Direct oral anticoagulants in patients with atrial fibrillation undergoing percutaneous coronary intervention PIONEERing the way for a new paradigm?
|
|
|
- Darrell Todd Horn
- 6 years ago
- Views:
Transcription
1 Direct oral anticoagulants in patients with atrial fibrillation undergoing percutaneous coronary intervention PIONEERing the way for a new paradigm? Sarah Alexis Hallowell, Pharm.D. PGY1 Pharmacy Resident South Texas Veterans Health Care System, San Antonio, Texas The University of Texas at Austin College of Pharmacy Pharmacotherapy Education and Research Center University of Texas Health San Antonio October 6 th, 2017 Learning Objectives: 1. Describe the significance and management of concomitant atrial fibrillation and acute coronary syndromes requiring percutaneous coronary intervention 2. Provide a basic overview of atrial fibrillation, acute coronary syndromes, percutaneous coronary intervention, and direct oral anticoagulants 3. Discuss the literature pertaining to the use of direct oral anticoagulants in patients with atrial fibrillation undergoing percutaneous coronary intervention 4. Recommend optimal antithrombotic regimens in patients with atrial fibrillation undergoing percutaneous coronary intervention
2 Acute Coronary Syndromes Requiring Percutaneous Coronary Intervention in Patients with Atrial Fibrillation I. Significance a. Atrial fibrillation (AF) most common arrhythmia, affecting approximately million Americans (~1-2 % of the general population) 1,2 i. Expected to double by 2030 ii. Contributes significantly to mortality 1) Underlying cause of death on ~21,000 death certificates in United States (US) in ) High risk of death in first four months after diagnosis 3) Many fatal complications: non-cardiovascular (CV) death, sudden cardiac death, progressive heart failure (HF), and stroke b. Acute coronary syndromes (ACS) acute manifestations of coronary heart disease (CHD), which affect an estimated 15.5 million Americans over age 20 1,3 i. Estimated 18% increase by 2030 ii. Responsible for greater than 1 million hospitalizations annually in the US approximately ~660,000 Americans with a new event and ~305,000 with recurrent events iii. Most common cause of CV disease death 1) Decreased mortality in the last 10 years due to: a) Primary and secondary prevention b) Initial treatment for ACS events or HF c) Coronary artery revascularization d) Shift in the incidence of different ACS event types II. Overlap a % of patients with AF have concomitant CHD 4 i. Incidence of both AF and ACS increases with age 1,2,4 1) Average age of patients with AF: 66.8 years for men and 74.6 years for women 2) Average age of patients with ACS: 65.1 years for men and 72 years for women ii. AF associated with increased mortality in patients with myocardial infarctions (MI) 1,2 III. Management a. Antithrombotic therapy is a core component of management of both AF and ACS after revascularization with percutaneous coronary intervention (PCI) 4 i. Purposes of antithrombotic therapy 1) AF: prevent cerebrovascular ischemia or systemic embolism 2,4 2) ACS post-pci: prevent recurrence of coronary ischemic events and stent thrombosis 4 b. Triple Therapy: dual antiplatelet therapy (DAPT) + oral anticoagulant 4 i. Guiding principles 1) Anticoagulant used to decrease risk of stroke or thromboembolic events in AF 2) DAPT used to decrease coronary ischemia and thrombosis after PCI for ACS a) DAPT = aspirin + P2Y 12 inhibitor 3) DAPT + anticoagulant 2-3x increased risk of bleeding complications 4,5 ii. Historical standard of care for triple therapy: warfarin + clopidogrel + aspirin 4 iii. Direct oral anticoagulants (DOACs) have evidence and indications for use in nonvalvular AF ) Until recently, relatively little literature about the use of DOACs in AF after PCI 2) Guideline recommendations regarding use of DOACs in patients with AF undergoing PCI are inconsistent SARAH HALLOWELL 2
3 c. Obstacle and objective of antithrombotic therapy: balance risk of clot with risk of bleed Thrombosis Bleeding d. Guideline recommendations: Table 1: Summary of Various Guideline Recommendations for Antithrombotic Therapy in Patients with AF Undergoing PCI 2,5,11-13 Antithrombotic Triple therapy with warfarin + aspirin + clopidogrel for 1 month after bare metal stent therapy (BMS) placement and 3-6 months after drug-eluting stent placement (DES) warfarin + single antiplatelet agent for total of 12 months, then warfarin targeted to international normalized ratio (INR) Risk stratification based on stroke, bleed, and ACS mortality or repeat MI risks 5,12 o Use validated scoring tools CHA 2DS 2-VASc and HAS-BLED (appendix A) 5 Warfarin targeted to INR may be used as anticoagulant with new AF 2,5,12 o Goal time in therapeutic range > 70% 12 Direct oral anticoagulant may be used as anticoagulant with new AF 2 o Lower stroke prevention dose from AF trials may be considered 12 Dual therapy with clopidogrel + oral anticoagulant may be considered 5,12,13 o Initial therapy option in patients with high bleed risk (HAS-BLED score 3) 12 or patients with CHA 2DS 2-VASc score 2 2 Antiplatelet Clopidogrel is P2Y 12 inhibitor of choice 5,12 Agents o Ticagrelor and prasugrel not part of triple therapy used in special circumstances 12 Aspirin doses 100 mg 5 Stent Type Consider BMS to minimize required duration of DAPT 2 May prefer newer generation DES in patients with low HAS-BLED scores (0-2) 12 Duration Triple therapy duration should be limited 5,13 based on risks of coronary events vs. risk of bleeding 13 o High bleed risk triple therapy for 1 month 12,13 up to 12 months of dual therapy 12 o High risk of stroke or low bleed risk relative to thrombosis risk consider triple therapy for 1-6 months 13 o Moderate-high ACS risk + low bleed risk triple therapy for 6 months regardless of stent type, may continue 6-12 months 12 SARAH HALLOWELL 3
4 e. Proposed DOAC-based strategy 14 i. Rationale 1) DOACs have lower intracranial hemorrhage risk and noninferior to lower risk of nongastrointestinal (GI) major bleeding vs. warfarin 2) Clopidogrel key to prevention of stent thrombosis and has lower bleed risk than newer P2Y 12 inhibitors 3) Stopping aspirin does not appear to increase risk of stent thrombosis ii. Algorithm: 1) 0-1 months: aspirin + clopidogrel + DOAC 2) 1-6 months: clopidogrel + DOAC 3) 6+ months: DOAC iii. Use lower dosage ranges than approved for clinical use Atrial Fibrillation I. Definition & Classifications 2 a. Type of supraventricular tachycardia characterized by rapid atrial rate, disorganized atrial activation, and irregularly irregular pulse b. Types: i. Valvular AF associated with mechanical or bioprosthetic heart valve, mitral valve stenosis, or mitral valve repair ii. Nonvalvular AF (NVAF) absence of above valvular complications II. Pathophysiology 2 Rapid Atrial Rate Desynchronized Atrial Contraction Variable Atrioventricular Node Impulse Penetration Irregular Ventricle Activiation Irregularly Irregular Pulse a. Mechanisms i. Atrial structural abnormalities extracardiac factors, oxidative stress, tachycardic remodeling, genetics, and renin-angiotensin-aldosterone system (RAAS) activation ii. Atrial electrical abnormalities RAAS activation, atrial tachycardic remodeling, genetics, and autonomic nervous system I. Presentation 2 a. Symptoms i. Rapid heartbeat, palpitations ii. Worsening HF symptoms dyspnea or fatigue iii. Asymptomatic b. Signs i. Irregularly irregular rhythm without P waves ventricular rate of beats per minute III. Risk factors & Complications a. Predictors of new onset AF 1, 2 i. Patient factors advanced age, greater height and body mass index, genetic variants, family history, moderate to heavy alcohol use, and smoking ii. CV factors left ventricular hypertrophy, left atrial enlargement, hypertension, and CV disease including CHD, HF, and valvular heart disease iii. Other factors hyperthyroidism, chronic kidney disease (CKD), diabetes SARAH HALLOWELL 4
