Update on Atherosclerosis Treatment and Prevention
|
|
|
- Kory Ford
- 6 years ago
- Views:
Transcription

 Optimizing Performance Identifying patients STAtin: Starts, Titrations, and")
1 Update on Atherosclerosis Treatment and Prevention Ronald D. Scott, MD Lipidology and Family Medicine West LA Med Center Regional CVD Colead Overview Lipids and CAD risk CVD is major killer and impacts morbidity Large statin benefit opportunity Treat high LDL (> 190) regardless of risk. Treat those at risk, regardless of LDL (>70) Optimizing Performance Identifying patients STAtin: Starts, Titrations, and Adherence Use tools to promote statins Safety / intolerance of statins Beyond statins 1
 Yusuf S. European Society of Cardiology Congress 2004 PAR adjusted for all (99% CI) ApoB/ApoA-1 (fifth 54.1 (49.6-58.")
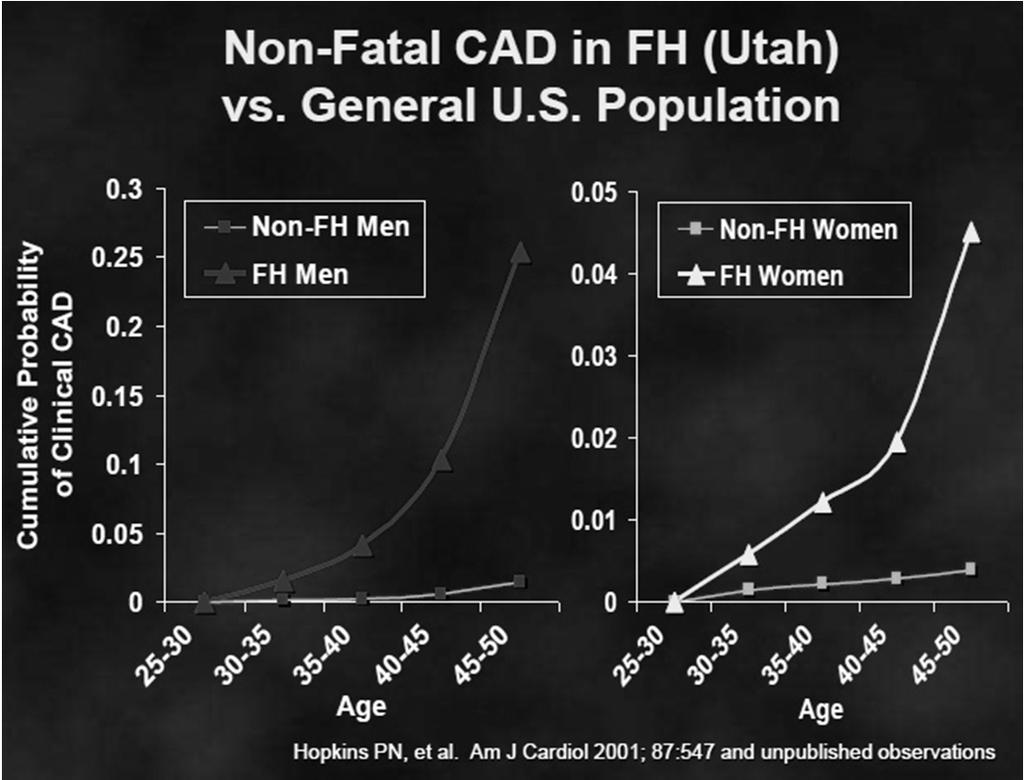
2 Also, stroke is #3 cause of mortality and much feared, significant morbidity. Heart disease and stroke are very costly. Risk factor INTER-HEART: MI risk PAR adjusted for age, sex, and smoking (99% CI) Yusuf S. European Society of Cardiology Congress 2004 PAR adjusted for all (99% CI) ApoB/ApoA-1 (fifth 54.1 ( ) 49.2 ( ) quintile compared with first) Current smoking 36.4 ( ) 35.7 ( ) Diabetes 12.3 ( ) 9.9 ( ) Hypertension 23.4 ( ) 17.9 ( ) Abdominal obesity 33.7 ( ) 20.1 ( ) Psychosocial 28.8 ( ) 32.5 ( ) Vegetable and fruits 12.9 ( ) 13.7 ( ) daily Exercise 25.5 ( ) 12.2 ( ) Alcohol intake 13.9 ( ) 6.7 ( ) All combined 90.4 ( ) 90.4 ( ) 2
3 3
4 Last LDL > 190 in KPSC 33,000 KP So Cal members. If lifestyle not successful, statins recommended if age > 10 years old. Easy to tell in inbox if patient needs statin by this criteria. Is regardless of risk. For adults, lower LDL at least 50%. Start atorvastatin 80 mg daily (53% LDL lowering) Protective PCSK9 mutations Lifelong decreased levels of LDL. Variant 1: 28% reduced LDL 88% reduction in CAD. Variant 2: 15% reduced LDL 50% reduction in CAD. Event reduction impressive: favorable impact of low cholesterol over a long time 4


5 Risk in Primary Prevention Trials 10 y risk 5.0 % 7.5% 5

6 avg A-risk of 7.5 % Entry LDL<130, mean 105 avg FRS of 12% Entry LDL<130, mean 105 6
7 Large statin benefit +/- disease (including Primary Prevention) Primary prevention Lancet Nov 9, 2010 Statins benefit across age span - including those over age 75 CCT. Lancet Nov 9,
8 Statins benefit across range of baseline lipids Baseline LDL mg/dl < > 135 LDL 150 to 89 same benefit as LDL 77 to 45 Lancet Nov 9, 2010 HPS: NNT NNT (simvastatin 40 mg) to prevent one MI, stroke or revascularization in 5 years. DX NNT Post MI 10 Angina 12.5 s/p Stroke, PAD, DM age > Young DM with 80% Lifetime risk of CAD Simvastatin 40 mg in Heart Protection Study
 6 excess cases of adverse effects per 1000 statintreated persons over 5 years NNH = 167 High intensity statin (atorvastatin 40-80 mg) 16 excess")
9 JUPITER: NNT Statin risks, NNH NNH of new onset DM, myopathy. Conservative estimates. Harm not as severe as MI or stroke. Low to Moderate intensity statin (< atorvastatin 20 mg) 6 excess cases of adverse effects per 1000 statintreated persons over 5 years NNH = 167 High intensity statin (atorvastatin mg) 16 excess cases of adverse effects per 1000 statintreated persons over 5 years NNH = 63 9
10 Starting Statins Acute Ischemic Stroke / Acute Coronary Syndrome: atorvastatin 80 mg LDL > 190 (regardless of risk): atorvastatin 80 mg CAD / IVD, DM (age > 40 or RF), or FRS > 10%: atorvastatin 40 mg simvastatin 40 mg for cost sensitive members with higher atorvastatin copayments Consider lower doses, clinical judgment and / or shared decision making in patients with: baseline LDL < 70, Age > 76 years, Liver disease or muscle disorders. Asian ancestry. % on statin CAD/IVD. In last 6 mos 84% DM age > 40. In last 6 mos 76% LDL > 190. ever on statins 66% FRS > 10%. About 30% Need about 500,000 statin starts 10

11 Generic statins are cost saving in lower risk primary prevention High intensity statin over 10 years is cost saving vs low/moderate intensity statin with > 2.5% 10-year CVD risk Generic statins cost saving with > 5% 10- year CHD risk Pletcher MJ, et al. Ann Intern Med. 2009;150: ; Heart Protection Study Collaborative G. Circ Cardiovasc Qual Outcomes. 2009;2(2):65-72; Conly J, et al. Can Med Assoc J. 2011;183(16):E1180-E1188. FRS > 20% FRS 15% With revised guidelines, FRS>10% (and more) in statin target population. Large population with large treatment potential 11
12 STAtins - key to lipid control Start statins in the untreated Titrate up on the undertreated Adherence promotion / working barriers 12


13 Finding the inclusion code: IVD Ischemic Vascular Disease CAD: post MI, post CABG, post PCTA, angina. Status post stroke, carotid artery occlusion. Peripheral arterial disease, AAA. NOT include aortic atherosclerosis, aortic ectasia. 13

14 Abdominal Aorta Screening Abdominal Aortic Aneurysm (AAA) is considered CAD risk equivalent by NHLBI / ATP and KP guidelines statins and LDL < 100 control recommended. Is part of our CAD POINT registry for targeting. Aortic Screening Rate Trend 17% increase in region so far! 28 14
15 Diagnosis and Actions by Aortic Diameter < 2.4 cm: Normal diameter. (check for aortic athero) cm: Aortic Ectasia, place on problem list. Start statin if FRS > 10%. > 3.0 cm: Abdominal Aortic Aneurysm (AAA), start statin, code and place on problem list. > 4.0 cm: above actions, plus referral to vascular surgery. Aortic Ectasia cm Risk Hazard Ratio (crude) Acute MI 1.60 ( ) Stroke 1.59 ( ) Heart Failure 1.85 ( ) Total Mortality 1.46 ( ) Vascular Mortality 1.77 ( ) Duncan JL et al. BMJ 2012 May 4; 344:e

16 Aortic Atherosclerosis and Aortic Ectasia Although not automatic risk equivalents, are markers of increased risk. Imaging findings show risk to patient. Revenue for KP. Patients more likely to have annual appointments. Imaging results can be used as opportunity to promote cardiovascular health. Positive imaging findings communicated with patients leads to higher statin and aspirin use (OR 7.0) J Am Coll Cardiol Apr 2008 Available to members with data elements Start atorvastatin 40 mg daily Framingham risk score (FRS) calculator. Expanding availability. Will change to A-risk in

: start aspirin")
17 "Pre-statin" and latest FRS are calculated and shown above. FRS > 10 %: start atorvastatin 40 mg FRS > 15% (or on treatment > 10 %): start aspirin 81 mg daily at kp.org for members 17


18 Artery image in-person patient education. Tear-off pads or posters, English or Spanish, illiterate. Order from Health Education and use in exam rooms. to reduce cholesterol, heart attacks and strokes in sig Smart Rx - Lipids 18

19 Titration Titration Table lovastatin or pravastatin dose Treated LDL-C level Change to: <= 20 mg atorvastatin 40 mg <= 20 mg > 129 atorvastatin 80 mg 40 mg atorvastatin 40 mg 40 mg >119 atorvastatin 80 mg 80 mg atorvastatin 40 mg 80 mg >109 atorvastatin 80 mg simvastatin dose Treated LDL-C level Change to: <=10 mg atorvastatin 40 mg <=10 mg >129 atorvastatin 80 mg 20 mg atorvastatin 40 mg 20 mg >119 atorvastatin 80 mg 40 mg atorvastatin 40 mg 40 mg >109 atorvastatin 80 mg 80 mg >99 atorvastatin 80 mg atorvastatin dose Treated LDL-C level Change to: < = 10 mg atorvastatin 40 mg < = 10 mg >119 atorvastatin 80 mg 20 mg atorvastatin 40 mg 20 mg >109 atorvastatin 80 mg 40 mg >99 atorvastatin 80 mg 19
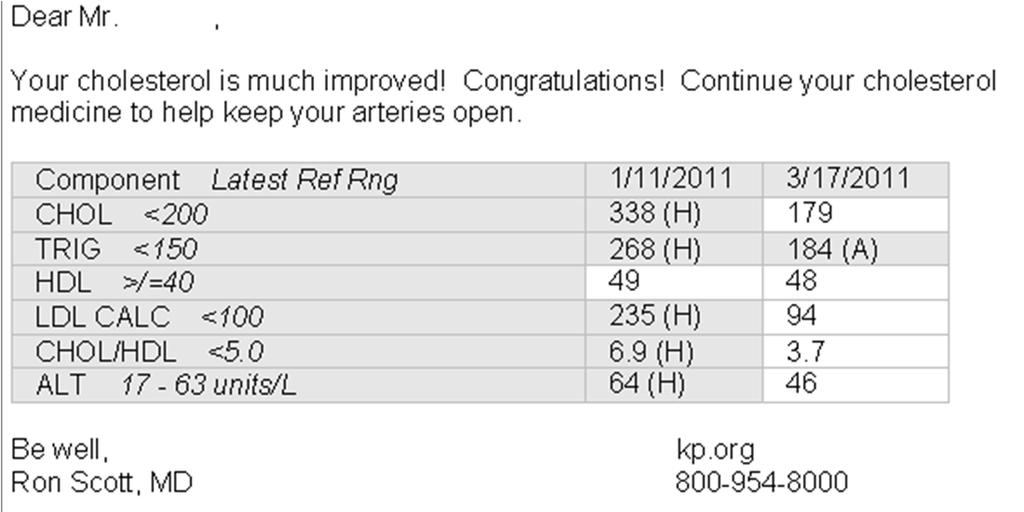


20 Encouraging Letter Safety, intolerance and barriers 20
21 Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study Lancet Nov 24, 2010 Increased baseline ALT increased statin benefit? GREACE study: rrr of recurrent cardiovascular event Elevated liver tests NAFLD: 68% Normal liver function: 39% Consistent with other studies that those with NAFLD and steatohepatitis are at higher CV risk and may benefit more from statins. The FDA statin labeling change 2/28/12 revised to remove the need for routine periodic monitoring of liver enzymes. 21
22 Rosuvastatin risk of new DM JUPITER rosuvastatin 20 mg daily: In those without RF for DM: 86 CV events prevented, and 0 cases of increased DM. In those with RF for DM: 134 CV events prevented (MI stroke, death) and 54 new cases of DM. (28% increase) 40 day acceleration of progression to DM. Compare to 55% reduced MI, 44% reduced combined endpoint, 20% lower mortality. DM risk drives NNH estimate of 63- Lancet 2012; 380: Atorvastatin risk of new DM Atorvastatin 80 mg overall OR 1.15 of New DM RF: FBS > 100, TG > 150, BMI > 30, HTN JACC, Jan Am J Car, Jan
23 statin muscle issues Risk Factors: interacting meds, statin dose relative to max, older age, female, cirrhosis... Check and treat high TSH (hypothyroid) before starting therapy. If muscle symptoms, double check if recent TSH. Consider treating low vitamin D. About 90% resolution of myopathy in 3 small studies. CoQ10, creatine,...? Muscle Risk lova simva prava rosuva atorva % LDL 20 mg 10 mg 20 mg % 40 mg 20 mg 40 mg mg 34% 80 mg 40 mg 80 mg 5 mg 20 mg 41% mg mg 40 mg 48% mg 80 mg 53% mg 58% Adapted from SLCO1B1 in Clin Pharm Ther. 2009;87(1):130-3 And FDA potency table 23

24 Muscle SE - options Low dose statin (relative to max) often with better tolerance. atorvastatin 10 mg daily 34% lowering. rosuvastatin 5 mg daily 41% lowering. If still not tolerating decrease frequency to 1-2 x a week atorvastatin or rosuvastatin most studied and long acting. If not tolerate multiple statins, red yeast rice? Red Yeast Rice has issues Arch Intern Med Oct
25 If non adherent, ask is cost a barrier? MFA program for patients that qualify. Mail order pharmacy incentive (3 months for cost of 2) Some Commercial Plans: Atorvastatin is not on KP CA Preventive Care Drug list, resulting in more copays and cost sharing than other generic statins. Medicare Senior Advantage Individual Plan patients make up 50% o our Medicare (age>65) patients. Tier 1 copay: $ 6 for 100 day supply with Mail Order. Simvastatin, lovastatin. Tier 2 copay: $ 14 for 100 day supply with Mail Order. Atorvastatin, pravastatin. Beyond Statins Priority is to optimize statin first, before going beyond statins to other lipid treatments. cost/yr % LDL atorvastatin 10 mg $ 34 % Red yeast rice $$ 17 % Add On Therapies ezetimibe 10 ½ tab $$$ (brand) 12 % Stanol Chews $$$ (OTC) 5-9 % Or sterols $$ (OTC) 9 % Bile acid sequest $$$ (gen) 10 % slo-niacin 500 bid $ (OTC) 5 % Factors to consider: tolerability, patient preference, cost, desired lipid changes, outcome evidence. 25


26 Ezetimibe (Zetia) Well tolerated, moves LDL well. Mixed results in imaging studies. Simvastatin / ezetimibe seemed to reduce events similar to equipotent statins in SHARP study. Await better event outcome data comparing statin alone to statin + ezetimibe (IMPROVE-IT). Brand cost about $500/yr (for ½ tab). Cost to pt depends on drug benefit. Plant Stanols / sterols 2 chews BID, $300/yr LDL 9% 1 chew BID, $150/yr, LDL 5%. 2 caps BID, $95/yr, LDL 9% NIH recommends 2 g daily. Dietary source is fat rich vegetables, fruits, and nuts Avg American gets 0.2 g daily Should not use in sitosterolemia - where pts get. xanthomas and CAD from inability to process plant stanols 26
, 1 scoop BID: $300 Colestipol powder or tab bid: $500 Colesevalam (Welchol) bid: > $2000 / yr SE: Constipation, dyspepsia, can raise elevated TG, interferes with")
27 Bile Acid Sequestrants (BAS) Lowers LDL about 23% (monotherapy) Favorable mono and combo outcome studies. Cholestyramine powder (Questran), 1 scoop BID: $300 Colestipol powder or tab bid: $500 Colesevalam (Welchol) bid: > $2000 / yr SE: Constipation, dyspepsia, can raise elevated TG, interferes with absorption of other meds (need to space timing). Slo-Niacin Slo-Niacin 500 mg bid LDL 5%, HDL 15% $ 51 / y Contraindicated with liver disease and active peptic ulcer disease. Glucose, uric acid Monotherapy studies benefit. Add on to statin no benefit in AIM-HIGH and HPS2-THRIVE Slo-Niacin 500 mg scored tabs ½ tab after dinner for 1 week, ½ tab bid for 1 week, then 1 tab po bid from then on. Time after dinner to decrease flushing. Flushing wanes over 2-3 months. 27


28 TG Therapy TG Guidance When statin indicated 1. If indication for statin, start statin. Statins are priority and can lower TG 20-30%. If TG are still > 200, 2. optimize potential contributing factors (hyperglycemia, excess alcohol, hypothyroid, obesity, medicines) and lifestyle interventions. If TG are still > 500, 3. Add/ or increase Omega-3 to 3-4 g daily and retest. If TG still > 500, then: consider add niacin consider intensify atorvastatin consider adding fenofibrate GFR > 30, use with sub-maximal dose statin 28


29 Both KP and Costco Omege 3 have 684 mg per softgel. (6 to 8 cents each) 5 caps / day = 3420 mg of Omega 3 for $110 / year. Diabetes: meds 4 CV reduction Screening: Hgb A1C > 6.5, Fasting Glucose > 126, 2 hr glu > ever. Metformin: Titrate up to 1000 mg bid right away, CV benefits. GFR use 500 bid. Statin: HEDIS measures performance in all DM. Guidelines rec: DM age > 40 or age < 40 with RF. Young DM with 80% lifetime CV risk. Aspirin 81 mg daily if 10 yr risk > 10% Men age with RF, all age Women age with RF. Lisinopril 20 mg for MA, HTN, or age > 55 with RF 29
30 Overview Lipids and CAD risk CVD is major killer and impacts morbidity Large statin benefit opportunity Treat high LDL (> 190) regardless of risk. Treat those at risk, regardless of LDL (>70) Optimizing Performance Identifying patients STAtin: Starts, Titrations, and Adherence Use tools to promote statins Safety / intolerance of statins Beyond statins Use tools and prevention to improve outcomes Use tools and prevention: integrated data / IT proactive care, CMSS, HC Artery graphic, patient relationship, clinical skill teamwork (care managers) Inexpensive generic atorvastatin, aspirin. To improve outcomes: Reduced CVD morbidity / mortality. Reduce costly CVD procedures, hospitalizations, and morbidity care. Better quality performance. Financial rewards for KP and for providers. 30
31 Question In JUPITER, rosuvastatin (Crestor) 20 mg (lowered LDL 50%) showed risk reduction of MI, and of combined endpoint of MI, stroke, revascularization, CV death of: A) MI 55% and combined endpoint 44%. B) MI 50% and combined endpoint 40%. C) MI 44% and combined endpoint 33%. 31
Implementation of CV Risk and. Dyslipidemia Guidelines. Impact on Americans 11/25/2014. Summary Implementing new. Dyslipidemia Guidelines
 Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Achieving Lipid Goals: 2008 Update. Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy
 Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Qué factores de riesgo lipídicos debemos controlar? En qué medida?
 Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
High ( 50%) Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ
 Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology
 Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study
 Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Presentation title. Better Health Care For Greater Cleveland Learning Collaborative March 5, Ron Adams, MD Regional Chief Internal Medicine
 Better Health Care For Greater Cleveland Learning Collaborative March 5, 2010 Presentation title Ron Adams, MD Regional Chief Internal Medicine SUB TITLE HERE Prevent Heart Attacks and Strokes Every Day
Better Health Care For Greater Cleveland Learning Collaborative March 5, 2010 Presentation title Ron Adams, MD Regional Chief Internal Medicine SUB TITLE HERE Prevent Heart Attacks and Strokes Every Day
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus
 Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Lipids: Translating Studies into Practice. WD04: Cortney Joneikis, MD, MS Bob Gleeson, MD Jeff Whittle, MD, MPH
 Lipids: Translating Studies into Practice WD04: Cortney Joneikis, MD, MS Bob Gleeson, MD Jeff Whittle, MD, MPH Discussants: Bob Gleeson, MD Assistant Professor of Medicine, General Internal Medicine Medical
Lipids: Translating Studies into Practice WD04: Cortney Joneikis, MD, MS Bob Gleeson, MD Jeff Whittle, MD, MPH Discussants: Bob Gleeson, MD Assistant Professor of Medicine, General Internal Medicine Medical
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane
 Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Targeting Lipids Strategies for Patients with Cardiometabolic Risk
 Targeting Lipids Strategies for Patients with Cardiometabolic Risk Faculty Disclosure David G. Carmouche, MD Director, Center for Cardiovascular Disease Prevention Baton Rouge Clinic ASH Specialist in
Targeting Lipids Strategies for Patients with Cardiometabolic Risk Faculty Disclosure David G. Carmouche, MD Director, Center for Cardiovascular Disease Prevention Baton Rouge Clinic ASH Specialist in
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Preventing Cardiovascular Disease With Lipid Management: Matching Therapy to Risk
 PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Is it an era for statin for life?
 Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for