Πποβλημαηιζμοί με ηην ανηιαιμοπεηαλιακή αγωγή ζηο οξύ έμθπαγμα ηος μςοκαπδίος με ανάζπαζη ηος διαζηήμαηορ ST.
|
|
|
- Erika Wilkerson
- 6 years ago
- Views:
Transcription
1 Patras University Hospital Πποβλημαηιζμοί με ηην ανηιαιμοπεηαλιακή αγωγή ζηο οξύ έμθπαγμα ηος μςοκαπδίος με ανάζπαζη ηος διαζηήμαηορ ST. Dimitrios Alexopoulos, MD, FACC, FESC Cardiology Department, Patras University Hospital, Patras, Rio, Greece.
2 Patras University Hospital I, Dimitrios Alexopoulos, have received honoraria for lecturing and research grants from: Astra Zeneca Boeringer Ingelheim

3
4 Platelet activation-impact on surrogate endpoints Clinical studies/ oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital

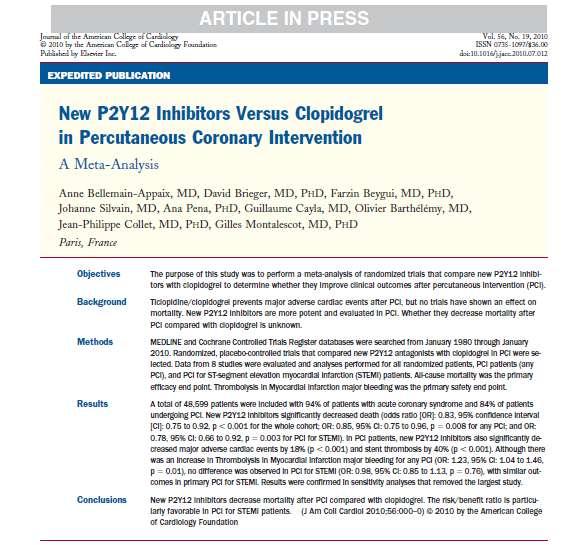
5 Activation of platelets in STEMI and mechanisms influencing adverse clinical outcomes Alexopoulos D, Intern J Cardiol 2011, Dec 20

6 Platelet activation mechanisms in STEMI patients Impact on surrogate end points Alexopoulos D, Xanthopoulou I, Goudevenos I (submitted)
7 Platelet activation-impact on surrogate endpoints Clinical studies/oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital
8 Patras University Hospital Drawbacks of clopidogrel use A marked interindividual response to clopidogrel High platelet reactivity in 1/4 to 1/3 Response to clopidogrel may be influenced by genetic polymorphisms, ethnicity, assay used, timing postloading, age, diabetes mellitus, renal dysfunction, obesity, acuity of the disease, drug-drug interactions, smoking
9 Patras University Hospital However, even after controlling for known factors affecting clopidogrel s pharmacokinetics/ pharmacodynamics, most of their variation remains unexplained Clopidogrel, compared to newer agents- prasugrel and ticagrelor- exhibits a slower onset of action and weaker antiplatelet effect Frelinger AL 3rd, et al J Am Coll Cardiol 2013; 61: Wallentin L, et al Eur Heart J 2008; 29: Gurbel PA,et al Circulation 2009; 120:

10 Patras University Hospital

11 Mehta SR, TCT 2009

12 Patras University Hospital

13 Patras University Hospital

14 Patras University Hospital
15 Proportion of patients (%) Primary EP (CV death, MI and stroke at 15 months) 15 Clopidogrel Prasugrel p=0.002 RRR=32% 10.0 p=0.02 RRR=21% HR=0.79 ( ) NNT=42 Age-adjusted HR=0.81 ( ) Time (Days) Montalescot et al. Lancet 2008 (in press)
16 Patras University Hospital
17 Proportion of patients (%) Patras University Hospital Montalescot et al. Lancet 2008 (in press) TRITON TIMI-38 STEMI cohort TIMI major non-cabg bleeding Clopidogrel Prasugrel p= HR=1.11 ( ) NNH=333 Age-adjusted HR=1.19 ( ) Time (Days)
18
19 TRITON TIMI-38 STEMI cohort Baseline characteristics of patients with Variable primary or secondary PCI Primary PCI (%) Secondary PCI (%) Age (years) p History of diabetes Prior CABG Multivessel PCI GPIIb/IIIa inhibitor Creatinine clear. < 60mL/min Patras University Hospital

20 Patras University Hospital
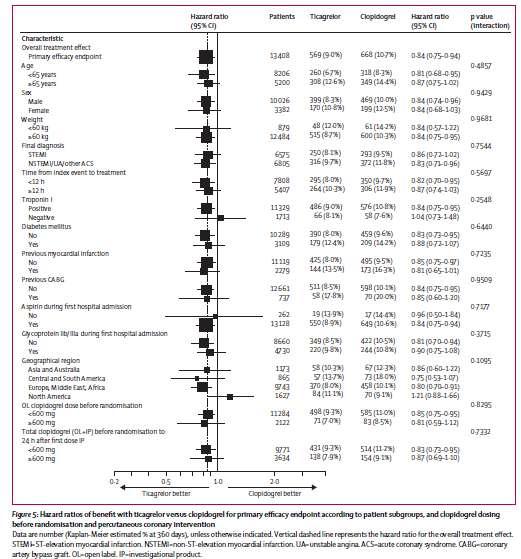
21 Wallentin L, et al. N Engl J Med. 2009;361: and supplementary tables
22 K-M estimated rate (% per year) All cause mortality 7 6 Clopidogrel Ticagrelor HR 0.82 (95% CI = ), p= No. at risk Months Ticagrelor 4,2014,005 3,962 3,876 3,150 2,413 1,993 Clopidogr 4,2294,029 3,989 3,912 3,195 2,471 1,980 el
23 Stent thrombosis (as per ARC definitions)* Ticagrelor (n=4,201) Clopidogrel (n=4,229) HR for ticagrelor (95% CI) p- value Definite Probable or definite Possible, probable, or definite ( ) 0.69 ( ) 0.73 ( ) Time-at-risk is calculated from the date of first stent insertion in the study or date of randomization *Cutlip et. al., Circulation. 2007;115: By univariate Cox model
24 K-M estimated rate (% per year) Primary safety event: major bleeding Clopidogrel Ticagrelor HR 0.96 (95% CI = ), p= No. at risk Months Ticagrelor 4,1653,431 3,254 3,137 2,440 1,786 1,640 Clopidogr 4,1813,430 3,297 3,159 2,441 1,804 1,635 el
25 Platelet activation-impact on surrogate endpoints Clinical studies/ oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital
26
27 CHAMPION PHOENIX Study Design CHAMPION PHOENIX N = 10,900 MITT SA/ NSTE-ACS/ STEMI Patients requiring PCI 1 P2Y 12 inhibitor naïve Rand OR Cangrelor 2 bolus & infusion (30ug/kg; 4ug/kg/min) PCI ~30 Placebo 3 oral (right before PCI or right after, per physician) Placebo 2 bolus & infusion OR Clopidogrel 600 mg oral Placebo oral Clopidogrel 3 (600 mg or 300 mg oral, per physician) to 4 hours 1 Randomization occurred once suitability for PCI was confirmed either by angiography or STEMI diagnosis. Double blind study medication was administered as soon as possible following randomization. 2 Study drug Infusion (cangrelor or matching placebo) was continued for 2-4 hours at the discretion of the treating physician. At the end of the infusion patients received a loading dose of clopidogrel or matching placebo and were transitioned to maintenance clopidogrel therapy. 3 Clopidogrel loading dose (or matching placebo) was administered as directed by the investigator. At the time of patient randomization, a clopidogrel loading dose of 600 mg or 300 mg was specified by the investigator. MITT=modified intent-to-treat; NSTE-ACS=non-ST-elevation acute coronary syndrome; PCI=percutaneous coronary intervention; SA=stable angina; STEMI=ST-elevation MI. Patras University Hospital
![Subgroups: Death/MI/IDR/ST at 48 Hours OR [95% CI] Overall 0.79 (0.67,0.93) Age 75 0.71 (0.50,1.02) Age <75 0.81 (0.67,0.98) Male 0.84 (0.69,1.03) Female 0.67 (0.50,0.92) Ethnicity: White 0.80 (0.](/docs-images/73/69575255/images/28-0.jpg "67,0.95) Ethnicity: Non-white 0.70 (0.35,1.41) United States 0.70 (0.53,0.92) Other Countries 0.85 (0.69,1.05) Stable Angina 0.78 (0.63,0.95) NSTE-ACS 0.80 (0.55,1.17) STEMI 0.75 (0.46,1.")
28 Subgroups: Death/MI/IDR/ST at 48 Hours OR [95% CI] Overall 0.79 (0.67,0.93) Age (0.50,1.02) Age < (0.67,0.98) Male 0.84 (0.69,1.03) Female 0.67 (0.50,0.92) Ethnicity: White 0.80 (0.67,0.95) Ethnicity: Non-white 0.70 (0.35,1.41) United States 0.70 (0.53,0.92) Other Countries 0.85 (0.69,1.05) Stable Angina 0.78 (0.63,0.95) NSTE-ACS 0.80 (0.55,1.17) STEMI 0.75 (0.46,1.25) Weight >= (0.66,0.94) Weight < (0.39,1.45) Biomarker Positive 0.90 (0.64,1.27) Biomarker Negative 0.75 (0.61,0.91) Diabetic No 0.74 (0.61,0.90) Diabetic Yes 0.92 (0.67,1.27) Insulin-Dependent Diabetes: Yes 0.74 (0.42,1.31) Insulin-Dependent Diabetes: No 0.79 (0.66,0.94) Prior MI 0.68 (0.47,0.97) No Prior MI 0.84 (0.69,1.02) 0.2 Patras University Hospital Cangrelor Better 1.0 Clopidogrel Better 5.0 P [Int]
29 CHAMPION Trials Study Designs Randomised, Double Blind, Controlled Trials of patients undergoing PCI CHAMPION PHOENIX n=10,942 mitt SA / NSTE-ACS / STEMI P2Y 12 naïve Placebo or clopidogrel before or after PCI Cangrelor bolus then infusion OR Clopidogrel 600 mg or 300 mg oral Clopidogrel 600 mg oral CHAMPION PCI n=8667 mitt SA / NSTE-ACS / STEMI Placebo or clopidogrel before PCI Cangrelor bolus then infusion Clopidogrel 600 mg oral Clopidogrel 600 mg oral CHAMPION PLATFORM n=5301 mitt SA / NSTE-ACS P2Y 12 naïve Placebo or clopidogrel after PCI Cangrelor bolus then infusion Clopidogrel 600 mg oral Clopidogrel 600 mg oral hours PCI ~30
30 Subgroups: Death, MI, IDR, Stent Thrombosis OR [95% CI] P [Int] Overall 0.81 (0.71, 0.91) Age >= (0.52, 0.91) Age < (0.73, 0.96) Male 0.85 (0.74, 0.99) 0.18 Female 0.71 (0.56, 0.89) Ethnicity: White 0.80 (0.70, 0.92) Ethnicity: Non-white 0.87 (0.60, 1.28) United States 0.82 (0.68, 0.98) ROW 0.80 (0.67, 0.94) Stable Angina 0.77 (0.64, 0.93) NSTE-ACS 0.82 (0.68, 0.99) STEMI 0.84 (0.55, 1.27) Weight >= (0.71, 0.92) Weight < (0.52, 1.30) Biomarker Positive 0.79 (0.62, 1.02) Biomarker Negative 0.79 (0.68, 0.91) Diabetic Yes 0.87 (0.69, 1.09) Diabetic No 0.78 (0.67, 0.91) Insulin-Dependent Diabetes: Yes 0.63 (0.41, 0.98) Insulin-Dependent Diabetes: No 0.83 (0.72, 0.94) Prior MI 0.72 (0.57, 0.92) 0.25 No Prior MI 0.85 (0.74, 0.99) Cangrelor better Clopidogrel better Steg et al. Lancet Sep 3, 2013
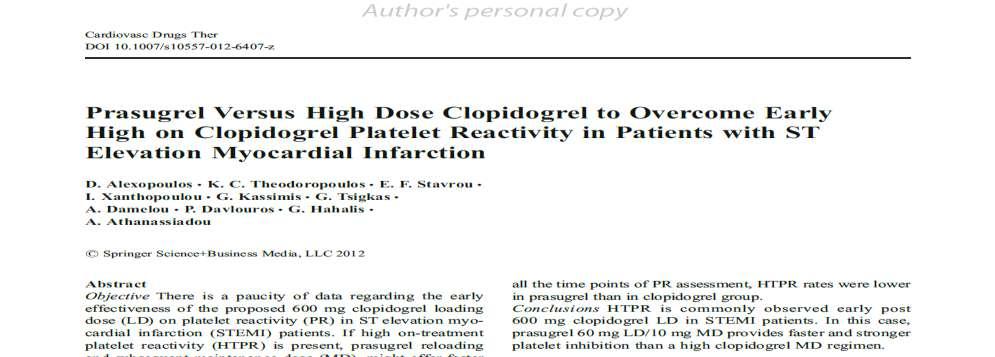
31 Patras University Hospital In primary PCI: regimens which increase platelet inhibition vs standard clopidogrel result in superior antiischemic effects consistent with the results in the whole trials populations (p-interaction not significant). Although subgroup analyses of the primary PCI populations showed no significant benefit in primary endpoints for more potent antiplatelet regimens versus clopidogrel, no study was designed specifically for primary PCI patients and even PLATO the largest one- was underpowered for detecting differences in this subgroup.
32
33 Platelet activation-impact on surrogate endpoints Clinical studies/oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital
34 Patras University Hospital P2Y12 receptor inhibitors in acute coronary syndromes: From the research laboratory to the clinic and vice versa. D. Alexopoulos Cardiology (Karger), 2014

35 Thromb Res 2008
36

37 Patras University Hospital
38 Alexopoulos D, et al. Circ J 2012;76:2183

39
40
41 Platelet activation-impact on surrogate endpoints Clinical studies/ oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital
42

43 Patras University Hospital
44

45 Patras University Hospital

46 Patras University Hospital

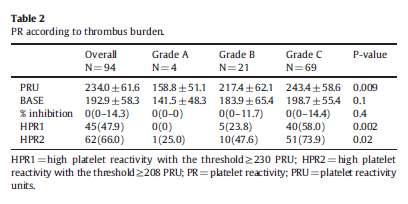
47 Circ Interv 2012; 5:
48 Alexopoulos et al, Circ Cardiovasc Interv. 2012;5:797
49 Randomized assessment of ticagrelor versus prasugrel antiplatelet effects in patients with ST elevation myocardial infarction. D. Alexopoulos et al, Circ Interv 2012; 5:

50 JACC 2013;61:1601

51 . Alexopoulos et al JACC 2013;62:940-1 Patras University Hospital
52 Platelet activation-impact on surrogate endpoints Clinical studies/ oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital
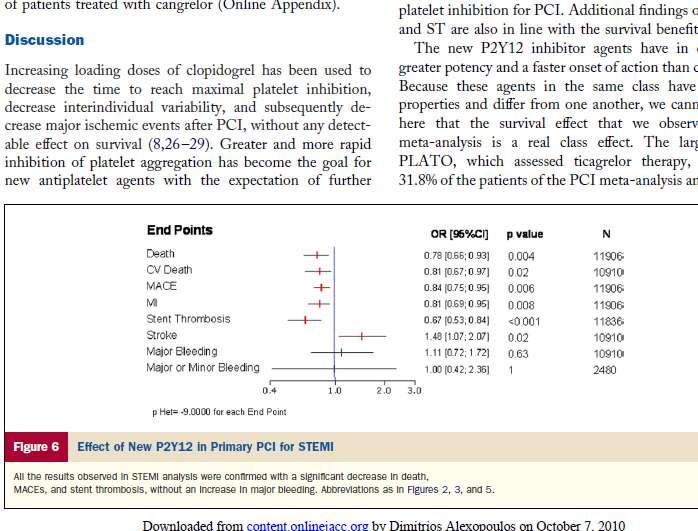
53 Patras University Hospital Intrinsic platelet reactivity Up to 30% patients do exhibit platelet reactivity below the thresholds predicting ischemic risk. It is not clear whether these patients had an even lower platelet reactivity prior to the acute event and the one assessed early in STEMI is increased compared with their baseline platelet reactivity. It is not clear either, whether these patients are at lower risk for future events or at lower need for strong P2Y12 inhibition.
54 Patras University Hospital HPR rates in the acute phase of STEMI. In close dependence primarily on the agent used, timing of platelet function assessment and platelet function test used. Co-administration of commonly used medication leading to platelet activation like e.g. heparin should also be considered.
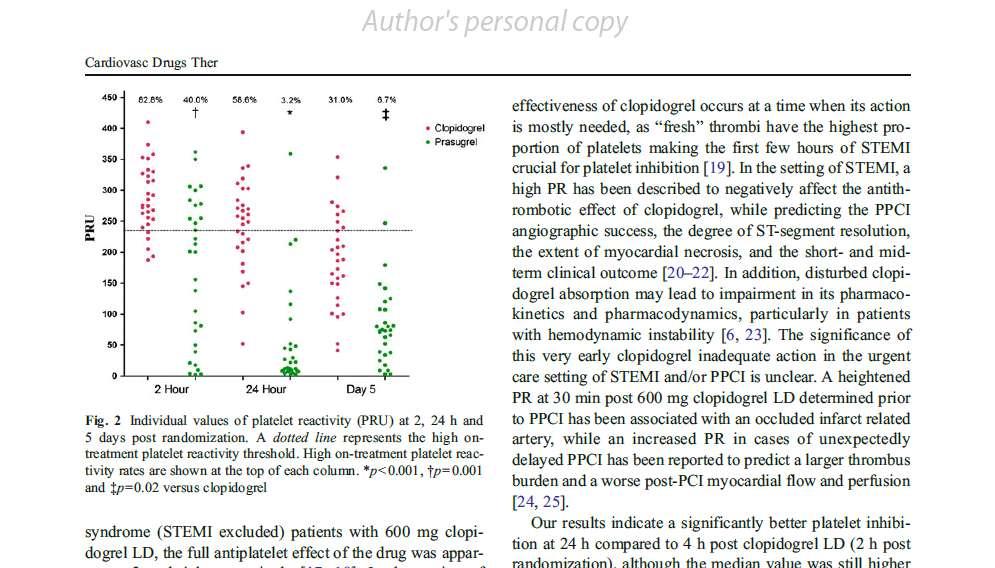
55 Patras University Hospital At 24 hours following post LD clopidogrel: almost half prasugrel: 3.2% to 4.2% ticagrelor: 0 and 2.8% 6-24 hours post LD might be expected with the VerifyNow and the VASP respectively. No pharmacodynamic studies with cangrelor exclusively in STEMI patients have been published so far
56 Patras University Hospital HPR thresholds value? No platelet reactivity cutoff points specifically for STEMI patients have been identified HPR thresholds used in pharmacodynamic studies in STEMI patients have been obtained from receiver operating characteristic analysis in post-pci studies involving stable or ACS patients Thresholds utility so far in STEMI for at least the first 24 hours, is mostly to characterize the onset of antiplatetelet action and it is not clear whether they carry any ability in predicting upcoming events.
57 Patras University Hospital Is the higher the platelet inhibition, the better? CURRENT OASIS 7: rates of definite stent thrombosis were reduced early (from randomization to 48 h) likely related to more potent platelet inhibition provided by high clopidogrel dose. Despite the undisputed higher antiplatelet potency of ticagrelor over clopidogrel and the overall reduction in stent thrombosis rate in PLATO, no difference in stent thrombosis rate between ticagrelor and clopidogrel in the acute phase (24 hours) was found. Similar findings have been reported with prasugrel in the TRITON TIMI-38. A relative higher significance of technical and stent placement issues rather than the level of platelet inhibition for affecting stent thrombosis rate has been implicated.
58 Patras University Hospital Ticagrelor Loading Dose Versus Clopidogrel Loading and Reloading With Ticagrelor Two-center, randomized, pharmacodynamic study of parallel design STEMI patients randomization immediately after coronary angiography (Hour 0) to: Ticagrelor 180mg LD or Clopidogrel 600mg LD and 2 hours later reloading with Ticagrelor 180mg Platelet reactivity (PR) assessment using the VerifyNow assay at randomization (Hour 0) and at 2, 4, 6 and 24 hours post randomization ClinicalTrials.gov NCT , Alexopoulos et al
59 Patras University Hospital
60 Patras University Hospital P2Y12 inhibition and thrombolysis Platelet reactivity is heightened after thrombolytic therapy Role of prasugrel or ticagrelor is unclear. In TRITON TIMI-38, there was a very limited experience with co-administration of thrombolysis with prasugrel, mainly in the secondary PCI cohort. In PLATO, thrombolysis was an exclusion criterion.
61

62 Patras University Hospital Adjunctive Antithrombotic Therapy to Support PCI After Fibrinolytic Therapy ACCF/AHA STEMI guidelines 2013
63 Montalescot et al, Lancet 2009
64
65 Ticagrelor vs high dose of clopidogrel in ST elevation myocardial infarction patients with high residual platelet reactivity post thrombolysis: a pharmacodynamic comparison Prospective, 2-center, randomized study of parallel design. Patients with STEMI and HPR (defined as PRU 208) 3 to 48 hours post fibrinolysis and standard clopidogrel treatment [300mg loading dose (LD) 75mg maintenance dose (MD)] are randomized pre coronary angiography to: Ticagrelor 180mg LD 90mg bid MD or Clopidogrel 600mg LD 150mg MD. Platelet reactivity (PR) assessment at randomization (Hour 0) and at 2, 24 hours after randomization, as well as pre-discharge, using the VerifyNow assay, in platelet reactivity units (PRU). Primary endpoint is PR at Hour 2 between groups. Patras University Hospital ClinicalTrials.gov NCT , Alexopoulos et al
66 Patras University Hospital
67 GReek AntiPlatelet REgistry (GRAPE) 8 GREEK PCI HOSPITALS Jan Aug patients

68
69 Multivariate log-poisson regression model for appropriate P2Y12 inhibitor selection initially (A)
70


