Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
|
|
|
- Clara Bell
- 6 years ago
- Views:
Transcription
1 Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016
2 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke remains: first leading cause of disability fifth leading cause of death (greater than 1 in 15 deaths are from stroke)»

3 Types of Stroke Divided into ischemic or hemorrhagic Ischemic: 88% Hemorrhagic: 12% Intracranial Hemorrhage: 67% SAH: 33%
4 Ischemic stroke subtypes Complex heterogeneous disease with different subtypes Cryptogenic stroke: 30% Penetrating Artery Disease/Lacunae: 25% Cardioembolic: 20% Atherosclerotic Cerebrovascular***: 20% Other: 5%
5 Ischemic stroke subtypes ICAS accounts for about 10% of ischemic stroke cases but depends on ethnicity 5 10% of strokes in white people 15 29% of strokes in black people 30 50% of strokes in Asian people Gorelick, et al. Stroke. 2008; 39:
6 ICAS mimickers Arterial dissection (subadvential vs. subintimal) Fibromuscular dysplasia Primary or secondary vasculitis Moya moya Cerebral vasocontriction syndrome Other vasculopathies
7 There are three main mechanisms of stroke related to ICAS hypoperfusion artery-to-artery embolism plaque extension over small penetrating artery ostia (also known as branch atheromatous disease)
8 Imaging for ICAS TCD and MRA useful screening tools for the exclusion of ICAS Unreliable to establish the diagnosis and the degree of stenosis CTA is more accurate than MRA for the diagnosis for ICAS Cerebral angiography remains the gold standard» Chimowitz, et al.lancet Neurol. 2013;
9 Case Presentation 56 RH M with DM, HTN, CAD with CABG Did not have sudden onset but insidious of swaying to the left one episode of difficulty word finding Fine the next two days but the swaying returned Came to the ED and was admitted was on aspirin 81 mg daily already
10 Case Presentation On neuro exam Very mild left upper motor neuron facial droop questionable arm/shoulder weakness Stroke work up performed Several areas of infarction in the right MCA territory
11 Several areas of infarction in his right MCA distribution

12 Several areas of infarction in his right MCA distribution
13 Case Presentation Etiology from severe right MCA stenosis Long segment in the M1 branch at 95%
14 Severe stenosis of the right middle cerebral artery

15 CTA brain was done to confirm the MRA
16 Case Presentation Unable to get a CTP Was placed on Clopidogrel with the aspirin Atorvastatin 80 mg Blood pressure medication was held If was to fluctuate neurologically Transfer to MICU IVF with HOB flat Even induce hypertension Was stable but a decision needed to be made
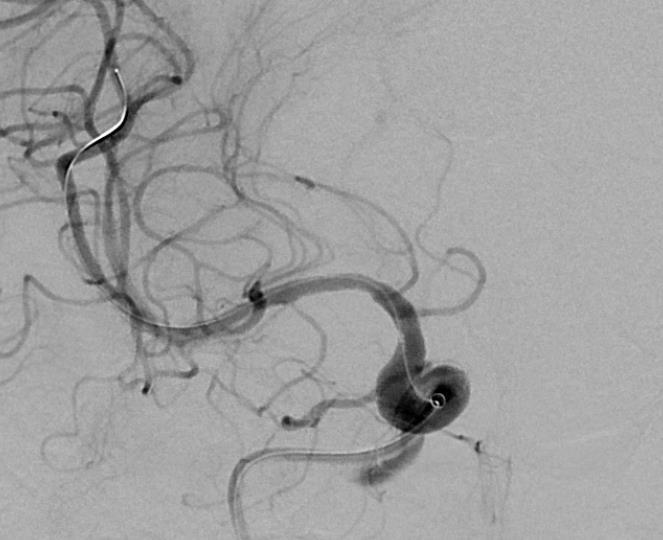
17 Case Presentation Conventional cerebral angiogram was done
18
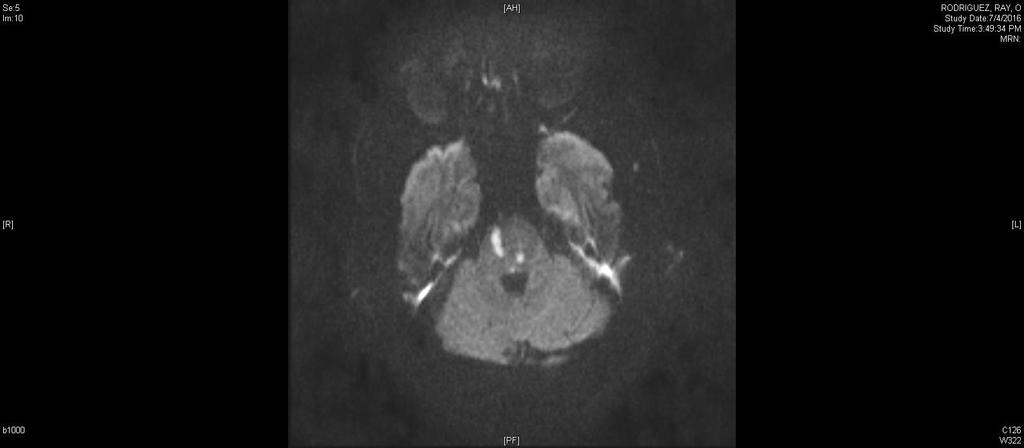
19 Case Presentation 2 72 RH M with DM, HTN, HL presented with RHP and dysarthria NIHSS was 10 Got IV tpa and NIHSS improved to 3 R facial droop (UMN), R arm ataxia, dysarthria CTA showed critical basilar artery stenosis and possible thrombus distal to the stenosis Since he was improved an emergent angiogram was not done
20 Case Presentation 2 That night a conventional cerebral angiogram was performed Confirmed the critical basilar artery stenosis (95%) and post-stenotic thrombus Distal basilar artery was supplied by the PCOM s Distal R vertebral artery was occluded proximal to the R PICA (which filled from the L vertebral) a MRI/DWI brain was done immediately after the cerebral angiogram Bilateral patchy pontine and a punctate right cerebellar strokes
21
22
23 Case Presentation 2 Heparin drip was started after 24 hours of systemic thrombolysis 3 days later Repeat MRI/DWI brain was without new infarcts*** Repeat CTA s showed resolution of the thrombus in the distal basilar artery and the critical basilar stenosis

24
25 Case Presentation 2 The Heparin gtt was stopped and the patient was placed on Clopidogrel with the aspirin Atorvastatin 80 mg was continued Blood pressure medications were held for perfusion purposes A decision needed to be made
26 Literature on ICAS
27 WARSS (Warfarin-Aspirin Recurrent Stroke Study) trial Though not directly evaluating ICAS; a lesson was learned in stroke management 2206 patients enrolled compared aspirin (325 mg/day) with warfarin at an INR 1.4 to 2.8 with non-cardioembolic ischemic stroke Oral anticoagulation (OAC) was not better than aspirin for preventing ischemic stroke in patients with ICAS Study found similar rates of ischemic stroke, death, or major hemorrhage for both warfarin and aspirin treatment arms Issue of why the trial was done Mohr, et al. NEJM 2001; 345: 1444
28 WASID (Warfarin-Aspirin Symptomatic Intracranial Disease) study First medical management trial of ICAS TIA or non-disabling stroke from an angiographic verified stenosis at 50 to 99% of a major intracranial vessel Compared aspirin 1300mg/day with Warfarin with an INR 2.0 to 3.0 study was stopped prematurely because of safety concerns for patients in the warfarin arm after enrolling 569 patients with an average follow-up of 1.8 years» Chimowitz et al. NEJM 2005; 352: 1305
29 WASID (Warfarin-Aspirin Symptomatic Intracranial Disease) study rate of stroke recurrence in the territory of the stenotic intracranial artery was high for both aspirin and warfarin treatment primarily occurred within the first year from the qualifying event Aspirin treatment was associated with a significantly lower rate of... death than warfarin major hemorrhage (mostly systemic) than warfarin Chimowitz et al. NEJM 2005; 352: 1305
30 WASID (Warfarin-Aspirin Symptomatic Intracranial Disease) study In reality, both warfarin and aspirin were ineffective, given the rate of stroke and death in both arms Warfarin arm 21.8% (n = 289) Aspirin arm 22.1% (n = 280) confirmed that OCA was no better than aspirin for preventing ischemic stroke in patients poorly controlled risk factors that contributed to recurrent vascular events systolic blood pressure > 140 mm Hg Mean cholesterol level > 200 mg/dl Chimowitz et al. NEJM 2005; 352: 1305
31 WASID (Warfarin-Aspirin Symptomatic Intracranial Disease) study Imaging characteristics associated with recurrent stroke risk Degree of stenosis did effect risk of recurrent events At least 70% stenosis had a higher risk of stroke compared to stenosis of 50 to 69% Presence of robust collaterals in patients > 70% stenosis mitigated the risk of stroke recurrence Timing of enrollment If within 17 days or fewer had significantly higher risk of recurrent stroke If more than 17 days (up to 90 days) of the qualifying event had lower risk of recurrent stroke Chimowitz, et al.lancet Neurol. 2013;
32 SAMMPRIS (Stenting and Aggressive Medical Management for the Prevention of Recurrent Ischemic Stroke ) The failure of WASID to answer the question led to this trial enrolled patients with percent stenosis of a intracranial vessel who had a TIA or ischemic stroke within 30 days prior randomly assigned to treatment with intracranial angioplasty and stenting (Wingspan system) plus aggressive medical management or to treatment with aggressive medical management alone Max antiplatelet regiment Systolic blood pressure < 140 mmhg LDL < 70 mg/dl comprehensive lifestyle modification program» Derdeyn et al. Lancet 2014; 383: 333
33 SAMMPRIS (Stenting and Aggressive Medical Management for the Prevention of Recurrent Ischemic Stroke ) enrollment was halted after recruitment of 451 of the planned 764 patients the combined rate of stroke or death within 30 days of enrollment (the primary outcome) significantly higher for patients treated with angioplasty and stenting (14%) compared with those treated with medical therapy alone (5.8%) the periprocedural rate of stroke was higher than expected for the stenting group, and lower than estimated for the medical management group Derdeyn et al. Lancet 2014; 383: 333
34 SAMMPRIS (Stenting and Aggressive Medical Management for the Prevention of Recurrent Ischemic Stroke ) Even at study end with a median follow up of 32 months max medical (12.2% rate of stroke) was superior to intracranial angioplasty (25%) The long term result were largely driven by the 30 day outcomes since the rate of stroke and death after 30 days were similar Derdeyn et al. Lancet 2014; 383: 333
35 SAMMPRIS (Stenting and Aggressive Medical Management for the Prevention of Recurrent Ischemic Stroke ) the higher stroke rate in the stenting arm was driven by Inclusion of patients with perforator syndromes Smaller vessel size Diffuse stenosis (oversizing of devices) Procedural considerations Stringent blood pressure control General anesthesia use Operator experience Improved max medical treatment* Interesting that the rate of stroke or death in the aggressive med management arm was substantially lower than in the historical WASID controls (5.8% vs. > 20%) Derdeyn et al. Lancet 2014; 383: 333
36 Intracranial bypass surgery (EC- IC bypass) was published in patients symptomatic extracranial carotid occlusion, distal carotid occlusive disease, or middle cerebral arteries (MCA) stenosis randomized to either medical therapy alone (aspirin 1300 mg/day in four divided doses) or to extracranial-intracranial anastomosis surgery (joining the superficial temporal artery and the middle cerebral artery) combined with medical therapy mean follow-up was 55.8 months Results revealed the EC-IC bypass was ineffective for preventing stroke The EC/IC Bypass Study Group. NEJM 1985; 313: 1191
37 Recommendations Max medical treatment Antihypertensive agents*** Statins Antiplatlet agents (aspirin and Plavix for 90 d) then monotherapy (even including aspirinextended-release dipyridamole)..match and CHARISMA trials Lifestyle modifications No smoking Exercise Weight reduction, etc.
38 Outcomes
39
40

41
42 Outcome Residual: No deficit but symptoms of being off balance Modified Rankin of one
43 Modified Rankin Scale No symptoms at all No significant disability despite symptoms; able to carry out all usual duties and activities Slight disability; unable to carry out all previous activities, but able to look after own affairs without assistance Moderate disability; requiring some help, but able to walk without assistance Moderately severe disability; unable to walk without assistance and unable to attend to own bodily needs without assistance 5 6 Severe disability; bedridden, incontinent and requiring constant nursing care and attention Dead» Bonita, et al. Stroke,

44

45
46 Outcome 2 Residual: Right INO Mild dysmetria of limbs (left > right) Modified Rankin of four at discharge to acute rehab
47 Evidence based medicine My thoughts No guidelines for ICAS from the American Stroke Association Dr. L. Caplan, M.D. argument Example of migraine prevention Topamax TCAs and BP medications that being said..must not be used as an excuse to do what one wants! Must be justification for reasoning
48 The future for ICAS? Angioplasty alone Indirect surgery bypass procedures Use of newer anticoagulants
49 Questions?
50

51
52 Case Presentation 2
53
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Slide 1. Slide 2 Conflict of Interest Disclosure. Slide 3 Stroke Facts. The Treatment of Intracranial Stenosis. Disclosure
 Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
Slide 1 The Treatment of Intracranial Stenosis Helmi Lutsep, MD Vice Chair and Dixon Term Professor, Department of Neurology, Oregon Health & Science University Chief of Neurology, VA Portland Health Care
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Intracranial Atherosclerosis in Asians
 Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
Intracranial Atherosclerosis in Asians Anthony S. Kim, MD Assistant Clinical Professor of Neurology UCSF Neurovascular Service February 27, 2010 Disclosures Research Support National Institutes of Health
SAMMPRIS. Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis. Khalil Zahra, M.D
 SAMMPRIS Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis Khalil Zahra, M.D Major points Patients with recent TIA or stroke and intra-cranial artery
SAMMPRIS Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis Khalil Zahra, M.D Major points Patients with recent TIA or stroke and intra-cranial artery
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
5/2/2016. Outpatient Stroke Management Sheila Smith MD May 5, 2016
 Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Outpatient Stroke Management Sheila Smith MD May 5, 2016 1 Management of Outpatient Stroke Objectives Review blood pressure management post stroke Review antithrombotic therapy Review statin therapy Discuss
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Advances in the treatment of posterior cerebral circulation symptomatic disease
 Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Advances in the treatment of posterior cerebral circulation symptomatic disease Athanasios D. Giannoukas MD, MSc(Lond.), PhD(Lond.), FEBVS Professor of Vascular Surgery Faculty of Medicine, School of Health
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco
 Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
Karl Meisel, MD MA Director of Stroke Clinic University of California San Francisco I have no financial disclosures 1 Hospital Management Thrombolytic and Thrombectomy Blood pressure Stroke in the Young
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
The learning curve associated with intracranial angioplasty and stenting: analysis from a single center
 Original Article Page 1 of 7 The learning curve associated with intracranial angioplasty and stenting: analysis from a single center Peiquan Zhou, Guang Zhang, Zhiyong Ji, Shancai Xu, Huaizhang Shi Department
Original Article Page 1 of 7 The learning curve associated with intracranial angioplasty and stenting: analysis from a single center Peiquan Zhou, Guang Zhang, Zhiyong Ji, Shancai Xu, Huaizhang Shi Department
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
collaterals offset ischemia
 Imaging of Intracranial Stenosis objectives & next steps collaterals offset ischemia systematic evaluation of collaterals hemodynamic impact, not % stenosis develop fractional flow measures collateral
Imaging of Intracranial Stenosis objectives & next steps collaterals offset ischemia systematic evaluation of collaterals hemodynamic impact, not % stenosis develop fractional flow measures collateral
2015 Update in Diagnosis and Management of Stroke
 2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
2015 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Senior Executive Vice Chair, Department
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Protocol. This trial protocol has been provided by the authors to give readers additional information about their work.
 Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: Chimowitz MI, Lynn MJ, Derdeyn CP, et al. Stenting versus aggressive
Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: Chimowitz MI, Lynn MJ, Derdeyn CP, et al. Stenting versus aggressive
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Cryptogenic Stroke: What Don t We Know. Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare
 Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Cryptogenic Stroke: What Don t We Know Siddharth Sehgal, MD Medical Director, TMH Stroke Center Tallahassee Memorial Healthcare Financial Disclosures None Objectives Principles of diagnostic evaluation
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million life insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS. 73 year old NS right-handed male applicant for $1 Million Life Insurance
 MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
MORTALITY AND MORBIDITY RISK FROM CAROTID ARTERY ATHEROSCLEROSIS October 17, 2012 AAIM Triennial Conference, San Diego Robert Lund, MD What Is The Risk? 73 year old NS right-handed male applicant for $1
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
2014 Update in Diagnosis and Management of Stroke
 2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
2014 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Acting Chairman, Department of Neurology
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Treatment Considerations for Carotid Artery Stenosis. Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery
 Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Treatment Considerations for Carotid Artery Stenosis Danielle Zielinski, RN, MSN, ACNP Rush University Neurosurgery 4.29.2016 There is no actual or potential conflict of interest in regards to this presentation
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Medical Management. Bogachan Sahin, M.D., Ph.D. Department of Neurology
 Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
Acute Medical Management Bogachan Sahin, M.D., Ph.D. Department of Neurology Outline Head-of-bed position Blood pressure management Antiplatelet therapy Anticoagulation Statin therapy Rehabilitation and
57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP
 Case # 1 Hx 57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP show left PCA occlusion, some basilar stenosis,
Case # 1 Hx 57y WRH woman, controlled HTN only, presents with sudden LOC, fixed and dilated, quadraplegic Intubated on arrival and CT is negative CTA and CTP show left PCA occlusion, some basilar stenosis,
2018 Update in Diagnosis and Management of Stroke
 2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
2018 Update in Diagnosis and Management of Stroke S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director,
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know. Case 1 4/5/11. What treatment should you initiate?
 Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Advances in Prevention and Treatment of Stroke: What Every Primary Care Physician Needs to Know S. Andrew Josephson, MD Director, Neurohospitalist Program Medical Director, Inpatient Neurology University
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
. 8. Pharmacological treatment in acute stroke 8.3 Antiplatelet and anticoagulant treatment in stroke due to arterial dissection
 . 8. Pharmacological treatment in acute stroke 8.3 Antiplatelet and anticoagulant treatment in stroke due to arterial dissection Reference Evidence Tables PHARM4 What is the safety and efficacy of anticoagulants
. 8. Pharmacological treatment in acute stroke 8.3 Antiplatelet and anticoagulant treatment in stroke due to arterial dissection Reference Evidence Tables PHARM4 What is the safety and efficacy of anticoagulants
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Association of Systolic Blood Pressure with Progression of Symptomatic Intracranial Atherosclerotic Stenosis
 Journal of Stroke 2017;19(3):304-311 Original Article Association of Systolic Blood Pressure with Progression of Symptomatic Intracranial Atherosclerotic Stenosis Jong-Ho Park, a Bruce Ovbiagele, b Keun-Sik
Journal of Stroke 2017;19(3):304-311 Original Article Association of Systolic Blood Pressure with Progression of Symptomatic Intracranial Atherosclerotic Stenosis Jong-Ho Park, a Bruce Ovbiagele, b Keun-Sik
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Balloon Angioplasty for Intracranial Atherosclerotic Disease: a Multicenter Study
 Balloon Angioplasty for Intracranial Atherosclerotic Disease: a Multicenter Study Lakshmi Sudha Prasanna Karanam 1, Mukesh Sharma 2, Anand Alurkar 3, Sridhar Reddy Baddam 1, Vijaya Pamidimukkala 1, and
Balloon Angioplasty for Intracranial Atherosclerotic Disease: a Multicenter Study Lakshmi Sudha Prasanna Karanam 1, Mukesh Sharma 2, Anand Alurkar 3, Sridhar Reddy Baddam 1, Vijaya Pamidimukkala 1, and
Alex Abou-Chebl, MD Medical Director, Stroke Baptist Health, Louisvile. Alex Abou-Chebl, MD
 Medical Director, Stroke Baptist Health, Louisvile No Conflicts or Disclosures Post SAMMPRIS Too many unanswered questions Is stenting too risky? What aspects of the procedure resulted in such a high-complication
Medical Director, Stroke Baptist Health, Louisvile No Conflicts or Disclosures Post SAMMPRIS Too many unanswered questions Is stenting too risky? What aspects of the procedure resulted in such a high-complication
TCD in Subclavian Steal Syndrome
 ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
ISSN 2005-7881 Journal of Neurosonology 2(Suppl. 1):25-30, 2010 TCD in Subclavian Steal Syndrome Soon-Tae Lee, M.D., Ph.D. Department of Neurology, Seoul National University Hospital, Seoul, South Korea
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist. neurointerventionist
 MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
MEET 2007: Evaluation and treatment of the stroke and TIA patient for the non-neurointerventionist neurointerventionist Steve Ramee, MD Ochsner Medical Center New Orleans DISCLOSURE Nothing Nothing to
Angioplasty Alone: May Be the Best Endovascular Treatment for ICAS
 Angioplasty Alone: May Be the Best Endovascular Treatment for ICAS David Fiorella Cerebrovascular Center Department of Neurosurgery State University of New York at Stony Brook Why did PTAS fail in SAMMPRIS?
Angioplasty Alone: May Be the Best Endovascular Treatment for ICAS David Fiorella Cerebrovascular Center Department of Neurosurgery State University of New York at Stony Brook Why did PTAS fail in SAMMPRIS?
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
GWTG Post-Discharge Follow-up Form
 Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Bold font = Required field Patient ID: Date of Hospital Admission: / / mm / dd / yyyy Date Follow-up Completed: / / mm / dd / yyyy PATIENT LOGISTICS Method used for Patient follow-up: Chart Review Health
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
PFO Management update
 PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
PFO Management update May 12, 2017 Peter Casterella, MD Swedish Heart and Vascular 1 PFO Update 2017: Objectives Review recently released late outcomes of RESPECT trial and subsequent FDA approval of PFO
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Cerebrovascular Disease. RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009
 Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
Cerebrovascular Disease RTC Conference Resident Presenter: Dr. Christina Bailey Faculty: Dr. Jeff Dattilo October 2, 2009 Cerebrovascular Disease Stroke is the 3 rd leading cause of death and the leading
How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion
 How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion November 1 st, 2017 Johanna T. Fifi, MD Director, Endovascular Ischemic Stroke Associate Professor of Neurology, Neurosurgery,
How to Manage LVO Stroke with Access Blocked by Cervical Carotid Occlusion November 1 st, 2017 Johanna T. Fifi, MD Director, Endovascular Ischemic Stroke Associate Professor of Neurology, Neurosurgery,
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Small Vessel Stroke. Domenico Inzitari Careggi University Hospital Florence (Italy)
") Small Vessel Stroke Domenico Inzitari Careggi University Hospital Florence (Italy) Topics Lacunar stroke The small vessel conundrum Small and large Conclusions Fisher s lacunar syndromes Pure motor hemiparesis
Small Vessel Stroke Domenico Inzitari Careggi University Hospital Florence (Italy) Topics Lacunar stroke The small vessel conundrum Small and large Conclusions Fisher s lacunar syndromes Pure motor hemiparesis
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Significant Relationships
 Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Opening Large Vessels During Acute Ischemic Stroke Significant Relationships Wade S Smith, MD, PhD Director UCSF Neurovascular Service Professor of Neurology Daryl R Gress Endowed Chair of Neurocritical
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur.
 A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
A CASE OF RECURRENT ALTERNATING TRANSIENT HEMIPARESIS Dr. Shunmuga Arumugasamy.S DNB Resident Railway Hospital, Perambur. 6 year old school going child. Apparently normal till 3 yrs when she developed
Recent Advances in Neurology Difficult Cases
 Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
Secondary Stroke Prevention
 Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Secondary Stroke Prevention Acute stroke conference, Sunnybrook Estates January 20, 2011 Rick Swartz HBSc, MD, PhD, FRCPC Assistant Professor, Department of Medicine, Divisions of Neurology and Obstetrical
Subject Expert. Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO
 Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Stroke 101 Subject Expert Michelle Whaley MSN, CNS, CCNS, ANVP-BC Swedish Medical Center Englewood, CO 2 Objectives Types of strokes Stroke warning signs Stroke risk factors Medical test performed following
Index. interventional.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Index Note: Page numbers of article titles are in boldface type. A ACAS (Asymptomatic Carotid Atherosclerosis Study), 65 66 ACST (Asymptomatic Carotid Surgery Trial), 6 7, 65, 75 Age factors, in carotid
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology
 Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
Guiding Secondary Stroke Prevention through Evaluation of Ischemic Stroke Etiology Ann M. Leonhardt Caprio, MS, RN, ANP-BC Program Coordinator Comprehensive Stroke Center, Strong Memorial Hospital Clinical
TIA triage in Not all that glitters is gold
 TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
TIA triage in 2016 Not all that glitters is gold Disclosures No industry related disclosures Expert witness work Overview Definition Implications Guidelines, secondary prevention Implementation of guidelines
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen
 What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
What the general cardiologist should know about arrhythmia Stroke prevention in AF" Peter Ammann Kantonsspital St. Gallen What the cardiologist should know about arrhythmia and stroke are there real low
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
New Trials in Progress: ACT 1. Jon Matsumura, MD Cannes, France June 28, 2008
 New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
New Trials in Progress: ACT 1 Jon Matsumura, MD Cannes, France June 28, 2008 Faculty Disclosure I disclose the following financial relationships: Consultant, CAS training director, and/or research grants
Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary
 SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
SOCIETY FOR VASCULAR SURGERY DOCUMENT Updated Society for Vascular Surgery guidelines for management of extracranial carotid disease: Executive summary John J. Ricotta, MD, a Ali AbuRahma, MD, FACS, b
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor