Angina Luis Tulloch, MD 03/27/2012
|
|
|
- Elijah Butler
- 6 years ago
- Views:
Transcription
1 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI, and right ventricular MI Work-up Telemetry Serial 12 lead ECGs Troponins and CK-MB q8 hours x3 Electrolytes (K, Ca, Mg), Cr, CBC, coags, urine toxicology, FLP Management STEMI* Medical therapy Reperfusion NSTEMI, UA Medical therapy Early risk stratification TIMI 0-2: Conservative management (=Stress testing) TIMI 3-4: MKSAP 15 recommends invasive management, but these patients usually undergo invasive management only if stress testing suggests that the patient may benefit from PCI^ TIMI 5-7: Invasive management (=PCI within 48 hours; Avoid fibrinolysis) TIMI score (1 point per item) Age 65 yrs 3 coronary artery ds RFs 50% coronary stenosis on angiography ST-segment change 0.6 mm 2 anginal episodes 24 hours prior to presentation Elevated cardiac enzymes Use of aspirin within 7 days of presentation *Or any ACS p/w: Persistent or recurrent rest angina despite optimized medical therapy Cardiogenic shock New severe ventricular dysfunction Hemodynamic instability d/t a new structural defect (mitral regurgitation, VSD) Sustained VT or VF Wellens sign/syndrome ^In practice, patients undergo invasive management w/out prior stress testing only if they have new ST depressions > 1mm, increased cardiac enzymes, (worsening angina over the past 2 months, or recent PCI or CABG) Early Medical therapy Drug Dose Contraindications Oxygen 2-4 LPM Aspirin 325 mg po daily
2 Nitroglycerin Morphine sulfate Βeta-blocker Clopidogrel Anticoagulant 0.4 mg sl q5 minutes PRN (up to 3 doses) 2-4 mg iv q10 minutes PRN (may increase dosage by 2-8 mg every 10 minutes) atenolol mg po bid or metoprolol tartrate mg po q6-12 hours 300 mg po once (600 mg po once if PCI w/in 24 hours and 75 mg po once in patients >= 75 yo regardless of management type) Initially UFH (no bolus protocol w/ PTT goal 60-80) then you may switch to LMWH treating for 2-8 days duration Right ventricular MI SBP <90, pulse <50, second degree AVB (only Mobitz type II?); Alternatively may use a CCB Ongoing/recent bleeding, platelets <50,000 Ongoing/recent bleeding; Alternatively may use bivalirudin or fondaparinux Late medical therapy and risk stratification (prior to discharge) Continue ASA 81 mg daily Clopidogrel 75 mg daily BMS: x1-12 months DES: x6-12 months Medical therapy: x9-12 months Continue beta-blocker Start a high-dose statin and an ACE-inhibitor or ARB Measure resting LVEF In patients treated w/ medical therapy only, stress testing Complications and broad treatment principles Complication Broad treatment principles Arrhythmias Avoid arrhythmogenic medications Keep K Rate and/or rhythm control Cardiogenic shock Vasopressors (dobutamine) + HF Avoid CCB Consider pre-load reduction and loop diuretics Contact CTS in patients w/ structural causes leading to HF (papillary muscle rupture causing MR or VSD) Recurrent MI Revascularization
3 Chronic stable angina Choosing a stress test Diagnostic: Patient's pre-test probability of coronary artery disease? Pre-test probability (Diamond NEJM 1979, Weiner NEJM 1979)* Age Non-anginal Atypical angina Typical angina^ M F M F M F ~ ~ *Not included: Prior ACS, on digitalis, resting EKG w/ LBBB or LVH, inability to reach 85% max exercise capacity ^Typical angina: 1) Substernal chest pain or discomfort 2) Aggravated by activity or psychological stress 3) Alleviated by rest or NTG ^Atypical angina: 2/3 ^Non-anginal: 1/3 or 0/3 ~ Low pre-test probability per MKSAP 15 Need to localize lesions or determine cardiac viability? Resting EKG Can the patient exercise? Co-morbidities General considerations Obtain a stress test only in patients with intermediate or high pre-test probabilities Exercise stress testing is superior to pharmacologic stress testing Intermediate or high pre-test probability Need to localize lesions or determine cardiac viability?* Abnormal EKG? On digitalis? No Yes to any Able to exercise? Able to exercise? Yes No Yes No Stress EKG Pharmacologic stress test Exercise stress test *Usually needed in patients in whom you re considering revascularization (patients w/ high pre-test probability or w/ prior revascularization and worsening symptoms) Pharmacologic stress test Types of pharmacologic stress test Pharmacologic stress test Contraindications Prior to the stress test Dobutamine TTE or NPS Severe arrhythmias or HTN Hold beta-blockers Adenosine or dipyridamole NPS *Nuclear perfusion scan Severe airway disease (not Lexiscan = regadenoson) and high degree second and third degree) AVB Hold caffeine and theophylline















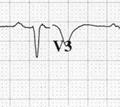
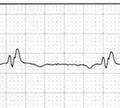
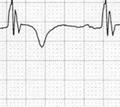
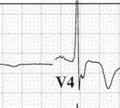
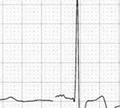
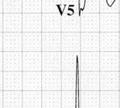
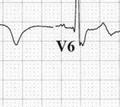
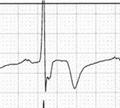
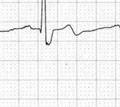
4 EKG atlas - ACS LBBB Ddx: A Pw precedes every QRS QRS > 120 ms Absent qw in I, (avl), V5, V6 Broad notched or slurred Rw in I, avl, V5, V6 ST and Tw usually opposite in direction to QRS QRS and Tw pos Okay QRS and depressed ST or Tw neg Suggests underlying ischemia Ventricular tachycardia and accelerated idioventricular rhythm: Has AV dissociation Ventricular pacing: Pacing spike replaces Pw WPW: Has a short PR Wellens sign/syndrom me = Critical plad stenosis in patients w/ UA Deep symmetric TWI and/or biphasic TW usually in V2 and V3, but may occur in V1-V6 when the patient is w/out chest pain RBBB w/ deep symmetric TWI in V3-V4 and biphasic TW in V5-V6




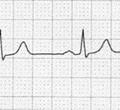
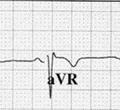
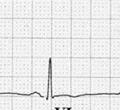
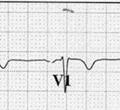
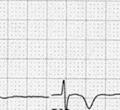
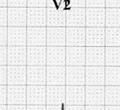
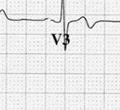
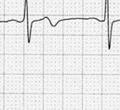
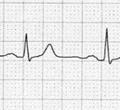
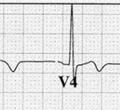
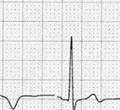
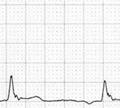
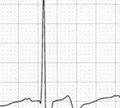
5 Deep symmetric TWI in V1-V2 and biphasic TW in V3-V5 Biphasic Tw Right ventricular MI Suspect in patients w/ inferior wall STEMI + STE in III > STE in II STE in V1 ST in V1 more upright than ST in V2 Confirm w/ STE anywheree from V3R-V6R Posteriorr wall MI Suspect in patients who have the following changes in V1-V3 Horizontal STD (as opposed to down-sloping or up-sloping) Very tall Rw Upright Tw Confirm w/ STE anywheree from V7-V9
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
2018 Acute Coronary Syndrome. Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute
 2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Pre Hospital and Initial Management of Acute Coronary Syndrome
 Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
Pre Hospital and Initial Management of Acute Coronary Syndrome Dr. Muhammad Fadil, SpJP 3rd SymCARD 2013 Classification of ACS ESC Guidelines for the management of Acute Coronary Syndrome in patients without
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD
 Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Evaluation and Management of the Patient with Cardiac Disease for Non-Cardiac Surgery WINTER CONFRENCE 2016 RONY GORGES, MD 67 yo man Asymptomatic carotid stenosis, CEA planned Golfs regularly, walks and
Case Question. Evaluation of Chest pain in the Office and Cardiac Stress Testing
 Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Evaluation of Chest pain in the Office and Cardiac Stress Testing Chad Link, DO FACC Sparrow Hospital Thoracic and Cardiovascular Institute Chairman- TCI Cardiology Section Disclosures Speakers Bureau
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Early Management of Acute Coronary Syndrome
 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Chapter 76 Acute Coronary Syndromes Part A
 Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
Marcin Dada, MD December 03, 2013
 STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
TOPICS IN EMERGENCY MEDICINE SEMI-FINAL
 RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
RISK ASSESSMENT IN PATIENTS WITH CHEST PAIN Nora Goldschlager, M.D. FACP, FACC, FAHA, FHRS Cardiology - San Francisco General Hospital UCSF Disclosures: None 1 CHEST PAIN NOT DUE TO MYOCARDIAL ISCHEMIA
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why?
 Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Severe Hypertension. Pre-referral considerations: 1. BP of arm and Leg 2. Ambulatory BP 3. Renal causes
 Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Severe Hypertension *Prior to making a referral, call office or Doc Halo, to speak with a Cardiologist or APP to discuss patient and possible treatment options. Please only contact the patient's cardiologist.
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Practitioner Education Course
 2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
2015 Practitioner Education Course ST Elevation Myocardial Infarction 2 Pathology Concept of vulnerable plaque Mild Atheroma Diagnosis IVUS OCT 3 Diagnosis This is based on : Clinical History ECG Changes.
Adult Acute Myocardial. Infarction
 Adult Acute Myocardial Infarction Preclinical stable CAD Acute Coronary Syndrome No cardiac enzyme elevation cardiac enzyme elevation Ischemia Cell Injurydeath UA NSTEMI STEMI Definition of Coronary Artery
Adult Acute Myocardial Infarction Preclinical stable CAD Acute Coronary Syndrome No cardiac enzyme elevation cardiac enzyme elevation Ischemia Cell Injurydeath UA NSTEMI STEMI Definition of Coronary Artery
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
* * FORM REV. 02/2019 Page 1 of 4. TNKASE (tenecteplase) / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:
 / ACUTE STEMI ORDERS SCHEDULED MEDICATIONS:") 1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
1. Is this a CMS inpatient only procedure? Yes, admit as inpatient, proceed to # 3 No, proceed to # 2 2. Do you expect that the patient s condition will require a hospital stay that will cross two midnights
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Therapies for ACS The Articles You ve Got to Know!!
 Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Cardiogenic Shock. Carlos Cafri,, MD
 Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Cardiogenic Shock Carlos Cafri,, MD SHOCK= Inadequate Tissue Mechanisms: Perfusion Inadequate oxygen delivery Release of inflammatory mediators Further microvascular changes, compromised blood flow and
Treatment of Acute Coronary Syndromes
 Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Treatment of Acute Coronary Syndromes UC SF Jeffrey Tabas, M.D. sf g h Associate Professor UCSF School of Medicine Emergency Services, San Francisco General Hospital Objectives Review the updated AHA/ACC
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
10/22/16. Lay of the land. Definition of ACS. Why do we worry about ST elevations?
 Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
DO NOT SUBMIT OR FAX THIS PAGE TO COR F M L DD MM YY
 DO NOT SUBMIT OR FAX THIS PAGE TO COR Patient # Patient Initials of Birth Medical Record Number F M L DD MM YY Patient Name Address Telephone (home) Telephone (work) Expected 6-month Follow-up Family Physician
DO NOT SUBMIT OR FAX THIS PAGE TO COR Patient # Patient Initials of Birth Medical Record Number F M L DD MM YY Patient Name Address Telephone (home) Telephone (work) Expected 6-month Follow-up Family Physician
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
Cardiology Updates: Syncope and Stress Testing. Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital
 Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
Cardiology Updates: Syncope and Stress Testing Kathleen Morris, DO Cardiology Fellow St. Vincent Hospital Disclosures NONE PART ONE: Let s start with SYNCOPE Objectives: Definition of Syncope Brief review
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
ISCHEMIC HEART DISEASE
 ISCHEMIC HEART DISEASE Introduction Coronary heart disease (CHD) is the most common form of heart disease An estimated 330 000 people have a myocardial infarct each year Approximately 1.3 million people
ISCHEMIC HEART DISEASE Introduction Coronary heart disease (CHD) is the most common form of heart disease An estimated 330 000 people have a myocardial infarct each year Approximately 1.3 million people
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
CHRONIC CAD DIAGNOSIS
 CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
CHRONIC CAD DIAGNOSIS Chest Pain Evaluation 1. Approach to diagnosis of CAD 2. Classification of chest pain 3. Pre-test likelihood CAD 4. Algorithm for chest pain evaluation in women 5. Indications for
Acute Coronary Syndromes: Review and Update
 Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology
Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Cardiac Arrhythmias in Acute Coronary Syndrome. Roj Rojjarekampai, MD Thammasart Hospital 26/5/59
 Cardiac Arrhythmias in Acute Coronary Syndrome Roj Rojjarekampai, MD Thammasart Hospital 26/5/59 OUTLINE Management of tachy and brady-arrhytmia related ACS : AF : VA [ sustained VT /VF] : conduction disturbance
Cardiac Arrhythmias in Acute Coronary Syndrome Roj Rojjarekampai, MD Thammasart Hospital 26/5/59 OUTLINE Management of tachy and brady-arrhytmia related ACS : AF : VA [ sustained VT /VF] : conduction disturbance
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
9/2/2016 CARDIOLOGY TESTING WHAT TO ORDER WHEN REFERENCE OBJECTIVES
 CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
ECG in coronary artery disease. By Sura Boonrat Central Chest Institute
 ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
Myocardial infarction
 CHAPTER-I CARDIOVASCULAR SYSTEM Myocardial infarction SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. Venugopal Pharm.D Assistant Professor Department of Pharm.D Kriahna Teja Pharmacy College,Tirupati. Definition
CHAPTER-I CARDIOVASCULAR SYSTEM Myocardial infarction SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. Venugopal Pharm.D Assistant Professor Department of Pharm.D Kriahna Teja Pharmacy College,Tirupati. Definition
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Choosing the Right Cardiac Test. Outline
 Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Choosing the Right Cardiac Test Atif Qasim, M.D., M.S.C.E. University of California, San Francisco Disclosures: None 2013 Outline Focus on choosing the optimal tests for coronary disease evaluation Overview
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
The PAIN Pathway for the Management of Acute Coronary Syndrome
 2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Objectives. Acute Coronary Syndromes; The Nuts and Bolts. Overview. Quick quiz.. How dose the plaque start?
 Objectives Acute Coronary Syndromes; The Nuts and Bolts Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Compare and contrast pathophysiology of unstable angina (UA), non-st segment elevation
Objectives Acute Coronary Syndromes; The Nuts and Bolts Michael P. Gulseth, Pharm. D., BCPS Pharmacotherapy II Spring 2006 Compare and contrast pathophysiology of unstable angina (UA), non-st segment elevation
Current Treatment Of Ischemic Heart Disease In the United States: An Overview. By Dr Gary Mo
 Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Current Treatment Of Ischemic Heart Disease In the United States: An Overview By Dr Gary Mo 1 Ischemic Heart Disease in the US 1. Cardiovascular disease remains the most common cause of death and is responsible
Acute Coronary Syndrome (ACS): Disease Management. Acute Coronary Syndrome (ACS)
: Disease Management. Acute Coronary Syndrome (ACS)") Acute Coronary Syndrome (ACS): Disease Management Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com 2009 1 Acute Coronary Syndrome (ACS) ST Elevation STEMI No ST Elevation NSTEMI Unstable
Acute Coronary Syndrome (ACS): Disease Management Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com 2009 1 Acute Coronary Syndrome (ACS) ST Elevation STEMI No ST Elevation NSTEMI Unstable
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Cardiac Ischemia ECG Workshop
 Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
VHA Performance Measurement In Cardiac Care
 VHA Performance Measurement In Cardiac Care A Map for VHA Cardiac Performance Measurement in FY 2005 and beyond Roxane Rusch, BSN, MPA, RN Department Of Veterans Affairs Office of Quality and Performance
VHA Performance Measurement In Cardiac Care A Map for VHA Cardiac Performance Measurement in FY 2005 and beyond Roxane Rusch, BSN, MPA, RN Department Of Veterans Affairs Office of Quality and Performance
(ClinicalTrials.gov ID: NCT ) Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris
 Title: The Italian Elderly ACS Study Author: Stefano Savonitto. Date: 29 August 2011 Meeting: ESC congress, Paris") Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
Early aggressive versus initially conservative strategy in elderly patients with non-st- elevation acute coronary syndrome: the Italian randomised trial (ClinicalTrials.gov ID: NCT00510185) Stefano Savonitto,
2018 HPN Provider Summary Guide. Adult Cardiology Patients (18 Years and Older) Referral Guidelines
 Referral Guidelines") 12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
12.2 CARDIOLOGY REFERRAL GUIDELINES Contracted Group: Southwest Medical Associates For Appointments: 888 S. Rancho Las Vegas, NV 89109 Phone: (702) 877-8654 Fax: (702) 242-7998 Adult Cardiology Patients
Maria Angela S. Cruz-Anacleto, MD
 Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Maria Angela S. Cruz-Anacleto, MD 57/Female Menopausal Non-HTN, non-dm Hypothyroid (s/p RAI 1997) Levothyroxine 100 ug OD 5 Months PTA Chest discomfort Stress Echocardiography 5 Months PTA Chest discomfort
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이
 Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Role of echocardiography in the assessment of ischemic heart disease 분당서울대학교병원윤연이 Outline Evaluation of Chest pain Evaluation of MI complications Prediction of Outcomes Evaluation of Chest pain Evaluation
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
Cardiogenic Shock in Acute MI
 Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
Cardiogenic Shock in Acute MI Mark Sheldon, MD UNMH Interventional Cardiology Objectives Overview Treatment Definition Shock profiles Causes Medical Mechanical Illustrative case Questions? Revascularization
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital
 What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
What is a myocardial infarction and how do we treat it? Paul Das Consultant Cardiologist North Wales Cardiac Centre Glan Clwyd Hospital What is a myocardial infarction? THEY AINT WHAT THEY USED TO BE Case
Coronary Heart Disease. Iqbal Malik
 Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
Coronary Heart Disease Iqbal Malik Pathophysiology IHD Case chest pain Question -interactive What is the result of the exercise test? 1. negative 2. positive 3. equivocal 4. other Q2 answer STEMI! What
Exercise Test: Practice and Interpretation. Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine
 Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008
Exercise Test: Practice and Interpretation Jidong Sung Division of Cardiology Samsung Medical Center Sungkyunkwan University School of Medicine 2 Aerobic capacity and survival Circulation 117:614, 2008