5 IV. b. Complications 1 i. Self-perpetuating arrhythmia ii. Ischemic stroke and other thromboembolic events iii. Increased risk of MI and HF Management a. Antiarrhythmic Therapy refer to guidelines for acute management, including discussion of rate vs. rhythm control strategies 2,11,13 b. Prevention of Thromboembolism 2,13 i. Individualized based on risk of stroke and bleeding 2 1) Stroke risk assessed by CHA 2DS 2-VASc score (appendix A) a) Score of 0 reasonable to omit oral antithrombotic medications b) Score of 1 consider antiplatelet therapy, oral anticoagulant, or aspirin c) Score 2 anticoagulant recommended 2) Bleed risk assessed by HAS-BLED score (appendix A) a) Score 3 high risk for bleeding ii. Vitamin K antagonist 2,11 1) Historical standard of care has the most evidence and a reversal agent 2) Limitations: genomics, interactions, monitoring, and narrow therapeutic index iii. DOACs 1) Four approved for NVAF 10 (appendix B) 2) Increased use due to evidence of efficacy in reducing stroke and systemic embolism (SSE), as well as noninferior or lower risk of bleeding 6-9 3) More predictable anticoagulation and no INR monitoring 11 4) Limitations: only one has reversal agent and limited evidence with renal dysfunction 2,10 Table 2. Summary of Atrial Fibrillation Guideline Recommendations 2,11,13 Valvular AF Warfarin recommended anticoagulant 2 NVAF Patients with prior stroke or transient ischemic attack (TIA) or CHA 2DS 2-VASc score 2 warfarin, dabigatran, rivaroxaban, 2 and edoxaban 13 all options 2016 European Society of Cardiology guidelines recommend DOACs over warfarin CHEST guidelines suggest dabigatran rather than warfarin based on individual patient factors and preferences 11 * DOAC recommended in patients unable to maintain therapeutic INR on warfarin Selection based on renal function 2 ** o Moderate to severe CKD may consider reduced doses of DOACs (no established safety and efficacy), or use warfarin o End-stage CKD or dialysis warfarin recommended *Dabigatran only DOAC approved for NVAF at time of publication ** Reassessed when clinically indicated and at least annually when DOACs selected SARAH HALLOWELL 5
 Apixaban (Eliquis ) Dabigatran (Pradaxa ) Edoxaban (Savaysa ) Rivaroxaban (Xarelto ) Table 3: Overview of DOACs Approved for NVAF 10 Approved Doses Mechanism")
6 Direct Oral Anticoagulants Figure 1: Clotting Cascade with Oral Anticoagulant Targets Name (Brand) Apixaban (Eliquis ) Dabigatran (Pradaxa ) Edoxaban (Savaysa ) Rivaroxaban (Xarelto ) Table 3: Overview of DOACs Approved for NVAF 10 Approved Doses Mechanism Monitoring Adjustments for Renal of Action Function 5 mg BID or 2.5 Factor Xa Renal and Avoid use with CrCl <25 mg BID if any 2: inhibitor hepatic ml/min age 80, weight function, 60 kg, serum bleeding creatinine 1.5 mg/dl 150 mg BID Direct thrombin inhibitor 60 mg daily Factor Xa inhibitor 20 mg daily with evening meal Factor Xa inhibitor Complete blood count (CBC), renal function, bleeding Bleeding, renal function prior to initiation CBC, renal and hepatic function CrCl ml/min: 75 mg BID Per CHEST: contraindicated in CrCl 30 ml/min Do not use if CrCl > 95 ml/min Dose reduce if CrCl ml/min: 30 mg daily Not recommended: CrCl < 15 ml/min Dose reduce if CrCl ml/min: 15 mg daily Avoid with CrCl < ml/min Reversal No specific reversal agent Not dialyzable Idarucizumab (Praxbind ) Dialysis removes ~57% over 4 hours No specific reversal agent Not dialyzable No specific reversal agent Not dialyzable SARAH HALLOWELL 6
7 Acute Coronary Syndromes I. Definitions & Classification a. ACS acute manifestations of CHD classified according to changes seen on electrocardiogram (ECG) and presence or absence of biomarkers for cardiac necrosis 3 i. ST segment elevation myocardial infarction (STEMI) ischemic injury to full thickness of myocardial wall 1) Symptoms of myocardial ischemia 2) ST segment elevation on ECG 3) Elevated troponin T or I or creatinine kinase-myocardial band (CK-MB) ii. Non-ST segment elevation myocardial infarction (NSTEMI) injury to subendocardial myocardium, usually smaller than STEMI 1) Symptoms of myocardial injury 2) Elevated troponin T or I or CK-MB iii. Unstable angina (UA) ischemia that does not produce tissue injury 1) Symptoms of myocardial ischemia II. Etiology & Pathophysiology 3,15 a. Disruption of atherosclerotic plaque is the cause of ACS in 90% of patients Atherosclerosis Plaque Progression Plaque Disruption Thrombus Formation ACS 1) STEMI large plaque fissures fixed, persistent thrombus abrupt cessation of myocardial perfusion transmural myocardium necrosis 16 2) NSTEMI plaque damage persistent thrombotic occlusion without complete cessation of myocardial perfusion 16 3) UA nonocclusive plaque thrombus, vasoconstriction, mechanical obstruction, inflammation/infection, or secondary UA 17 III. Presentation 15 a. Substernal chest pain or pressure, may radiate to jaw, neck, left arm or shoulder b. May be accompanied by nausea, vomiting, diaphoresis, fatigue, or shortness of breath IV. Risk Factors & Complications a. Risk factors: smoking, hypertension, diabetes, hyperlipidemia, obesity, lack of physical activity, family history of heart disease, and prior atherosclerotic ischemic stroke 1,18 b. Complications 19 i. Ischemic angina, reinfarction, or infarct extension ii. Mechanical cardiogenic shock, HF, valve dysfunction, aneurysm, myocardium rupture iii. Arrhythmic node dysfunction, atrial or ventricular arrhythmias iv. Embolic stroke and systemic embolism v. Inflammatory pericarditis V. Management a. Choice of reperfusion therapy by ACS type i. STEMI 1) Primary PCI treatment of choice within 12 hours of symptom onset and minutes of first medical contact 20 2) PCI reasonable with ongoing ischemia hours after symptom onset 21 ii. UA/NSTEMI SARAH HALLOWELL 7
8 1) Choice of therapy based on risk assessment 21,22 2) Primary PCI refractory angina, hemodynamic or electrical instability, absence of major comorbidities or contraindications, and higher risk patients 21 b. Pharmacotherapy 5,20,22 i. Aspirin given immediately and continued indefinitely, clopidogrel if patient aspirin intolerant ii. Parenteral anticoagulation regardless of treatment strategy iii. DAPT started upon presentation in patients in whom early invasive strategy selected 1) P2Y 12 inhibitor loading dose + aspirin loading dose maintenance doses 2) Reasonable to use ticagrelor over clopidogrel, and prasugrel reasonable over clopidogrel in patients at low bleed risk without history of stroke or TIA Percutaneous Coronary Intervention I. PCI & Stents a. PCI goal: open narrowed or blocked coronary arteries due to atherosclerotic plaques to restore blood flow to the heart, relieve symptoms, and reduce ischemia 23,24 i. Performed during cardiac catheterization ii. Tube with balloon or another device inserted into vessel, deployed, and stent placed b. Stenting insertion of a metallic mesh tube to keep the artery open i. Stent types: BMS and DES 24 ii. Potential complications: bleeding, vessel damage, thrombosis, arrhythmias, and stroke II. DAPT Duration Debate Guideline Recommendations a. Older guidelines recommend P2Y 12 inhibitor for 12 months 21 i. 12 months BMS, at least 30 days ii. 12 months DES b. Newer guidelines provide guidance for shortening or extending DAPT duration 5 i. Shorter duration in patients with higher risk of bleeding ii. Longer duration in patients with higher risk of clot and ischemia c. In patients on DAPT with high bleed risk, such as those on oral anticoagulation, reasonable to discontinue P2Y 12 inhibitor after 6 months 5 Clinical Controversy: DOACs in Patients with AF Undergoing PCI Past Literature Review Table 4: Subgroup Analyses of DOAC AF Trials Study Summary Conclusions Analyzed apixaban vs. warfarin with concomitant aspirin in patients with AF Apixaban ARISTOTLE 25 Dabigatran RE-LY 26 Assessed efficacy and safety of dabigatran vs. warfarin in patients who did and did not Higher major bleed rates overall, but even with concomitant aspirin, apixaban showed significantly less bleeding and retained beneficial effects on SSE vs. warfarin Aspirin + apixaban vs. warfarin nonsignificantly higher MI Antiplatelet therapy had little effect on dabigatran s advantages over warfarin; similar increase in bleed risk seen with dabigatran and warfarin SARAH HALLOWELL 8
9 Edoxaban ENGAGE AF- TIMI Rivaroxaban ROCKET AF 28 receive concomitant antiplatelet therapy Evaluated effects of single antiplatelet agent on edoxaban efficacy and safety Assessed DAPT use and associated outcomes in patients who underwent PCI Dabigatran 110 mg safer for major bleed and equally effective in lowering SSE risk vs. warfarin regardless of antiplatelet therapy Dabigatran 150 mg similar major bleed risk vs. warfarin, but benefit in SSE possibly attenuated by concomitant antiplatelet use Antiplatelet therapy + edoxaban significantly greater bleed risk but no alteration in relatively increased safety and efficacy of edoxaban over warfarin Increased event rates of SSE, MI, and bleeding in patients on DAPT + rivaroxaban compared with warfarin Table 5: DOACs in ACS Trials Study Summary Conclusions Apixaban APPRAISE 29 APPRAISE-2 30 RE-DEEM 31 ATLAS ACS- TIMI ATLAS ACS- 2-TIMI Phase II, placebo-controlled, apixaban dose-ranging study in patients with recent ACS on concomitant single or DAPT Phase III, placebo-controlled trial of apixaban 5 mg BID vs. placebo + DAPT in high risk recent ACS patients Double blind, placebo controlled, dose escalation trial of dabigatran + DAPT vs. placebo post-acs Phase II, double-blind, multicenter, dose-escalation trial of rivaroxaban in patients post-acs Phase III, placebo-controlled trial of DAPT + rivaroxaban 2.5 mg or 5 mg BID or placebo in patients with recent ACS Dose dependent increase in major or clinically relevant nonmajor bleeding not significant for 2.5 mg BID only More bleeding and ischemic event reduction on DAPT vs. aspirin alone Discontinued prematurely due to significantly increased major bleeding without a reduction in ischemic events more intracranial and fatal bleeding with apixaban vs. placebo Dabigatran Linear increase in major or clinically relevant bleeding with dose, and numerically lower incidence of CV death, nonfatal MI, or non-hemorrhagic stroke composite endpoint with dabigatran vs. placebo Higher incidence of non-fatal MI with dabigatran Highest incidence of severe recurrent ischemia with dabigatran 150 mg, and highest incidence of major or clinically relevant bleeding with dabigatran 110 mg Rivaroxaban Dose dependent increase in clinically significant bleeding but significant reduction in death, MI, or stroke with rivaroxaban Lowest bleeding with 2.5 mg BID + single or DAPT Lowest event rates with 2.5 mg BID and 5 mg BID + DAPT Significant reduction in CV death, MI, and stroke, significant increase in major bleed and intracranial hemorrhage rates, and nonsignificant increase in fatal and minor bleeding with rivaroxaban vs. warfarin Significant decrease in fatal bleeds, minor bleeding, and bleeding requiring medical attention with 2.5 mg BID SARAH HALLOWELL 9
10 Major Trials I. Rivaroxaban PIONEER AF-PCI: Gibson CM, Mehran R, Bode C, et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N Engl J Med. 2016; 375(25): doi: /NEJMoa Purpose Compare the safety and efficacy of different treatment strategies after PCI with stent placement in patients with paroxysmal, persistent, or permanent NVAF Study Design Open-label, randomized, controlled, multicenter, international trial Duration of DAPT and P2Y 12 inhibitor prespecified by investigator prior to randomization Patients randomized 1:1:1 to groups Group 1 Low Dose Group 2 Very Low Dose Group 3 Standard Therapy Rivaroxaban 15 mg Rivaroxaban 2.5 mg BID + DAPT Warfarin daily + DAPT daily* + P2Y 12 Low dose aspirin for 12 months Adjusted to INR inhibitor P2Y 12 inhibitor for specified Low dose aspirin for 12 P2Y 12 inhibitor DAPT duration months for 12 months Patients in 1 and 6 month P2Y 12 inhibitor for groups switched to 15 mg daily specified DAPT duration for remainder of 12 months* P2Y 12 inhibitors: clopidogrel 75 mg daily, ticagrelor 90 mg BID, or prasugrel 10 mg daily** given for DAPT durations of 1, 6, or 12 months in groups 2 and 3 Patient Population Endpoints Statistics Inclusion: patients age 18 years with NVAF who had undergone PCI AF documented within 1 year prior to screening or documented > 1 year prior if patient receiving oral anticoagulation 3 months before PCI *10 mg if patient s CrCl between ml/min ** Ticagrelor and prasugrel used in 15% of patients Exclusion: History of stroke/tia Clinically significant GI bleed within 12 months CrCl < 30 ml/min Unknown cause anemia, hemoglobin < 10 g/dl Condition with increased risk for bleeding Primary endpoint: clinically significant bleeding composite of Thrombolysis in Myocardial Infarction (TIMI) criteria major and minor bleeding and bleeding requiring medical attention Secondary endpoints: Incidence of individual primary endpoint components Efficacy endpoints: composite major adverse CV events (composite of death from CV causes, stroke, or MI), individual components of CV event endpoint, and stent thrombosis Analyses performed on pooled data including all DAPT durations within treatment groups Modified intention to treat analyses based on data for all patients who underwent randomization and received at least one dose of trial drug during treatment period Cox proportional hazards model: analyze time from first dose to first occurrence of primary safety event, provide hazard ratio (HR) and two-sided 95% confidence interval (CI) Kaplan-Meier method: cumulative event rates estimated at 360 days, P values calculated using two-sided log-rank test SARAH HALLOWELL 10
11 Results Baseline Characteristics: 2124 patients stratified between May 2013 through July 2015 Predominantly white males, average age 70 years, most common CHA 2DS 2-VASc scores 3-5 for all groups no major between group differences o Fewer than 10% enrolled in North America o P2Y 12 inhibitors: clopidogrel used in ~93-96% o Warfarin mean percentage of time in the therapeutic range: 65.0% Outcomes: Safety Outcomes: % of Participants with Events, HR (95% CI) Primary: Clinically Significant Bleeding Major Bleeding Minor Bleeding Bleeding Requiring Medical Attention Low dose (n=696) vs. Standard (n=697) 16.8 vs ( ) 2.1 vs ( ) 1.1 vs ( ) 14.6 vs ( ) P value <0.001* <0.001* Very low dose (n=706) vs. Standard (n=697) 18.0 vs ( ) 2.0 vs ( ) 1.1 vs ( ) 15.8 vs ( ) P value <0.001* <0.001* Efficacy: no significance difference for any events with either rivaroxaban group vs. warfarin Power to detect 15% lower risk in rivaroxaban group = 11.4% Author s Conclusions DAPT: Clinically Significant Bleeding by Duration of DAPT: Event Rates, HR (95% CI) Very low dose vs. Standard P value Patients assigned to 1 month DAPT 19.4 vs. 25.7, 0.68 ( ) 0.20 Patients assigned to 6 months DAPT 17.5 vs. 31.2, 0.51 ( ) <0.001* Patients assigned to 12 months DAPT 17.9 vs. 23.9, 0.74 ( ) 0.08 Efficacy composite event remained nonsignificant across all DAPT stratifications o 12-month DAPT group: narrowest CIs MI 2.3 vs. 4.8, 0.44 ( ), P=0.07 o 6-month DAPT group: % patients with events higher across all endpoints Stroke 2.7 vs. 0, P=0.02 Additional Findings: significantly lower permanent discontinuation rate prior to scheduled termination date with both rivaroxaban groups vs. warfarin (P<0.001, both comparisons) Administration of either low dose rivaroxaban + P2Y 12 inhibitor for 12 months or very low dose rivaroxaban + DAPT for 1, 6, 12 months was associated with lower rate of clinically significant bleeding vs. standard therapy warfarin + DAPT for 1, 6, 12 months, with similar efficacy rates Limitations: Few secondary efficacy endpoints not powered for noninferiority or superiority, broad CIs Trial underpowered individual efficacy outcomes power between %, would need ~40,794 patients total to detect 15% event difference 2.5 BID ACS CV event prevention indication only in some countries, 15 mg and 10 mg in renal dysfunction daily doses not approved in ACS or AF DAPT stratification by clinician choice baseline characteristics unbalanced SARAH HALLOWELL 11
12 Critique Take Away Strengths: First trial directly comparing DOAC with standard therapy in patient with NVAF undergoing PCI Well-designed trial evaluating multiple dosing strategies of rivaroxaban Limitations: Little insights regarding efficacy No insight on DAPT duration Dosages not available or indicated in US Excluded high risk patients and those with decreased renal function Few US patients Sheds light on bleeding-related safety of two dosing strategies of rivaroxaban with antiplatelet agents, but questions of efficacy of these non-fda approved dosing strategies remain PIONEER Post-hoc: Gibson CM, Pinto DS, Chi G, et al. Recurrent hospitalization among patients with atrial fibrillation undergoing intracoronary stenting treated with 2 treatment strategies of rivaroxaban or a dose adjusted oral vitamin K antagonist treatment strategy. Circulation. 2017; 135: doi: /CIRCULATIONAHA Purpose Assess whether low dose rivaroxaban + P2Y 12 inhibitor or very low dose rivaroxaban + DAPT Study Design Patient Population Endpoints Statistics Results could reduce bleeding and, therefore, favorably impact all-cause mortality or rehospitalization Non-prespecified, post-hoc analysis of patients in the PIONEER AF-PCI trial Group 1 Low Dose Group 2 Very Low Dose Group 3 Standard Rivaroxaban 15 mg daily + Rivaroxaban 2.5 mg BID + DAPT Warfarin daily + DAPT P2Y 12 inhibitor Same as PIONEER AF-PCI trial patients with NVAF who had undergone PCI Primary endpoint: all-cause mortality or recurrent hospitalization for an adverse event (AE) AEs classified by investigators using International Conference on Harmonization guidelines Those leading to hospitalization included in study and classified as a result of bleeding, CV cause, or other cause blinded to treatment assignment Patients receiving 1 dose of study drug included analyzed as-treated, DAPT strata pooled Groups compared via two specific, simultaneous pair-wise comparisons without adjustment Cox proportional hazard model: HR and 95% CI to compare time from first study drug dose to first occurrence of all-cause death or hospitalization for AE treatment group covariate Kaplan-Meier method: summarize cumulative event rates at 360 days Baseline characteristics: 2124 patients well-matched, no significant between group differences Outcomes: Risk of All-Cause Mortality or Rehospitalization: % risk, HR (95% CI) All-Cause Mortality or Rehospitalization for Any Cause Low dose vs. Standard 34.9 vs ( ) P value 0.008*, NNT = 15 Very low dose vs. Standard 31.9 vs ( ) P value 0.002*, NNT = 10 Significance retained for all-cause mortality or rehospitalization due to bleeding or CV cause, due to bleeding alone, and due to CV cause alone No difference in other all-cause death or recurrent hospitalization, all-cause death alone No significant differences between low dose or very low dose rivaroxaban groups SARAH HALLOWELL 12
13 Author s Conclusions Critique Take Away First Recurrent Hospitalization: % events, HR (95% CI) Low dose vs. P value Very low dose vs. Standard P value Standard Overall 34.1 vs vs * 0.001* Rehospitalization 0.77 ( ) 0.74 ( ) Significance retained for rehospitalization for bleeding or CV cause, bleeding, or CV cause AEs: severe bleeding adverse events reduced in low dose (P=0.021) and very low dose (P=0.003) Administration of either strategy of rivaroxaban associated with reduced risk of all-cause mortality or recurrent hospitalization for adverse events compared with standard of care Results added strength to PIONEER AF-PCI trial and suggests potential for improved value Rehospitalization greater sensitivity, less specificity than original efficacy endpoints greater power (90%) to observe 20% difference between groups All-cause death and rehospitalization as endpoints are objective, comprehensive endpoints Limitations: Post-hoc analysis, no multiplicity testing adjustment, method of event allocation not a priori Only generalizable to PIONEER AF-PCI population and clopidogrel Rivaroxaban 2.5 mg not available/indicated in all countries, including US Bias to admit more patients on open-label warfarin therapy Strengths: Limitations: Adequately powered, more sensitive Non-prespecified analysis, inclusion of endpoints DAPT analysis questionable Analyzed relevant rehospitalization causes Justification for lack of original efficacy and Sought to demonstrate clinical significance new endpoints of previous findings Limited generalizability Provides insight into clinical relevance of bleeding reduction with rivaroxaban but little in the way of understanding efficacy of these lower doses of rivaroxaban in reducing thrombosis risk true balance in bleeds vs. clots remains uncertain II. Dabigatran RE-DUAL PCI: Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. [Epub ahead of print August 27, 2017]. N Engl J Med doi: /NEJMoa Purpose Compare use of two regimens of dual antithrombotic therapy with dabigatran etexilate (DE) with Study Design warfarin triple antithrombotic therapy among patients with AF undergoing PCI Randomized, open-label, multicenter, international, controlled noninferiority trial Patients randomized by permuted blocks, stratified by age and region 1:1:1 ratio to: Group 1 Group 2 Group 3 DE 110 Dual Therapy DE 150 Dual Therapy Triple Therapy DE 110 mg BID + DE 150 mg BID + P2Y 12 Warfarin** daily + P2Y 12 inhibitor for 12 P2Y 12 inhibitor* 12 inhibitor* 12 months months + aspirin discontinued after 1 months month with BMS and 3 months with DES Continued until patients had 6 month of follow up, target number of events reached * Clopidogrel 75 mg daily or ticagrelor 90 mg BID ** Adjusted to INR SARAH HALLOWELL 13
14 Patient Population Endpoints Inclusion patients 18 years with NVAF who underwent PCI in previous 120 hours Eligible regardless of whether or not on oral anticoagulant prior to PCI ACS or stable CAD as PCI indications Exclusion NVAF due to reversible disorder without anticipated long-term anticoagulation Severe renal insufficiency (CrCl < 30 ml/min) Other major coexisting conditions Primary Safety Endpoint: first major or clinically relevant nonmajor International Society on Thrombosis and Haemostasis (ISTH) bleeding event Secondary: Composite efficacy: thromboembolic events (MI, SSE), death, unplanned revascularization Combined endpoint of thrombotic events or death, individual events, and stent thrombosis Statistics Primary analysis: intention-to-treat for all patients randomized Noninferiority margin: upper limit (UL) of 95% confidence interval = 1.38 Estimated sample size: 2500 patients assumed primary endpoint 14% event rate per group, 83.6% power for noninferiority, one-sided alpha of Cox proportional-hazards model for primary endpoint Initial protocol: planned for coprimary endpoint comparison of thromboembolic event rates Changed to secondary, sample size changed from 8520 to 2500 Results Baseline characteristics: 2725 patients randomized between July 2014 through October 2016 Mean age 70.8, predominantly male, average CHA 2DS 2-VASc score 3.6 and HAS-BLED 2.7 o Warfarin group higher rate of previous stroke o P2Y 12 inhibitor: 88% clopidogrel o Warfarin mean percentage of time with therapeutic INR: 64% Outcomes: Safety: Event Rate %, HR (95% CI) First major or clinically relevant nonmajor bleeding event Intracranial hemorrhage DE 110 (n=981) vs. Triple (n=981) 15.4 vs ( ) 0.3 vs ( ) P value <0.001* noninferiority and superiority 0.06 DE 150 (n=763) vs. Triple (n=764) 20.2 vs ( ) 0.1 vs ( ) P value <0.001* noninferiority, <0.002* superiority 0.047* Efficacy: Event Rate %, HR (95% CI) Main composite efficacy endpoint: DE 110 and DE 150 (n=1744) vs. triple (n=981): 13.7 vs. 13.4, 1.04 ( ), P=0.005 for noninferiority, P=0.74 for superiority Secondary composite efficacy endpoint: thromboembolic events or death DE 110 and DE 150 vs. triple: 9.6 vs. 8.5, 1.17 ( ), P=0.11 for noninferiority, P=0.25 superiority DE 110 (n=981) vs. DE 150 (n=763) vs. P value Triple (n=981) Triple (n=764) P value Composite efficacy 15.2 vs vs endpoint 1.13 ( ) 0.89 ( ) 0.44 Thromboembolic 11.0 vs vs events or death 1.30 ( ) 0.97 ( ) 0.88 MI 4.5 vs vs ( ) 1.16 ( ) 0.61 Trend favoring triple therapy No significant difference in DE groups for death, stroke, or definite stent thrombosis SARAH HALLOWELL 14
15 Author s Conclusions Critique Take Away Other findings: Serious AEs: 42.7% DE 110, 39.6% DE 150, and 41.8% triple therapy Fatal serious AEs: 3.9% DE 110, 3.2% DE 150, and 4.3% triple therapy Premature discontinuation: 13.3% DE 110, 13% DE 150, and 16.6% triple therapy Risk of bleeding lower with dual therapy with dabigatran + P2Y 12 vs. triple therapy with warfarin + P2Y 12 + aspirin; dual therapy noninferior for risk of thromboembolic events reaffirms safety and net clinical benefit of DE regimens and supports changes in guidelines DE 110 significantly lower major bleeding, nonsignificantly higher thromboembolic events DE 150 significantly lower major bleeding, nonsignificantly lower thromboembolic events Limitations: Not powered for individual endpoints and amended protocol Combined DE groups for efficacy to get 83.6% power Noninferiority margin used for SSE in AF trials Can only speculate on impact of aspirin omissions in safety and efficacy outcomes Strengths: Limitations: Tested multiple dosing strategies with Combined DE groups to show composite NVAF approved doses efficacy endpoint noninferiority Tested omission of aspirin and found MI rates higher with DE, especially DE 110 higher bleeding rates even with Lack of power for individual endpoints shortened duration of aspirin Questionable claims about DE 110 clinical Slightly more efficacy insight to be benefit, effectiveness, and safety gleamed vs. PIONEER AF-PCI DE dual therapy superior to classic triple therapy with warfarin for bleeding Questions about effectiveness and even safety of DE 110 dual therapy Ultimately favors DE 150 dual therapy for superior bleeding and noninferior efficacy Future Studies Apixaban and Edoxaban Trial Apixaban AUGUSTUS 37 Apixaban SAFE-A 38 Edoxaban ENTRUST- AF-PCI 39 Design & Endpoints An open-label, 2 x 2 factorial, randomized controlled trial evaluating safety of apixaban 5 mg or 2.5 mg BID vs. warfarin, as well as aspirin vs. placebo in patients with AF and ACS or PCI Primary: time to first occurrence of major or clinically relevant nonmajor bleeding with apixaban vs. warfarin, with no aspirin vs. aspirin Secondary: apixaban vs. warfarin superiority for major and clinically relevant nonmajor bleeding, composite endpoints of death and ischemic events, and first any cause rehospitalization Multicenter, prospective, randomized, open-label, blinded-endpoint, parallel-group, comparative study of safety and efficacy of 1-month and 6 months of P2Y 12 inhibitor plus 12 months of aspirin and apixaban 5 mg BID in patients with NVAF undergoing PCI with DESs Primary: incidence of bleeding occurrences in 12 months Secondary: composite of all-cause death, MI, SSE, net clinical benefit, and individual endpoints Open-label, randomized clinical trial to evaluate safety and efficacy of edoxaban-based antithrombotic regimen (60 mg daily) vs. warfarin-based antithrombotic regimen in patients with AF post-pci with stent placement Primary: incidence of major or clinically relevant nonmajor ISTH-defined bleeding Secondary: composite of CV death, SSE, MI, and stent thrombosis events SARAH HALLOWELL 15
16 Summary, Conclusion, and Recommendations I. Summary: a. In patients with AF undergoing PCI, goal is balance between thrombosis and bleed risk b. Triple therapy with warfarin + aspirin + clopidogrel is the historical standard of care c. Triple therapy holds an inherently increased risk of bleeding d. Shifting paradigms are increasing the use of DOACs in the management of NVAF ease of use and reduction in risk of bleeding compared to warfarin i. Increasing number of patients coming into the hospital on a DOAC requiring PCI ii. Increased push from clinicians to utilize these newer medications as literature accumulates II. Conclusions & Recommendations: a. Is it time to change our paradigm? i. No overall, definitive conclusion to move to utilization of DOACs in all patients with NVAF undergoing PCI can be made based on evidence available to date 1) Good evidence for decreased bleeding, noninferior efficacy with single strategy of single DOAC dabigatran 150 dual therapy a) Requires additional research into trend towards increased MI b) Only generalizable to patient population used in RE-DUAL 2) Insufficient evidence to recommend any other DOAC ii. Certain situations exist in which a DOAC, specifically dabigatran, should be considered b. Recommendations i. Patients admitted therapeutic on warfarin consider patient s lifestyle, compliance, preferences, and bleed risk and history 1) Patient prefers warfarin, no compliance or lifestyle barriers, and has lower bleed risk continue warfarin targeting INR between ) Patient would prefer less monitoring, has lifestyle barriers, and has higher bleed risk dabigatran 150 dual therapy ii. Patients not therapeutic on warfarin or with difficulty complying with INR monitoring dabigatran 150 dual therapy iii. Patients admitted on DOAC for PCI depends on DOAC 1) Edoxaban: not enough data to recommend continuation change anticoagulant 2) Apixaban: increased risk of bleeding with apixaban + DAPT in ACS trials and questionable trend towards increased MI in patients on aspirin + apixaban in ARISTOTLE subgroup analysis leaves questions of safety change anticoagulant 3) Rivaroxaban: based on lack of efficacy conclusions from PIONEER change anticoagulant 4) Dabigatran: based on RE-DUAL s safety and noninferior efficacy continue dabigatran 150 mg and start clopidogrel iv. Initiating new anticoagulant post-pci 1) Assess patient s stroke, bleed, and ACS event risks, as well as preference, likely compliance, and lifestyle a) Patient with higher bleed risk dabigatran 150 dual therapy or warfarin + clopidogrel with decision based on patient factors and preference b) Patient with lower bleed risk dabigatran 150 dual therapy or warfarin triple therapy with decision based on patient factors and preference v. Patients with renal dysfunction, either stable or recent onset warfarin triple therapy targeting INR between SARAH HALLOWELL 16
17 References 1. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics: 2016 update: a report from the American Heart Association. Circulation. 2016; 133(4): e doi: /cir January CT, Wann LS, Alpert JS, et al AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2014; 64(21): e1-76. doi: /j.jacc Eisen A, Giugliano RP, Braunwald E. Updates on acute coronary syndrome: a review. JAMA Cardiol. 2016; 1(6): doi: /jamacardio Cho JR, Angiolillo DJ. Percutaneous coronary intervention and atrial fibrillation: the triple therapy dilemma. J Thromb Thrombolysis. 2015; 39(2): doi: /s z. 5. Levine GN, Bates ER, Bittl JA, et al ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016; 68(10): doi: /j.jacc Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011; 365(11): doi: /NEJMoa Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009; 361(12): doi: /NEJMoa Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013; 369(22): doi: /NEJMoa Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011; 365(10): doi: /NEJMoa Lexi-Drugs. Lexicomp. Wolters Kluwer Health, Inc. Riverwoods, IL. Accessed September 4, You JJ, Singer DE, Howard PA, et al. Antithrombotic therapy for atrial fibrillation antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012; 141(2): e531s-75s. doi: /chest Lip GYH, Windecker S, Huber K, et al. Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology Working Group on Thrombosis, European Heart Rhythm Association (EHRA), European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS). Eur Heart J. 2014; 35: doi: /eurheartj/ehu Kirchhof P, Benussi S, Kotecha D, et al ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37: doi: /eurheartj/ehw Steg PG, Bhatt DL. Viewpoint: a proposal for a simple algorithm for managing oral anticoagulation and antiplatelet therapy in patients with non-valvular atrial fibrillation and coronary stents. Eur Heart J Acute Cardiovasc Care. 2017; 6(1): doi: / Kumar A, Cannon CP. Acute coronary syndromes: diagnosis and management, part I. Mayo Clinic Proceedings. 2009; 84(10): doi: /S (11) Théroux P, Fuster V. Acute coronary syndromes: unstable angina and non Q-wave myocardial infarction. Circulation. 1998; 97(12): doi: /01.CIR Braunwald E. Unstable angina: an etiologic approach to management. Circulation. 1998; 98(21): doi: /01.CIR American Heart Association. Acute coronary syndrome. American Heart Association. Syndrome_UCM_428752_Article.jsp#.WdKI6zYUkdU. Updated April 26, Accessed September 4, Grass AW, Brener SJ. Complications of acute myocardial infarction. Cleveland Clinic Disease Management. Updated Accessed September 16, O Gara PT, Kushner FG, Ascheim DD, et al ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013; 61(4): e doi: /j.jacc SARAH HALLOWELL 17
18 21. Levine GN, Bates ER, Blankeship JC, et al ACCF/AHA/SCAI guideline for percutaneous coronary intervention: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011; 58: e doi: /CIR.0b013e31823ba Amsterdam EA, Wenger NK, Brindis RG, et al AHA/ACC guideline for the management of patients with non STelevation acute coronary syndromes: executive summary a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014; 130(25): doi: /j.jacc National Heart, Lung, and Blood Institute. Percutaneous coronary intervention. National Institutes of Health. Updated December 9, Accessed September 4, National Heart, Lung, and Blood Institute. Stents. National Institutes of Health. gov/health/healthtopics/topics/stents. Updated December 17, Accessed September 4, Alexander JH, Lopes RD, Thomas L, et al. Apixaban vs. warfarin with concomitant aspirin in patients with atrial fibrillation: insights from the ARISTOTLE trial. Eur Heart J. 2014; 35: doi: /eurheartj/eht Dans AL, Connolly SJ, Wallentin L, et al. Concomitant use of antiplatelet therapy with dabigatran or warfarin in the randomized evaluation of long-term anticoagulation therapy (RE-LY) trial. Circulation. 2013; 127: doi: /CIRCULATIONAHA Xu H, Ruff CT, Giugliano RP, et al. Concomitant use of single antiplatelet therapy with edoxaban or warfarin in patients with atrial fibrillation: analysis from the ENGAGE AF-TIMI48 trial. J Am Heart Assoc. 2016; 5(2): e doi: /JAHA Sherwood MW, Cyr DD, Jones WS, et al. Use of dual antiplatelet therapy and patient outcomes in those undergoing percutaneous coronary intervention: the ROCKET AF trial. JACC Cardiovasc Interv. 2016; 9(16): doi: /j.jcin APPRAISE Steering Committee and Investigators. Apixaban, an oral, direct, selective factor Xa inhibitor, in combination with antiplatelet therapy after acute coronary syndrome: results of the apixaban for prevention of acute ischemic and safety events (APPRAISE) trial. Circulation. 2009; 119: doi: /CIRCULATIONAHA Alexander JH, Lopes RD, James S, et al. Apixaban with antiplatelet therapy after acute coronary syndrome. N Engl J Med. 2011; 365(8): doi: /NEJMoa Oldgren J, Budaj A, Granger CB, et al. Dabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trial. Eur Heart J. 2011; 32(22): doi: /eurheartj/ehr Mega JL, Braunwald E, Mohanavelu S, et al. Rivaroxaban versus placebo in patients with acute coronary syndromes (ATLAS ACS-TIMI 46): a randomized, double-blind, phase II trial. Lancet. 2009; 374: doi: /S (09) Mega JL, Braunwald E, Wiviott SD, et al. Rivaroxaban in patients with a recent acute coronary syndrome. N Engl J Med. 2012; 366(1): doi: /NEJMoa Gibson CM, Mehran R, Bode C, et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. N Engl J Med. 2016; 375(25): doi: /NEJMoa Gibson CM, Pinto DS, Chi G, et al. Recurrent hospitalization among patients with atrial fibrillation undergoing intracoronary stenting treated with 2 treatment strategies of rivaroxaban or a dose adjusted oral vitamin K antagonist treatment strategy. Circulation. 2017; 135: doi: /CIRCULATIONAHA Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med [Epub ahead of print]. doi: /NEJMoa Bristol-Myers Squibb. An open-label, 2 x 2 factorial, randomized controlled, clinical trial to evaluate the safety of apixaban vs. vitamin k antagonist and aspirin vs. aspirin placebo in patients with atrial fibrillation and acute coronary syndrome or percutaneous coronary intervention. Available at: NCT ClinicalTrials.gov identifier: NCT Accessed September 4, Hoshi T, Sato A, Nogami A, Gosho M, Aonuma K. Rationale and design of the SAFE-A study: SAFety and Effectiveness trial of Apixaban use in association with dual antiplatelet therapy in patients with atrial fibrillation undergoing percutaneous coronary intervention. Journal of Cardiology. 2017; 69(4): doi: /j.jjcc Daiichi Sankyo, Inc. Edoxaban treatment versus vitamin K antagonist in patients with atrial fibrillation undergoing percutaneous coronary intervention (ENTRUST-AF-PCI). Available at: NCT ClinicalTrials.gov Identifier: NCT Accessed October 1, SARAH HALLOWELL 18

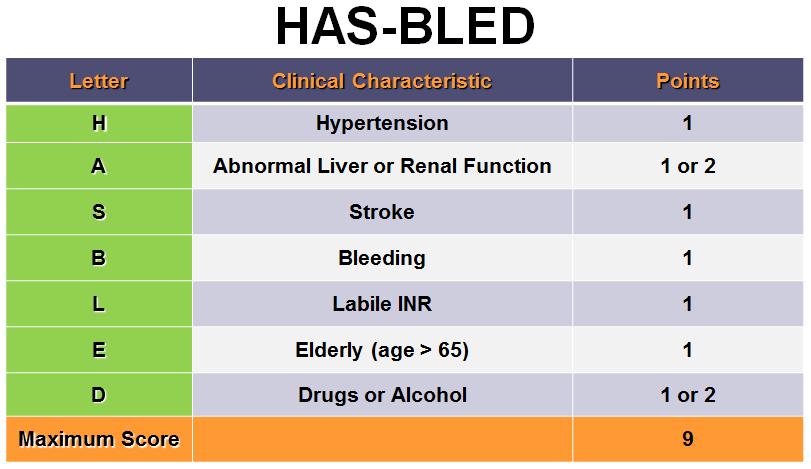
19 Appendices Appendix A CHA2DS2-VASc 13 and HAS-BLED scores
