Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
|
|
|
- Rosamund Roberts
- 6 years ago
- Views:
Transcription
1 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
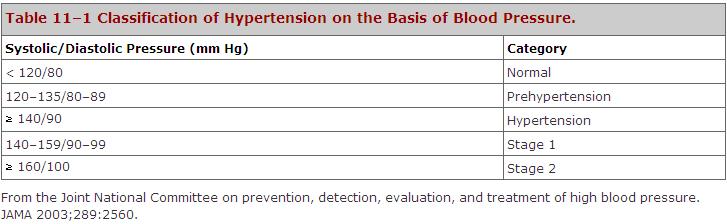
2 Antihypertensive Drugs What is Hypertension: A common, incurable, persistent, but usually asymptomatic disease whose treatment provides no obvious benefit.
3 Introduction Thirty percent of people with high blood pressure don t know they have it. Of all people with high blood pressure, 11 percent aren t on therapy (special diet or drugs), 25 percent are on inadequate therapy, and 34 percent are on adequate therapy. 3

4 Average 14 readings: two per session, taken morning and Nov-14 evening for 7 days. Munir Gharaibeh MD, PhD, MHPE 4
5 BP variations Increased BP variability is associated with increased organ damage and cardiovascular morbidity. White Coat or isolated office hypertension. Masked hypertension. Morning surge of BP. During Sleep: Non dipping and extreme dipping. 5
6 6
7 7
8 8
9 Benefits of Lowering BP Antihypertensive therapy has been associated with: 35% to 40% mean reduction in stroke incidence. 20% to 25% reduction in myocardial infarction. More than 50% reduction in HF. 9
10 10
11 Non-pharmacologic Treatment Lifestyle Modifications: Weight reduction Diet rich in potassium and calcium and sodium reduction. Dietary Approaches to Stop Hypertension (DASH) eating plan( 1600-mg sodium) has effects similar to single drug therapy. Physical activity. 11
12 Goals of Therapy Maximal protection against cardiovascular consequences with minimal bother to the patient. Stroke, coronary, and renal complications increase when BP is vigorously lowered (Why?) 12
13 Sites of action of antihypertensive drugs. 13

14 Sites of action of antihypertensive drugs. 14
15 15
16 Hemodynamic Effects of Antihypertensive Drugs 16
17 17
18 Diuretics (Saluretics) Widely recommended as first-line therapy, especially in the elderly, the obese, and black patients. Better at reducing coronary heart disease, HF, stroke, and mortality. Inexpensive. Combine well with others. Lower doses, with sodium restriction, cause fewer metabolic side effects, but retain antihypertensive activity. All have same efficacy in lowering BP, although not same diuretic activity. 18
19 Diuretics (Saluretics) Early Effects (3-4 days): Diuresis lowers blood volume and cardiac output. Mainly affects the systolic BP. Late Effects (3-4 weeks): Decreased Na+ & Cl-, lowers blood vessel contractility. Appear even with low doses. Increase Plasma Renin Side Effects: 19
20 Diuretics (Saluretics) Thiazide diuretics: Effective in mild and moderate Ht with normal renal and heart function. Hydrochlorthiazide. Chlorthalidone: long acting. Bendrofluazide. Indapamide: vasodilating and lipid neutral. Also induces regression of LVH 20
21 Diuretics (Saluretics) Loop Diuretics: Needed in severe Ht, in renal insufficiency, and in heart failure or cirrhosis. Furosemide: not ideal, short acting. Torsemide: free of metabolic side effects. Potassium- sparing diuretics: Useful in heart failure. Spironolactone: Eplerenone. Ameloride. Nov-14 Triamterene Munir Gharaibeh MD, PhD, MHPE 21
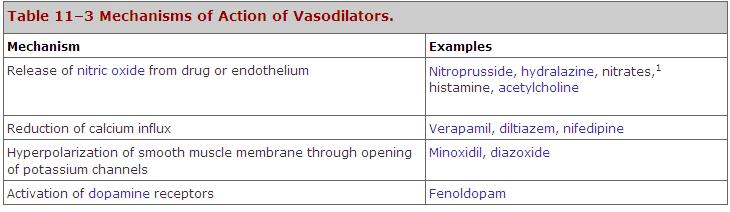
22 VASODILATORS Work directly on arterial blood vessels, or veins(organic nitrates and nitroprusside). Actions not antagonized by known blockers. Reduce peripheral resistance, which will elicit compensatory mechanisms leading to tolerance, resistance or pseudoresistance. Usually other drugs are combined with vasodilators to avoid this problem. 22
23 Compensatory responses to vasodilators 23
24 24
25 VASODILATORS Hydralazine: Oldest vasodilator(1950s), was withdrawn and then came back. Arteriolar dilator, works by release of NO. Tachyphylaxis (Tolerance or Peusdoresistance). Activates baroreceptor reflex. Metabolized by acetylation. Drug-induced lupus syndrome. Other side effects. Replaced by CCBs. Used in heart failure, combined with isosorbide dinitrate 25
26 Diazoxide: VASODILATORS Thiazide derivative, but not a diuretic. Potent arterial dilator, works by opening potassium channels. Causes excessive hypotension. Used in emergencies by rapid I.V. bolus injection. Rapidly bound to albumin. Onset seconds. Duration 2-4 hours. Does not require constant monitoring. 26
27 VASODILATORS Sodium Nitroprusside: Cyanide-containing molecule. Useful in emergencies, surgery and heart failure. Relaxes both arterial and venous smooth muscle, works by release of NO. No excessive reflex increase in cardiac output. Might increase C.O. if there is failure. 27
28 VASODILATORS Sodium Nitroprusside: Short half life. Action is immediate, requires constant monitoring in ICU. Drug is light sensitive. Thiocyanate levels and acid-base balance: weakness, nausea, tinnitus, flushing, lactic acidosis and anoxia. 28
29 29
30 Minoxidil: VASODILATORS K+ channel-opener: increases efflux leading to hyperpolarization. Prolonged arterial relaxation. Superior to hydralazine. For severe intractable hypertension, or renal insufficiency, usually in combination with a diuretic and β blocker. Hypertrichosis, so useful for baldness. Pericarditis. Nov Munir Gharaibeh MD, PhD, MHPE
31 Fenoldopam: VASODILATORS Dopamine D1 agonist, which results in vasodilation, renal vessel dilation, and natriuresis. Rapidly metabolized, short acting. Used by continuous infusion in emergencies or postoperatively. 31
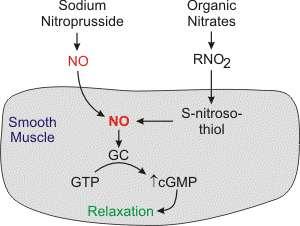
32 Calcium Channel Blockers More effective than others in protection against stroke. Primarily act to reduce PVR, aided by at least an initial diuretic effect, especially with the short-acting DHPs. Effective in the elderly. Equally effective in blacks and nonblacks. Cause no metabolic disturbances 32
33 33
34 Calcium Channel Blockers PVR HR CO Nifedipine (Reflexly) Diltiazem Verapamil
35 Angiotensin - Converting Enzyme Inhibitors (ACEI) Angiotensin II: Potent vasoconstrictor by itself. Facilitates release of NE. Central actions to increase BP. Promotes release of aldosterone. Regulates tubular function. Regulates intra-renal blood flow. 35
36 Angiotensin - Converting Enzyme Inhibitors (ACEI) Inhibit ACE in the lungs. Also inhibit kinin metabolism. 36

37 Sites of action of drugs that interfere with the renin-angiotensin-aldosterone system. 37
38 Angiotensin - Converting Enzyme Inhibitors (ACEI) Captopril Prototype. Enalapril Quinapril Lisinopril. Benazepril Fosonopril All are similarly effective 38 Might differ in toxicity
39 Angiotensin - Converting Enzyme Inhibitors (ACEI) Therapeutic Benefits: Effective in high-rennin hypertension (20%), HF and Ischemic Heart Disease. Do not increase HR. Useful in diabetic nephropathy by dilating efferent arterioles thus reducing intraglomerular pressure and consequently protects against progressive glomerulosclerosis. No need for a diuretic but can be added. Can be combined with CCBs. Should not be combined with Beta blockers. No metabolic effects. * Contraindicated in pregnancy and bilateral renal artery stenosis. Nov Munir Gharaibeh MD, PhD, MHPE
40 Angiotensin - Converting Enzyme Inhibitors (ACEI) Side Effects: Captopril is SH containing drug, so very toxic( bone marrow suppression, disguesia, proteinuria, allergic skin rash, fever) Hypotension( First Dose Phenomena) especially with renovascular hypertension. K+ retention, especially in the presence of renal dysfunction or when combined with K+ sparing diuretics or ARBs. Cough(10% of patients). Angioedema. Nov Munir Gharaibeh MD, PhD, MHPE
41 Angiotensin II Receptor Blockers (AT-1) Result in more complete inhibition of angiotensin actions (Chymase?) with no effects on bradykinins. May be only indicated when ACEI are intolerable. Most expensive, but fastest growing class of antihypertensive drugs. Free of side effects, especially cough. May be better than ACEI in protection against stroke (activation of AT-2 receptor facilitates collateral vessels and neuronal resistance). 41
42 Angiotensin II Receptor Blockers Losartan. Valsartan. Candesartan. Irbesartan. (AT-1) Telmisartan ( additional peroxisome proliferator- activated receptor-g agonist activity). Eprosartan. 42
43 Renin Enzyme Inhibitors Aliskiren. 43
44 Sympatholytics or Adrenergic Blockers Alpha Adrenergic Antagonist Non selective Antagonists 1 -Selective Antagonists. Beta Adrenergic Blockers Adrenergic Neurone Blockers. Ganglionic Blockers 44
45 Non selective Alpha Adrenergic Antagonist Phentolamine Phenoxybenzamine Block both 1 and 2 receptors, so cause reflex tachycardia and increased contractility. Used only for pheochromocytoma. 45
46 1 -selective Alpha Adrenergic Antagonists Prazosin Terazocin Doxazosin First - Dose Phenomenon. All are free of metabolic effects, but can cause drowsiness, diarrhea, postural hypotension, tachycardia, and tolerance due to fluid retention. Effective in moderate hypertension as well as benign prostatic hypertrophy. Munir Gharaibeh MD, PhD, MHPE 46
47 Beta Adrenergic Blockers Antihypertensive Mechanisms: 1. Decrease HR, SV, and consequently C.O. 2. Decrease Rennin Release 3. Central Action 4. Inhibit NE release 47
48 Beta Adrenergic Blockers Preparations: 30 Propranolol: Prototype,1957 Timolol Lipophilic Nadolol Long acting Pindolol ISA Acebutelol ISA Esmolol Short half life Metoprolol β1 selective Atenolol β1 selective. Betaxolol β1 selective. Bisoprolol β1 selective. 48
49 Beta Adrenergic Blockers Therapeutic Effectiveness: Effect not immediate. High - rennin hypertension Combination or monotherapy Hyperkinetic hearts Used in other cardiovascular conditions Ineffective in blacks No postural hypotension 49
50 Beta Adrenergic Blockers Side Effects: Bronchospasm, especially with the non selective Heart Failure? CNS: fatigue, depression, impotence..etc Impair lipid and glucose metabolism Masked hypoglycemia!!! Claudication Withdrawal Syndrome 50
51 Vasodilating Beta Adrenergic Blockers Labetalol:, 1 (20% of ) antagonist & 2 partial agonist. Useful for pheochromocytoma and emergencies. Carvedilol:, 1 (10% of ) antagonist. Esmolol: 1 selective, rapidly metabolized. Used by continuous IV infusion. Nebivolol 51
52 Adrenergic Neurone Blockers Guanethidine Bethanedine Debrisoquin Guanadrel Hydrophilic. Uptake 1. Block NE release. Displace NE from vesicles MAO. Cause depletion of NE. 52

53 Life Cycle of Norepinephrine 53
54 Adrenergic Neurone Blockers Reserpine (Rauwolfia Alkaloids): Lipophilic Binds to the sympathetic vesicles. Prevents DA uptake into vesicles. Amines are metabolized by MAO. Depletes: NE, 5HT, ACTH, DA. Old fashioned, slow onset and offset, very cheap. 54
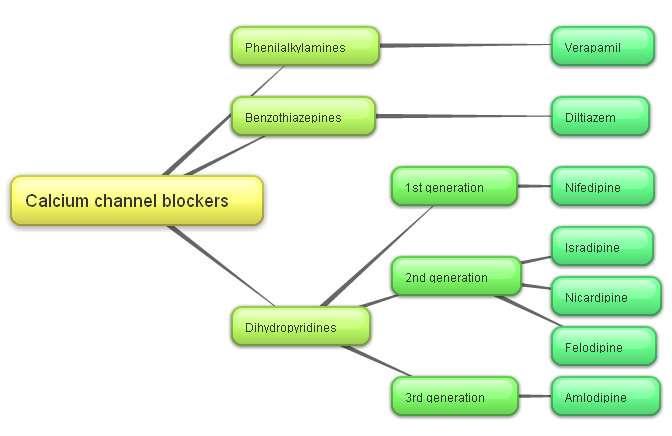
55 Ganglionic Blockers Trimethaphan Pentolinium Mecamylamine Block transmission in both symp & parasypathetic systems. Act immediately and are very efficacious. Effect rapidly reversed, so used for short term control of BP, e.g. intraoperatively or emergency. 55 Many side effects.
56 56
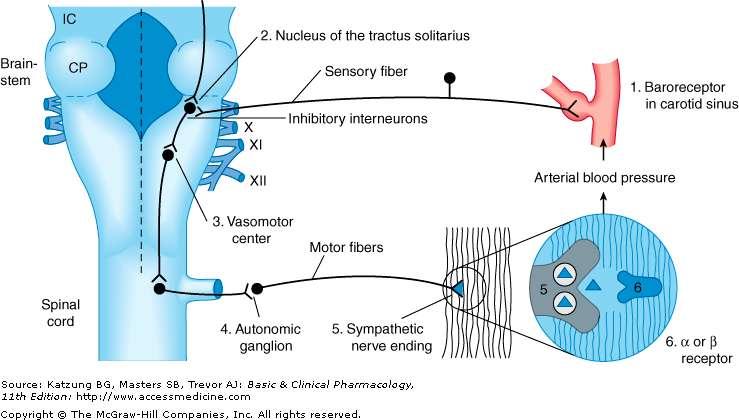
57 Centrally Acting Antihypertensive Drugs Vasomotor Center: Receptor activation decreases BP Receptor activation increases BP Nucleus Tractus Solitarius Nucleus Ambiguus Rostral Ventral Medulla 57

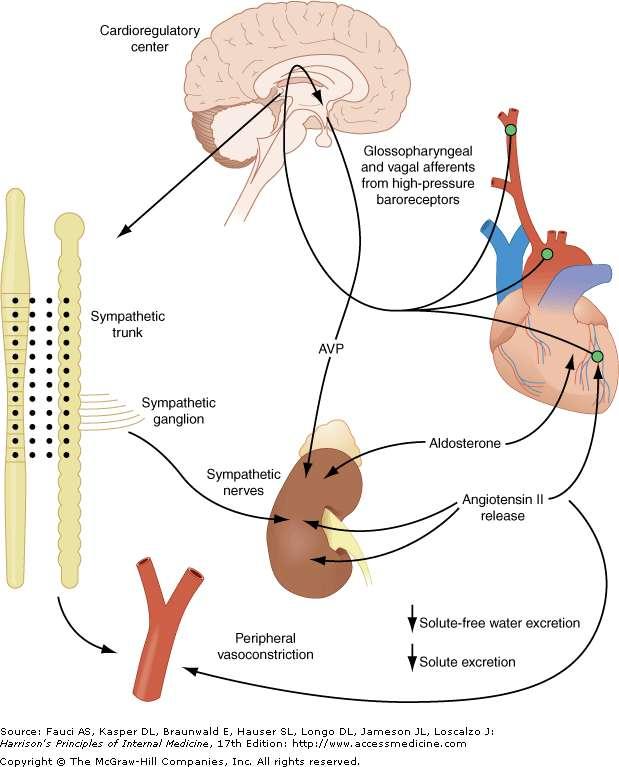
58 Autonomic and hormonal control of cardiovascular function 58
59 Centrally Acting Antihypertensive Drugs Common Properties: Cross BBB. Reduce preganglionic sympathetic activity. Orthostasis is unusual, due to preservation of peripheral sympathetic activity. CNS side effects. 59
60 Centrally Acting Antihypertensive Drugs 1. Propranolol 2. Reserpine Methyl Dopa: Old drug, thought to work by forming a pseudo transmitter which works peripherally. Central agonist. MD MDA MNE. Lowers BP but not CO or renal blood flow. Can cause lactation and positive Coomb s test. Safe in pregnancy. 60
61 Centrally Acting Antihypertensive Drugs 4. Clonidine: Imidazoline derivative, tried initially as a nasal decongestant. Central agonist. I.V: Biphasic Effect: peripheral then central actions. Oral. Transdermal Patch(7 days). 61

62 Step Therapy of Hypertension 62
63 Causes of Resistant Hypertension Improper blood pressure measurement, White Coat Hypertension. Noncompliance. Psychological stresses, secondary hypertension, sleep disorders Volume overload and pseudotolerance. Excess sodium intake Volume retention from kidney disease. Inadequate diuretic therapy. Nov Munir Gharaibeh MD, PhD, MHPE
64 Causes of Resistant Hypertension Inadequate doses. Inappropriate combinations. NSAID; cyclooxygenase 2 inhibitors. Cocaine, amphetamines, other illicit drugs. Sympathomimetics, e.g. decongestants, anorectics 64
65 Causes of Resistant Hypertension Oral contraceptives Adrenal steroids Cyclosporine Erythropoietin Licorice (including some chewing tobacco). Excess alcohol intake. 65
66 66
Antihypertensive Drugs. Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017
 Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Antihypertensive Drugs Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan October, 2017 Antihypertensive Drugs What is Hypertension? A common, incurable, persistent, but usually
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Antihypertensive Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Antihypertensive Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Agents that block production or action of angiotensin Angiotensin-converting
Beta 1 Beta blockers A - Propranolol,
 Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Pharma Lecture 3 Beta blockers that we are most interested in are the ones that target Beta 1 receptors. Beta blockers A - Propranolol, it s a non-selective competitive antagonist of beta 1 and beta 2
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
sympatholytics sympatholytics sympatholytics
 sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
sympatholytics sympatholytics sympatholytics CNS-ACTING SYMPATHOPLEGICS Sympathetic brain signals Doesn t affect baroreceptor reflex (no orthostatic hypotension) Methyldopa α-methylne crosses BBB (+) α-adrenoreceptors
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents
 Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Antihypertensive Agents Öner Süzer www.onersuzer.com osuzer@istanbul.edu.tr Last update: 13.11.2009 1 Süzer Farmakoloji 3. Baskı 2005 2 1 Süzer Farmakoloji 3. Baskı 2005 3 Süzer Farmakoloji 3. Baskı 2005
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Chapter 23. Media Directory. Cardiovascular Disease (CVD) Hypertension: Classified into Three Categories
 Hypertension: Classified into Three Categories") Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Chapter 23 Drugs for Hypertension Slide 37 Slide 41 Media Directory Nifedipine Animation Doxazosin Animation Upper Saddle River, New Jersey 07458 All rights reserved. Cardiovascular Disease (CVD) Includes
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
HYPERTENSION: Sustained elevation of arterial blood pressure above normal o Systolic 140 mm Hg and/or o Diastolic 90 mm Hg
 Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Lecture 39 Anti-Hypertensives B-Rod BLOOD PRESSURE: Systolic / Diastolic NORMAL: 120/80 Systolic = measure of pressure as heart is beating Diastolic = measure of pressure while heart is at rest between
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
ANTIHYPERTENSIVE DRUGS
 ANTIHYPERTENSIVE DRUGS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: September 28, 2010 Materials on: Exam #3 Required reading: Katzung, Chapter 11 1 1 in 3 adults HYPERTENSION 64% of
ANTIHYPERTENSIVE DRUGS Course: Integrated Therapeutics 1 Lecturer: Dr. E. Konorev Date: September 28, 2010 Materials on: Exam #3 Required reading: Katzung, Chapter 11 1 1 in 3 adults HYPERTENSION 64% of
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias
 1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
1. Antihypertensive agents 2. Vasodilators & treatment of angina 3. Drugs used in heart failure 4. Drugs used in arrhythmias Only need to know drugs discussed in class At the end of this section you should
Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Introduction. Factors affecting blood pressure: 1-COP = HR X SV mainly affect SBP. 2-TPR = diameter of arterioles X viscosity of blood affect DBP
 Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Introduction Hypertension is a persistent elevation of blood pressure above 140 / 90 mmhg for more than three sitting. (0ptimal level
Antihypertensive Agents
 1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
1. Blood Pressure Regulation Antihypertensive Agents - 2007 Edward JN Ishac. Ph.D. Associate Professor, Dept. Pharmacology & Toxicology Office: Smith 742; Tel: 828 2127 eishac@hsc.vcu.edu Frank's formula,
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI
 DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
DRUGS USED TO TREAT HYPERTENSION BY ALI ALALAWI 3. Vasodilators Drugs which dilate blood vessels ( decrease peripheral vascular resistance) by acting on smooth muscle cells through non-autonomic mechanisms:
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D
 University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
University of Al Qadisiyah College of Pharmacy Dr. Bassim I Mohammad, MBChB, MSc, Ph.D Cardiovascular Pharmacology 1. Antihypertensives 2. Antianginal 3. Drugs for HF 4. Antiarrythemics 5. Drugs for Hyperlipoproteniemia
ANTIHYPERTENSIVE AGENTS AND VASODILATORS. Lecture 5
 ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
ANTIHYPERTENSIVE AGENTS AND VASODILATORS Lecture 5 Hypertension Blood pressure BP = CO x PVR n Interaction between autonomic nervous system, cardiovascular system and renal system Normal: 110/70 Prehypertension
ANTIHYPERTENSIVES. Assoc. Prof. Bilgen Başgut
 ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
ANTIHYPERTENSIVES Assoc. Prof. Bilgen Başgut Hypertension Hypertension is a condition in which the blood pressure is persistently higher than normal Hypertension > 140 mmhg > 90 mmhg Systolic Blood Pressure
Treatment of Essential Hypertension
 2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
2016 edition by Mark A. Simmons, PhD Department of Pharmaceutical Sciences School of Pharmacy University of Maryland Eastern Shore Originally developed by Hugh J. Burford, PhD, FCP Department of Pharmacology
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Categories of HTN. Overview of Hypertension. Types of Hypertension
 Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
Categories of HTN Overview of Hypertension Normal SBP 100 Quick review of the Basics: What is
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
New classification of HT Systolic Diastolic Normal <120 <80 Prehypertension Stage1HT Stage 2 HT >160 or >100
 Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
Hypertension 1 Definition Hypertension can be defined as a condition where blood pressure is elevated to an extent that clinical benefit is obtained from blood pressure lowering. it is an important risk
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
Pharmacology of the Sympathetic Nervous System II
 Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Heart failure. Failure? blood supply insufficient for body needs. CHF = congestive heart failure. increased blood volume, interstitial fluid
 Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Failure? blood supply insufficient for body needs CHF = congestive heart failure increased blood volume, interstitial fluid Underlying causes/risk factors Ischemic heart disease (CAD) 70% hypertension
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Chapter 2 ~ Cardiovascular system
 Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Dr. Vishaal Bhat. anti-adrenergic drugs
 Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ASEBP and ARTA TARP Drugs and Reference Price by Categories
 ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
ASEBP Pantoprazole Sodium 40 mg (generic) $0.2016 ASEBP Dexlansoprazole 30 mg Dexlansoprazole 60 mg Esomeprazole 10 mg Esomeprazole 20 mg Esomeprazole 40 mg Lansoprazole 15 mg Lansoprazole 30 mg Omeprazole
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Prof dr Aleksandar Raskovic DIRECT VASODILATORS
 Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Prof dr Aleksandar Raskovic DIRECT VASODILATORS Direct vasodilators Minoxidil (one of the most powerful peripheral arterial dilators) Opening of KATP channels, efflux of K, lose of Ca and smooth muscle
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
8/20/2018. Objectives. What is hypertension? cont. What is hypertension? Epidemiology cont. Epidemiology
 Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Objectives Hypertension (high blood pressure): Clinical Pearls for the Pharmacy Technician Tanya Schmidt PharmD, RPh Director of Central Operations at Thrifty White Pharmacy North Dakota Board of Pharmacy
Drug Therapy of Heart Failure. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014
 Drug Therapy of Heart Failure Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Drug Therapy of Heart Failure Definition of Heart Failure Causes Classifications
Drug Therapy of Heart Failure Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Drug Therapy of Heart Failure Definition of Heart Failure Causes Classifications
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood:
 Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
Towards a Greater Understanding of Cardiac Medications Foundational Cardiac Concepts That Must Be Understood: Cardiac Output (CO) CO=SVxHR (stroke volume x heart rate) Cardiac output: The amount of blood
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC
 DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
DROGAS PARA HIPERTENSION ARTERIAL JONATHAN POVEDA FERNANDEZ HSJD / 2013 FACC/FSCAI/FESC Pharmacotherapy of HTN Rationale for reducing arterial pressure Reduce cardiac output Reduce heart rate Reduce stroke
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
How to Manage Resistant Hypertension Min Su Hyon, MD
 How to Manage Resistant Hypertension Min Su Hyon, MD Cardiovascular Medicine, Internal Medicine Soonchunhyang University College of Medicine Definition Resistant to conventional medical therapy Definition
How to Manage Resistant Hypertension Min Su Hyon, MD Cardiovascular Medicine, Internal Medicine Soonchunhyang University College of Medicine Definition Resistant to conventional medical therapy Definition
Heart Failure. Dr. Alia Shatanawi
 Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Heart Failure Dr. Alia Shatanawi Left systolic dysfunction secondary to coronary artery disease is the most common cause, account to 70% of all cases. Heart Failure Heart is unable to pump sufficient blood
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
LESSON ASSIGNMENT. After completing this lesson you will be able to:
 LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
LESSON ASSIGNMENT SUBCOURSE MD0806 LESSON 7 Therapeutics III. Antihypertensive Agents. LESSON ASSIGNMENT Paragraphs 7-1--7-12. LESSON OBJECTIVES After completing this lesson you will be able to: 7-1. From
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide
 Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
Lab Period: Name: Physiology Chapter 14 Blood Flow and Blood Pressure, Plus Fun Review Study Guide Main Idea: The function of the circulatory system is to maintain adequate blood flow to all tissues. Clinical
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
Drug Treatment of Ischemic Heart Disease
 Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine, The University of Jordan November, 2014 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Drug Treatment of Ischemic Heart Disease
 Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan November, 2017 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
Drug Treatment of Ischemic Heart Disease Munir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan November, 2017 Categories of Ischemic Heart Disease Fixed "Stable, Effort Angina Variant
BIMM118. Autonomic Nervous System
 Autonomic Nervous System Autonomic Nervous System Ganglia close to the innervated organs Myelinated axons Ganglia close to the spinal column Preganglionic axons are myelinated; postganglionic axons are
Autonomic Nervous System Autonomic Nervous System Ganglia close to the innervated organs Myelinated axons Ganglia close to the spinal column Preganglionic axons are myelinated; postganglionic axons are
Antihypertensive Drugs. Nafrialdi
 Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Antihypertensive Drugs Nafrialdi 1 Mechanisms of Blood Pressure Regulation Blood Presure Cardiac Output Peripheral Resistance Heart Rate Stroke volume Vascular tone Vessel elasticity Myocardial contractility
Cardiovascular Pharmacotherapy
 Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Cardiovascular Pharmacotherapy Overview Mechanism of cardiovascular drugs Indications and clinical use in cardiology Renin-Angiotensin Inhibitors: Angiotensin-Converting Enzyme Inhibitors, Angiotensin
Hypertension. Antihypertensive Agents
 Hypertension and Antihypertensive Agents Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 8-2127 8-2126 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia
Hypertension and Antihypertensive Agents Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 8-2127 8-2126 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Therefore MAP=CO x TPR = HR x SV x TPR
 Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Regulation of MAP Flow = pressure gradient resistance CO = MAP TPR Therefore MAP=CO x TPR = HR x SV x TPR TPR is the total peripheral resistance: this is the combined resistance of all blood vessels (remember
Adrenergic Receptor Antagonists
 Adrenergic Receptor Antagonists α-adrenergic Receptor Antagonists Unlike the β-adrenergic receptor antagonists, which bear clear structural similarities to the adrenergic agonists E, epinephrine, and isoproterenol,
Adrenergic Receptor Antagonists α-adrenergic Receptor Antagonists Unlike the β-adrenergic receptor antagonists, which bear clear structural similarities to the adrenergic agonists E, epinephrine, and isoproterenol,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Factors Involved in Poor Control of Risk Factors
 Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
Factors Involved in Poor Control of Risk Factors Patient compliance Clinical inertia Health Care System structure 14781 M Limitations of Formal Studies Selection of patients Recruitment and follow-up alter
12.5mg, 25mg, 50mg. 25mg, 50mg. 2.5mg, 5mg, 10mg. 5mg, 10mg, 20mg, 100mg. 25mg. -- $2.81 Acetazolamide (IR, 125mg, 250mg, 500mg (ER)
") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 9/15, 2/13, 2/08, 5/07 LOB
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Blood Pressure P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular Disorders REVIEW HISTORY: 9/15, 2/13, 2/08, 5/07 LOB
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Drugs Used in Heart Failure. Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia
 Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to
Drugs Used in Heart Failure Assistant Prof. Dr. Najlaa Saadi PhD pharmacology Faculty of Pharmacy University of Philadelphia Heart Failure Heart failure (HF), occurs when cardiac output is inadequate to