|
|
|
- Darcy Dennis
- 6 years ago
- Views:
Transcription

1 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo Clinic, Rochester, MN
2 DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None


3 Dobutamine Echo and Prediction of LV Recovery % Sensitivity Specificity Biphasic Any improvement Qureshi: Circ, 2/4/97 DSE

4 Improvement Throughout Study with Dobutamine

5 Biphasic Response with Dobutamine
6 Cases 1. Soccer coach receives a red card 2. Let Lord Murphy Reign 3. Bigger is not always better 4. Very Tight 5. Two for the price of one 6. Go With the Flow
7 Case: 51 yo male, soccer coach New onset chest pain while biking No CV risk factors Referred for Exercise Echo 12 minutes on Bruce Protocol 118% FAC 13 METS Fatigue Positive ECG Flat BP response: 158/92 to 160/84 mmhg

8 Exercise Echo Rest Exercise 4ch LV LV 2ch

9 Exercise Echo Rest Exercise 5ch LV LV SA
10 What does the Exercise Echo show? 1. Normal 2. Inferior ischemia 3. Circumflex ischemia 4. LAD ischemia 5. Multivessel disease
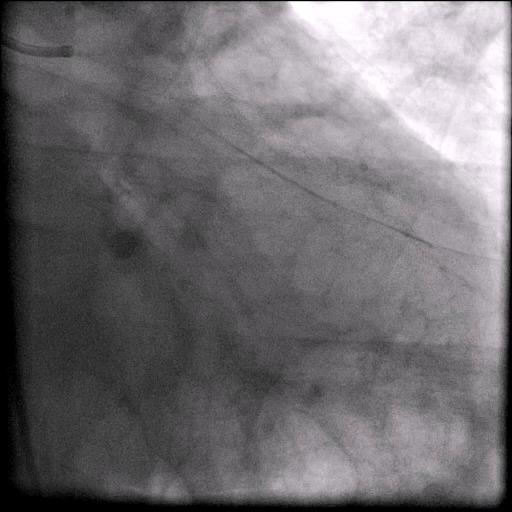
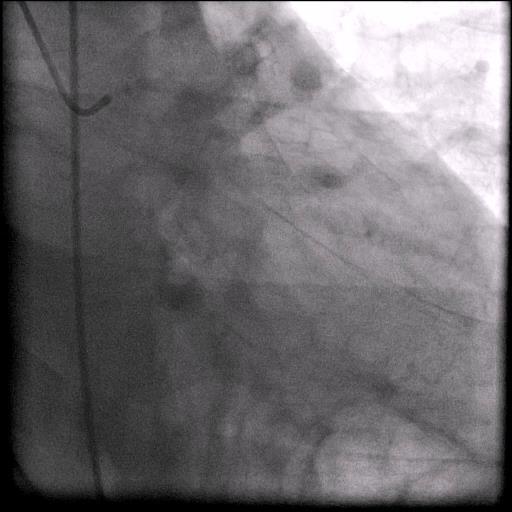
11 Catheterization Post stent
12 Case: 67 yo male Referred for pre-op clearance for 7 cm Thoracic Aortic Aneurysm repair No cardiac hx (no CP, no dyspnea) HTN, hyperlipidemia, obesity, ex-smoker Sedentary lifestyle exercise involves getting up from sofa to get TV remote controller Referred for dobutamine stress echo

