Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
|
|
|
- Linette Davis
- 6 years ago
- Views:
Transcription

1 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June
2 Supraventricular Tachycardia (SVT) An atrial ectopic focus continuously discharges at rapid rate ECG Recognition: ventricular rate > 150 rhythm - regular P wave early, distorted or may be hidden PR interval usually shorter QRS - narrow T wave - upright 2

3 Supraventricular Tachycardia 3
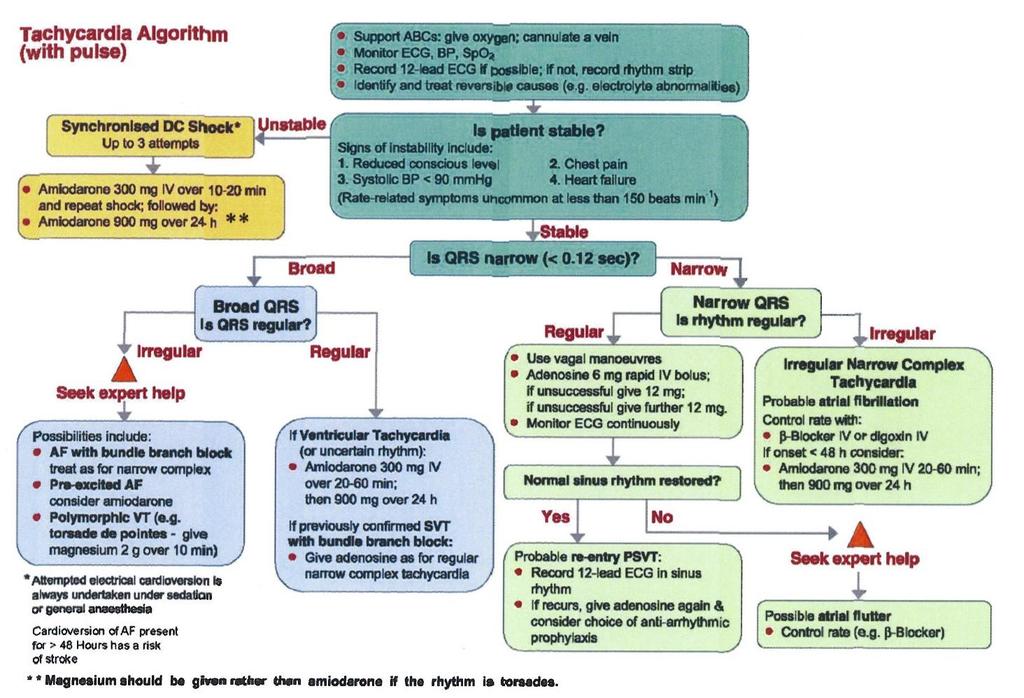
4 Tachyarrhythmia Algorithm 4
5 Supraventricular Tachycardia If stable Valsalva manoeuvre Carotid sinus massage (Medical procedure) Treat cause Correct electrolytes Adenosine 6mg + 12mg + 12mg Other drugs Amiodarone 300mg over 20mins Beta-blockers If unstable (cardiovascularly compromised) Immediate synchronized cardioversion 5
6 Heart Block Caused by defect in the conduction system, resulting in a delay in conduction through the AV node and Bundle Branches. Common Causes: Ischaemia Infarction (inferior Vs anterior) Carditis Digoxin toxicity Degenerative heart disease Other drugs 6
7 Types of Heart Block Each degree of block indicates a more ischaemic and lower functioning conduction system First degree Second degree (Mobitz) Type I (Wenckebach) (Mobitz) Type 2 Third degree (Complete heart block) 7
8 1st Degree Heart Block A delay in conduction through the AV junction ECG Recognition: rate - variable rhythm - regular P wave - normal PR interval > 0.20 sec QRS - narrow T wave - normal 8
9 1st degree Heart Block 9
10 2nd Degree Heart Block Type I Conduction through AV node is progressively delayed until an atrial impulse is not conducted. This will occur in a sequential pattern. ECG Recognition: rate - variable rhythm - irregular (Wenckebach footprints) P wave - present PR interval - increases until non conduction RR interval - decreases until dropped beat QRS - narrow T wave - normal 10
11 2nd degree Heart Block Type I 11
12 2nd Degree Heart Block Type II Intermittent block of atrial conduction characterised by P wave not conducted. ECG Recognition: rate - variable but usually slow rhythm - irregular P wave - present PR interval constant with each conducted beat RR - interval normal QRS usually narrow T wave - normal 12

13 2nd Degree Heart Block Type 2 13
14 3rd Degree Heart Block No impulses conducted through AV node. AV dissociation - atria and ventricle conduct independently. ECG Recognition: rate < 60 rhythm - atrial rate regular, ventricular rate regular P wave - present PR interval variable with no relationship to the QRS QRS depends on site of escape usually > 0.12 sec T wave - normal 14

15 3rd Degree Heart Block 15
16 Heart Block Treatment Considerations: Oxygen if below 95% Rule out drug toxicity e.g. digoxin, beta blockers, calcium channel blockers Treat cause Continuous monitoring Correct electrolyte imbalances e.g. K +, Mg ++ Atropine 500mcg mg bolus (max 3mg) Adrenaline mcg bolus may be considered at BHS Adrenaline infusion may be required Isoprenaline infusion may be considered External/Temporary/Permanent pacing 16
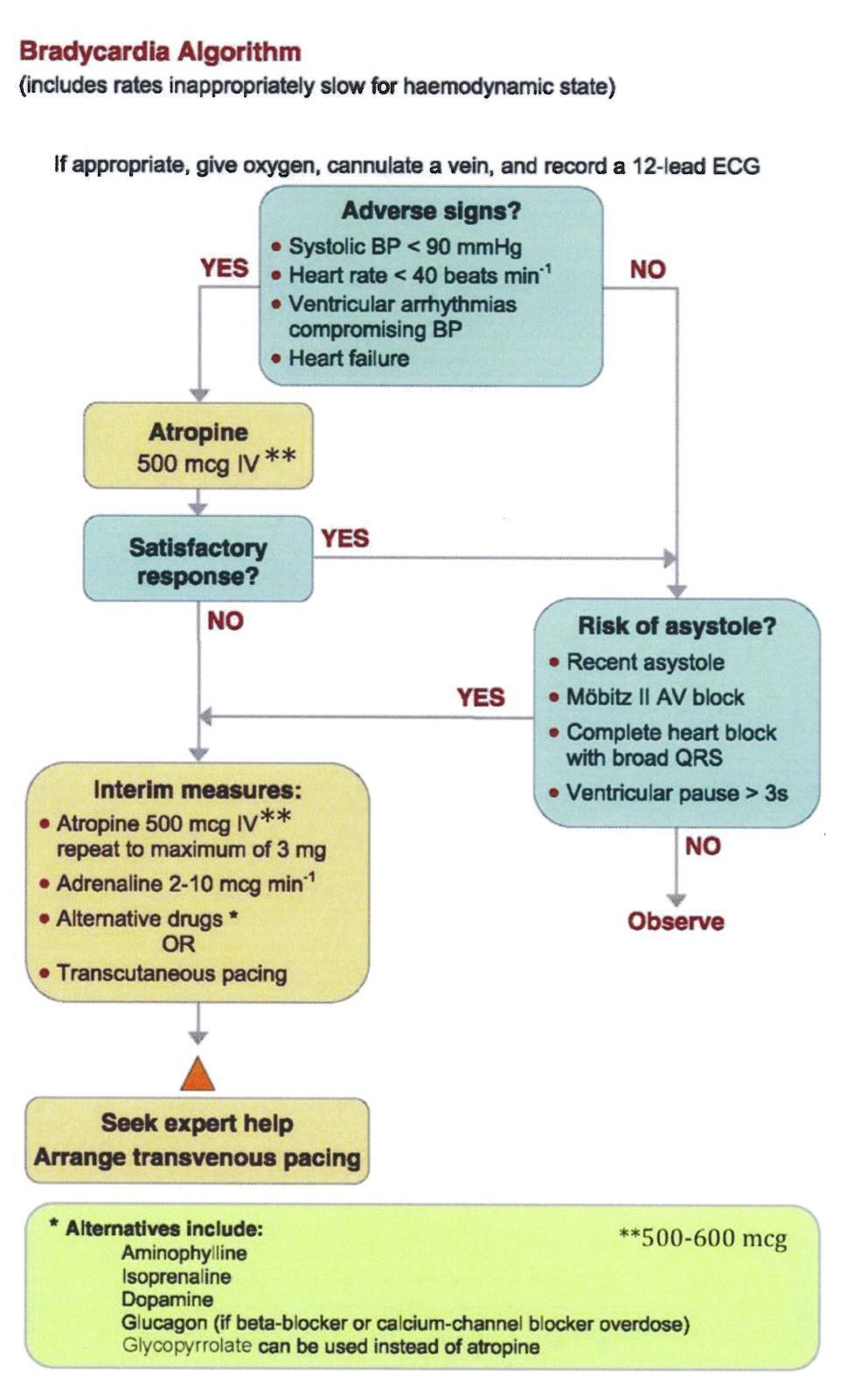
17 Bradyarrhythmia Algorithm 17
