The Fontan patient: Anesthetic aspects of the Fontan patient. Stan Outtier & Mathias Mund
|
|
|
- Juniper Willis
- 6 years ago
- Views:
Transcription
1 The Fontan patient: Anesthetic aspects of the Fontan patient Stan Outtier & Mathias Mund Dr. L. Altmimi
2 Overview 1. Brief overview of congenital heart diseases 2. History of Fontan procedure 3. Today s Fontan procedure 4. Physiology after Fontan repair 5. Preoperative assessment 6. Peri-operative management after Fontan repair 7. Outcomes and complications 8. Conclusion
3 Brief overview of congenital heart diseases incidence of congenital heart disease: 4 to 50 in 1,000 live births in addition, another 20 in 1,000 live births have: o bicuspid aortic valves o isolated anomalous lobar pulmonary veins o a silent patent ductus arteriosus Hoffmann, JI; The incidence of congenital heart disease. J Am Coll Cardiol Jun 19;39(12):

4 Many complex cardiac malformations are characterized by the existence of only one functional ventricle = Univentricular hearts 7.7% of congenital heart disease diagnosed in childhood birth incidence of approximately 4 8 per 10,000 increasing fraction are being recognized by prenatal ultrasound O Leary, P.; Prevalence, clinical presentation and natural history of patients with single ventricle, Rochester, MN, USA, El Sevier, 2002
5 History of Fontan procedure "Fontan procedure" or "Fontan - Kreutzer procedure" is a palliative surgical procedure performed in children with univentricular hearts. 2 major disadvantages of a single ventricle: o o Arterial desaturation Chronic volume overload CHF death

 1958:")
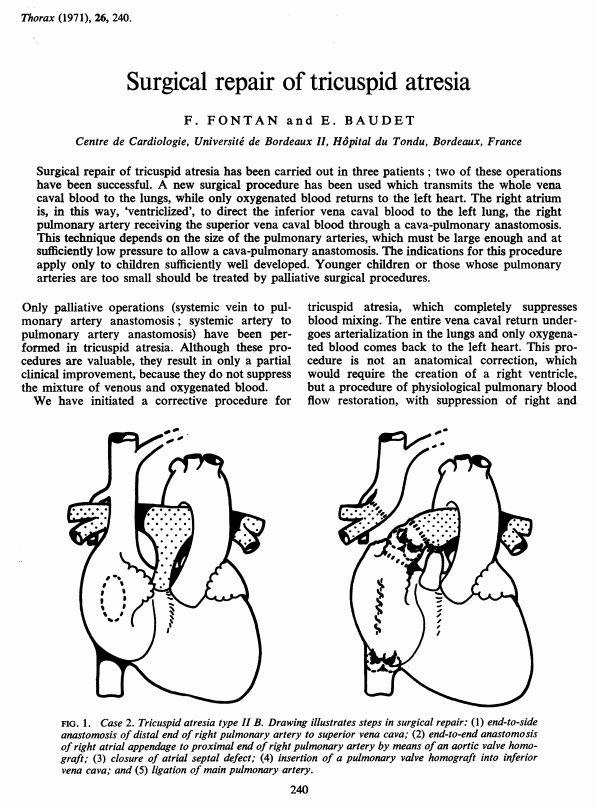
6 - described as a surgical treatment for tricuspid atresia separately by: Dr. François Fontan, Bordeaux, France (1971) Dr. Guillermo Kreutzer, Buenos Aires, Argentina (1973) 1958: Glenn procedure (= hemi-fontan) 1943: Blalock-Thomas-Taussig shunt
7
8 1973: Kreutzer s alternative to the Fontan procedure
9 Today s Fontan procedure Indications Contra-indications Recommendations for a successful Fontan circulation Approach
10 Indications for Fontan repair Cardiac malformations with a single functional ventricle abscence of an AV heart valve (e.g. tricuspid or mitral atresia) absence of pumping ability of the heart (e.g. hypoplastic right/left heart syndrome) a complex congenital heart disease where a bi-ventricular repair is impossible or inadvisable
11 Indications for Fontan repair Tricuspid atresia Double inlet left ventricle Hypoplastic left heart syndrome unbalanced atrioventricular septum defect
12 Univentricular heart The single ventricle is doing nearly twice the expected amount of work because it has to pump blood for the body and the lungs. Clinical manifestations (typically cyanosis and CHF) hinge on the presence or absence of pulmonary and systemic outflow obstruction. Natural history Left ventricle dominant = 70% died before age of 16. Right ventricle dominant = 50% died before age of 4. Fontan operation: 20-year survival rate and freedom of heart transplantation of 80%. Staged repair allows progressive adaption of the heart and lungs and reduces the overall perioperative morbidity and mortality.
13 Contra-indications for Fontan repair After Fontan completion, blood must flow through the lungs without being pumped by the heart Few absolute contraindications: o high pulmonary vascular resistance (> 4 Wood units.m 2 ) o o severe hypoplasia of the pulmonary arteries severe diastolic dysfunction of the single ventricle After birth the pulmonary vascular resistance is high in utero and takes months to drop Fontan procedure cannot be done immediately after birth.
14 Timing for Fontan repair Age at which Fontan is performed is steadily lowered o 2 years or younger if good anatomy and physiology Advantage: o o o o oxygenation somatic growth neurodevelopmental outcomes volume load on the single ventricle

15 1977: Choussat s Ten Commandments Age >4 years Sinus rhythm Normal systemic venous return Normal right atrial volume Mean pulmonary artery pressure <15 mm Hg Pulmonary arteriolar resistance <4 Wood units.m 2 Pulmonary artery aorta ratio >0.75 Left-ventricular ejection fraction >0.60 Competent mitral valve Absence of pulmonary artery distortion Stern HJ, Fontan "Ten Commandments" revisited and revised, Pediatr Cardiol Nov;31(8): doi: /s Epub 2010 Oct 20.
16 Recommendations for a successful Fontan circulation Cardiac requirements: Unobstructed ventricular inflow no AV valve stenosis, no regurgitation Reasonable ventricular function Unobstructed outflow no subaortic stenosis, no AHT, no coarctation Pulmonary requirements: Non restrictive connection from systemic veins to pulmonary arteries Good sized pulmonary arteries Well developed distal vascular bed (near) normal pulmonary vascular resistance

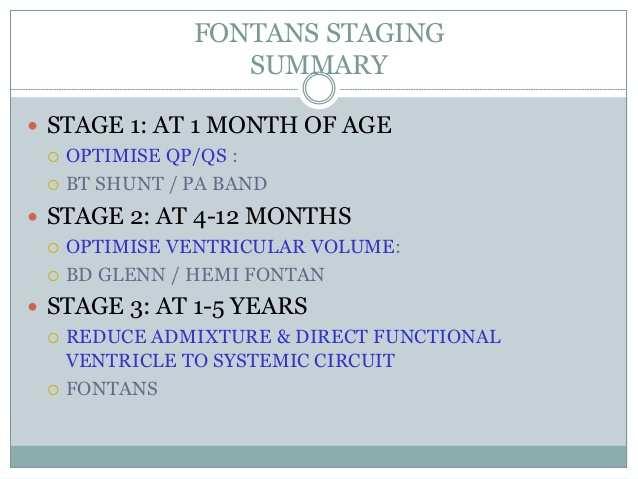
17 Approach Operative stages for achieving a Fontan circulation: 1. Newborn period: aim to balance the blood flow between the lungs and the body, achieving stable oxygen levels and adequate heart function. not enough blood flow into the lungs hypoxemia PDA stenting

18 Approach Operative stages for achieving a Fontan circulation: 1. Newborn period: aim to balance the blood flow between the lungs and the body, achieving stable oxygen levels and adequate heart function. not enough blood flow into the lungs hypoxemia systemic to pulmonary artery shunt = Blalock-Taussig shunt
19 Approach Advantages of BTS: oxygen saturation growth of pulmonary arteries Disadvantages of BTS: ventricular volume overload pulmonary arterial pressure distortion of pulmonary arteries
20 Approach Operative stages for achieving a Fontan circulation: 1. Newborn period: aim to balance the blood flow between the lungs and the body, achieving stable oxygen levels and adequate heart function. too much blood flow into the lungs extra burden on ventricle pulmonary hypertension Pulmonary banding

21 Approach Operative stages for achieving a Fontan circulation: 1. Newborn period: aim to balance the blood flow between the lungs and the body, achieving stable oxygen levels and adequate heart function. Setting: HLHS Modified Norwood 1 Sano repair o o o o First 2 weeks of life Permanent systemic outflow utilising the right ventricle Temporary pulmonary blood supply to allow the pulmonary vasculature to develop Up to 20-25% mortality rate
22 Approach Operative stages for achieving a Fontan circulation: HLHS: Modified Norwood 1 Main pulmonary artery is divided Proximal MPA is anastomosed to the ascending aorta Aortic arch is repaired Augmented pulmonary blood flow is maintained via a modified BTS


23 Approach Operative stages for achieving a Fontan circulation: HLHS: Modified Norwood 1

24 Approach Operative stages for achieving a Fontan circulation: HLHS: Sano repair Similar to NW1 RV-PA instead of BTS Theoretical advantage: no competitive flow between the lungs and coronary arteries Theoretical disadvantage: may be more invasive, obstruction
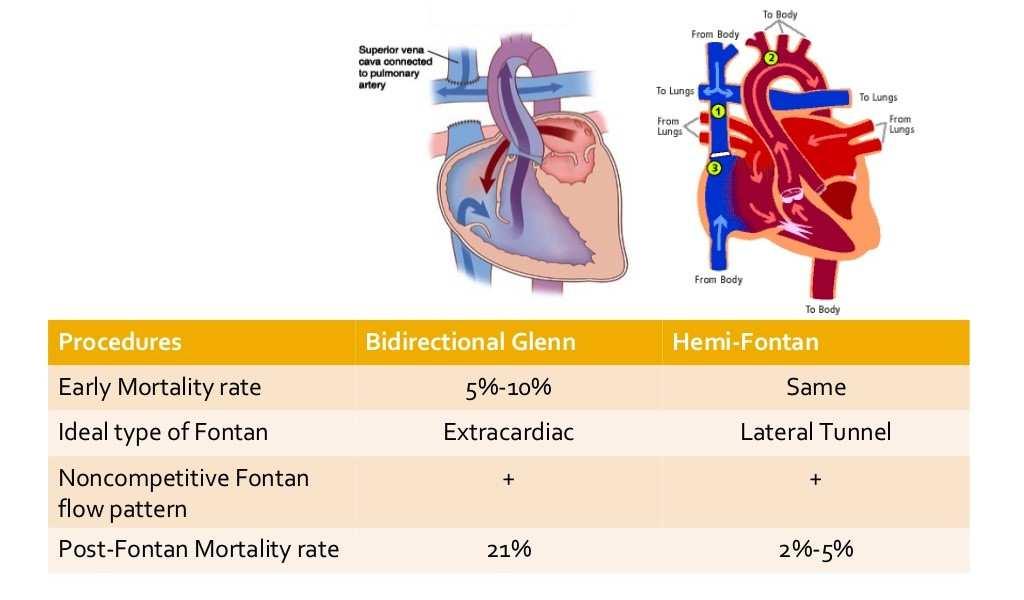
25 Approach Operative stages for achieving a Fontan circulation: 2. Late infancy: Bi-directional Glenn Superior cavopulmonary anastomosis Hemi-Fontan Around 3 to 6 months of age, when PVR If BTS present, it is removed If PA banding is present, it may be removed but can also be left in place

26 Approach Operative stages for achieving a Fontan circulation: 2. Late infancy: Bi-directional Glenn


27 Approach Operative stages for achieving a Fontan circulation: 2. Late infancy: Hemi-Fontan
28 Approach Operative stages for achieving a Fontan circulation: 2. Late infancy: Bi-directional Glenn or Hemi-Fontan Advantages of superior cavopulmonary anastomosis: o o ability to grow with the child >< BTS intracardiac volume overload o cyanosis (oxygen saturation levels 75-85%) Disadvantage of superior cavopulmonary anastomosis: o PAVMs occur in 20% of SCPA (exclusion of growth modulating factor liver?) This stage is tolerated best of all stages with a survival rate of 95% or better.
29
30
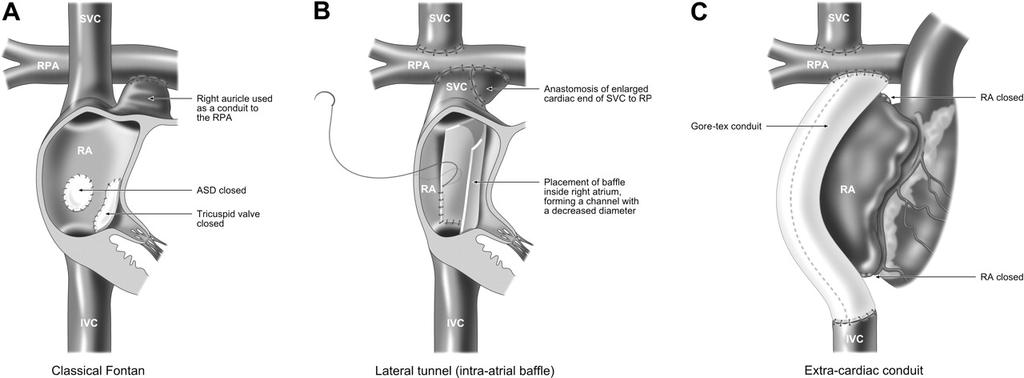
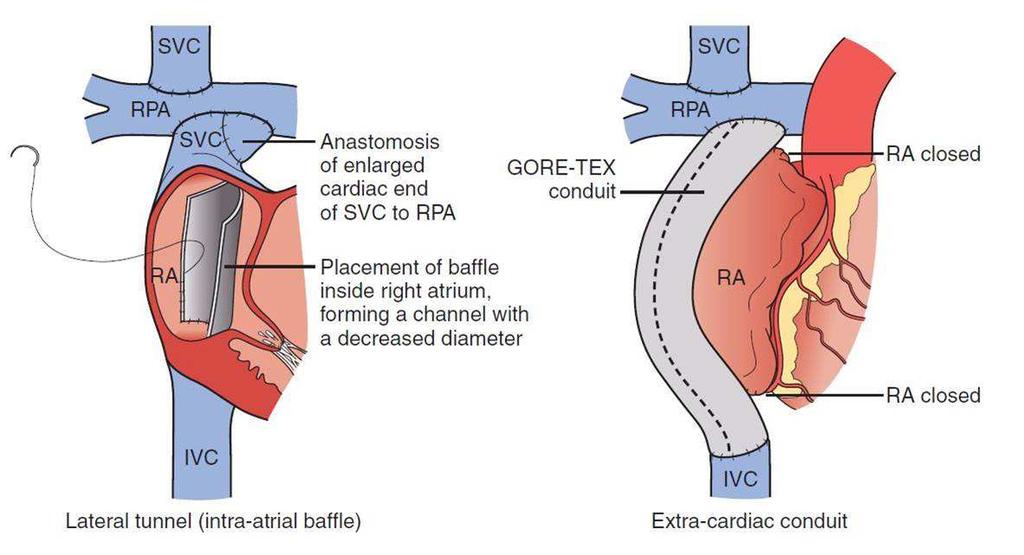
31 Approach Operative stages for achieving a Fontan circulation: 3. Childhood: Total cavopulmonary connection Fontan completion 18 months 4 years old 6-18 months post-glenn or hemi-fontan: if later risk for intrapulmonary arteriovenous shunts 3 types: o o o Atriopulmonary connection = Original Fontan Intracardiac total cavopulmonary connection (lateral tunnel) Extracardiac total cavopulmonary connection Modified Fontan
32

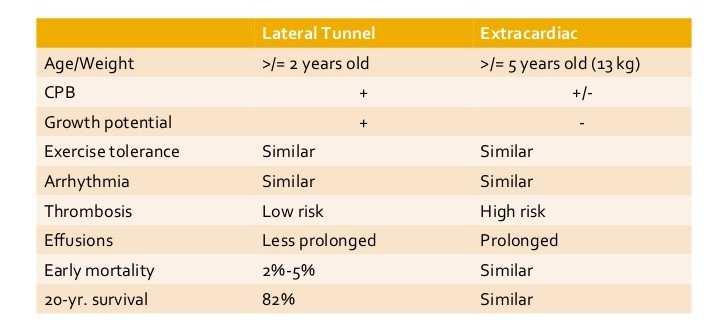
33 The modern Fontan operation: Lateral Tunnel Fontan improved pulmonary blood flow only the lateral wall of the atrium is exposed to central venous hypertension no dilated atrium to serve as a source of thrombus extensive atrial suture lines = risk for arrhythmia.

34 The modern Fontan operation: Extracardiac Fontan Conduit made of polytetrafluroethylene connects VCI to RPA. greatly reduces the number of atrial incisions and hopefully the long-term development of atrial arrhythmias.
35
36
37
38 Physiology after Fontan repair The normal cardiovascular circulation
39 Physiology after Fontan repair The patient with a univentricular heart
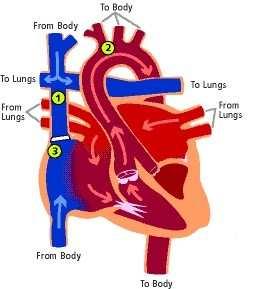
40 Physiology after Fontan repair The Fontan Circulation
41 Preoperative assessment of the Fontan patient directed history: o functional status o presence of major complications after Fontan surgery striking reductions in anaerobic threshold (< 50% of control subjects) o VO2 max (< 33% of control subjects) patients' self-assessment grossly overestimates their objective exercise capacity. (Cardiac Anesthesia, Kaplan J., El Sevier, Sixth edition, 2006, pp. 645)
42 The functional state of Fontan patients falls into two groups: 1. Majority of patients: New York Heart Association Class I-II level of function much less cardiorespiratory reserve than age-matched two-ventricle control subjects will tolerate most surgical procedures with an acceptably low risk. 2. Minority of patients: manifested one of more of the failing Fontan criteria. surgery = greater risk should only be undertaken after careful consultation
43 Failing Fontan = a marked limitation of functional status. manifests as combination of Refractory arrhythmias Protein loosing enteropathy Liver dysfunction Hypoxemia Congestive heart failure How to deal with Failing Fontan? search for correctable lesions obstructions within the Fontan pathway percutaneous techniques of dilation and stenting loss of sinus rhythm pacing severe tachyarrhythmias Fontan conversion surgery
44 Aortopulmonary collaterals progressive volume overload single ventricle. Collaterals from the venous system to the systemic atrium or ventricle hypoxemia. If collateral vessels: o coil occlusion in the catheterization lab. o creation of a fenestration cardiac output lower central venous pressures right-to-left shunt.
45 Technical investigations TTE = initial preoperative investigation o o Mandatory except for minor surgery Normal ventricular function = low risk only in the context of patients with Fontan circulation. Further testing is guided by the results of the TTE and in consultation with an cardiologist experienced in CHD. CXR: lung disease ECG: rhythm MRI: pulmonary arterial anatomy and flows, collateral circulation Cardiac cath: pulmonary arterial anatomy, PVR

46 Pregnancy Can a Fontan patient cope with increased cardiovascular demands of pregnancy? o myocardial oxygenconsumption 20% o heart rate 20% o stroke volume 40% Fontan patients are known to have decreased cardiac reserve Because pregnancy is a stress test, who will pass this test and who will fail? Carp H, Jayaram A, Vadhera R, et al: Epidural anesthesia for cesarean delivery and vaginal birth after maternal Fontan repair: report of two cases, Anesth Analg 78: , Fyfe DA, Gillette PC, Jones JS, et al: Successful pregnancy following modified Fontan procedure in a patient with tricuspid atresia and recurrent atrial flutter, Am Heart J 117: , 1989.
47 Pregnancy Literature provides conflicting data: 1 series of 33 pregnancies found women tolerated pregnancy, labor, and delivery well, but there was an increased risk for spontaneous abortion. A smaller series found live birth pregnancies complicated by: o o o o o high rates of NYHA class deterioration atrial arrhythmia thromboembolism prematurity intrauterine growth retardation
48 Pregnancy What can be made of these reports? retrospective and self-reporting provide reassuring information pregnancy only in patients with relatively good functional status o high infertility rate (21%) pregnancy can be successfully carried to term o miscarriage (33%) o premature delivery (70%) epidural analgesia is well tolerated and recommended for the first stage of labor
49 Pregnancy Caesarian section rate = 50% neuraxial anesthesia for Caesarian section preserves spontaneous ventilation no increased risk from general anesthesia was identified perioperative complications are low peripartum cardiac decompensation is rare
50 Perioperative management after Fontan repair Management principles for patients with Fontan physiology: 1. Maintenance of preload. Avoid a prolonged period without intravenous hydration. Vascular capacitance in the Fontan patient 2. Use regional and neuraxial techniques. Attention to volume status Bad choice if high level of block is required Slowly titrated epidural > spinal anesthetic 3. Avoid increases in pulmonary vascular resistance Avoid hypercarbia, hypoxemia, acidosis, stress, pain, high intrathoracic pressures
51 4. Adequate levels of anesthesia during laryngoscopy. catecholamines dangerous tachycardia. 5. Spontaneous ventilation if possible. pulmonary blood flow and venous return cave: hypercarbia! 6. Treat tachyarrhythmias. 7. Check pacemakers Avoid interference electrocautery 8. invasive monitoring with central lines and transesophageal echocardiography Fluid management guided by CVP or TEE Assess contractility
52 9. Anesthetic technique Similar to patients with acquired coronary artery disease no right drug for these patients It is not the drugs used, but rather how they are used 10. postoperative pain management. Adequate analgesia improves pulmonary mechanics and oxygenation Avoid the effects of hypercapnia secondary to opioids Epidural analgesia useful but may not be possible because of anticoagulation 11. Experienced cardiologist should be involved perioperatively
53 Ventilatory Management minimize pulmonary vascular resistance, avoid hypercarbia. functional residual capacity should be maintained by the application of small amounts of PEEP or CPAP (<6 cm H2O) excessive lung volumes should be avoided limit peak inspiratory pressure (<20 cmh2o) use spontaneous ventilation to o minimize intrathoracic pressure o encourage forward flow into the pulmonary circulation
54 Outcome Fontan procedure is palliative, not curative can result in normal or near-normal growth, development, exercise tolerance, and good quality of life. but freedom from morbidity is unlikely in the long term. in 20-30% cases patients will eventually require heart transplantation
55 Survival curves representing the observed outcomes for patients with single ventricle after the Fontan operation. Fontan F, Kirklin J, Fernandez G, et al. Outcome after a perfect Fontan operation. Circulation 1990;81: Driscoll D, Offord K, Feldt R, Schaff H, Puga F, Danielson G. Five- to fifteen-year follow-up after Fontan operation. Circulation 1992;85: Gentles T, Mayer J, Gauvreau K, et al. Fontan operation in five hundred consecutive patients: factors influencing early and late outcome. J. Thorac. Cardiovasc. Surg. 1997;114: Cetta F, Feldt RH, O Leary PW, et al. Improved early morbidity and mortality after Fontan operation: the Mayo Clinic experience, 1987 to J. Am. Coll. Cardiol. 1996;28: Stamm C, Friehs I, Mayer J, et al. Long-term results of the lateral tunnel Fontan operation. J. Thorac. Cardiovasc. Surg. 2001;121:28 41.
56
57 While early reports showed improved long-term survival rates, recent modifications have produced even better results. Multiple centers have reported greater than 80% survival rates at more than 5 years after Fontan. Stamm et al. from Boston Children s Hospital achieved a 10-year survival of 87%. Evolving surgical techniques, improved selection criteria and the ability to perform the operation at younger ages with low early risk have all contributed to improved outcomes.
58
59 Significant risk factors for early mortality Cetta et al. development of postoperative renal failure elevated postoperative right atrial pressures: 20 mmhg presence of a common atrioventricular valve. (duration of follow-up in this group was not long enough to identify factors associated with late mortality) Cetta F, Feldt RH, O Leary PW, et al. Improved early morbidity and mortality after Fontan operation: the Mayo Clinic experience, 1987 to J. Am. Coll. Cardiol. 1996;28:
.")
60 Complications Short term complications after Fontan pleural effusions (25%) o fenestration from the venous circulation atrium When the pressure in the veins is high, some of the oxygen-poor blood can escape through the fenestration to relieve the pressure. This results in hypoxia, so the fenestration may eventually need to be closed by an interventional cardiologist. Rychik, Jack (2016). Relentless Effects of the Fontan Paradox. Seminars in Thoracic and Cardiovascular Surgery. 19 (1): doi: /j.pcsu
61 Long term complications after Fontan Arrythmia (10-40%) high incidence related to multiple suture lines near the sinus node atrial enlargement atrial pressure. Loss of atrioventricular synchronisation pulmonary venous atrial pressure ventricular preload Poorly tolerated: immediate cardioversion may be necessary full anticoagulation
62 Thromboembolism (30%) low flow state atrial scarring arrythmias dehydration hypercoagulable state
63 Lymphatic abnormalities venous pressure impaired thoracic duct drainage 1. Interstitial pulmonary edema 2. Lymphedema 3. Protein loosing enteropathy (13%) Excessive loss of serum proteins in intestinal lumen with mesenteric vascular inflammation Poor prognosis: 60% 5 year survival, 20% 10 year survival after diagnosis
64 Lymphatic abnormalities 3. Protein loosing enteropathy (13%) Manifestations: o edema o immunodeficiency o ascites o fat malabsorption o hypercoagulopathy o hypocalcemia o Hypomagnesaemia Treatment: - diet low in salt, high in calories, protein content and MCT - diuretics, CS, heparin, octreotide - fenestration, Fontan revision, hearttransplant
65 Shunts Left to right Aortopulmonary collaterals volume overload high regional pulmonary flow PVR Right to left Residual shunt through fenestration Drainage coronary sinus into systemic circulation Desaturation
66 Lymphatic abnormalities 4. Plastic bronchitis (1-2%) Non-inflammatory mucinous casts that form in the tracheobronchial tree and obstruct the airway enteric loss of alpha-1-antitrypsin Manifestations: o Dyspnea o Cough asphyxia o Wheezing cardiac arrest o Expectoration of casts death Treatment: - management is difficult: repeat bronchoscopy - fenestration, Fontan revision, hearttransplant
67 Diminished exercise tolerance and ventricular dysfunction (70%) Volume overloaded ventricle underloaded ventricle The deprived ventricle shows signs of systolic and diastolic dysfunction Low preload remodeling reduced compliance poor ventricular filling cardiac output This phenomenon occurs at a chronic preload of less than 70% of the due preload = Progressive disuse hypofunction
68 Sources: Kaplan Joel, Kaplan s Cardiac Anesthesia: The Echo Era. Sixth edition. D'Udekem Y, Iyengar AJ, Cochrane AD, et al: The Fontan procedure: Contemporary techniques have improved long-term outcomes.circulation 116:I157, 2007 Fontan, F.,1971, Surgical repair of tricuspid atresia Gutfried, C., 2003, Ventrikeldimension, Masse und Funktion spät nach Fontan-Operation Quantifizierung durch Magnet Resonanz Tomographie O Leary, P.; Prevalence, clinical presentation and natural history of patients with single ventricle, Rochester, MN, USA, El Sevier, 2002 Hoffmann, JI; The incidence of congenital heart disease. J Am Coll Cardiol Jun 19;39(12): Stern HJ, Fontan "Ten Commandments" revisited and revised, Pediatr Cardiol Nov;31(8): doi: /s Epub 2010 Oct 20. Carp H, Jayaram A, Vadhera R, et al: Epidural anesthesia for cesarean delivery and vaginal birth after maternal Fontan repair: report of two cases, Anesth Analg 78: , Fyfe DA, Gillette PC, Jones JS, et al: Successful pregnancy following modified Fontan procedure in a patient with tricuspid atresia and recurrent atrial flutter, Am Heart J 117: , Fontan F, Kirklin J, Fernandez G, et al. Outcome after a perfect Fontan operation. Circulation 1990;81: Driscoll D, Offord K, Feldt R, Schaff H, Puga F, Danielson G. Five- to fifteen-year follow-up after Fontan operation. Circulation 1992;85: Gentles T, Mayer J, Gauvreau K, et al. Fontan operation in five hundred consecutive patients: factors influencing early and late outcome. J. Thorac. Cardiovasc. Surg. 1997;114: Cetta F, Feldt RH, O Leary PW, et al. Improved early morbidity and mortality after Fontan operation: the Mayo Clinic experience, 1987 to J. Am. Coll. Cardiol. 1996;28: Stamm C, Friehs I, Mayer J, et al. Long-term results of the lateral tunnel Fontan operation. J. Thorac. Cardiovasc. Surg. 2001;121: Rychik, Jack (2016). Relentless Effects of the Fontan Paradox. Seminars in Thoracic and Cardiovascular Surgery. 19 (1): doi: /j.pcsu

69 Thank you for your attention!
Survival Rates of Children with Congenital Heart Disease continue to improve.
 DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
DOROTHY RADFORD Survival Rates of Children with Congenital Heart Disease continue to improve. 1940-20% 1960-40% 1980-70% 2010->90% Percentage of children with CHD reaching age of 18 years 1938 First Patent
Glenn Shunts Revisited
 Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Glenn Shunts Revisited What is a Super Glenn Patricia O Brien, MSN, CPNP-AC Nurse Practitioner, Pediatric Cardiology No Disclosures Single Ventricle Anatomy Glenn Shunt Cavopulmonary Anastomosis Anastomosis
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Index Note: Page numbers of article titles are in boldface type. A ACHD. See Adult congenital heart disease (ACHD) Adult congenital heart disease (ACHD), 503 512 across life span prevalence of, 504 506
Congenital heart disease: When to act and what to do?
 Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
Leading Article Congenital heart disease: When to act and what to do? Duminda Samarasinghe 1 Sri Lanka Journal of Child Health, 2010; 39: 39-43 (Key words: Congenital heart disease) Congenital heart disease
The complications of cardiac surgery:
 The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
The complications of cardiac surgery: a walk on the Dark Side? Prof Rik De Decker Red Cross Children s Hospital CME Nov/Dec 2011 http://www.cmej.org.za Why should you care? You are about to leave your
Leitlinien. Hypoplastisches Linksherzsyndrom. Hypoplastic left heart syndrome (HLHS)
") 1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
1.Title Hypoplastic left heart syndrome (HLHS) N.A. Haas, Bad Oeynhausen Ch. Jux, Giessen J. Photiadis, Berlin H.-H. Kramer, Kiel Typical forms: Mitral atresia/aortic atresia (MA/AoA) Mitral stenosis/aortic
Anatomy & Physiology
 1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
1 Anatomy & Physiology Heart is divided into four chambers, two atrias & two ventricles. Atrioventricular valves (tricuspid & mitral) separate the atria from ventricles. they open & close to control flow
Fontan Deterioration in Pediatric Cardiologist s s View. Pusan National University Hospital Hyoung Doo Lee M.D.
 Fontan Deterioration in Pediatric Cardiologist s s View Pusan National University Hospital Hyoung Doo Lee M.D. Outcomes of Fontan operation JTCS 2006:131;172-80 Mitchell ME et al Jan. 1992~Dec. 1999, 332
Fontan Deterioration in Pediatric Cardiologist s s View Pusan National University Hospital Hyoung Doo Lee M.D. Outcomes of Fontan operation JTCS 2006:131;172-80 Mitchell ME et al Jan. 1992~Dec. 1999, 332
Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery
 Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients
Page 1 Congenital Heart Disease in the Adult Presenting for Non-Cardiac Surgery Susan S. Eagle, M.D. Nashville, Tennessee Introduction: Advancement of surgical techniques and medical management patients
Congenital Heart Defects
 Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
Normal Heart Congenital Heart Defects 1. Patent Ductus Arteriosus The ductus arteriosus connects the main pulmonary artery to the aorta. In utero, it allows the blood leaving the right ventricle to bypass
5.8 Congenital Heart Disease
 5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
5.8 Congenital Heart Disease Congenital heart diseases (CHD) refer to structural or functional heart diseases, which are present at birth. Some of these lesions may be discovered later. prevalence of Chd
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
More History. Organization. Maternal Cardiac Disease: a historical perspective. The Parturient with Cardiac Disease 9/21/2012
 The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
The Parturient with Cardiac Disease Pamela Flood M.D. Professor of Anesthesia and Perioperative Care Obstetrics, Gynecology and Reproductive Sciences University of California, San Francisco Maternal Cardiac
Outline. Congenital Heart Disease. Special Considerations for Special Populations: Congenital Heart Disease
 Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Special Considerations for Special Populations: Congenital Heart Disease Valerie Bosco, FNP, EdD Alison Knauth Meadows, MD, PhD University of California San Francisco Adult Congenital Heart Program Outline
Introduction. Study Design. Background. Operative Procedure-I
 Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Risk Factors for Mortality After the Norwood Procedure Using Right Ventricle to Pulmonary Artery Shunt Ann Thorac Surg 2009;87:178 86 86 Addressor: R1 胡祐寧 2009/3/4 AM7:30 SICU 討論室 Introduction Hypoplastic
Management of a Patient after the Bidirectional Glenn
 Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
Management of a Patient after the Bidirectional Glenn Melissa B. Jones MSN, APRN, CPNP-AC CICU Nurse Practitioner Children s National Health System Washington, DC No Disclosures Objectives qbriefly describe
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Anesthetic Considerations in Adults with Congenital Heart Disease
 CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Anesthetic
CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals and Ski Holiday! CRASH Vail, Colorado 2018 Colorado Review of Anesthesia for SurgiCenters and Hospitals Anesthetic
Hybrid Stage I Palliation / Bilateral PAB
 Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Hybrid Stage I Palliation / Bilateral PAB Jeong-Jun Park Dept. of Thoracic & Cardiovascular Surgery Asan Medical Center, University of Ulsan CASE 1 week old neonate with HLHS GA 38 weeks Birth weight 3.0Kg
Intracardiac Lateral Tunnel Fontan by using Right Atrial Wall
 Intracardiac Lateral Tunnel Fontan by using Right Atrial Wall Md Zahidul Islam¹, AM Asif Rahim², Kazi Abul Hasan¹, Syed Imtiaz Ahsan¹ 1 Department of Paediatric Cardiac Surgery, National Institute of Cardiovascular
Intracardiac Lateral Tunnel Fontan by using Right Atrial Wall Md Zahidul Islam¹, AM Asif Rahim², Kazi Abul Hasan¹, Syed Imtiaz Ahsan¹ 1 Department of Paediatric Cardiac Surgery, National Institute of Cardiovascular
Hemodynamic assessment after palliative surgery
 THERAPY AND PREVENTION CONGENITAL HEART DISEASE Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome PETER LANG, M.D., AND WILLIAM I. NORWOOD, M.D., PH.D. ABSTRACT Ten patients
THERAPY AND PREVENTION CONGENITAL HEART DISEASE Hemodynamic assessment after palliative surgery for hypoplastic left heart syndrome PETER LANG, M.D., AND WILLIAM I. NORWOOD, M.D., PH.D. ABSTRACT Ten patients
Absent Pulmonary Valve Syndrome
 Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Absent Pulmonary Valve Syndrome Fact sheet on Absent Pulmonary Valve Syndrome In this condition, which has some similarities to Fallot's Tetralogy, there is a VSD with narrowing at the pulmonary valve.
Congenital Heart Disease
 Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
Congenital Heart Disease Mohammed Alghamdi, MD, FRCPC, FAAP, FACC Associate Professor and Consultant Pediatric Cardiology, Cardiac Science King Fahad Cardiac Centre King Saud University INTRODUCTION CHD
LONG TERM OUTCOMES OF PALLIATIVE CONGENITAL HEART DISEASE
 LONG TERM OUTCOMES OF PALLIATIVE CONGENITAL HEART DISEASE S Bruce Greenberg, MD, FACR, FNASCI Professor of Radiology and Pediatrics Arkansas Children's Hospital University of Arkansas for Medical Sciences
LONG TERM OUTCOMES OF PALLIATIVE CONGENITAL HEART DISEASE S Bruce Greenberg, MD, FACR, FNASCI Professor of Radiology and Pediatrics Arkansas Children's Hospital University of Arkansas for Medical Sciences
9/8/2009 < 1 1,2 3,4 5,6 7,8 9,10 11,12 13,14 15,16 17,18 > 18. Tetralogy of Fallot. Complex Congenital Heart Disease.
 Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Current Indications for Pediatric CTA S Bruce Greenberg Professor of Radiology Arkansas Children s Hospital University of Arkansas for Medical Sciences greenbergsbruce@uams.edu 45 40 35 30 25 20 15 10
Cardiac Emergencies in Infants. Michael Luceri, DO
 Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
Cardiac Emergencies in Infants Michael Luceri, DO October 7, 2017 I have no financial obligations or conflicts of interest to disclose. Objectives Understand the scope of congenital heart disease Recognize
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE
 SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
SURGICAL TREATMENT AND OUTCOME OF CONGENITAL HEART DISEASE Mr. W. Brawn Birmingham Children s Hospital. Aims of surgery The aim of surgery in congenital heart disease is to correct or palliate the heart
The evolution of the Fontan procedure for single ventricle
 Hemi-Fontan Procedure Thomas L. Spray, MD The evolution of the Fontan procedure for single ventricle cardiac malformations has included the development of several surgical modifications that appear to
Hemi-Fontan Procedure Thomas L. Spray, MD The evolution of the Fontan procedure for single ventricle cardiac malformations has included the development of several surgical modifications that appear to
Coarctation of the aorta
 T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
T H E P E D I A T R I C C A R D I A C S U R G E R Y I N Q U E S T R E P O R T Coarctation of the aorta In the normal heart, blood flows to the body through the aorta, which connects to the left ventricle
The Fontan operation. Choussat s 10 commandments revisited. Early palliative approach: systemic to pulmonary shunt or banding
 Echographic assessment in Fontan patients: sequential segmental approach Functionnaly Single Ventricle Glenn and Fontan echocardiographic assessment Xavier Iriart 1. Cavopulmonary connection 2. Branch
Echographic assessment in Fontan patients: sequential segmental approach Functionnaly Single Ventricle Glenn and Fontan echocardiographic assessment Xavier Iriart 1. Cavopulmonary connection 2. Branch
Foetal Cardiology: How to predict perinatal problems. Prof. I.Witters Prof.M.Gewillig UZ Leuven
 Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Foetal Cardiology: How to predict perinatal problems Prof. I.Witters Prof.M.Gewillig UZ Leuven Cardiopathies Incidence : 8-12 / 1000 births ( 1% ) Most frequent - Ventricle Septum Defect 20% - Atrium Septum
Perioperative Management of DORV Case
 Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
Perioperative Management of DORV Case James P. Spaeth, MD Department of Anesthesia Cincinnati Children s Hospital Medical Center University of Cincinnati Objectives: 1. Discuss considerations regarding
The Single Ventricle. Karim Rafaat, M.D.
 The Single Ventricle Karim Rafaat, M.D. The title single ventricle includes those lesions designated as both HLHS HRHS HLHS is far more common, and the strategy for palliation of both lesions similar,
The Single Ventricle Karim Rafaat, M.D. The title single ventricle includes those lesions designated as both HLHS HRHS HLHS is far more common, and the strategy for palliation of both lesions similar,
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions
 Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
Appendix A.1: Tier 1 Surgical Procedure Terms and Definitions Tier 1 surgeries AV Canal Atrioventricular Septal Repair, Complete Repair of complete AV canal (AVSD) using one- or two-patch or other technique,
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
M/3, cc-tga, PS, BCPC(+) Double Switch Operation
 Double Switch Operation") 2005 < Pros & Cons > M/3, cc-tga, PS, BCPC(+) Double Switch Operation Congenitally corrected TGA Atrio-Ventricular & Ventriculo-Arterial discordance Physiologically corrected circulation with the morphologic
2005 < Pros & Cons > M/3, cc-tga, PS, BCPC(+) Double Switch Operation Congenitally corrected TGA Atrio-Ventricular & Ventriculo-Arterial discordance Physiologically corrected circulation with the morphologic
veins. This mixing of oxygenated and deoxygenated blood in the functionally single atrium means that the patient will continue to be desaturated, with
 Sandeep Nayak MBBS MD FRCA PD Booker MBBS MD FRCA Key points Increasing numbers of patients with a Fontan circulation are reaching adulthood and requiring anaesthesia for non-cardiac surgery Understanding
Sandeep Nayak MBBS MD FRCA PD Booker MBBS MD FRCA Key points Increasing numbers of patients with a Fontan circulation are reaching adulthood and requiring anaesthesia for non-cardiac surgery Understanding
Glenn and Fontan Caths:
 Glenn and Fontan Caths: Pre-operative evaluation and Trouble-shooting Cavo-Pulmonary Shunts Daniel H. Gruenstein, M.D. Director, Pediatric Interventional Cardiology University of Minnesota Children s Hospital,
Glenn and Fontan Caths: Pre-operative evaluation and Trouble-shooting Cavo-Pulmonary Shunts Daniel H. Gruenstein, M.D. Director, Pediatric Interventional Cardiology University of Minnesota Children s Hospital,
Adults with Congenital Heart Disease. Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP
 Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
Adults with Congenital Heart Disease Michael E. McConnell MD, Wendy Book MD Teresa Lyle RN NNP Outline History of CHD Statistics Specific lesions (TOF, TGA, Single ventricle) Erythrocytosis Pregnancy History
3/14/2011 MANAGEMENT OF NEWBORNS CARDIAC INTENSIVE CARE CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 WITH HEART DEFECTS
 CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
CONFERENCE FOR HEALTH PROFESSIONALS IRVINE, CA. MARCH 7, 2011 MANAGEMENT OF NEWBORNS WITH HEART DEFECTS A NTHONY C. CHANG, MD, MBA, MPH M E D I C AL D I RE C T OR, HEART I N S T I T U T E C H I LDRE N
The Challenging Pediatric Cardiac Patient. Edmund Jooste
 The Challenging Pediatric Cardiac Patient Edmund Jooste A 5 -year old female with hypoplastic left heart syndrome s/p the Fontan procedure presents for laparoscopic appendectomy for acute appendicitis.
The Challenging Pediatric Cardiac Patient Edmund Jooste A 5 -year old female with hypoplastic left heart syndrome s/p the Fontan procedure presents for laparoscopic appendectomy for acute appendicitis.
What is the Definition of Small Systemic Ventricle. Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University
 What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
What is the Definition of Small Systemic Ventricle Hong Ryang Kil, MD Department of Pediatrics, College of Medicine, Chungnam National University Contents Introduction Aortic valve stenosis Aortic coarctation
CONGENITAL HEART DISEASE (CHD)
") CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
CONGENITAL HEART DISEASE (CHD) DEFINITION It is the result of a structural or functional abnormality of the cardiovascular system at birth GENERAL FEATURES OF CHD Structural defects due to specific disturbance
Research Presentation June 23, Nimish Muni Resident Internal Medicine
 Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Children with Single Ventricle Physiology: The Possibilities
 Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Children with Single Ventricle Physiology: The Possibilities William I. Douglas, M.D. Pediatric Cardiovascular Surgery Children s Memorial Hermann Hospital The University of Texas Health Science Center
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!!
 Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
Clinicians and Facilities: RESOURCES WHEN CARING FOR WOMEN WITH ADULT CONGENITAL HEART DISEASE OR OTHER FORMS OF CARDIOVASCULAR DISEASE!! Abha'Khandelwal,'MD,'MS' 'Stanford'University'School'of'Medicine'
The Fontan circulation. Folkert Meijboom
 The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome(s), anticoagulant therapy in, 706, 707 antiplatelet therapy in, 702 ß-blockers in, 703 cardiac biomarkers in,
Common Defects With Expected Adult Survival:
 Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Common Defects With Expected Adult Survival: Bicuspid aortic valve :Acyanotic Mitral valve prolapse Coarctation of aorta Pulmonary valve stenosis Atrial septal defect Patent ductus arteriosus (V.S.D.)
Born Blue. Anesthesia and CHD. Kristine Faust, CRNA, MS, MBA, DNAP
 Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Born Blue Anesthesia and CHD Kristine Faust, CRNA, MS, MBA, DNAP Disclosures Disclosures None to Report Objectives Review all congenital defects in which the patient is blue Describe physiology of the
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS Pediatric Cardiology
 Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
Cardiovascular Pathophysiology: Right to Left Shunts aka Cyanotic Lesions Ismee A. Williams, MD, MS iib6@columbia.edu Pediatric Cardiology Learning Objectives To discuss the hemodynamic significance of
MEDICAL MANAGEMENT WITH CAVEATS 1. In one study of 50 CHARGE patients with CHD, 75% required surgery. 2. Children with CHARGE may be resistant to chlo
 CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
CARDIOLOGY IN CHARGE SYNDROME: FOR THE PHYSICIAN Angela E. Lin, M.D. Teratology Program/Active Malformation Surveillance, Brigham and Women's Hospital, Old PBBH-B501, 75 Francis St., Boston, MA 02115 alin@partners.org
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment
 Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Hypoplastic Left Heart Syndrome: Echocardiographic Assessment Craig E Fleishman, MD, FACC, FASE Director, Non-invasive Cardiac Imaging The Hear Center at Arnold Palmer Hospital for Children, Orlando SCAI
Mechanical Support in the Failing Fontan-Kreutzer
 Mechanical Support in the Failing Fontan-Kreutzer Stephanie Fuller MD, MS Thomas L. Spray Endowed Chair in Congenital Heart Surgery Associate Professor, The Perelman School of Medicine at the University
Mechanical Support in the Failing Fontan-Kreutzer Stephanie Fuller MD, MS Thomas L. Spray Endowed Chair in Congenital Heart Surgery Associate Professor, The Perelman School of Medicine at the University
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
The Chest X-ray for Cardiologists
 Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Mayo Clinic & British Cardiovascular Society at the Royal College of Physicians, London : 21-23-October 2013 Cases-Controversies-Updates 2013 The Chest X-ray for Cardiologists Michael Rubens Royal Brompton
Heart and Lungs. LUNG Coronal section demonstrates relationship of pulmonary parenchyma to heart and chest wall.
 Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Heart and Lungs Normal Sonographic Anatomy THORAX Axial and coronal sections demonstrate integrity of thorax, fetal breathing movements, and overall size and shape. LUNG Coronal section demonstrates relationship
Total Cavopulmonary Connections in Children With a Previous Norwood Procedure
 Total Cavopulmonary Connections in Children With a Previous Norwood Procedure Anthony Azakie, MD, Brian W. McCrindle, MD, FRCP(C), Lee N. Benson, MD, FRCP(C), Glen S. Van Arsdell, MD, Jennifer L. Russell,
Total Cavopulmonary Connections in Children With a Previous Norwood Procedure Anthony Azakie, MD, Brian W. McCrindle, MD, FRCP(C), Lee N. Benson, MD, FRCP(C), Glen S. Van Arsdell, MD, Jennifer L. Russell,
Cardiac Catheterization Cases Primary Cardiac Diagnoses Facility 12 month period from to PRIMARY DIAGNOSES (one per patient)
") PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
PRIMARY DIAGNOSES (one per patient) Septal Defects ASD (Atrial Septal Defect) PFO (Patent Foramen Ovale) ASD, Secundum ASD, Sinus venosus ASD, Coronary sinus ASD, Common atrium (single atrium) VSD (Ventricular
CARDIOVASCULAR SURGERY
 Volume 107, Number 4 April 1994 The Journal of THORACIC AND CARDIOVASCULAR SURGERY Cardiac and Pulmonary Transplantation Risk factors for graft failure associated with pulmonary hypertension after pediatric
Volume 107, Number 4 April 1994 The Journal of THORACIC AND CARDIOVASCULAR SURGERY Cardiac and Pulmonary Transplantation Risk factors for graft failure associated with pulmonary hypertension after pediatric
Early outcome after Fontan operation for univentricular
 Thrombus Formation After the Fontan Operation Patrick D. Coon, RDCS, RCVT, Jack Rychik, MD, Rita T. Novello, RDCS, Pamela S. Ro, MD, J. William Gaynor, MD, and Thomas L. Spray, MD Cardiac Center at the
Thrombus Formation After the Fontan Operation Patrick D. Coon, RDCS, RCVT, Jack Rychik, MD, Rita T. Novello, RDCS, Pamela S. Ro, MD, J. William Gaynor, MD, and Thomas L. Spray, MD Cardiac Center at the
Adult Congenital Heart Disease: A Growing Problem. Dr. Gary Webb Cincinnati Children s Hospital Heart Institute
 Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
Adult Congenital Heart Disease: A Growing Problem Dr. Gary Webb Cincinnati Children s Hospital Heart Institute ACHD Resources in Ohio ACHAHEART.ORG Situations When We Might Help When you don t know a
PEDIATRIC CARDIOLOGY. Philadelphia, Pennsylvania
 JACC Vol. 17, No.5 April 1991:1143-9 1143 PEDIATRIC CARDIOLOGY Hypoplastic Left Heart Syndrome: Hemodynamic and Angiographic Assessment After Initial Reconstructive Surgery and Relevance to Modified Fontan
JACC Vol. 17, No.5 April 1991:1143-9 1143 PEDIATRIC CARDIOLOGY Hypoplastic Left Heart Syndrome: Hemodynamic and Angiographic Assessment After Initial Reconstructive Surgery and Relevance to Modified Fontan
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death
 Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Congenital Heart Disease Certification Examination Blueprint
 Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Adult Congenital Heart Disease Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
A teenager with tetralogy of fallot becomes a soccer player
 ISSN 1507-6164 DOI: 10.12659/AJCR.889440 Received: 2013.06.06 Accepted: 2013.07.10 Published: 2013.09.23 A teenager with tetralogy of fallot becomes a soccer player Authors Contribution: Study Design A
ISSN 1507-6164 DOI: 10.12659/AJCR.889440 Received: 2013.06.06 Accepted: 2013.07.10 Published: 2013.09.23 A teenager with tetralogy of fallot becomes a soccer player Authors Contribution: Study Design A
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
T who has survived first-stage palliative surgical management
 Intermediate Procedures After First-Stage Norwood Operation Facilitate Subsequent Repair Richard A. Jonas, MD Department of Cardiac Surgery, Children s Hospital, Boston, Massachusetts Actuarial analysis
Intermediate Procedures After First-Stage Norwood Operation Facilitate Subsequent Repair Richard A. Jonas, MD Department of Cardiac Surgery, Children s Hospital, Boston, Massachusetts Actuarial analysis
How pregnancy impacts adult cyanotic congenital heart disease
 How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
How pregnancy impacts adult cyanotic congenital heart disease Magalie Ladouceur Adult Congenital Heart Disease Unit, Hôpital Européen Georges Pompidou, Centre de reference des Malformations Cardiaques
Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016
 1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
1 Adult Congenital Heart Disease: What All Echocardiographers Should Know Sharon L. Roble, MD, FACC Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Why should all echocardiographers
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
How Does Imaging Inform Fetal Cardiovascular Treatment?
 How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
How Does Imaging Inform Fetal Cardiovascular Treatment? Edgar Jaeggi, MD Head, Fetal Cardiac Program Labatt Family Heart Center Department of Pediatrics The Hospital for Sick Children University of Toronto
TGA atrial vs arterial switch what do we need to look for and how to react
 TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
AORTIC COARCTATION. Synonyms: - Coarctation of the aorta
 AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
AORTIC COARCTATION Synonyms: - Coarctation of the aorta Definition: Aortic coarctation is a congenital narrowing of the aorta, usually located after the left subclavian artery, near the ductus or the ligamentum
Use of the Total Artificial Heart in the Failing Fontan Circulation J William Gaynor, M.D.
 Use of the Total Artificial Heart in the Failing Fontan Circulation J William Gaynor, M.D. Daniel M. Tabas Endowed Chair in Pediatric Cardiothoracic Surgery at The Children s Hospital of Philadelphia The
Use of the Total Artificial Heart in the Failing Fontan Circulation J William Gaynor, M.D. Daniel M. Tabas Endowed Chair in Pediatric Cardiothoracic Surgery at The Children s Hospital of Philadelphia The
CYANOTIC CONGENITAL HEART DISEASES. PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU
 CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CYANOTIC CONGENITAL HEART DISEASES PRESENTER: DR. Myra M. Koech Pediatric cardiologist MTRH/MU DEFINITION Congenital heart diseases are defined as structural and functional problems of the heart that are
CASE DISCUSSION. Dr JAYASREE VEERABOINA 2nd yr PG MS OBG
 CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
CASE DISCUSSION Dr JAYASREE VEERABOINA 2nd yr PG MS OBG Normal Cardiovascular changes in Pregnancy CARDIAC OUTPUT 5 th wk -- starts 12 wks -- 30-35% 30-32 wks -- 40% During labour -- 50% After delivery
Management of Heart Failure in Adult with Congenital Heart Disease
 Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
Management of Heart Failure in Adult with Congenital Heart Disease Ahmed Krimly Interventional and ACHD consultant King Faisal Cardiac Center National Guard Jeddah Background 0.4% of adults have some form
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Extracardiac vs Intra-atrial Lateral Tunnel Fontan: Extracardiac is Better. No it s not: (They both have problems)
") Extracardiac vs Intra-atrial Lateral Tunnel Fontan: Extracardiac is Better No it s not: (They both have problems) Why is it difficult to analyze outcomes after the Fontan procedure? Wide range of patient
Extracardiac vs Intra-atrial Lateral Tunnel Fontan: Extracardiac is Better No it s not: (They both have problems) Why is it difficult to analyze outcomes after the Fontan procedure? Wide range of patient
DIAGNOSIS, MANAGEMENT AND OUTCOME OF HEART DISEASE IN SUDANESE PATIENTS
 434 E AST AFRICAN MEDICAL JOURNAL September 2007 East African Medical Journal Vol. 84 No. 9 September 2007 DIAGNOSIS, MANAGEMENT AND OUTCOME OF CONGENITAL HEART DISEASE IN SUDANESE PATIENTS K.M.A. Sulafa,
434 E AST AFRICAN MEDICAL JOURNAL September 2007 East African Medical Journal Vol. 84 No. 9 September 2007 DIAGNOSIS, MANAGEMENT AND OUTCOME OF CONGENITAL HEART DISEASE IN SUDANESE PATIENTS K.M.A. Sulafa,
When to implant an ICD in systemic right ventricle?
 When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
When to implant an ICD in systemic right ventricle? Département de rythmologie et de stimulation cardiaque Nicolas Combes n.combes@clinique-pasteur.com Pôle de cardiologie pédiatrique et congénitale Risk
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
cctga patients need lifelong follow-up in an age-appropriate facility with expertise in
 ONLINE SUPPLEMENT ONLY: ISSUES IN THE ADULT WITH CCTGA General cctga patients need lifelong follow-up in an age-appropriate facility with expertise in congenital heart disease care at annual intervals.
ONLINE SUPPLEMENT ONLY: ISSUES IN THE ADULT WITH CCTGA General cctga patients need lifelong follow-up in an age-appropriate facility with expertise in congenital heart disease care at annual intervals.
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Multimodality Imaging of Septal Defects
 Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide
Multimodality Imaging of Septal Defects Ohio-ACC 2018 Annual Meeting October 27, 2018 Kan N. Hor, MD Director, Cardiac Magnetic Resonance Imaging Associate Professor of Pediatrics The Heart Center, Nationwide
Cardiac CT in Infants with Congenital heart disease Sunrise Session. LaDonna Malone, MD May 17, 2018
 Cardiac CT in Infants with Congenital heart disease Sunrise Session LaDonna Malone, MD May 17, 2018 None Disclosures Objectives Describe cardiac CT techniques used in infants with congenital heart disease.
Cardiac CT in Infants with Congenital heart disease Sunrise Session LaDonna Malone, MD May 17, 2018 None Disclosures Objectives Describe cardiac CT techniques used in infants with congenital heart disease.
Debate in Management of native COA; Balloon Versus Surgery
 Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Debate in Management of native COA; Balloon Versus Surgery Dr. Amira Esmat, El Tantawy, MD Professor of Pediatrics Consultant Pediatric Cardiac Interventionist Faculty of Medicine Cairo University 23/2/2017
Patent ductus arteriosus PDA
 Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Patent ductus arteriosus PDA Is connecting between the aortic end just distal to the origin of the LT sub clavian artery& the pulmonary artery at its bifurcation. Female/male ratio is 2:1 and it is more
Cardiac disease in pre pr gnancy
 IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
IN THE NAME OF GOD Cardiac disease in pregn nancy MITRAL STENOSIS 33 y/o G3L2(2c/s) GA 34 + 5 CC: LP & dyspnea PMHx: MS sinse 4 yrs ago due to Rheumatism PSHx: 2c/s DHx: metoral 50 mg q6h/ ASA/ Enoxaparin
The Double Switch Using Bidirectional Glenn and Hemi-Mustard. Frank Hanley
 The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
The Double Switch Using Bidirectional Glenn and Hemi-Mustard Frank Hanley No relationships to disclose CCTGA Interesting Points for Discussion What to do when. associated defects must be addressed surgically:
Adult Congenital Heart Disease: The New Reality. Disclosures
 Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Adult Congenital Heart Disease: The New Reality Kathryn Rouine-Rapp, MD Professor of Anesthesia Disclosures I have nothing to disclose 1 Outline Historic perspective Our reality Common lesions Guidelines
Impact of the Evolution of the Fontan Operation on Early and Late Mortality: A Single-Center Experience of 405 Patients Over 3 Decades
 Impact of the Evolution of the Fontan Operation on Early and Late Mortality: A Single-Center Experience of 405 Patients Over 3 Decades Hideo Ohuchi, MD, PhD, Koji Kagisaki, MD, Aya Miyazaki, MD, Masataka
Impact of the Evolution of the Fontan Operation on Early and Late Mortality: A Single-Center Experience of 405 Patients Over 3 Decades Hideo Ohuchi, MD, PhD, Koji Kagisaki, MD, Aya Miyazaki, MD, Masataka