Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
|
|
|
- Samson Daniels
- 6 years ago
- Views:
Transcription

1 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1
2 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes Rapidly improving strokes Aneurysm Tumor Mimics 3 to 4.5 hour criteria 2
3 Objective Give More tpa!! 3
4 Case 1 67M with PMH of HTN arrived with EMS at 1502 with NIHSS 4 (1 aphasia, 2 right arm, 1 mouth droop) LSW per spouse Direct to CT scan (negative for ICH), glucose 104, BP 147/ NIHSS at 2 after improvement in speech and arm strength Decision made to NOT give tpa 1650 Admitted to inpatient unit with an NIHSS of 2 4
5 Stroke Across the United States Affects approximately 800,000 patients annually 5 th leading cause of death in the United States Leading cause of long term disability in the United States IV tpa has class IA recommendation for stroke patients meeting eligibility criteria Only 5% of stroke patients receive IV tpa 5
6 6
7 Risk Factors for sich 1. SIZE OF INFARCT NIHSS >22, Edema Damage to underlying basal lamina and integrity of the vasculature Reperfusion (especially delayed) Hemorrhagic transformation is a natural evolution of stroke, thrombolytics exacerbate it. 2. Treatment with antiplatelets/anticoagulants 3. Medical Comorbidities HTN, DM, Fever 4. Older Age 7

8 43% good outcome 6 % sich NNT 8 56% good outcome 2.5 % sich (7% with NINDS criteria) NNT 14
9 tpa Recommendations Past 15 Years 2003 AHA/ASA Guideline for Early Management of Patients with Acute ischemic Stroke 2005 AHA/ASA Update to Guideline for Early Management of Patients with Acute ischemic Stroke AHA/ASA Guideline for Early Management of Patients with Acute ischemic Stroke 2009 AHA/ASA Expansion of the Time Window for Treatment with IV tpa 2013 AHA/ASA Guideline for Early Management of Patients with Acute ischemic Stroke 2015 Updated FDA label and Package insert for Alteplase 2015 AHA/ASA Scientific Rationale for Inclusion/Exclusion Criteria of IV tpa in Acute Ischemic Stroke 9
10 2013 AHA/ASA Inclusion Criteria Diagnosis of ischemic stroke causing measurable deficit Onset less than 3 hours before beginning treatment Age >18 Onset within 3 to 4.5 hours before beginning treatment Relative exclusions: Age >80 NIHSS >25 Use of oral anticoagulant regardless INR History of stroke and diabetes 10
11 2013 AHA/ASA Exclusion Criteria Significant head trauma or prior stroke in the previous 3 months Arterial puncture at non-compressible site in previous 7 days History of previous ICH or symptoms suggesting SAH Intracranial neoplasm, arteriovenous malformation, or aneurysm Recent intracranial or intraspinal surgery Elevated blood pressure (SBP >185 mm Hg or DBP >110 mm Hg) Active internal bleeding Platelet count < /mm3 Heparin received within 48 hours with abnormally elevated aptt Current use of anticoagulant with INR >1.7 or PT >15 seconds Use of direct thrombin inhibitors or direct factor Xa inhibitors with elevated aptt, INR, ECT, TT, factor Xa activity assays) Blood glucose concentration <50 mg/dl (2.7 mmol/l) CT demonstrates large infarction 11
12 2013 AHA/ASA Relative Exclusion Criteria Minor or rapidly improving stroke symptoms Pregnancy Seizure at onset with postictal residual neurological impairments Major surgery or serious trauma within previous 14 days Recent gastrointestinal or urinary tract hemorrhage (within previous 21 days) Recent acute myocardial infarction (within previous 3 months) 12
13 Relative Exclusions 3 to 4.5 Hour Window Age >80 NIHSS >25 Use of oral anticoagulant regardless INR History of stroke and diabetes 13
14 14

15 15 Understand why patients are not receiving IV tpa Maximize number of patients eligible to IV tpa
16 Why Are Patients Not Receiving tpa? Delays in presentation Only 22% arrive within 3 hours Strict eligibility criteria 6-8% of all AIS are eligible for tpa If ALL AIS patients arrived in <3 hours, only 29% would be eligible based on NINDS criteria Mild stroke(43), HTN (10), Seizure (7), Bleeding Diathesis (6), Glucose (3) 16
17 17 Stroke Severity Mild and Rapidly Improving Strokes 31% of strokes arriving within 2 hours of LSW are excluded for mild or rapidly improving strokes 28% not discharged home 2 % mortality 10 % SNF 28% unable to ambulate independently at time of discharge Overall 2-15 % of mild AIS are treated with IV tpa
18 Case 1 67M with PMH of HTN arrived with EMS at 1502 with NIHSS 4 (1 aphasia, 2 right arm, 1 mouth droop) LSW per spouse Direct to CT scan (negative for ICH), glucose 104, BP 147/ NIHSS at 2 after improvement in speech and arm strength Decision made to NOT give tpa 1650 Admitted to inpatient unit with NIHSS MRI confirmed L parietal infarct and distal MCA branch occlusion Discharged to rehab on hospital day 3 NIHSS 5 ( 1 mouth droop, 2 R arm, 1 R leg, 1 aphasia) mrs at 8 week clinic visit 2 18

19 Stroke Severity Milder strokes with NIHSS < 4 have sich rate 0-2% Demonstrated benefit of IV tpa in mild stroke Think: Is this neurologic deficit disabling? 19

20 Disabling Symptoms? 20
21 Severe Strokes Stroke Severity Mild stroke (NIHSS <20) is the number one predictor of good outcome with or without treatment The treatment effect is consistent 22% vs 12% in patients with NIHSS >20 and age < 65 High NIHSS is a predictor of sich This does NOT outweigh the benefit of IV tpa in these patients High NIHSS is predictor of sich with or without tpa 21
22 AHA/ASA RECOMMENDATIONS For severe stroke symptoms, IV tpa is indicated within 3 hours despite increased risk of hemorrhage IV tpa is reasonable for patients with moderate to severe symptoms who demonstrate early improvement. Delaying treatment to monitor for further improvement is NOT recommended For patients with mild but none the less disabling symptoms who arrive within 3 hours IV tpa should be given, there should be NO exclusions because there is proven clinical benefit 22
23 The AHA recommends this as a treatment for acute ischemic stroke, it has also been used as first line treatment for urosepsis, seizures, and conversion disorder. What is IV tpa? Courtesy of Neuro ICU jeopardy. C Ratay
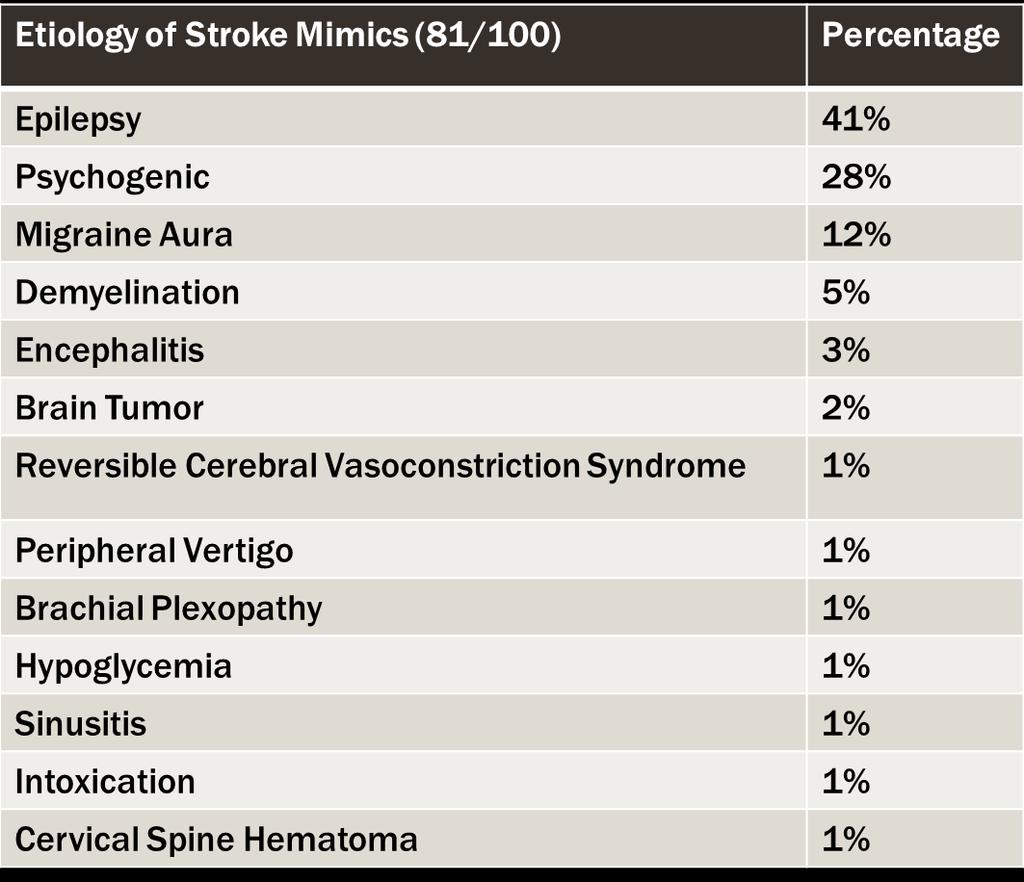
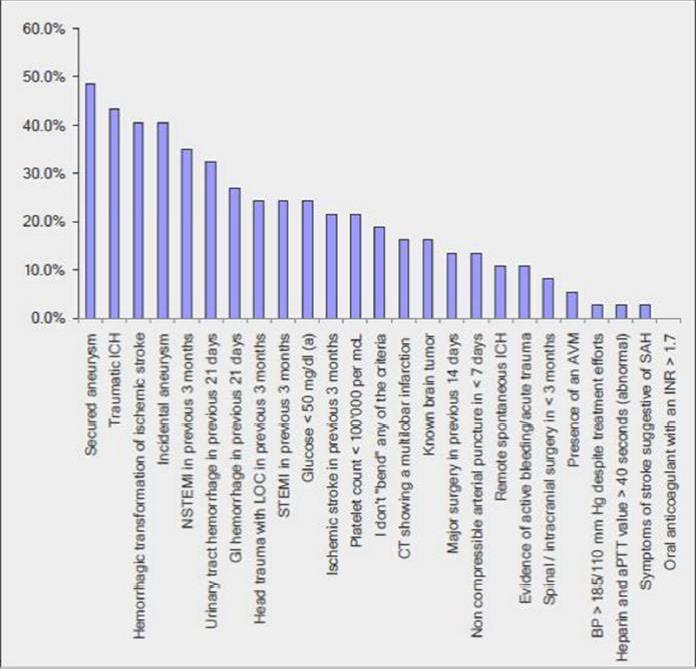
24 Mimics 24
25 Mimics 25
26 Risk Factors for sich 1. SIZE OF INFARCT (only independent risk factors) Damage to underlying basal lamina and integrity of the vasculature Reperfusion (especially delayed) Hemorrhagic transformation is a natural evolution of stroke, thrombolytics exacerbate it. 2. Treatment with antiplatelets/anticoagulants 3. Medical Comorbidities HTN, DM, Fever 4. Older Age These risk factors are generally not present in stroke mimics! 26
27 Mimics Blood glucose levels account for < 1 % of mimics and rarely result in focal neurologic deficits Generally accompanies other symptoms diaphoresis Hypo/hyperglycemia has not been shown to pose an increased risk of complications after IV tpa (0-2%) 27
28 Mimics Seizures at onset of AIS traditionally considered at contraindication Seizures can occur at onset of an AIS Of 300 patients described in reports of having received IV tpa after seizure, only 2 had sich 28
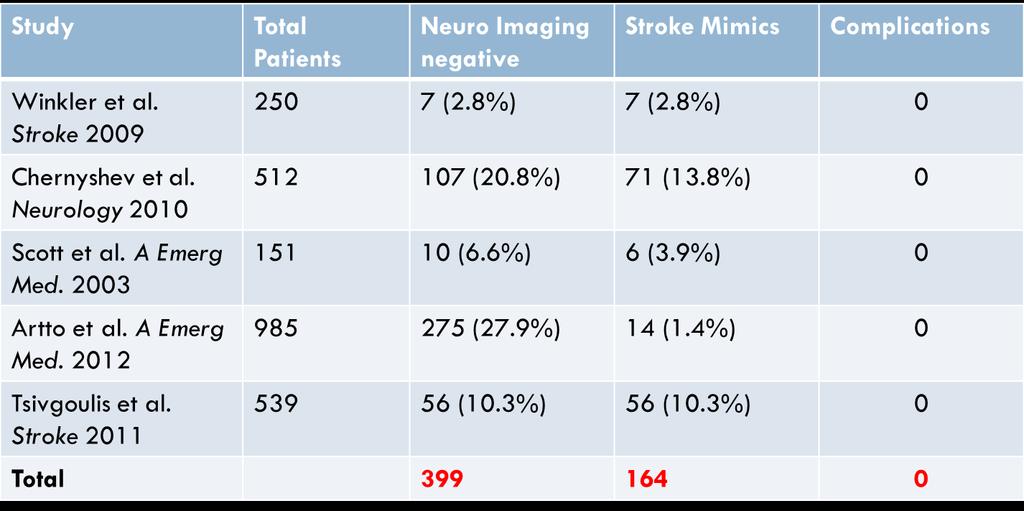
29 Mimics Low rate of mimics (<1%) Relative safety of IV tpa in mimics (0-2% sich) Frequent strokes accompanying glucose abnormalities and seizures Known harm in not administering IV tpa to AIS 29
30 AHA/ASA RECOMMENDATIONS IV tpa is reasonable in patients with a seizure at the time of onset of AIS if evidence suggests that residual symptoms are secondary to AIS Treating clinicians should be aware that hypo/hyperglycemia may mimic AIS and check blood glucose levels Treatment with IV tpa in patients with AIS who present with blood glucose >400mg/dl with subsequent correction is reasonable The risk of sich in conversion/psychogenic/malingering stroke mimics is quite low; starting intravenous t-pa is probably recommended in preference over delaying treatment to pursue additional testing 30
31 Intracranial Lesions Un-ruptured intracranial aneurysm is listed as exclusion for IV tpa in 2013 AHA/ASA guidelines Intracranial neoplasm is listed as exclusion for IV tpa in 2013 AHA/ASA guidelines 31
32 Aneurysm Unruptured aneurysm occurs in 2-3% of general population Case reports have been published on IV tpa in the setting of incidental aneurysm Mostly anterior circulation, mostly aneurysms <5mm NO difference in sich as compared to those without aneurysm AHA/ASA Recommendation for patients with acute ischemic stroke who are known to harbor a small or moderate-sized (<10mm) unruptured and unsecured aneurysm, IV tpa is reasonable 32
33 Intracranial Neoplasm Several case reports of sich in the setting of GBM have shown increased risk of sich Publications on IV tpa in extra-axial lesions (meningioma, paranasal tumors, etc.), show NO increase in sich AHA/ASA Recommendation IV tpa treatment is recommended for patients with acute ischemic stroke who harbor a known extra-axial intracranial neoplasm 33
34 3 to 4.5 Hour Exclusions Age > 80 NIHSS>25 PMH diabetes and CVA Use of oral anticoagulant, regardless of INR 34
35 3 to 4.5 Hour Window sich Ambulatory Age > 80 8 % vs 6.7% 19.5 % vs 17.7% NIHSS > % vs 10% 7.8% vs 10% OAC INR< % vs 6.8% 26.6% vs 24.7% PMH CVA and DM 6.9% vs 4.5% 34.9% vs 30.8% 35
36 3 to 4.5 Hour Exclusions Age > 80 AHA/ASA: IV tpa in the 3 to 4.5 hour window is safe and as effective as in younger patients NIHSS>25 AHA/ASA: Limited data, unclear benefit PMH diabetes and CVA AHA:ASA: IV tpa is as effective and safe as in the 0 to 3 hour window Use of Oral anticoagulant, regardless of INR AHA/ASA: For patients with INR < 1.7 in the 3 to 4.5 hour window IV tpa is safe and beneficial 36
37 Emergency Nursing Priorities Establish LSW Prioritize Diagnostics CT imaging and lab testing Perform and monitor NIHSS/neurologic exam within 15 minutes of arrival Obtain IV access - 1 peripheral IV Obtain weight for tpa dosing, ideally actual weight Administer thrombolytic therapy when ordered Monitor the post IV t-pa patient every 15 minutes with Vital Signs and NIHSS Observe for bleeding complications and neurologic changes 37
38 General Considerations Mix early Forget the Foley Coagulation studies are not required One IV is fine Written consent is not required 38

39 Conclusions Spread the word! Time to presentation is the number one reason for exclusion 39
40 Conclusions Do not delay for any reason Exclusion criteria are not always exclusions Consider symptom impact over NIHSS value and aggressively treat mild but disabling strokes Assess each case individually and consider risk benefit of treating AND of not treating 40
41 References Damaerschalk BM, Kleindorfer DO, Adeoye OM, Demchuk AM, Fugate JE, & Grotta JC, et al. Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. 2016; Stroke; 47: Nasr DM, Brinjiki W, Cloft HJ, Rabinstein AA.. Utilization of intravenous thrombolysis is increasing in the United States. Int J Stroke. 2013; 8: Tissue Plasminogen activator for acute ischmic stroke: the National Institute of Neurologic Disorders and Stroke rt-pa Stroke Study Group. N Eng J Med. 1995; 333: Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Eng J Med. 2008; 359: Kleindorfer DO, Kissela B, Schneider A, Woo D, Khoury J, Miller, R, et al. Eligibility for recombinant tissue-type plasminogen activator in acute ischemic stroke: a population based study. Stroke. 2004; 35: e27-e29. Smith EE et al. Outcomes in mild and rapidly improving stroke not treated with intravenous recombinant tissue-type plasminogen activator: findings from Get With the Guidelines Stroke. Stroke. 2011; 42: De Los Rios la Rosa F, Khoury J, Kissela BM, Flaherty ML, Alwell K, Moomaw CJ, et al. Eligibility for intravenous recombinant tissue-type plasminogen activator within a population: the effect of the European Cooperative Acute Stroke Tsudy (ECASS0 III Trial. Stroke. 2012; 43: Jauch EC, Saver JL, Adams HP, Bruno A, Connors JJ, Demaershalk BM, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals form the American Heart Association/American Stroke Association. Stroke. 2013; 44: Demchuk AM, Tuanne D, Hill MD, Kasner SE, Hanson S, Grond M, et al. Predictors of good outcome after intravenous t-pa for acute ischemic stroke. Neurology. 2001; 57: Levine SR, Khatri P, Broderick JP, Grotta JC, Kasner SE, Kim D, et al. Review, historical context, and clarification of the NINDS rt-pa stroke trials exclusion criteria: Part 1: rapidly improving symptoms. Stroke. 2013; 44: Scott P, Seilbergliet R. Misdiagnosis of stroke in tissue plasminogen activator treated stroke patients: Characteristics and outcomes. Annals of Emergency Medicine. 2003; 42: Winkler DT, Fluri F, Fuhr P, Wetzel SG, Lyrer PA, Ruegg S, et al. Thrombolysis in stroke mimics: Frequency, clinical characteristics, and outcomes. Stroke. 2009; 40: Urra X, Ariño H, Llull L, Amaro S, et al. (2013) The Outcome of Patients with Mild Stroke Improves after Treatment with Systemic Thrombolysis. PLoS ONE 8(3): e doi: /journal.pone
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Table 1. Specific changes to the FDA labeling for recombinant tissue plasminogen activator (Alteplase, Activase, Genentech, inc).
.") Acute Ischemic Stroke Controversies Steven R. Messé, MD, FAAN Associate professor of Neurology, Pereleman School of Medicine at the University of Pennsylvania, Philadelphia, PA Using the term controversy
Acute Ischemic Stroke Controversies Steven R. Messé, MD, FAAN Associate professor of Neurology, Pereleman School of Medicine at the University of Pennsylvania, Philadelphia, PA Using the term controversy
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Thrombolytic Therapy in Acute Ischemic Stroke: Time is Brain -How to Move the Needle on Door-to-Needle
 Thrombolytic Therapy in Acute Ischemic Stroke: Time is Brain -How to Move the Needle on Door-to-Needle Alissa Rich, Pharm.D., M.B.A. Robyn Stakley, Pharm.D. Oct. 12, 2017 2 Disclosures The presenters have
Thrombolytic Therapy in Acute Ischemic Stroke: Time is Brain -How to Move the Needle on Door-to-Needle Alissa Rich, Pharm.D., M.B.A. Robyn Stakley, Pharm.D. Oct. 12, 2017 2 Disclosures The presenters have
Thrombolysis administration
 Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Thrombolysis administration Liz Mackey Stroke Nurse Practitioner Western Health Sunshine & Footscray Hospital, Melbourne Thanks ASNEN committee members Skye Coote, Acute Stroke Nurse, Eastern Health (slide
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Current US guidelines for the treatment of acute ischemic
 Eligibility for Intravenous Recombinant Tissue-Type Plasminogen Activator Within a Population The Effect of the European Cooperative Acute Stroke Study (ECASS) III Trial Felipe de los Ríos la Rosa, MD;
Eligibility for Intravenous Recombinant Tissue-Type Plasminogen Activator Within a Population The Effect of the European Cooperative Acute Stroke Study (ECASS) III Trial Felipe de los Ríos la Rosa, MD;
o Unenhanced Head CT
 Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
Drip & Ship Protocol Acute Stroke Ready Hospital (ASRH) Duluth Area Primary Stroke Center (St. Luke s & St. Mary s Essentia) PATIENT LABEL Patient displays strokelike symptoms EMS/ED CSS > 0 Glucose >
AHA/ASA Scientific Statement
 AHA/ASA Scientific Statement Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke A Statement for Healthcare Professionals From the American
AHA/ASA Scientific Statement Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke A Statement for Healthcare Professionals From the American
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial
 Trial") The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
The Multi arm Optimization of Stroke Thrombolysis (MOST) Trial Study Team Principal Investigators: Opeolu Adeoye, University of Cincinnati (Lead) Andrew Barreto, University of Texas Houston Jim Grotta,
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke. We are against it!!
 Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Recent Changes in IV TPA Recommendations. Ashish Masih, M.D Vascular Neurology
 Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Page 1 of 7. Intraparenchymal hemorrhage or subarachnoid hemorrhage. Consult neurosurgery
 Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Management of Acute Ischemic Stroke in Adult Patients INITIAL ASSESSMENT Look for signs and symptoms of stroke (see Appendix A) STAT finger stick glucose STAT 12-lead EKG Inform radiology that patient
Acute Stroke Care: the Nuts and Bolts of it. ECASS I and II ATLANTIS. Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center
 Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
Acute Stroke Care: the Nuts and Bolts of it Chris V. Fanale, MD Colorado Neurological Institute Swedish Medical Center ECASS I and II tpa for patients presenting
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
Disclosure. + Outline. What is a stroke? Role of imaging in stroke Ischemic stroke Venous infarct Current topics
 + Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
+ Kathleen R. Fink, MD University of Washington 5 th Nordic Emergency Radiology Course May 21, 2015 + Disclosure My spouse receives research salary support from: Bracco BayerHealthcare Guerbet Thank you
CVA Updates Karen Greenberg, DO, FACOEP. Director Neurologic Emergency Department Crozer Chester Medical Center
 CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
CVA Updates 2018 Karen Greenberg, DO, FACOEP Director Neurologic Emergency Department Crozer Chester Medical Center Disclosure I have the following financial relationship with the manufacturer of any commercial
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1
 VERSION 2.1") New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
New Jersey Department of Health ACUTE STROKE REGISTRY (NJASR) VERSION 2.1 A. DEMOGRAPHIC DATA *Hospital Type (1): 1=Primary 2=Comprehensive 3=Other *Hospital Code (2): *Hospital Transferred From Code (3):
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Acute ischemic stroke is a major cause of morbidity
 Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
Outcomes of Treatment with Recombinant Tissue Plasminogen Activator in Patients Age 80 Years and Older Presenting with Acute Ischemic Stroke Jennifer C. Drost, DO, MPH, and Susana M. Bowling, MD ABSTRACT
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group
 Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
AMSER Case of the Month: March 2019
 AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
AMSER Case of the Month: March 2019 62 year-old male with left-sided weakness Ashley Graziano OMS IV, Lake Erie College of Osteopathic Medicine Erik Yannone MD, Charles Q. Li MD, Warren Chang MD, Matthew
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE
 Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Objectives Acute Stroke Management LUKE BRADBURY, MD 10/8/14 FALL WAPA CONFERENCE Recognize the clinical signs of acute stroke Differentiate between stroke and some of the more common stroke mimics Review
Telemedicine. Gabriel A. Vidal, MD
 Telemedicine Gabriel A. Vidal, MD Director Comprehensive Stroke Center Ochsner Medical Center, New Orleans Vascular and Interventional Neurology Gulf States Chapter of the Society of Hospital Medicine
Telemedicine Gabriel A. Vidal, MD Director Comprehensive Stroke Center Ochsner Medical Center, New Orleans Vascular and Interventional Neurology Gulf States Chapter of the Society of Hospital Medicine
Mohamed Al-Khaled, MD,* Christine Matthis, MD, and J urgen Eggers, MD*
 Predictors of In-hospital Mortality and the Risk of Symptomatic Intracerebral Hemorrhage after Thrombolytic Therapy with Recombinant Tissue Plasminogen Activator in Acute Ischemic Stroke Mohamed Al-Khaled,
Predictors of In-hospital Mortality and the Risk of Symptomatic Intracerebral Hemorrhage after Thrombolytic Therapy with Recombinant Tissue Plasminogen Activator in Acute Ischemic Stroke Mohamed Al-Khaled,
The Outcome of Patients with Mild Stroke Improves after Treatment with Systemic Thrombolysis
 The Outcome of Patients with Mild Stroke Improves after Treatment with Systemic Thrombolysis Xabier Urra 1,2, Helena Ariño 1, Laura Llull 1, Sergio Amaro 1,2,Víctor Obach 1,Álvaro Cervera 1,2, Ángel Chamorro
The Outcome of Patients with Mild Stroke Improves after Treatment with Systemic Thrombolysis Xabier Urra 1,2, Helena Ariño 1, Laura Llull 1, Sergio Amaro 1,2,Víctor Obach 1,Álvaro Cervera 1,2, Ángel Chamorro
Update on Acute Stroke Management
 Murray Flaster, M.D., Ph.D. Stroke Medical Director Lancaster General Health INTRODUCTION Over the last 20 years, there have been major advances in the care of patients with acute stroke due to progress
Murray Flaster, M.D., Ph.D. Stroke Medical Director Lancaster General Health INTRODUCTION Over the last 20 years, there have been major advances in the care of patients with acute stroke due to progress
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2
 Measure Set Session 2") Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Thrombolytics and Beyond
 Thrombolytics and Beyond Greenville Memorial Rodney Leacock MD Introduction 795,000 strokes per year in the US 87% ischemic 13% hemorrhage, 3% SAH Fourth leading cause of death - was third Mortality rate
Thrombolytics and Beyond Greenville Memorial Rodney Leacock MD Introduction 795,000 strokes per year in the US 87% ischemic 13% hemorrhage, 3% SAH Fourth leading cause of death - was third Mortality rate
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
RBWH ICU Journal Club February 2018 Adam Simpson
 RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
RBWH ICU Journal Club February 2018 Adam Simpson 3 THROMBOLYSIS Reperfusion therapy has become the mainstay of therapy for ischaemic stroke. Thrombolysis is now well accepted within 4.5 hours. - Improved
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Review of the TICH-2 Trial
 Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Review of the TICH-2 Trial Mikaela Hofer, PharmD PGY-1 Pharmacy Resident Pharmacy Grand Rounds September 18, 2018 2018 MFMER slide-1 Objectives Review the pharmacologic options to limit hematoma expansion
Ischemic Stroke: Treatment Update. American College of Physicians Northern California Chapter Scientific Meeting October 21, 2017 Kwan Ng MD, PhD
 Ischemic Stroke: Treatment Update American College of Physicians Northern California Chapter Scientific Meeting October 21, 2017 Kwan Ng MD, PhD Objectives Understand the treatment of acute stroke Thrombectomy
Ischemic Stroke: Treatment Update American College of Physicians Northern California Chapter Scientific Meeting October 21, 2017 Kwan Ng MD, PhD Objectives Understand the treatment of acute stroke Thrombectomy
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care
 Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Activase Therapy. Contact Hours: 2.0 First Published: April 12, 2012 Updated: June, 2018 Course Expires: June 30, 2020
 Activase Therapy Contact Hours: 2.0 First Published: April 12, 2012 Updated: June, 2018 Course Expires: June 30, 2020 Copyright 2012 by RN.com All Rights Reserved Reproduction and distribution of these
Activase Therapy Contact Hours: 2.0 First Published: April 12, 2012 Updated: June, 2018 Course Expires: June 30, 2020 Copyright 2012 by RN.com All Rights Reserved Reproduction and distribution of these
Stroke in the Emergency Room: What do we need to know?
 Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
Stroke in the Emergency Room: What do we need to know? Salah G. Keyrouz, MD, FAHA March 10, 2012 Stroke in the Emergency Room: What do we need to know? Disclosure: None 2 1 Outline Definition Introduction
ST Elevated Myocardial Infarction- Latest AHA recommendations
 ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
ST Elevated Myocardial Infarction- Latest AHA recommendations Sherry Turner, DO, MPH, FACOEP Medical Director Emergency Services Wesley Medical Center The Problem 250,000 Americans each year 30% fail to
Role of recombinant tissue plasminogen activator in the updated stroke approach
 Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Outcomes of Patients Requiring Blood Pressure Control Before Thrombolysis with tpa for Acute Ischemic Stroke
 Original Research Outcomes of Patients Requiring Blood Pressure Control Before Thrombolysis with tpa for Acute Ischemic Stroke Bryan Darger, BA* Nicole Gonzales, MD Rosa C. Banuelos, PhD* Hui Peng, PhD
Original Research Outcomes of Patients Requiring Blood Pressure Control Before Thrombolysis with tpa for Acute Ischemic Stroke Bryan Darger, BA* Nicole Gonzales, MD Rosa C. Banuelos, PhD* Hui Peng, PhD
Clinical Features of Patients Who Come to Hospital at the Super Acute Phase of Stroke
 Research Article imedpub Journals http://www.imedpub.com Clinical Features of Patients Who Come to Hospital at the Super Acute Phase of Stroke Abstract Background: The number of patients who are adopted
Research Article imedpub Journals http://www.imedpub.com Clinical Features of Patients Who Come to Hospital at the Super Acute Phase of Stroke Abstract Background: The number of patients who are adopted
IV tpa and mechanical thrombectomy case selection
 IV tpa and mechanical thrombectomy case selection 22 April 2017, 9.50-10.30 Deidre De Silva SGH campus, NNI, Singapore OUTLINE Reperfusion concept Case Selection factors IV tpa & Mechanical Thrombectomy
IV tpa and mechanical thrombectomy case selection 22 April 2017, 9.50-10.30 Deidre De Silva SGH campus, NNI, Singapore OUTLINE Reperfusion concept Case Selection factors IV tpa & Mechanical Thrombectomy
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Treatment and Outcome of Hemorrhagic Transformation after Intravenous Alteplase in Acute Ischemic Stroke
 Treatment and Outcome of Hemorrhagic Transformation after Intravenous Alteplase in Acute Ischemic Stroke A Scientific Statement for Healthcare Professionals from the American Heart Association/American
Treatment and Outcome of Hemorrhagic Transformation after Intravenous Alteplase in Acute Ischemic Stroke A Scientific Statement for Healthcare Professionals from the American Heart Association/American
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Update on Neurologic Emergencies
 Update on Neurologic Emergencies KAREN GREENBERG, DO, FACOEP ARIA JEFFERSON HEALTH SYSTEM VIRTUA HEALTH SYSTEM KENNEDY HEALTH SYSTEM Disclosures Genentech Speakers Bureau I have disclosed a relevant relationship
Update on Neurologic Emergencies KAREN GREENBERG, DO, FACOEP ARIA JEFFERSON HEALTH SYSTEM VIRTUA HEALTH SYSTEM KENNEDY HEALTH SYSTEM Disclosures Genentech Speakers Bureau I have disclosed a relevant relationship
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
TENNESSEE STROKE REGISTRY QUARTERLY REPORT
 TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 2 July 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender distributions,
TENNESSEE STROKE REGISTRY QUARTERLY REPORT Volume 1, Issue 2 July 2018 This report is published quarterly using data from the Tennessee Stroke Registry. Inside this report Data on diagnosis, gender distributions,
Quality ID #187: Stroke and Stroke Rehabilitation: Thrombolytic Therapy National Quality Strategy Domain: Effective Clinical Care
 Quality ID #187: Stroke and Stroke Rehabilitation: Thrombolytic Therapy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #187: Stroke and Stroke Rehabilitation: Thrombolytic Therapy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process