18 Idioventricular Rhythm Ventricular initiated contraction = rate < 60 No visible P waves QRS > 0.12 secs - broad Regular T wave opposite polarity When the rate is it is referred to as Accelerated Idioventricular Rhythm 18
19 Idioventricular Rhythm Clinical Significance: If stable investigate and treat as necessary If unstable i.e. haemodynamic compromise Atropine 500mcg mg bolus Isoprenaline 20mcg bolus &/or infusion Adrenaline 50mcg bolus &/or infusion 19
20 Idioventricular Rhythm 20
21 Ventricular Ectopics Ectopic focus in the ventricular muscle discharges prior to the SA node ECG Recognition: rate - variable rhythm - irregular P wave usually lost PR interval absent QRS > 0.12 sec T wave - opposite polarity EARLY wide bizarre beat 21
22 Pattern of Ventricular Ectopics Unifocal - VEs look the same as each other as they originate from a similar focus Multifocal - VEs look different to each other as they come from different foci Bigeminy - every second beat is an ectopic Trigeminy - every third beat is an ectopic Salvos - paired VEs VT (Ventricular Tachycardia) - 3 or more VEs 22


23 Ventricular Ectopics Uniform ventricular ectopic beats Multiform ventricular ectopic beats 23
24 Ventricular Ectopics Causes: Normal, fatigue, alcohol, caffeine, smoking Myocardial infections - endocarditis Electrolyte disturbances (hyperkalaemia or hypokalaemia) Acute Coronary Syndrome Drug overdose (digoxin, tricyclic antidepressants) Clinical Significance: Hypotension depends on cause, rate, type and number of ectopics Potential for R on T phenomena 24
25 Ventricular Ectopics Treatment: Depends on cause and if patient is symptomatic Oxygen Drug therapy e.g. antiarrhythmic Electrolyte replacement 25
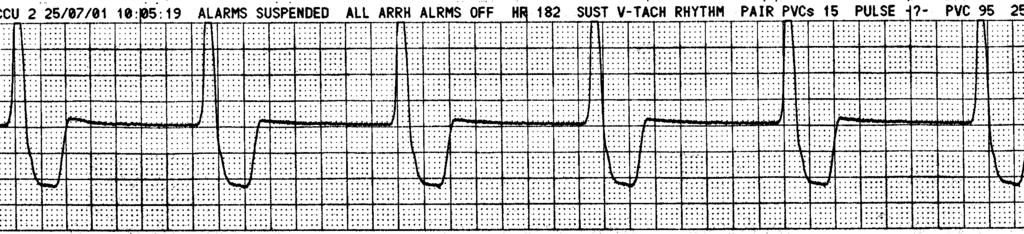
26 Ventricular Tachycardia Consists of 3 or more Ventricular Ectopics Ectopic focus in the ventricular muscle discharges at a rate greater than 110 per minute ECG Recognition: rate > 110 rhythm - regular P - absent QRS > 0.12 sec, broad T wave - opposite in polarity to the QRS complex often occurs following R on T 26
27 Ventricular Tachycardia Causes: Same as ventricular ectopic beats Prolonged QT interval - Torsades de pointes Clinical Significance: Hypotension depends on rate and number of ectopics Hence, patient may be conscious or unconscious May deteriorate to other arrhythmia's e.g. Ventricular fibrillation 27
28 Ventricular Tachycardia Stable May be self limiting treat cause Oxygen if SaO2 below 95% correct electrolytes suppress ectopic focus with antiarrhythmics eg Amiodarone 300mg over 20 mins Or Lignocaine mg/kg synchronised cardioversion Unstable (cardiovascularly compromised) Immediate synchronized cardioversion Pulseless Treat as per ALS algorithm 28

29 Ventricular Tachycardia 29
30 Torsades de Pointes Polymorphic type of Ventricular Tachycardia which is associated with prolonged QT interval (delayed repolarization) The QRS appears positive and negative, with some degree of regularity 30
31 Torsades de Pointes ECG Recognition: rate > 110 rhythm irregular P absent PR interval absent QRS > 0.12 sec, broad T wave opposite in polarity QRS twists on axis 31
32 Torsades de Pointes Causes: Prolonged QT (congenital or drug induced) Acute Coronary Syndrome Drugs - amiodarone, quinidine 32
