Sepsis. Ethan Sterk, DO. Assistant Professor Department of Emergency Medicine Medical Director, Sepsis Program Loyola University Medical Center
|
|
|
- Deborah Walker
- 6 years ago
- Views:
Transcription
1 Sepsis Ethan Sterk, DO Assistant Professor Department of Emergency Medicine Medical Director, Sepsis Program Loyola University Medical Center Grand Rounds 2/5/13
2 Why? It is common, lethal and expensive. Of the 750,000+ severe sepsis cases each year in the US, an estimated 215, 000 (28.6%) pts die. Mortality associated with severe sepsis has been reported as high as 30-50% The incidence is likely to increase even more Aging population Medical and technological advances Widespread use of antibiotics It is costly Accounts for ~ 40% of all ICU expenditures, totaling $16.7B in the US Average LOS/cost per case: 19.6 days and $22,100 Angus, DC et al. Critical Care Medicine. 2001; 29: With early recognition and aggressive treatment = better pt outcomes
3 SIRS Criteria: Temp > 38 C or < 36 C Heart Rate > 90 Respiratory Rate > 20 or PaCO2 < 32 WBC > 12K, < 4K or > 10% Bands Sepsis = 2/4 SIRS + infection Severe sepsis = sepsis-induced tissue hypoperfusion (inc lactate) / organ dysfunction (AMS, lungs, kidney, etc) Septic shock = sepsis-induced hypotension (SBP < 90, MAP < 70, SBP dec > 40 from baseline) persisting despite adequate fluid resuscitation
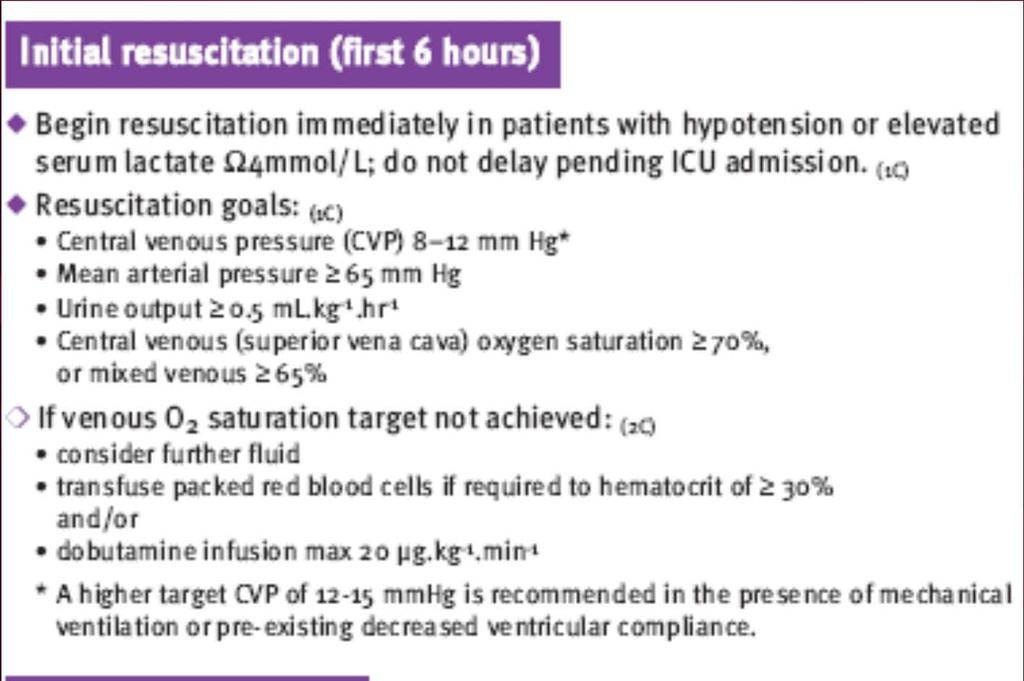
4 What is Early Goal Directed Therapy? EGDT is a comprehensive strategy for identifying and treating septic pts that include: ** Identification of high risk pts ** Mobilization of resources for intervention Performance of a consensus-derived protocol to reverse early hemodynamic disturbances The core objectives of EGDT in sepsis are to: ** Detect and treat occult global tissue hypoxia early before organ damage becomes irreversible ** Achieve a systemic oxygen delivery and demand balance

5 Landmark Literature (NEJM 2001)
6
7 Results In hospital Mortality Standard therapy 46.5 % EGDT 30.5 % Mean LOS in days (for pts who survived to hospital discharge) Standard therapy 18.4 days EGDT 14.6 days
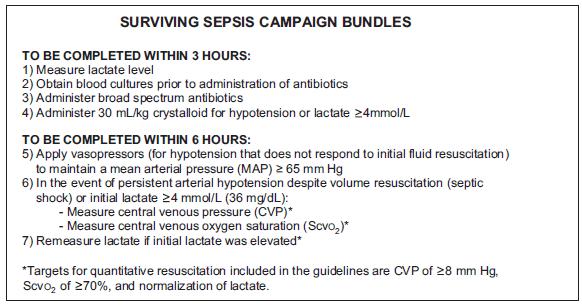
8 Surviving Sepsis Campaign The Society of Critical Care Medicine, the European Society of Intensive Care Medicine and the International Sepsis Forum joined forces to develop a three-phase Surviving Sepsis Campaign. First phase: six-point action plan to reduce global mortality from severe sepsis by 25% by Second phase: focused on creating guidelines for sepsis management. Crit Care Med 2004; 32: Update Crit Care Med 2008; 36(1): Update February 2013 issues of Critical Care Medicine and Intensive Care Medicine Phase three: translating the guidelines into clinical practice.
9
10 Controversy? Which part makes a difference? Does everyone need an invasive approach?
11 Which part makes a difference? Early recognition of sepsis more aggressive txt / EGDT / better outcomes The research supports it Aggressive IVFs In Rivers original study, average total IVFs within first 6 hours: Standard therapy: 3.5L EGDT: 5L Early antibiotics Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Kumar, et al. Critical Care Medicine: June Volume 34 - Issue 6 - pp Each hour of delay in antimicrobial administration over the first 6 hrs was associated with an average decrease in survival of 7.6% RBC transfusion, steroids, glycemic control, xigris???
12 Is it necessarily Rivers/SSC guidelines that make a difference? The effect of a quantitative resuscitation strategy on mortality in patients with sepsis: a meta-analysis Crit Care Med Oct;36(10): Applying an early quantitative resuscitation strategy (EGDT) to patients with sepsis imparts a significant reduction in mortality. They observed distinct variations in the goals / end points targeted among the studies. = pts did better with just using goals (not necessarily Rivers/SSC guidelines/goals) and early treatment

13 Does everyone need an invasive approach? Hemodynamic / Perfusion Goals Fluid resuscitation CVP IVC US MAP > 65 Tissue oxygenation ScvO2 Lactate
14 Fluid resuscitation: CVP vs IVC US CVP Invasive can lead to complications, more time consuming & is typically started later (BP not responding to IVFs, increasing lactate). Not reliable as 1 measurement better to follow trends. Made up numbers (based on EGDT recs) How well does a CVP 8-12 translate to evidence that the tank is full? the evidence is WEAK at best. Bottom line: Even reaching CVP thresholds does not guarantee adequate fluid loading. While a very low CVP indicates an under-resuscitated pt, the opposite is not true. IVC US Non-invasive Can be used during initial evaluation / earlier in the course of resuscitation. Can also assess global heart function and r/o pericardial effusion.
15 Emergency Department Bedside Ultrasonographic Measurement of the Caval Index for Noninvasive Determination of Low Central Venous Pressure Annals of Emergency Medicine, Volume 55, Issue 3, Pages , March 2010 Bedside ultrasonographic measurement of caval index (IVC collapsibility) > 50% is strongly associated with a low CVP (< 8 mm Hg). It could be a useful noninvasive tool in determining a patients volume status / need for aggressive fluid replacement well before invasive monitoring can be established. Dr Scott Weingart - EMCrit Blog Greater New York Hospital Association - STOP Sepsis Collaborative 50% has been validated more often, but requires caliper measurement. 30% is essentially what you can eyeball. I would prefer people err on the side of too much fluid early in the resus
16 Tissue oxygenation Lactate Why use this? When to use it? Suspect sepsis If you are drawing/sending blood cultures (Dec added to panel) If you are admitting a pt who you think might be infected Dx: UTI, PNA, fever, cellulitis, etc. Currently working adding sepsis screening question to admit orders

17 Clinical manifestations of disordered microcirculatory perfusion in severe sepsis. Stephen Trzeciak and Emanuel P Rivers; Critical Care Aug 2005

18 Lactate Nonspecific for anaerobic metabolism Impaired microcirculatory flow is one of the many possible mechanisms for elevated lactate in severe sepsis Consensus recommendations advocate using lactate measurements to help identify normotensive pts who are in cryptic shock and in need of aggressive resuscitation. Cryptic Septic Shock: A Sub-analysis of Early, Goal-Directed Therapy Chest 2003 Subgroup analysis of Rivers original study: MAP > lactate > 4 had mortality rate 60.9% MAP < 70 had mortality rate 42%
19 The Surviving Sepsis Campaign: results of an international guidelinebased performance improvement program targeting severe sepsis Critical Care Medicine. 38(2): , February Hypotension and lactate > 4: 46.1% Hypotension alone: 36.7% Lactate > 4 alone: 30% Prognostic value of incremental lactate elevations in emergency department patients with suspected infection. Acad Emerg Med 2012 Aug; 19:983. Mortality rose continuously across a continuum of incremental lactate elevations 6% in pts with lactate levels <1.0 mmol/l 39% in pts with levels of 19 to 20 mmol/l.


20 ScvO2 -or- SmvO2 Normal ScvO2 > 70% Normal SmvO2 > 65% If low = tissue not seeing enough hgb (so it is taking more O2) 1. Not enough hgb to come around (relative anemia) 2. Hgb not coming around fast enough (cardiac output inadequate)
21 Tissue oxygenation Lactate Clearance vs Central Venous Oxygen Saturation as Goals of Early Sepsis Therapy JAMA. Feb 2010; 303(8): To test the hypothesis of noninferiority between lactate clearance and central venous oxygen saturation (ScvO2) as goals of early sepsis resuscitation ScvO2 group: resuscitated to normalize CVP, MAP & ScvO2 > 70% Lactate clearance group: resuscitated to normalize CVP, MAP & lactate clearance of at least 10%. Lactate clearance was not inferior to ScvO2 and did not result in significantly different in-hospital mortality. Lactate clearance: 17% vs ScvO2: 23%
22 Metabolic goals Adrenal replacement txt: Hydrocortisone 100 mg IV q8 Vasopressor-refractory hypotension, suspect adrenal insufficiency (if pts endocrine / steroid history warrants it, got etomidate?) ACTH stim test, cortisol levels no longer recommended Glycemic control Controversial history but most recent studies / recommendations (tight control no change in mortality, increased incidence of mod-severe hypoglycemia) Insulin therapy when 2 consecutive glucose levels > 180 with a goal < 180 NICE-SUGAR study Activated Protein C (xigris) On October 25, 2011, Eli Lilly announced a voluntary-recall of Xigris following the results of the PROWESS-SHOCK trial, which demonstrated no survival benefit when using the drug when compared to placebo.
23 Blood controversy Original Rivers study and SSC recs were to transfuse prbcs to hgb > 10 Increase the O2 carrying capacity Multiple studies: has not shown a mortality benefit + potential transfusion risks/reactions Now more conservative approach If Hgb < 7: transfuse 1 unit prbc If Hgb 7-10: consider transfusion especially in elderly pts or with CAD
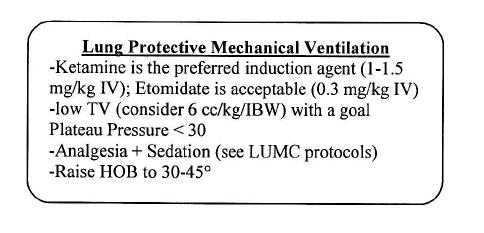
24 Airway/O2 Maximize O2 delivery with supplemental O2 to keep O2 sats > 90% Indications for Intubation Airway protection Oxygenation / Ventilation Expected clinical course 75% of pts with sepsis (severe/shock) require mechanical ventilation Increased work of breathing d/t hypoxia + compensation for metabolic/lactic acidosis ARDSNET Compared TV: 12 cc/kg/ibw vs 6 cc/kg/ibw with goal plateau pressure < 30 cm H2O 22% dec mortality, inc in ventilator-free / organ failure-free days Maintain HOB decrease risk of aspiration PNA
25 Special circumstance Pt with severe metabolic acidosis and needing mechanical ventilation Compensation occurs via hyperventilation When these patients require intubation and mechanical ventilation, be sure to provide the same level of respiratory compensation when setting the ventilator. Failing to provide a rate sufficient to compensate for the pre-intubation acidosis leads to a rapid drop in ph, bradycardia and eventually asystole. Observe their MV (minute ventilation) just prior to paralysis/intub = this should be your vent setting RR. In general, rates can be increased to about 30 breaths per minute, after which auto-peep becomes problematic. If you anticipate a difficult intub/delay, consider giving IV Bicarb to maintain ph during RSI
26 Etomidate controversy known to cause transient adrenal suppression the clinical significance of this drug effect continues to be debated No compelling evidence to eliminate RSI etomidate in sepsis 0.3 mg/kg IV Consider Ketamine mg/kg IV Stimulates SNS augments HR/BP Bronchodilator Analgesia + Sedation A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial The Lancet, Vol 375, Pages , February 2010 Morphine prn vs Propofol/Versed + Morphine prn Analgesia only group less days on vent & shorter ICU stays, but increased agitated delirium Refer to LUMC protocols Fentanyl (1 mcg/kg/hr) + Versed (1 mg/hr) drips titrated to effect
27 Cultural change We have Stroke / STEMI / Trauma protocols/teams and Sepsis should be viewed just as important To be successful we need a multidisciplinary team approach + acceptance within
28
29
30
31
32
33
34
35
36
37
38
39

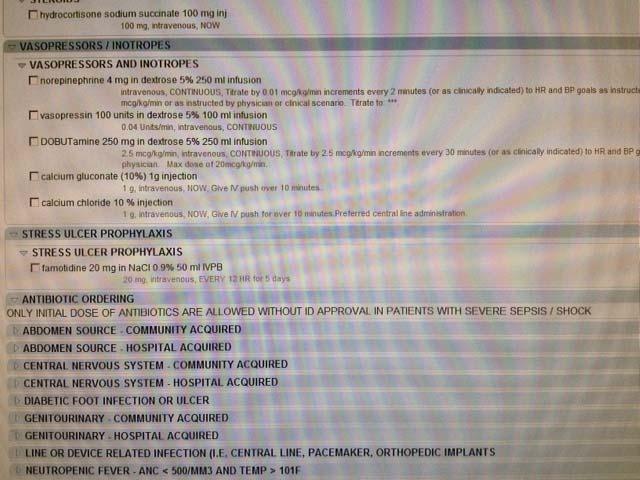
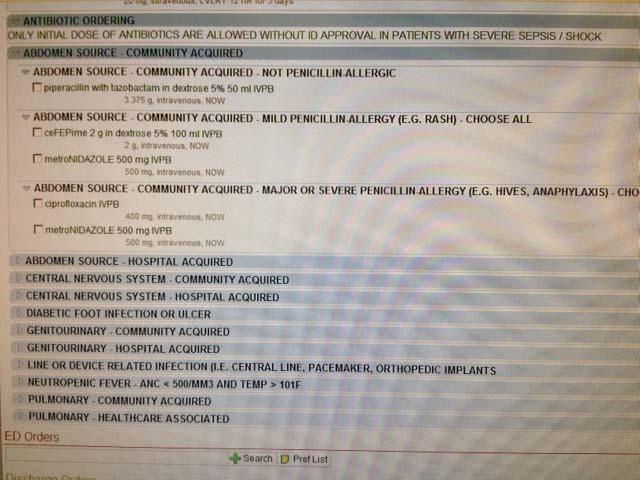
40 Order set: Sepsis Adult
41
42
43 2012 SSC guidelines A formal conflict of interest policy was developed at the onset of the process and enforced throughout. The entire guideline process was conducted independent of any industry funding. The recommendations in this document are intended to provide guidance for the clinician. cannot replace the clinicians decision-making capability when he or she is presented with a patients unique set of clinical variables. These recommendations are intended to be best practice and not created to represent standard of care. The committee believes that the greatest outcome improvement can be made through education and process change. Emphasize routine screening for earlier identification/txt Sending more lactates, etc.
44 Fluid resuscitation? Recognized limitations of static measures (CVP) and that targeting dynamic measures of fluid responsiveness may have advantages. However the efficacy of these techniques remains incomplete and requires further study before endorsement. In pts with elevated lactate, they suggest targeting resuscitation to normalize lactate.
45
46 EMCrit Lessons from the STOP Sepsis Collaborative Dec ,000 patient mark Screening Send lots of lactates Make lactate > 4 a panic value (LUMC Dec 2012) Non-invasive protocols have evidence and seem to be working Early appropriate antibiotics Simultaneous Infusions Check Your Work Mandate repeat lactates
47 Headline news - New York State Adopts Sepsis Rules NY Times Dec 2012: One Boy s Death Moves State to Action to Prevent Others WSJ Jan 2013: NY plans new hospital rules for treating sepsis In a precedent-setting statement during his State of the State Message, New York's Governor Andrew M. Cuomo announced that every hospital in the state must adopt sepsis screening procedures. State Health Commissioner Dr. Nirav Shah said the regulations, which are expected to take effect in May after a public comment period, could prevent 5,000 to 8,000 deaths a year. "New York will become the first state in the nation to require our hospitals to adopt best practices for the early identification and treatment of sepsis"
48 Conclusion Sepsis is common, lethal and expensive EGDT can make a difference Have a high index of suspicion (SIRS + suspected infection) Send lactate early and often Be more aggressive with IVFs Early Antibiotics Use the ultrasound early and often if available Not everyone needs an Invasive strategy use the guidelines created Treat it as important as a Stroke / STEMI / Trauma
49
Sepsis. Ethan Sterk, DO. Assistant Professor Department of Emergency Medicine Medical Director, Sepsis Program Loyola University Medical Center
 Sepsis Ethan Sterk, DO Assistant Professor Department of Emergency Medicine Medical Director, Sepsis Program Loyola University Medical Center Why? It is common, lethal and expensive. Of the 750,000+ severe
Sepsis Ethan Sterk, DO Assistant Professor Department of Emergency Medicine Medical Director, Sepsis Program Loyola University Medical Center Why? It is common, lethal and expensive. Of the 750,000+ severe
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Looking for sepsis. Sepsis: Update. Prevalence of High Profile Dzs. Screening and risk stratification. Mortality of High Profile Diseases
 Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Sepsis: Update Prevalence of High Profile Dzs Edward A. Panacek, MD, MPH Professor and Chair, Emergency Medicine USA Medical Center, Mobile, AL NDAFP Conference Big Sky. 2016 Syllabus Angus Crit Care Med
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Introduction. Centers for Disease Control and Prevention (CDC),
,") When Prevention Fails: The Clinical and Economic Impact of Sepsis Introduction Healthcare-associated infections are one of the top 0 leading causes of death in the U.S. The US Centers for Disease Control
When Prevention Fails: The Clinical and Economic Impact of Sepsis Introduction Healthcare-associated infections are one of the top 0 leading causes of death in the U.S. The US Centers for Disease Control
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Key Points. Angus DC: Crit Care Med 29:1303, 2001
 Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Key Points Sepsis is the combination of a known or suspected infection and an accompanying systemic inflammatory response (SIRS) Severe sepsis is sepsis with acute dysfunction of one or more organ
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Critical Care Medicine Update for Non-Intensivists 2015
 27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
Inflammation. Sepsis Ladder
 Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Billion
 Surviving : Are we? The 7th National Emergency Medicine Congress Antalya, Turkey Alexander L. Eastman, MD, MPH Department of Surgery UTSW Severe : A Significant Healthcare Challenge Major cause of morbidity
Surviving : Are we? The 7th National Emergency Medicine Congress Antalya, Turkey Alexander L. Eastman, MD, MPH Department of Surgery UTSW Severe : A Significant Healthcare Challenge Major cause of morbidity
Severe Sepsis/ Septic Shock. Fereshte Sheybani, MD. Assistant Professor in Infectious Diseases
 Severe Sepsis/ Septic Shock Fereshte Sheybani, MD. Assistant Professor in Infectious Diseases Sepsis is one of the oldest and most elusive syndromes in medicine. Hippocrates claimed that sepsis (σήψις)
Severe Sepsis/ Septic Shock Fereshte Sheybani, MD. Assistant Professor in Infectious Diseases Sepsis is one of the oldest and most elusive syndromes in medicine. Hippocrates claimed that sepsis (σήψις)
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia
 Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
AVOIDING THE CRASH 3: RELAX, OPTIMAL POST-AIRWAY MANAGEMENT AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis: Update on Diagnosis, Evaluation and Management
 Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
From Bench to Bedside: Reducing Sepsis Mortality
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/from-bench-to-bedside-reducing-sepsismortality/4009/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/from-bench-to-bedside-reducing-sepsismortality/4009/
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
The Management of Septic Shock
 The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Welcome! While we wait, please open PollEv.com/jhhicu012
 Welcome! While we wait, please open PollEv.com/jhhicu012 Login username jhhicu012 Password jhhicupoll OR Text JHHICU012 to 0427541357 once to join the poll response and be able to answer polls by SMS Same
Welcome! While we wait, please open PollEv.com/jhhicu012 Login username jhhicu012 Password jhhicupoll OR Text JHHICU012 to 0427541357 once to join the poll response and be able to answer polls by SMS Same
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates in Emergency Department Management of Sepsis
 Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Resident Journal Review Updates in Emergency Department Management of Sepsis Authors: Eli Brown, MD; Allison Regan, MD; Kaycie Corburn, MD; Jacqueline Shibata, MD Edited by: Jay Khadpe, MD FAAEM; Michael
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
A Critical Review of Early Goal Directed Therapy and Government Endorsement
 A Critical Review of Early Goal Directed Therapy and Government Endorsement Charles Natanson M.D. Critical Care Medicine Department Clinical Center National Institutes of Health Clinical Center None Conflicts
A Critical Review of Early Goal Directed Therapy and Government Endorsement Charles Natanson M.D. Critical Care Medicine Department Clinical Center National Institutes of Health Clinical Center None Conflicts
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some