13 Dobutamine Stress Echo 4 Ch View Baseline 10 mcg/kg/min LV LV LV LV

14 Dobutamine Stress Echo 3 Ch View Baseline 10 mcg/kg/min LV LV LV LV

15 Dobutamine Stress Echo 2 Ch View

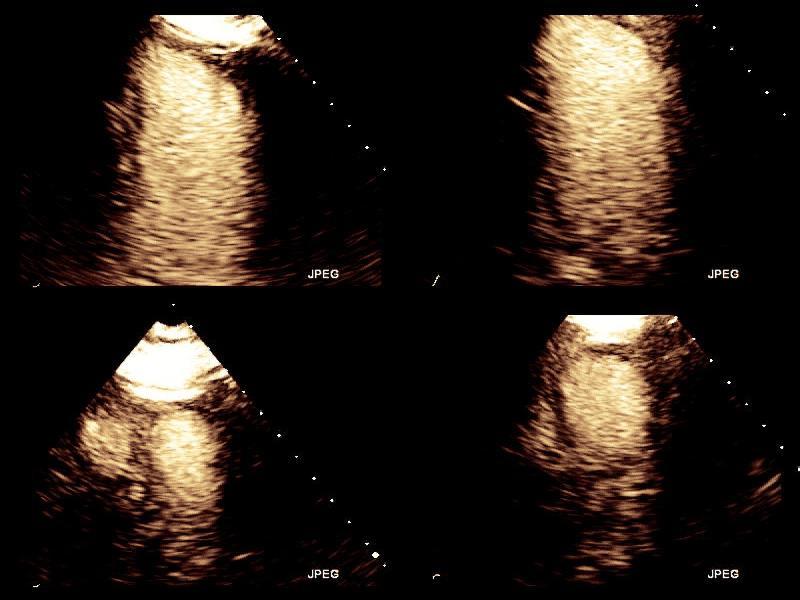
16 Dobutamine Stress Echo Short Axis View
17 What does the DSE show? 1. Normal 2. Inferior, Inferolateral Ischemia 3. Anterior ischemia 4. Apical ischemia
18 Cx Cath
19 67 yo male pre-op for TAA repair Multivessel CAD, diffuse disease Medical Rx TAA repair 28-mm woven Hemashield graft Rocky post-op course; delayed extubation, afib, elevated troponin, worsening of inferolateral RWMA on echo d/c d after 16 day hospitalization 1 yr later: dx d with metastatic stomach CA Hospice
20 70 year old male with dyspnea on exertion PMH DM HTN Hyperlipidemia Referred for exercise echo
21 Exercise Echocardiogram 5ch Rest Rest 4ch 5ch Immediately Postexercise Stress 4ch SA 2ch SA 2ch
22 What does the DSE show? 1. Normal 2. RCA ischemia 3. Circumflex ischemia 4. Mutlivessel ischemia


23 Exercise Echocardiogram 5ch Rest Rest 4ch 5ch Immediately Postexercise Stress 4ch SA 2ch SA 2ch LVEF: 60 to 50% LV size: Dilatation

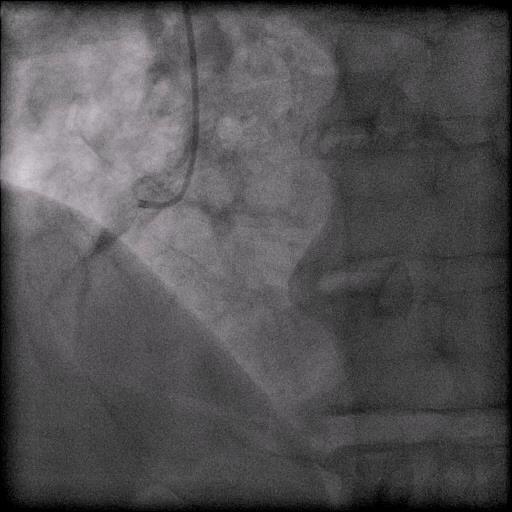
24 High grade stenosis of the left anterior descending and 1st diagonal coronary arteries
25 40 Year Old Executive Male Heartburn and eructation with exertion HTN Hyperlipidemia Smoker Referred for exercise echo 6 minutes on Bruce Protocol heartburn and positive EKG changes

26 Exercise Echocardiogram LV LV
27 Exercise Echocardiogram
28 What does the DSE show? 1. Normal 2. RCA ischemia 3. Circumflex ischemia 4. LAD ischemia

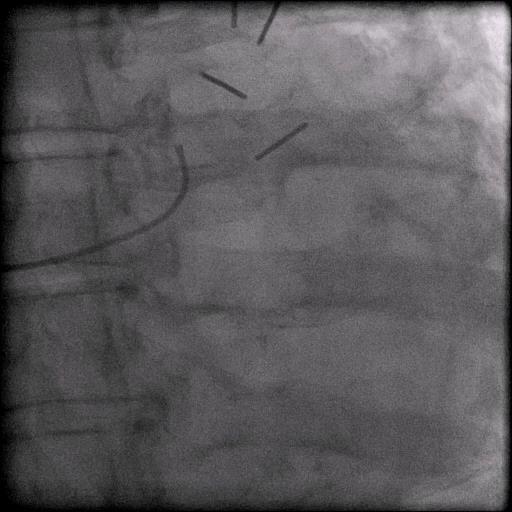
29 Cath

30 Cath: Post Stenting
31 64 yo male, engineer from Bagdad with chest pain Hx PTCA, DES to D1 and LAD ASA, Plavix, Cardiac rehab Returns 1 yr later; asymptomatic, but sedentary, wants ex echo? Medication compliance

32 64 yo male, engineer, Hx stent to D1/LAD

33 64 yo male, engineer with chest pain
34 What does the DSE show? 1. Normal 2. RCA ischemia 3. Circumflex ischemia 4. LAD/D1 ischemia 5. Non-diagnostic study

35 What does the cath show?
36 Case 70 year old male PMH: Anteroapical MI, CABG after MI ICD placed: NSVT, EF 30% Asymptomatic for 5 years Now presents with CHF, NYHA class III Physical Exam: Grade 3/6 late peaking SEM Diminished carotid upstroke Single component S2

37 2D Echo: Severe LV Dysfunction EF: 20%


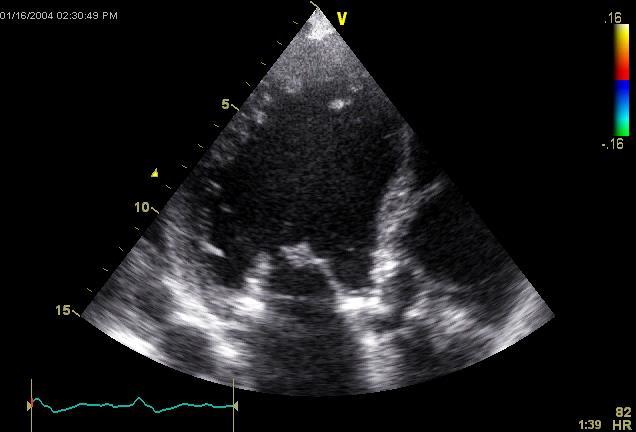
38 Aortic Valve Parasternal Long-Axis Parasternal Short-Axis

39 Aortic Valve Gradient Pk Gr = 27 mmhg Mn Gr = 14 mmhg AVA = 0.8 cm2


40 Coronary Angiogram Patent LIMA Patent SVG to OM1 Occluded LAD 90% proximal Left Circumflex stenosis No significant disease in RCA Viability Study: Apical scar, all other areas viable
41 Question What would you do next? A. Aortic valvuloplasty B. Refer to CT Surgery for AVR C. Dobutamine stress study D. Prayer

42 Dobutamine in Low Gradient- Low EF Aortic Stenosis True severe AS SV, transvalvular gradient; No change in calculated AVA remains in severe range Pseudo severe AS SV and AVA; No significant transvalvular gradient




43 Baseline Pseudo Aortic Stenosis Dobutamine AVA 0.8 cm cm 2 Stroke volume TVI 8 cm TVI 16 cm cc Mean gradient TVI 42 cm Dimensionless Index = 0.19 TVI 51 cm Dimensionless Index = mmhg Eleid M, Mankad S et al. Heart Fail Rev. 2012

44 True Low Gradient/Low EF Aortic Stenosis Baseline Dobutamine Stroke volume cc Frederick-04-still.jpg Mean gradient mmhg Dimensionless Index = 0.22 Dimensionless Index = 0.23 AVA = 0.7 cm 2 Eleid M, Mankad S et al. Heart Fail Rev. 2012

45 Yes 15 patients 21 pt AVR Contractile reserve Increase in SV >20% Periop mortality 7% 12 survive Class I-II 2 late deaths Non-cardiac
46 Yes 15 patients 21 pt AVR Contractile reserve No 6 patients In pt with LV systolic dysfunction and AS with a Periop low output and a low MG, dobutamine Periop mortality challenge 7% may aid in selecting mortality those 33% who would benefit from an AV operation. 2 late deaths 2 late deaths Circulation Non-cardiac 2002; 106: CHF 12 survive Class I-II 2 survive Class I-II Nishimura: Circulation, 2002
47 Low Gradient Aortic Stenosis Monin et al - Circulation 2003; 108: AS pt - AVA 0.7, MG 29 mmhg LV contractile reserve assessed by DSE Present in 92 (Group I) Absent in 44 (Group II)
48 Kaplan-Meier Survival Estimates by Group and Treatment Operative Mortality 5% Group I Valve replacement Pt survival (%) Operative Mortality 32% Group II Valve replacement Group I Medical treatment Group II Medical treatment Follow-up (mo)
49 Case: Results of Dobutamine Stress Echo V1 TVI (cm) V2 TVI (cm) AVA (cm2) Baseline /14 5 mcg/kg/min dobutamine 10 mcg/kg/min dobutamine 20 mcg/kg/min dobutamine / / /17 Peak/Mean AV Gradient (mmhg) * No significant change in EF during study


50 Change in LVEF after AVR Severe AS with low EF Contractile Reserve No Contractile Reserve % Before AVR After AVR Quere, J.-P. et al. Circulation 2006;113:

51 Influence of Contractile Reserve in Low-gradient AS Absence of CR related to operative mortality, but it does not predict the absence of LVEF recovery in pt surviving AVR These data further support the concept that surgery should not be contraindicated on the basis of absence of CR alone Quere, J.-P. et al. Circulation 2006;113:

52 Take Home Points Dobutamine stress testing is helpful in low gradient-low EF AS Importance of contractile reserve True AS vs Pseudo AS Absence of contractile reserve substantially increases operative mortality with AVR in low EF-low gradient AS But if patients survive, EF improves and outcome good


53 Thank You! Acknowledgements: Dr. Sharon Mulvagh
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Cases in Stress Echo DISCLOSURE
 Cases in Stress Echo Susan Wilansky, MD, FRCP(C), FACC, FASE Mayo Clinic, AZ DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None 1 Exercise Testing in Patients with HCM (Class IIa)
Cases in Stress Echo Susan Wilansky, MD, FRCP(C), FACC, FASE Mayo Clinic, AZ DISCLOSURE Relevant Financial Relationship(s) None Off Label Usage None 1 Exercise Testing in Patients with HCM (Class IIa)
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
J. Schwitter, MD, FESC Section of Cardiology
 J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
J. Schwitter, MD, FESC Section of Cardiology CMR Center of the CHUV University Hospital Lausanne - CHUV Switzerland Centre de RM Cardiaque J. Schwitter, MD, FESC Section of Cardiology CMR Center of the
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
CASES IN ADVANCED IMAGING
 CASES IN ADVANCED IMAGING DAVID A. ORSINELLI, MD PROFESSOR, CLINICAL INTERNAL MEDICINE THE OHIO STATE UNIVERSITY DIVISION OF CARDIOVASCULAR MEDICINE OHIO ACC ANNUAL CONFERENCE OCTOBER 2010 WHICH IMAGING
CASES IN ADVANCED IMAGING DAVID A. ORSINELLI, MD PROFESSOR, CLINICAL INTERNAL MEDICINE THE OHIO STATE UNIVERSITY DIVISION OF CARDIOVASCULAR MEDICINE OHIO ACC ANNUAL CONFERENCE OCTOBER 2010 WHICH IMAGING
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Case Presentations TAVR: The Good Bad and The Ugly
 Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Case Presentations TAVR: The Good Bad and The Ugly Vincent J. Pompili, MD, FACC, FSCAI Professor of Internal Medicine Director of Interventional Cardiovascular Medicine and Cardiac Catheterization Laboratories
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
DISCLOSURE. Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Case Presentation #1
 Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Case Presentation #1 SCAI Fellows Course December 7, 2013 Barry F Uretsky, MD University of Arkansas for Medical Sciences Central Arkansas Veterans Health System Little Rock, AR Case Presentation #1 65
Case based learning: CMR in Heart Failure
 Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Case based learning: CMR in Heart Failure Milind Y Desai, MD FACC FAHA FESC Associate Professor of Medicine Heart and Vascular Institute, Cleveland Clinic Cleveland, OH Disclosures: none Use of Gadolinium
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users
 Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Use of Nuclear Cardiology in Myocardial Viability Assessment and Introduction to PET and PET/CT for Advanced Users February 1 5, 2011 University of Santo Tomas Hospital Angelo King A-V Auditorium Manila,
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Complications of Myocardial Infarction
 Complications of Myocardial Infarction Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Complications of Myocardial Infarction Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Getting the Most Out of Stress Echo
 Getting the Most Out of Stress Echo Vera H. Rigolin, MD, FASE, FACC, FAHA Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern
Getting the Most Out of Stress Echo Vera H. Rigolin, MD, FASE, FACC, FAHA Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD. Teo et al, Canadian Journal of Cardiology 2014;30:
 CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
CCS/CAIC/CSCS Position Statement on Revascularization Multi-vessel CAD Teo et al, Canadian Journal of Cardiology 2014;30: 1482-1491 Parallel Paper: Canadian Cardiovascular Society Guidelines for the Diagnosis
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Aortic Stenosis Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan
 Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Aortic Stenosis - 2011 Steven F. Bolling, M.D. Professor of Cardiac Surgery University of Michigan Aortic Surgery Aortic Stenosis EB CT - Ca++ everywhere! Surgery for Aortic Stenosis 100,000 USA + 100,000
Rational use of imaging for viability evaluation
 EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
EUROECHO and other imaging modalities 2011 Rational use of imaging for viability evaluation Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology, CHU Liège, Belgium
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Case #1 2017/09/16 Age: 66 Target Vessel: RCA proximal Relevant Diagnosis: Single vessel CAD with normal LVEF Coronary Risk Factors: Hypertension, smoke (90py) ECG abnormality:
Clinical Summary Live Cases I - IX Case #1 2017/09/16 Age: 66 Target Vessel: RCA proximal Relevant Diagnosis: Single vessel CAD with normal LVEF Coronary Risk Factors: Hypertension, smoke (90py) ECG abnormality:
@02-126_Coronary_calcification.ppt. Professor Molecular and Medical Pharmacology
 Assessment of Myocardial Viability Jamshid Maddahi, M.D., FACC, FASNC Professor Molecular and Medical Pharmacology (Nuclear Medicine) and Medicine (Cardiology) David Geffen School of Medicine at UCLA Director,
Assessment of Myocardial Viability Jamshid Maddahi, M.D., FACC, FASNC Professor Molecular and Medical Pharmacology (Nuclear Medicine) and Medicine (Cardiology) David Geffen School of Medicine at UCLA Director,
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Michigan Society of Echocardiography 30 th Year Jubilee
 Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Michigan Society of Echocardiography 30 th Year Jubilee Stress Echocardiography in Valvular Heart Disease Moving Beyond CAD Karthik Ananthasubramaniam, MD FRCP (Glas) FACC FASE FASNC Associate Professor
Affecting the elderly Requiring new approaches. Echocardiographic Evaluation of Hemodynamic Severity. Increasing prevalence Mostly degenerative
 Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Echocardiographic Evaluation of Hemodynamic Severity Steven J. Lester MD, FACC, FRCP(C), FASE Mayo Clinic, Arizona Relevant Financial Relationship(s) None Off Label Usage None A re-emerging public-health
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Stress Echo Cases Sunday, October 8, :10 3:30 PM 20 min
 2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
2017 ASE Echo Florida, Orlando, FL Stress Echo Cases Sunday, October 8, 2016 3:10 3:30 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t o r o f E c h o c a r d i o g r a p h y L a b A s s o
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
2/26/2013. NCDR.13 Case Scenario Presentation Cath PCI Registry. Disclosures. Objectives. Dashboard Implications of Some Major Metrics
 NCDR.13 Case Scenario Presentation Cath PCI Registry Dashboard Implications of Some Major Metrics Disclosures Tony Hermann has nothing to disclose Mark Hutcheson has nothing to disclose Cornelia Anderson
NCDR.13 Case Scenario Presentation Cath PCI Registry Dashboard Implications of Some Major Metrics Disclosures Tony Hermann has nothing to disclose Mark Hutcheson has nothing to disclose Cornelia Anderson
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Clinical Summary. Live Cases I - IX
 Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Clinical Summary Live Cases I - IX Patient: Male, 66 years Diagnosis: Single vessel CAD with normal LVEF Target lesion: proximal RCA Coronary risk factor: Hypertension, smoke (90py) Clinical course: ECG
Conflict Disclosures. Vermont Cardiac Network. Outline. Series Learning Objectives 4/27/2016. Scott E. Friedman April 28, 2016
 Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Conflict Disclosures Vermont Cardiac Network The Speaker has reported no significant financial relationship with any companies whose product may be germane to the content of their presentations or who
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand
 CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
CHRONIC HEART FAILURE : WHAT ELSE COULD WE OFFER TO OUR PATIENTS? Cardiac Rehabilitation Society of Thailand ENHANCED EXTERNAL COUNTER PULSATION Piyanuj Ruckpanich, MD. Cardiac Rehabilitation Center Perfect
Form 4: Coronary Evaluation
 Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one. Angio NOT DONE: n invasive test performed Followup
Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one. Angio NOT DONE: n invasive test performed Followup
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Ve V rmont rmon Card Car iac d Netw Ne ork tw Scott E. Friedman April 28, 2016
 Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Vermont Cardiac Network Scott E. Friedman April 28, 2016 Conflict Disclosures Th S k h d i ifi fi i l l i hi ih The Speaker has reported no significant financial relationship with any companies whose product
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome
 Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Surgical vs. Percutaneous Revascularization in Patients with Diabetes and Acute Coronary Syndrome Chris C. Cook, MD Associate Professor of Surgery Director, CT Residency Program, WVU ACOI 10/17/18 No Disclosures
Cardiac Care Network of Ontario
 Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Cardiac Care Network of Ontario Cardiac Wait Times Patient Triage Business Rules December 2016 TABLE OF CONTENTS 1. Introduction... 3 1.1. Document Purpose... 3 1.2. Document Structure... 3 2. Algorithms...
Disclosures. Stress Echocardiography 2010 Appropriate Use & Further Applications. Stress Echo Clinical Utility 9/8/10
 2010 & Further Applications Disclosures None Geoffrey A. Rose, MD FACC FASE Director, Cardiac Ultrasound Laboratory Sanger Heart & Vascular Institute Clinical Utility and Event-free Survival Cortigiani,
2010 & Further Applications Disclosures None Geoffrey A. Rose, MD FACC FASE Director, Cardiac Ultrasound Laboratory Sanger Heart & Vascular Institute Clinical Utility and Event-free Survival Cortigiani,
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
UPMCJAM XCCU CCU 10 PORTERFIELD, CAROL R COLEMAN MD, SILVIA E General
 UPMCJAM XCCU CCU 10 PORTERFIELD, CAROL R 784945341 COLEMAN MD, SILVIA E General Medicine 72 years 10/2/1945 Female 0210384908200 AROMATORIO Patient is admitted with acute anterior MI, DES stent LAD. Ejection
UPMCJAM XCCU CCU 10 PORTERFIELD, CAROL R 784945341 COLEMAN MD, SILVIA E General Medicine 72 years 10/2/1945 Female 0210384908200 AROMATORIO Patient is admitted with acute anterior MI, DES stent LAD. Ejection
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Stress Testing:Which Study is Indicated for My Patient?
 Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Stress Testing:Which Study is Indicated for My Patient? Cardiology-Primary Care Conference 7/14/17 Peter Casterella, MD Co-Executive Director Swedish Heart and Vascular Institute 1 Stress Testing Options
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease. Alexander (Sandy) Dick, MD
 Dick, MD") Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease Alexander (Sandy) Dick, MD Outline Pericardial Constriction Diagnosis: Imaging, Hemodynamics
Constrictive/Restrictive Cardiomyopathies: Diagnosis and Management Update; Radiation Induced Heart Disease Alexander (Sandy) Dick, MD Outline Pericardial Constriction Diagnosis: Imaging, Hemodynamics
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO
 AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
AS with reduced LV ejection fraction: Contractile reserve should be systematically assessed: PRO Jean-Luc MONIN, MD, PhD Henri Mondor University Hospital Créteil, FRANCE Potential conflicts of interest
Radiologic Assessment of Myocardial Viability
 November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
November 2001 Radiologic Assessment of Myocardial Viability Joshua Moss, Harvard Medical School Year III Patient EF 66yo female with a 3-year history of intermittent chest pain previously relieved by sublingual
Coronary interventions
 Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Controversial issues in the management of ischemic heart failure Coronary interventions Maciej Lesiak Department of Cardiology, University Hospital in Poznan none DECLARATION OF CONFLICT OF INTEREST CHF
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Form 4: Coronary Evaluation
 Patient Details Hidden Show Show/Hide Annotations Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one.
Patient Details Hidden Show Show/Hide Annotations Form : Coronary Evaluation Print this Form t Started Date of Coronary Evaluation Coronary Evaluation Indication for Coronary Evaluation Check only one.
Culprit vs Multivalve Transcatheter Intervention
 Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Culprit vs Multivalve Transcatheter Intervention Howard C. Herrmann, MD, FACC, MSCAI John Bryfogle Professor of Cardiovascular Medicine and Surgery Health System Director for Interventional Cardiology
Cardiology Cath Conference
 Cardiology Cath Conference David Stultz, MD Cardiology Fellow, PGY-6 February 14, 2006 Case #1 84 yo WM brought by squad this am for? syncope Pt reports Chest pain stuttering over several days. This am
Cardiology Cath Conference David Stultz, MD Cardiology Fellow, PGY-6 February 14, 2006 Case #1 84 yo WM brought by squad this am for? syncope Pt reports Chest pain stuttering over several days. This am
Cardiac Perioperative Risk Assessment American Heart Association Guidelines
 Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Cardiac Perioperative Risk Assessment American Heart Association Guidelines Dr Gary Liew, MBBS, PhD, FRACP US Board Certified in Cardiovascular CT Executive Committee, Cardiac Institute, Epworth Healthcare
Stable Angina: Indication for revascularization and best medical therapy
 Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Stable Angina: Indication for revascularization and best medical therapy Cardiology Basics and Updated Guideline 2018 Chang-Hwan Yoon, MD/PhD Cardiovascular Center, Department of Internal Medicine Bundang
Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization
 Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization + K Spargias, MD, PhD THV Director Hygeia Hospital Disclosures - Proctor
Patient with low-flow low-gradient aortic stenosis and ischemic cardiomyopathy TAVR and possibly percutaneous revascularization + K Spargias, MD, PhD THV Director Hygeia Hospital Disclosures - Proctor
History of Stress Testing. Disclosure. Overview. Stress Echocardiography New Applications. and Comparison with Other Stress.
 Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
Stress Echocardiography New Applications and Comparison with Other Stress Modalities Robert T. Palac, MD April 28, 2016 Overview Stress Testing Basics Stress Echocardiography and Stress Nuclear Perfusion
That unprotected LM: To STENT or NOT to STENT. Vasilios Papademetriou, MD Professor of Medicine Georgetown University
 That unprotected LM: To STENT or NOT to STENT Vasilios Papademetriou, MD Professor of Medicine Georgetown University Vasilios Papademetriou, MD I have no relevant financial relationships Patients are complicated
That unprotected LM: To STENT or NOT to STENT Vasilios Papademetriou, MD Professor of Medicine Georgetown University Vasilios Papademetriou, MD I have no relevant financial relationships Patients are complicated
Peripheral Arterial Disease Medical Approach and Management
 Peripheral Arterial Disease Medical Approach and Management April 2, 2016 Michael F. Hagerty, MD FACC PAD: Classic and New Concepts Let s take a look at what s new and what s old or classic in 2016. PAD:
Peripheral Arterial Disease Medical Approach and Management April 2, 2016 Michael F. Hagerty, MD FACC PAD: Classic and New Concepts Let s take a look at what s new and what s old or classic in 2016. PAD:
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis
 TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr..
 Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Patient: was admitted to the Cardiology Service at the from Y /M /D to Y / M / D under the care of Dr.. Discharge Diagnoses include: q CAD-CCS Class: m 0 m 1 m 2 m 3 m 4 q Unstable angina q Non STEMI (non-st
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
12 th Annual West Virginia ACC Meeting April 8, 2017
 12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
12 th Annual West Virginia ACC Meeting April 8, 2017 Rameez Sayyed, M.D., FACC, FSCAI Associate professor of Medicine Program Director for interventional cardiology Marshall University Joan C. Edwards
Richard Grocott Mason
 Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Richard Grocott Mason What to do with a 50 year old man with chest pain? Does the pain sound cardiac? Is this a possible acute coronary syndrome? Does patient have a previous cardiac history? Natural history
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium. Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute
 Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Cardiac Viability Testing A Clinical Perspective Annual Cardiac Imaging Symposium Lisa M Mielniczuk MD FRCPC University of Ottawa Heart Institute 62 year old male Anterior STEMI late presentation, occluded
Robotic & Hybrid Coronary Revascularization
 Robotic & Hybrid Coronary Revascularization Michael Chu, MD, FRCSC Associate Professor of Surgery Western University, London Health Sciences Centre, London, ON, Canada Saudi Heart Association 2017 Riyadh,
Robotic & Hybrid Coronary Revascularization Michael Chu, MD, FRCSC Associate Professor of Surgery Western University, London Health Sciences Centre, London, ON, Canada Saudi Heart Association 2017 Riyadh,
Revascularization Strategies in Patients with Severe LV Dysfunction
 Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
Revascularization Strategies in Patients with Severe LV Dysfunction Richard Lee, M.D., M.B.A. Saint Louis University The Center for Comprehensive Cardiovascular Care C4 Severe LV Dysfunction Defined as
Clinical Outcome in Patients with Aortic Stenosis
 Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Clinical Outcome in Patients with Aortic Stenosis Is the Prognosis Worse in Patients with Low-Gradient Severe Aortic Stenosis? Yoel Angel BSc, Shemy Carasso MD, Diab Mutlak MD, Jonathan Lessick MD Dsc,
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Assessment Of Myocardial Viability
 Assessment Of Myocardial Viability James K. Min, MD FACC President, Society of Cardiovascular Computed Tomography Associate Professor of Medicine, UCLA School of Medicine Associate Professor of Medicine
Assessment Of Myocardial Viability James K. Min, MD FACC President, Society of Cardiovascular Computed Tomography Associate Professor of Medicine, UCLA School of Medicine Associate Professor of Medicine
Chronic Primary Mitral Regurgitation
 Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Chronic Primary Mitral Regurgitation The Case For Early Surgical Intervention William K. Freeman, MD, FACC, FASE DISCLOSURES Relevant Financial Relationship(s) None Off Label Usage None Watchful Waiting......
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
STEMI ST Elevation Myocardial Infarction
 STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
STEMI ST Elevation Myocardial Infarction Breakout Session One Moderators: Quinn Capers IV, MD and Scott M. Lilly, MD, PhD Cases Presented by: Umair S. Ahmad, MD 1 Outline 1. Multivessel Revascularization
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO!
 Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Can Angiographic Complete Revascularization Improve Outcomes for Patients with Decreased LV Function? NO! Young-Hak Kim, MD, PhD Heart Institute, University of Ulsan College of Medicine Asan Medical Center,
Pearls & Pitfalls in nuclear cardiology
 Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Pearls & Pitfalls in nuclear cardiology Maythinee Chantadisai, MD., NM physician Division of Nuclear Medicine, Department of radiology, KCMH Principle of myocardial perfusion imaging (MPI) Radiotracer
Interventions in the Elderly
 Interventions in the Elderly Satya Reddy Atmakuri MD FIFTH ANNUAL SYMPOSIUM I Have No Financial Interest to Disclose People greater than 65 years of age will increase from 12% of population in 2000 to
Interventions in the Elderly Satya Reddy Atmakuri MD FIFTH ANNUAL SYMPOSIUM I Have No Financial Interest to Disclose People greater than 65 years of age will increase from 12% of population in 2000 to
Paris, August 28 th Gian Paolo Ussia on behalf of the CoreValve Italian Registry Investigators
 Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Paris, August 28 th 2011 Is TAVI the definitive treatment in high risk patients? Impact Of Coronary Artery Disease In Elderly Patients Undergoing TAVI: Insight The Italian CoreValve Registry Gian Paolo
Chronic Total Occlusion: A case for coronary artery bypass grafting
 Chronic Total Occlusion: A case for coronary artery bypass grafting Prof. Alfredo R Galassi MD, FESC, FACC, FSCAI Director of Cardiac Catheterization and Interventional Cardiology Unit Department of Medical
Chronic Total Occlusion: A case for coronary artery bypass grafting Prof. Alfredo R Galassi MD, FESC, FACC, FSCAI Director of Cardiac Catheterization and Interventional Cardiology Unit Department of Medical
Severe Aortic Stenosis in Elderly Patients: Surgical Versus Transcatheter Aortic Valve Replacement (TAVR)
") Severe Aortic Stenosis in Elderly Patients: Surgical Versus Transcatheter Aortic Valve Replacement (TAVR) James Dralle, MD Chief, Cardiothoracic Surgery AtlantiCare Regional Medical Center Transcatheter
Severe Aortic Stenosis in Elderly Patients: Surgical Versus Transcatheter Aortic Valve Replacement (TAVR) James Dralle, MD Chief, Cardiothoracic Surgery AtlantiCare Regional Medical Center Transcatheter
New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations
 Interactive Case Presentations") New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations Dr. Richard Bon Surrey Memorial Hospital, Surrey, BC Canadian Cardiovascular Congress 2014 October 26, 2014 Conflicts
New Concepts in Acute Coronary Syndromes Beyond 2000 (XX) Interactive Case Presentations Dr. Richard Bon Surrey Memorial Hospital, Surrey, BC Canadian Cardiovascular Congress 2014 October 26, 2014 Conflicts