33 Torsades de Pointes Clinical Significance: May deteriorate into other arrhythmias e.g. Ventricular Fibrillation May be paroxysmal in nature Haemodynamic stability will be short lived Treatment: Defibrillation & BLS Treat cause Magnesium 5mmol bolus, can repeat once Avoid drug therapy that may prolong the QT e.g. amiodarone 33

34 Torsades de Pointes 34
35 Ventricular Fibrillation Several ectopic foci in the ventricles fire rapidly and chaotically No discernable QRS complexes, ventricular muscle contraction uncoordinated and chaotic = no C.O. = brain not being perfused = always unconscious 35
36 Ventricular Fibrillation ECG recognition: bizarre configuration No recognisable QRS 36

37 Ventricular Fibrillation 37
38 VF / Pulseless VT management BLS if defibrillator not immediately available The only initial effective treatment for VF and pulseless VT is DEFIBRILLATION 38
39 Asystole No electrical activity in the heart. No recognisable complexes on ECG No cardiac output. Confirming Asystole: If ECG looks like an isoelectric flat/wandering line, check your patient, try changing monitoring lead and increase the amplitude of the lead This will aid differentiation between asystole and fine ventricular fibrillation 39
40 Asystole Treatment: BLS Identify and treat reversible causes Drugs: Adrenaline 1mg repeat every 4 mins Electrolyte replacement Consider pacing 40

41 Asystole 41
42 Pulseless Electrical Activity (PEA) There is electrical activity with no cardiac output. ECG Recognition: rate & rhythm variable P wave, PR interval, QRS, and T wave may all be normal 42
43 Pulseless Electrical Activity (PEA) Treatment: BLS Identify and treat cause fluid replacement if hypovolaemic Drugs: Adrenaline 1mg every 4 mins Consider electrolyte replacement Consider pacing 43
44 Ventricular Standstill Atrial activity with no ventricular activity. ECG Recognition: Ventricular activity absent P waves normal No QRS complex s or T waves 44
45 Ventricular Standstill Treatment: BLS treat cause drug therapy adrenaline electrolyte replacement emergency pacing 45

46 Ventricular Standstill 46
47 Resuscitation Drugs 47
48 Resuscitation Drugs Not shown to improve survival Good quality CPR, Defibrillation are the priorities IV preferable peripheral, jugular, avoid lower limbs IV admin. followed by 20 ml flush and CPR for 2 minutes Administer via a CVC if available Intraosseous if 2 attempts to cannulate or 1 attempt in children 48
49 ETT administration De-emphasized by the ARC. I/O is the preferred method if IV access not possible. Technique suction airway insert clear catheter e.g Y suction dilute drug in 10 ml Water for Injection dose 2-3 times normal IV dose flush with 20mls N/Saline follow with 2 vigorous inflations Adrenaline, lignocaine and atropine are the only drugs that may be administered via the ETT in ALS NEVER give drugs via a Laryngeal Mask Airway 49

50 ETT administration Water for Injection 50
51 Drugs of ALS Adrenaline Amiodarone Atropine (not for use in Asystole/ PEA) Lignocaine Potassium Magnesium 51
52 Adrenaline Natural catecholamine alpha - peripheral effects beta 1 & 2 - cardiac & bronchial effect Role in ALS most important drug of ALS vasoconstriction directs blood to heart / brain increases aortic root pressure facilitates defibrillation by improving myocardial blood flow and reducing acidosis 52
53 Adrenaline Indications: VF / pulseless VT after defibrillation has failed Asystole / PEA initial treatment Complications: tachycardia hypertension Dosage: 1 mg initially (if no cardiac output) Repeated 4 minutely No maximum dose Post resuscitation if bradycardic & hypotensive may need to administer increments of 50mcg &/or preferably commence an infusion 53
54 Action: Amiodarone Depresses SA node and slows AV conduction increases repolarisation lowers defibrillation threshold restores fibrillation threshold Indications: First line antiarrhythmic of choice in VF/VT If defibrillation & adrenaline failed to revert VF/VT Atrial tachyarrhythmias SVT, WPW, Rapid AF/Aflutter 54
55 Amiodarone Dosage: 300mg bolus diluted up to 20 mls 5% Glucose over 1 min Incompatible with 0.9% Saline Can repeat bolus at 150mg Infusion 15mg/kg over 24 hours Complications: Hypotension prolonged QT Heart blocks Bradycardia 55
56 Atropine Action: Parasympathetic antagonist that suppresses vagus nerve activity Indications: symptomatic bradyarrhythmias Dosage: 1 mg bolus in severe bradycardia Can be repeated up to a maximum of 3mg Complications: Tachycardia Dilated pupils and dry mouth 56
57 Action: Lignocaine Membrane stabilising antiarrhythmic drug Indications: Monomorphic VT If defibrillation & adrenaline failed to revert pulseless VT If IV route unavailable and ETT route only available Complications: CNS: drowsiness, agitation, fitting hypotension, bradycardia, heart block increases defibrillation threshold Dosage: mg/ kg slow IV bolus repeat at half the dose if required 57
58 Action: Potassium Chloride An electrolyte required for membrane stability Decreased K+ leads to arrhythmias Indications: VT / VF where low potassium suspected Dosage: 5 mmol IV diluted to 20mls Complications: hyperkalaemia - bradycardia, asystole tissue necrosis 58
59 Magnesium Sulphate Action: Electrolyte essential for membrane stability Indications: Torsades des pointes Cardiac arrest/arrhythmias associated with Digoxin Toxicity VF/pulseless VT Hypokalaemia or hypomagnesium 59
60 Magnesium Sulphate Dosage: 5 mmol bolus Can repeat 5mmol bolus once Infusion of 20mmol over 2 hours Complications: muscle weakness Hypotension paralysis respiratory failure bradycardia 60
61 Sodium bicarbonate Action: Alkalising solution used to reverse the acidosis of hypoxia and cardiac arrest Indications: NOT FOR ROUTINE USE IN RESUSCITATION OD tricyclic antidepressants 61
62 Sodium bicarbonate Dosage: bolus 1 mmol / kg over 2-3 minutes adequate CPR and ventilation (ETT) is essential for effective stabilisation of ph in conjunction as a priority over - sodium bicarbonate Complications: Intracellular acidosis risk of alkalosis, hypernatreamia rebound acidosis as CO 2 liberated from HCO 3 62
63 Additional drugs used in cardiac emergencies Adenosine Isoprenaline Calcium 63
64 Action Adenosine Slows sinus node rate prolongs AV conduction, causing high grade block half life < 5 secs Indications: treatment SVT diagnosis of Atrial flutter Atrial fibrillation broad complex tachycardia (where VT is unlikely) 64
65 Adenosine Dosage; 6mg IV quickly, then if required 12mg and if required repeat a further 12 mgs Side Effects: flushing, shortness of breath, chest discomfort, SENCE OF IMPENDING DOOM Cautions: asthmatics, patients with heart blocks 65
66 Isoprenaline Action: Synthetic sympathomimetic related to adrenaline Purely Beta receptor stimulator, bronchodilator, positive inotrope, chronotrope and dromotrope Indications Bradyarrhythmias with pulse refractory to atropine Dose mcg bolus Complications Tachyarrhythmias Increased MVO2 66
67 Calcium Seldom indicated in management of cardiac arrest Action: Electrolyte essential for muscle activity Increases excitability/ contractility & peripheral resistance Indications: Arrhythmias associated with hyperkalaemia hypocalcaemia Overdose of calcium channel blockers Dosage: 5-10mls 10% calcium chloride 20mls 10% calcium gluconate 67
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University. OBHG Education Subcommittee
 -RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
-RHYTHM PRACTICE- By Dr.moanes Msc.cardiology Assistant Lecturer of Cardiology Al Azhar University The Normal Conduction System Sinus Node Normal Sinus Rhythm (NSR) Sinus Bradycardia Sinus Tachycardia
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Course Objectives. Proper Lead Placements. Review the ECG print paper. Review the mechanics of the Myocardium. Review basics of ECG Rhythms
 ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
ECG Interpretations Course Objectives Proper Lead Placements Review the ECG print paper Review the mechanics of the Myocardium Review basics of ECG Rhythms How Leads Work The ECG Leads we use are Bipolar
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
Rhythm ECG Characteristics Example. Normal Sinus Rhythm (NSR)
") Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Normal Sinus Rhythm (NSR) Rate: 60-100 per minute Rhythm: R- R = P waves: Upright, similar P-R: 0.12-0.20 second & consistent P:qRs: 1P:1qRs Sinus Tachycardia Exercise Hypovolemia Medications Fever Substances
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
a lecture series by SWESEMJR
 Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
Electrolyte disturbances Hypokalaemia Decreased extracellular potassium increases excitability in the myocardial cells and consequently the effect of very severe hypokalaemia is ventricular arrhythmia.
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Rate: The atrial and ventricular rates are equal; heart rate is greater than 100 bpm (usually between bpm).
.") Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Sinus Bradycardia Regularity: The R-R intervals are constant; the rhythm is regular. Rate: The atrial and ventricular rates are equal; heart rate is less than 60 bpm. P wave: There is a uniform P wave
Basic Dysrhythmia Interpretation
 Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Basic Dysrhythmia Interpretation Objectives 2 To understand the Basic ECG To understand the meaning of Dysrhythmia To describe the normal heart conduction system. To describe the normal impulse pathways.
Step by step approach to EKG rhythm interpretation:
 Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
Sinus Rhythms Normal sinus arrhythmia Small, slow variation of the R-R interval i.e. variation of the normal sinus heart rate with respiration, etc. Sinus Tachycardia Defined as sinus rhythm with a rate
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Cardiac arrhythmias. Janusz Witowski. Department of Pathophysiology Poznan University of Medical Sciences. J. Witowski
 Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Cardiac arrhythmias Janusz Witowski Department of Pathophysiology Poznan University of Medical Sciences A 68-year old man presents to the emergency department late one evening complaining of increasing
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms
 Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Arrhythmia Study Guide 3 Junctional and Ventricular Rhythms JUNCTIONAL RHYTHMS The AV Junction (Bundle of His and surrounding cells) only acts as pacemaker of the heart when the SA Node is not firing normally
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
ACLS Study Guide for Precourse Self-Assessment
 20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
20 rhythm strips on Precourse Self-Assessment with the following matching choices: Agonal Rhythm/Asystole Atrial Fibrillation Flutter Ventricular Fibrillation Monomorphic Ventricular Normal Sinus Rhythm
2017 BDKA Review. Regularity Rate P waves PRI QRS Interpretation. Regularity Rate P waves PRI QRS Interpretation 1/1/2017
 1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
1. 2017 BDKA Review 2. 3. 4. Interpretation 5. QT 6. 7. 8. 9. 10. QT 11. 12. 13. 14. 15. 16. 17. 18. QT 19. 20. QT 21. 22. QT 23. 24. Where are pacer spikes? Before the P wave or before the QRS complex?
! YOU NEED TO MONITOR QT INTERVALS IN THESE PATIENTS.
 Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Antiarrhythmic Pharmacopoeia Powerful drugs, split into 4 major classes, according to the predominant receptor they effect. Some fit into several classes at once, like sotolol. Some don t fit at all, owing
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด
 Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
Cardiac Arrhythmia How to approach นพ.พ น จ แกวส วรรณะ หน วยโรคห วใจและหลอดเล อด EKG paper is a grid where time is measured along the horizontal axis. Each small square is 1 mm in length and represents
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT
 Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
Link download full: http://testbankair.com/download/test-bank-for-ecgs-made-easy-5thedition-by-aehlert/ TEST BANK FOR ECGS MADE EASY 5TH EDITION BY AEHLERT Chapter 5 TRUE/FALSE 1. The AV junction consists
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
EKG Abnormalities. Adapted from:
 EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
EKG Abnormalities Adapted from: http://www.bem.fi/book/19/19.htm Some key terms: Arrhythmia-an abnormal rhythm or sequence of events in the EKG Flutter-rapid depolarizations (and therefore contractions)
ABCs of ECGs. Shelby L. Durler
 ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
ABCs of ECGs Shelby L. Durler Objectives Review the A&P of the cardiac conduction system Placement and obtaining 4-lead and 12-lead ECGs Overview of the basics of ECG rhythm interpretation Intrinsic
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
KNOW YOUR ECG. G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada
 KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
KNOW YOUR ECG G. Somasekhar MD DM FEp Consultant Electro physiologist, Aayush Hospital, Vijayawada CASE DETAILS A 48-year-old female non hypertensive, non diabetic presented with history of shortness of
ARRHYTHMIAS IN THE INTENSIVE CARE UNIT
 ARRHYTHMIAS IN THE INTENSIVE CARE UNIT Nicole Van Israël, DVM, CESOpht, CertSAM, CertVC, DECVIM-CA (Cardiology), MSc, MRCVS European Specialist in Veterinary Cardiology Animal CardioPulmonary Consultancy
ARRHYTHMIAS IN THE INTENSIVE CARE UNIT Nicole Van Israël, DVM, CESOpht, CertSAM, CertVC, DECVIM-CA (Cardiology), MSc, MRCVS European Specialist in Veterinary Cardiology Animal CardioPulmonary Consultancy
ARRHYTHMIAS IN THE ICU
 ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
ARRHYTHMIAS IN THE ICU Nora Goldschlager, MD MACP, FACC, FAHA, FHRS SFGH Division of Cardiology UCSF IDENTIFIED VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar) Electrolyte imbalance Proarrhythmia
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
Diploma in Electrocardiography
 The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
The Society for Cardiological Science and Technology Diploma in Electrocardiography The Society makes this award to candidates who can demonstrate the ability to accurately record a resting 12-lead electrocardiogram
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
ANTI-ARRHYTHMICS AND WARFARIN. Dr Nithish Jayakumar
 ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT
 ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
ARRHYTHMIAS IN THE ICU: DIAGNOSIS AND PRINCIPLES OF MANAGEMENT Nora Goldschlager, M.D. MACP, FACC, FAHA, FHRS SFGH Division of Cardiogy UCSF CLINICAL VARIABLES IN ARRHYTHMOGENESIS Ischemia/infarction (scar)
Educational Resource Advanced Life Support (ALS) Adult
 Adult") Educational Resource Advanced Life Support (ALS) Adult June 2012 TABLE OF CONTENTS Table of Contents... 2 Introduction... 3 Acknowledgements... 3 Advanced Life Support (ALS)... 4 Defibrillation... 6 Medications
Educational Resource Advanced Life Support (ALS) Adult June 2012 TABLE OF CONTENTS Table of Contents... 2 Introduction... 3 Acknowledgements... 3 Advanced Life Support (ALS)... 4 Defibrillation... 6 Medications
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Dysrhythmias. Dysrythmias & Anti-Dysrhythmics. EKG Parameters. Dysrhythmias. Components of an ECG Wave. Dysrhythmias
 Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
Dysrhythmias Dysrythmias & Anti-Dysrhythmics Rhythm bad in the heart: Whitewater rafting Electrical impulses coordinate heart Reduction in Cardiac Output PEA Asystole Components of an ECG Wave EKG Parameters
CARDIAC ARRHYTHMIAS IN NEONATE
 Introduction: CARDIAC ARRHYTHMIAS IN NEONATE DR. PANKAJ SAKHUJA Neonatologist Average heart rate in a healthy newborn is 120-160 beats/min and the range is from 80-230 beats/min. A normal (sinus) rhythm
Introduction: CARDIAC ARRHYTHMIAS IN NEONATE DR. PANKAJ SAKHUJA Neonatologist Average heart rate in a healthy newborn is 120-160 beats/min and the range is from 80-230 beats/min. A normal (sinus) rhythm
HTEC 91. Performing ECGs: Procedure. Normal Sinus Rhythm (NSR) Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway
 Topic for Today: Sinus Rhythms. Characteristics of NSR. Conduction Pathway") HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
HTEC 91 Medical Office Diagnostic Tests Week 3 Performing ECGs: Procedure o ECG protocol: you may NOT do ECG if you have not signed up! If you are signed up and the room is occupied with people who did
Electrocardiography for Healthcare Professionals
 Electrocardiography for Healthcare Professionals Chapter 9: Ventricular Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 9.1 Describe the various ventricular dysrhythmias 9.2
Electrocardiography for Healthcare Professionals Chapter 9: Ventricular Dysrhythmias 2012 The Companies, Inc. All rights reserved. Learning Outcomes 9.1 Describe the various ventricular dysrhythmias 9.2
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
ANZCOR Guideline 12.4 Medications and Fluids in Paediatric Advanced Life Support
 ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
Ventricular tachycardia Ventricular fibrillation and ICD
 EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
EKG Conference Ventricular tachycardia Ventricular fibrillation and ICD Samsung Medical Center CCU D.I. Hur Ji Won 2006.05.20 Ventricular tachyarrhythmia ventricular tachycardia ventricular fibrillation
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment
 Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
Intraoperative and Postoperative Arrhythmias: Diagnosis and Treatment Karen L. Booth, MD, Lucile Packard Children s Hospital Arrhythmias are common after congenital heart surgery [1]. Postoperative electrolyte
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
COURSE DESCRIPTION. Rev 2.0 7/2013. Page 1 of 26
 COURSE DESCRIPTION Ventricular dysrhythmias (arrhythmias) are unique and potentially dangerous cardiac rhythms. They are often associated with Code Blue calls, and life and death situations. The only two
COURSE DESCRIPTION Ventricular dysrhythmias (arrhythmias) are unique and potentially dangerous cardiac rhythms. They are often associated with Code Blue calls, and life and death situations. The only two
ECG Interactive Session
 SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
SA HEART 2018 PRE-CONGRESS WORKSHOP 4 OCTOBER 2018 ECG Interactive Session Ashley Chin Cardiologist/Electrophysiologist University of Cape Town Groote Schuur Hospital ECG 1 Which ONE of the following is
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/AV Blocks Connie J. Mattera, M.S., R.N., EMT-P
 Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Northwest Community Healthcare Paramedic Education Program AV Conduction Defects/ Connie J. Mattera, M.S., R.N., EMT-P Reading assignments: Bledsoe Vol. 3: pp. 88-93; 120-121 (atropine, norepinephrine,
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Chapter 28, Part 1 Cardiology. Cardiac Physiology. Cardiovascular Anatomy
 Chapter 28, Part 1 Cardiology Part 1: Cardiovascular Anatomy & Physiology, ECG Monitoring, and Dysrhythmia Analysis 1 2 Cardiovascular Anatomy Coronary Circulation Cardiac Physiology The cardiac cycle
Chapter 28, Part 1 Cardiology Part 1: Cardiovascular Anatomy & Physiology, ECG Monitoring, and Dysrhythmia Analysis 1 2 Cardiovascular Anatomy Coronary Circulation Cardiac Physiology The cardiac cycle
Practical Approach to Arrhythmias
 Outline Practical Approach to Arrhythmias Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Conduction System ECG Acquisition ECG Interpretation Heart rate Rhythm Arrhythmias Tachyarrhythmias Supraventricular
Outline Practical Approach to Arrhythmias Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Conduction System ECG Acquisition ECG Interpretation Heart rate Rhythm Arrhythmias Tachyarrhythmias Supraventricular
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE. Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology
 PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
PATIENT WITH ARRHYTHMIA IN DENTIST S OFFICE Małgorzata Kurpesa, MD., PhD. Chair&Department of Cardiology Medical University of Łódź The heart is made up of four chambers Left Atrium Right Atrium Left Ventricle
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
Cardiology Flash Cards
 Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
Cardiology Flash Cards EKG in a nut shell www.brain101.info Conduction System www.brain101.info 2 Analyzing EKG Step by step Steps in Analyzing ECG'S 1. Rhythm: - Regular _ Sinus, Junctional or Ventricular.
physiology 6 Mohammed Jaafer Turquoise team
 15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
15 physiology 6 Mohammed Jaafer 22-3-2016 Turquoise team Cardiac Arrhythmias and Their Electrocardiographic Interpretation Today, we are going to talk about the abnormal excitation. As we said before,
CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017
 CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017 The Heart The heart is undoubtedly the most important organ in the body. Unfortunately, when it is not functioning properly, it can have dire consequences.
CRITICAL CARE OF THE CARDIAC PATIENT WEBINAR VET 2017 The Heart The heart is undoubtedly the most important organ in the body. Unfortunately, when it is not functioning properly, it can have dire consequences.
Patient Examination. Objectives for Presentation RECOGNITION OF COMMON ARRHYTHMIAS THEIR CAUSES AND TREATMENT OPTIONS 9/8/2016
 RECOGNITION OF COMMON ARRHYTHMIAS THEIR CAUSES AND TREATMENT OPTIONS Ryan Fries, DVM, DACVIM (Cardiology) Clinical Assistant Professor University of Illinois Department of Clinical Veterinary Medicine
RECOGNITION OF COMMON ARRHYTHMIAS THEIR CAUSES AND TREATMENT OPTIONS Ryan Fries, DVM, DACVIM (Cardiology) Clinical Assistant Professor University of Illinois Department of Clinical Veterinary Medicine
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
Synopsis of Management on Ventricular arrhythmias. M. Soni MD Interventional Cardiologist
 Synopsis of Management on Ventricular arrhythmias M. Soni MD Interventional Cardiologist No financial disclosure Premature Ventricular Contraction (PVC) Ventricular Bigeminy Ventricular Trigeminy Multifocal
Synopsis of Management on Ventricular arrhythmias M. Soni MD Interventional Cardiologist No financial disclosure Premature Ventricular Contraction (PVC) Ventricular Bigeminy Ventricular Trigeminy Multifocal
Cardiac Arrhythmias in Sleep
 Cardiac Arrhythmias in Sleep Only 53 Slides! Gauresh H Kashyap, MD, FACP, FCCP, FAASM 1 2 Cardiac Arrhythmias in Sleep Out of 400 Patients with OSA, 48% had some Arrhythmias 20% - 2 PVCs/min 7% - Bradycardia
Cardiac Arrhythmias in Sleep Only 53 Slides! Gauresh H Kashyap, MD, FACP, FCCP, FAASM 1 2 Cardiac Arrhythmias in Sleep Out of 400 Patients with OSA, 48% had some Arrhythmias 20% - 2 PVCs/min 7% - Bradycardia
3. AV Block 1. First-degree AV block 1. Delay in AV node 2. Long PR interval 3. QRS complex follows each P wave 4. Benign, no tx
 1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
MAT vs AFIB. Henry Clemo. Fast & Easy ECGs, 2E 2013 The McGraw-Hill Companies, Inc. All rights reserved.
 MAT vs AFIB Henry Clemo 1 Multifocal Atrial Tachycardia (MAT) > 3 P wave morphologies HR > 100 HR < 100 wandering pacemaker I 2 Multifocal Atrial Tachycardia 3 Multifocal Atrial Tachycardia 4 Multifocal
MAT vs AFIB Henry Clemo 1 Multifocal Atrial Tachycardia (MAT) > 3 P wave morphologies HR > 100 HR < 100 wandering pacemaker I 2 Multifocal Atrial Tachycardia 3 Multifocal Atrial Tachycardia 4 Multifocal
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
Basic EKG Interpretation. Nirja Parikh, PT, DPT
 Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Basic EKG Interpretation Nirja Parikh, PT, DPT Electrocardiogram (EKG) Using surface electrodes record the electrical activity of the heart electrical activity (usually) correlates to mechanical function
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,