TIA triage in Not all that glitters is gold
|
|
|
- Kevin Kristopher Fowler
- 6 years ago
- Views:
Transcription
1 TIA triage in 2016 Not all that glitters is gold
2 Disclosures No industry related disclosures Expert witness work
3 Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
4 Definition A TIA is a sudden neurological deficit, caused by a vascular problem, that completely resolves.
5 Definition A TIA is a sudden neurological deficit, caused by a vascular problem, that completely resolves. Key features 1 Sudden, as opposed to rapid Absence of nonspecifc symptoms
6 TIA A TIA is a sudden neurological deficit, caused by a vascular problem, that completely resolves. 20 min to 3 hrs There may or may not be evidence of infarction on MRI/DWI
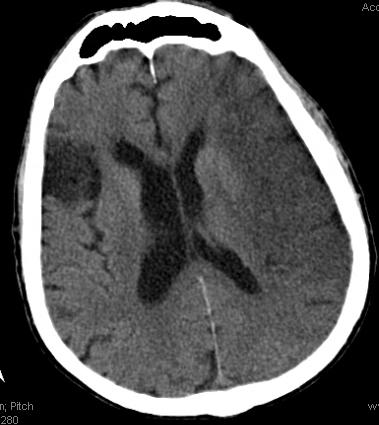
7 Case 1 82yoM with Atrial Fibrillation (INR 1.6) and old right frontal lobe ischemic stroke. P/W sudden speech problems, 19:45, totally resolved by 21:00 in the ED NIHSS=0 in the ED HCT unremarkable (except old infarct) HB
8 TIA: short term risk of stroke Study (year) 2 days 7 days 30 days Johnston (2000) 5% Lovett (2003) 9% 12% Gladstone (2004) 8% Coull (2004) 8% 12% Kleindorfer (2004) 4% 7% 11% Correia (2006) 13% Average 4.5% 8.5% 11%
9 TIA: short term risk of stroke Study (year) 2 days 7 days 30 days Johnston (2000) 5% Lovett (2003) 9% 12% Gladstone (2004) 8% Coull (2004) 8% 12% Kleindorfer (2004) 4% 7% 11% Correia (2006) 13% Average 4.5% 8.5% 11%
10 ABCD 2 score 2 Factor, points OR (95% CI) Age ( 60yrs = 1 point) 1.4 ( ) BP ( 140 mmhg systolic or 90 diastolic 1 point) 1.6 ( ) Clinical Features:.Unilateral weakness 2 points.speech impairment without weakness 1 point Duration: 60 minutes 2 points minutes 1 point 2.9 ( ) 1.4 ( ) 2.3 ( ) 2.0 ( ) Diabetes (Presence 1 point) 1.6 ( )
11 Risk stratification with ABCD 2 score 2 Days stroke Risk after TIA ABCD2 Score 25% 20% 15% 10% 5% 0% 0% 0% Low risk Moderate risk 1% 1% 4% 5% High risk 8% 6% 2 Day Stroke Risk
12 Risk stratification with ABCD 2 score Stroke Risk 25% 20% 15% 10% 5% 0% 2 day and 90 day stroke risk after TIA High risk Low risk 0% 2% 3% 3% Moderate risk 8% 12% 17% 22% 2 Day 90 Day ABCD2 score 4799 patients
13 Case 1 Who are the 0-8% of patients with TIA, who develop stroke in the fist 2 days?
14 Case 1 The patient s ABCD 2 score =4 2-day risk of stroke is 4% 90-day risk of stroke is 8% The mechanism of the TIA is probably known a-fib, while sub-therapeutic on warfarin
15 Case 1 We know the cause We have the treatment Our management options: A) Obtain immediate vascular imaging in ED B) Admit to hospital, observation, workup, anticoagulation C) Discharge home with bridge anticoagulation D) Discharge to home without bridge, but augment warfarin dose and recheck INR in 48hrs
16 Case 1 82yoM with Atrial Fibrillation (INR 1.6) and old right frontal lobe ischemic stroke. P/W sudden slurred speech, 19:45, totally resolved by 21:00 in the ED NIHSS=0 in the ED HCT unremarkable (except old infarct) Cr = 1.5, CTA deferred, pt admitted for MRA HB
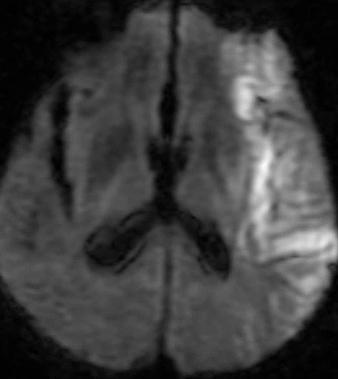
17 Case 1 Admitted, MRA pending Discovered in room, aphasic, right hemiparetic NIHSS = 22 HB
18 HB
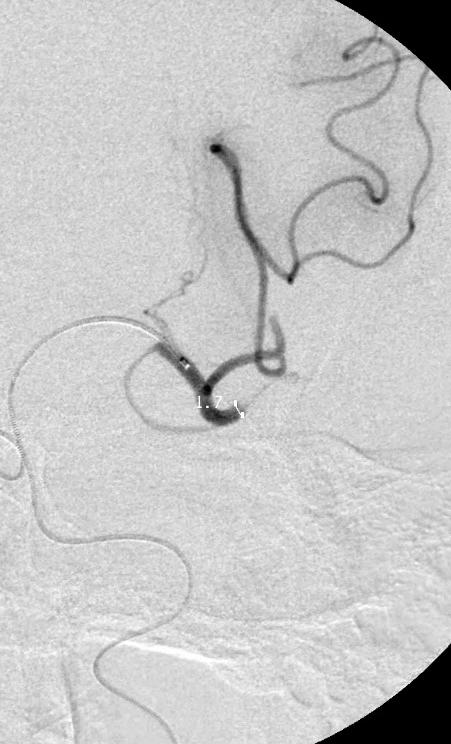
19 Case 1 Despite successful technical revascularization of a left M2 occlusion, the patient s deficits did not improve. Based on prior medical problems, was already dependent (mrs 2), the family withdrew care and the patient expired. HB
20 Case 1 Despite successful technical revascularization, of a left M2 occlusion, the patient s deficits did not improve. Based on prior medical problems, was already dependent (mrs 2), the family withdrew care and the patient expired. The patient went from no deficit to death. HB
21 Case 1 The left M2 occlusion caused the large stroke
22 Case 1 The left M2 occlusion caused the large stroke Was the left M2 occlusion present initially when his NIHSS resolved to 0?
23 Case 1 The left M2 occlusion caused the large stroke Was the left M2 occlusion present initially when his NIHSS resolved to 0? The ABCD score predicted low risk of stroke, so why did this happen?
24 Case 1 The left M2 occlusion caused the large stroke Was the left M2 occlusion present initially when his NIHSS resolved to 0? The ABCD score predicted low risk of stroke, so why did this happen? Is the ABCD score a tool we can use to triage the TIA patient?
25 Case 1 The left M2 occlusion caused the large stroke Was the left M2 occlusion present initially when his NIHSS resolved to 0? The ABCD score predicted low risk of stroke, so why did this happen? Is the ABCD score a tool we can use to triage the TIA patient? What is the cause of stroke following TIA?
26 What causes TIA in general?
27 What causes TIA in general? Cardioembolism Atrial fibrillation Cardiomyopathy Paradoxical Septic Atherothrombo/embolism Arch Extrancranial ICA, VA COW: MCA, iica, BA Dissection ICA, VA Lacunar lipohyalinosis Small vessel Cerebral Venous Thrombosis
28 Hypothesis One feature that characterized Case 1 is the presence of large vessel occlusion (LVO)
29 Hypothesis One feature that characterized Case 1 is the presence of large vessel occlusion (LVO) Hypothesis: LVO is associated with increased risk of stroke following TIA, regardless of ABCD 2 score.
30 Coutts et al (2008) 3 Prospective cohort study 180 pts with TIA or minor stroke (NIHSS 0-3), followed for 90 days Intracranial Vessel Occlusion n=24 (13%) In the 24 with LVO, 46% had symptomatic clinical progression Compared with 6% without LVO, RR 7.9 ( ) Presence of LVO raised the risk of stroke 8-fold University of Calgary
31 Coutts et al (2009) 4 Retrospective cohort, mild AIS or TIA, Had CT + CTA i/e 297 pts identified, 90 day follow up Outcome poor mrs 2 at 90d or d/c to other than home (rehab or nursing home) CTA: presence or absence of large vessel occlusion or severe (>50%) stenosis in either the circle of Willis (COW) or extracranial circulation
32 Coutts et al (2009) 4 In the poor outcome category, 27/57 (48%) had an LVO/SS COW + LVO/SS in 17/57(30%) of poor outcome vs 45/400(11%) of good outcome, p= Extracran + LVO/SS in 10/57 (18%) of poor outcome vs 35/400 (9%) of good outcome, p=0.054 The presence of LVO/SS is correlates with a poor outcome, especially if the lesion is in the Circle of Willis.
33 Smith et al (2009) STOPStroke 5, prospective cohort Stroke/TIA and CT/A 33 months, 735 enrolled, n=97 TIA Of the TIA cases, 13 (13%) had LVO Overall, +LVO associated with 4.5-fold increased odds of death (95%CI , p<0.001) and absent LVO +3.2-fold increased odds of good outcome (95% CI , p<0.001) They did not have enough TIA cases to study TIA specifically UCSF-MGH, Screening Technology and Outcome Project in Stroke Study
34 Predictors of risk of early stroke Higher ABCD 2 score Presence of LVO/SS
35 Predictors of risk of early stroke Higher ABCD 2 score Presence of LVO/SS But, does high ABCD 2 = LVO?
36 Predictors of risk of early stroke Higher ABCD 2 score Presence of LVO/SS But, does high ABCD 2 = LVO? There is little data Arterial dissection First presentation of atherosclerotic disease
37 Management Guidelines 7 Class 1 Evidence Patients with TIA should preferably undergo neuroimaging evaluation within 24 hours of symptom onset. Noninvasive imaging of the cervicocephalic vessels should be performed. Patients with suspected TIA should be evaluated as soon as possible.
38 Management Guidelines 7 ECG should occur as soon as possible; prolonged cardiac monitoring is useful in patients with an unclear Echocardiography (at least TTE) is reasonable, especially in patients in whom no cause has been identified by other elements of the
39 Prevention Guidelines 8 Antiplatelet medication BP control HMG CoA reductase inhibitors Revascularization for symptomatic carotid stenosis Anticoagulation for afib
40 What s lacking Hospitalization Admit, observation, or discharge Selection Testing Urgency of vascular imaging Urgency of echo, rhythm analysis, blood work Ranta and Barber (2016) 9 University of Otago, Auckland University, NZ
41 Model 1 Admit all TIA cases to hospital or ED observation unit, with input from a stroke specialist. Pro: expert-driven, ability to observe and treat in case of worsening Con: clinical benefit unproven; no cost benefit
42 Model 2 Sanders et al (2012) 10 ED assessment Persistent signs, crescendo TIA, other medical issues: admission Otherwise TIA clinic same or next day Vascular imaging: same or next day CDUS Afib: anticoagulation, priority for TIA clinic No afib, +CDUS ICAS>50%: CTA and priority to TIA clinic Monash University, Australia
43 Model patients with 90 day follow up 150 control admission method Outcome = stroke at 90 days Stroke 1.50% (7/468) in Model 2, vs 4.67% (7/150) in admission method
44 Model 3 SOS-TIA, Lavallee et al (2007) 11 Specialized 24/7 clinic Not clear who saw the pts, but 24/7 vascular neurologist available at least by phone CDUS, TCD and ECG If high suspicion, then urgent TTE Direct communication bw VN and PCP re secondary prevention strategy Discharge to home The Paris model, Bichat-Claude Bernard University
45 Model pts had definite TIA Overall 1.24% ( ) risk of stroke at 90 days, compared with estimated 5.96% based on ABCD 2 scores for this cohort
46 Model 4 Rothwell et al (2007) 12, EXPRESS study Compared routine TIA outpatient referral (med 3 days, CDUS, TTE, no immediate initiation of meds) to same-day open-access clinic (M-F) with immediate initiation of meds. Reduction of 90-day stroke from 10.3% to 2.1%, HR 0.2., , p = ) The Oxford model,
47 Model 5 Olivot (2011) 13 TWO ACES stud Prospective study, 224 pts that came to ED ABCD 2 = 0-3: sent from ED to TIA clinic (<48hr), MRA i/e or CTA i/e between ED and TIA clinic ABCD 2 = 4-5: CTA i/e CTA i/e lesion >50% stenosis, admission Otherwise, TIA clinic The Stanford model
48 Model 5 Pts referred to TIA clinic had a stroke rate of 0.6% at 7 days (same at 90 d!), compared with expected 4.0, 7.1 % risk based on ABCD 2 score, p<0.034, p<0.001
49 Model 6 Wasserman et al (2010) 14 ED visit, dx of TIA Outpt CDUS, TTE, FLP ABCD 2 6: 7 day f/u in TIA clinic ABCD 2 = 3-5: 14 day f/u in TIA clinic ABCD 2 < 4: >14 day f/u The Ottawa model
50 Model 6 >1000 pts, outcome stroke at 90 days ABCD2 score Strokes Predicted P <4 (n=321) 3, 0.9% (0-1.98) (n=469) 18, 3.8% ( ) 9.8 < (n=192) 10, 5.2% ( ) 17.8 < Combined 31, 3.2% ( ) 9.1 <0.0001
51 Model 7 Ranta et al (2015)15 PCP with web-based decision tool triage to TIA clinic vs usual care by PCP Web based tool High risk ABCD2>3, 2 or more recent events, presence of afib referral to TIA clinic 24 hrs Low risk TIA clinic within 7 days
52 Model 7 90-day stroke outcomes Intervention, 2/172 (1.2%) Control, 5/119 (4.2%) P = 0.098
53 Comparison Model Pro Con 1 -Full and immediate vascular imaging -Ability to intervene if patient worsens 2-7 -Avoids most hospitalization, cost savings -Unproven clinical benefit, higher cost -There is clinical benefit when compared with the ABCD 2 risk, ie compared with doing nothing.
54 What is the goal? Cost savings? Reduction of stroke risk?
55 Hypothetical goals Reduction of cost, hospitalization Elimination (not reduction) of risk of stroke This must include imaging of all cervicocranial vessels, knowing what we know about LVO and its strong correlation with poor outcome.
56 The UPMC-Mercy Model Brain and vascular imaging in ED MRI brain, MRA head and neck If no infarct, and no LVO/SS, then observe 24h: ABCD 2 >3, observe inpatient, complete workup ABCD 2 <3, observe in clinical decision unit in the ED, then discharge home
57 Beyond Mercy If there is no afib and no LVO/SS, then Antiplatelet Address BP, glucose, LDL Discharge home Outpatient Holter Follow up in Stroke clinic, next business day
58 1. Cerebrovasc Dis 2008;26: Lancet 2007; 369: Stroke 2008; 39: Intnl. J. Stroke, 2009; 4: Stroke 2009; 40: Neurohospitalist 2011; 1(4): Stroke 2009; 40: Stroke 2014; 45: Neurology 2016; 86: Stroke 2012; 43: Lancet Neurology 2007; 6: Lancet 2007;370: Stroke 2011; 42: Stroke 2010; 41: Neurology 2015;84: References
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Disclosures. An Update on TIA and Minor Stroke. The Agenda PROGNOSIS PATHOPHYSIOLOGY GUIDELINES AND PROVEN MANAGEMENT STRATEGIES AGGRESSIVE TREATMENT
 Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Disclosures An Update on TIA and Minor Stroke Dr. Johnston is principal investigator for the POINT trial, sponsored by the NIH but with drug and placebo contributed by Sanofi-Aventis. S. Claiborne Johnston,
Critical Review Form Therapy
 Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Critical Review Form Therapy A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects, Lancet-Neurology 2007; 6: 953-960 Objectives: To evaluate the effect of
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Emergently? Michigan Institute for Neurological Disorders. Garden City Hospital, Garden City, Michigan
 Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
Why Should TIA be Treated Emergently? Anne M. Pawlak, D.O. F.A.C.N. Michigan Institute for Neurological Disorders Director Neurology Residency Program, Garden City Hospital, Garden City, Michigan According
TRANSIENT ISCHEMIC ATTACK (TIA)
") TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
TRANSIENT ISCHEMIC ATTACK (TIA) AND MINOR STROKE Dr. Leanne K. Casaubon, MD MSc FRCPC Associate Professor, University of Toronto Director, TIA and Minor Stroke (TAMS) Unit University Health Network - Toronto
Redgrave JN, Coutts SB, Schulz UG et al. Systematic review of associations between the presence of acute ischemic lesions on
 6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
6. Imaging in TIA 6.1 What type of brain imaging should be used in suspected TIA? 6.2 Which patients with suspected TIA should be referred for urgent brain imaging? Evidence Tables IMAG1: After TIA/minor
Therapy for Acute Stroke. Systems of Care for TIA
 Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
Therapy for Acute Stroke and Systems of Care for TIA Gregory W. Albers, MD Coyote Foundation Professor of Neurology and Neurological Sciences Director, Stanford Stroke Center Stanford University Medical
David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK
 Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Risk Stratification in TIA/Stroke? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
How do we assess risk in TIA?
 How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
How do we assess risk in TIA? David Strain, Diabetes and Vascular Research Centre University of Exeter Medical School, UK Disclaimer I would never allow a scientist to partake in my government Give them
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE Dr. Grant Stotts Staff Neurologist, Ottawa Hospital Director, Ottawa Stroke Program Medical Director, Champlain Regional Stroke Program
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
TIA. What it is, What it isn t, What to do about it, and When WM. BLAINE BENDURE, MD, MS BOARD CERTIFIED NEUROLOGIST
 TIA What it is, What it isn t, What to do about it, and When WM. BLAINE BENDURE, MD, MS BOARD CERTIFIED NEUROLOGIST Disclosures I have no financial disclosures. Goals By the end of the talk the audience
TIA What it is, What it isn t, What to do about it, and When WM. BLAINE BENDURE, MD, MS BOARD CERTIFIED NEUROLOGIST Disclosures I have no financial disclosures. Goals By the end of the talk the audience
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017
 KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017 1 Faculty Disclosure Faculty: Grant Stotts MD, FRCPC Assistant Professor, uottawa Brain and Mind Institute
KEEPING YOUR PATIENT OUT OF THE HOSPITAL BY PREVENTING A SECOND STROKE OR TIA December 8, 2017 1 Faculty Disclosure Faculty: Grant Stotts MD, FRCPC Assistant Professor, uottawa Brain and Mind Institute
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Document Title: The Management of Acute Ischemic Stroke & TIA
 Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Project: Ghana Emergency Medicine Collaborative Document Title: The Management of Acute Ischemic Stroke & TIA Author(s): Rashmi U. Kothari, M.D. (KCMS/MSU), 2012 License: Unless otherwise noted, this material
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Intracranial Atherosclerosis in Asians
 Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Can ABCD 2 score predict the need for in-hospital intervention in patients with transient ischemic attacks?
 Int J Emerg Med (2010) 3:75 80 DOI 10.1007/s12245-010-0176-x ORIGINAL RESEARCH ARTICLE Can ABCD 2 score predict the need for in-hospital intervention in patients with transient ischemic attacks? Min Lou
Int J Emerg Med (2010) 3:75 80 DOI 10.1007/s12245-010-0176-x ORIGINAL RESEARCH ARTICLE Can ABCD 2 score predict the need for in-hospital intervention in patients with transient ischemic attacks? Min Lou
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
The annual incidence of TIA in the United States is
 TWO ACES Transient Ischemic Attack Work-Up as Outpatient Assessment of Clinical Evaluation and Safety Jean-Marc Olivot, MD, PhD; Connie Wolford, NP; James Castle, MD; Michael Mlynash, MD, MS; Neil E. Schwartz,
TWO ACES Transient Ischemic Attack Work-Up as Outpatient Assessment of Clinical Evaluation and Safety Jean-Marc Olivot, MD, PhD; Connie Wolford, NP; James Castle, MD; Michael Mlynash, MD, MS; Neil E. Schwartz,
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Does ABCD 2 Score Below 4 Allow More Time to Evaluate Patients With a Transient Ischemic Attack?
 Does Below 4 Allow More Time to Evaluate Patients With a Transient Ischemic Attack? Pierre Amarenco, MD; Julien Labreuche, BS; Philippa C. Lavallée, MD; Elena Meseguer, MD; Lucie Cabrejo, MD; Tarik Slaoui,
Does Below 4 Allow More Time to Evaluate Patients With a Transient Ischemic Attack? Pierre Amarenco, MD; Julien Labreuche, BS; Philippa C. Lavallée, MD; Elena Meseguer, MD; Lucie Cabrejo, MD; Tarik Slaoui,
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease
 Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
Clinical Decision Making: Hyperacute Management of Symptomatic Carotid Artery Disease Tarvinder Singh, MS, MD Neurohospitalist Swedish Neuroscience Institute 1 Objectives Definition Why the urgency? Evidence/Guidelines
44TH ANNUAL RECENT ADVANCES IN NEUROLOGY
 Presenter Disclosure Information J. Donald Easton, MD Clinical Professor of Neurology February 17, 2011 44TH ANNUAL RECENT ADVANCES IN NEUROLOGY TIA: Definition, Evaluation, and Treatment J. Donald Easton,
Presenter Disclosure Information J. Donald Easton, MD Clinical Professor of Neurology February 17, 2011 44TH ANNUAL RECENT ADVANCES IN NEUROLOGY TIA: Definition, Evaluation, and Treatment J. Donald Easton,
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Early Hospitalization of Patients with TIA: A Prospective, Population-based Study
 Early Hospitalization of Patients with TIA: A Prospective, Population-based Study Mohamed Al-Khaled, MD, and J urgen Eggers, MD Background: The German Stroke Society (GSS) recommends early hospitalization
Early Hospitalization of Patients with TIA: A Prospective, Population-based Study Mohamed Al-Khaled, MD, and J urgen Eggers, MD Background: The German Stroke Society (GSS) recommends early hospitalization
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Direct oral anticoagulants for Embolic Strokes of Undetermined Source? George Ntaios University of Thessaly, Larissa/Greece
 Direct oral anticoagulants for Embolic Strokes of Undetermined Source? George Ntaios University of Thessaly, Larissa/Greece Disclosures Scholarships: European Stroke Organization; Hellenic Society of Atherosclerosis.
Direct oral anticoagulants for Embolic Strokes of Undetermined Source? George Ntaios University of Thessaly, Larissa/Greece Disclosures Scholarships: European Stroke Organization; Hellenic Society of Atherosclerosis.
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia
 GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
GROUPE HOSPITALIER BICHAT-CLAUDE BERNARD PARIS DIDEROT UNIVERSITY - PARIS 7 Session Antiplatelet Therapy: How, Why and When? In patients with ischemic stroke/tia Pierre Amarenco INSERM U-698 and Denis
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
GOVERNANCE BOARD. 14th January Clinical Audit of Stroke Services. At Shrewsbury and Telford Hospitals NHS Trust
 GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
GOVERNANCE BOARD 14th January 2014 Clinical Audit of Stroke Services At Shrewsbury and Telford Hospitals NHS Trust 1.0 Introduction A clinical review of cases recorded and coded as with a 0-1 day length
Supplementary Online Content
 Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Management of TIA. Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital
 Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Management of TIA Dr Ali Ali Consultant Stroke and Geriatrics Royal Hallamshire Hospital Objectives Definition TIA and stroke TIA: Diagnosis & mimics Risk assessment Referral and emergency management Secondary
Reducing delays to outpatient assessment of strokes and TIAs
 Reducing delays to outpatient assessment of strokes and TIAs Prof Martin Dennis Stroke Physician (Lothian) Clinical lead for Scottish Stroke Care Audit The patient pathway Step 1 Possible TIA, minor stroke
Reducing delays to outpatient assessment of strokes and TIAs Prof Martin Dennis Stroke Physician (Lothian) Clinical lead for Scottish Stroke Care Audit The patient pathway Step 1 Possible TIA, minor stroke
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
The Atrial Fibrillation Clinic in Llanelli. Dr Lena Marie Izzat Consultant Cardiovascular Physician
 The Atrial Fibrillation Clinic in Llanelli Dr Lena Marie Izzat Consultant Cardiovascular Physician Llanelli Multidisciplinary AF Clinic Went live January 2009 Based on the fact that Carmarthenshire has
The Atrial Fibrillation Clinic in Llanelli Dr Lena Marie Izzat Consultant Cardiovascular Physician Llanelli Multidisciplinary AF Clinic Went live January 2009 Based on the fact that Carmarthenshire has
Recent Advances in Neurology Difficult Cases
 Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute Quotes Benjamin Franklin: All would live long, but none would be old.
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to
 It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
It is the nature of a stroke to partly take away the use of a man s limbs and to throw him onto the parish if he had no children to look to George Eliot The Cripples (1949) All cerebrovascular events in
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Endovascular Neurointervention in Cerebral Ischemia
 Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Endovascular Neurointervention in Cerebral Ischemia Beyond Thrombolytics Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington 72 y/o female with a recent diagnosis
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015
 Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
Carotid Artery Surgery for the Prevention and Treatment of Ischemic Stroke Update 2015 John L. Crawford, MD, FACS Neuroscience Summit 2015 UNT Health Sciences Center September 12, 2015 www.cdc.gov/datastatistics2013
A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects
: feasibility and effects") A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects Philippa C Lavallée, Elena Meseguer, Halim Abboud, Lucie Cabrejo, Jean-Marc Olivot, Olivier Simon, Mikael
A transient ischaemic attack clinic with round-the-clock access (SOS-TIA): feasibility and effects Philippa C Lavallée, Elena Meseguer, Halim Abboud, Lucie Cabrejo, Jean-Marc Olivot, Olivier Simon, Mikael
Alma Mater Studiorum Università di Bologna
 Alma Mater Studiorum Università di Bologna S.Orsola-Malpighi, Bologna, Italia Chirurgia Vascolare The volume of cerebral ischaemic lesion predicts the outcome after symptomatic carotid revascularisation
Alma Mater Studiorum Università di Bologna S.Orsola-Malpighi, Bologna, Italia Chirurgia Vascolare The volume of cerebral ischaemic lesion predicts the outcome after symptomatic carotid revascularisation
Session : Why do stroke patients need a cardiologist? PREVALENCE OF CORONARY ATHEROSCLEROSIS IN PATIENTS WITH CEREBRAL INFARCTION
 Session : Why do stroke patients need a cardiologist? PREVALENCE OF CORONARY ATHEROSCLEROSIS IN PATIENTS WITH CEREBRAL INFARCTION The Asymptomatic Myocardial Ischemia in Stroke and Atherosclerotic Disease
Session : Why do stroke patients need a cardiologist? PREVALENCE OF CORONARY ATHEROSCLEROSIS IN PATIENTS WITH CEREBRAL INFARCTION The Asymptomatic Myocardial Ischemia in Stroke and Atherosclerotic Disease
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Retrospective Study on the Safety and Efficacy of Clopidogrel in the Treatment of Acute Cerebral Infarction
 International Journal of Neurologic Physical Therapy 2018; 4(1): 24-28 http://www.sciencepublishinggroup.com/j/ijnpt doi: 10.11648/j.ijnpt.20180401.14 ISSN: 2575-176X (Print); ISSN: 2575-1778 (Online)
International Journal of Neurologic Physical Therapy 2018; 4(1): 24-28 http://www.sciencepublishinggroup.com/j/ijnpt doi: 10.11648/j.ijnpt.20180401.14 ISSN: 2575-176X (Print); ISSN: 2575-1778 (Online)
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Emergency Department Stroke Registry Process of Care Indicator Specifications (July 1, 2011 June 30, 2012 Dates of Service)
") Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Specifications Description Methodology NIH Stroke Scale (NIHSS) Performed in Initial Evaluation used to assess the percentage of adult stroke patients who had the NIHSS performed during their initial evaluation
Chinook Regional Hospital Stroke Alert Cases
 Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Chinook Regional Hospital Stroke Alert Cases Background 53,260 ED Department visits last year Stroke Alert started October 19, 2015 106 minutes Median DTN at beginning of QuiCR project 73 Stroke Alert
Supplementary Online Content
 Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Supplementary Online Content Inohara T, Xian Y, Liang L, et al. Association of intracerebral hemorrhage among patients taking non vitamin K antagonist vs vitamin K antagonist oral anticoagulants with in-hospital
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew