6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
|
|
|
- Jasmine Sparks
- 6 years ago
- Views:
Transcription




1 Novas diretrizes da Surviving Sepsis Campaign
2 2012 o que foi atualizado?
3
4 Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores Controle glicêmico i Otimização de PVC Pressão de platô < 30 cmh 2 O Otimização de SvO 2
5 Os pacotes da sepse 3-horas Coleta de lactato Hemoculturas Antibióticos Fluidos 6 horas Vasopressores Mensuração de PVC Mensuração de SvO 2 Alvos são PVC > 8 mmhg, SvcO2 > 700% e normalização do lactato
6 Screening for sepsis and performance improvement We recommend routine screening of potentially infected seriously ill patients for severe sepsis to increase the early identification of sepsis and allow implementation of early evidence-based sepsis therapy (1C). STRONG RECOMMENDATION New!!! Performance improvement efforts in severe sepsis should be used to improve patient outcomes (UG).
7
8 Diagnosis We recommend obtaining appropriate cultures before antimicrobial therapy is initiated if such cultures do not cause significant delay (> 45 minutes) in the start of antimicrobial(s) administration (grade 1C). STRONG RECOMMENDATION O
9 Diagnosis We suggest the use of the 1,3 β-d-glucan assay (grade 2B), mannan and anti-mannan antibody assays (grade 2C) when invasive candidiasis is in the differential diagnosis of infection. WEAK RECOMMENDATION O
10
11 Antimicrobial therapy The administration of effective intravenous antimicrobials within the first hour of recognition of septic shock (grade 1B) and severe sepsis without septic shock (grade 1C) should be the goal of therapy. STRONG RECOMMENDATION Reworded


12 Coorte N= 261



13 Subanálise de Jones et al N = centros

14 Subanálise de Jones et al N = centros
15 Antimicrobial therapy We recommend that initial empiric anti-infective therapy include one or more drugs that have activity against all likely pathogens (bacterial and/or fungal or viral) and that penetrate in adequate concentrations ce o into the tissues presumed ed to be the source of sepsis (grade 1B). STRONG RECOMMENDATION Reworded
16 Antimicrobial therapy 2c. Given the high risk of mortality from sepsis, empiric therapy should cover all the likely pathogens based on the clinical circumstances and local susceptibility patterns. In light of the increasing frequency of resistance sta to antimicrobial a agents in many parts of the world, such broad-spectrum coverage generally requires initial use of combinations of antimicrobial agents (grade 2B). WEAK RECOMMENDATION New!!!
17
18
19 Antimicrobial therapy 2d. We suggest combination empirical therapy for neutropenic patients with severe sepsis (2B) and for patients with difficult to treat, multidrug- resistant bacterial pathogens such as Acinetobacter and Pseudomonas spp. (grade 2B). WEAK RECOMMENDATION Changed from 2D to 2B For selected patients with severe infections associated with respiratory failure and septic shock, combination therapy with an extended spectrum beta-lactam and either an aminoglycoside or a fluoroquinolone is suggested for P. aeruginosa bacteremia (grade 2B). Similarly, a more complex combination of beta-lactam and a macrolide is suggested for patients with septic shock from bacteremic Streptococcus pneumoniae infections (grade 2B). STRONG RECOMMENDATION New!!!
20
21
22 Antimicrobial therapy We suggest that combination therapy, when used empirically in patients with severe sepsis, should not be administered for longer than 3 to 5 days. De-escalation to the most appropriate single-agent therapy should be performed as soon as the susceptibility profile is known (grade 2B). Exceptions would include aminoglycoside monotherapy, which should be generally avoided, particularly for P. aeruginosa sepsis, and for selected forms of endocarditis, where prolonged courses of combinations of antibiotics are warranted. WEAK RECOMMENDATION New!!!
23 Antimicrobial therapy We suggest that the duration of therapy typically be 7 to 10 days if clinically indicated; longer courses may be appropriate in patients who have a slow clinical response, undrainable foci of infection, bacteremia with S. aureus; some fungal and viral infections, or immunologic deficiencies, including neutropenia (grade 2C). WEAK RECOMMENDATION
24 Antimicrobial therapy We suggest the use of low procalcitonin levels or similar biomarkers to assist the clinician in the discontinuation of empiric antibiotics in patients who appeared septic, but have no subsequent evidence of infection (grade 2C) WEAK RECOMMENDATION New!!!