20 Appendix B DOACs in AF Apixaban ARISTOTLE 6 Table 1: Summary of Direct Oral Anticoagulant NVAF Trials 6-9 Study Endpoints Results Primary efficacy: SSE Primary efficacy outcome: apixaban superior Primary safety: major bleeding Major bleeding: apixaban superior Other: death from any cause, MI Death from any cause: apixaban superior UL 95% CI for noninferiority: 1.38 MI: numerically lower event rate with apixaban Double blind, double dummy noninferiority trial of apixaban 5 mg BID vs. warfarin (N=18,2011) Dabigatran RE-LY 7 Blinded noninferiority trial of DE 110 mg or 150 mg vs. warfarin in SSE prevention (N=18,113) Edoxaban ENGAGE AF-TIMI 48 8 Double-blind, double-dummy noninferiority trial of edoxaban 60 mg or 30 mg daily vs. warfarin (N=21,105) Rivaroxaban ROCKET AF 9 Double blind noninferiority trial of rivaroxaban 20 mg daily vs. warfarin (N=14,264) Primary efficacy: SSE Primary safety: major hemorrhage Secondary: SSE and death Other: MI, bleeding Upper limit 95% CI for noninferiority: 1.46 Primary efficacy: SSE Principle safety: major bleeding Other: death from CV cause, ischemic stroke, GI bleeding UL 97.5% CI for noninferiority: 1.38 Primary efficacy: SSE Principle safety: composite of major and nonmajor clinically relevant bleeding events Other: other bleeding measures UL 95% CI for noninferiority: 1.46 Primary efficacy outcome: DE 110 mg noninferior, DE 150 mg superior Major hemorrhage: DE both doses superior MI: DE 110 mg nonsignificantly and DE 150 mg significantly higher Bleeding: significantly lower rate of major bleed with DE 110 mg, and significantly lower rates of life-threatening bleeding, intracranial bleeding, and major or minor bleeding with DE Dose comparison: Greater SSE reduction with DE 150 mg Primary efficacy outcome: edoxaban 60 mg superior, edoxaban 30 mg noninferior Major bleeding: significantly lower in both edoxaban groups Death from CV causes: lower rates with edoxaban Ischemic stroke: equal with edoxaban 60 mg, significantly higher with edoxaban 30 mg GI bleeding: significantly higher with edoxaban 60 mg Comparison of doses: edoxaban 60 mg lower primary outcome Primary efficacy outcome: per protocol annual event rate with rivaroxaban noninferior ITT efficacy: rivaroxaban noninferior, not superior Safety population efficacy for superiority: rivaroxaban superior Principle safety: rivaroxaban numerically higher than warfarin Other: similar rates of major bleeding, significant reductions in intracranial hemorrhage and fatal bleeding, significantly more major GI bleeding, significantly greater decrease in hemoglobin 2 g/dl, and significantly higher transfusion rates with rivaroxaban SARAH HALLOWELL 20
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Xarelto (rivaroxaban)
") Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Xarelto (rivaroxaban) Policy Number: 5.01.575 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Xarelto
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Stable CAD, Elective Stenting and AFib
 Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Study design: multicenter, randomized, open-label trial following a PROBE design
 Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Oral Anticoagulation Drug Class Prior Authorization Protocol
 Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Oral Anticoagulation Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
ACCP Cardiology PRN Journal Club 1 Non-Vitamin K Antagonist Oral Anticoagulants in Patients with Atrial Fibrillation and Valvular Heart Disease Cody A. Carson, PharmD, BCPS PGY2 Cardiology Pharmacy Resident
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
What s new with DOACs? Defining place in therapy for edoxaban &
 What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
What s new with DOACs? Defining place in therapy for edoxaban & Use of DOACs in cardioversion Caitlin M. Gibson, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy University of North Texas
Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου
, FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου") Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018 Disclosures: None Primary efficacy outcome* (%/year) Antiplatelet Therapy
Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018 Disclosures: None Primary efficacy outcome* (%/year) Antiplatelet Therapy
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015
 Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Atrial Fibrillation: Risk Stratification and Treatment New Cardiovascular Horizons St. Louis September 19, 2015 Christopher E. Bauer, MD, FACC, FHRS SSM Health Heart & Vascular Care Clinical Cardiac Electrophysiology
Drug Class Monograph
 Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Drug Class Monograph Class: Oral Anticoagulants Drug: Coumadin (warfarin), Eliquis (apixaban), Pradaxa (dabigatran), Savaysa (edoxaban), arelto (rivaroxaban) Formulary Medications: Eliquis (apixaban),
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원
 Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Pradaxa (dabigatran)
") Pradaxa (dabigatran) Policy Number: 5.01.574 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Pradaxa
Pradaxa (dabigatran) Policy Number: 5.01.574 Last Review: 7/2018 Origination: 6/2014 Next Review: 7/2019 LoB: ACA Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Pradaxa
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA
 INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
INR as a Biomarker: Anticoagulation in Atrial Fib, Heart Failure, and Cardiovascular Disease Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular
Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy
 Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central
Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central
Atrial Fibrillation. Alan Bell, MD, CCFP. Staff Physician, Humber River Regional Hospital. University of Toronto
 Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy
 Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central
Should It Stay or Should It Go? Aspirin Therapy for Patients with Stable CAD Post MI/TIA with Atrial Fibrillation on Concurrent DOAC Therapy Erin R. Pilcher, Pharm.D. PGY1 Pharmacy Practice Resident Central
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease
 Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Practical Considerations for Using Oral Anticoagulants in Patients with Chronic Kidney Disease Cyrille K. Cornelio, Pharm.D. PGY2 Cardiology Pharmacy Resident The University of Oklahoma College of Pharmacy
Results from RE-LY and RELY-ABLE
 Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Results from RE-LY and RELY-ABLE Assessment of the safety and efficacy of dabigatran etexilate (Pradaxa ) in longterm stroke prevention EXECUTIVE SUMMARY Dabigatran etexilate (Pradaxa ) has shown a consistent
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis
 Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA
 Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
Update on the NOAC s: 2018 Daniel Blanchard, MD, FACC, FAHA Professor of Medicine Director, Cardiology Fellowship Program Sulpizio Cardiovascular Center UC San Diego The NOACS, chronologically Dabigatran:
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
ADC Slides for Presentation 02/10/2017
 ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
ADC 2017 Slides for Presentation ANTI THROMBOTIC THERAPY FOR NON VALVULAR ATRIAL FIBRILLATION IN PATIENTS WITH CHRONIC KIDNEY DISEASE: CURRENT VIEWS Martin A. Alpert, MD Brent M. Parker Professor of Medicine
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Edoxaban in Atrial Fibrillation
 Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Edoxaban in Atrial Fibrillation Glenn Gormley, MD, PhD Senior Executive Officer and Global Head of R&D, Daiichi Sankyo Co., Ltd Nov. 4, 2014 Tuesday Background Based on the results of ENGAGE AF-TIMI 48,
Oral Anticoagulants Update. Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation
 Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
Oral Anticoagulants Update Elizabeth Renner, PharmD, BCPS, BCACP, CACP Outpatient Cardiology and Anticoagulation Objectives List the direct oral anticoagulant (DOAC) drugs currently available Describe
controversies in anticoagulation: optimizing outcome for atrial fibrillation
 controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
controversies in anticoagulation: optimizing outcome for atrial fibrillation SUNDAY, NOVEMBER 13, 2016 WESTIN HOTEL NEW ORLEANS CANAL PLACE COLLABORATE INVESTIGATE EDUCATE PROVIDING PERSPECTIVE: CURRENT
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients. Giancarlo Agnelli
 NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
NOAs for stroke prevention in Atrial Fibrillation: potential advantages in the elderly patients Giancarlo Agnelli Internal & Cardiovascular Medicine - Stroke Unit University of Perugia, Italy My talk today
Atrial Fibrillation. 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018
 2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
2 nd Annual National Hospitalist Conference San Antonio, TX September 7, 2018, MSc, FACP, SFHM Division of Hospital Medicine Henry Ford Hospital Detroit, USA Clinical Associate Professor of Medicine Wayne
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely
 Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulation: Novel Agents
 Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Anticoagulation: Novel Agents Scott C. Woller, MD Medical Director, Anticoagulation Management, Intermountain Healthcare Central Region, co-director Venous Thromboembolism Program, Intermountain Medical
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Session 7: Cardiology I and II Answer Explanations
 Session 7: Cardiology I and II Answer Explanations Cardiology I 1. Answer A: Intravenous heparin 4000-unit intravenous bolus, followed by a 1000-unit/hour continuous infusion. The NSTE-ACS guidelines recommend
Session 7: Cardiology I and II Answer Explanations Cardiology I 1. Answer A: Intravenous heparin 4000-unit intravenous bolus, followed by a 1000-unit/hour continuous infusion. The NSTE-ACS guidelines recommend
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia
 6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
6 th ACC-SHA Joint Meeting Jeddah, Saudi Arabia October 31 st - November 1 st, 2015 NOACS vs. Coumadin in Atrial Fibrillation: Is It Worth to Switch? Raed Sweidan, MD, FACC Consultant and Head of Cardiac
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
After acute coronary syndromes patients continue to have recurrent ischemic events despite revascularization and dual antiplatelet therapy
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure?
 The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
North Wales Cardiac Network Guidelines on oral antiplatelet therapy in cardiovascular disease
 Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Lessons from recent antithrombotic studies and trials in atrial fibrillation
 Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
Lessons from recent antithrombotic studies and trials in atrial fibrillation Thromboembolism cause of stroke in AF Lars Wallentin Uppsala Clinical Research Centre (UCR) Uppsala Disclosures for Lars Wallentin
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
A New Era for NOACs: What Does the Future Hold? CME
 This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/884772 www.medscape.org A New Era for NOACs: What Does the Future Hold? CME Manesh
This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/884772 www.medscape.org A New Era for NOACs: What Does the Future Hold? CME Manesh
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained
 Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation
 Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation September 14, 2018 Nina Maguire, PharmD PGY1 Pharmacy Resident Seton Healthcare Family Christina.maguire@ascension.org ASCENSION TEXAS Direct
Direct Oral Anticoagulant Use in Valvular Atrial Fibrillation September 14, 2018 Nina Maguire, PharmD PGY1 Pharmacy Resident Seton Healthcare Family Christina.maguire@ascension.org ASCENSION TEXAS Direct
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES
 Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Pros and Cons of Individual Agents Based on Large Trial Results: RELY, ROCKET, ARISTOTLE, AVERROES Ralph L. Sacco, MS MD FAAN FAHA Olemberg Family Chair in Neurological Disorders Miller Professor of Neurology,
Scoring Systems in AF 8/10/2016. Strategies in the Prevention of Atrial Fibrillation-Related Strokes. Overview
 Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Strategies in the Prevention of Atrial Fibrillation-Related Strokes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania September
Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism
 Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Disclosures Updates in Anticoagulation for Atrial Fibrillation and Venous Thromboembolism No financial conflicts of interest Member of the ABIM Focused- Practice in Hospital Medicine Self Examination Process
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging
 and advances in peri-procedural interruption of anticoagulation-- Bridging") Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Anticoagulation with Direct oral anticoagulants (DOACs) and advances in peri-procedural interruption of anticoagulation-- Bridging Scott C. Woller, MD Co-Director, Thrombosis Program Intermountain Medical
Drug Use Criteria: Direct Oral Anticoagulants
 Texas Vendor Drug Program Drug Use Criteria: Oral Anticoagulants Publication History 1. Developed March 2017. 2. Revised February 2018. Notes: Information on indications for use or diagnosis is assumed
Texas Vendor Drug Program Drug Use Criteria: Oral Anticoagulants Publication History 1. Developed March 2017. 2. Revised February 2018. Notes: Information on indications for use or diagnosis is assumed
TSHP 2014 Annual Seminar 1
 Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Debate: Versus the Rest of the World for Stroke Prevention in Non-valvular Atrial Fibrillation Matthew Wanat, PharmD, BCPS Clinical Assistant Professor University of Houston College of Pharmacy Clinical
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events
 Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome
 State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
Old and New Anticoagulants For Stroke Prevention Benefits and Risks
 Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
Old and New Anticoagulants For Stroke Prevention Benefits and Risks September 15, 2014 Jonathan L. Halperin, M.D. The Cardiovascular Institute Mount Sinai Medical Center Disclosure Relationships with Industry
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction
 Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
Transient Atrial Fibrillation and Risk of Stroke after Acute Myocardial Infarction Doron Aronson MD, Gregory Telman MD, Fadel BahouthMD, Jonathan Lessick MD, DSc and Rema Bishara MD Department of Cardiology
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές
 4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia
 Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Is Apixaban Effective for the Prevention of Stroke in Patients With Non-Valvular Atrial Fibrillation?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 Is Apixaban Effective for the Prevention
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 2014 Is Apixaban Effective for the Prevention
Disclosure. Financial disclosure: National Advisory Board & Research Grant from Boehringer-Ingelheim
 Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Randomised Dabigatran Etexilate Dose Finding Study In Patients With Acute Coronary Syndromes Post Index Event With Additional Risk Factors For Cardiovascular Complications Also Receiving Aspirin and Clopidogrel
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines: