Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine
|
|
|
- Solomon Payne
- 6 years ago
- Views:
Transcription


1 Simon A. Mahler MD, MS, FACEP Associate Professor Department of Emergency Medicine Wake Forest School of Medicine
2 Research funding: American Heart Association Donaghue Foundation/ Association of American Medical Colleges NIH: Heart Lung and Blood Institute Author for Up-to-Date No conflict of interest No commercial bias: No products or devices will be discussed
3 Introduction: Heart disease & Chest Pain Role of Observation Units for patients with chest pain Observation Unit Chest Pain Care Overview Inclusion/Exclusion Criteria Protocols and Testing Strategies

4 #1 cause of death in the US Chest pain is a top cause of US ED visits Emergency providers care for patients with chest pain on virtually every shift 8-10 million patients annually

5 Providers are tasked with determining if the patient s pain is cardiac or noncardiac High stakes decision for providers and patients Patients: high risk for morbidity and mortality from an incorrect diagnosis Providers: high risk for a medical malpractice claim
6 Medical malpractice Chest pain is the highest per claim payout for emergency physicians ACC/AHA guidelines: If there is concern for ischemic chest pain, patients should receive comprehensive evaluation: serial troponins followed by stress testing or angiography

7 Most patients with chest pain receive comprehensive hospital-based testing Annual cost $10-13 Billion ~2-5% of patients with AMI are inappropriately discharged from the ED every year. Patients discharged with AMI have an 11-25% risk of death
 The most risk-averse quartile of providers had higher admission")
8 Significant variability among providers in their chest pain care Pines et al. AJEM 2010; Measured providers risk aversion using a risk taking scale(rts) The most risk-averse quartile of providers had higher admission rates compared to the least risk-averse quartile. (P <0.001)
9 Mitigate risk and reduce care variability Protocol-driven care Comprehensive chest pain evaluations Potential answer to inefficiency Avoids inpatient admissions Safe and decreases length of stay and costs relative to an inpatient strategy.* *Gomez MA, et al. J Am Coll Cardiol. Jul 1996;28(1): Goodacre S, et al. BMJ. Jan ;328(7434):254. Jagminas L, et al. Am J Emerg Med. Mar 2005;23(2): Roberts RR, et al. JAMA. Nov ;278(20): Zalenski RJ, et al. Arch Intern Med. May ;157(10): Graff L. Md Med. Spring 2001;Suppl:40-42.
10 Improved rate of diagnosis of ACS in hospitals with OU -Graff et al Physicians without access to OU may have difficulties completing a rapid cardiac protocol -Ellrodt et al 34% of low risk chest pain patients were not discharged at 3 days Approximately half the cost as Inpatient care - shown in multiple clinical trials

11 ACC/AHA: Class I recommendation to manage patients with possible ACS in OUs Institute of Medicine (2006): clinical decision units reduce boarding and diversion, avoid expensive hospitalization, and appear to contribute to improved management of common ambulatory-care sensitive conditions.
12 Two Questions: What is the likelihood that presenting symptoms represent ACS? Serial troponins and ECGs -Class I recommendation ACC/AHA Guidelines What is the likelihood of an ACS event occurring in the near future? Stress testing or CT coronary angiography -Class I recommendation ACC/AHA Guidelines
 Objective cardiac testing (Excludes UA) Chest pain not from ACS Chest pain not from")
13 Primary evaluation Emergency Department History Physical Exam Electrocardiogram First set of cardiac markers (may not be needed for clearly non-cardiac chest pain) Possible ACS Definite ACS or High risk features Secondary evaluation Observation unit or inpatient Serial ECGs Serial Cardiac Markers (Excludes AMI) Objective cardiac testing (Excludes UA) Chest pain not from ACS Chest pain not from ACS Treat alternative diagnosis Admission to coronary care unit or revascularization Treat alternative diagnosis
?")
14 Successful utilization of an OU chest pain pathway requires adequate patient selection Are they absolutely noncardiac? Send them home. Do they need a cath (positive biomarkers, ECG changes, hemodynamically unstable)? Admit

 Alternative: TIMI")
15 Evaluates a patient s: History EKG Age Risk factors Troponin Validated in >6,000 patients Observation Care HEART Score (4-6) Alternative: TIMI (0-2)

16 Low Risk Early discharge Discharged from ED with follow up with a primary care physician No stress testing or cardiac imaging High Risk Further evaluation Observation Unit or inpatient ward Patients identified for stress testing or cardiac imaging

17 Exclusion criteria Troponin > 99 th percentile New EKG changes High risk (Known CAD) Disruptive behavior Hemodynamic instability Active CHF New or uncontrolled dysrhythmias Contraindications to stress testing or coronary CT Admission criteria Recurrent chest pain EKG or biomarker changes Positive stress test Hemodynamic instability

18 Has a single medical issue No acute psychiatric issues Including intoxication Chronic pain patients do not do well in OU
19 Good evidence that cocaine chest pain can be observed without stress testing chemical/ecg rule out suffices Hemodynamically stable, ECG nondiagnostic, initial troponin negative, and chest pain free
20 ACC/AHA Guidelines Class I Recommendation Patients with definite or possible ACS but whose initial 12-lead ECG and cardiac marker levels are normal should be observed in a facility with cardiac monitoring (eg, chest pain unit), and a repeat ECG and cardiac marker measurement should be obtained (Level of Evidence: B)
21 Goal of serial markers is to detect those who have already infarcted - Evolving MI 4% of ED patients with possible ACS will have an EMI and an ECG that is not consistent with MI / ischemia 0 3 hours 6 hours Onset of ischemia First troponin not elevated Second troponin elevated

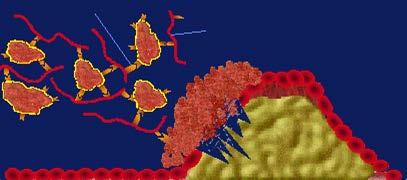
22 Activated GP llb/llla Fibrinogen And/or Positive Troponin
23 ACC/AHA Guidelines Class I Recommendation If the follow-up 12-lead ECG and cardiac marker measurements are normal, a stress test (exercise or pharmacological) to provoke ischemia may be performed in the ED, in a chest pain unit, or on an outpatient basis shortly after discharge. Low-risk patients with a negative stress test can be managed as outpatients. (Level of Evidence: C)

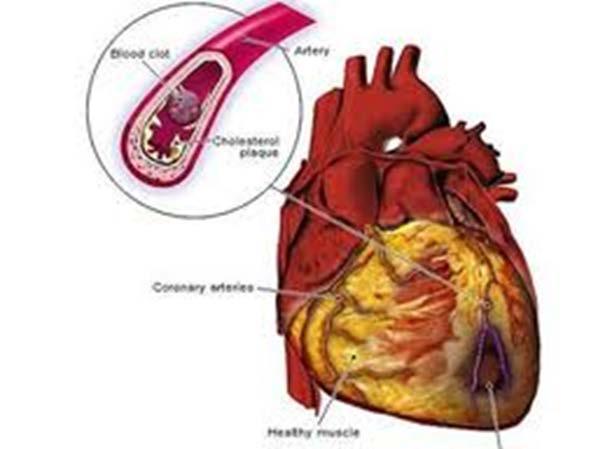
24 Fixed obstructions causing inducible ischemia UA Risk of near-term MI and cardiac death
25 Stress ECG (1-3) Sensitivity 68% for significant CAD Specificity 77% for significant CAD Stress echo (4) 80% for significant CAD 84% for significant CAD Stress nuclear imaging(5-6) 86-97% for shortterm cardiac events 88-90% for shortterm cardiac events Negative predictive value for adverse cardiac events >98%
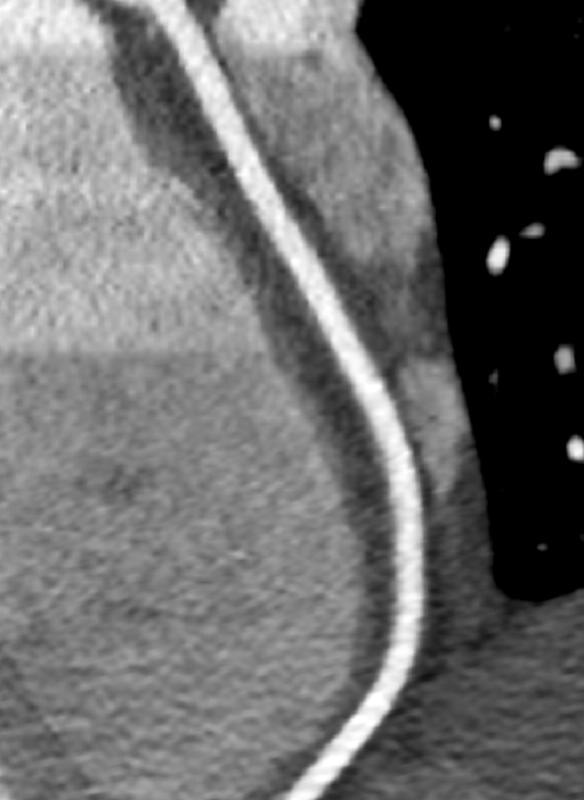
26 Class IIa recommendation: In patients with suspected ACS with a low or intermediate probability of CAD, in whom the follow-up 12-lead ECG and cardiac biomarkers measurements are normal, performance of a noninvasive coronary imaging test (i.e., CCTA) is reasonable as an alternative to stress testing. (Level of Evidence: B)


27 1-year event rate following a normal CCTA = 0.17% Stress echo = 0.54%; stress nuclear = 0.45% Hulten EA, et al J Am Coll Cardiol.
28 Cost of index hospitalization $4,500 $4,000 $3,500 $3,000 $2,500 $2,000 $1,500 $1,000 $500 $0 Immediate CCTA CCTA in OU Stress test inou Inpatient CTA less costly than hospital admission or stress testing Chang et al. (Acad Emerg med 2008)
29 Risk factors for poor image quality: High heart rate Diabetes Hypertension Older age History of CAD Bamberg et al. European Journal of Radiology (2010).
30 Highly dependent on the imaging team Earlier techniques were routinely msv 2007 median 12 msv* 10 msv common using dose reduction techniques** Now some scans being obtained with <1 msv *Hausleiter J et al. JAMA 2009 ** Raff et al. JAMA 2009 Heilbron and Leipsic, Can J Cariol, 2010

31


32 >4,000 patients with chest pain present to ED annually >600 patients per year with chest pain managed in OU Most receive stress echocardiography ACS rates very low 1-2% Admit rate ~12% Staffing Nurse -24 hours Mid-level coverage 8a-Mn ED physician always available, 8a

33 Telemetry Q 4 vitals Oxygen NPO at midnight 0,4,6 hours

34 Stress test or Coronary CT Serial ECGS IV access Meds ACS Pain & nausea
35 Serial ECGs and troponins (0,4,6) Objective cardiac testing availability: Stress Echo 7 days / week Coronary CT weekdays Cardiac MRI weekdays

36 OU provides high value care for patients with chest pain Safe, efficient, lower cost Patient selection for OU is key Lower-risk patients, but not very-low-risk Single medical issue OU protocol should involve: Serial troponins and ECGs Rule out evolving MI/ acute ACS event Stress testing or coronary CT Prediction of near-term ACS risk
High Value Evaluation of Chest Pain. Zoom Tips
 High Value Evaluation of Chest Pain California Quality Collaborative s Cardiology Webinar Series Webinar 1 December 7, 2017 Zoom Tips Attendees are automatically MUTED upon entry Refrain from using the
High Value Evaluation of Chest Pain California Quality Collaborative s Cardiology Webinar Series Webinar 1 December 7, 2017 Zoom Tips Attendees are automatically MUTED upon entry Refrain from using the
Current and Future Imaging Trends in Risk Stratification for CAD
 Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Current and Future Imaging Trends in Risk Stratification for CAD Brian P. Griffin, MD FACC Department of Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic Disclosures: None Introduction
Troponin = 35. Objectives. Low Risk Chest Pain. Does this patient have ACS? Does this patient have ACS? Objectives
 Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
Objectives Low Risk Chest Pain Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine Improve speed and accuracy in assessing patients with possible ACS! Avoid pitfalls
The 2016 NASCI Keynote: Trends in Utilization of Cardiac Imaging: The Coronary CTA Conundrum. David C. Levin, M.D.
 The 2016 NASCI Keynote: Trends in Utilization of Cardiac Imaging: The Coronary CTA Conundrum David C. Levin, M.D. October 16, 2016 MPI Utilization Rates/1000[includes PET] total radiologists 2014 total
The 2016 NASCI Keynote: Trends in Utilization of Cardiac Imaging: The Coronary CTA Conundrum David C. Levin, M.D. October 16, 2016 MPI Utilization Rates/1000[includes PET] total radiologists 2014 total
Chest Pain Wave I Webinar. May, 30 th 2017
 Chest Pain Wave I Webinar May, 30 th 2017 Disclaimer The project described is supported by Funding Opportunity Number CMS-1L1-15-002 from the U.S. Department of Health & Human Services, Centers for Medicare
Chest Pain Wave I Webinar May, 30 th 2017 Disclaimer The project described is supported by Funding Opportunity Number CMS-1L1-15-002 from the U.S. Department of Health & Human Services, Centers for Medicare
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
FFR-CT Not Ready for Primetime
 FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
FFR-CT Not Ready for Primetime Leslee J. Shaw, PhD, MASNC, FACC, FAHA, FSCCT R. Bruce Logue Professor of Medicine Co-Director, Emory Clinical CV Research Institute Emory University School of Medicine Atlanta,
Version 4.4. Institutional Outcomes Report 2014Q3. National Outcomes Report Aggregation Date: Jan 12, :59:59 PM
 Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Version 4.4 Institutional Outcomes Report 2014Q3 National Outcomes Report 999997 Aggregation Date: Jan 12, 2015 11:59:59 PM Publish Date: Jan 29, 2015 If User desires to publish or otherwise distribute
Low Risk Chest Pain. Objectives. Disclosure. Case 1. Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine
 Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients
 Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Optimal testing for coronary artery disease in symptomatic and asymptomatic patients Alexandre C Ferreira, MD Clinical Chief of Cardiology Jackson Health System Director, Interventional Cardiology Training
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
CHEST PAIN CDU INCLUSION CRITERIA
 CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
CHEST PAIN CDU INCLUSION CRITERIA No clinical criteria for ACS Stable vital signs Initial ECG and cardiac biomarkers not consistent with ACS Low to intermediate ACS risk (HEART score 0-6) [Ref 1, 2] Plan
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
When Should I Order a Stress Test or an Echocardiogram
 When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
When Should I Order a Stress Test or an Echocardiogram Updates in Cardiology 2015 March 7, 2015 Donald L. Lappé, MD, FAHA, FACC Chairman, Cardiovascular Department Medical Director, Intermountain Cardiovascular
The Value of Stress MRI in Evaluation of Myocardial Ischemia
 The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
The Value of Stress MRI in Evaluation of Myocardial Ischemia Dr. Saeed Al Sayari, MBBS, EBCR, MBA Department of Radiology and Nuclear Medicine Mafraq Hospital, Abu Dhabi United Arab Emirates Introduction
Overview. Health and economic burden of coronary artery disease (CAD) Pitfalls in care of patients suspected of having CAD
 Pitfalls in care of patients suspected of having CAD") Quality Challenges and Pitfalls in the Evaluation of Patients with Suspected Heart Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine
Quality Challenges and Pitfalls in the Evaluation of Patients with Suspected Heart Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine
New Stable Chest Pain Guidance in the UK NICE to have, difficult to implement
 New Stable Chest Pain Guidance in the UK NICE to have, difficult to implement Dr Tim Fairbairn MBChB, MRCP, PhD Consultant Imaging Cardiologist Liverpool Heart and Chest Hospital, United Kingdom 2010 Risk
New Stable Chest Pain Guidance in the UK NICE to have, difficult to implement Dr Tim Fairbairn MBChB, MRCP, PhD Consultant Imaging Cardiologist Liverpool Heart and Chest Hospital, United Kingdom 2010 Risk
. θωρακικούάλγουςστα εξωτερικά ιατρεία
 . θωρακικούάλγουςστα εξωτερικά ιατρεία Ε.Γ. ΑΛΑΜΑΓΚΑ ΚΑΡ ΙΟΛΟΓΟΣ ιδάκτωρ Ιατρικής Σχολής ΑΠΘ ΓΕΝΙΚΗ ΚΛΙΝΙΚΗ ΘΕΣΣΑΛΟΝΙΚΗΣ ΕΠΙΣΤΗΜΟΝΙΚΟΣ ΣΥΝΕΡΓΑΤΗΣ Α ΚΑΡ ΙΟΛΟΓΙΚΗΣ ΚΛΙΝΙΚΗΣ ΝΟΣΟΚΟΜΕΙΟ ΑΧΕΠΑ Panic attack
. θωρακικούάλγουςστα εξωτερικά ιατρεία Ε.Γ. ΑΛΑΜΑΓΚΑ ΚΑΡ ΙΟΛΟΓΟΣ ιδάκτωρ Ιατρικής Σχολής ΑΠΘ ΓΕΝΙΚΗ ΚΛΙΝΙΚΗ ΘΕΣΣΑΛΟΝΙΚΗΣ ΕΠΙΣΤΗΜΟΝΙΚΟΣ ΣΥΝΕΡΓΑΤΗΣ Α ΚΑΡ ΙΟΛΟΓΙΚΗΣ ΚΛΙΝΙΚΗΣ ΝΟΣΟΚΟΜΕΙΟ ΑΧΕΠΑ Panic attack
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why?
 Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Screening for Asymptomatic Coronary Artery Disease: When, How, and Why? Joseph S. Terlato, MD FACC Clinical Assistant Professor, Brown Medical School Coastal Medical Definition The presence of objective
Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain
 Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain Michael Perera Advanced Trainee in General and Acute Medicine Leena Aggarwal Director, Medical
Unnecessary hospitalisation and investigation of low risk patients presenting to hospital with chest pain Michael Perera Advanced Trainee in General and Acute Medicine Leena Aggarwal Director, Medical
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Impact of use of the HEART score in chest pain patients. Judith Poldervaart, MD, PhD Julius Center
 Impact of use of the HEART score in chest pain patients Judith Poldervaart, MD, PhD Julius Center The HEART-score Diagnostic risk score for chest pain patients at ED 5 clinical elements Supports direct
Impact of use of the HEART score in chest pain patients Judith Poldervaart, MD, PhD Julius Center The HEART-score Diagnostic risk score for chest pain patients at ED 5 clinical elements Supports direct
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Reducing the Population Health Burden of Cardiovascular Disease
 Reducing the Population Health Burden of Cardiovascular Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine Disclosures: K23 HL116787
Reducing the Population Health Burden of Cardiovascular Disease Joseph A. Ladapo, MD, PhD Assistant Professor of Medicine Department of Population Health NYU School of Medicine Disclosures: K23 HL116787
Which Test When? Avoid the Stress of Stress Testing. Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute
 Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Which Test When? Avoid the Stress of Stress Testing Marc Newell, MD, FACC, FSCCT Minneapolis Heart Institute Outline Understand the importance of coronary artery disease assessment Understand the basics
Congreso Nacional del Laboratorio Clínico 2016
 Can biomarkers help us make a better use of cardiac imaging for myocardial ischaemia rule-out in the Emergency Department? Alessandro Sionis Director Acute and Intensive Cardiac Care Unit Hospital de la
Can biomarkers help us make a better use of cardiac imaging for myocardial ischaemia rule-out in the Emergency Department? Alessandro Sionis Director Acute and Intensive Cardiac Care Unit Hospital de la
Impact of Chest Pain Protocol Targeting Intermediate Cardiac Risk Patients in an Observation Unit of an Academic Tertiary Care Center
 Elmer ress Original Article J Clin Med Res. 2016;8(2):111-115 Impact of Chest Pain Protocol Targeting Intermediate Cardiac Risk Patients in an Observation Unit of an Academic Tertiary Care Center Tariq
Elmer ress Original Article J Clin Med Res. 2016;8(2):111-115 Impact of Chest Pain Protocol Targeting Intermediate Cardiac Risk Patients in an Observation Unit of an Academic Tertiary Care Center Tariq
Baseline Data Collection Tool
 Endorsed by the Vanderbilt Department of Emergency Medicine Research Partner of the ED Benchmarking Alliance Baseline Data Collection Tool The data collected via this form is the baseline member data for
Endorsed by the Vanderbilt Department of Emergency Medicine Research Partner of the ED Benchmarking Alliance Baseline Data Collection Tool The data collected via this form is the baseline member data for
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018
 Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
Choosing the Appropriate Stress Test: Brett C. Stoll, MD, FACC February 24, 2018 Choosing the Appropriate Stress Test: Does it Really Matter? Brett C. Stoll, MD, FACC February 24, 2018 Conflicts of Interest
My Patient Needs a Stress Test
 My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
My Patient Needs a Stress Test Amy S. Burhanna,, MD, FACC Coastal Cardiology Cape May Court House, New Jersey Absolute and relative contraindications to exercise testing Absolute Acute myocardial infarction
2/20/2013. Why use imaging in CV prevention? Update on coronary CTA in 2013 Coronary CTA for 1 0 prevention: pros and cons Are we there yet?
 Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
Evolving Role of Coronary CTA in Primary Cardiovascular Disease Prevention: Are We There Yet? Ron Blankstein, M.D., F.A.C.C. Co-Director, Cardiovascular Imaging Training Program Associate Physician, Preventive
STRESSED ABOUT STRESS TESTS
 STRESSED ABOUT STRESS TESTS Problem Based Lecture Jennifer W. Hsieh Department of Emergency Medicine PGY-3 Question 6 What is the diagnostic accuracy of cardiac testing in low risk chest pain patients?
STRESSED ABOUT STRESS TESTS Problem Based Lecture Jennifer W. Hsieh Department of Emergency Medicine PGY-3 Question 6 What is the diagnostic accuracy of cardiac testing in low risk chest pain patients?
Clinical Investigations
 Clinical Investigations Application of Appropriate Use Criteria to Cardiac Stress Testing in the Hospital Setting: Limitations of the Criteria and Areas for Improved Practice Address for correspondence:
Clinical Investigations Application of Appropriate Use Criteria to Cardiac Stress Testing in the Hospital Setting: Limitations of the Criteria and Areas for Improved Practice Address for correspondence:
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD
 Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
Imaging ischemic heart disease: role of SPECT and PET. Focus on Patients with Known CAD Hein J. Verberne Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands International Conference
The Emerging Role of Cardiac CT in Cardiovascular Imaging. Anthony Gemignani, MD Vermont Cardiac Network April 28, 2016
 The Emerging Role of Cardiac CT in Cardiovascular Imaging Anthony Gemignani, MD Vermont Cardiac Network April 28, 2016 Conflict Disclosures I have no significant financial relationship with any companies
The Emerging Role of Cardiac CT in Cardiovascular Imaging Anthony Gemignani, MD Vermont Cardiac Network April 28, 2016 Conflict Disclosures I have no significant financial relationship with any companies
The PAIN Pathway for the Management of Acute Coronary Syndrome
 2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
Evidence for Everyone: Expanding the Reach of Health Technology Assessment 2016 CADTH Symposium, April 10-12, Shaw Centre, Ottawa
 Dr. Ross Davies President Dr. Benjamin Chow Vice-President Dr. Jonathan Leipsic Secretary/Treasurer Office 222 Queen Street Suite 1403 Ottawa, ON K1P 5V9 www.ccs.ca/ nuclear_ct@ccs.ca Evidence for Everyone:
Dr. Ross Davies President Dr. Benjamin Chow Vice-President Dr. Jonathan Leipsic Secretary/Treasurer Office 222 Queen Street Suite 1403 Ottawa, ON K1P 5V9 www.ccs.ca/ nuclear_ct@ccs.ca Evidence for Everyone:
Coronary Artery Disease - Reporting and Data System (CAD-RADS)
") A joint publication of the Department of Radiology and Corrigan Minehan Heart Center November 2016 Issue 66 Coronary Artery Disease - Reporting and Data System (CAD-RADS) Sandeep S. Hedgire, MD; Udo Hoffmann,
A joint publication of the Department of Radiology and Corrigan Minehan Heart Center November 2016 Issue 66 Coronary Artery Disease - Reporting and Data System (CAD-RADS) Sandeep S. Hedgire, MD; Udo Hoffmann,
2008, American Heart Association. All rights reserved.
 AHA 2008 Cocaine-Associated Chest Pain and Myocardial Infarction Slide Set Based on the AHA 2008 Scientific Statement for Management of Cocaine-Associated Chest Pain and Myocardial Infarction George J.
AHA 2008 Cocaine-Associated Chest Pain and Myocardial Infarction Slide Set Based on the AHA 2008 Scientific Statement for Management of Cocaine-Associated Chest Pain and Myocardial Infarction George J.
Troponin when is an assay high sensitive?
 Troponin when is an assay high sensitive? Professor P. O. Collinson MA MB BChir FRCPath FRCP edin MD FACB EurClin Chem Consultant Chemical Pathologist and Professor of Cardiovascular Biomarkers, Departments
Troponin when is an assay high sensitive? Professor P. O. Collinson MA MB BChir FRCPath FRCP edin MD FACB EurClin Chem Consultant Chemical Pathologist and Professor of Cardiovascular Biomarkers, Departments
ROMICAT II - Rule Out Myocardial
 ROMICAT II - Rule Out Myocardial Ischemia/Infarction Using Computer Assisted Tomography NHLBI U01HL092040 A Multicenter Randomized Comparative Effectiveness Trial of Cardiac CTA vs. Standard Evaluation
ROMICAT II - Rule Out Myocardial Ischemia/Infarction Using Computer Assisted Tomography NHLBI U01HL092040 A Multicenter Randomized Comparative Effectiveness Trial of Cardiac CTA vs. Standard Evaluation
CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON CCS Perioperative Guidelines When to order a BNP and What to do with a Positive Troponin Dr. Vikas Tandon Associate Professor, Cardiology
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease?
 CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
CT FFR: Are you ready to totally change the way you diagnose Coronary Artery Disease? Madan Mohan MD MRCP FACC CQO, Division of Cardiovascular Medicine University Hospitals Case Medical Center Assistant
The Role of Computed Tomography in the Diagnosis of Coronary Atherosclerosis
 The Role of Computed Tomography in the Diagnosis of Coronary Atherosclerosis Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiology The Ohio State University
The Role of Computed Tomography in the Diagnosis of Coronary Atherosclerosis Saurabh Rajpal, MBBS, MD Assistant Professor Department of Internal Medicine Division of Cardiology The Ohio State University
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Patient referral for elective coronary angiography: challenging the current strategy
 Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
Patient referral for elective coronary angiography: challenging the current strategy M. Santos, A. Ferreira, A. P. Sousa, J. Brito, R. Calé, L. Raposo, P. Gonçalves, R. Teles, M. Almeida, M. Mendes Cardiology
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures?
 Keenan Research Centre Li Ka Shing Knowledge Institute Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures? Howard Leong-Poi, MD, FRCPC Associate Professor of Medicine St.
Keenan Research Centre Li Ka Shing Knowledge Institute Cardiology for the Practitioner Advanced Cardiac Imaging: Worth the pretty pictures? Howard Leong-Poi, MD, FRCPC Associate Professor of Medicine St.
Heart 101. Objectives. Types of Heart Failure How common is HF? Sign/Symptoms, when to see a doctor? Diagnostic testing
 EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
EXAMING HEART FAILURE: HOW TO RECOGNIZE AND TREAT THE WEAK HEART What is Heart Failure? Treatment of Heart Failure End Stage Heart Failure Munir S. Janmohamed M.D. FACC Assistant Clinical Professor of
Measuring Natriuretic Peptides in Acute Coronary Syndromes
 Measuring Natriuretic Peptides in Acute Coronary Syndromes Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Consultant Cardiologist Chief Academic and Scientific Officer St. John Providence Health
Measuring Natriuretic Peptides in Acute Coronary Syndromes Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Consultant Cardiologist Chief Academic and Scientific Officer St. John Providence Health
Risk Stratification for CAD for the Primary Care Provider
 Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
Risk Stratification for CAD for the Primary Care Provider Shimoli Shah MD Assistant Professor of Medicine Directory, Ambulatory Cardiology Clinic Knight Cardiovascular Institute Oregon Health & Sciences
9/2/2016 CARDIOLOGY TESTING WHAT TO ORDER WHEN REFERENCE OBJECTIVES
 CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
CARDIOLOGY TESTING WHAT TO ORDER WHEN A J W A D F A R A H, M S, P A - C A S S O C I A T E D I R E C T O R O F M E D I C A L O P E R A T I O N S O F A D V A N C E D P R A C T I C E P R O V I D E R S W I
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
Mario Plebani University-Hospital of Padova, Italy
 Mario Plebani University-Hospital of Padova, Italy CK-MB mass assay CHF guidelines use BNP for rule out AST in AMI CK in AMI INH for CK-MB electrophoresis for CK and LD isoenzymes RIA for myoglobin WHO
Mario Plebani University-Hospital of Padova, Italy CK-MB mass assay CHF guidelines use BNP for rule out AST in AMI CK in AMI INH for CK-MB electrophoresis for CK and LD isoenzymes RIA for myoglobin WHO
New Technologies for Cardiac CT. Geoffrey D. Rubin, MD, MBA, FACR, FNASCI Duke University
 1996 New Technologies for Cardiac CT Geoffrey D. Rubin, MD, MBA, FACR, FNASCI Duke University New Technology The Long View Levels of Efficacy Endpoint Examples 1: Technical Imaging resolution 2: Diagnostic
1996 New Technologies for Cardiac CT Geoffrey D. Rubin, MD, MBA, FACR, FNASCI Duke University New Technology The Long View Levels of Efficacy Endpoint Examples 1: Technical Imaging resolution 2: Diagnostic
Standard emergency department care vs. admission to an observation unit for low-risk chest pain patients. A two-phase prospective cohort study
 Standard emergency department care vs. admission to an observation unit for low-risk chest pain patients A. STUDY PURPOSE AND RATIONALE Rationale: A two-phase prospective cohort study IRB Proposal Sara
Standard emergency department care vs. admission to an observation unit for low-risk chest pain patients A. STUDY PURPOSE AND RATIONALE Rationale: A two-phase prospective cohort study IRB Proposal Sara
Women and Ischemic Heart Disease Lessons Learned
 Women and Ischemic Heart Disease 2017- Lessons Learned Bina Ahmed MD Interventional Cardiology Dartmouth-Hitchcock Medical Center Assistant Professor of Medicine Geisel School of Medicine Lebanon, NH ba@hitchcock.org
Women and Ischemic Heart Disease 2017- Lessons Learned Bina Ahmed MD Interventional Cardiology Dartmouth-Hitchcock Medical Center Assistant Professor of Medicine Geisel School of Medicine Lebanon, NH ba@hitchcock.org
Chest Pain. Dr Robert Huggett Consultant Cardiologist
 Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
Chest Pain Dr Robert Huggett Consultant Cardiologist Outline Diagnosis of cardiac chest pain 2016 NICE update on stable chest pain Assessment of unstable chest pain/acs and MI definition Scope of the
ORIGINAL INVESTIGATION. Outcomes of Patients Admitted for Observation of Chest Pain
 ORIGINAL INVESTIGATION Outcomes of Patients Admitted for Observation of Chest Pain Srikanth C. Penumetsa, MD, MRCP; Jaya Mallidi, MD, MHS; Jennifer L. Friderici, MS; William Hiser, MD; Michael B. Rothberg,
ORIGINAL INVESTIGATION Outcomes of Patients Admitted for Observation of Chest Pain Srikanth C. Penumetsa, MD, MRCP; Jaya Mallidi, MD, MHS; Jennifer L. Friderici, MS; William Hiser, MD; Michael B. Rothberg,
Cardiac evaluation for the noncardiac. Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology
 Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
Cardiac evaluation for the noncardiac patient Nathaen Weitzel MD University of Colorado Denver Dept of Anesthesiology Objectives! Review ACC / AHA guidelines as updated for 2009! Discuss new recommendations
2/26/2013. Appropriateness Use Criteria (Drilldown) Disclosures. Tony Hermann has nothing to disclose. Mark Hutcheson has nothing to disclose
 Disclosures. Tony Hermann has nothing to disclose. Mark Hutcheson has nothing to disclose") Appropriateness Use Criteria (Drilldown) Disclosures Tony Hermann has nothing to disclose Mark Hutcheson has nothing to disclose Connie Anderson has nothing to disclose Issam Moussa has nothing to disclose
Appropriateness Use Criteria (Drilldown) Disclosures Tony Hermann has nothing to disclose Mark Hutcheson has nothing to disclose Connie Anderson has nothing to disclose Issam Moussa has nothing to disclose
Guideline Number: NIA_CG_024 Last Review Date: January 2011 Responsible Department: Last Revised Date: May 2, 2011 Clinical Operations
 National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
National Imaging Associates, Inc. Clinical guidelines NUCLEAR CARDIAC IMAGING (MYOCARDIAL PERFUSION STUDY) CPT Codes: 78451, 78452, 78453, 78454, 78466, 78468, 78469, 78481, 78483, 78494, 78499 Original
Chest pain management. Ruvin Gabriel and Niels van Pelt August 2011
 Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Chest pain management Ruvin Gabriel and Niels van Pelt August 2011 Introduction Initial assessment Case 1 Case 2 and 3 Comparison of various diagnostic techniques Summary 1-2 % of GP consultations are
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics
 Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Acute Myocardial Infarction: Difference in the Treatment between Men and Women
 Quality Assurance in Hcahh Can, Vol. 5, No. 3, pp. 261-265,1993 Printed in Great Britain 1040-6166/93 $6.00 + 0.00 1993 Pergamon Press Ltd Acute Myocardial Infarction: Difference in the Treatment between
Quality Assurance in Hcahh Can, Vol. 5, No. 3, pp. 261-265,1993 Printed in Great Britain 1040-6166/93 $6.00 + 0.00 1993 Pergamon Press Ltd Acute Myocardial Infarction: Difference in the Treatment between
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Contrast-Enhanced Coronary Computed Tomography Angiography (CCTA) Page 1 of 27 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Contrast-Enhanced Coronary Computed
Contrast-Enhanced Coronary Computed Tomography Angiography (CCTA) Page 1 of 27 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Contrast-Enhanced Coronary Computed
New Challenges in Nuclear Cardiology Practice
 New Challenges in Nuclear Cardiology Practice Brian G. Abbott, MD, FACC, FASNC, FAHA President, ASNC 2016 Associate Professor of Medicine Warren Alpert Medical School of Brown University Director, Cardiovascular
New Challenges in Nuclear Cardiology Practice Brian G. Abbott, MD, FACC, FASNC, FAHA President, ASNC 2016 Associate Professor of Medicine Warren Alpert Medical School of Brown University Director, Cardiovascular
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period
 Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period Marysia Tweet, MD NASCI Annual Meeting October 18 th, 2016 2016 MFMER slide-1 DISCLOSURE No relevant financial relationship(s)
Multimodality Imaging in Spontaneous Coronary Artery Dissection in the Peripartum Period Marysia Tweet, MD NASCI Annual Meeting October 18 th, 2016 2016 MFMER slide-1 DISCLOSURE No relevant financial relationship(s)
Chest Pain: To Cath or Not? Part I
 Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Chest Pain: To Cath or Not? Part I Georgios Papaioannou, MD Ioannis Karavas, MD Newton-Wellesley Hospital 5/3/2000 1 A Typical Scenario... 57 year old female, Mrs. X., presents to your office with a 2
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction
 Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
Undetectable High Sensitivity Cardiac Troponin T Level in the Emergency Department and Risk of Myocardial Infarction Nadia Bandstein, MD; Rickard Ljung, MD, PhD; Magnus Johansson, MD, PhD; Martin Holzmann,
Prehospital and Hospital Care of Acute Coronary Syndrome
 Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
Diagnostic Algorithms
 Diagnostic Algorithms Udo Sechtem Robert-Bosch-Krankenhaus Stuttgart Germany Montalescot G et al. ESC Guideline on the Management of Stable Coronary Artery Disease Eur Heart J. 2013;34:2949-3003. European
Diagnostic Algorithms Udo Sechtem Robert-Bosch-Krankenhaus Stuttgart Germany Montalescot G et al. ESC Guideline on the Management of Stable Coronary Artery Disease Eur Heart J. 2013;34:2949-3003. European
David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine The Ohio State University Division of Cardiovascular Medicine Columbus, Ohio
 1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
1 STABLE ISCHEMIC HEART DISEASE: A NON-INVASIVE CARDIOLOGIST S PERSECTIVE 2018 Cardiovascular Course for Trainees and Early Career Physicians APRIL 20, 2018 David A. Orsinelli, MD, FACC, FASE Professor,
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Centre for Clinical Practice Review consultation document Review of Clinical Guideline (CG95) Chest pain of recent onset: Assessment and diagnosis
MEDICAL POLICY SUBJECT: CORONARY CALCIUM SCORING
 MEDICAL POLICY PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg
 Rotation: or: Faculty: Coronary Care Unit (CVICU) Dr. Jeff Rottman Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg Duty Hours: Mon Fri, 7 AM to 7 PM, weekend call shared with consult
Rotation: or: Faculty: Coronary Care Unit (CVICU) Dr. Jeff Rottman Drs. Rottman, Salloum, Campbell, Muldowney, Hong, Bagai, Kronenberg Duty Hours: Mon Fri, 7 AM to 7 PM, weekend call shared with consult
VHA Performance Measurement In Cardiac Care
 VHA Performance Measurement In Cardiac Care A Map for VHA Cardiac Performance Measurement in FY 2005 and beyond Roxane Rusch, BSN, MPA, RN Department Of Veterans Affairs Office of Quality and Performance
VHA Performance Measurement In Cardiac Care A Map for VHA Cardiac Performance Measurement in FY 2005 and beyond Roxane Rusch, BSN, MPA, RN Department Of Veterans Affairs Office of Quality and Performance
CARDIAC IMAGING FOR SUBCLINICAL CAD
 CARDIAC IMAGING FOR SUBCLINICAL CAD WHY DON'T YOU ADOPT MORE SMART TECHNIQUE? Whal Lee, M.D. Seoul National University Hospital Department of Radiology We are talking about Coronary artery Calcium scoring,
CARDIAC IMAGING FOR SUBCLINICAL CAD WHY DON'T YOU ADOPT MORE SMART TECHNIQUE? Whal Lee, M.D. Seoul National University Hospital Department of Radiology We are talking about Coronary artery Calcium scoring,
Imaging of the Heart Todd Tessendorf MD FACC
 Imaging of the Heart Todd Tessendorf MD FACC Outline Imaging Modalities for Structural Heart Disease ECHO, MRI Imaging Modalities for Ischemic Heart Disease SPECT, PET, CCTA Show lots of pretty pictures
Imaging of the Heart Todd Tessendorf MD FACC Outline Imaging Modalities for Structural Heart Disease ECHO, MRI Imaging Modalities for Ischemic Heart Disease SPECT, PET, CCTA Show lots of pretty pictures
Acute coronary syndrome (ACS) is a potentially
 is a potentially") DIAGNOSING ACUTE CORONARY SYNDROME AND DETERMINING PATIENT RISK Edith A. Nutescu, PharmD* ABSTRACT Acute coronary syndrome is a form of coronary artery disease and has a broad range of clinical presentations.
DIAGNOSING ACUTE CORONARY SYNDROME AND DETERMINING PATIENT RISK Edith A. Nutescu, PharmD* ABSTRACT Acute coronary syndrome is a form of coronary artery disease and has a broad range of clinical presentations.
Horizon Scanning Technology Summary. Magnetic resonance angiography (MRA) imaging for the detection of coronary artery disease
 imaging for the detection of coronary artery disease") Horizon Scanning Technology Summary National Horizon Scanning Centre Magnetic resonance angiography (MRA) imaging for the detection of coronary artery disease April 2007 This technology summary is based
Horizon Scanning Technology Summary National Horizon Scanning Centre Magnetic resonance angiography (MRA) imaging for the detection of coronary artery disease April 2007 This technology summary is based
Appropriate Timing for Coronary Revascularization Post - MI. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Appropriate Timing for Coronary Revascularization Post - M Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center Disclosures nterventional cardiologist Clinical Cardiovascular
Lahey Clinic Internal Medicine Residency Program: Curriculum for Cardiovascular Medicine Rotation
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Cardiovascular Medicine Rotation Faculty representative: David Venesy, MD Resident representative: David Kahan, MD Revision date: June 29,
Lahey Clinic Internal Medicine Residency Program: Curriculum for Cardiovascular Medicine Rotation Faculty representative: David Venesy, MD Resident representative: David Kahan, MD Revision date: June 29,
Type of intervention Diagnosis. Economic study type Cost-effectiveness analysis.
 The utility and potential cost-effectiveness of stress myocardial perfusion thallium SPECT imaging in hospitalized patients with chest pain and normal or non-diagnostic electrocardiogram Ben-Gal T, Zafrir
The utility and potential cost-effectiveness of stress myocardial perfusion thallium SPECT imaging in hospitalized patients with chest pain and normal or non-diagnostic electrocardiogram Ben-Gal T, Zafrir
Acute Coronary Syndromes. Erika Newton, MD Emergency Medicine July 2, 2009
 Acute Coronary Syndromes Erika Newton, MD Emergency Medicine July 2, 2009 Pathophysiology 3 paths to ACS demand substrate acute blockage Acute blockage = unstable plaque. #1 unsolved problem in Cardiology:
Acute Coronary Syndromes Erika Newton, MD Emergency Medicine July 2, 2009 Pathophysiology 3 paths to ACS demand substrate acute blockage Acute blockage = unstable plaque. #1 unsolved problem in Cardiology:
I have no financial disclosures
 Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
Manpreet Singh MD I have no financial disclosures Exercise Treadmill Bicycle Functional capacity assessment Well validated prognostic value Ischemic assessment ECG changes ST segments Arrhythmias Hemodynamic
The use of Cardiac CT and MRI in Clinical Practice
 The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
The use of Cardiac CT and MRI in Clinical Practice Matthew W. Martinez, MD Assistant Professor of Medicine LVPG - Lehigh Valley Heart Specialists Lehigh Valley Health Network Oct. 3, 2009 DISCLOSURE Relevant
Hospital OQR Quality Measures and Timelines for CY 2015 and Subsequent Payment Determinations
 OQR Quality Measures and Timelines for CY 2015 and Subsequent Payment Determinations Data collection, implementation, and public reporting information for each measure are detailed by measure set in the
OQR Quality Measures and Timelines for CY 2015 and Subsequent Payment Determinations Data collection, implementation, and public reporting information for each measure are detailed by measure set in the
DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN
 DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN DISCLOSURES financial or pharmaceutical affiliations related to topic JOSHUA MESKIN, MD, FACC -Medical College of Wisconsin -Associate Professor of
DIAGNOSTIC TESTING IN PATIENTS WITH STABLE CHEST PAIN DISCLOSURES financial or pharmaceutical affiliations related to topic JOSHUA MESKIN, MD, FACC -Medical College of Wisconsin -Associate Professor of
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Assessing Cardiac Risk in Noncardiac Surgery. Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington
 Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Assessing Cardiac Risk in Noncardiac Surgery Murali Sivarajan, M.D. Professor University of Washington Seattle, Washington Disclosure None. I have no conflicts of interest, financial or otherwise. CME
Detection and Assessment of MI: Use of Imaging Methods. Robert O. Bonow, M.D.
 Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. No Relationships to Disclose Expert Consensus Document
Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. Detection and Assessment of MI: Use of Imaging Methods Robert O. Bonow, M.D. No Relationships to Disclose Expert Consensus Document