Ischemic stroke: management, prevention and follow up. Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
|
|
|
- Debra Lewis
- 6 years ago
- Views:
Transcription
1 Ischemic stroke: management, prevention and follow up Amit Kansara MD Providence Stroke Center Providence Brain and Spine Institute
2 Quotes Benjamin Franklin: All would live long, but none would be old. Abraham Lincoln: And in the end, it s not the years in your life that count. It s the life in your years.
3 Ischemic stroke: management and prevention Epidemiology Acute management Prevention and follow up
4 Epidemiology Lifetime risk for incident stroke at 65 years has decreased to % from 19.5% in men % from 18% in women Number of incident strokes is expected to more than double by 2050 Majority in aged 75 years Cost increase - $71.6 billion to $184.1 billion
5 Prevalence of stroke by age and sex

6 Mortality in 1 year after the stroke Recurrent stroke within 5 years of first stroke
7 Disabilities after stroke in more >65 years old 50% hemiparesis 30% unable to walk without some assistance 46% cognitive deficits 35% depressive symptoms 19% aphasia 26% dependent in activities of daily living 26% institutionalized in a nursing home

8 The most FAQs to stroke neurologists What is the appropriate anti platelet management when my patient has a stroke or TIA on aspirin? What is the appropriate diagnostic work up for a patient admitted with a TIA or stroke? MRI or CT? Carotid ultrasound, CTA or MRA? TTE or TEE? When do I order a hypercoaguable panel? What do I do if echocardiography shows a patent foramen ovale (PFO)? How long should I monitor a patient to assess for paroxysmal atrial fibrillation (PAF)?
9 The most FAQs to stroke neurologists (cont). If patient has afib and an acute stroke, how soon do I start anticoagulation? Are the new anticoagulants superior to warfarin for stroke prevention with afib? What is the recommendation for blood pressure management in the hours and days after stroke? Carotid stenosis, symptomatic vs asymtomatic, when to treat?

10 Ischemic stroke etiologies The most frequent sites of arterial and cardiac abnormalities causing ischemic stroke. Chest. 2001;119:300S320S.)
11 Stroke Subtypes and Incidence Other 5% Hemorrhagic stroke 15% Ischemic stroke 85% Cryptogenic 30% Cardiogenic embolism 20% Atherosclerotic cerebrovascular disease 20% Small vessel disease lacunes 25% Albers et al. Chest 2004; 126 (3 Suppl): 438S 512S.
12 Acute stroke management- Intravenous thrombolytic IV tpa up to 3 hours (NINDS trial) IV tpa up to 4.5 hours (ECASS III trial) - Age < 80 - Not on anti coagulation - NIHSS < 25 - No h/o DM and stroke combined
13 Intra arterial treatment and mechanical thrombectomy IA therapy 6 hours (Class I; level of evidence B) Various FDA approved devices; SOLITAIRE FR, MERCI, PENUMBRA, TREVO Multiple case series of positive outcome Class IIa; level of evidence B MR CLEAN, SWIFT PRIME, ESCAPE and EXTEND IA,
14 Case 75 yr female came with acute left side of weakness, NIHSS 18 Stroke team paged 7 pm Confusion about time of onset 11 am vs 3 pm More detailed history- time of onset 3 pm Out of tpa window
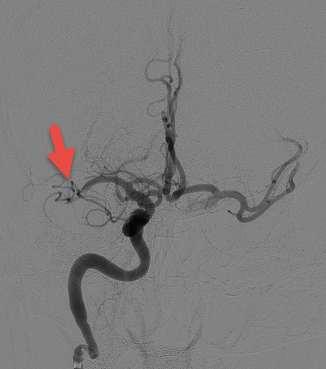
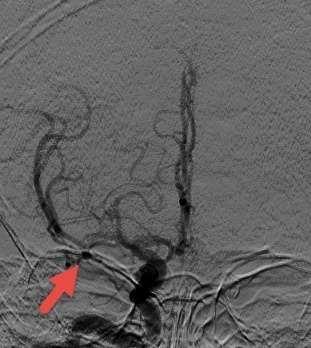
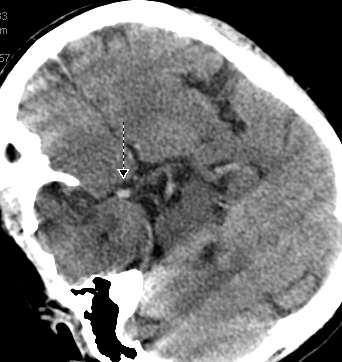
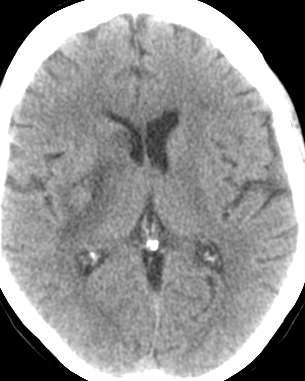
15
16 Follow up at 1, 4 months Full recovery in 4 months Patient found to have a fib; started on newer anticoagulation Able to drive, no need for PT/OT after 2 months, no cognitive deficits
17
18 Atrial Fibrillation and stroke Prevalence 5% of people over age 65 10% of people over age 80 50% of all patients with a fib are over age 80 Detection with tele monitoring PAF detection over average hosp LOS: ~3% 48 holter 2-3% 30 day monitor % 6 month monitor 22% 12 month 25% 36 months 30%
19 75 Y/F with HTN, HPL, right sided weakness and mod left atrial enlargement. Telemetry neg during 2 days hospitalization, no large vessel occlusion or carotid stenosis Start anticoagulation Aspirin and no further work up 48 hour holter monitoring on discharge 30 days or longer holter monitoring

20 When to suspect cardioembolic stroke? Peripheral cortical wedge shaped infarct or multi focal infarcts Enlarged left atrium on TTE No significant stenosis/irregular ulcerated plaques in carotid arteries or in intracranial circulation

21 What are we worried about? Risk of fall Risk of ICH Other major bleeds Which anti coagulation to choose When to restart after ICH What to do if patient has MCI or dementia
22 Stroke and bleeding risk stratification with A fib
23 Case 79 year male with new a fib, h/o of HTN, MI (score 3) But he was alcoholic with altered renal function and with uncontrolled HTN (HAS BLED 5) Not started on anticoagulation
24 After 6 months, new ischemic stroke Now risk score is 5 Discussed better control of BP and alcohol abstinence Goal to bring HAS BLED score from 5 to 3 Started on Warfarin
25 Bleeding risk with anticoagulation ICH Debigatran 0.3%/year to warfarin 0.74%/year Rivaroxaban 0.5%/year to warfarin 0.7%/year Apixaban 0.33%/year to warfarin 0.8%/year GI bleed Debigatran 1.5%/year to warfarin 1.02%/year Rivaroxaban 2.8%/year to warfarin 2.3%/year Apixaban 0.76%/year to warfarin 0.86%/year Summary of evidence-based guideline update: Prevention of stroke in nonvalvular atrial fibrillation. Neurology February 25, 2014 vol. 82 no
26 Newer anticoagulation reversal agent FDA approved Praxbind under accelerated approval program in October, 2015 In patient requiring emergent surgery who received Praxbind, 89% patients had decrease in blood concentration of Pradaxa within 4 hours In 283 healthy volunteers, immediate decrease in Pradaxa concetration that lasted for 24 hours Need to see practical effectiveness
27 When to start anticoagulation after ischemic stroke Standard answer within 2 weeks Would favor starting earlier if patient has small embolic infarct Would favor at 2 weeks if large hemispheric infarct where risk of hemorrhagic transformation is high In some cases with large infarct and petechial hemorrhages, CT scan head is advised before starting anticoagulation
28 Long term cardiac monitoring for suspected cardioembolic stroke EMBRACE trial- 15% AF detection at 30 days CRYSTAL AF- 13% AF detection at 1 year Gladstone DJ et al. N Engl J Med 2014;370: Sanna T et al. N Engl J Med 2014;370:
29 75 Y/F with HTN, HPL, right sided weakness and mod left atrial enlargement. Telemetry neg during 2 days hospitalization, no large vessel occlusion or carotid stenosis Start anticoagulation Aspirin and no further work up 48 hour cardiac monitoring on discharge 30 days or longer cardiac monitoring
30 Risk of falls and bleeding on anti coagulation Not many studies Published study in 2012 Prospective, 515 patients, 308 patients (59%) at high risk of falls Follow up for 12 months 35 patients with first major bleed No difference between high risk and law risk group What AAN says Clinicians might offer anticoagulation in patients with mild dementia and occasional falls. Risk benefit ratio is uncertain in patients with frequent falls and mod to severe dementia. Summary of evidence-based guideline update: Prevention of stroke in nonvalvular atrial fibrillation. Neurology February 25, 2014 vol. 82 no Am J Med Aug;125(8): doi: /j.amjmed

31 Amyloid angiopathy and microbleeds Anticoagulation contraindicated Increase the chances of microbleeds and large lobar hemorrhage Anti platelets would be a safer option particularly with h/o of ischemic stroke, CAD and stent placement In case of recurrent microbleeds, even anti platelets are not a safe alternative Role of procedure/device?
32 Cardiac procedure/devices for patients with contraindication to anticoagulation Future promise- Left atrial appendage closure devices WATCHMAN device LARIAT closure procedure Not FDA approved yet Investigational use and research trial use only
33 Anticoagulation after ICH Individualized to each patient High risk of recurrent ICH (lobar ICH or probable amyloid angiopathy) antiplatelets may be considered Risk of ICH - 9.3% in patients with microbleeds compared with 1.3% without microbleeds Optimal timing to restart uncertain Wait time to start 4 weeks or longer

34 Case 82 years with h/o of HTN, a fib, lupus anticoagulant disorder, h/o of bladder and prostate cancer Large rt cerebellar hemorrhage. He received FEIBA And FFP to reverse his INR. Managed with osmolar therapy for raised ICP. Fortunately, he did not require surgery for large ICH. Partial code/no intubation/no CPR/no life saving surgery F/up at 6 months- imbalance, mild cognitive dysfunction, on aspirin
35 Antiplatelet agents after ischemic stroke/tia 65 Y/M with uncontrolled HTN, HPL and DM who is on ASA on 81 mg and with new mild rt sided symptoms Increase ASA to 325 mg daily Change to Clopidogrel Change to Aggrenox Keep ASA 81 mg, add high intensity statin, intensive control of DM, HTN, diet and lifestyle modifications
36 Antiplatelet agents after ischemic stroke/tia Aspirin, Clopidogrel, Aspirin- Dypiridamole combination, Ticlopidine (rarely used) Aspirin or Aggrenox should be initiated for secondary stroke prevention Clopidogrel is a reasonable alternative No clear data to show effectiveness of increasing dose of aspirin after having stroke on low dose aspirin
37 Antiplatelet agents after ischemic stroke/tia Combination of Aspirin and Clopidogrel might be considered for 21 days after minor ischemic stroke Our practice is to look for optimal control of stroke risk factors (HTN, HPL, DM, sleep apnea, obesity, physical activity etc.) before making decision on changing anti platelet agent No difference between Clopidogrel and combination of Aspirin- Dypiridamole (CHARISMA trial)
38 Antiplatelet agents after ischemic stroke/tia CHANCE trial- Combination of Aspirin and Clopidogrel for 21 days initiated within 24 hours may be more effective in secondary stroke prevention SPS 3 and MATCH trial- Combination of aspirin and Clopidogrel for longer duration like 2-3 years initiated within 6 months of lacunar stroke increases the risk of ICH and GI bleed without any significant additional benefit POINT trial (On going)- Aspirin vs aspirin plus Plavix for 90 days in patients with high risk TIA or minor ischemic stroke
39 Dual antiplatelet agents after ischemic stroke/tia SAMMPRIS trial -For symptomatic intracranial stenosis (>70%), combination of Aspirin plus Clopidogrel for 90 days along with aggressive risk factors modification is more effective and less harmful than stenting Caveat- there was no single anti platelet agent arm in that trial

40 Antiplatelet agents after ischemic stroke/tia 65 Y/M with uncontrolled HTN, HPL and DM who is on ASA on 81 mg and with new mild rt sided symptoms Increase ASA to 325 mg daily Change to Clopidogrel Change to Aggrenox ASA 81 mg, add high intensity statin, intensive control of DM, HTN, diet and lifestyle modifications
41 Prevention of stroke in carotid stenosis Symptomatic and asymptomatic Stroke/TIA within last 6 months, carotid stenosis is defined as symptomatic Optimum medical management CEA CAS
42 Prevention of stroke in carotid stenosis 74 year old male with CAD, HTN and HPL with sudden dizziness, near syncope episode. Work up showed 50-69% narrowing of rt carotid artery, CTA shows 65-70%% stenosis with calcified regular plaque. Patient is on Plavix, 20 mg of simvastatin and partially controlled blood pressure. CAS CEA Continue same management Change to high intensity statin, better control of HTN, exercise, diet and follow up carotid duplex
43 Management of symptomatic carotid stenosis CEA for ipsilateral severe (70% 99%) carotid artery stenosis if the perioperative morbidity and mortality risk is estimated to be <6% Proven in multiple trials, NASCET, ECST and VACS Standard of care Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: Stroke. 2014;45:
44 Management of symptomatic carotid stenosis For 50-69% stenosis, CEA is recommended depending on patient-specific factors, such as age, sex, and co morbidities For > 70% stenosis, CAS is a reasonable alternative to CEA EC-IC bypass is not recommended Should be done within 2 weeks of TIA/stroke
45 Management of symptomatic carotid stenosis Favoring CEA (usually first line) > 70 years? Medical co morbidities Favoring CAS Radiation induced stenosis Non favorable anatomy like high cervical bifurcation Contra lateral carotid occlusion
46 Management of asymptomatic carotid stenosis 3% per year stroke risk with 80-99% (previous trials) 5% per year with 90-99% (previous trials) Recent data shows stroke risk of 0.5% to 1% per year when carotid stenosis > 50%. A recent meta analysis showed decrease stroke rates 2.83% before 2000 to 1.13%per year after Management of Asymptomatic Internal Carotid Artery Stenosis:JAMA. 2013;310(15):
47 Management of asymptomatic carotid stenosis: Pearls Benefit of CEA in women is not clear Benefit in men > 75 years is not clear Medical management is a first line of management in mod degree stenosis Carotid revascularization may be indicated in selected group of high risk/high degree stenosis CREST-2 trial will have medical therapy arm along with stenting and CEA
48 Management of asymptomatic carotid stenosis: Pearls Ill-defined dizziness generalized weakness syncope or near-syncope blurry vision, or transient positive visual phenomena Life expectancy of less than 5 years are unlikely to benefit from the modest risk reduction afforded by surgery
49 Management of asymptomatic carotid stenosis: Pearls High risk group among asymptomatic patients Carotid Revascularization and Medical Management for Asymptomatic Carotid Stenosis Trial (CREST-2) Embolic signals on TCD Stenosis progression rate Plaque morphology Serum biomarker Cerebrovascular reserve Intensive medical management vs carotid revascularization in asymptomatic patient with > 70% carotid stenosis Medical management vs stenting Medical management vs CEA
50 Prevention of stroke in carotid stenosis 74 year old male with CAD, HTN and HPL with sudden dizziness, near syncope episode. Work up showed 50-69% narrowing of rt carotid artery, CTA shows 65-70%% stenosis with calcified regular plaque. Patient is on Plavix, 20 mg of simvastatin and partially controlled blood pressure. CAS CEA Continue same management Change to high intensity statin, better control of HTN, exercise, diet and follow up carotid duplex
51 PFO and stroke RESPECT trial In the primary intention-to-treat analysis, there was no significant benefit associated with closure of a patent foramen ovale in adults who had had a cryptogenic ischemic stroke. However, closure was superior to medical therapy alone in the prespecified per-protocol and astreated analyses, with a low rate of associated risks.
52 PFO and stroke CLOSURE trial In patients with cryptogenic stroke or TIA who had a patent foramen ovale, closure with a device did not offer a greater benefit than medical therapy alone for the prevention of recurrent stroke or TIA.
53 PFO and stroke In patient with cryptogenic stroke and PFO, closure of PFO is not recommended routinely In the presence of PFO and venous source of embolism, anticoagulation is indicated If anticoagulation is not possible then IVC filter should be considered In patient with PFO and recurrent venous thrombosis, PFO closure can be considered depending on the risk of recurrence
54 Statin therapy and risk of ICH Conflicting reports about statin use and risk of ICH SPARCL trial reported an increased risk of ICH among patients with high dose of atorvastatin and with h/o ICH Might have resulted from high crossover rates in the SPARCL trial itself Likely that many clinicians have been wary of prescribing statins to patients with ICH
55 Statin therapy and risk of ICH A meta analysis of 31 RCT More than patients in statin and non statin arm No increased risk of ICH in statin arm Decrease in stroke rate and all cause mortality rate in statin arm
56 JAMA Neurol. doi: /jamaneurol Published online September 22, 2014.


57 Statin therapy and risk of ICH
58 Statin therapy and risk of ICH Use caution In patients with unexplained lobar bleeds When high degree suspicion of amyloid angiopathy MRI shows cortical micro bleeds Statin is ok if No micro bleeds on MRI s/o of probable amyloid angiopathy ICH is secondary to hypertensive bleed High risk of recurrent infarcts and small vessel disease
59 Arterial dissection and stroke prevention Antiplatelet or anticoagulation CADISS trial, published in Lancet Neurology 250 patients, carotid and VA dissection 126 received antiplatelet, 124 anticoagulation 4 patient with stroke or death over follow up- 2% No difference between 2 group Antiplatelet is being used more Anticoagulation when burden of overlying thrombus and risk of thromboembolism is high (subjective- no clear criteria to define) Anticoagulation when vessel diameter is compromised significantly with long segment dissections
60 Post stroke depression Prevalence after stroke 29 percent (95% CI percent). * Major predictors of depression - disability - depression pre-stroke - cognitive impairment - stroke severity - anxiety. In a study with mean age of 74, at 1 year post stroke - 51% impairment of ADL - 33% clinically significant levels of depression. ** Depression screening is important in post stroke clinic follow up. *Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis:br J Psychiatry Jan;202:14-21 **Predictors of depression at one year post stroke in older adults: Brain Impairment. 2013; 14:
61 Other things to control for secondary stroke prevention Blood pressure goal: Usually less than 140/90; lacunar- Less than 130/85; Will SPRINT trial result change these goals? Good glycemic control with goal of HBA1C less than 7 Screen for sleep apnea Screen for metabolic syndrome Diet and exercise
62 Primary prevention of stroke (AHA/ASA Oct 28, 2014, published guideline) BP goal less than 140/90 Home monitoring of blood pressure Migraine with aura- avoid estrogen containing contraception, smoking cessation NOAC reasonable option with high risk AF ASCVD risk calculator reasonable to use but with limitations Mediterranean diet with nuts, DASH style diet
63 Complex cases which require follow up Cryptogenic stroke Recurrent strokes Stroke due to hypercoagulopathy Arterial dissection A fib and high risk of bleed Venous sinus thrombosis Stroke in young Complex carotid stenosis

64
, East Campus")
65 Thank you Providence Stroke Center West Campus (PSVMC), East Campus (PPMC)
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Cryptogenic Stroke: A logical approach to a common clinical problem
 Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Cryptogenic Stroke: A logical approach to a common clinical problem Alphonse M. Ambrosia, DO, FACC Interventional Cardiologist CardioVascular Associates of Mesa Mesa, Arizona Speakers Bureau Boston Scientific
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Asymptomatic Carotid Stenosis To Do or Not To Do
 Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
Asymptomatic Carotid Stenosis To Do or Not To Do October 22, 2016 Neurosciences: Updates and Controversies Andrew C. MacDougall, MD Advocate Medical Group Advocate Lutheran General Hospital Principle
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO
 La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
La gestione dell ictus ischemico o emorragico nel paziente sotto NAO Antonio Carolei e Cindy Tiseo Clinica Neurologica e Stroke Unit Avezzano - Sulmona Università degli Studi dell Aquila Abano Terme, 10
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE
 Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Thrombolysis-WAKE UP Intra-arterial interventions DEFUSE 3 Haemorrhagic Stroke - TICH 2 Secondary Prevention CROMIS 2 Secondary Prevention NAVIGATE ESUS Progression of haematoma Anticoagulation Large ICH
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Stroke Case Studies. Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow
 Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Stroke Case Studies Dr Stuti Joshi Neurology Advanced Trainee Telestroke fellow Case 1 64 year old female with dysphasia and right arm weakness 3 hours prior CT head: dense M1 sign. No established ischaemia
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Long-Term Care Updates
 Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Long-Term Care Updates October/November 2015 By Daniel Kerner, PharmD A stroke occurs when blood flow to the brain is stopped or slowed, resulting in death or damage to brain cells. There are three main
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Lecture Outline: 1/5/14
 John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
John P. Karis, MD Lecture Outline: Provide a clinical overview of stroke: Risk Prevention Diagnosis Intervention Illustrate how MRI is used in the diagnosis and management of stroke. Illustrate how competing
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
How Can We Properly Manage Patients With Stroke of Undetermined Origin?
 How Can We Properly Manage Patients With Stroke of Undetermined Origin? : Spotlight on Embolic Stroke of Undetermined Source (ESUS) MI SUN OH Department of Neurology, Hallym University Scared Heart Hospital,
How Can We Properly Manage Patients With Stroke of Undetermined Origin? : Spotlight on Embolic Stroke of Undetermined Source (ESUS) MI SUN OH Department of Neurology, Hallym University Scared Heart Hospital,
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
DEBATE: PFO MANAGEMENT TO CLOSE OR NOT TO CLOSE. Matthew Starr, MD Stroke Attending
 DEBATE: PFO MANAGEMENT TO CLOSE OR NOT TO CLOSE Matthew Starr, MD Stroke Attending DISCLOSURES None DEBATE Should PFO be closed? * * Sometimes yes THE CASE AGAINST PFO CLOSURE 1. Did the PFO cause the
DEBATE: PFO MANAGEMENT TO CLOSE OR NOT TO CLOSE Matthew Starr, MD Stroke Attending DISCLOSURES None DEBATE Should PFO be closed? * * Sometimes yes THE CASE AGAINST PFO CLOSURE 1. Did the PFO cause the
Patients presenting with acute stroke while on DOACs
 Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
Patients presenting with acute stroke while on DOACs Vemmos Kostas, MD, PhD Stroke Medicine Hellenic Cardiovascular Research Society Conflicts of interest Honoraria and speaker fees from: BAYER, SANOFI,
I, (Issam Moussa) DO NOT have a financial interest/arrangement t/ t or affiliation with one or more organizations that could be perceived as a real
 DO NOT have a financial interest/arrangement t/ t or affiliation with one or more organizations that could be perceived as a real") PFO Closure: Where We Are Going to after CLOSURE I Study? Issam D. Moussa, MD Professor of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida Disclosure Statement of
PFO Closure: Where We Are Going to after CLOSURE I Study? Issam D. Moussa, MD Professor of Medicine Chair, Division of Cardiovascular Diseases Mayo Clinic Jacksonville, Florida Disclosure Statement of
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor
 Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
Mike Previti, MD UW Valley Medical Center, Stroke Program Medical Director UW, Dept of Neurology, Clinical Instructor What is TIA? TIA vs CVA, does it matter? Who needs the hospital? What is the ABCD 2
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
True cryptogenic stroke
 True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
True cryptogenic stroke Arne Lindgren, MD, PhD Dept of Clinical Sciences Lund, Neurology, Lund University Dept of Neurology and Rehabilitation Medicine Skåne University Hospital Lund, Sweden Disclosures
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
APPENDIX A NORTH AMERICAN SYMPTOMATIC CAROTID ENDARTERECTOMY TRIAL
 APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
APPENDIX A Primary Findings From Selected Recent National Institute of Neurological Disorders and Stroke-Sponsored Clinical Trials That Have shaped Modern Stroke Prevention Philip B. Gorelick 178 NORTH
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Carotid Artery Stenting
 Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
Carotid Artery Stenting Woong Chol Kang M.D. Gil Medical Center, Gachon University of Medicine and Science, Incheon, Korea Carotid Stenosis and Stroke ~25% of stroke is due to carotid disease, the reminder
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Carotid Artery Revascularization: Current Strategies. Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014
 Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Carotid Artery Revascularization: Current Strategies Shonda Banegas, D.O. Vascular Surgery Carondelet Heart and Vascular Institute September 6, 2014 Disclosures None 1 Stroke in 2014 Stroke kills almost
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Section Editor Scott E Kasner, MD
 1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
1 of 6 9/29/2013 6:55 PM Official reprint from UpToDate www.uptodate.com 2013 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis,
Carotid Artery Stenosis
 Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
Evidence-Based Approach to Carotid Artery Stenosis Seong-Wook Park, MD Division of Cardiology, Asan Medical Center University of Ulsan College of Medicine, Seoul, Korea Carotid Artery Stenosis Carotid
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
03/30/2016 DISCLOSURES TO OPERATE OR NOT THAT IS THE QUESTION CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE
 CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
CAROTID INTERVENTION IS INDICATED FOR ASYMPTOMATIC CAROTID OCCLUSIVE DISEASE Elizabeth L. Detschelt, M.D. Allegheny Health Network Vascular and Endovascular Symposium April 2, 2016 DISCLOSURES I have no
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
M. Edip Gurol, MD, MSc Stroke Service/Neurology, Massachusetts General Hospital, Harvard Medical School
 High Risk of Thromboembolism and ICH: Problems with Medical Management M. Edip Gurol, MD, MSc Stroke Service/Neurology, Massachusetts General Hospital, Harvard Medical School Disclosures Funding from NIH
High Risk of Thromboembolism and ICH: Problems with Medical Management M. Edip Gurol, MD, MSc Stroke Service/Neurology, Massachusetts General Hospital, Harvard Medical School Disclosures Funding from NIH
Do Not Cite. Draft for Work Group Review.
 Defect Free Acute Inpatient Ischemic Stroke Measure Bundle Measure Description Percentage of patients aged 18 years and older with a diagnosis of ischemic stroke OR transient ischemic attack who were admitted
Defect Free Acute Inpatient Ischemic Stroke Measure Bundle Measure Description Percentage of patients aged 18 years and older with a diagnosis of ischemic stroke OR transient ischemic attack who were admitted
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion. Greg Francisco, MD, FACC
 Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Page 1. Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion. Atrial fibrillation: Scope of the problem
 Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion Benjamin A. D Souza, MD, FACC, FHRS Assistant Professor of Clinical Medicine Penn Presbyterian Medical Center Cardiac
Current Trends in the Management of Atrial Fibrillation: Left Atrial Appendage Occlusion Benjamin A. D Souza, MD, FACC, FHRS Assistant Professor of Clinical Medicine Penn Presbyterian Medical Center Cardiac
Patients selection criteria for LAA occlusion. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Patients selection criteria for LAA occlusion Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Atrial Fibrillation The most common cardiac arrhythmia. Confers
Patients selection criteria for LAA occlusion Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Atrial Fibrillation The most common cardiac arrhythmia. Confers
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth. May 23, 2018
 Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Andrew Barreto, MD MS Associate Professor of Neurology Stroke Neurologist UTHealth May 23, 2018 Disclosure No personal financial relationships with any company. Presentation Outline Definitions, signs
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France
 Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
Occlusion de l'auricule gauche: Niche ou réel avenir? D Gras, MD, Nantes, France LAA Occlusion Is there a real future? Background Protect AF Trial Other Studies CAP, ASAP, Prevail Left Atrial Appendage
NeuroPI Case Study: Anticoagulant Therapy
 Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
Case: An 82-year-old man presents to the hospital following a transient episode of left visual field changes. His symptoms lasted 20 minutes and resolved spontaneously. He has a normal neurological examination
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Updates from 2017 International Stroke Conferences
 Updates from 2017 International Stroke Conferences Ravi Menon, MD Swedish Neuroscience Institute May 11, 2017 Seattle, WA 1 Disclosures No relevant financial disclosures Clinical trial involvement: Former
Updates from 2017 International Stroke Conferences Ravi Menon, MD Swedish Neuroscience Institute May 11, 2017 Seattle, WA 1 Disclosures No relevant financial disclosures Clinical trial involvement: Former
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute ischemic stroke TOAST classification of, 270 Acute myocardial infarction (AMI) cardioembolic stroke following, 207 208 noncardioembolic
Index Note: Page numbers of article titles are in boldface type. A Acute ischemic stroke TOAST classification of, 270 Acute myocardial infarction (AMI) cardioembolic stroke following, 207 208 noncardioembolic
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근
 Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Management of Patients with Atrial Fibrillation Undergoing Coronary Artery Stenting 경북대의전원내과조용근 Case (2011, 5) 74-years old gentleman Exertional chest pain Warfarin with good INR control Ex-smoker, social(?)
Stroke Update. Claire J. Creutzfeldt, MD January 12, 2018
 Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Stroke Update Claire J. Creutzfeldt, MD January 12, 2018 Disclosures None relevant to this presentation I receive funding from the NINDS What s new in stroke? A new model for cardioembolic stroke: atrial
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Atrial Fibrillation. Alan Bell, MD, CCFP. Staff Physician, Humber River Regional Hospital. University of Toronto
 Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
Pearls in Thrombosis 1 Atrial Fibrillation Alan Bell, MD, CCFP Staff Physician, Humber River Regional Hospital Assistant tprofessor, Department tof Family and Community Mdii Medicine University of Toronto
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
2017 Cardiovascular Symposium CRYPTOGENIC STROKE: A CARDIOVASCULAR PERSPECTIVE DR. WILLIAM DIXON AND DR. VENKATA BAVAKATI SOUTHERN MEDICAL GROUP, P.A.
 CRYPTOGENIC STROKE: 2017 Cardiovascular Symposium A CARDIOVASCULAR PERSPECTIVE DR. WILLIAM DIXON AND DR. VENKATA BAVAKATI SOUTHERN MEDICAL GROUP, P.A. CRYPTOGENIC STROKE CRYPTOGENIC: OF OBSCURE OR UNKNOWN
CRYPTOGENIC STROKE: 2017 Cardiovascular Symposium A CARDIOVASCULAR PERSPECTIVE DR. WILLIAM DIXON AND DR. VENKATA BAVAKATI SOUTHERN MEDICAL GROUP, P.A. CRYPTOGENIC STROKE CRYPTOGENIC: OF OBSCURE OR UNKNOWN
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Watchman Implantation Case Presentation and Discussion
 Watchman Implantation Case Presentation and Discussion Walid Saliba, MD, FHRS Director Atrial Fibrillation Center Co-Director AF Stroke Prevention Center Cleveland Clinic Indication FDA NonValvular AF
Watchman Implantation Case Presentation and Discussion Walid Saliba, MD, FHRS Director Atrial Fibrillation Center Co-Director AF Stroke Prevention Center Cleveland Clinic Indication FDA NonValvular AF
Management of Atrial Fibrillation. Leon Ptaszek, MD, PhD, FACC, FHRS 25 March 2018
 Management of Atrial Fibrillation Leon Ptaszek, MD, PhD, FACC, FHRS 25 March 2018 Disclosures Speaker: St. Jude Medical, Biotronik Consultant: St. Jude Medical, World Care Clinical Objectives Recognize
Management of Atrial Fibrillation Leon Ptaszek, MD, PhD, FACC, FHRS 25 March 2018 Disclosures Speaker: St. Jude Medical, Biotronik Consultant: St. Jude Medical, World Care Clinical Objectives Recognize
Sixth Annual Intensive Update in Neurology 9/15-16/2016. W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist
 W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist 1 One Strategy for cryptogenic stroke: ESUS Positively defined criteria FDA allows clinical trials NOACs have lower risk profile Another strategy
W Tom Kushner DO Swedish Stroke Clinic Neurohospitalist 1 One Strategy for cryptogenic stroke: ESUS Positively defined criteria FDA allows clinical trials NOACs have lower risk profile Another strategy
Overview. Example Case. Current Topics in Stroke Management. Whats the next best step in imaging? 4/9/14
 Overview Current Topics in Stroke Management Kenneth A. Fox, M.D. Assistant Clinical Professor - UCSF Department of Medicine Chief Department of Neurology Medical Director J.C.C. Primary Stroke Center
Overview Current Topics in Stroke Management Kenneth A. Fox, M.D. Assistant Clinical Professor - UCSF Department of Medicine Chief Department of Neurology Medical Director J.C.C. Primary Stroke Center
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Overview. Example Case Whats the next best step in imaging? Current Topics in Stroke Management 2/22/2012
 Overview Current Topics in Stroke Management Kenneth A. Fox, M.D. Chief Department of Neurology Medical Director J.C.C. Primary Stroke Center Kaiser Permanente San Francisco Board of Directors American
Overview Current Topics in Stroke Management Kenneth A. Fox, M.D. Chief Department of Neurology Medical Director J.C.C. Primary Stroke Center Kaiser Permanente San Francisco Board of Directors American