Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου
|
|
|
- Magdalen Boyd
- 6 years ago
- Views:
Transcription

1 Dr Αντώνιος Στ. Ντάτσιος MSc, MRCP(UK), FESC. Επεμβατικός Καρδιολόγος Επιμελητής Β Γ. Ν. Θ. Παπαγεωργίου Θεσσαλονίκη, 9/2/2018
2 Disclosures: None
3
4 Primary efficacy outcome* (%/year) Antiplatelet Therapy Alone Does Not Provide Adequate Protection from AF-Related Stroke A randomized trial for DAPT (n=3,335) vs VKA (n=3,371) for prevention of vascular events in patients with AF demonstrated superiority of OAC therapy 6 RR=1.44 (95% CI ) p= , , VKA (INR ) DAPT (75 mg clopidogrel *Composite of stroke, non-cns embolus, MI and vascular death The ACTIVE Writing Group. Lancet 2006;367:
5 ACC/AHA 2007 Guidelines for management of patients with NSTE-ACS UA/NSTEMI patient groups at discharge with indication for anticoagulation Drug-eluting stent group Bare-metal stent group ASA* mg/day for at least 3 6 months, then mg/day indefinitely Clopidogrel # 75 mg/day for at least 1 year Warfarin When added to ASA plus clopidogrel an INR of is recommended ASA* mg/day for at least 1 month, then mg/day indefinitely Clopidogrel # 75 mg/day for at least 1 month and ideally up to 1 year Warfarin When added to ASA plus clopidogrel an INR of is recommended *For ASA allergic patients, use clopidogrel alone (indefinitely), or try desensitization; # for clopidogrel allergic patients, use ticlopidine 250 mg by mouth twice daily; continue ASA indefinitely and warfarin longer term as indicated for specific conditions such as AF Anderson JL et al, Circulation 2007;116:e148 e304
6 Crude incidence rates (events per 100 person-years ± SE) Triple Therapy with a VKA Reduces Thromboembolic Events but Increases Bleeding after PCI in AF Patients Danish registry data ( ; N=11,480 patients) Triple therapy (VKA plus ASA plus clopidogrel) VKA plus single antiplatelet therapy DAPT (ASA plus clopidogrel) VKA monotherapy Single antiplatelet therapy 10 0 CV death plus MI plus ischaemic stroke Fatal and non-fatal bleeding Lamberts M et al, Circulation 2012;126:
7 Major bleeding in PCI is associated with an increase in mortality Background risk Bleeding Shock Anaemia Transfusion Discontinuation of APT Ischaemia Inflammation Stent thrombosis Mortality Compared with patients without bleeding, patients who experience bleeding are more likely to die, not only early (in hospital) but also late (after discharge) APT, antiplatelet therapy; PCI, percutaneous coronary intervention; Steg et al. Eur Heart J
8 Incidence at 1 year (%) Reduced bleeding risk and no increase in thrombosis with double vs triple antithrombotic therapy in patients on OACs and undergoing PCI 50 P< ,4 WOEST study: OAC-treated patients undergoing PCI were randomized to additional clopidogrel (dual therapy) or clopidogrel + ASA (triple therapy) Dual therapy (n=279) Triple therapy (n=284) ,4 Any bleeding P=0.159 P=0.027 P=0.382 P= ,6 6,3 3,2 2,5 3,2 Major bleeding* All-cause death 4,6 7,2 6,7 P=0.128 P= ,8 3,2 1,1 1,4 MI TVR Stroke Stent thrombosis OAC + clopidogrel associated with significant reduction in major bleeding and no increase in thrombotic events vs triple therapy with OAC + clopidogrel + ASA Bold values indicate statistical significance; *TIMI classification. 573 patients receiving OAC and undergoing PCI in open-label WOEST (What is the Optimal antiplatelet and anticoagulant therapy in patients with oral anticoagulation and coronary StenTing) trial. AF was not a prerequisite; however, 69% of patients in both the double therapy and triple therapy treatment groups were using OACs for AF/atrial flutter; ASA, acetylsalicylic acid; PCI, percutaneous coronary intervention; TVR, target vessel revascularization; TIMI, Thrombolysis in Myocardial Infarction; Dewilde et al. Lancet
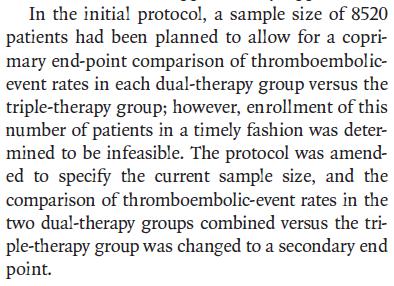
9 Design: An open-label, randomized, controlled phase IIIb safety study Population: patients with paroxysmal, persistent or permanent NVAF undergoing PCI (with stent placement) N=2,124 Decision for DAPT duration: 1, 6 or 12 months 1:1:1 R Rivaroxaban 15 mg OD* # plus single antiplatelet Rivaroxaban 2.5 mg BID # plus DAPT VKA (INR ) plus DAPT Rivaroxaban 15 mg OD* plus low-dose ASA VKA plus low-dose ASA 12 mos: 100% 1 mo: 16% 6 mos: 35% 12 mos: 49% 1 mo: 16% 6 mos: 35% 12 mos: 49% DAPT duration (1 or 6 months) End of treatment (12 months) *CrCl ml/min: 10 mg OD; # first dose hours after sheath removal; clopidogrel (75 mg daily) (alternative use of prasugrel or ticagrelor allowed, but capped at 15%); ASA ( mg daily) plus clopidogrel (75 mg daily) (alternative use of prasugrel or ticagrelor allowed, but capped at 15%); first dose hours after sheath removal 1. Janssen Scientific Affairs, LLC [accessed 10 Oct 2016]; 2. Gibson CM et al, Am Heart J 2015;169: e5; 3. Gibson CM et al, New Engl J Med 2016; doi: /NEJMoa
; p<0.001 Rivaroxaban 2.5 mg BID plus DAPT vs VKA plus DAPT: HR=0.63 (95% CI 0.50 0.80); p<0.001 30 25 20 15 26.7% 18.0% 16.8% ARR 8.7% NNT= 12 ARR 9.")
10 TIMI major, TIMI minor or bleeding requiring medical attention (%) Both Rivaroxaban Strategies was Associated With Significantly Improved Safety Rivaroxaban 15 mg OD plus single antiplatelet vs VKA plus DAPT: HR=0.59; (95% CI ); p<0.001 Rivaroxaban 2.5 mg BID plus DAPT vs VKA plus DAPT: HR=0.63 (95% CI ); p< % 18.0% 16.8% ARR 8.7% NNT= 12 ARR 9.9% NNT= Time (days) Group 3 (VKA plus DAPT) Group 2 (Rivaroxaban 2.5 mg BID plus DAPT) Group 1 (Rivaroxaban 15 mg OD plus single antiplatelet) Gibson CM et al, New Engl J Med 2016; doi: /NEJMoa ]
11 CV death, MI or stroke (%) Efficacy was Comparable Between All Three Treatment Strategies* Rivaroxaban 15 mg OD plus single antiplatelet vs VKA plus DAPT: HR=1.08; (95% CI ); p=0.750 Rivaroxaban 2.5 mg BID plus DAPT vs VKA plus DAPT: HR=0.93 (95% CI ); p= % 6.0% 5.6% 4 Group 3 (VKA plus DAPT) Time (days) Group 2 (Rivaroxaban 2.5 mg BID plus DAPT) Group 1 (Rivaroxaban 15 mg OD plus single antiplatelet) *Trial not powered to definitively demonstrate either superiority or non-inferiority for efficacy endpoints Gibson CM et al, New Engl J Med 2016; doi: /NEJMoa
12
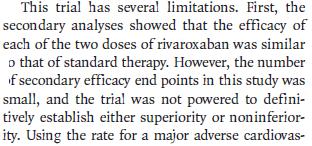
13 Study Design: Multicenter, randomized, open-label trial following a PROBE design Patients with AF undergoi ng PCI with stenting N=2725 Randomizatio n 120 hours post-pci* R Dabigatran 150 mg BID + P2Y12 inhibitor Dabigatran 110 mg BID + P2Y12 inhibitor Warfarin (INR ) + P2Y12 inhibitor + ASA 6-month minimum treatment duration with visits every 3 months for the first year, then visits and telephone contact alternating every 3 months and a 1-month post-treatment visit Mean duration of follow-up: ~14 months Dabigatran (110 or 150 mg) P2Y12 inhibitor Warfarin P2Y12 inhibitor 1 month of ASA (BMS) 3 months of ASA (DES) *Study drug should be administered 6 hours after sheath removal and no later than 120 hrs post-pci ( 72 hrs is preferable). PROBE, prospective, randomized, open, blinded end-point; R, randomization; BMS, bare metal stent; DES, drug-eluting stent. ClinicalTrials.gov: NCT ; Cannon et al. Clin Cardiol 2016
 Non-inferiority P<0.0001 P=0.")
14 Probability of event (%) Primary Endpoint: Time to first ISTH major or clinically relevant non-major bleeding event HR: 0.52 (95% CI: ) Non-inferiority P< P< Warfarin triple therapy HR: 0.72 (95% CI: ) Non-inferiority P< P=0.002 Warfarin triple therapy Dabigatran 110 mg dual therapy Dabigatran 150 mg dual therapy Time to first event (days) Time to first event (days) Full analysis set presented. HRs and Wald CIs from Cox proportional-hazard model. For the dabigatran 110 mg vs warfarin comparison, the model is stratified by age, non-elderly vs elderly (<70 or 70 in Japan and <80 or 80 years old elsewhere). For the dabigatran 150 mg vs warfarin comparison, an unstratified model is used, elderly patients outside the USA are excluded. Non-inferiority P value is one sided (alpha=0.025). Wald two-sided P value from (stratified) Cox
15 Patients with outcome event (%) Probability of event (%) 20 Time to death or thromboembolic event, or unplanned revascularization HR: 1.04 (95% CI: ) Non-inferiority 13.7% P= % Dabigatran (combined do dual therapy Warfarin triple therapy Dabigatran (combined dose) dual therapy (n=1744) Warfarin triple therapy (n=981) Time to first event (days) Non-inferiority P value is one sided (alpha=0.025). Results presented are Step 3 of hierarchical testing procedure, testing non-inferiority of dabigatran dual therapy (combined doses) to warfarin triple therapy in death or thromboembolic event and unplanned revascularization
16 Additional individual thromboembolic endpoints All-cause death Dabigatra n 110 mg dual therapy (n=981) n (%) Warfarin triple therapy (n=981) n (%) 55 (5.6) 48 (4.9) Stroke 17 (1.7) 13 (1.3) Unplanned revascularizat ion 76 (7.7) 69 (7.0) MI 44 (4.5) 29 (3.0) Stent thrombosis 15 (1.5) 8 (0.8) D110 DT vs warfarin TT Dabigatra n 150 mg dual therapy (n=763) Warfarin triple therapy (n=764) D150 DT vs warfarin TT HR (95% CI) P value HR (95% CI) P value n (%) n (%) 1.12 ( ) 1.30 ( ) 1.09 ( ) 1.51 ( ) 1.86 ( ) (3.9) 35 (4.6) (1.2) 8 (1.0) (6.7) 52 (6.8) (3.4) 22 (2.9) (0.9) 7 (0.9) 0.83 ( ) 1.09 ( ) 0.96 ( ) 1.16 ( ) 0.99 ( ) Results presented are times to event. Stent thrombosis is time to definite stent thrombosis
17
18


19 58 ετών, άρρεν Πρόσθιο NSTEMI
20
21
22

23 What are the implications for clinical practice in PCI? RE-DUAL PCI PIONEER AF-PCI PCIAF AF PCIAF AF AF R15 P2Y12 inhib. AF OR D150 AF D150 P2Y12 inhib. PCIAF D150 AF R20 AF PCIAF R2.5 ASA P2Y12 inhib. R20 AF D110 D110 P2Y12 inhib. D110 R15 PCIAF R10 P2Y12 inhib. R15 23
24 Canadian Cardiovascular Society Guidelines Recommend OAC + single AP after Elective PCI For patients with AF and recent elective PCI Age <65 and CHADS 2 =0 Age 65 or CHADS 2 1 ASA plus clopidogrel for 12 months OAC* plus clopidogrel for 12 months ASA alone after 12 months OAC* alone after 12 months *A NOAC is preferred over warfarin for patients with NVAF Macle L et al, Can J Cardiol 2016;32:
25
26
27
28
29


30 ΕΥΧΑΡΙΣΤΩ
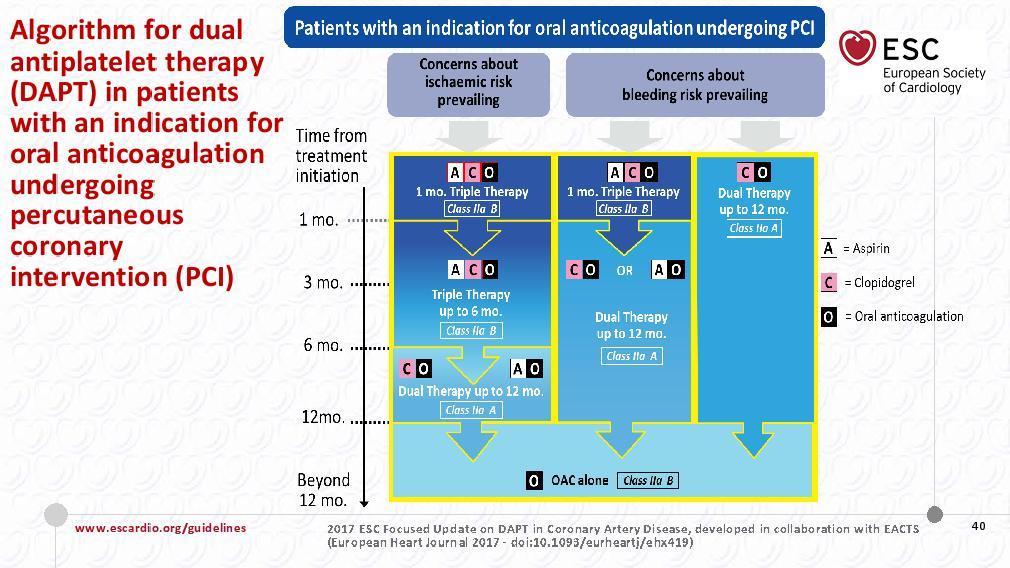
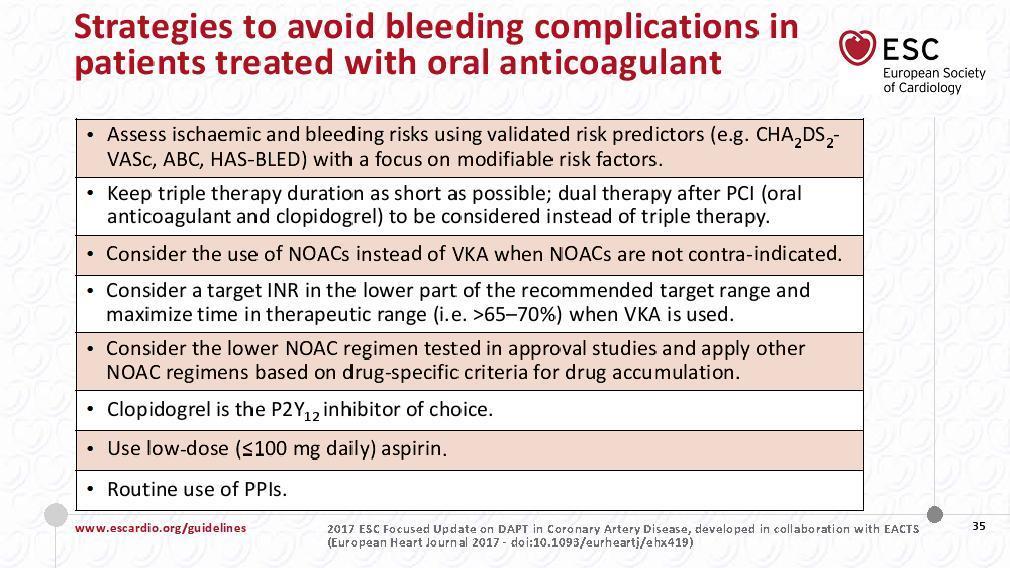
31 For patients requiring OAC, new ESC focused update recommends dual or triple therapy after PCI with stent depending on individual patient risk factors High bleeding risk + OAC + clopidogrel OAC + ASA + clopidogrel OAC + ASA or clopidogrel OAC alone High ischaemic risk* Class IIa B Class IIa A Class IIa B 1 month Up to 6 months Up to 12 months Beyond 12 months When a NOAC is used, the lowest dose effective for stroke prevention in AF should be applied Dabigatran 110 mg is the only reduced-dose NOAC to be fully tested for effectiveness in stroke prevention in AF *High ischaemic risk is considered as an acute clinical presentation or anatomical/procedural features, which might increase the risk for MI; Dabigatran 110 mg BID (Class IIa C), rivaroxaban 15 mg OD (Class IIb B), or apixaban 2.5 mg BID (Class IIa C) according to selected study population in pivotal studies; ASA, acetylsalicylic acid; Valgimigli et al. Eur Heart J
32 Guidelines recommend the following in patients with AF after PCI: 0 months 1 month 6 months 12 months Elective PCI with stent 1,2 Triple therapy OAC+A+C Dual therapy OAC+A or C OAC monotherapy High bleeding risk/low atherothrombotic risk: shorten dual therapy Urgent PCI after ACS 1 3 Triple therapy OAC+A+C Dual therapy OAC+A or C OAC monotherapy High bleeding risk/low atherothrombotic risk: shorten triple therapy High atherothrombotic risk/low bleeding risk: lengthen triple therapy In selected patients, dual therapy may be considered instead of triple therapy 1 European guidelines suggest that NOACs may be used in triple/dual therapy, 1 3 whereas US guidelines recommend a VKA 4,5 1. Kirchhof P et al, Eur Heart J 2016; doi: /eurheartj/ehw210; 2. Heidbuchel H et al, Europace 2015;17: ; 3. Windecker S et al, Eur Heart J 2014;35: ; 4. Amsterdam EA et al, Circulation 2014;130:e344 e426; 5. O Gara PT et al, J Am Coll Cardiol 2013;61:e78 e140

.")
33 Time to first ISTH major or CRNM bleeding event in relation to ticagrelor or clopidogrel Dabigatran 110 mg 110 DE-DAT dual Dabigatran 150 mg DE-DAT 150 dual therapy therapy Full analysis set presented. HRs and Wald CIs from Cox proportional-hazard model. For the dabigatran 110 vs warfarin comparison, the model is stratified by age, non-elderly vs elderly (<70 or 70 years in Japan and <80 or 80 years old elsewhere). For the dabigatran 150 vs warfarin comparison, an unstratified model is used, elderly patients outside the United States are excluded. Non-inferiority P value is one sided (alpha=0.025). Wald two-sided P value from (stratified) Cox proportional-hazard model (alpha=0.05). CI, confidence interval; CRNM, clinically relevant non-major; HR, hazard ratio; ISTH, International Society on Thrombosis and Haemostasis.
34 Early discontinuations (n) Primary reason for early discontinuation from treatment period 30 Group 3 (VKA plus DAPT) (n=697) Group 2 (rivaroxaban 2.5 mg BID plus DAPT) (n=706) Group 1 (rivaroxaban 15 mg OD plus single antiplatelet) (n=696) ** ** Early discontinuations (all-cause) Adverse event Bleeding adverse event Death Non-compliance with study drug Cause of early discontinuation * Physician decision ** ** Patient decision Early discontinuations were highest in the VKA plus DAPT group; discontinuation due to patient decision was significantly higher in this group vs both rivaroxaban groups. *p=0.016; **p<0.001 Gibson CM et al, New Engl J Med 2016; doi: /NEJMoa ] There were no patients lost to follow up.
35
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen
 PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
PCI in Patients with AF Optimizing Oral Anticoagulation Regimen Walid I. Saliba, MD Director, Atrial Fibrillation Center Heart and Vascular Institute Cleveland Clinic 1 Epidemiology and AF and PCI AF and
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ
 ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ Χρήστος Δ.Καλλιάνος Α Καρδιολογικό τμήμα και Ηλεκτροφυσιολογικό Εργαστήριο ΓΝΑ «Ο Ευαγγελισμός»
ΔΙΑΧΕΙΡΙΣΗ ΑΣΘΕΝΩΝ ΜΕ ΣΤΕΦΑΝΙΑΙΑ ΚΑΡΔΙΟΠΑΘΕΙΑ ΚΑΙ ΚΟΛΠΙΚΗ ΜΑΡΜΑΡΥΓΗ:ΚΙΝΔΥΝΟΙ ΚΑΙ ΟΦΕΛΗ ΔΙΠΛΗΣ ΚΑΙ ΤΡΙΠΛΗΣ ΘΕΡΑΠΕΙΑΣ Χρήστος Δ.Καλλιάνος Α Καρδιολογικό τμήμα και Ηλεκτροφυσιολογικό Εργαστήριο ΓΝΑ «Ο Ευαγγελισμός»
Study design: multicenter, randomized, open-label trial following a PROBE design
 Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Subgroup Analysis from the RE-DUAL PCI Trial Dual Antithrombotic Therapy with in Patients with Atrial Fibrillation Undergoing Percutaneous Coronary Intervention Jonas Oldgren, Philippe Gabriel Steg, Stefan
Which drug do you prefer for stable CAD? - P2Y12 inhibitor
 Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Which drug do you prefer for stable CAD? - P2Y12 inhibitor Jung Rae Cho, MD, PhD Cardiovascular Division, Department of Internal Medicine Kangnam Sacred Heart Hospital, Hallym University Medical Center,
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained
 Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
Triple Therapy After PCI in AF: A Quagmire Soon to be Drained Freek W.A. Verheugt Department of Cardiology, Onze Lieve Vrouwe Gasthuis (OLVG) Amsterdam, Netherlands DISCLOSURES FOR FREEK W. A. VERHEUGT
Stable CAD, Elective Stenting and AFib
 Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Stable CAD, Elective Stenting and AFib Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Intensive Care Medicine Wilhelminenhospital & Sigmund Freud Private University, Medical School
Clinical and Economic Value of Rivaroxaban in Coronary Artery Disease
 CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
CHRISTOPHER B. GRANGER, MD Professor of Medicine Division of Cardiology, Department of Medicine; Director, Cardiac Care Unit Duke University Medical Center, Durham, NC Clinical and Economic Value of Rivaroxaban
The Challenge. Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Anticoagulation/Stroke
 Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
Anticoagulation/Stroke Warfarin v new oral anticoagulants post PCI Warfarin or Novel Oral Anti-Coagulants in the PCI patient? Gerry Devlin Chairs: Phillip Matsis & Tony Scott Gerry Devlin Honorary Associate
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING
 NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
NAVIGATING THROMBOSIS AND BLEEDING AT THE INTERSECTION OF ATRIAL FIBRILLATION AND CORONARY STENTING Snehal H. Bhatt, Pharm.D., BCPS-AQ Cardiology, FASHP, AACC Associate Professor of Pharmacy Practice MCPHS
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many?
 Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
Management of Patients with Atrial Fibrillation and Stents: Is Three Drugs Too Many? Neal S. Kleiman, MD Houston Methodist DeBakey Heart and Vascular Center, Houston, TX Some Things Are Really Clear 2013
3/23/2017. Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate Europace Oct;14(10): Epub 2012 Aug 24.
: Epub 2012 Aug 24.") Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017
 Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
Angelika Cyganska, PharmD Austin T. Wilson, MS, PharmD Candidate 2017 Explain the efficacy and safety of triple therapy, in regards to thromboembolic and bleeding risk Summarize the guideline recommendations
TRIPLE THERAPY, NOACs with concurrent indication for DAPT. Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust
 TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
TRIPLE THERAPY, NOACs with concurrent indication for DAPT Paul Wright Lead Cardiac Pharmacist The Heart, UCLH NHS Foundation Trust Content Why consider triple therapy What we know of triple therapy Current
Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές
 4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
4 ο ΠΑΝΕΛΛΗΝΙΟ ΑΡΡΥΘΜΙΟΛΟΓΙΚΟ ΣΥΝΕΔΡΙΟ 21-22 ΣΕΠΤΕΜΒΡΙΟΥ 2018 HILTON, ΑΘΗΝΑ Στεφανιαίος ασθενής με μη βαλβιδική Κολπική Μαρμαρυγή - Νέες στρατηγικές Ι. Κανακάκης MD, PhD Διευθυντής Αιμοδυναμικού Τμήματος
Optimal lenght of DAPT in different clinical scenarios
 Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
Optimal lenght of DAPT in different clinical scenarios After PCI with DES in the light of recent and ongoing studies Dr Grégoire Rangé / CH Chartres / France DAPT duration depend on the evolution of risk
When and how to combine antiplatelet agents and anticoagulant?
 When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
When and how to combine antiplatelet agents and anticoagulant? Christophe Beauloye, MD, PhD Head, Division of Cardiology Cliniques Universitaires Saint-Luc Brussels, Belgium Introduction Anticoagulation
Robert C. Welsh, MD, FRCPC Professor of Medicine, University of Alberta Zone Clinical Department Head, Cardiac Sciences
 Managing Atrial Fibrillation and ACS/PCI Applying New Evidence to Clinical Practice Dual Anti-Thrombotic Therapy in Acute Coronary Syndromes (ACS) and Afib + PCI/ACS Patients Robert C. Welsh, MD, FRCPC
Managing Atrial Fibrillation and ACS/PCI Applying New Evidence to Clinical Practice Dual Anti-Thrombotic Therapy in Acute Coronary Syndromes (ACS) and Afib + PCI/ACS Patients Robert C. Welsh, MD, FRCPC
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference Dubai: October Acute Coronary Syndromes
 8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
8th Emirates Cardiac Society Congress in collaboration with ACC Middle East Conference 2017 Dubai: 19-21 October 2017 Acute Coronary Syndromes Antonio Colombo Centro Cuore Columbus and S. Raffaele Scientific
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원
 Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
Special Conditions of NOAC PCI 가톨릭의대 순환기내과 장성원 Issues on Patients with NOAC PCI Peri-procedural management CKD or dialysis Cardioversion Neurological situations Dual Antiplatelet Therapy with Oral Anticoagulants
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome
 State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
State of the Art in the ACS Atrial Fibrillation Overlap Syndrome C. Michael Gibson, M.S., M.D. Professor of Medicine, Harvard Medical School Chief, Clinical Research, Beth Israel Deaconess CV Division
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1)
") Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Low Dose Rivaroxaban Versus Aspirin, in Addition to P2Y12 Inhibition, in Acute Coronary Syndromes (GEMINI-ACS-1) Caitlin C. Akerman, PharmD PGY2 Cardiology Resident WakeMed Health & Hospitals Raleigh,
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Triple Therapy: A review of the evidence in acute coronary syndrome. Stephanie Kling, PharmD, BCPS Sanford Health
 Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
Triple Therapy: A review of the evidence in acute coronary syndrome Stephanie Kling, PharmD, BCPS Sanford Health Objectives 1. Describe how the presented topic impacts patient outcomes. 2. Review evidence
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY. Nick Collins February 2017
 GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
GRAND ROUNDS - DILEMMAS IN ANTICOAGULATION AND ANTIPLATELET THERAPY Nick Collins February 2017 DISCLOSURES Before I commence Acknowledge.. Interventional Cardiologist Perception evolved. Interventional
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
News Release. For UK Media
 News Release For UK Media Bayer plc 400 South Oak Way Reading RG2 6AD www.bayer.co.uk Bayer s Xarelto (rivaroxaban) in combination with single antiplatelet therapy receives positive CHMP opinion for treatment
News Release For UK Media Bayer plc 400 South Oak Way Reading RG2 6AD www.bayer.co.uk Bayer s Xarelto (rivaroxaban) in combination with single antiplatelet therapy receives positive CHMP opinion for treatment
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events
 Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Changing Course: Anticoagulation in Secondary Prevention of Cardiovascular Disease Events Deepak L. Bhatt, MD, MPH Executive Director Interventional Cardiovascular Programs Brigham and Women s Hospital
Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland
 Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Advances in Antiplatelet Therapy in PCI and ACS Stephan Windecker Department of Cardiology Swiss Cardiovascular Center and Clinical Trials Unit Bern Bern University Hospital, Switzerland Targets for Platelet
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs
 Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
Thrombin Receptor Antagonists and Other New Oral Antiplatelets Drugs David J. Moliterno, MD Professor and Chairman Department of Internal Medicine The University of Kentucky Linda and Jack Gill Heart Institute
DECLARATION OF CONFLICT OF INTEREST. Lecture fees: AstraZeneca, Ely Lilly, Merck.
 DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
DECLARATION OF CONFLICT OF INTEREST Lecture fees: AstraZeneca, Ely Lilly, Merck. Risk of stopping dual therapy. S D Kristensen, FESC Aarhus Denmark Acute coronary syndrome: coronary thrombus Platelets
Antiplatelet and Anti-Thrombotic Therapy. Ivan Anderson, MD RIHVH Cardiology
 Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Antiplatelet and Anti-Thrombotic Therapy Ivan Anderson, MD RIHVH Cardiology Outline Anti-thrombotic therapy Risk stratification of stroke with atrial fibrillation DVT and PE treatment Pharmacology Anti-platelet
Byeong-Keuk Kim, M.D. Ph D. Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea
 Byeong-Keuk Kim, M.D. Ph D Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea CASE, M/64 C.C; Recently aggravated chest discomfort for 3 days
Byeong-Keuk Kim, M.D. Ph D Division of Cardiology, Severance Cardiovascular Hospital Yonsei University College of Medicine, Seoul, Korea CASE, M/64 C.C; Recently aggravated chest discomfort for 3 days
Antiplatelet Therapy in Patients on Anticoagulation
 Antiplatelet Therapy in Patients on Anticoagulation Ziad A Ali MD DPhil Cardiovascular Research Foundation Columbia University New York, Medical NY Center Cardiovascular Research Foundation Disclosure
Antiplatelet Therapy in Patients on Anticoagulation Ziad A Ali MD DPhil Cardiovascular Research Foundation Columbia University New York, Medical NY Center Cardiovascular Research Foundation Disclosure
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015
 in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015") Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Dual antiplatelet therapy (DAPT) in the era of Novel Oral Anticoagulants (NOACs) SACIS 2015 Wesam A Alhejily MD FRCPC FACP FACC FSCAI Assistant Professor of Medicine Chief Of Adult Cardiology Consultant
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Antithrombotic therapy in the ACS patient with atrial fibrillation
 Antithrombotic therapy in the ACS patient with atrial fibrillation Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Emergency Medicine Wilhelminenhospital Vienna, Austria Great Minds,
Antithrombotic therapy in the ACS patient with atrial fibrillation Kurt Huber, MD, FESC, FACC, FAHA 3 rd Medical Department Cardiology & Emergency Medicine Wilhelminenhospital Vienna, Austria Great Minds,
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation
 Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
Let s Gi e The So ethi g To Clot About: Controversies in Anticoagulation Janna Beavers, MS, PharmD, BCPS Cardiology Clinical Pharmacy Specialist WakeMed Health & Hospitals Raleigh, NC March 13, 2018 Pharmacist
New Study Presented at American Heart Association (AHA) Scientific Sessions 2016:
 Scientific Sessions 2016:") Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com New Study Presented at American Heart Association (AHA) Scientific Sessions
Investor News Not intended for U.S. and UK Media Bayer AG Investor Relations 51368 Leverkusen Germany www.investor.bayer.com New Study Presented at American Heart Association (AHA) Scientific Sessions
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely
 Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
Anticoagulants and antiplatelet therapy in the older patient: Choosing wisely Rajiv Gulati, MD PhD Advances in Cardiac Arrhythmias & Great Innovations in Cardiology Torino, October 2015 2015 MFMER 3477310-1
TRIAL UPDATE 1. ISAR TRIPLE SECURITY Trial. Dr Deven Patel Royal Free Hospital
 TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
TRIAL UPDATE 1 ISAR TRIPLE SECURITY Trial Dr Deven Patel Royal Free Hospital NO CONFLICT OF INTEREST TO DECLARE ISAR TRIPLE Comparison of 6 weeks vs 6 months Triple Therapy in patients on oral anticoagulation
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure?
 The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
The Poor Long-Term Candidate for Warfarin: NOAC or Left Atrial Appendage Closure? Suneet Mittal, MD, FACC, FHRS Director, Electrophysiology Laboratory Valley Health System Ridgewood, NJ and New York, NY
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES
 UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
UPDATES FROM THE 2018 ANTIPLATELET GUIDELINES Claudia Bucci BScPhm, PharmD Clinical Coordinator, Cardiovascular Diseases Sunnybrook Health Sciences Centre 21st Annual Contemporary Therapeutic Issues in
DIRECT ORAL ANTICOAGULANTS
 2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
2017 Cardiovascular Symposium DIRECT ORAL ANTICOAGULANTS ERNESTO UMAÑA, MD, FACC ORAL ANTICOAGULANTS Vitamin K Antagonists (VKAs): Warfarin Non Vitamin K Antagonists Direct oral anticoagulants Novel Oral
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants
 Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
Antiplatelet Therapy: Current Recommendations for Choice of Agent and Concurrent Therapy with Warfarin and Novel Oral Anticoagulants S. Hinan Ahmed, MD Anti-platelet Therapy: Simple Answer Bare metal stent
NOACs in AF. Dr Colin Edwards Auckland Heart Group and Waitemata DHB. Dr Fiona Stewart Auckland Heart Group and Auckland DHB
 NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
NOACs in AF Dr Colin Edwards Auckland Heart Group and Waitemata DHB Dr Fiona Stewart Auckland Heart Group and Auckland DHB Conflict of Interest Dr Fiona Stewart received funding from Pfizer to attend the
Additional Contributor: Glenn Levine (USA).
.") 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the Management
2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) The Task Force for the Management
Disclosure Slide. Controversies in Anticoagulation. Presenter Disclosure Information. Challenges in Anticoagulation
 1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
1:15 2:15 PM Challenges in Anticoagulation SPEAKER Nasser Lakkis, MD, FACC, FSCAI Presenter Disclosure Information The following relationships exist related to this presentation: Nasser Lakkis, MD, FACC,
RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in
 RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in Christopher P. Cannon Deepak L Bhatt, patients Jonas Oldgren, Gregory with YH Lip, atrial Stephen G
RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in Christopher P. Cannon Deepak L Bhatt, patients Jonas Oldgren, Gregory with YH Lip, atrial Stephen G
ΔΟΡΥΦΟΡΙΚΟ ΣΥΜΠΟΣΙΟ. Αντιπηκτική αγωγή στη σύγχρονη κλινική πράξη το 2017
 ΔΟΡΥΦΟΡΙΚΟ ΣΥΜΠΟΣΙΟ Αντιπηκτική αγωγή στη σύγχρονη κλινική πράξη το 2017 Διαχείριση του θρομβωτικού κινδύνου σε ασθενείς με μη βαλβιδική κολπική μαρμαρυγή και υψηλό καρδιαγγειακό κίνδυνο Γ.Ν.Α. «Ο Ευαγγελισμός»
ΔΟΡΥΦΟΡΙΚΟ ΣΥΜΠΟΣΙΟ Αντιπηκτική αγωγή στη σύγχρονη κλινική πράξη το 2017 Διαχείριση του θρομβωτικού κινδύνου σε ασθενείς με μη βαλβιδική κολπική μαρμαρυγή και υψηλό καρδιαγγειακό κίνδυνο Γ.Ν.Α. «Ο Ευαγγελισμός»
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS
 A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
A Randomized Trial Evaluating Clinically Significant Bleeding with Low-Dose Rivaroxaban vs Aspirin, in Addition to P2Y12 inhibition, in ACS Magnus Ohman MB, on behalf of the GEMINI-ACS-1 Investigators
Simon Robinson. (on behalf of CCS Guideline Group)
") 2018 Canadian Cardiovascular Society (CCS)/Canadian Association of Interventional Cardiology (CAIC) Focused Update of the Guidelines for the use of Antiplatelet Therapy Simon Robinson (on behalf of CCS
2018 Canadian Cardiovascular Society (CCS)/Canadian Association of Interventional Cardiology (CAIC) Focused Update of the Guidelines for the use of Antiplatelet Therapy Simon Robinson (on behalf of CCS
Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients
 SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
SYP.CLO-A.16.07.01 Balancing Efficacy and Safety of P2Y12 Inhibitors for ACS Patients dr. Hariadi Hariawan, Sp.PD, Sp.JP (K) TOPICS Efficacy Safety Consideration from Currently Available Antiplatelet Agents
A New Era for NOACs: What Does the Future Hold? CME
 This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/884772 www.medscape.org A New Era for NOACs: What Does the Future Hold? CME Manesh
This article is a CME certified activity. To earn credit for this activity visit: http://www.medscape.org/viewarticle/884772 www.medscape.org A New Era for NOACs: What Does the Future Hold? CME Manesh
Acute coronary syndromes A European viewpoint. Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT
 Acute coronary syndromes A European viewpoint Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT Potential conflicts of interest In the past 2 years Felicita
Acute coronary syndromes A European viewpoint Felicita Andreotti, MD PhD FESC Catholic University Hospital Cardiovascular Diseases - Rome, IT Potential conflicts of interest In the past 2 years Felicita
The Korean Society of Cardiology COI Disclosure
 The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
The Korean Society of Cardiology COI Disclosure Name of First Author: Yongwhi Park The authors have no financial conflicts of interest to disclose concerning the presentation 2017 Annual Spring Scientific
The Great debate: thrombocardiology post-compass
 The Great debate: thrombocardiology post-compass Anticoagulation should replace antiplatelets in CAD prevention - CON Jean-Philippe COLLET Jean-philippe.collet@psl.aphp.fr Sorbonne Université_Action Study
The Great debate: thrombocardiology post-compass Anticoagulation should replace antiplatelets in CAD prevention - CON Jean-Philippe COLLET Jean-philippe.collet@psl.aphp.fr Sorbonne Université_Action Study
ANTIPLATELET REGIMENS:
 ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
ANTIPLATELET REGIMENS: How Long, How Many? John Carter Hemphill, M.D., F.A.C.C. Chattanooga Heart Institute February 10, 2018 I have no financial disclosures. DISCLOSURES: OBJECTIVES Understand current
CURRENT OPINION. European Heart Journal (2014) 35, doi: /eurheartj/ehu298
 35, doi: /eurheartj/ehu298") European Heart Journal (2014) 35, 3155 3179 doi:10.1093/eurheartj/ehu298 CURRENT OPINION Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or
European Heart Journal (2014) 35, 3155 3179 doi:10.1093/eurheartj/ehu298 CURRENT OPINION Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death!
 Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Oral anticoagulation/antiplatelet therapy in the secondary prevention of ACS patients the cost of reducing death! Robert C. Welsh, MD, FRCPC Associate Professor of Medicine Director, Adult Cardiac Catheterization
Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia
 Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Anticoagulanti e mono-antiaggregazione: a chi, quali e per quanto tempo Paolo Gresele Dipartimento di Medicina Sezione di Medicina Interna e Cardiovascolare Università di Perugia Anticoagulazione: Bologna,
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Days
 Post ACS Care 2013 Clinical dilemmas Christopher Granger, MD Professor of Medicine Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic
Post ACS Care 2013 Clinical dilemmas Christopher Granger, MD Professor of Medicine Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic
Optimal Duration of Dual Anti- Platelet Therapy. December 19, 2015
 Optimal Duration of Dual Anti- Platelet Therapy December 19, 2015 John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco Source: The New Yorker 1 Optimal Duration of
Optimal Duration of Dual Anti- Platelet Therapy December 19, 2015 John S. MacGregor, M.D., Ph.D. Professor of Medicine University of California San Francisco Source: The New Yorker 1 Optimal Duration of
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME. TARGET AUDIENCE: All Canadian health care professionals.
 OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
OUTPATIENT ANTITHROMBOTIC MANAGEMENT POST NON-ST ELEVATION ACUTE CORONARY SYNDROME TARGET AUDIENCE: All Canadian health care professionals. OBJECTIVE: To review the use of antiplatelet agents and oral
FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS
 New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
New Horizons In Atherothrombosis Treatment 2012 순환기춘계학술대회 FACTOR Xa AND PAR-1 BLOCKER : ATLAS-2, APPRAISE-2 & TRACER TRIALS Division of Cardiology, Jeonbuk National University Medical School Jei Keon Chae,
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
North Wales Cardiac Network Guidelines on oral antiplatelet therapy in cardiovascular disease
 Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Guidelines on oral antiplatelet therapy in cardiovascular disease This guidance should be considered as one part of the wider therapeutic management of patients. The indication for antiplatelet therapy
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center
 Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Prasugrel vs. Ticagrelor in ACS/PCI Which one to choose? V. Voudris MD FESC FACC 2 nd Cardiology Division Onassis Cardiac Surgery Center Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes
Προβληματισμοι στην χρηση αντιαιμοπεταλιακων στα οξέα ισχαιμικά σύνδρομα
 Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Α ΚΑΡΔΙΟΛΟΓΙΚΗ ΚΛΙΝΙΚΗ ΚΑΙ ΟΜΩΝΥΜΟ ΕΡΓΑΣΤΗΡΙΟ ΙΑΤΡΙΚΗ ΣΧΟΛΗ ΠΑΝΕΠΙΣΤΗΜΙΟΥ ΑΘΗΝΩΝ ΙΠΠΟΚΡΑΤΕΙΟ ΓΕΝΙΚΟ ΝΟΣΟΚΟΜΕΙΟ ΑΘΗΝΩΝ Διευθυντής: Καθηγητής ΔΗΜΗΤΡΙΟΣ ΤΟΥΣΟΥΛΗΣ Προβληματισμοι στην χρηση αντιαιμοπεταλιακων
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
AF & CAD. Management and prognosis
 AF & CAD Management and prognosis Maria Agelaki Cons. Cardiologist Red Cross GN Hosp. AF and CAD share in common Most common arrhythmia and cardiovascular disease respectively High prevalence in general
AF & CAD Management and prognosis Maria Agelaki Cons. Cardiologist Red Cross GN Hosp. AF and CAD share in common Most common arrhythmia and cardiovascular disease respectively High prevalence in general
A Patient with Chest Pain and Atrial Fibrillation
 A Patient with Chest Pain and Atrial Fibrillation Kurt Huber, Vienna, Austria Declaration of Interest Lecturing & Consulting Activities: AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi
A Patient with Chest Pain and Atrial Fibrillation Kurt Huber, Vienna, Austria Declaration of Interest Lecturing & Consulting Activities: AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, Daiichi
Triple Antithrombotic Therapy: Is it Time to Drop the Aspirin?
 HOSPITAL CHRONICLES 2015, 10(1): 7 18 Review Triple Antithrombotic Therapy: Is it Time to Drop the Aspirin? Prokopis Papadimitriou, MD, MSc Abstract Department of Cardiology, Evagelismos General Hospital
HOSPITAL CHRONICLES 2015, 10(1): 7 18 Review Triple Antithrombotic Therapy: Is it Time to Drop the Aspirin? Prokopis Papadimitriou, MD, MSc Abstract Department of Cardiology, Evagelismos General Hospital
Eliquis and plavix combination therapy
 Eliquis and plavix combination therapy ELIQUIS Dosing for Patients With NVAF. patients treated with aspirin or the combination of bleeding or completion of a course of therapy,. 9-11-2011 Thrombosis is
Eliquis and plavix combination therapy ELIQUIS Dosing for Patients With NVAF. patients treated with aspirin or the combination of bleeding or completion of a course of therapy,. 9-11-2011 Thrombosis is
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium
 ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
ACS: What happens after the acute phase? Frans Van de Werf, MD, PhD Leuven, Belgium 4/14/2011 Cumulative death rates in 3721 ACS patients from UK and Belgium at ± 5 year (GRACE) 25 20 15 19% TOTAL 14%
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008.
 Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Cardiovascular Health Nova Scotia Update to Antiplatelet Sections of the Nova Scotia Guidelines for Acute Coronary Syndromes, 2008. ST Elevation Myocardial Infarction (STEMI)-Acute Coronary Syndrome Guidelines:
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI
 Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Δοκιμασίες λειτουργικότητας αιμοπεταλίων και PCI Ομάδες Εργασίας Φεβρουάριος 2016 Ξανθοπούλου Ιωάννα Καρδιολόγος Επιμ Β ΠΓΝΠατρών Nothing to disclose Platelet function testing (PFT) is helpful in identifying
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural. Miguel Valderrábano, MD
 Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
Individual Therapeutic Selection Of Anti-coagulants And Periprocedural Management Miguel Valderrábano, MD Outline Does the patient need anticoagulation? Review of clinical evidence for each anticoagulant
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable?
 SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
SCA ST- : recommandations européennes 2015 La durée de la bithérapie : à géométrie variable? tielle est 2 ré Totielle est interdite. Prof. Marco Roffi Hôpitaux Universitaires de Genève Research funding
Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom?
 Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom? Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Patients (%) Patients
Antithrombotic therapy in CAD patients with concomitant NAFV: why and for whom? Institut de Cardiologie de la Pitié-Salpêtrière jean-philippe.collet@psl.aphp.fr www.action-coeur.org Patients (%) Patients
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Is there enough evidence for DAPT after endovascular intervention for PAOD?
 Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
Is there enough evidence for DAPT after endovascular intervention for PAOD? Prof. I. Baumgartner Head Clinical & Interventional Angiology University Hospital Bern Disclosure Speaker name:...i. Baumgartner...
ANTIPLATELET THERAPY ANTIPLATELET THERAPY ANTIPLATELET THERAPY
 ANTIPLATELET THERAPY 2018 UPDATE ANTIPLATELET THERAPY ANTIPLATELET THERAPY About this Pocket Guide This pocket guide is a quick-reference tool that features diagnostic and management recommendations based
ANTIPLATELET THERAPY 2018 UPDATE ANTIPLATELET THERAPY ANTIPLATELET THERAPY About this Pocket Guide This pocket guide is a quick-reference tool that features diagnostic and management recommendations based
PRACTICAL MANAGEMENT OF NOAC s December 8,
 PRACTICAL MANAGEMENT OF NOAC s December 8, 2017 1 Faculty Disclosure Faculty: John Eikelboom MBBS, MSc, FRCPC Jack Hirsh/PHRI Chair in Thrombosis and Atherosclerosis Career Award, Heart and Stroke Foundation
PRACTICAL MANAGEMENT OF NOAC s December 8, 2017 1 Faculty Disclosure Faculty: John Eikelboom MBBS, MSc, FRCPC Jack Hirsh/PHRI Chair in Thrombosis and Atherosclerosis Career Award, Heart and Stroke Foundation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital
 Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Complicated issues in GI bleeding for internists? Nonthalee Pausawasdi, M.D. Faculty of Medicine Siriraj Hospital Complicated issues in GI bleeding; Survey results from internists Optimal resuscitation
Study Design 5/2/2018. Complex NOAC Cases. Outcomes Overall Population. Key Inclusion and Exclusion Criteria
 /2/218 Med Work: Complex OAC Cases Kori Leblanc, PharmD Cardiovascular Pharmacotherapy Specialist and Research Coordinator Department of Pharmacy - University Health etwork Assistant Professor, Leslie
/2/218 Med Work: Complex OAC Cases Kori Leblanc, PharmD Cardiovascular Pharmacotherapy Specialist and Research Coordinator Department of Pharmacy - University Health etwork Assistant Professor, Leslie
Role of Clopidogrel in Acute Coronary Syndromes. Hossam Kandil,, MD. Professor of Cardiology Cairo University
 Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Role of Clopidogrel in Acute Coronary Syndromes Hossam Kandil,, MD Professor of Cardiology Cairo University ACS Treatment Strategies Reperfusion/Revascularization Therapy Thrombolysis PCI (with/ without
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management
 Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Surveying the Landscape of Oral Antiplatelet Therapy in Acute Coronary Syndrome Management Jeffrey S Berger, MD, MS Assistant Professor of Medicine and Surgery Director of Cardiovascular Thrombosis Disclosures
Quoi de neuf en cardio-gériatrie? Pr Olivier Hanon Hôpital Broca, Paris
 Quoi de neuf en cardio-gériatrie? Pr Olivier Hanon Hôpital Broca, Paris Déclaration de relations professionnelles et liens d intérêt Novartis, Daiichi-Sankyo, Boehringer-Ingelheim, Bayer, BMS, Pfizer,
Quoi de neuf en cardio-gériatrie? Pr Olivier Hanon Hôpital Broca, Paris Déclaration de relations professionnelles et liens d intérêt Novartis, Daiichi-Sankyo, Boehringer-Ingelheim, Bayer, BMS, Pfizer,
RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in patients with atrial fibrillation
 RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in patients with atrial fibrillation Christopher P. Cannon Deepak L Bhatt, Jonas Oldgren, Gregory YH Lip,
RE-DUAL PCI: dual antithrombotic therapy with dabigatran after percutaneous coronary intervention in patients with atrial fibrillation Christopher P. Cannon Deepak L Bhatt, Jonas Oldgren, Gregory YH Lip,
Dual Antiplatelet Therapy: Time for a Paradigm Shift?
 Dual Antiplatelet Therapy: Time for a Paradigm Shift? 5 years after PLATO Experience from the Daily Clinical Practice Hans Rickli Goals with antithrombotic treatment Acute coronary syndrome Risk reduction
Dual Antiplatelet Therapy: Time for a Paradigm Shift? 5 years after PLATO Experience from the Daily Clinical Practice Hans Rickli Goals with antithrombotic treatment Acute coronary syndrome Risk reduction
Novel Anticoagulants PHYSICIANS UPDATE 2014
 Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Novel Anticoagulants PHYSICIANS UPDATE 2014 Farouk Mookadam MD FRCPC FACC MSc Professor College of Medicine Mayo Consultant Cardiovascular Diseases Medical Director Anticoagulation Clinic Assoc Programme
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Anti-thromboticthrombotic drugs
 Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
Atrial Fibrillation 2011: Anticoagulation strategies and clinical outcomes Panos E. Vardas President Elect of the ESC, Prof. of Cardiology, University Hospital of Crete Clinical outcomes affected by AF
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Secondary Stroke Prevention: A Precautionary Tale
 Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
Secondary Stroke Prevention: A Precautionary Tale Kirsten George-Phillips, BSP Clinical Practice Leader, AHS Clinical Pharmacist, AHS Owen Stroke Prevention Clinic Learning Objectives! Examine literature
A new era in the treatment of peripheral artery disease (PAD)?
?") A new era in the treatment of peripheral artery disease (PAD)? Prof. Dr. Jan Beyer-Westendorf Head of Thrombosis Research, University Hospital Carl Gustav Carus, TU Dresden; Germany Senior Lecturer Thrombosis
A new era in the treatment of peripheral artery disease (PAD)? Prof. Dr. Jan Beyer-Westendorf Head of Thrombosis Research, University Hospital Carl Gustav Carus, TU Dresden; Germany Senior Lecturer Thrombosis