Draft a protocol for a RCT for assessing the effectiveness of Alveolar Recruitment Maneuver During Cesarean Section in Improvement of Lung Compliance
|
|
|
- Meredith Cameron
- 6 years ago
- Views:
Transcription
1 Draft a protocol for a RCT for assessing the effectiveness of Alveolar Recruitment Maneuver During Cesarean Section in Improvement of Lung Compliance Diamanto Aretha Πρόγραμμα Μεταπτυχιακών Σπουδών ΜΕΘΟΔΟΛΟΓΙΑ ΒΙΟÏΑΤΡΙΚΗΣ ΕΡΕΥΝΑΣ, ΒΙΟΣΤΑΤΙΣΤΙΚΗ ΚΑΙ ΚΛΙΝΙΚΗ ΒΙΟΠΛΗΡΟΦΟΡΙΚΗ ΠΑΝΕΠΙΣΤΗΜΙΟ ΛΑΡΙΣΣΑΣ ΤΜΗΜΑ ΙΑΤΡΙΚΗΣ
2 Table of Contents Title page... 5 Study Title... 5 Recruitment maneuver (RM) and Positive End Expiratory Pressure (PEEP)... 5 Indication studied... 5 Brief Description... 5 Patient Enrollment, Start and Completion date... 5 Protocol Identification... 5 Principal Investigator and more information... 5 Sponsor... 6 Ethics... 6 Patient Information and Consent... 6 Abbreviations... 7 Abstract... 8 Introduction... 9 Atelectasis formation... 9 Atelectasis during Anesthesia... 9 Ventilation Induced Lung Injury... 9 Cesarean Section and General Anesthesia Study objectives Investigational Plan Study Population and control group Inclusion criteria Exclusion criteria Removal of Patients from therapy Randomization
3 Treatments Anesthetic technique (prior and post-manipulation therapy) Ventilatory Management (time and method of RM) Study Design Ventilatory Management Flowchart Blinding procedure Measurements Primary end-point Secondary measurements Follow up measurements Statistical analysis Patients Records Data Presentation Plan Flow chart: Efficacy and Safety issues: End of treatment End of Study Adverse events: Preliminary Data Results Discussion: Previous studies Limitations of the study Appendix Appendix Appendix 3 - Demographic intra- and post-operative patient s data Appendix 4 - Mechanical ventilation patient s data Appendix 5 - Haemodynamic patient s data
4 Appendix 6 Patient s Blood gas data References
5 Title page Study Title A phase II Randomized Control Trial to assess the effectiveness of Alveolar Recruitment Maneuver During Cesarean Section in Improvement of Lung Compliance Recruitment maneuver (RM) and Positive End Expiratory Pressure (PEEP) RM is the application of a sustained increase in positive pressure to the breathing airway in order to re-open collapsed alveoli or, in other words, the periodic delivery of passive breaths at high pressure and volume, which may improve alveolar recruitment and oxygenation. PEEP is defined as an elevation of transpulmonary pressures at the end of expiration. PEEP contributes to the re-opening of collapsed alveoli and opposes alveolar collapse thus improving V/Q matching (ventilation/perfusion ratio). Indication studied The investigators will test the hypothesis that RM during cesarean section, in women under general anesthesia improves lung compliance and gas exchange. The investigators will apply RM and leave PEEP at 8cmH2O and ventilation with low tidal volume in pregnant women who decided to have a cesarean section under general anesthesia. The investigators believe and will try to prove that RM improves lung compliance. Brief Description This will be an Interventional, Prevention, Parallel Assignment, Double Blind (patient, caregiver, outcomes Assessor), Randomized; Safety/Efficacy Study. We will use two parallel groups of pregnant women. In the first group we will use RM, PEEP and low tidal volume during mechanical ventilation (RM Group) while in the second group (Control Group) we will use the standard method (not RM, not PEEP and standard tidal volume). The estimated duration of the study will be 6 months. Patient Enrollment, Start and Completion date Enrollment: 90 patients Study Start Date: April 2015 Primary Completion Date: September 2015 Study Completion Date: September 2015 Protocol Identification ClinicalTrials.gov Identifier: NCT Study ID Number: Lung Recruitment in Cesareans GHPyrgosRECProt [RECProt010113] Principal Investigator and more information
6 Diamanto Aretha, Anesthesiology Consultant, MD, PhD, General Hospital of Pyrgos, tel: , mob: Sponsor General Hospital Of Pyrgos, Syntriada Pyrgos, 27100, tel: Ethics The Institutional Review Board will review and approve the study. The study will be performed in compliance with good clinical practice (GCP): INTERNATIONAL CONFERENCE ON HARMONISATION OF TECHNICAL REQUIREMENTS FOR REGISTRATION OF PHARMACEUTICALS FOR HUMAN USE ICH HARMONISED TRIPARTITE GUIDELINE STRUCTURE AND CONTENT OF CLINICAL STUDY REPORTS Patient Information and Consent Written informed consent will be obtained obtained from all patients at allocation. 6
7 Abbreviations RM: Recruitment Maneuver FRC: functional residual capacity Com dyn: Dynamic compliance dv/dp: difference in alveolar volume/difference in inspiratory pressure P peak: Peak airway inspiratory pressure PEEP: Positive end expiratory pressure V/Q: ventilation/perfusion ratio VILI: ventilation induced lung injury GA: General anesthesia ALI: Acute lung injury SBP: Systolic blood pressure DBP: Diastolic blood pressure MAP: Mean arterial pressure BPM: Beats per minute (heart rate) ETCO 2: End tidal CO 2 ITT: Intension to Treat LOCF: last observation carried forward PCV: Pressure Control Ventilation VCV: Volume Control Ventilation
8 Abstract Introduction: In pregnant women the supine position, during cesarean section, reduces functional residual capacity (FRC) and worsens lung compliance. In a prospective randomized double-blind clinical trial the investigators will test the hypothesis that alveolar recruitment maneuver (RM) during cesarean section, and after delivery, in women under general anesthesia improves lung compliance. The primary end point of the study will be the improvement in dynamic lung compliance (dv/dp) while the improvement in gas exchange (increase in PO 2, PO 2/FiO 2, PH and SpO 2 and decrease in PCO 2 and end-tidal CO 2) and difference in P peak will be the secondary endpoints of the study. Materials and Methods: Women undergoing cesarean section will prospectively assigned to one of two groups. In the RM group, one minute after delivery, the investigators will apply RM: The ventilator will be switched to pressure control mode (from volume control) and the inspiratory time will be increased to 50%. The Positive End Expiratory Pressure (PEEP) will be increased up to 15cmH 2O and the Positive End Inspiratory Pressure (Ppeak) progressively will be increased up to 45cmH 2O. The whole RM will last 2 minutes. Then, volume control ventilation will be used again and PEEP step wised will be decreased to 8cmH 2O. Women in the RM group will be ventilated with low tidal volume after the RM (6 ml/kg). In the control group, the investigators will not use lung RM at all. Women in this group will be ventilated with higher tidal volume (8 ml/kg), which is a common tidal volume in everyday clinical practice. In both groups, lung compliance will be measured (dynamic compliance) as dv/dp (ml/cmh 2O). Measures will be assessed before RM but after delivery, 3 minutes after delivery and after recruitment, 10 and 20 minutes after recruitment. At all time points Ppeak, blood pressure, heart beats per minutes, oxygen saturation, end-tidal CO 2 and blood gas will also be measured too. In order to detect clinically meaningful differences, a power analysis will be conducted between the two study groups with regards to dynamic lung compliance (dv/dp), which is the primary outcome of the study. Women will be assigned to one of the two groups using computergenerated blocks. Results and Discussion: Data will be presented as mean value (+/- SD) while p< 0.05 will be considered significant. Mixed Analysis of Variance will be used for comparisons between and within group. There will be no significant difference in lung compliance between groups before RM (p>0.05). Two-sample t-test to compare the two groups at each time point will be used as supplementary analysis, while chi-square test for categorical variables and two-sample t-test for continuous variables for patient and procedural characteristics differences between the two groups, will be used. In the RM group, according to similar studies, the investigators are expecting to see a significant increase in lung compliance after RM compared to control group were RM was not applied. In the RM group the investigators estimate that dynamic lung compliance will be significantly higher at all time points (3 minutes, 10 and 20 minutes) compared to baseline compliance or compliance before RM too. In the control group there should be no significant difference in dynamic lung compliance at the different time points. There should be no significant demographic differences between groups while the investigators estimate that there will be no statistical or/and clinical significant differences in SpO 2, blood gas, end-tidal CO2, Ppeak, and women hemodynamic.
9 Introduction General anesthesia (GA) can cause changes in respiratory mechanics and lung function, which persist for days after surgery. These changes occurs immediately after induction of anesthesia but aggravated with mechanical ventilation 1-5. The reduction in lung compliance and the formation of atelectasis after the induction of GA is a significant cause of abnormalities in regional ventilation and gas exchange 4. Two different types of atelectasis, compression atelectasis and resorption atelectasis have an impact on patient s condition. The reduced activity of the diaphragm and the weight of lung or abdominal organs in the supine position promote the formation of compression atelectasis. Atelectasis formation Compression atelectasis form rapidly, whereas resorption atelectasis arise slowly and can be linked directly to small tidal volumes in combination with an FiO2 of This second kind of atelectasis appears in regions with a low ventilation/perfusion ratio (V/Q). Perfusion enables transportation of oxygen from the alveolus into the blood much faster than oxygen enters the alveolus from the upper airways. Due to oxygen s rapid diffusing capacity and the pressure difference across the membrane, gas is sucked out of the alveolus until it collapses. The pressure in the collapsed alveolus is almost zero, and re-opening of this reabsorption sticky atelectasis requires a positive pressure of cmh2o. Compression atelectasis (in which gas remains in the occluded acinar compartment) can be re-opened more easily ( loose atelectasis) with pressures between 10 and 12cmH2O. The onsets of compression atelectasis dependents on patient s position, for example during sleep or bed rest. In healthy patients, the areas of atelectasis and V/Q mismatch are reduced and minimized by physiological mechanisms (mainly changes in perfusion, Q). Co- morbidities that enhance the shunt fraction such as oedematous lungs [for example in acute respiratory distress syndrome (ARDS) or cardiac failure] have a markedly disturbed V/Q and lung function in these patients is worsened further as soon as anaesthesia is inducted 3. Atelectasis during Anesthesia Atelectasis is a major cause of impaired oxygenation during anaesthesia. The supine position alone reduces the functional residual capacity (FRC) by approximately l. The FRC falls by another l after induction of anaesthesia. Anesthetic induction results in a loss of inspiratory muscle tone and additionally, the loss of the dorsal flattening moves the diaphragm cephalad. The change in chest wall rigidity on one hand and the upwards shift of the diaphragm on the other decrease the transpulmonary pressure (the difference between alveolar and pleural pressure) and promote alveolar collapse and compression atelectasis. The formation of atelectasis occurs in up to 90% of patients, but it is observed particularly in obese patients in whom the regions of the lung that are atelectatic are increased by 10% compared to those of healthy patients, and can lead to clinical difficulty. Compression atelectasis can develop with spontaneous ventilation, resulting in a high shunt fraction independent of the mode of GA (intravenous or inhalational agent). The secondary reduced oxygenation due to formation of atelectasis under GA does not lead to intraoperative or postoperative morbidity in most patients, who will be extubated immediately at the end of surgery. Also mechanisms such as coughing or sneezing reopen their atelectasis. Nevertheless, some atelectasis is still present in healthy patients for 24 h after surgery, despite the area affected and, therefore, the clinical relevance may be small. However, these poorly aerated areas may become a site of infection 6. In obese patients, 7.6% of the lung volume remains atelectatic after extubation, and this increases to 9.7% over the first 24 h after surgery. In these patients, the use of long-acting neuromuscular blocking agents should be avoided as they have been found to be a risk factor in developing hypoxemia and muscle weakness in the recovery room due to their inhibition of diaphragmatic muscle recovery after anaesthesia 7. Our healthy population pregnant women mimics obese patients. Ventilation Induced Lung Injury There is probably a strong link between ventilation induced lung injury (VILI) and the repetitive 9
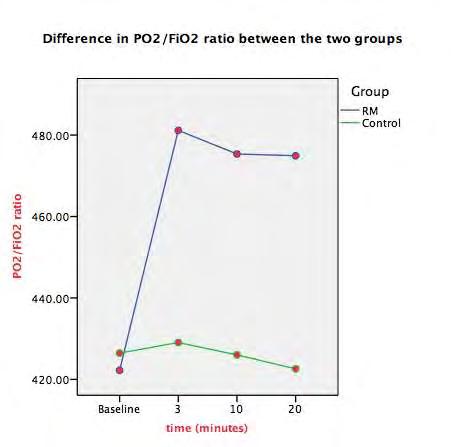
10 shear stress applied to the lung parenchyma, the repetitive opening and closing of the atelectatic lung areas which finally destroys the lung tissue 1,4. Alveolar Recruitment Maneuver (RM) and positive end-expiratory pressure (PEEP) could ameliorate these atelectatic lung areas and improve lung mechanics and oxygenation 3,4,8,9. Repetitive recruitment and de-recruitment of collapsed lung units disrupt endothelial and epithelial cells, leading to increased permeability of the alveolo-capillary membrane and increased production of IL-b, IL-6, IL-8, and other inflammatory cytokines. Even short- term mechanical ventilation may act as a proinflammatory stimulus in non-injured lungs, and is dependent on the ventilator settings used 1. Cesarean Section and General Anesthesia Although cesarean section is usually performed under regional anesthesia, GA is always a possibility mainly in emergency situations. Pregnant women have healthy lungs but, on the other hand, pregnancy induces pathophysiological changes, which in combination with the induction of GA make these women prone to perioperative pulmonary complications. During pregnancy there is an increase in intraabdominal pressure, which causes cranial shift of the diaphragm and a reduction in FRC. The above changes become more pronounced in the supine position and predispose pregnant women to airway closure mainly in the dependent lung regions. Mechanical ventilation strategies, which could improve lung compliance and oxygenation in pregnant women, have never been investigated. In previous studies RM in combination with PEEP improved oxygenation and lung compliance after induction of anesthesia in healthy weight and obese patients The feasibility of the above ventilation strategy has been tested in laparoscopic and in major abdominal surgery too 2,17,18. The above concept resembles the lung-protective ventilation strategy (low tidal volumes, PEEP and RM), which is considered the best practice in critical care patients and which reduce mortality among patients with acute respiratory distress syndrome 19. Total compliance (CT) is the relationship between changes in pressure (dp) and changes in volume (dv) of the lungs and thorax, as expressed by the equation: CT (ml/cm H2O) = dv/ dp, where CT is a function of lung compliance (CL) and chest wall compliance (CCW): CT = 1/ (1/CL+1/CCW). In clinical practice, only CT is measured dynamically or statically, depending on whether a peak or plateau inspiratory dp is used for the CT calculation. During a positive pressure inspiration, transthoracic pressure increases to a peak value and then decreases to a lower plateau value. Transthoracic pressure decreases to a plateau value after the peak value because over time, gas is redistributed from stiff alveoli into more compliant alveoli. Less pressure is required to contain the same amount of gas, which explains why the pressure decreases. Dynamic compliance (Com dyn) is the volume change divided by the peak inspiratory transthoracic pressure, and static compliance is the volume change divided by the plateau inspiratory transthoracic pressure. Therefore, static CT tends to be slightly greater than dynamic CT, although the measurements are quite similar in patients without pulmonary diseases. Study objectives Overall, we will test the hypothesis that the application of RM after delivery (during cesarean section) and then the maintenance of low tidal volume and PEEP throughout the operation, improves lung Com dyn and perioperative oxygenation. The aim of the study is to prove that the above anesthetic technique is effective in preventing lung atelectasis, which is a major cause of abnormalities in lung mechanics, lung ventilation and gas exchange in women under cesarean section. For safety reasons a preliminary data analysis has already been performed, before the beginning of the study. At all time points after intervention there is a significant difference in Comdyn between the two groups (p<0.001) while Ppeak was significantly lower in the RM group too (p=0.021). PO2/FiO2 and PO2 were also significantly higher in the RM group vs the control group (p<0.001). For more details see the preliminary data results section too. 10
11 Investigational Plan Study Population and control group This will be a prospective randomized double-blind clinical trial. After approval of the Institution Ethics Committee (General Hospital of Pyrgos Scientific and Ethic Committee), this trial will conducted at Pyrgos General Hospital between April 2015 and September After having written informed consent for the participation to the study and in order to obtain GA, ninety pregnant women (the number originates from the power analysis - see below) with Anesthesiologists Physical status Classification scores (ASA) 1-2 will be scheduled for cesarean section. The control group will be managed with the usual anesthetic technique as mentioned before (no recruitment maneuver, no PEEP, usual tidal volumes). This is a no treatment concurrent control trial. Inclusion criteria Pregnant women > 18 years old with BMI < 40 will be eligible for the study. They should accept to have GA instead of regional anesthesia. Women with >130 beats/minute and concomitant pulmonary or/and cardiac pathologies will be excluded from the study (see next section too). Exclusion criteria Exclusion criteria will be age<18 years old, patient refusal, body mass index (BMI) more than 40 kg/m 2, active asthma (requiring bronchodilator therapy), pulmonary hypertension, severe pulmonary disease, intracranial hypertension, low arterial blood pressure (hemodynamically unstable patient), heart rate >130 beats/minute, cardiac dysfunction (left ventricular ejection fraction <40%) and emergency surgery. Removal of Patients from therapy The major cause for removing patients from therapy will be the serious hemodynamic instability and mainly persistent hypotension (mean arterial blood pressure < 50 mmhg). The majority of our population is a healthy population and the hemodynamic impact of the RM is not suspected to be serious. However possible underlying co-morbidities could amplify a minor to median drop in blood pressure during the RM 3,20,21. Of course except of the RM, other reason could have a serious hemodynamic impact in pregnant women during cesarean section (inferior vena cava syndrome, blood loose etc.). Tachycardia or bradycardia could be other possible reasons for patient s removal. In many cases pregnant women suffers from tachycardia, which is due to the increased stress. We will decided to remove patients from therapy only if tachycardia (>120 beats/minute) persists after delivery. In pregnant women bradycardia (<50 beats/minute) is extremely seldom. A possible asthma attack during the operation, and after induction of anesthesia, would be another reason for removing patients from therapy.
12 Randomization Randomization will be performed using computer-generated blocks (available at: and each pregnant woman assigned to participate in the study will have a sequentially numbered sealed envelope (from 1 to 90) containing a randomization code (A or B). Only the main investigator (DA) will be responsible to wit what A or B means (for example A=RM and B= control). Patients will be randomized to one of two ventilator management groups (RM, control) with 45 patients per group. The envelopes will be concealed until after consent will be obtained. All cesarean sections will be performed by the same team of surgeons and by the same anesthesiologists (DA, AM). In appendix 1 there is an example of manually performed permuted blocks randomization with 90 patients, which could also be used. Treatments Anesthetic technique (prior and post-manipulation therapy) The anesthetic technique will be the same for both groups of patients and is standardized as follows: Anesthesia will be induced with propofol (1.5-2 mg/kg), fentanyl (1 μg/kg) and rocuronium (1.5 mg/kg) and will be maintained with sevoflurane (minimal alveolar concentration ) and fentanyl ( μg). The minimum alveolar concentration of sevoflurane will be titrated from the attending anesthesiologist according to the arterial blood pressure (± mmhg baseline) and beats per minute (± baseline). Rocuronium for muscle paralysis will be used once, during induction of anesthesia to facilitate tracheal intubation (cuffed tube no Portex, Inc., London) and without subsequent bolus doses, while at the end of the operation sugammadex (200 mg) will be used for neuromuscular block reversal. Intraoperatively ondasentron 4 mg, omeprazole 40 mg, paracetamol 1000 mg and Parecoxib 40 mg will be used to all the patients. The time between the end of preoxygenation and tracheal intubation must be standard (40-60 seconds) and will be recorded for all the patients. The Perioperative use of crystalloids and colloids, blood products and vasopressors will be recorded while fluid management will be left to the discretion of the attending anesthesiologist (Ringers Lactated). Hypotension (mean arterial pressure <60 mmhg) will be treated with ephedrine bolus 5 mg i.v and if insists bolus doses of hydroxyethylstarch (HES 130/0.4, Voluven; Fresenious Kabi, Germany) up to 1000 ml will be given. The standard monitors of the American Society of Anesthesiologists will be used while the radial artery will be cannulated for invasive blood pressure monitoring and blood gas measurements. Ventilatory Management (time and method of RM) Before induction of anesthesia preoxygenation (100% oxygen via face mask) for 2 minutes will be conducted to all the patients. After tracheal intubation, pregnant women in both groups will be mechanically ventilated (Datex-Ohmeda, Aestiva/5, Madison, WI, USA) with volume-controlled mode and with tidal volume at 8-ml/kg ideal body weights. Inspiratory to expiratory time ratio will be set to 1:2 while 40% oxygen fraction (balanced with air) will be used. The respiratory rate will be adjusted to maintain an end-tidal CO 2 between mmhg and zero end-expiratory pressure will be applied (ZEEP). Immediately after delivery the control group of women will continue with exactly the same ventilator management while in the RM group lung recruitment will be achieved as follows: 12
13 The ventilator will be switched to pressure-controlled mode and the inspiratory time will be increased to 50% (inspiratory /expiratory ratio will be set to 1:1). The Peak inspiratory pressure (P peak) will firstly be set to 20 cmh 2O (for 3 breaths) and then the investigators progressively will increase the positive end-expiratory pressure (PEEP) to have a P peak up to cmh 2O. The PEEP sequential will increase in four steps from 0 to 5 cmh 2O (for 3 breaths), from 5 to 10 cmh 2O (for 5 breaths), from 10 to 15 cmh 2O (for 7 breaths) and from 15 to 20 cmh 2O (for 10 breaths). The whole RM will last about 2 minutes. After the RM the investigators will use volume control ventilation again with the baseline settings mentioned above, tidal volume 6ml/kg and PEEP step-wise decrease to 8 cmh 2O, which must be maintained until the end of the operation. Lung recruitment in the RM group will not be repeated, as cesarean section is a short lasting operation. After completion of the operation and neuromuscular block reversal women in both groups will breath spontaneously before tracheal extubation and PEEP will be eliminated in the RM group. Also see flowchart below: 13
14 RM Group Study Design Ventilatory Management Flowchart Baseline (usual ventilation management ) RM Measurements PEEP and low tidal volume Measurement s Measurements stop mechanical ventilation Postoperative measurements Control Group Baseline (usual ventilation management ) No RM Measurements Measurement s Measurements stop mechanical ventilation Postoperative measurements Blinding procedure This will be a double blind clinical study. The patients will not know the kind of the mechanical ventilation that they will receive. The only person who will be un-blind will be the primary investigator (DA). After the RM (or not), a second anesthesiologist (AM) will come into the operating room and records the monitor measurements. The same person will also receive blood for blood gas analysis according to the specified time points. Every different patient is just a number (1,6,3 9, 43, 78. etc.) for the investigator. The measurements will be recorded in special files for each separate patient (see appendix 3,4,5, and 6) and then in a SPSS data file (SPSS version 22) and will be analyzed by two different persons (the primary investigator who can find the treatment of each patient and a second statistician who is blind). The results should be matched. Of course for this kind of study a single blind procedure (only for the investigator who record the measurements) would be enough, as the placebo effect does not exist in anesthetized patients. We decided to conduct a double blind study just for the postoperative period records. Measurements Primary end-point The improvement of Com dyn will be the primary end-point of the study. In the RM group Com dyn will be recorded both before (baseline) and after the RM and the application of PEEP (3 minutes) and then at 10 and 20 minutes, while it will also be measured at the same time points in the control group of women. Com dyn (ml/cmh2o) will be measured automatically by the monitor spirometry (Datex- Ohmeda Capnomac Ultima, P&V spirometry) according to the following formula: dv/dp where maximum tidal volume will be used for dv and the difference Ppeak-PEEP will be used for dp. Secondary measurements Ppeak is the maximum end-inspiratory airway pressure and will be measured too. The same monitor will be also used to measure the following parameters: ETCO2, alveolar minute ventilation (tidal
15 volume multiplied by ventilatory frequency) and expiratory tidal volume. In both groups of patients Com dyn will be measured after delivery, but before RM (baseline measurement), and then 3, 10 and 20 minutes after the RM. At the same time points arterial blood pressure (systolic, diastolic and mean), heart rate, SpO2, blood gas, ETCO2, Ppeak, expiratory tidal volume and minute volume will be measured too. SpO2 and blood gas will be also measured postoperatively (10 minutes after extubation). Tables 2 and 3 present the basic patient s measurements. Data analysis example comes from preliminary data analysis before the beginning of the study. Follow up measurements Patients will be followed up for postoperative respiratory failure, which is defined as the need for non-invasive ventilation and/or mechanical ventilation after extubation. In cases of respiratory failure, the possible pulmonary complications are also being defined: pneumonia, atelectasis, pulmonary embolism, pneumothorax, acute lung injury (ALI), asthma, non-cardiogenic pulmonary oedema and severe hypercapnia. The routine postoperative oxygen use will also be noted and will be applied for half an hour postoperatively. Statistical analysis Before the beginning of the study, and for determination of sample size, we will conduct power analysis, in an attempt to estimate the sample size required so that the study would have adequate power to detect clinically meaningful differences between the two study groups with regards to lung compliance (dv/dp), which is the primary outcome of the study. For this analysis, we used the G*Power Software that is freely available online at from the Psychology Department of the University of Dusseldorf, in Germany. Our power analysis is based on previous studies but is even more generous 17,22. The required sample size calculation was based on the following assumptions: Clinically meaningful difference between the two groups is 20% of the mean value, and SD of the observed lung compliance is 25% of the mean value (rather generous), therefore size effect d= 20% /25% = 0.8, with two-sided testing, with alpha = 0.05 and b = 0.1 (therefore, power = 1-b = 0.9). Under these assumptions, G*Power indicated that we will need minimum 34 patients per group for this study to have adequate power. To confirm accuracy of this calculation, we will also conduct sample size estimation using the Statistica v 7.0 Statistical Software package (StatSoft Inc, Tulsa, Oklahome, USA), in order to find out if this confirmatory analysis will produce identical results. Finally we will confirm our results using the suitable mathematic formula (see appendix 2). In order to allow for possible protocol violations, errors, patient attrition or other study shortcomings, we will enroll 45 patients in each arm of the study (about 10 women more in each group of patients). As pregnant women are a very sensitive population and we are afraid of much protocol violation (removal women from protocol mainly due to hemodynamic instability) we will chose to randomize 45 women per group, which is a generous number. We will check if data are normally distributed (Kolmogorov Smirnoff and Shapiro Wilks test). Ventilatory and haemodynamic data and intraoperative and postoperative variables (all continuous variables) will be presented as mean values (+/- SD). Data will be compared between and within groups using Mixed Analysis of Variance (Mixed Anova-General Linear Model) if are normally distributed or with Kruskal Wallis test in case that we do not have normally distributed data. 15
16 Bonferoni correction will be used for multiple comparisons correction. In order to check and supplement our Mixed Analysis of Variance we will also use two-sample t-test to compare the two groups at each time point (for ventilatory and haemodynamic variables). Patient and procedural characteristics will be compared between groups using chi-square test for categorical variables and independent-sample t-test for continuous variables. Two tailed P-values <0.05 will be considered statistically significant. For data analysis SPSS statistical software version 22 will be used. Patients Records For each patient we will have four data files: 1. Demographic intra- and post-operative patient data (appendix 3) 2. Mechanical ventilation data (appendix 4) 3. Haemodynamic data (appendix 5) 4. Blood gas data (appendix 6) Data Presentation Plan Number of eligible women and number of women excluded before randomization (lets say ): Possible reasons for exclusion: 1 women could decline participation and choose regional anesthesia, 2 could have emergency surgery, 3 will have active asthma, 4 will have BMI >40, 4 will be < 18 years old, 5 will suffer arterial hypertension etc. If we add: i= Finally we will include 45 patients in each group. Number of women that will complete the study = F (For example 40 women in the RM group and 41 women in the Control group) Give reasons for not complete the study: Heart rate >110bpm, Low arterial blood pressure, hypertension, asthmatic attack during the surgical procedure etc. 16
17 Flow chart: Number of Eligible women (pts screened) Number of women excluded () 1=reason, 2=reason, 3=reason, etc Women Randomized (n=90) 45 in the RM Group Finally completed the study :40 women Give reasons for not complete the study for 5 women 45 in the Control Group Finally completed the study : 41 women Give reasons for not complete the study for 4 women If all, or almost all of the patients will complete the study (we will have the most of the measurements in each time point) we will use a per protocol analysis. If we have many missing data we will use an intention to treat analysis of data (ITT). According to ITT analysis of data I will use all the data of all the randomized patients regardless of whether they completed the trial or not. For the missing values I will use the last observation carried forward (LOCF) approach Patient characteristics should be similar between the two groups (table 1). If not we will have to mention the differences and this would be a serious limitation of our study. Intraoperative characteristics (time to delivery, anesthesia duration, estimated blood lose, administration of crystalloids and/or colloids, administration of blood products and intraoperative use of ephedrine should be similar between the two groups (table 1). The length of hospital stay and the possible differences between the two groups should be mentioned (table 1). The number of patients that will suffer postoperative pulmonary complications (mainly pneumonia, diagnosed with chest radiogram and clinical evaluation) and possible differences between the two groups should also be mentioned. Pneumothorax would be a serious adverse event, which could have a strong relationship with the RM manipulation of the patients and should be recorded. See adverse event section below.
18 Table 1: Patient characteristics presented as mean (SD) or n=number of patients. Intra- and postoperative characteristics presented as mean (SD). Patient Characteristics Age (yrs.) [mean (SD)] BMI (kg/m 2 ) [mean (SD)] Smoking status (n) Intraoperative Characteristics Duration of anesthesia (min) Time to delivery (min) Crystalloids (ml) Colloids (ml) Blood (units)* Ephedrine dose (mg) Postoperative Characteristics Length of hospital stay (days) Pulmonary complications (n) Pneumothorax (n) Pneumonia (n) Other (n) RM Group n=45 A1 A2 A3 A4 A5 A6 A7 A8 A9 A10 A11 A12 A13 A14 Control Group n=45 B1 B2 B3 B4 B5 B6 B7 B8 B9 B10 B11 B12 B13 B14 Efficacy and Safety issues: The efficacy of the RM to improve lung compliance and gas exchange will be the main efficacy issues of the study. The investigators believe that the Com dyn (dv/dp) will be statistical significantly improved in the RM group compared to the control group (statistical significant difference between groups). A 20% increase in mean Com dyn in the RM group compared to the control group would be clinically significant. This change in lung compliance perhaps would not have any significant impact for the majority of the patients of our study (young and healthy patients). However, underlying comorbidities may amplify changes in lung and cardiovascular physiology and anaesthesia may serve as a second-hit that worsens patient outcome. For this reason a RM and the application of protective lung ventilation (low tidal volumes and PEEP) perhaps should be the suitable anesthetic practice for all the patients. The investigators also believe that there would be statistical significant difference within groups too. In the RM group possibly there would be a difference in lung compliance (increase) between baseline and all the other time points (3, 10 and 20 minutes after the RM). Again a 20% increase in Com dyn would be clinically significant, at least for some patients. The investigators believe that the recruitment manoeuvre will improve the intraoperative and/or postoperative PO 2, the PO 2/FiO 2 and the SpO 2. Again for the population of our study (all women have a baseline PO 2/FiO 2>400) this improvement will not have a significant impact. All the data will be presented in tables 2 and 3 (see next example with preliminary data analysis). Because of the higher inspiratory pressures during RM and PEEP used, the P plateau and P peak are anticipated to be significantly higher in the RM group, compared with those in the control group, and this would be a possible serious safety issue, as high alveolar pressures could result in pneumothorax or/and barotrauma. As the study involves young and healthy population, the investigators believe that the above safety issues will not be a serious problem of the study. A second safety issue will be the hemodynamic instability during RM. Patients with serious hemodynamic instability will be removed from the study, as already mentioned. 18
19 End of treatment The treatment (RM) will start after delivery (3 minutes) and will last until the end of the surgery. Specifically, in the RM group the RM will be performed 3 minutes after delivery but PEEP and low tidal volume (which are part of the whole RM technique) will be continued until the end of the operation. End of Study The patients will be monitored throughout the operation and in the postoperative period too (see also the measurements section-primary end point, secondary measurements and follow up). The follow up will last for all the length of hospital stay. The length of hospital stay will be recorded while all the adverse events that will be occurred during this period they will be recorded too. For this kind of population the hospital stay is usually short (<5 days). Adverse events: Hemodynamic instability during the RM will be the most important adverse event of the study. During the RM all women should be closely monitored for the occurrence of hypotension or the administration of a fluid bolus or vasopressor medication to support haemodynamic variables. Of course during the whole course of anesthesia the need for vasopressor should be monitored. Possible differences between the two groups should be mentioned for all the above parameters (table 1). Postoperative lung complications (pneumonia, atelectasis, pulmonary embolism, pneumothorax, acute lung injury (ALI), asthma, non-cardiogenic pulmonary oedema and severe hypercapnia) should also be recorded. As we will mainly include young and healthy population serious lung complications and differences between groups are not anticipated. Preliminary Data Results For safety issues we decided to perform a preliminary data analysis before the beginning of the study. We used 7 patients in each group, and we will use these data analysis as an example of our data presentation plan and to show the most important measurements of our study. At all time points (3, 10 and 20 minutes) after intervention there is a significant difference in Com dyn between the two groups (p<0.001). The Com dyn is much higher in the RM group vs control group (table 2). The significant difference in lung Com dyn depicts in figure 1a too. Post intervention the peak inspiratory pressure at all time points (3, 10 and 20 minutes) is significantly lower in the RM group compared to control group (p=0.021, table 2, figure 1b). PO 2/F io 2 and PO 2 are also significantly higher in the RM group vs the control group (p<0.001) at all time points post intervention (3, 10 and 20 minutes) while PO 2 is also significantly higher in the RM vs control group postoperatively (p<0.001). SpO 2 is significantly difference between the two groups at 10 and 20 minutes post intervention and postoperatively (p=0.04) table 2 There are no significant differences in expiratory tidal volume, minute volume, end tidal CO 2, PCO 2 and in hemodynamic data between the two groups (tables 2, 3). 19
20 Table 2. Respiratory Mechanics and Gas Exchange in the two groups of pregnant women (recruitment vs control, respectively-example). Data are presented as mean ± SD. The P-value corresponds to the tests of between subject main effects using the mixed Anova test (recruitment vs control group). The two groups were also compared separately at each time point using the independent two-sample t- test (*) and (**). (*) denotes significant differences from the control when P<0.01 while (**) is used whenever P<0.05. PaO 2, arterial blood oxygen; PaCO 2, arterial blood CO 2; SpO 2, arterial blood oxygen saturation; FiO 2, oxygen concentration. Peak Inspiratory Pressure (cmh 2O) Baseline After intervention (minutes) 3 min 10 min 20 min Postoperative P -value Recruitment Control 23.9 (2.9) 23.0 (2.8) 19.9 (2.5)* 22.1 (2.8) 20.2 (2.9)* 22.5 (2.7) 20.3 (3.0)* 22.2 (2.7) Com dyn (ml/cmh 2O) - <0.001 Recruitment Control Pa O2 (mmhg) Recruitment Control PaO2/FiO2 Recruitment Control ET CO2 (mmhg) Recruitment Control Expiratory Tidal Volume (ml) Recruitment Control 33.6 (6.8) 31.1 (7.9) (10.6) 214 (18.4) (22.1) (43.3) 30.9 (3.4) 30.4 (2.9) (63,1) (54.2) 51.4 (12.8)* 29.6 (7.2) (26.9)* (22.6) (48.6)* 429 (39.2) 29.2 (3.4) 30.0 (3.0) 588 (65.3) 582 (66.3) 49.9 (11.2)* 30.6 (8.1) (22.0)* 214 (22.3) (42.7)* 426 (41.5) 28.4 (3.8) 29.4 (2.8) 578 (66.2) 585 (58.4) 49.7 (10.9)* 30.9 (8.1) (27.6)* 212 (38.4) 474 (50.3)* (37.5) 28.1 (3.6) 28.6 (2.7) 581 (65.1) 579 (66.3) (6.7)* 98.4 (5.3) < < (62.8) 585 (64.8) 0.5 Minute Volume (lit) Recruitment Control PCO 2 (mmhg) Recruitment Control 7.0 (7.74) 6.8 (0.63) 33.9 (2.2) 34.4 (1.9) 7.1 (0.63) 6.9(0.67) 32.7 (3.0) 33.7 (2.9) 6.9 (0.65) 6.8 (0.72) 32.7(3.8) 33.8 (2.9) 7.1 (0.68) 7.1 (0.65) 32.7 (3.7) 33.6 (3.2) 6.9 (0.65) 6.8 (0.59) 35.6 (1.9)** 36.5 (1.4)** SpO 2 Recruitment Control 98.8 (0.7) 99 (0.7) 99 (0.7) 98.9 (0.7) 99.1 (0.8)** 98.7 (0.6) 98.9 (0.8)** 98.6 (0.5) 98.3 (0.8)* 97.7 (0.7)
21 Table 3. Systolic Arterial Pressure, Diastolic Arterial Pressure, Mean Arterial Pressure and Heart rate between the two groups of pregnant women (recruitment vs control, n=40 and n=41 respectively- Example). Data are presented as mean ± SD. The P-value corresponds to the tests of between subject main effects using the mixed Anova test (recruitment vs control group). The two groups were also compared separately at each time point using the independent two-sample t-test. Baseline After Intervention (minutes) 3 min 10 min 20 min P- Value Systolic Arterial Pressure (mmhg) Recruitment Control (6.2) (9.1) (8.4) (9.5) (9.8) (10.7) (10) (10.5) 0.63 Diastolic Arterial Pressure (mmhg) Recruitment Control 73.6 (10.5) 72.7 (8.0) 70.5 (10.0) 70.6 (7.6) 70.3 (9.6) 71.1 (7.6) 69.6 (9.0) 71.1 (6.3) 0.8 Mean Arterial Pressure (mmhg) Recruitment Control 88.8 ( ( (10.1) 85.8 (7.4) 84.4 (10.3) 83.8 (7.2) 83.8 (10.3) 82.4 (7.2) 0.98 Heart Rate (beats per minute) Recruitment Control 95.1 (12.3) 96.2 (6.7) 92.5 (12.4) 91.6 (6.2) 91.6 (11.6) 91.5 (6.6) 91.4 (12.0) 91.0 (7.0)

22 Figure 1a and 1b: RM=recruitment maneuver group, Baseline=before intervention, 3, 10 and 20 minutes=post intervention time. 22

23 Figure 2: 23
24 Discussion: Lung-protective ventilation, which refers to the use of low tidal volumes PEEP, and which may also include the use of RM, has been shown to reduce mortality among patients with the acute respiratory distress syndrome and is now considered best practice caring of many critically ill patients 2,9,15,19,23,24. Over the last years many physicians have questioned the benefits of using lung-protective ventilation in the surgical setting, and in many surgical procedures the results are very positive 2,9,15-18,22, Previous studies In a recent multicenter, double-blind, parallel-group trial with 400 patients the investigator concluded that as compared with a practice of nonprotective mechanical ventilation, the use of a lung-protective ventilation strategy in intermediate-risk and high-risk patients undergoing major abdominal surgery was associated with improved clinical outcomes and reduced health care utilization 2. In this trial the primary outcome was a composite of major pulmonary and extrapulmonary complications occurring within the first 7 days after surgery. In a systematic review published in 2014 the investigators developed the benefits of lung protective ventilation during surgery and general anesthesia and offers some recommendations (Lung-protective ventilation, which refers to the use of lower tidal volume and limited Pplateau to minimize overdistension, and PEEP to prevent alveolar collapse at end-expiration) for mechanical ventilation in the surgical context 9. In another systematic review and meta-analysis which published in 2012 the investigators concluded that although the ideal intraoperative ventilation strategy in obese patients remains obscure there is some evidence that RM added to PEEP compared with PEEP alone improves intraoperative oxygenation and compliance without adverse effects. There was no evidence of any difference between PCV and VCV 16. In three other prospective clinical trials the RM proved very effective in restoration of lung compliance and lung mechanics in laparoscopic surgery 15,17,18 while one more study in normal weight and obese patients undergoing laparoscopic surgery had the same beneficial results 22. One more study published in 2012 showed ventilation improvement during thoracic surgery 30 while RM strategy improved arterial oxygenation after cardiopulmonary bypass too 25. In 2010 Tusman et al. insisted that the application of RMs during anaesthesia normalizes lung function along the intraoperative period and that there is physiological evidence that patients of all ages and any kind of surgery benefit from such an active intervention 29. Atelectasis is the main cause of postoperative pulmonary complication while the danger is mainly noted in high-risk patients 1,3. Pregnant women are considered healthy women and low risk for GA, but on the other hand mimic they obese patients. This will be the first study, where it will be perform RM in this special population. Limitations of the study In our study we will check for differences in Com dyn but not in the static compliance, which is also a very important record of the pulmonary performance. The reason is the lack of the special instruments. Many other records could be performed for respiratory mechanics too. As we will use both RM and PEEP we will not be able to know if the compliance increasement (if exist) will be due to RM or to PEEP. While this study will probably demonstrate a restoration in pulmonary compliance and in oxygenation, it will not be powered to describe pulmonary outcomes, such as postoperative atelectasis or pneumonia. 24
25 Appendix 1 Clinical Trial Methodology, Elias Zintzaras Permuted blocks: We consider a block of 10 patients and two treatments RM and Control. Then we define an array of 10 numbers, from 1 to 10: A permutation of the array may produce the following blocks: Block 1: Block 2: Block 9: We need 9 blocks (90 patients) We assign digits 1-5 to A Digits 6-10 to B Block Sequence Treatment Patients 3 A 1 5 A 2 1 A 3 4 A 4 Block 1 9 B 5 8 B 6 10 B 7 2 A 8 6 B 9 7 B 10 1 A 11 6 B 12 8 B 13 9 B 14 Block 2 10 B 15 2 A 16 4 A 17 5 A 18 7 B 19 3 A 20 3 A 21 1 A 22 7 B 23 9 B 24 Block 3 2 A 25 4 A B 27 8 B 28 5 A 29 6 B 30 25
26 Block 4 Block 5 Block 6 Block 7 Block 8 Block 9 9 B 31 3 A 32 2 A B 34 7 B 35 1 A 36 4 A 37 8 B 38 5 A 39 6 B 40 5 A 41 1 A 42 9 B 43 7 B 44 2 A B 46 3 A 47 4 A 48 6 B 49 8 B 50 9 B 51 1 A 52 3 A 53 7 B 54 2 A 55 4 A 56 5 A 57 8 B B 59 6 B B 61 5 A 62 1 A 63 8 B 64 3 A 65 2 A 66 9 B 67 4 A 68 6 B 69 7 B 70 3 A 71 8 B B 73 1 A 74 9 B 75 2 A 76 7 B 77 6 B 78 4 A 79 5 A 80 7 B 81 1 A 82 4 A 83 8 B 84 3 A B 86 2 A 87 5 A 88 26
27 Διπλωματική Εργασία Diamanto Aretha 9 6 B B Appendix 2 We will use power analysis Two independent groups (comparison of means)-clinical Trial Methodology, Elias Zintzaras Sample size in two independent groups. The formula for calculating the sample size is: n S = SD (from previous trials it was found that the between subject variance of compliance is 25) Δ =20 (difference in compliance that is considered clinically significant) Consequently, *n n 33 patients on each group * If we include +10% to compensate for potential loss then the final sample size should be at least 37 patients on each group Appendix 3 - Demographic intra- and post-operative patient s data Patient ID: Age (years) BMI (kg/m2) Smoking status (n) Duration of anesthesia (min) Time to delivery (min) Crystalloids (ml) Colloids (ml) Blood (units) Ephedrine dose (mg) Length of hospital stay (days) Pulmonary complications (n) Appendix 4 - Mechanical ventilation patient s data Patient ID: Minute volume (ml) Tidal volume (ml) Compliance (dyn) P (peak) End tidal CO2 Baseline 3 minutes 10 minutes 20 minutes Postoperative 27
28 Appendix 5 - Haemodynamic patient s data Patient ID: Baseline 3 minutes 10 minutes 20 minutes Postoperative SBP (mmhg) DBP (mmhg) MAP (mmhg) BPM Appendix 6 Patient s Blood gas data Patient ID: Baseline 3 minutes 10 minutes 20 minutes Postoperative PO 2 (mmhg) PCO 2 (mmhg) PH SpO 2 (%) PO 2/FiO 2 References 1. Tusman G, Bohm SH, Warner DO, Sprung J. Atelectasis and perioperative pulmonary complications in high-risk patients. Curr Opin Anaesthesiol 2012;25: Futier E, Constantin JM, Paugam-Burtz C, et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med 2013;369: Bruells CS, Rossaint R. Physiology of gas exchange during anaesthesia. Eur J Anaesthesiol 2011;28: Duggan M, Kavanagh BP. Pulmonary atelectasis: a pathogenic perioperative entity. Anesthesiology 2005;102: Hedenstierna G, Edmark L. The effects of anesthesia and muscle paralysis on the respiratory system. Intensive Care Med 2005;31: van Kaam AH LR, Herting E, et al. Reducing atelectasis attenuates bacterial growth and translocation in experimental pneumonia. Am J Respir Crit Care Med 2004;169: Bissinger U SF, Lenz G. Postoperative residual paralysis and respiratory status: a comparative study of pancuronium and vecuronium. Physiol Res 2000;49: Hemmes SN, Serpa Neto A, Schultz MJ. Intraoperative ventilatory strategies to prevent postoperative pulmonary complications: a meta-analysis. Curr Opin Anaesthesiol 2013;26: Futier E, Constantin JM, Jaber S. Protective lung ventilation in operating room: a systematic review. Minerva Anestesiol 2014;80: Pelosi P, Gregoretti C. Perioperative management of obese patients. Best Pract Res Clin Anaesthesiol 2010;24: Pelosi P, Ravagnan I, Giurati G, et al. Positive end-expiratory pressure improves respiratory function in obese but not in normal subjects during anesthesia and paralysis. Anesthesiology 1999;91: Reinius H, Jonsson L, Gustafsson S, et al. Prevention of atelectasis in morbidly obese patients during general anesthesia and paralysis: a computerized tomography study. Anesthesiology 2009;111: Severgnini P, Selmo G, Lanza C, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology 2013;118: Tusman G, Bohm SH, Vazquez de Anda GF, do Campo JL, Lachmann B. 'Alveolar recruitment strategy' improves arterial oxygenation during general anaesthesia. Br J Anaesth 1999;82:
Effect of peak inspiratory pressure on the development. of postoperative pulmonary complications.
 Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Anaesthetic considerations for laparoscopic surgery in canines
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Supplementary Online Content
 1 Supplementary Online Content Leme AC, Hajjar LA, Volpe MS, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications:
1 Supplementary Online Content Leme AC, Hajjar LA, Volpe MS, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications:
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Sub-Study. PRotective Ventilation with Higher versus Lower PEEP during General Anesthesia for Surgery in OBESE Patients
 PRotective Ventilation with Higher versus Lower PEEP during General Anesthesia for Surgery in OBESE Patients The PROBESE Randomized Controlled Trial Preliminary evaluation of postural reduction of peripheral
PRotective Ventilation with Higher versus Lower PEEP during General Anesthesia for Surgery in OBESE Patients The PROBESE Randomized Controlled Trial Preliminary evaluation of postural reduction of peripheral
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Original Article Effects of prone position on lung function of patients undergoing mechanical ventilation under total intravenous anesthesia
 Int J Clin Exp Med 2017;10(4):6769-6774 www.ijcem.com /ISSN:1940-5901/IJCEM0045140 Original Article Effects of prone position on lung function of patients undergoing mechanical ventilation under total
Int J Clin Exp Med 2017;10(4):6769-6774 www.ijcem.com /ISSN:1940-5901/IJCEM0045140 Original Article Effects of prone position on lung function of patients undergoing mechanical ventilation under total
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Effects of pressure controlled and volume controlled ventilation on respiratory mechanics and systemic stress response during prone position
 DOI 10.1186/s40064-016-3435-3 RESEARCH Open Access Effects of pressure controlled and volume controlled ventilation on respiratory mechanics and systemic stress response during prone position Oznur Sen
DOI 10.1186/s40064-016-3435-3 RESEARCH Open Access Effects of pressure controlled and volume controlled ventilation on respiratory mechanics and systemic stress response during prone position Oznur Sen
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
THE EFFECT OF POSITIVE PRESSURE VENTILATORY PATTERNS ON POST-BYPASS LUNG FUNCTIONS
 THE EFFECT OF POSITIVE PRESSURE VENTILATORY PATTERNS ON POST-BYPASS LUNG FUNCTIONS MOHAMED ESSAM A-MEGUID *, EMAD EL-DIN MANSOUR * AND KHALED M. ABDULLAH ** Abstract Background: This study aimed at evaluating
THE EFFECT OF POSITIVE PRESSURE VENTILATORY PATTERNS ON POST-BYPASS LUNG FUNCTIONS MOHAMED ESSAM A-MEGUID *, EMAD EL-DIN MANSOUR * AND KHALED M. ABDULLAH ** Abstract Background: This study aimed at evaluating
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Mechanical Ventilation Strategies in Anesthesia
 Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Does the Use of Positive End Expiratory Pressure (PEEP) During Surgery Decrease Respiratory Complications Twenty-Four Hours Post Operative?
 During Surgery Decrease Respiratory Complications Twenty-Four Hours Post Operative?") Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 2016 Does the Use
Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 2016 Does the Use
British Journal of Anaesthesia 104 (5): (2010) doi: /bja/aeq080 Advance Access publication March 30, 2010
: (2010) doi: /bja/aeq080 Advance Access publication March 30, 2010") RESPIRATION AND THE AIRWAY Lung recruitment and positive airway pressure before extubation does not improve oxygenation in the post-anaesthesia care unit: a randomized clinical trial A. B. Lumb 1, S. J.
RESPIRATION AND THE AIRWAY Lung recruitment and positive airway pressure before extubation does not improve oxygenation in the post-anaesthesia care unit: a randomized clinical trial A. B. Lumb 1, S. J.
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Trial protocol - NIVAS Study
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 Trial protocol - NIVAS Study METHODS Study oversight The Non-Invasive Ventilation after Abdominal Surgery
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION
 SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
SECTION 1: INCLUSION, EXCLUSION & RANDOMISATION INFORMATION DEMOGRAPHIC INFORMATION Given name Family name Date of birth Consent date Gender Female Male Date of surgery INCLUSION & EXCLUSION CRITERIA YES
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Alveolar Recruitment Maneuvers and Noninvasive Positive Pressure Ventilation in Obese Patients: A Quality Improvement Project
 The University of Southern Mississippi The Aquila Digital Community Doctoral Projects Fall 10-1-2018 Alveolar Recruitment Maneuvers and Noninvasive Positive Pressure Ventilation in Obese Patients: A Quality
The University of Southern Mississippi The Aquila Digital Community Doctoral Projects Fall 10-1-2018 Alveolar Recruitment Maneuvers and Noninvasive Positive Pressure Ventilation in Obese Patients: A Quality
Exclusion Criteria 1. Operator or supervisor feels specific intra- procedural laryngoscopy device will be required.
 FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
1. What is delayed sequence intubation? Can it be used for severe Asthma exacerbation? 2. What about pregnancy and Asthma is so important?
 Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Chapter 073 Asthma Episode Overview 1. 10 different causes of a wheeze. 2. List 8 risk factors for death from asthma 3. List 6 objective findings of severe asthma 4. 10 therapies for an acute severe asthma
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Respiratory Complications of Obesity. Diana Wilson, M.D. ACP Educational Session September 16, 2017
 Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Preoperative Pulmonary Evaluation. Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine
 Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1).
.") PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
PATIENT CHARACTERISTICS AND PREOPERATIVE DATA (ecrf 1). 1 Inform Consent Date: / / dd / Mmm / yyyy 2 Patient identifier: Please enter the 6 digit Patient identification number from your site patient log
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Evaluation of Low Tidal Volume During General Anesthesia in Prone Position on Respiratory Functions
 Journal of Anesthesiology 2018; 6(1): 26-32 http://www.sciencepublishinggroup.com/j/ja doi: 10.11648/j.ja.20180601.15 ISSN: 2376-7766(Print); ISSN: 2376-7774(Online) Evaluation of Low Tidal Volume During
Journal of Anesthesiology 2018; 6(1): 26-32 http://www.sciencepublishinggroup.com/j/ja doi: 10.11648/j.ja.20180601.15 ISSN: 2376-7766(Print); ISSN: 2376-7774(Online) Evaluation of Low Tidal Volume During
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
LAS VEGAS Case Report Form 1 Intra-Operative
 LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
LAS VEGAS Case Report Form 1 Intra-Operative Patient Informed Consent 1. Informed consent applicable: yes no (choose no if waived by local EC) 1.1 If applicable; was consent obtained? yes no 1.2 If yes,
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
A Comparative Study for the Lung Mechanics during One-Lung Ventilation in Thoracic Surgeries Using Two Different Modes of Mechanical Ventilation
 Med. J. Cairo Univ., Vol. 85, No. 3, June: 967-972, 2017 www.medicaljournalofcairouniversity.net A Comparative Study for the Lung Mechanics during One-Lung Ventilation in Thoracic Surgeries Using Two Different
Med. J. Cairo Univ., Vol. 85, No. 3, June: 967-972, 2017 www.medicaljournalofcairouniversity.net A Comparative Study for the Lung Mechanics during One-Lung Ventilation in Thoracic Surgeries Using Two Different
Assessing perioperative risk
 Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Cricoid pressure: useful or dangerous?
 Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
Cricoid pressure: useful or dangerous? Francis VEYCKEMANS Cliniques Universitaires Saint Luc Bruxelles (2009) Controversial issue - Can J Anaesth 1997 JR Brimacombe - Pediatr Anesth 2002 JG Brock-Utne
EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode!
 EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode! Antony Carrier-Boucher! PGY 3 Anesthesiology! Laval University! None! Conflict of interest! 2. Anesth Analg
EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode! Antony Carrier-Boucher! PGY 3 Anesthesiology! Laval University! None! Conflict of interest! 2. Anesth Analg
A simple case of.. Acute severe asthma. MasterclassIC Schiermonnikoog 2017
 A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
A simple case of.. Acute severe asthma MasterclassIC Schiermonnikoog 2017 Case (1) Female, 27 - G1P0 (26 weeks) PMH - several admissions for severe acute asthma (no MV) Progressive dyspnea for 1 week Admitted
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Perioperative Lung Protective Ventilatory Management During Major Abdominal Surgery: a Hungarian Nationwide Survey
 Online ahead-of-print. Page numbers NOT for citation purposes. RESEARCH ARTICLE Perioperative Lung Protective Ventilatory Management During Major Abdominal Surgery: a Hungarian Nationwide Survey Zoltán
Online ahead-of-print. Page numbers NOT for citation purposes. RESEARCH ARTICLE Perioperative Lung Protective Ventilatory Management During Major Abdominal Surgery: a Hungarian Nationwide Survey Zoltán
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT
, RPSGT") BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
JMSCR Vol 04 Issue 01 Page January 2016
 www.jmscr.igmpublication.org Impact Factor 3.79 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i1.04 Haemodynamic Effects during Induction in
www.jmscr.igmpublication.org Impact Factor 3.79 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i1.04 Haemodynamic Effects during Induction in