonia as quickly as possible Keep it there until you get metabolic control Extracorporeal therapy options include: Peritoneal dialysis (slow) Hemodialysis (efficient) CRRT (can be as efficient as HD for the neonate)
44 CRRT vs IHD for Inborn Errors IHD had been the standard Rapid detoxification due to high Qb and Qd Hemodynamic stability Small infant Rebound after cessation CRRT has gained popularity Detoxification can be as rapid if Rx adjusted to increase clearance
45

46 21 infants with IEM Clearance was all > 2000 ml/1.73m2/min Prior IHD did not affect outcome 100% of the non-survivors were > 10% FO
47
48 Case #3 Additional Discussion How do you address medical management of inborn errors while providing extracorporeal therapy? Does your approach to hyperammonemia or metabolic intoxication differ for an older/larger child? 5 year old with MSUD crisis? 15 year old with hyperammonemia in liver failure?
49 Case #3 Summary Inborn errors of metabolism are lifethreatening disorders in which rapid reduction of ammonia is imperative CRRT can effectively reduce and stabilize ammonia in small children with inborn errors of metabolism Larger children may require a different or combined approach to achieve NH 3 clearance
50 Case #4 CRRT IN PEDIATRIC LIVER FAILURE
51 Case #4 Clinical Scenario 12 year old girl (previously healthy); weight 35kg Admitted to PICU with fulminant hepatic failure INR 9, NH 3 814, lactate 11, AST >20,000, ALT >3,500 T 40C, altered mental status, seizures, hypotension Resuscitated, intubated, massive blood product requirement 10% FO within first 24 hours of admission BUN 45mg/dL, Creatinine 1.8mg/dL Urine output 100ml last 12 hours
52 Case #4 Clinical Scenario (Continued) Clinical problems at this time include Liver failure AKI Fluid overload Large volume requirements Elevated ammonia levels Increased bleeding risk Nephrology consulted; CRRT initiated
53 Case #4 Discussion What prescription/clearance challenges are posed by this patient? What are the priming considerations? What are our options for anticoagulation?
54 Case #4 Prescription and Clearance Can use fairly standard Rx May want to run blood flow rate higher to reduce clotting Clearance In a smaller patient with large volume needs, UF alone will lend a tremendous amount of clearance Citrate 100mL/hr Ca 50mL/hr Average 2.6L/day 110mL/hr Total 260mL/hr à10kg ptà26ml/kg/hr
55 Clearance: Goals and Delivery UF: may give target CRRT clearance (20-25mL/kg/hr) Minimum Qd (50mL/hr) and Qr (50-100mL/hr) settings on some devices add another 10-15mL/kg/hr High rates of clearance may have their own risks for complications (metabolic imbalance, etc.) Intensity of Continuous Renal-Replacement Therapy in Critically Ill Patients The RENAL Replacement Therapy Study Investigators N Engl J Med 2009; 361: October 22, 2009
56 Case #4 Prescription and Clearance Recognizing caveats should we treated like a hyperammonemic neonate? 8000mL/1.73m 2 /hr Our patient is 1.1m 2 Target a Qd+Qr of 5000mL/hr Advantages: rapid metabolic correction, clearance of NH 3, mediator clearance (theoretical) Disadvantages: negative impact on electrolytes, medication dosing, nutrition, calcium balance
57 Anticoagulation Anticoagulation options: Heparin, citrate, others(?) None Heparin Citrate No anticoagulation: circuit loss (bad) Citrate and heparin have equal circuit survival More bleeding with heparin Accumulation risk with citrate Brophy PD, et al. Multi-centre evaluation of anticoagulation in patients receiving continuous renal replacement therapy (CRRT). Nephrol Dial Transplant (2005) 20:
58 Case #4 Clinical Case (Continued) 24 hours later: Total calcium 19.7mg/dL Patient ph 7.09 (HCO3 12meq/L) Pt ical 1.15mmol/L, circuit ical 0.38mmol/L Qb 100mL/min Citrate infusion 150mL/hr Calcium chloride infusion 450mg/hr Suspected citrate accumulation Elevated total calcium = Ca-citrate Although alkalosis is more common, unmetabolized citrate can cause acidosis
59 Citrate Accumulation: Management Techniques to mitigate citrate accumulation Increase clearance Reset citrate/calcium Increase circuit ical target/reduce citrate delivery Reduce Qb (less citrate required) Heparin (wholesale switch or low dose infusion into arterial lumen with higher circuit ical range) Look the other way and hope for transplant J
60 Case #4 Additional Discussion How do you determine clearance goals ( dose ) for your patients? What is your approach to anticoagulation? In special clinical circumstances (e.g. liver failure) does your approach differ from a standard patient with AKI?
61 Case #4 Summary Clearance maintains metabolic balance but data on best goals for dose are lacking Anticoagulation is necessary, and sometimes it can be tricky Highly complex patients are more challenging to manage
62 Clinical Application of CRRT for Infants and Children: Summary Pediatric CRRT can present many challenges: Prescription Coordination with other therapies/interventions Complications We have touched upon some common problems and some unique issues CRRT is a team effort: Between colleagues at the bedside Among colleagues around the world
63 Any Other Comments or Questions?

64 Thanks for Your Participation!
Pediatric AKI & CRRT: Caring for my Patient & Program? David Selewski, MD Theresa Mottes, RN, NP
 Pediatric AKI & CRRT: Caring for my Patient & Program? David Selewski, MD Theresa Mottes, RN, NP Introduction Pediatric AKI is no longer a mystery issue Growing data on epidemiology and outcome Pediatric
Pediatric AKI & CRRT: Caring for my Patient & Program? David Selewski, MD Theresa Mottes, RN, NP Introduction Pediatric AKI is no longer a mystery issue Growing data on epidemiology and outcome Pediatric
Practice Based Learning in CRRT: The Science and the Art Pediatric Session. David Askenazi Theresa Mottes Scott Sutherland
 Practice Based Learning in CRRT: The Science and the Art Pediatric Session David Askenazi Theresa Mottes Scott Sutherland 1 Objectives Brief Epidemiology Challenges with Pediatric CRRT Indications Prescription
Practice Based Learning in CRRT: The Science and the Art Pediatric Session David Askenazi Theresa Mottes Scott Sutherland 1 Objectives Brief Epidemiology Challenges with Pediatric CRRT Indications Prescription
Renal replacement therapy in Pediatric Acute Kidney Injury
 Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Recent advances in CRRT
 Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
Technical Considerations for Renal Replacement Therapy in Children
 Technical Considerations for Renal Replacement Therapy in Children Timothy E. Bunchman, MD,* Patrick D. Brophy, MD, and Stuart L. Goldstein, MD Summary: Provision of renal replacement therapy to the critically
Technical Considerations for Renal Replacement Therapy in Children Timothy E. Bunchman, MD,* Patrick D. Brophy, MD, and Stuart L. Goldstein, MD Summary: Provision of renal replacement therapy to the critically
03/19/2019. Michael Zappitelli, MD, MSc Hospital for Sick Children, Toronto. Symposium on Pediatric Dialysis, ADC, Dallas, 2019
 Michael Zappitelli, MD, MSc Hospital for Sick Children, Toronto Symposium on Pediatric Dialysis, ADC, Dallas, 2019 Baxter: Reimbursed for a CRRT workshop to PICU nurses Slides: S. Goldstein D. Askenazi
Michael Zappitelli, MD, MSc Hospital for Sick Children, Toronto Symposium on Pediatric Dialysis, ADC, Dallas, 2019 Baxter: Reimbursed for a CRRT workshop to PICU nurses Slides: S. Goldstein D. Askenazi
Pediatric AKI & CRRT: How Do I Care for my Patient and my Program?
 Pediatric AKI & CRRT: How Do I Care for my Patient and my Program? Theresa Mottes Zaccaria Ricci Jordan Symons 23 rd International Conference on Advances in Critical Care Nephrology San Diego 2018 Introduction
Pediatric AKI & CRRT: How Do I Care for my Patient and my Program? Theresa Mottes Zaccaria Ricci Jordan Symons 23 rd International Conference on Advances in Critical Care Nephrology San Diego 2018 Introduction
CRRT for the Experience User 1. Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018
 CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2
 Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes. Richard Beale
 Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Rationale for renal replacement therapy in ICU: indications, approaches and outcomes Richard Beale RIFLE classification (ADQI group) 2004 Outcome AKIN classification Definition: Abrupt (within 48 hrs)
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
Admission Day 2 Na Potassium Cl Bicarb BUN Cr Hb Hct platelets
 Nithin Karakala Mr. Clark Kent was admitted to the hospital with multiple injuries after an epic battle with the Kryptonians. He was hypotensive at the time of admission. Over the next 24 hours he develops
Nithin Karakala Mr. Clark Kent was admitted to the hospital with multiple injuries after an epic battle with the Kryptonians. He was hypotensive at the time of admission. Over the next 24 hours he develops
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
ST. DOMINIC-JACKSON MEMORIAL HOSPITAL JACKSON, MISSISSIPPI. CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) HEPARIN ANTICOAGULATION Page 1 of 5
 HEPARIN ANTICOAGULATION Page 1 of 5") HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
Active UMMC Protocols
 UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
UAB CRRT Primer Ashita Tolwani, MD, MSc University of Alabama at Birmingham
 UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
Essential in Renal Replacement Therapy Pediatrics CRRT
 Essential in Renal Replacement Therapy Pediatrics CRRT Konggrapun Srisuwan MD. Dialysis and Transplantation Program, Department of Pediatrics, Phramongkutklao Hospital Correction of fluid overload in patients
Essential in Renal Replacement Therapy Pediatrics CRRT Konggrapun Srisuwan MD. Dialysis and Transplantation Program, Department of Pediatrics, Phramongkutklao Hospital Correction of fluid overload in patients
CRRT Procedures. and Guidelines. CRRT: Guidelines
 CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
Dialysis Dose Prescription and Delivery. William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012
 Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background
 Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background Index: 1. Introduction Pg. 1 1.1 Definitions Pg. 2 1.2 Renal replacement therapy principles Pg. 2 2. Continuous
Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background Index: 1. Introduction Pg. 1 1.1 Definitions Pg. 2 1.2 Renal replacement therapy principles Pg. 2 2. Continuous
Renal Replacement Therapy in ICU. Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine
 Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
ASN Board Review: Acute Renal Replacement Therapies
 ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
Pediatric AKI in Bad Pediatric CRRT is Hard
 Pediatric AKI in Bad Pediatric CRRT is Hard David Askenazi MD, MSPH Professor of Pediatrics Director Pediatric and Infant Center for Acute Nephrology (PICAN) Potential COI Speaker for Baxter, and the AKI
Pediatric AKI in Bad Pediatric CRRT is Hard David Askenazi MD, MSPH Professor of Pediatrics Director Pediatric and Infant Center for Acute Nephrology (PICAN) Potential COI Speaker for Baxter, and the AKI
Pediatric Continuous Renal Replacement Therapy
 Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
CRRT in Pediatrics: Indications, Techniques & Outcome. Overview
 CRRT in Pediatrics: Indications, Techniques & Outcome Timothy E. Bunchman Pediatric Nephrology & Transplantation Grand Rapids, MI Overview (Please interrupt me at any time) Access Solutions Anticoagulation
CRRT in Pediatrics: Indications, Techniques & Outcome Timothy E. Bunchman Pediatric Nephrology & Transplantation Grand Rapids, MI Overview (Please interrupt me at any time) Access Solutions Anticoagulation
MODALITIES of Renal Replacement Therapy in AKI
 MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement
 Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Timing, Dosing and Selecting of modality of RRT for AKI - the ERBP position statement Prof. Dr. Achim Jörres Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
PICANet Renal Dataset supplement Renal Daily Interventions
 PICANet Renal Dataset supplement Renal Daily Interventions Version 2.0 (March 2017) 1 Contents PICANet Renal Dataset supplement... 1 Renal Daily Interventions... 1 Version 2.0 (March 2017)... 1 Recording
PICANet Renal Dataset supplement Renal Daily Interventions Version 2.0 (March 2017) 1 Contents PICANet Renal Dataset supplement... 1 Renal Daily Interventions... 1 Version 2.0 (March 2017)... 1 Recording
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
ECLS Registry Form Extracorporeal Life Support Organization (ELSO)
") ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
ECLS Registry Form Extracorporeal Life Support Organization (ELSO) Center ID: Center name: Run No (for this patient) Unique ID: Birth Date/Time Sex: (M, F) Race: (Asian, Black, Hispanic, White, Other)
Renal Replacement Therapy in Acute Renal Failure
 CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
CHAPTER 82 Renal Replacement Therapy in Acute Renal Failure R. Deshpande Introduction Acute renal failure (ARF) is defined as an abrupt decrease in renal function sufficient to result in retention of nitrogenous
Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of
 Update on CRRT: Pearls for the Clinician Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of Medicine tbunchman@mcvh-vcu.edu
Update on CRRT: Pearls for the Clinician Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of Medicine tbunchman@mcvh-vcu.edu
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT)
") TABLE OF CONTENTS The purpose of this practice support document is to outline the procedures and guidelines related to care of the patient having continuous renal replacement therapy (CRRT) in the pediatric
TABLE OF CONTENTS The purpose of this practice support document is to outline the procedures and guidelines related to care of the patient having continuous renal replacement therapy (CRRT) in the pediatric
UNDERSTANDING THE CRRT MACHINE
 UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
higher dose with progress in technical equipment. Continuous Dialysis: Dose and Antikoagulation. prescribed and delivered
 1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
Fluid Management in Critically Ill AKI Patients
 Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Fluid Management in Critically Ill AKI Patients Sang Kyung Jo, MD, PhD Department of Internal Medicine Korea University Medical College KO/MG31/15-0017 Outline Fluid balance in critically ill patients:
Symposium. Principles of Renal Replacement Therapy in Critically ill children- Indian Perspective
 Symposium DOI- 10.21304/2018.0502.00376 in Critically ill children- Indian Perspective Sidharth Kumar Sethi *, Aliza Mittal**, Rupesh Raina***, Manindar Dhaliwal**** * Senior Consultant, Pediatric Nephrology
Symposium DOI- 10.21304/2018.0502.00376 in Critically ill children- Indian Perspective Sidharth Kumar Sethi *, Aliza Mittal**, Rupesh Raina***, Manindar Dhaliwal**** * Senior Consultant, Pediatric Nephrology
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Physiology of Blood Purification: Dialysis & Apheresis. Outline. Solute Removal Mechanisms in RRT
 Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy
 Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
BPG 03: Continuous Renal Replacement Therapy (CRRT)
") BPG 03: Continuous Renal Replacement Therapy (CRRT) Statement of Best Practice Patient s requiring Continuous Renal Replacement Therapy (CRRT) will receive appropriate therapy to meet their individual
BPG 03: Continuous Renal Replacement Therapy (CRRT) Statement of Best Practice Patient s requiring Continuous Renal Replacement Therapy (CRRT) will receive appropriate therapy to meet their individual
Decision making in acute dialysis
 Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Decision making in acute dialysis Geoffrey Bihl MB.BCh M.MED FCP(SA) Nephrologist and Director Winelands Kidney and Dialysis Centre Somerset West South Africa Important questions in AKI What is the cause?
Pediatric CRRT The Basics
 Pediatric CRRT The Basics Patrick Brophy Geoffrey Fleming Jordan Symons Michael Zappitelli 16 th International CRRT Conference San Diego 2011 Epidemiology Of and Indications For Pediatric CRRT ACUTE KIDNEY
Pediatric CRRT The Basics Patrick Brophy Geoffrey Fleming Jordan Symons Michael Zappitelli 16 th International CRRT Conference San Diego 2011 Epidemiology Of and Indications For Pediatric CRRT ACUTE KIDNEY
ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN. Bashir Admani KPA Precongress 24/4/2018
 ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN Bashir Admani KPA Precongress 24/4/2018 Case presentation SP 11month old Presenting complaint: bloody diarrhea, lethargy On exam: dehydration,
ACUTE KIDNEY INJURY AND RENAL REPLACEMENT THERAPY IN CHILDREN Bashir Admani KPA Precongress 24/4/2018 Case presentation SP 11month old Presenting complaint: bloody diarrhea, lethargy On exam: dehydration,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
RENAL FAILURE IN ICU. Jo-Ann Vosloo Department Critical Care SBAH
 RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015)
 CITRATE GUIDELINES (Approved May 2015)") Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015) BCU Citrate Guideline v6 Nov 2015 (Approved by CCSC May 15) 1 BCU Critical Care Guideline for Renal Replacement Therapy
Wales Critical Care & Trauma Network (North) CITRATE GUIDELINES (Approved May 2015) BCU Citrate Guideline v6 Nov 2015 (Approved by CCSC May 15) 1 BCU Critical Care Guideline for Renal Replacement Therapy
GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS
 GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS RRCV CMG Nephrology Service 1. Introduction A first acute or chronic haemodialysis session may induce disequilibrium syndrome
GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS RRCV CMG Nephrology Service 1. Introduction A first acute or chronic haemodialysis session may induce disequilibrium syndrome
ECMO CPR. Ravi R. Thiagarajan MBBS, MPH. Cardiac Intensive Care Unit
 ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ECMO CPR Ravi R. Thiagarajan MBBS, MPH Staff Intensivist Cardiac Intensive Care Unit Children s Hospital Boston PCICS 2008, Miami, FL No disclosures Disclosures Outline Outcomes for Pediatric in-hospital
ECCO 2 Removal The Perfusionists Perspective
 ECCO 2 Removal The Perfusionists Perspective BelSECT Education evening 2016-06-15 D. Hella, Th. Amand, J-N Koch Definition ECCO 2 Removal: Process by which an extracorporeal circuit is used for removing
ECCO 2 Removal The Perfusionists Perspective BelSECT Education evening 2016-06-15 D. Hella, Th. Amand, J-N Koch Definition ECCO 2 Removal: Process by which an extracorporeal circuit is used for removing
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Ricky Bell Renal/ICM Registrar
 Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
Ricky Bell Renal/ICM Registrar Objectives When to call renal How to manage the patient with AKI How the manage the patient with CKD (HD/PD) Special AKI situations What do the guidelines say? My referral
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO
 ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Technical aspects of RRT in AKI: access, anticoagulation, drug dosage and nutrition. Marlies Ostermann
 Technical aspects of RRT in AKI: access, anticoagulation, drug dosage and nutrition Marlies Ostermann AKI guideline Chapter 3: Nutrition Chapter 5.3: Anticoagulation Chapter 5.4: Vascular access for RRT
Technical aspects of RRT in AKI: access, anticoagulation, drug dosage and nutrition Marlies Ostermann AKI guideline Chapter 3: Nutrition Chapter 5.3: Anticoagulation Chapter 5.4: Vascular access for RRT
CRRT. ICU Fellowship Training Radboudumc
 CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
CRRT ICU Fellowship Training Radboudumc Timing RRT Consider the following: Underlying cause and reversibility. Rapid improvement unlikely with high dose vasopressors and continuous exposure to other risk
TOO SWEET TOO STORMY. CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth. PRESENTOR: Dr. Abhinaya PG I (M.D Paeds)
") TOO SWEET TOO STORMY PRESENTOR: Dr. Abhinaya PG I (M.D Paeds) CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth Unit IV, Dept. Of Paediatrics, SRMC & RI 14year old female complaints of
TOO SWEET TOO STORMY PRESENTOR: Dr. Abhinaya PG I (M.D Paeds) CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth Unit IV, Dept. Of Paediatrics, SRMC & RI 14year old female complaints of
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
Olistic Approach to Treatment Adequacy in AKI
 Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
Toronto - Canada, 2014 Olistic Approach to Treatment Adequacy in AKI Claudio Ronco, MD Department of Nephrology, St. Bortolo Hospital, International Renal Research Institute Vicenza - Italy 1) RRT
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Management of the patient with established AKI. Kelly Wright Lead Nurse for AKI King s College Hospital
 Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done?
 Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Comparing RRT Modalities: Does It Matter What You Use If The Job Is Done? Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta Disclosure Consulting: Alere, Baxter, Gambro,
Continuous Renal Replacement Therapy. Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
PROGRAMME. 8th INTERNATIONAL CONFERENCE ON PAEDIATRIC CONTINUOUS RENAL REPLACEMENT THERAPY (pcrrt)
") www.pcrrtconferences.com Abstract deadline: 15th April 2015 8th INTERNATIONAL CONFERENCE ON PAEDIATRIC CONTINUOUS RENAL REPLACEMENT THERAPY (pcrrt) 16th - 18th July 2015 Queen Elizabeth II Conference Centre,
www.pcrrtconferences.com Abstract deadline: 15th April 2015 8th INTERNATIONAL CONFERENCE ON PAEDIATRIC CONTINUOUS RENAL REPLACEMENT THERAPY (pcrrt) 16th - 18th July 2015 Queen Elizabeth II Conference Centre,
Continuous Renal Replacement Therapy
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators
 oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators Heparin-grafted for reduced thrombogenicity Supports renal function POWERED
oxiris A single CRRT set with multiple benefits for managing critically ill patients with AKI Adsorption of inflammatory mediators Heparin-grafted for reduced thrombogenicity Supports renal function POWERED
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen
 When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
When and how to start RRT in critically ill patients? Intensive Care Training Program Radboud University Medical Centre Nijmegen Case history (1) 64 Hypertension 2004 AVR 2009 Paravalvular leak - dilated
Acute Kidney Injury Care in the Chronic Unit
 Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Acute Kidney Injury Care in the Chronic Unit BONNIE B GREENSPAN WITH ASSIST FROM: DENISE MURCEK, JINA BOGLE, MARY SCHIRA, OCTOBER 5, 2017 Objectives At the completion of the session, engaged participants
Kit Assembly. Enhanced Simplicity OPERATIONAL BENEFITS. Automatic venous chamber adjustment. User friendly interface
 System for CRRT Kit Assembly Enhanced Simplicity User friendly interface Flexible AcuSmart touch screen can be turned 180 degrees with up to 100 degrees of tilt in order to ensure visibility from various
System for CRRT Kit Assembly Enhanced Simplicity User friendly interface Flexible AcuSmart touch screen can be turned 180 degrees with up to 100 degrees of tilt in order to ensure visibility from various
404FM.2 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU. (Based on Gambro and Kalmar Hospital protocols)
 USING CITRATE Target Audience: Hospital only ICU. (Based on Gambro and Kalmar Hospital protocols)") 404FM.2 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU (Based on Gambro and Kalmar Hospital protocols) CRRT using regional citrate anticoagulation This is
404FM.2 CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) USING CITRATE Target Audience: Hospital only ICU (Based on Gambro and Kalmar Hospital protocols) CRRT using regional citrate anticoagulation This is
Vascular access, Gp1 BO2, Wed. Feb 27 th 1100 hrs
 Vascular access, Gp1 BO2, Wed. Feb 27 th 1100 hrs San Diego, AKI & CRRT Conference Professor Ian Baldwin, RN PhD, FACCCN Dept. of Intensive Care Austin Health, Melbourne Australia Deakin & RMIT University
Vascular access, Gp1 BO2, Wed. Feb 27 th 1100 hrs San Diego, AKI & CRRT Conference Professor Ian Baldwin, RN PhD, FACCCN Dept. of Intensive Care Austin Health, Melbourne Australia Deakin & RMIT University
Dialysis in the Acute Setting
 Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Regional Citrate Anticoagulation for RRTs in Critically Ill Patients with AKI
 In-Depth Review Regional Citrate Anticoagulation for RRTs in Critically Ill Patients with AKI Santo Morabito,* Valentina Pistolesi,* Luigi Tritapepe, and Enrico Fiaccadori Abstract Hemorrhagic complications
In-Depth Review Regional Citrate Anticoagulation for RRTs in Critically Ill Patients with AKI Santo Morabito,* Valentina Pistolesi,* Luigi Tritapepe, and Enrico Fiaccadori Abstract Hemorrhagic complications
THERAPEUTIC PLASMA EXCHANGE
 THERAPEUTIC PLASMA EXCHANGE DIRECTORATE OF NEPHROLOGY AND TRANSPLANTATION Background and Indications Therapeutic plasma exchange (TPE) is an extracorporeal blood purification technique in which plasma
THERAPEUTIC PLASMA EXCHANGE DIRECTORATE OF NEPHROLOGY AND TRANSPLANTATION Background and Indications Therapeutic plasma exchange (TPE) is an extracorporeal blood purification technique in which plasma
Continuous renal replacement therapy in children with multiple organ dysfunction syndrome: A case series
 CHALLENGING CLINICAL CASES Vol. 40 (6): 846-852, November - December, 2014 doi: 10.1590/S1677-5538.IBJU.2014.06.18 Continuous renal replacement therapy in children with multiple organ dysfunction syndrome:
CHALLENGING CLINICAL CASES Vol. 40 (6): 846-852, November - December, 2014 doi: 10.1590/S1677-5538.IBJU.2014.06.18 Continuous renal replacement therapy in children with multiple organ dysfunction syndrome:
Manual CVVH Automatic machine
 Blood pump & infusion pumps Manual CVVH Automatic machine Anticoagulant Predisposing factors : blood flow, hemofilter type, coagulation pathway activation, convective mass transfer Site of thrombus formation
Blood pump & infusion pumps Manual CVVH Automatic machine Anticoagulant Predisposing factors : blood flow, hemofilter type, coagulation pathway activation, convective mass transfer Site of thrombus formation
Welcome to the UK Primary Hyperoxaluria family support day
 Welcome to the UK Primary Hyperoxaluria family support day Understanding Primary Hyperoxaluria (PH) / Oxalosis together Dr Sally-Anne Hulton Kim Hollander % PH Patients PH is diagnosed at any age 50 45
Welcome to the UK Primary Hyperoxaluria family support day Understanding Primary Hyperoxaluria (PH) / Oxalosis together Dr Sally-Anne Hulton Kim Hollander % PH Patients PH is diagnosed at any age 50 45
Vascular access, Gp1 BO2
 Vascular access, Gp1 BO2 San Diego, 21 st AKI & CRRT Conference, Feb 16 th 19 th 2016 Professor Ian Baldwin, RN PhD, FACCCN Dept. of Intensive Care Austin Health, Melbourne Australia Deakin & RMIT University
Vascular access, Gp1 BO2 San Diego, 21 st AKI & CRRT Conference, Feb 16 th 19 th 2016 Professor Ian Baldwin, RN PhD, FACCCN Dept. of Intensive Care Austin Health, Melbourne Australia Deakin & RMIT University
There are no shortcuts to Dialysis
 There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
There are no shortcuts to Dialysis 1 Outcomes John Sweeny Wednesday, March 21 st, 2018 (3:10 pm 4:10 pm) 2 Quality in Hemodialysis Quality Health Care is the degree to which health services increases the
Section 5: Dialysis Interventions for Treatment of AKI Kidney International Supplements (2012) 2, ; doi: /kisup.2011.
 2, ; doi: /kisup.2011.") http://www.kidney-international.org chapter 5.1 & 2012 KDIGO Section 5: Dialysis Interventions for Treatment of AKI Kidney International Supplements (2012) 2, 89 115; doi:10.1038/kisup.2011.35 Chapter
http://www.kidney-international.org chapter 5.1 & 2012 KDIGO Section 5: Dialysis Interventions for Treatment of AKI Kidney International Supplements (2012) 2, 89 115; doi:10.1038/kisup.2011.35 Chapter
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital
 Renal Dialysis Centre Hong Kong Sanatorium & Hospital") Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in