71 681 patients with STEMI
72 Patras University Hospital 30-day outcomes (excluding in hospital events for patients who subjected to P2Y12 inhibitor upgrade at discharge) Clopidogrel treated N =102 P2Y12 inhibitor upgrade N=102 P value BARC type 1 1(1.0) 17(16.7) <0.001 BARC type 2 0(0) 2(2.0) NA BARC type 3 1(1.0) 1(1.0) 1.0 Bleeding BARC any type 2(2.0) 20(19.6) <0.001 MACEs 6(5.9) 4(3.9) 0.7
73 Platelet activation-impact on surrogate endpoints Clinical studies/oral P2Y12 inhibitors Clinical studies/ IV P2Y12 inhibitors Clopidogrel pharmacodynamic studies New P2Y12 inhibitors pharmacodynamic studies Unsettled issues Perspectives Patras University Hospital
74 Level of platelet inhibition? How fast we should achieve this by P2Y12 blockade An immediate, e.g. at first medical contact, platelet inhibition appears as the most attractive pathophysiologic target. Whether this offers clinical superiority over a more conservative approach allowing a few hours delay in antiplatelet activity has to be proved. The combination of cangrelor with prasugrel or ticagrelor appears theoretically as the best possible P2Y12 inhibitors strategy in primary PCI. This too, has to be tested against an oral-only, potent P2Y12 inhibitor regimen. Patras University Hospital
75 Patras University Hospital It is appreciable that the antiischemic benefit provided by a strong antiplatelet regimen may be offset by an accompanying increased bleeding potential. Fortunately, at least in STEMI patients no signs of excess bleeding have been identified so far Future drug combinations particularly if these include other oral antiplatelet (e.g. vorapaxar) or antithrombin (e.g. low dose rivaroxaban?

76 Patras University Hospital
77 Patras University Hospital
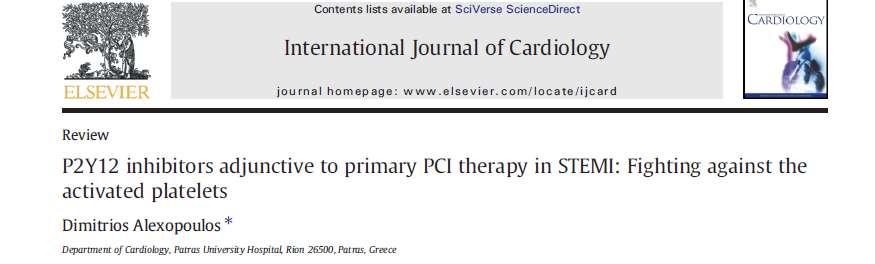
![Infarct size, %LV INFUSE-AMI: Infarct size at 30 days* 50 40 Median [IQR] 15.1% [6.8, 22.7] Median [IQR] 17.9% [10.](/docs-images/73/69575255/images/78-0.jpg "3, 25.4] 30 P=0.")
78 Infarct size, %LV INFUSE-AMI: Infarct size at 30 days* Median [IQR] 15.1% [6.8, 22.7] Median [IQR] 17.9% [10.3, 25.4] 30 P= IC abciximab N=229 No abciximab N=223 Patras University Hospital *Core laboratory assessed
79 CONCLUSIONS Several areas of unmet need in antiplatelet therapy in patients with STEMI undergoing primary PCI exist. A clear demand for additional research at both basic science and clinical levels to understand the underlying mechanisms by which STEMI patients may benefit. Large randomized clinical studies dedicated to STEMI patients will be necessary to precisely define the impact of P2Y12 blockade by oral -with or without concomitant intravenous- agents on the outcome of this high-risk population. Patras University Hospital
80 TAKE HOME MESSAGES In STEMI, high rate of HPR following 600 mg clopidogrel LD Delay in the onset of action of prasugrel/ticagrelor New agents of marginal clinical superiority to clopidogrel in primary PCI patients Cangrelor: need for more data/comparison to prasugrel/ticagrelor Switching from clopidogrel to prasugrel or ticagrelor may be an alternative for STEMI patients GP IIb/IIIa antagonicts: IIa indication
81 Patras University Hospital Platelet reactivity variability before P2Y12 blockade and its evolution over time, genetic predisposition, antiplatelet agent used, timing and method of platelet function testing significantly affect the rates of high on-treatment platelet reactivity. Although ominus signs of higher bleeding potential of antiplatelet stronger regimens have not appeared in STEMI, this should be carefully tested. Additional research at both the basic science level along with large randomized clinical studies dedicated to STEMI patients are necessary to precisely assess the impact of P2Y12 blockade on the outcome of this high risk population.
82 CURRENT-OASIS 7 In the STEMI subgroup- mostly treated with primary PCI and 40.6% of them receiving a IIb/IIIa inhibitor- the reduction in the primary endpoint with the high dose, was nominally non significant 4.2% vs 5%, [HR (95% CI), 0.83 ( ), p=0.117]. However, the results were consistent with the overall PCI cohort ( p for interaction=0.817).
83 In a substudy of PLATO on angiographic outcomes, in the STEMI subgroup no difference was observed in the incidence of post-pci TIMI (Thrombolysis In Myocardial Infarction) myocardial perfusion grade 3 between ticagrelor and clopidogrel receiving patients consistently with the overall cohort (44). Nevertheless, this was not unexpected since angiography was performed earlier than 1 h post antiplatelet administration in >80% of the cases, when most likely the drugs antiplatelet action had not been developed. Patras University Hospital
84 In a study of pre-hospital bivalirudin administration, bivalirudin treated patients still exhibited higher than controls early stent thrombosis rate. This occurred despite loading with prasugrel or ticagrelor in 50% of the cases suggestive of new oral P2Y12 inhibitors insufficiency to address this risk (46). Patras University Hospital
85
86
87
88

89 Patras University Hospital
90 Patras University Hospital Antiplatelet Therapy to Support Primary PCI for STEMI I IIa IIb III A loading dose of a P2Y 12 receptor inhibitor should be given as early as possible or at time of primary PCI to patients with STEMI. Options include: Clopidogrel 600 mg; or Prasugrel 60 mg; or Ticagrelor 180 mg P2Y12 inhibitor therapy should be given for 1 year to patients with STEMI who receive a stent (BMS or DES) during primary PCI 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 ACCF/AHA STEMI guidelines 2013 Patras University Hospital")
91 Adjunctive Antithrombotic Therapy to Support Reperfusion With Primary PCI (cont.) ACCF/AHA STEMI guidelines 2013 Patras University Hospital
92 Patras University Hospital Results Table 2 Platelet reactivity (VerifyNow PRU) at 0, 2, 4, 6 and 24 hours post randomization Time post randomization Ticagrelor N=16 Clopidogrel Ticagrelor N=13 LS mean difference (95%CI) p-value 0 hour 220.0± ± hour (63.3 to 195.5) 4 hour 89.7 (43.6 to 135.8) 6 hour 57.4 (28.5 to 86.3) 24 hours 50.2 (25.5 to 74.9) (110.8 to 406.3) (47.3 to 176.1) 82.6 (36.2 to 129.1) 23.2 (10.5 to 35.9) ( to 37.9) ( to 60.9) (-81.4 to 30.9) 26.9 (-0.95 to 54.9) Generalized linear model with gamma distribution and logarithmic transformation of the dependent variable, treatment as factor and baseline PR as covariate

93 Patras University Hospital

94 Patras University Hospital
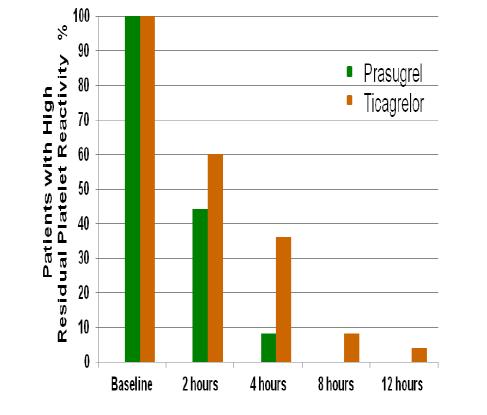
95 Patras University Hospital Results Out of 36 screened patients, 23(63.9%) presented HPR (87% men, 21.7% diabetics) and were all randomized (Ticagrelor N=12, Clopidogrel N=11). Median time of pain onset to fibrinolysis was 2.5( ) hours. There were no differences in baseline and clinical characteristics between groups. The primary endpoint was significantly lower for Ticagrelor compared to high Clopidogrel (79.1 PRU, 95%CIs vs PRU, 95%CIs , p<0.001). PR at Hour 24 and pre-discharge was also significantly lower for Ticagrelor compared to Clopidogrel (32.1 PRU, 95%CIs -3.6 to 67.8 vs PRU, 95%CIs and 20.7 PRU, 95%CIs -7.2 to 48.7 vs PRU, 95%CIs respectively, p<0.001 for both). HPR rates at Hour 2 and 24 were significantly lower for Ticagrelor compared to high Clopidogrel regimen (8.3% vs 90.9%, p<0.001 and 0% vs 45.5%, p=0.01 respectively).

96 Patras University Hospital
97 A high platelet reactivity in STEMI patients Negatively impacts on the clopidogrel effect, Predicts PPCI success on angiography, degree of STsegment resolution, extent of myocardial necrosis, Predicts short- and mid-term clinical outcome Is associated with larger intracoronary thrombus and worse post-pci myocardial flow and perfusion. Gawaz M, et al.circulation 1996; 93: Campo G, et al. J Am Coll Cardiol 2006; 48: Matetzky S, et al Circulation 2004; 109: Vavuranakis M, et al. Circ J 2011; 75:
98 Switch and non switch in P2Y12 inhibition: the real life use of clopidogrel and prasugrel in patients with acute myocardial infarction. Insights from the FAST MI 2010 registry Schiele F et al ESC 2012 Nationwide French registry 4169 patients with AMI in 213 centres received thienopyridines, 1259 received prasugrel (31%). 391 received de novo prasugrel, 807 (64%) were treated with clopidogrel first and then switched to prasugrel 11% had a 60mg loading dose of prasugrel. No evidence of excess risk of bleeding or in-hospital complications in the patients who were switched, compared with those who received prasugrel treatment only.
99 Patras University Hospital In-Hospital Switching of ADP Receptor Inhibitors in Myocardial Infarction Patients Treated with Percutaneous Coronary Intervention: Insights from the TRANSLATE-ACS Study. 6,362 MI pts treated with PCI at 196 hospitals from 4/2010-4/2012 Among 4,778 patients initially treated with a 1 st generation ADP receptor inhibitor, 491 (10%) were switched to a 2 nd generation drug Among 1,584 patients initially treated with a 2 nd generation ADP receptor inhibitor, 186 (12%) were switched to a 1 st generation drug BagaiA, et al Circulation 2012;126:A15573
100 Patras University Hospital INFUSE-AMI Trial 452 pts with anterior STEMI Anticipated Sx to PCI <5 hrs, TIMI 0-2 flow in prox or mid LAD Primary PCI with bivalirudin anticoagulation Pre-loaded with aspirin and clopidogrel 600 mg or prasugrel 60 mg Manual aspiration R 1:1 Stratified by symptoms to angio <3 vs 3 hrs, and prox vs mid LAD occlusion No aspiration R 1:1 R 1:1 IC Abcx No Abcx IC Abcx No Abcx Primary endpoint: Infarct size at 30 days (cmri) 2º endpoints: TIMI flow, blush, ST-resolution, MACE (30d, 1 yr)

101 Patras University Hospital

102 Montalescot G et al Lancet 2009 Patras University Hospital
103 Patras University Hospital

104 Patras University Hospital
105 Bhatt DL, Stone GW, Mahaffey KW, et al. Harrington RA. NEJM 2013 at Patras University Hospital
106
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο)
") Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Αντιαιμοπεταλιακη αγωγη (ποια, πο τε και για πο σο) Dimitrios Alexopoulos, MD, FESC, FACC Cardiology Department, Patras University Hospital, Patras, Rio, Greece. Patras University Hospital I, Dimitrios
Switching antiplatelet regimens: alternatives to clopidogrel in STEMI patients
 Patras University Hospital Switching antiplatelet regimens: alternatives to clopidogrel in STEMI patients Dimitrios Alexopoulos, MD, FESC, FACC Professor of Cardiology Patras University Hospital Greece
Patras University Hospital Switching antiplatelet regimens: alternatives to clopidogrel in STEMI patients Dimitrios Alexopoulos, MD, FESC, FACC Professor of Cardiology Patras University Hospital Greece
Is Cangrelor hype or hope in STEMI primary PCI?
 Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
Is Cangrelor hype or hope in STEMI primary PCI? ARUN KALYANASUNDARAM MD, MPH, FSCAI HOPE Issues with platelet inhibition in STEMI Delayed onset In acute settings, achieving the expected antiplatelet effect
LA TERAPIA ANTIAGGREGANTE PER VIA PARENTERALE
 LA TERAPIA ATIAGGREGATE PER VIA PARETERALE Sergio Leonardi, MD, MHS, FESC Cardiovascular Clinical Research Center Fondazione IRCCS Policlinico San Matteo Pavia, Italy 28 March 2015 Induno, BG CI-1 Terapia
LA TERAPIA ATIAGGREGATE PER VIA PARETERALE Sergio Leonardi, MD, MHS, FESC Cardiovascular Clinical Research Center Fondazione IRCCS Policlinico San Matteo Pavia, Italy 28 March 2015 Induno, BG CI-1 Terapia
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Updated and Guideline Based Treatment of Patients with STEMI
 Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Updated and Guideline Based Treatment of Patients with STEMI Eli I. Lev, MD Director, Cardiac Catheterization Laboratory Hasharon Hospital, Rabin Medical Center Associate Professor of Cardiology Tel-Aviv
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute
 Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute Implications of Pre-loading on Patients Undergoing Coronary Angiography Angiography Define
Tim Henry, MD Director, Division of Cardiology Professor, Department of Medicine Cedars-Sinai Heart Institute Implications of Pre-loading on Patients Undergoing Coronary Angiography Angiography Define
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor
 Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Quale terapia antiaggregante nello STEMI? Prasugrel vs ticagrelor Leonardo Bolognese Cardiovascular Department, Arezzo, Italy Platelet Reactivity in Patients with STEMI Undergoing Primary PCI Campo G et
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Νεώτερα στην αντιαιμοπεταλιακή αγωγή
 Patras University Hospital Νεώτερα στην αντιαιμοπεταλιακή αγωγή Δημήτριος Αλεξόπουλος MD, FESC, FACC Καθηγητής Καρδιολογίας Παν/μίου Πατρών ΟΕ 2014 Patras University Hospital I, Dimitrios Alexopoulos,
Patras University Hospital Νεώτερα στην αντιαιμοπεταλιακή αγωγή Δημήτριος Αλεξόπουλος MD, FESC, FACC Καθηγητής Καρδιολογίας Παν/μίου Πατρών ΟΕ 2014 Patras University Hospital I, Dimitrios Alexopoulos,
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Ticagrelor vs prasugrel in patients with ST elevation myocardial infarction undergoing primary percutaneous coronary intervention
 DISCLOSURES: NONE Ticagrelor vs prasugrel in patients with ST elevation myocardial infarction undergoing primary percutaneous coronary intervention I. Xanthopoulou, KC. Theodoropoulos, G. Kassimis, V.
DISCLOSURES: NONE Ticagrelor vs prasugrel in patients with ST elevation myocardial infarction undergoing primary percutaneous coronary intervention I. Xanthopoulou, KC. Theodoropoulos, G. Kassimis, V.
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Clopidogrel vs New Antiplatelet Therapy (Prasugrel) Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany
 Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany") Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Clopidogrel vs New Antiplatelet Therapy () Adnan Kastrati, MD Deutsches Herzzentrum, Technische Universität München, Germany Seoul, April 3, 21 Dual Antiplatelet Therapy for Stenting MACE, % 12 1 8 6 In
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary
 Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
Platelet function testing to guide P2Y 12 -inhibitor treatment in ACS patients after PCI: insights from a national program in Hungary Dániel Aradi MD PhD Interventional Cardiologist Assistant professor
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
P2Y 12 blockade. To load or not to load before the cath lab?
 UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
UPDATE ON ANTITHROMBOTICS IN ACUTE CORONARY SYNDROMES P2Y 12 blockade. To load or not to load before the cath lab? Franz-Josef Neumann Personal: None Institutional: Conflict of Interest Speaker honoraria,
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Optimal antithrombotic therapy:
 Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Optimal antithrombotic therapy: upstream and during primary PCI. Steen D Kristensen, MD, DMSc, FESC Professor and Consultant Interventional Cardiologist Aarhus University, Denmark UNIVERSITY OF AARHUS
Novel Anticoagulation Therapy in Acute Coronary Syndrome
 Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
Novel Anticoagulation Therapy in Acute Coronary Syndrome Soon Jun Hong Korea University Anam Hospital 1 Thrombus Formation Cascade Coagulation Cascade Platelet Cascade TXA2 Aspirin R Inhibitor Fondaparinux
COME ORIENTARSI TRA I NUOVI. Maria Rosa Conte H. Mauriziano Torino
 COME ORIENTARSI TRA I NUOVI ANTIPIASTRINIC I Maria Rosa Conte H. Mauriziano Torino Sulle sponde del Ticino- Novara 10 maggio 2013 NEW ORAL ANTIPLATET AGENT PRASUGREL TICAGRELOR (Cangrelor) Death/ MI/
COME ORIENTARSI TRA I NUOVI ANTIPIASTRINIC I Maria Rosa Conte H. Mauriziano Torino Sulle sponde del Ticino- Novara 10 maggio 2013 NEW ORAL ANTIPLATET AGENT PRASUGREL TICAGRELOR (Cangrelor) Death/ MI/
Bivalirudin Clinical Trials Update Evidence and Future Perspectives
 Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Bivalirudin Clinical Trials Update Evidence and Future Perspectives Andreas Baumbach Consultant Cardiologist/ hon. Reader in Cardiology Bristol Heart Institute University Hospitals Bristol MY CONFLICTS
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 8, 2014
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 8, 2014 Theodore A Bass, MD FSCAI Immediate Past-President SCAI Professor of Medicine, University of Florida Medical Director UF Health CV
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
New insights in stent thrombosis: Platelet function monitoring. Franz-Josef Neumann Herz-Zentrum Bad Krozingen
 New insights in stent thrombosis: Platelet function monitoring Franz-Josef Neumann Herz-Zentrum Bad Krozingen New insights in stent thrombosis: Platelet function monitoring Variability of residual platelet
New insights in stent thrombosis: Platelet function monitoring Franz-Josef Neumann Herz-Zentrum Bad Krozingen New insights in stent thrombosis: Platelet function monitoring Variability of residual platelet
Why and How Should We Switch Clopidogrel to Prasugrel?
 Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Case Presentation Why and How Should We Switch Clopidogrel to Prasugrel? Shaul Atar Western Galilee Medical Center Nahariya, ISRAEL Case Description A 67 Y. Old Pt. admitted to IM with anginal CP. DM,
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Improving Patient Outcomes: Updated Treatment Strategies in the Management of Acute Coronary Syndrome
 Improving Patient Outcomes: Updated Treatment Strategies in the Management of Acute Coronary Syndrome E. Magnus Ohman, MB, FRCPI, FESC, FACC Professor of Cardiovascular Medicine The Kent and Siri Rawson
Improving Patient Outcomes: Updated Treatment Strategies in the Management of Acute Coronary Syndrome E. Magnus Ohman, MB, FRCPI, FESC, FACC Professor of Cardiovascular Medicine The Kent and Siri Rawson
ΠΑΝΕΠΙΣΤΗΜΙΟ ΙΩΑΝΝΙΝΩΝ. Εξατοµικευµένη αντιαιµοπεταλιακή αγωγή. Ποιο είναι το µέλλον?
 ΠΑΝΕΠΙΣΤΗΜΙΟ ΙΩΑΝΝΙΝΩΝ ΕΡΕΥΝΗΤΙΚΟ ΚΕΝΤΡΟ ΑΘΗΡΟΘΡΟΜΒΩΣΗΣ Εξατοµικευµένη αντιαιµοπεταλιακή αγωγή. Ποιο είναι το µέλλον? Αλέξανδρος Δ. Τσελέπης, MD, PhD Καθηγητής Βιοχηµείας - Κλινικής Χηµείας Disclosures
ΠΑΝΕΠΙΣΤΗΜΙΟ ΙΩΑΝΝΙΝΩΝ ΕΡΕΥΝΗΤΙΚΟ ΚΕΝΤΡΟ ΑΘΗΡΟΘΡΟΜΒΩΣΗΣ Εξατοµικευµένη αντιαιµοπεταλιακή αγωγή. Ποιο είναι το µέλλον? Αλέξανδρος Δ. Τσελέπης, MD, PhD Καθηγητής Βιοχηµείας - Κλινικής Χηµείας Disclosures
STEMI Primary Percutaneous Coronary Intervention
 STEMI Primary Percutaneous Coronary Intervention Abdul Razek Maaty, MD Professor of Medicine Outline Primary PCI Aspiration, manual thrombectomy and distal protection devices Choice of stent Pharmacothaerpy,
STEMI Primary Percutaneous Coronary Intervention Abdul Razek Maaty, MD Professor of Medicine Outline Primary PCI Aspiration, manual thrombectomy and distal protection devices Choice of stent Pharmacothaerpy,
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Clinical Seminar. Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective
 Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Clinical Seminar Which Diabetic Patient is a Candidate for Percutaneous Coronary Intervention - European Perspective Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical
Speaker s name: Thomas Cuisset, MD, PhD
 Speaker s name: Thomas Cuisset, MD, PhD X I have the following potential conflicts of interest to report: x Consulting: Daiichi Sankyo, Eli Lilly Employment in industry Stockholder of a healthcare company
Speaker s name: Thomas Cuisset, MD, PhD X I have the following potential conflicts of interest to report: x Consulting: Daiichi Sankyo, Eli Lilly Employment in industry Stockholder of a healthcare company
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta
 Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
Razionale ed evidenze scientifiche di Doppia Antiaggregazione Piastrinica a lungo termine nel Paziente con Sindrome Coronarica Acuta Giuseppe Musumeci SC Cardiologia Ospedale Santa Croce e Carle Cuneo
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
New antiplatelets in NSTEMI. Overview: dual anti-platelet oral therapy
 Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Cairo, Egypt 2010 New antiplatelets in NSTEMI Steen D. Kristensen, FESC Department of Cardiology Aarhus University Hospital Skejby Denmark Overview: dual anti-platelet oral therapy Aspirin Clopidogrel
Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor
 Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor Nicolas W. Shammas, MS, MD, FACC Coronary and Peripheral Interventionalist Cardiovascular Medicine, PC Research Director,
Oral Antiplatelet Therapy in Patients with ACS: A Focus on Prasugrel and Ticagrelor Nicolas W. Shammas, MS, MD, FACC Coronary and Peripheral Interventionalist Cardiovascular Medicine, PC Research Director,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI
 Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
compared with clopidogrel in patients with acute coronary syndromes the PLATelet Inhibition and patient Outcomes trial Outcomes in patients with and planned PCI Ph.Gabriel Steg*, Stefan James, Robert A
Dual Antiplatelet duration in ACS: too long or too short?
 Dual Antiplatelet duration in ACS: too long or too short? Leonardo Bolognese, MD, FESC, FACC Cardiovascular Department, Arezzo, Italy Paradigm Shift the ideal duration of DAPT: a moving target Early (stent-related)
Dual Antiplatelet duration in ACS: too long or too short? Leonardo Bolognese, MD, FESC, FACC Cardiovascular Department, Arezzo, Italy Paradigm Shift the ideal duration of DAPT: a moving target Early (stent-related)
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
On admission Acute extensive anterior STEMI
 Mr B 52 years old male Smoker No prior known CAD Presents with 1 hour intermittent crushing retrosternal chest pain Transferred by MICU directly to CCU (ASA, Heparin) On admission Intense pain, diaphoretic
Mr B 52 years old male Smoker No prior known CAD Presents with 1 hour intermittent crushing retrosternal chest pain Transferred by MICU directly to CCU (ASA, Heparin) On admission Intense pain, diaphoretic
Clopidogrel Use in ACS and PCI: Clinical Trial Update
 Clopidogrel Use in ACS and PCI: Clinical Trial Update Matthew J. Price MD Director, Cardiac Catheterization Laboratory, Scripps Clinic, La Jolla, CA Assistant Professor, Scripps Translational Science Institute
Clopidogrel Use in ACS and PCI: Clinical Trial Update Matthew J. Price MD Director, Cardiac Catheterization Laboratory, Scripps Clinic, La Jolla, CA Assistant Professor, Scripps Translational Science Institute
Dual Antiplatelet Therapy: Time for a Paradigm Shift?
 Dual Antiplatelet Therapy: Time for a Paradigm Shift? 5 years after PLATO Experience from the Daily Clinical Practice Hans Rickli Goals with antithrombotic treatment Acute coronary syndrome Risk reduction
Dual Antiplatelet Therapy: Time for a Paradigm Shift? 5 years after PLATO Experience from the Daily Clinical Practice Hans Rickli Goals with antithrombotic treatment Acute coronary syndrome Risk reduction
Horizon Scanning Centre November 2012
 Horizon Scanning Centre November 2012 Cangrelor to reduce platelet aggregation and thrombosis in patients undergoing percutaneous coronary intervention99 SUMMARY NIHR HSC ID: 2424 This briefing is based
Horizon Scanning Centre November 2012 Cangrelor to reduce platelet aggregation and thrombosis in patients undergoing percutaneous coronary intervention99 SUMMARY NIHR HSC ID: 2424 This briefing is based
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
DECLARATION OF CONFLICT OF INTEREST How to manage antiplatelet treatment in patients with diabetes in acute coronary syndrome Lars Wallentin Professor of Cardiology, Chief Researcher Cardiovascular Science
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Optimal Duration and Dose of Antiplatelet Therapy after PCI
 Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
Optimal Duration and Dose of Antiplatelet Therapy after PCI Donghoon Choi, MD, PhD Severance Cardiovascular Center Yonsei University College of Medicine Optimal Duration of Antiplatelet Therapy after PCI
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN
 What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
What is new in the Treatment of STEMI? Malcolm R. Bell, MBBS Mayo Clinic Rochester, MN October 2011 Part 2 Summary of newer antithrombotic and antiplatelet agents in STEMI Role of thrombectomy in PPCI
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
Do We Need Platelet Function Assays?
 Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Do We Need Platelet Function Assays? Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic, La Jolla, CA The Antiplatelet Effect of Clopidogrel Varies Widely Among Individuals
Relationships Relevant to this Presentation
 Relationships Relevant to this Presentation Research grants/contracts to DCRI NHLBI, ACC, AHA, sanofi-aventis, Lilly, Daiichi- Sankyo, GSK, TMC, BMS, Astra, J&J, BI, Portola, Novartis, Merck, Regado Consulting
Relationships Relevant to this Presentation Research grants/contracts to DCRI NHLBI, ACC, AHA, sanofi-aventis, Lilly, Daiichi- Sankyo, GSK, TMC, BMS, Astra, J&J, BI, Portola, Novartis, Merck, Regado Consulting
How to Predict & Prevent It! George D. Dangas, MD, FACC, FESC
 Stent Thrombosis How to Predict & Prevent It! George D. Dangas, MD, FACC, FESC Professor of Cardiology & Vascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Καθηγητής Καρδιολογίας ΕΚΠΑ
Stent Thrombosis How to Predict & Prevent It! George D. Dangas, MD, FACC, FESC Professor of Cardiology & Vascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Καθηγητής Καρδιολογίας ΕΚΠΑ
Antiplatelet Agents in Acute Coronary Syndromes, NSTE-ACS
 Antiplatelet Agents in Acute Coronary Syndromes, NSTE-ACS Is There Still a Role for IV Antiplatelet Agents (Cangrelor, GPIIbIIIA inhibitors)? François Schiele, MD, PhD Department of Cardiology, University
Antiplatelet Agents in Acute Coronary Syndromes, NSTE-ACS Is There Still a Role for IV Antiplatelet Agents (Cangrelor, GPIIbIIIA inhibitors)? François Schiele, MD, PhD Department of Cardiology, University
P 2 Y 12 Receptor Inhibitors
 P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
P 2 Y 12 Receptor Inhibitors Clopidogrel, Prasugrel and Ticagrelor Which Drug and for Whom? Cheol Whan Lee, MD Professor of Medicine, University of Ulsan College of Medicine, Heart Institute, Asan Medical
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון מרכז רפואי רבין
 תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
תרופות מעכבות טסיות חדשות ד"ר אלי לב מנהל שרות הצנתורים ח השרון בי""י מרכז רפואי רבין 1. Why should clopidogrel be replaced? 2. Prasugrel 3. Ticagrelor 4. Conclusions CURE TRIAL ACS pts 20 % reduction
Μιχάλης Χαμηλός, MD, PhD, FESC
 Αντίσταση στα αντιαιμοπεταλιακά. Πως μετράται, πότε πρέπει να εκτιμάται, και πως αντιμετωπίζεται Μιχάλης Χαμηλός, MD, PhD, FESC Πανεπιστημιακό Νοσοκομείο Ηαρκλείου Disclosures Speakers Honoraria: Astra
Αντίσταση στα αντιαιμοπεταλιακά. Πως μετράται, πότε πρέπει να εκτιμάται, και πως αντιμετωπίζεται Μιχάλης Χαμηλός, MD, PhD, FESC Πανεπιστημιακό Νοσοκομείο Ηαρκλείου Disclosures Speakers Honoraria: Astra
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
Ticagrelor compared with clopidogrel in patients with acute coronary syndromes the PLATO trial
 compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
compared with clopidogrel in patients with acute coronary syndromes the PLATO trial August 30, 2009 at 08.00 CET PLATO background In NSTE-ACS and STEMI, current guidelines recommend 12 months aspirin and
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
Pharmaco-Invasive Approach for STEMI
 Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
Pharmaco-Invasive Approach for STEMI Michael C. Kontos, MD Medical Director, Coronary Intensive Care Unit Director, Chest Pain Evaluation Center Associate Professor Departments of Internal Medicine (Cardiology),
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
What hematologists should know about VerifyNow
 What hematologists should know about VerifyNow Hematology fellows conference 12/13/2013 Presenter: Christina Fitzmaurice, MD, MPH Discussant: Daniel Sabath, MD, PhD HMC consult patient 54 yo woman admitted
What hematologists should know about VerifyNow Hematology fellows conference 12/13/2013 Presenter: Christina Fitzmaurice, MD, MPH Discussant: Daniel Sabath, MD, PhD HMC consult patient 54 yo woman admitted
Antiplatelet therapy is the mainstay of pharmacological
 Contemporary Reviews in Interventional Cardiology Pretreatment With Antiplatelet Drugs in Invasively Managed Patients With Coronary Artery Disease in the Contemporary Era Review of the Evidence and Practice
Contemporary Reviews in Interventional Cardiology Pretreatment With Antiplatelet Drugs in Invasively Managed Patients With Coronary Artery Disease in the Contemporary Era Review of the Evidence and Practice
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Antiplatelet Therapy: how, why, when? For Coronary Stenting
 Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Antiplatelet Therapy: how, why, when? For Coronary Stenting Dominick J. Angiolillo, MD, PhD, FACC, FESC, FSCAI Director of Cardiovascular Research Associate Professor of Medicine University of Florida
Dimitrios Alexopoulos, MD, FESC, FACC Patras University Hospital, Patras, Rio, Greece. Patras University Hospital
 Patras University Hospital Κατευθυντη ριες Οδηγιές της Ευρωπαι κη ς Καρδιολογικη ς Εταιρειάς στην αντιαιμοπεταλιακη θεραπειά γιαοξεάστεφανιαιάσυ νδρομα. Απο τις συστα σεις στην εφαρμογη στην καθ ημε ρα
Patras University Hospital Κατευθυντη ριες Οδηγιές της Ευρωπαι κη ς Καρδιολογικη ς Εταιρειάς στην αντιαιμοπεταλιακη θεραπειά γιαοξεάστεφανιαιάσυ νδρομα. Απο τις συστα σεις στην εφαρμογη στην καθ ημε ρα
Case Challenges in ACS The Very Elderly in the Cath Lab
 Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Case Challenges in ACS The Very Elderly in the Cath Lab Sameh Salama, MD, FSCAI Professor of Cardiology, Cairo University 86 yrs old male IDDM (controlled on insulin and oral hypoglycemics) Hypertensive
Oral Antiplatelet Therapy in PCI/ACS. Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine
 Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Oral Antiplatelet Therapy in PCI/ACS Dominick J. Angiolillo, MD, PhD, FACC, FESC Director of Cardiovascular Research Assistant Professor of Medicine Basic Concepts Thrombus Formation Two key elements:
Disclosures. Research consulting with: Sanofi-Regeneron Pfizer The Medicines Company Astra Zeneca
 Antiplatelet Therapy in Coronary Artery Disease -2015 What are the roles for newer therapies? How do you decide what to cover? R. Scott Wright, MD, FACC, FESC, FAHA Professor of Medicine, Mayo Clinic College
Antiplatelet Therapy in Coronary Artery Disease -2015 What are the roles for newer therapies? How do you decide what to cover? R. Scott Wright, MD, FACC, FESC, FAHA Professor of Medicine, Mayo Clinic College
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs
 Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
Session Objectives. Clopidogrel Resistance. Clopidogrel (Plavix )
") Session Objectives New Antithrombotics and Real Time Genetic Testing: Their Role in the Vascular Patient Margaret C. Fang, MD, MPH Associate Professor of Medicine Division of Hospital Medicine Medical
Session Objectives New Antithrombotics and Real Time Genetic Testing: Their Role in the Vascular Patient Margaret C. Fang, MD, MPH Associate Professor of Medicine Division of Hospital Medicine Medical
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Clopidogrel Response Variability and Platelet Function Testing: Should Routine Practice Be Changed in Interventional Cardiology?
 Clopidogrel Response Variability and Platelet Function Testing: Should Routine Practice Be Changed in Interventional Cardiology? Matthew J. Price MD, FACC Director, Cardiac Catheterization Laboratory Scripps
Clopidogrel Response Variability and Platelet Function Testing: Should Routine Practice Be Changed in Interventional Cardiology? Matthew J. Price MD, FACC Director, Cardiac Catheterization Laboratory Scripps
and Ticagrelor Professor of Medicine (Cardiology), Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center
, Georgetown University Associate Director, Division of Cardiology, Washington Hospital Center") Role of Genotyping and Point-of-Care of Testing in Clopidogrel, Prasugrel, and Ticagrelor Ron Waksman, MD Ron Waksman, MD Professor of Medicine (Cardiology), Georgetown University Associate Director, Division
Role of Genotyping and Point-of-Care of Testing in Clopidogrel, Prasugrel, and Ticagrelor Ron Waksman, MD Ron Waksman, MD Professor of Medicine (Cardiology), Georgetown University Associate Director, Division
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας. A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο
 Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο Europe* 2001 2011 Incident MI 291,100 327,700 US 2001 2011 Incident MI 405,100 485,200
Κωνσταντίνος Π. Τούτουζας Επ. Καθηγηηής Καρδιολογίας A Πανεπιζηημιακή Καρδιολογική Κλινική, Ιπποκράηειο Νοζοκομείο Europe* 2001 2011 Incident MI 291,100 327,700 US 2001 2011 Incident MI 405,100 485,200
The Korean Society of Cardiology COI Disclosure
 The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
Columbia University Medical Center Cardiovascular Research Foundation
 STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
STEMI and NSTEMI Pharmacology Confusion: How to Choose and Use Antithrombins (Unfractionated and Low Molecular Heparins, Bivalirudin, Fondaparinux) and Antiplatelet Agents (Aspirin, Clopidogrel and Prasugrel)
in High-risk PCI Patients?
 Lunchtime Activities Is Potent t Oral P2Y 12 Inhibitor Enough to Prevent Thrombotic Events in High-risk PCI Patients? Young-Hoon Jeong, MD M.D., PhD Ph.D. Department of Internal Medicine, Gyeongsang National
Lunchtime Activities Is Potent t Oral P2Y 12 Inhibitor Enough to Prevent Thrombotic Events in High-risk PCI Patients? Young-Hoon Jeong, MD M.D., PhD Ph.D. Department of Internal Medicine, Gyeongsang National
Optimal Duration of Dual Anti- Platelet Therapy. December 19, 2015
 Optimal Duration of Dual Anti- Platelet Therapy December 19, 2015 John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco Source: The New Yorker 1 Optimal Duration of
Optimal Duration of Dual Anti- Platelet Therapy December 19, 2015 John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco Source: The New Yorker 1 Optimal Duration of
ISCHEMIC HEART DISEASE
 ESC CONGRESS HIGHLIGHTS ISCHEMIC HEART DISEASE Francesco Cosentino (Stockholm, S) Declaration of Interest Advisory Board/Speaker: AstraZeneca, Roche, Boehringer-Ingelheim, Bristol-Myers Squibb, Merck,
ESC CONGRESS HIGHLIGHTS ISCHEMIC HEART DISEASE Francesco Cosentino (Stockholm, S) Declaration of Interest Advisory Board/Speaker: AstraZeneca, Roche, Boehringer-Ingelheim, Bristol-Myers Squibb, Merck,
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction. Is it beneficial to patients?
 Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Facilitated Percutaneous Coronary Intervention in Acute Myocardial Infarction Is it beneficial to patients? Seung-Jea Tahk, MD. PhD. Suwon, Korea Facilitated PCI.. background Degree of coronary flow at
Bivalirudin should be indicated for all patients with STEMI. Adnan Kastrati Deutsches Herzzentrum, Munich, Germany
 Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,
Bivalirudin should be indicated for all patients with STEMI Adnan Kastrati Deutsches Herzzentrum, Munich, Germany 1 Heparin+IIb/IIIa, heparin alone or bivalirudin in STEMI: Do we have the answer? 2 Heparin+IIb/IIIa,