25 Antimicrobial therapy We suggest thatt antiviral i therapy be initiatediti t as early as possible in patients with severe sepsis or septic shock of viral origin, when available, such as for severe influenza infection (2C). New!!! WEAK RECOMMENDATION
26 Infection prevention We suggest that SOD and SDD should be introduced and investigated as a method to reduce the incidence of ventilatorassociated pneumonia; this infection control measure can then in instituted in health care settings in regions where this methodology has been found to be effective (2B). New!!! We suggest oral CHG be used as a form of oropharyngeal decontamination to reduce the risk of ventilator-associated pneumonia in ICU patients with severe sepsis (2B) WEAK RECOMMENDATIONS New!!!
27 Initial resuscitation We recommend the protocolized, quantitative resuscitation of a patient with sepsis-induced shock, defined as tissue hypoperfusion (hypotension persisting after initialiti fluid challenge or blood lactate t concentration 4 mmol/l). During the first 6 hrs of resuscitation, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as one part of a treatment protocol: Central venous pressure 8 12 mm Hg Mean arterial pressure (MAP) 65 mm Hg Urine output 0.5 ml kg-1 hr-1 Central venous (superior vena cava) or mixed venous oxygen saturation 70% or 65%, respectively. STRONG RECOMMENDATION
28 N = ,6 para 78 por
 vs 2.9 (-2.3, -3,5) p-= 0.")
29 Redução de mortalidade: (-3.2, - 4.2) vs 2.9 (-2.3, -3,5) p-= 0.016
30 Initial resuscitation We suggest targeting resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion (grade 2C). WEAK RECOMMENDATION New!!!
31


32 Near future answers??? N=1600 N=1260 N=1935
33 Fluid therapy 1. We recommend crystalloids be used as the initial fluid of choice in the resuscitation of severe sepsis and septic shock (Grade 1B). New!!! STRONG RECOMMENDATION 2. We recommend against the use of hydroxyethyl ethyl starches for fluid resuscitation of severe sepsis and septic shock. (Grade 1B). STRONG RECOMMENDATION New!!! 3. We suggest the use of albumin in the fluid resuscitation of severe sepsis and septic shock when patients require substantial ti amounts of crystalloids (Grade 2C). New!!! WEAK RECOMMENDATION
34 Albumin in sepsis
35 Albumin in sepsis
36
37 N=196
38
39
40
41 Fluid therapy 6. We recommend an initial fluid challenge in patients with sepsis-induced tissue hypoperfusion with suspicion of hypovolemia to achieve a minimum of 30 ml/kg of crystalloids (a portion of this may be albumin equivalent.). More rapid administration and greater amounts of fluid may be needed in some patients (see Initial Resuscitation recommendations) (grade 1C). STRONG RECOMMENDATIONS Slight changed 7. We recommend that a fluid challenge technique be applied wherein fluid administration is continued as long as there is hemodynamic improvement either based on dynamic (eg, change in pulse pressure, stroke volume variation) or static (eg, arterial pressure, heart rate) variables continues (UG). New!!!
42 Vasopressors We recommend norepinephrine as the first choice vasopressor (Grade 1B) STRONG RECOMMENDATION New!!! We suggest epinephrine p (added to and potentially substituted for norepinephrine) when an additional agent is needed to maintain adequate blood pressure (Grade 2B). STRONG RECOMMENDATION
43 Vasopressors Vasopressin (up to 0.03 U/min) can be added to norepinephrine with the intent of raising MAP to target or decreasing norepinephrine dosage (UG). Low-dose vasopressin is not recommended as the single initial vasopressor for treatment of sepsis-induced hypotension, and vasopressin doses higher than U/min should be reserved for salvage therapy (failure to achieve an adequate MAP with other vasopressor agents) (UG). UNGRADED RECOMMENDATION New!!!
44 Vasopressors We suggest dopamine as an alternative vasopressor agent to norepinephrine only in highly selected patients (eg, patients with low risk of tachyarrhythmias and absolute or relative bradycardia) (grade 2C). WEAK RECOMMENDATION New!!! Phenylephrine is not recommended in the treatment of septic shock except in the following circumstances: (a) norepinephrine is associated with serious arrhythmias, (b) cardiac output is known to be high and blood pressure persistently low, or (c) as salvage therapy when combined inotrope/ vasopressor drugs and low-dose vasopressin have failed to achieve the MAP target (grade 1C). STRONG RECOMMENDATION New!!!
45
46
47 Corticosteroides 1. We suggest not using intravenous hydrocortisone in adult septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore hemodynamic stability (see recommendations for initial resuscitation). In case this is not achievable, we suggest intravenous hydrocortisone at a dose of 200 mg per day (grade 2C). WEAK RECOMMENDATION Reworded


48 Corticosteroides N=16
49 Immunoglobulin We suggest not using intravenous immunoglobulin in adult patients with severe sepsis and septic shock (2B) WEAK RECOMMENDATION New!!!
50 Selenium We suggest not using intravenous selenium to treat severe sepsis WEAK RECOMMENDATION New!!!
51 Redução da pneumonia...
52
53 Mechanical Ventilation (ARDS) We recommend that clinicians target a tidal volume of 6 ml/kg predicted body weight in patients with sepsis induced acute respiratory distress syndrome (ARDS) (grade 1A vs. 12 ml/kg). We recommend that plateau pressures be measured in patients with ARDS and that the initial upper limit goal for plateau pressures in a passively inflated lung be 30 cm H2O (grade 1B). STRONG RECOMMENDATION slightly changed
54 Mechanical Ventilation (ARDS) We recommend PEEP be applied to avoid alveolar collapse at end expiration (atelectotrauma) (Grade 1B). STRONG RECOMMENDATION We suggest strategies based on higher rather than lower levels of PEEP for patients with sepsis induced moderate to severe ARDS (grade 2C). WEAK RECOMMENDATION New!!!
55 PEEP alta vx PEEP baixa PEEP alta vx PEEP baixa Mortalidade- 34.1% vs 39.1%; RR, 0.90; 95% CI, ;P=.049) Desmame OR 1.16; 95% CI, ; P=.01
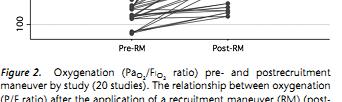
56 Mechanical Ventilation (ARDS) We suggest recruitment t maneuvers in sepsis patients t with severe refractory hypoxemia due to ARDS (Grade 2C). WEAK RECOMMENDATION New!!! We suggest prone positioning in sepsis-induced ARDS patients with a PaO2/FiO2 ratio 100 mm Hg in facilities that have experience with such practices (grade 2B). WEAK RECOMMENDATION
57
58 Sedation, Analgesia, and Neuromuscular Blockade 1. We suggest a short course of NMBA (< 48 hours) for patients with early, severe sepsis-induced induced ARDS and po 2 /FiO 2 < 150 mmhg ( grade 2C). New!!! WEAK RECOMMENDATION

59 N=340 Use for 24 hours Adjusted d mortality OR (0.48 to 0.98) P = 0.04 Longer MV free days Longer MV free days Longer ICU free days Barotrauma reduction
60 Glucose control 1. We recommend a protocolized approach to blood glucose management age e in ICU patients ts with severe e e sepsis s commencing insulin dosing when two consecutive blood glucose levels are >180 mg/dl. This approach should target an upper blood glucose < 180 mg/dl rather than an upper target blood glucose < 110 mg/dl (grade 1A). New!!! STRONG RECOMMENDATION



61 The literature...
62 Renal replacement We suggest that continuous renal replacement therapies and intermittent hemodialysis are equivalent in patients with severe sepsis and acute renal failure because they achieve similar short-term survival rates (grade 2B). We suggest the use of continuous therapies to facilitate management of fluid balance in hemodynamically unstable septic patients (grade 2D). WEAK RECOMMENDATIONS
63 Nutrition NEW TOPIC!!! We suggest administering oral or enteral (if necessary) feedings, as tolerated, rather than either complete fasting or provision of only intravenous glucose within the first 48 hours after a diagnosis of severe sepsis/septic shock. (Grade 2C). We suggest avoiding mandatory full caloric feeding in the first week but rather suggest low dose feeding (eg, up to 500 cal per day), advancing only as tolerated (Grade 2B). WEAK RECOMMENDATIONS
64 Nutrition in SSC NEW TOPIC!!! We suggest using intravenous glucose and enteral nutrition rather than total parenteral nutrition (TPN) alone or parenteral nutrition in conjunction with enteral feeding in the first 7 days after a diagnosis of severe sepsis/septic shock (Grade 2B) WEAK RECOMMENDATION
65 Nutrition in SSC NEW TOPIC!!! We suggest using nutrition titi with no specific immunomodulating supplementation in patients with severe sepsis (grade 2C). WEAK RECOMMENDATION
66 Conclusões SOBREVIDA = RECONHECIMENTO PRECOCE + TRATAMENTO ADEQUADO
67
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012
 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012 Definition Sepsis the presence of infection with
本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時, 須獲得原期刊之同意授權 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock 2012 Definition Sepsis the presence of infection with
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
TERMINOLOGY SIRS 10/30/2014 SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU
 Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
SEPSIS MANAGEMENT. Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah
 Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah") SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
EBM EGDT 每次都是RCT.有點煩 本來想簡單處理 那些年我們曾經打拼過的~~ By Maxy Lu 這次想要放鬆一下~~ EGDT (Early goal-directed therapy) Early go to ICU
 Early go to ICU") EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
EBM 2014.03.24 By Maxy Lu 每次都是RCT.有點煩 這次想要放鬆一下~~ 本來想簡單處理 EGDT (Early goal-directed therapy) 那些年我們曾經打拼過的~~ EGDT Early go to ICU 想說這下開心了 Best practice Not Standard of care Screening and practice improvement
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Sepsis Update Disclosures. Definitions. Objectives. Diagnosis. Diagnosis 9/21/15
 Sepsis Update 2015 Nathaniel D. Curl, MD FACEP UnityPoint Health-Trinity Disclosures I received an all-expenses paid trip in March 2011 from Edwards, the manufacturer of the PreSep catheter, to attend
Sepsis Update 2015 Nathaniel D. Curl, MD FACEP UnityPoint Health-Trinity Disclosures I received an all-expenses paid trip in March 2011 from Edwards, the manufacturer of the PreSep catheter, to attend
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
The Management of Septic Shock
 The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
The Management of Septic Shock Anthony J. Courey, MD Assistant Professor of Medicine Associate Director, CCMU Pulmonary & Critical Care Medicine No conflicts No disclosures Conflicts & Disclosures Overview
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
PICO Questions (From Supplemental Digital Content 1)...6
...6") SUPPLEMENTAL DIGITAL CONTENT 2 CONTENTS PICO Questions (From Supplemental Digital Content 1)...6 HEMODYNAMICS... 31 Table 1. Crystalloid with supplemental Albumin compared to Crystalloids alone for resuscitating
SUPPLEMENTAL DIGITAL CONTENT 2 CONTENTS PICO Questions (From Supplemental Digital Content 1)...6 HEMODYNAMICS... 31 Table 1. Crystalloid with supplemental Albumin compared to Crystalloids alone for resuscitating
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Sepsis Review. Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center
 Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org Discuss the Updated International Guidelines Discuss how you
Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center acraig@crmchealth.org Discuss the Updated International Guidelines Discuss how you
Septic shock. Babak Tamizi Far M.D Isfahan university of medical sciences
 Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Septic shock Babak Tamizi Far M.D Isfahan university of medical sciences Definitions Used to Describe the Condition of Septic Patients Approximately 750,000 cases of severe sepsis or septic shock occur
Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP
 Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP Objectives Review the changes to the 2012 sepsis guidelines and the 2016 Sepsis Guidelines Discuss the literature impacting the sepsis
Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP Objectives Review the changes to the 2012 sepsis guidelines and the 2016 Sepsis Guidelines Discuss the literature impacting the sepsis
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Infectious Diseases II
 Simon W. Lam, Pharm.D., FCCM, BCPS Cleveland Clinic Cleveland, Ohio Seth R. Bauer, Pharm.D., FCCM, BCPS Cleveland Clinic Cleveland, Ohio Infectious Diseases II Simon W. Lam, Pharm.D., FCCM, BCPS Cleveland
Simon W. Lam, Pharm.D., FCCM, BCPS Cleveland Clinic Cleveland, Ohio Seth R. Bauer, Pharm.D., FCCM, BCPS Cleveland Clinic Cleveland, Ohio Infectious Diseases II Simon W. Lam, Pharm.D., FCCM, BCPS Cleveland
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012
 Intensive Care Med (2013) 39:165 228 DOI 10.1007/s00134-012-2769-8 GUIDELINES R. P. Dellinger Mitchell M. Levy Andrew Rhodes Djillali Annane Herwig Gerlach Steven M. Opal Jonathan E. Sevransky Charles
Intensive Care Med (2013) 39:165 228 DOI 10.1007/s00134-012-2769-8 GUIDELINES R. P. Dellinger Mitchell M. Levy Andrew Rhodes Djillali Annane Herwig Gerlach Steven M. Opal Jonathan E. Sevransky Charles
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
SEPSIS AND SEPTIC SHOCK INTERNATIONAL GUIDLINES 2016
 SEPSIS AND SEPTIC SHOCK INTERNATIONAL GUIDLINES 2016 Sepsis is defined as organ dysfunction due to excessive reaction to infection It is a consequence of sepsis Needs vasoactive drug administration for
SEPSIS AND SEPTIC SHOCK INTERNATIONAL GUIDLINES 2016 Sepsis is defined as organ dysfunction due to excessive reaction to infection It is a consequence of sepsis Needs vasoactive drug administration for
Surviving Sepsis: A CRASH Course. Justin Jones, PharmD Sanford Medical Center, Fargo Staff Education 2015
 Surviving Sepsis: A CRASH Course Justin Jones, PharmD Sanford Medical Center, Fargo Staff Education 2015 Disclosures No financial conflicts of interest Abbreviations ULN Upper limit of normal SVCO2 Central
Surviving Sepsis: A CRASH Course Justin Jones, PharmD Sanford Medical Center, Fargo Staff Education 2015 Disclosures No financial conflicts of interest Abbreviations ULN Upper limit of normal SVCO2 Central
Educational Workshop
 Educational Workshop EW02: Management of severe sepsis and septic shock anno 2015 Arranged with ESGBIS & International Sepsis Forum (ISF) Convenors: W. Joost Wiersinga, Amsterdam, NL Tom van der Poll,
Educational Workshop EW02: Management of severe sepsis and septic shock anno 2015 Arranged with ESGBIS & International Sepsis Forum (ISF) Convenors: W. Joost Wiersinga, Amsterdam, NL Tom van der Poll,
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Is nosocomial infection the major cause of death in sepsis?
 Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
Is nosocomial infection the major cause of death in sepsis? Warren L. Lee, MD PhD, FRCPC Department of Medicine University of Toronto There are no specific therapies for sepsis the graveyard for pharmaceutical
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
Vasopressors for shock
 Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Vasopressors for shock Background Reviews and Observational Studies Holler 2015. Nontraumatic Hypotension and Shock in the Emergency Department and Prehospital Setting Prevalence, Etiology and Mortality:
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
Note: Page numbers of article titles are in boldface type. A Abdomen, and aorta, as causes of shock, point-of-care ultrasonography in assessment of, 915 917 Abdominal compartment syndrome, trauma patient
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Practical. Septic shock resuscitation ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล
 Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Practical Septic shock resuscitation ไ ไชยร ตน เพ มพ ก ล พบ. ภาคว ชาอาย รศาสตร คณะแพทยศาสตร ศ ร ราชพยาบาล ประช มว ชาการ 101 ป อาย รศาสตร ศ ร ราช 6 ก มภาพ นธ 2561 Early recognition Early resuscitation Early
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid