Acute Coronary Syndromes: Review and Update
|
|
|
- Amie Miles
- 6 years ago
- Views:
Transcription
1 Acute Coronary Syndromes: Review and Update Core Curriculum for the Cardiovascular Clinician September 14-17, 2016 R. David Anderson, MD, MS, FACC Professor of Medicine Director of Interventional Cardiology Director of the UF Health Cardiac Cath Lab Program Director: Interventional Cardiology Fellowship University of Florida Health Gainesville, Florida
2 Disclosures Biosense Webster (a J&J Co.) consultant
3 Objectives background of acute coronary syndromes update on the new 2014 NSTEMI/ACS guidelines highlights of the 2013 STEMI and 2015 PCI guidelines some clinical trial data case examples


4

5 World Heath Organization 2012 Ischemic Heart Disease Still the leading cause of death worldwide
6 Hospital Discharges for ACS: UA/NSTEMI vs STEMI UA * ACS 1.67 Million Hospital Discharges ACS MI 700, ,000 UA/NSTEMI Million Discharges per Year * UA=unstable angina. NSTEMI=non ST-segment elevation myocardial infarction (also known as non Q-wave MI). ** STEMI=ST-segment elevation MI (also known as Q-wave MI). American Heart Association. Heart Disease and Stroke Statistics 2009 Update. Circulation. 2009;119:e21-E181. NSTEMI 652,000 Discharges per Year STEMI ** 321,000 Discharges per Year


7 Acute Coronary Syndromes Wright, R. S. et al. J Am Coll Cardiol 2011;57:e215-e367
8 Identification of ACS Patients in the ED Patients with the following symptoms and signs require immediate assessment by the triage nurse for the initiation of the ACS protocol: Chest pain or severe epigastric pain, nontraumatic in origin, with components typical of myocardial ischemia or MI: Central/substernal compression or crushing chest pain Pressure, tightness, heaviness, cramping, burning, aching sensation Unexplained indigestion, belching, epigastric pain Radiating pain in neck, jaw, shoulders, back, or 1 or both arms Associated dyspnea Associated nausea/vomiting Associated diaphoresis Adapted from the National Heart Attack Alert Program. Emergency Department: rapid identification and treatment of patients with acute myocardial infarction. US Department of Health and Human Services. US Public Health Service. National Institutes of Health. National Heart, Lung and Blood Institute; September 1993; NIH Publication No Also see Table 2 of Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157.
9 Causes of UA/NSTEMI or STEMI Thrombus or thromboembolism, usually arising on disrupted or eroded plaque Occlusive thrombus (STEMI), usually with collateral vessels (NSTEMI) Subtotally occlusive thrombus on pre-existing plaque (NSTEMI) Distal microvascular thromboembolism from plaque-associated thrombus (NSTEMI) Thromboembolism from plaque erosion (STEMI or NSTEMI) Non plaque-associated coronary thromboembolism Dynamic obstruction (coronary spasm or vascoconstriction) of epicardial and/or microvascular vessels Progressive mechanical obstruction to coronary flow Coronary arterial inflammation Coronary artery dissection *These causes are not mutually exclusive; some patients have 2 or more causes. DeWood MA, et al. N Engl J Med 1986;315: May occur on top of an atherosclerotic plaque, producing missed-etiology angina or UA/NSTEMI. Rare. Modified with permission from Braunwald E. Circulation 1998;98: Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157, Table 3.
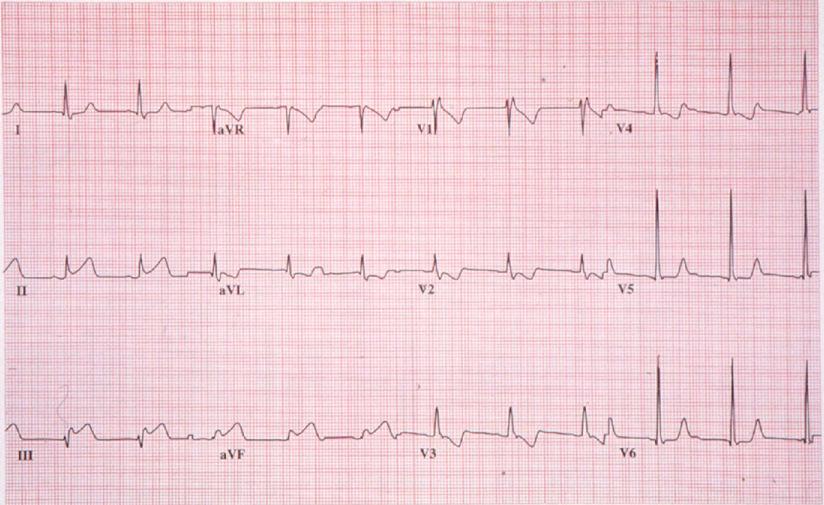
10 Case Presentation #1 78-year-old woman presented to the ED with 3 hours of acute onset shortness of breath with associated chest pain Hypertension, hyperlipidemia on treatment Nonsmoker Stable angina Taking aspirin, β-blocker, statin
11 Case Presentation #1 cont. Physical Findings in the ED Blood pressure: 170/90 mm Hg, wt 128 lbs. Heart rate: 75 bpm, regular Lungs clear Chest auscultation and heart sounds: normal S 1, S 2 ; no S 3 No peripheral edema ECG: LVH with lateral ST-segment and T-wave abnormalities unchanged Other examination findings normal
12 Case Presentation #1 cont. Initial Risk Stratification Chest pain resolved with NTG Troponin T positive = 0.14 ng/ml (ULN = 0.1) CKMB = 3 (ULN = 5) BNP = 180 mg /dl Creatinine = 1.6
13 What is the diagnosis? a) Unstable angina b) Non-ST Elevation MI (NSTEMI) c) ST-Elevation MI (STEMI)
14 What is the diagnosis? a) Unstable angina b) Non-ST Elevation MI (NSTEMI) chest pain positive biomarkers lack of ST-elevation on ECG a) ST-Elevation MI (STEMI)
15 Prognosis: Early Risk Stratification Recommendations COR LOE In patients with chest pain or other symptoms suggestive of ACS, a 12-lead ECG should be performed and evaluated for ischemic changes within 10 minutes of the patient s I C arrival at an emergency facility. If the initial ECG is not diagnostic but the patient remains symptomatic and there is a high clinical suspicion for ACS, serial ECGs (e.g., 15- to 30-minute intervals during the first I C hour) should be performed to detect ischemic changes. Serial cardiac troponin I or T levels (when a contemporary assay is used) should be obtained at presentation and 3 to 6 hours after symptom onset (see Section 3.4, Class I, #3 recommendation if time of symptom onset is unclear) in all patients who present with symptoms consistent with ACS to identify a rising and/or falling pattern of values. I A J Am Coll Cardiol. 2014;():. doi: /j.jacc
16 Prognosis: Early Risk Stratification (cont d) Recommendations COR LOE It is reasonable to obtain supplemental electrocardiographic leads V 7 to V 9 in patients whose initial ECG is nondiagnostic IIa B and who are at intermediate/high risk of ACS. Continuous monitoring with 12-lead ECG may be a reasonable alternative in patients whose initial ECG is IIb B nondiagnostic and who are at intermediate/high risk of ACS. Measurement of B-type natriuretic peptide or N-terminal pro B-type natriuretic peptide may be considered to assess risk in patients with suspected ACS. IIb B J Am Coll Cardiol. 2014;():. doi: /j.jacc
17 What should be done next for this patient? a) take her directly to the cath lab b) thrombolytic therapy c) adenosine stress nuclear imaging d) further risk stratification
18 What should be done next for this patient? a) take her directly to the cath lab b) thrombolytic therapy c) adenosine stress nuclear imaging d) further risk stratification
19 Prognosis: Early Risk Stratification (cont d) Recommendations COR LOE Additional troponin levels should be obtained beyond 6 hours after symptom onset (see Section 3.4, Class I, #3 recommendation if time of symptom onset is unclear) in patients with normal troponin levels on serial examination I A when changes on ECG and/or clinical presentation confer an intermediate or high index of suspicion for ACS. Risk scores should be used to assess prognosis in patients with NSTE-ACS. I A Risk-stratification models can be useful in management. IIa B J Am Coll Cardiol. 2014;():. doi: /j.jacc
20 Biomarkers: Diagnosis Recommendations COR LOE Cardiac-specific troponin (troponin I or T when a contemporary assay is used) levels should be measured at presentation and 3 to 6 hours after symptom onset in all I A patients who present with symptoms consistent with ACS to identify a rising and/or falling pattern. Additional troponin levels should be obtained beyond 6 hours after symptom onset in patients with normal troponins on serial examination when electrocardiographic changes I A and/or clinical presentation confer an intermediate or high index of suspicion for ACS. If the time of symptom onset is ambiguous, the time of presentation should be considered the time of onset for I A assessing troponin values. With contemporary troponin assays, creatine kinase myocardial isoenzyme (CK-MB) and myoglobin are not useful for diagnosis of ACS. III: No Benefit A J Am Coll Cardiol. 2014;():. doi: /j.jacc
21 Our Patient s TIMI Risk Sore 1. Age 65 y 2. 3 CAD risk factors (high cholesterol, family history, hypertension, diabetes, smoking) 3. Prior coronary stenosis 50% 4. Aspirin in last 7 days 5. 2 anginal events 24 h 6. ST-segment deviation 7. Elevated cardiac markers (CK-MB or troponin) % Death / MI / Urgent Revasc at 14 d / /7 Number of Predictors Antman EM, et al. JAMA. 2000;284(7):


22 Our Patient s GRACE Prediction Score for All-Cause Mortality From Discharge to 6 Months NSTEMI 6-Month Postdischarge Mortality Risk GRACE Probability Category Score of Death Medical History Age in Years Points History of Congestive Heart Failure...24 History of Myocardial Infarction Findings at Initial Hospital Presentation Resting Heart Rate Points Beats/min Systolic Blood Pressure, Mm Hg ST-Segment Depression Findings During Hospitalization Initial Serum Points Creatinine, mg/dl Elevated Cardiac Enzymes..15 No In-Hospital Percutaneous Coronary Intervention 14 Low 1-88 <3% Medium % High >8% table.cfm. Reprinted with permission from Eagle KA, et al. JAMA. 2004;291(22): Points Total Risk Score 150 (sum of points) 10% Mortality Risk (from plot) Probability Predicted All-Cause Mortality from Hospital Discharge to 6 Months X Total Risk Score
23 What Treatments Should be Initiated? a) aspirin b) clopidogrel c) ticagrelor d) anti-thrombotic therapy e) A, B, and D f) A, C, and D
24 What Treatments Should be Initiated? a) aspirin b) clopidogrel c) ticagrelor d) anti-thrombotic therapy e) A, B, and D A, C, and D no prasugrel given age and body weight prasugrel only given in cath lab unless STEMI
25 Treatment Case Presentation #1 cont. Patient is given ASA 325 mg enoxaparin 1 mg/kg (no bolus) Ticagrelor 180 mg x 1 no GP IIb/IIIa in ED Admit to CCU
26 Treated With an Initial Invasive or Ischemia-Guided Strategy Recommendations COR LOE Non enteric-coated, chewable aspirin (162 mg to 325 mg) should be given to all patients with NSTE-ACS without contraindications as soon as possible after presentation, I A and a maintenance dose of aspirin (81 mg/d to 162 mg/d) should be continued indefinitely. In patients with NSTE-ACS who are unable to take aspirin because of hypersensitivity or major gastrointestinal intolerance, a loading dose of clopidogrel followed by a daily maintenance dose should be administered. I B J Am Coll Cardiol. 2014;():. doi: /j.jacc
27 Treated With an Initial Invasive or Ischemia-Guided Strategy (cont d) Recommendations COR LOE A P2Y 12 inhibitor (either clopidogrel or ticagrelor) in addition to aspirin should be administered for up to 12 months to all patients with NSTE-ACS without contraindications who are treated with either an early invasive or ischemia-guided strategy. Options include: I B Clopidogrel: 300-mg or 600-mg loading dose, then 75 mg daily Ticagrelor : 180-mg loading dose, then 90 mg twice daily B ǁ The recommended maintenance dose of aspirin to be used with ticagrelor is 81 mg daily. J Am Coll Cardiol. 2014;():. doi: /j.jacc
28 Treated With an Initial Invasive or Ischemia-Guided Strategy (cont d) Recommendations COR LOE It is reasonable to use ticagrelor in preference to clopidogrel for P2Y 12 treatment in patients with NSTE-ACS who undergo an early invasive or ischemia-guided strategy. IIa B In patients with NSTE-ACS treated with an early invasive strategy and dual antiplatelet therapy (DAPT) with intermediate/high-risk features (e.g., positive troponin), a GP IIb/IIIa inhibitor may be considered as part of initial antiplatelet therapy. Preferred options are eptifibatide or tirofiban. IIb B J Am Coll Cardiol. 2014;():. doi: /j.jacc
29 Treatment of Unstable Angina Results of a study from the Montreal Heart Institute % Developing MI placebo aspirin heparin ASA+hep Treatment Data from Theroux P, Quimet H, McCans J, et al. Aspirin, heparin, or both to treat acute unstable angina. N Engl J Med. 1988;319:
 The primary outcome occurred in 9.")
30 Why do we give clopidogrel after ACS? CURE risk of MI, stroke or CV death (N=12,562) Cumulative Hazard Rate Placebo + ASA Months of Follow-up Clopidogrel + ASA % Relative Risk Reduction P= Study subjects had ACS (UA/non ST-elevation MI) The primary outcome occurred in 9.3% of patients in the clopidogrel + ASA group and 11.4% in the placebo + ASA group CURE Trial Investigators. N Engl J Med. 2001;345:
31 Initial Parenteral Anticoagulant Therapy in Patients With Definite NSTE-ACS Recommendations COR LOE In patients with NSTE-ACS, anticoagulation, in addition to antiplatelet therapy, is recommended for all patients irrespective of initial treatment strategy. Treatment options include: Enoxaparin: 1 mg/kg subcutaneous (SC) every 12 hours (reduce dose to 1 mg/kg SC once daily in patients with creatinine clearance [CrCl] <30 ml/min), continued for the duration of hospitalization or until PCI is performed. An initial intravenous loading dose is 30 mg. I A J Am Coll Cardiol. 2014;():. doi: /j.jacc
32 Initial Parenteral Anticoagulant Therapy in Patients With Definite NSTE-ACS (cont d) Recommendations COR LOE (cont d) Bivalirudin: 0.10 mg/kg loading dose followed by 0.25 mg/kg per hour (only in patients managed with an early invasive strategy), continued until diagnostic angiography or B PCI, with only provisional use of GP IIb/IIIa inhibitor, I provided the patient is also treated with DAPT. Fondaparinux: 2.5 mg SC daily, continued for the duration of hospitalization or until PCI is performed. B J Am Coll Cardiol. 2014;():. doi: /j.jacc
33 Initial Parenteral Anticoagulant Therapy in Patients With Definite NSTE-ACS (cont d) Recommendations COR LOE (cont d) If PCI is performed while the patient is on fondaparinux, an B additional anticoagulant with anti-iia activity (either UFH or bivalirudin) should be administered because of the risk of catheter thrombosis. UFH IV: initial loading dose of 60 IU/kg (maximum 4,000 I IU) with initial infusion of 12 IU/kg per hour (maximum 1,000 B IU/h) adjusted per activated partial thromboplastin time to maintain therapeutic anticoagulation according to the specific hospital protocol, continued for 48 hours or until PCI is performed. In patients with NSTE-ACS (i.e., without ST elevation, true III: posterior MI, or left bundle-branch block not known to be A Harm old), intravenous fibrinolytic therapy should not be used. J Am Coll Cardiol. 2014;():. doi: /j.jacc
34 2014 ACC/AHA Recommendations for Initial Management and Anti-Ischemic Therapy Supplemental O 2 to maintain SaO 2 >90% COR1 NTG (IV or PO as dictated clinically) COR1 Avoid nitrates with phosphodiesterase inhibitors COR 3 IV morphine for persistent chest pain COR 2B Avoid NSAIDs other than aspirin COR 3 High-intensity statin therapy COR 1 J Am Coll Cardiol. 2014;():. doi: /j.jacc
35 Factors Associated With Appropriate Selection of Early Invasive Strategy or Ischemia-Guided Strategy in Patients With NSTE-ACS Immediate invasive (within 2 h) Ischemiaguided strategy Early invasive (within 24 h) Delayed invasive (within h) Refractory angina Signs or symptoms of HF or new or worsening mitral regurgitation Hemodynamic instability Recurrent angina or ischemia at rest or with low-level activities despite intensive medical therapy Sustained VT or VF Low-risk score (e.g., TIMI [0 or 1], GRACE [<109]) Low-risk Tn-negative female patients Patient or clinician preference in the absence of high-risk features None of the above, but GRACE risk score >140 Temporal change in Tn (Section 3.4) New or presumably new ST depression None of the above but diabetes mellitus Renal insufficiency (GFR <60 ml/min/1.73 m²) Reduced LV systolic function (EF <0.40) Early postinfarction angina PCI within 6 mo Prior CABG GRACE risk score ; TIMI score 2
36 Early Invasive and Ischemia: Guided Strategies Recommendations COR LOE An urgent/immediate invasive strategy (diagnostic angiography with intent to perform revascularization if appropriate based on coronary anatomy) is indicated in patients (men and women) with NSTE-ACS who have I A refractory angina or hemodynamic or electrical instability (without serious comorbidities or contraindications to such procedures). An early invasive strategy (diagnostic angiography with intent to perform revascularization if appropriate based on coronary anatomy) is indicated in initially stabilized patients with NSTE-ACS (without serious comorbidities or contraindications to such procedures) who have an elevated risk for clinical events. I B J Am Coll Cardiol. 2014;():. doi: /j.jacc
37 Early Invasive and Ischemia: Guided Strategies (cont d) Recommendations COR LOE An early invasive strategy (i.e., diagnostic angiography with intent to perform revascularization) is not recommended in patients with: a. Extensive comorbidities (e.g., hepatic, renal, pulmonary failure, cancer), in whom the risks of revascularization and comorbid conditions are likely to outweigh the benefits of revascularization. (Level of Evidence: C) b. Acute chest pain and a low likelihood of ACS (Level of Evidence: C) who are troponin-negative, especially women. (Level of Evidence: B) III: No Benefit C C B J Am Coll Cardiol. 2014;():. doi: /j.jacc
38 What should be the next step in our patient s care? a) dobutamine stress echocardiography b) cardiac catheterization c) CT Angiography d) PET Scanning
39 What should be the next step in our patient s care? a) dobutamine stress echocardiography b) cardiac catheterization c) CT Angiography d) PET Scanning


40 2013 and 2015 STEMI/PCI Guidelines
41 Case Presentation # F untreated HTN ongoing tobacco use intermittent chest discomfort x 4 days day of admission crushing chest pain at 4pm presented to AGH hospital Inferior STEMI arrest in ambulance with return of spontaneous circulation but not responsive transferred to UF Health for PCI
42 Case - Presentation ECG
43 Case Presentation cont. urgent trip to UF cardiac cath lab coronary angiography severe disease of the left anterior descending (LAD) moderate disease of the circumflex occluded right coronary artery (RCA) percutaneous coronary intervention PCI balloon angioplasty paclitaxel drug-eluting stent (Taxus) in distal RCA second paciltaxel stent in mid-rca. resolution of ST-elevation and chest discomfort
44 Case Presentation What to do next? a) aspirin b) clopidogrel, prasugrel or ticagrelor? c) hypothermia d) all of the above
45 Case Presentation What to do next? a) aspirin b) clopidogrel, prasugrel or ticagrelor? c) hypothermia d) all of the above
46 Evaluation and Management of Patients With STEMI and Out-of-Hospital Cardiac Arrest I IIa IIb III I IIa IIb III Therapeutic hypothermia should be started as soon as possible in comatose patients with STEMI and out-of-hospital cardiac arrest caused by VF or pulseless VT, including patients who undergo primary PCI. Immediate angiography and PCI when indicated should be performed in resuscitated out-of-hospital cardiac arrest patients whose initial ECG shows STEMI. J Am Coll Cardiol. 2013;61(4):e78-e140
47 What about the LAD?
48 Culprit Artery Only Versus Multivessel PCI COR LOE Recommendation IIb B-R PCI of a noninfarct artery may be considered in selected patients with STEMI and multivessel disease who are hemodynamically stable, either at the time of primary PCI or as a planned staged procedure Modified recommendation from 2013 Guideline (changed class from III: Harm to IIb and expanded time frame in which multivessel PCI could be performed).
49 Aspiration Thrombectomy COR LOE Recommendations IIb III: No Benefit C-LD A The usefulness of selective and bailout aspiration thrombectomy in patients undergoing primary PCI is not well established. 1 Routine aspiration thrombectomy before primary PCI is not useful Modified recommendation from 2013 guideline (Class changed from IIa to IIb for selective and bailout aspiration thrombectomy before PCI) 2. New recommendation
50 Case Presentation cont now 63 hypertension, hyperlipidemia still smoking stopped clopidogrel interval history includes CVA admitted with same symptoms of chest/jaw pain inferior ST-elevation on ECG
51 How do we treat her now? prasugrel now available ticagrelor not yet available has history of CVA and weighs < 65 kg increase the clopidogrel dose? genotyping? assess platelet function? smoking cessation try to assure compliance!?!?!?!

52 2012 Focused Guideline Update Jneid et al UA/NSTEMI Focused Update. J Am Coll Cardiol 2011;60:645
53 Adjunctive Antithrombotic Therapy to Support Reperfusion With Primary PCI *The recommended maintenance dose of aspirin to be used with ticagrelor is 81 mg daily. J Am Coll Cardiol. 2013;61(4): doi: /j.jacc

54 Adjunctive Antithrombotic Therapy to Support Reperfusion With Primary PCI (cont.) *The recommended maintenance dose of aspirin to be used with ticagrelor is 81 mg daily. Balloon angioplasty without stent placement may be used in selected patients. It might be reasonable to provide P2Y 12 inhibitor therapy to patients with STEMI undergoing balloon angioplasty alone according to the recommendations listed for BMS. (LOE: C). J Am Coll Cardiol. 2013;61(4): doi: /j.jacc
55 Beta Blockers I IIa IIb III I IIa IIb III Oral beta blockers should be initiated in the first 24 hours in patients with STEMI who do not have any of the following: signs of HF, evidence of a low output state, increased risk for cardiogenic shock,* or other contraindications to use of oral beta blockers (PR interval >0.24 seconds, second- or third-degree heart block, active asthma, or reactive airways disease). Beta blockers should be continued during and after hospitalization for all patients with STEMI and with no contraindications to their use. *Risk factors for cardiogenic shock (the greater the number of risk factors present, the higher the risk of developing cardiogenic shock) are age >70 years, systolic BP <120 mm Hg, sinus tachycardia >110 bpm or heart rate <60 bpm, and increased time since onset of symptoms of STEMI. J Am Coll Cardiol. 2013;61(4): doi: /j.jacc
56 Renin-Angiotensin-Aldosterone System Inhibitors I IIa IIb III An ACE inhibitor should be administered within the first 24 hours to all patients with STEMI with anterior location, HF, or EF less than or equal to 0.40, unless contraindicated. I IIa IIb III An ARB should be given to patients with STEMI who have indications for but are intolerant of ACE inhibitors. J Am Coll Cardiol. 2013;61(4): doi: /j.jacc
57 Lipid Management I IIa IIb III High-intensity statin therapy should be initiated or continued in all patients with STEMI and no contraindications to its use. I IIa IIb III It is reasonable to obtain a fasting lipid profile in patients with STEMI, preferably within 24 hours of presentation. J Am Coll Cardiol. 2013;61(4): doi: /j.jacc
58 Long-Term Medical Therapy and Secondary Prevention-cont. smoking cessation weight management physical activity patient education influenza vaccine depression (Class 2A) hormone replacement therapy (Class 3)

59
Acute Coronary Syndrome. Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine
 Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Acute Coronary Syndrome Cindy Baker, MD FACC Director Peripheral Vascular Interventions Division of Cardiovascular Medicine Topics Timing is everything So many drugs to choose from What s a MINOCA? 2 Acute
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Case Presentation 46 year old
ST Elevation Myocardial Infarction
 ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
ST Elevation Myocardial Infarction Scott M. Lilly, MD, PhD Assistant Professor Clinical Department of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline Case Presentation STEMI
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Guideline for STEMI. Reperfusion at a PCI-Capable Hospital
 MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
MANSOURA. 2015 Guideline for STEMI Reperfusion at a PCI-Capable Hospital Mahmoud Yossof MANSOURA 2015 Reperfusion Therapy for Patients with STEMI *Patients with cardiogenic shock or severe heart failure
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines
 A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction 1
Learning Objectives. Epidemiology of Acute Coronary Syndrome
 Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Cardiovascular Update: Antiplatelet therapy in acute coronary syndromes PHILLIP WEEKS, PHARM.D., BCPS-AQ CARDIOLOGY Learning Objectives Interpret guidelines as they relate to constructing an antiplatelet
Non ST Elevation-ACS. Michael W. Cammarata, MD
 Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
Non ST Elevation-ACS Michael W. Cammarata, MD Case Presentation 65 year old man PMH: CAD s/p stent in 2008 HTN HLD Presents with chest pressure, substernally and radiating to the left arm and jaw, similar
MI MANAGEMENT: ACS Guideline Review. Ben Ochoa BS, RCIS, RCS
 MI MANAGEMENT: ACS Guideline Review en Ochoa S, RCIS, RCS Objectives Discuss management of patients with Non-ST-Elevation Acute Coronary Syndromes. Discuss management of patients with ST-Elevation Acute
MI MANAGEMENT: ACS Guideline Review en Ochoa S, RCIS, RCS Objectives Discuss management of patients with Non-ST-Elevation Acute Coronary Syndromes. Discuss management of patients with ST-Elevation Acute
Acute Coronary Syndromes: Different Continents, Different Guidelines?
 Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes: Different Continents, Different Guidelines? Robert A. Harrington MD, MACC, FAHA, FESC Arthur L. Bloomfield Professor of Medicine Chair, Department of Medicine Stanford University
Acute Coronary Syndromes. January 9, 2013 Chris Chiles M.D. FACC
 Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Acute Coronary Syndromes January 9, 2013 Chris Chiles M.D. FACC Disclosures None- not even a breakfast burrito from a drug company Hospitalizations in the U.S. Due to ACS Acute Coronary Syndromes* 1.57
Timing of Surgery After Percutaneous Coronary Intervention
 Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
Timing of Surgery After Percutaneous Coronary Intervention Deepak Talreja, MD, FACC Bayview/EVMS/Sentara Outline/Highlights Timing of elective surgery What to do with medications Stopping anti-platelet
An update on the management of UA / NSTEMI. Michael H. Crawford, MD
 An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
An update on the management of UA / NSTEMI Michael H. Crawford, MD New ACC/AHA Guidelines 2007 What s s new in the last 5 years CT imaging advances Ascendancy of troponin and BNP Clarification of ACEI/ARB
Acute Coronary Syndrome. Sonny Achtchi, DO
 Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Acute Coronary Syndrome Sonny Achtchi, DO Objectives Understand evidence based and practice based treatments for stabilization and initial management of ACS Become familiar with ACS risk stratification
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI
 Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Tailoring adjunctive antithrombotic therapy to reperfusion strategy in STEMI Adel El-Etriby; MD Professor of Cardiology Ain Shams University President of the Egyptian Working Group of Interventional Cardiology
Acute Coronary syndrome
 Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Acute Coronary syndrome 7th Annual Pharmacotherapy Conference ACS Pathophysiology rupture or erosion of a vulnerable, lipidladen, atherosclerotic coronary plaque, resulting in exposure of circulating blood
Objectives. Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2
 10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
10/2013 1 Objectives Identify early signs and symptoms of Acute Coronary Syndrome Initiate proper protocol for ACS patient 10/2013 2 Purpose of this Education Module: Chest Pain Center Accreditation involves
Acute Myocardial Infarction
 Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Acute Myocardial Infarction Hafeza Shaikh, DO, FACC, RPVI Lourdes Cardiology Services Asst.Program Director, Cardiology Fellowship Associate Professor, ROWAN-SOM Acute Myocardial Infarction Definition:
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC
 Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Cindy Stephens, MSN, ANP Kelly Walker, MS, ACNP Peter Cohn, MD, FACC Define Acute Coronary syndromes Explain the Cause Assessment, diagnosis and therapy Reperfusion for STEMI Complications to look for
Acute Myocardial Infarction. Willis E. Godin D.O., FACC
 Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Acute Myocardial Infarction Willis E. Godin D.O., FACC Acute Myocardial Infarction Definition: Decreased delivery of oxygen and nutrients to the myocardium Myocardial tissue necrosis causing irreparable
Clinical Case. Management of ACS Based on ACC/AHA & ESC Guidelines. Clinical Case 4/22/12. UA/NSTEMI: Definition
 Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
Clinical Case Management of ACS Based on ACC/AHA & ESC Guidelines Dr Badri Paudel Mr M 75M Poorly controlled diabetic Smoker Presented on Sat 7pm Intense burning in the retrosternal area Clinical Case
FastTest. You ve read the book now test yourself
 FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
FastTest You ve read the book...... now test yourself To ensure you have learned the key points that will improve your patient care, read the authors questions below. The answers will refer you back to
STEMI 2014 YAHYA KIWAN. Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital
 STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
STEMI 2014 YAHYA KIWAN Consultant Cardiologist Head Of Cardiology Belhoul Specialty Hospital Aspiration Thrombectomy Manual aspiration thrombectomy is reasonable for patients undergoing primary PCI. I
2010 ACLS Guidelines. Primary goals of therapy for patients
 2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
2010 ACLS Guidelines Part 10: Acute Coronary Syndrome Present : 內科 R1 鍾伯欣 Supervisor: F1 吳亮廷 991110 Primary goals of therapy for patients of ACS Reduce the amount of myocardial necrosis that occurs in
Acute Coronary Syndrome. ACC/AHA 2002 Guidelines
 Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
Acute Coronary Syndrome ACC/AHA 2002 Guidelines ACS Unstable Angina Non ST elevation MI ST elevation MI ACS UA and Non STEMI described in these guidelines Management of STEMI described in separate guidelines
STEMI, Non-STEMI, Chest Pain?
 Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
Minnesota Chest Pain / Acute Coronary Syndrome Tool-Kit Patient with Chest Pain Or Potential Acute Coronary Syndrome STEMI, n-stemi, Chest Pain? Follow MN STEMI Guideline Follow MN n-stemi Guideline Follow
What oral antiplatelet therapy would you choose? a) ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor
 ASA alone b) ASA + Clopidogrel c) ASA + Prasugrel d) ASA + Ticagrelor") 76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
76 year old female Prior Hypertension, Hyperlipidemia, Smoking On Hydrochlorothiazide, Atorvastatin New onset chest discomfort; 2 episodes in past 24 hours Heart rate 122/min; BP 170/92 mm Hg, Killip Class
Appendix: ACC/AHA and ESC practice guidelines
 Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Appendix: ACC/AHA and ESC practice guidelines Definitions for guideline recommendations and level of evidence Recommendation Class I Class IIa Class IIb Class III Level of evidence Level A Level B Level
Management of Acute Myocardial Infarction
 Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
Management of Acute Myocardial Infarction Prof. Hossam Kandil Professor of Cardiology Cairo University ST Elevation Acute Myocardial Infarction Aims Of Management Emergency care (Pre-hospital) Early care
CLINICIAN INTERVIEW RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE. An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA
 RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
RECOGNIZING ACS AND STRATIFYING RISK IN PRIMARY CARE An interview with A. Michael Lincoff, MD, and Eric R. Bates, MD, FACC, FAHA Dr Lincoff is an interventional cardiologist and the Vice Chairman for Research
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA
 Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Case Study 50 YEAR OLD MALE WITH UNSTABLE ANGINA Case History A 50-year-old man with type 1 diabetes mellitus and hypertension presents after experiencing 1 hour of midsternal chest pain that began after
Update on Antithrombotic Therapy in Acute Coronary Syndrome
 Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
Update on Antithrombotic Therapy in Acute Coronary Syndrome Laura Tsang November 13, 2006 Objectives: By the end of this session, you should understand: The role of antithrombotics in ACS Their mechanisms
2014 AHA/ACC Guideline for the Management of Patients With Non ST-Elevation Acute Coronary Syndromes
 2014 AHA/ACC Guideline for the Management of Patients With Non ST-Elevation Acute Coronary Syndromes Developed in Collaboration with the Society of Thoracic Surgeons and Society for Cardiovascular Angiography
2014 AHA/ACC Guideline for the Management of Patients With Non ST-Elevation Acute Coronary Syndromes Developed in Collaboration with the Society of Thoracic Surgeons and Society for Cardiovascular Angiography
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction
 2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
2017 AHA/ACC Clinical Performance and Quality Measures for Adults With ST-Elevation and Non ST-Elevation Myocardial Infarction Ramzi Khalil MD FACC Assistant Professor Allegheny Gen.Hospital AHN Speakers
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
NSTEACS Case Presentation
 NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
NSTEACS Case Presentation Shaul Atar, MD Director of Cardiology Western Galilee Hospital Nahariya Dan Caesrea, 2010 Case Presentation 64 Y. old male HLP, HTN, smoker Prolonged typical CP at rest, multiple
Measuring Natriuretic Peptides in Acute Coronary Syndromes
 Measuring Natriuretic Peptides in Acute Coronary Syndromes Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Consultant Cardiologist Chief Academic and Scientific Officer St. John Providence Health
Measuring Natriuretic Peptides in Acute Coronary Syndromes Peter A. McCullough, MD, MPH, FACC, FACP, FAHA, FCCP Consultant Cardiologist Chief Academic and Scientific Officer St. John Providence Health
Disclosures. Inpatient Management of Non-ST Elevation Acute Coronary Syndromes. Edward McNulty MD, FACC. None
 Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
Inpatient Management of Non-ST Elevation Acute Coronary Syndromes Edward McNulty MD, FACC Assistant Clinical Professor UCSF Director, SF VAMC Cardiac Catheterization Laboratory Disclosures None New Guidelines
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction
 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction Developed in Collaboration with American College of Emergency Physicians and Society for Cardiovascular Angiography and
Acute Coronary Syndrome (ACS) Initial Evaluation and Management
 Initial Evaluation and Management") Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
Acute Coronary Syndrome (ACS) Initial Evaluation and Management Symptoms of Possible ACS Chest discomfort with or without radiation to the arm(s), jaw, or epigastrium Short of breath Weakness Diaphoresis
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Angina Luis Tulloch, MD 03/27/2012
 Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
Angina Luis Tulloch, MD 03/27/2012 Acute coronary syndromes ACS STE > 1 mm, new LBBB* Increased cardiac enzymes STEMI Yes Yes NSTEMI No Yes UA No No *Recognize Wellen s sign/syndrome, posterior wall MI,
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS 9/30/14 TYPICAL WHAT IS ACUTE CORONARY SYNDROME? SYMPTOMS, IDENTIFICATION, MANAGEMENT
 OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
OVERVIEW ACUTE CORONARY SYNDROME SYMPTOMS, IDENTIFICATION, MANAGEMENT OCTOBER 7, 2014 PETE PERAUD, MD SYMPTOMS TYPICAL ATYPICAL IDENTIFICATION EKG CARDIAC BIOMARKERS STEMI VS NON-STEMI VS USA MANAGEMENT
Clopidogrel and ASA after CABG for NSTEMI
 Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
Clopidogrel and ASA after CABG for NSTEMI May 17, 2007 Justin Lee Pharmacy Resident University Health Network Objectives At the end of this session, you should be able to: Explain the rationale for antiplatelet
2018 Acute Coronary Syndrome. Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute
 2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
2018 Acute Coronary Syndrome Robert Bender, DO, FACOI, FACC Central Maine Heart and Vascular Institute Definitions: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation MI (NSTEMI) }2/3 ST-Elevation
Update on STEMI Guidelines. Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center
 Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
Update on STEMI Guidelines Manesh R. Patel, MD Assistant Professor of Medicine Duke University Medical Center All Rights Reserved, Duke Medicine 2008 Disclosures Research Grants: NHLB, AHRQ, AstraZeneca,
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN
 DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
DIFFERENTIATING THE PATIENT WITH UNDIFFERENTIATED CHEST PAIN Objectives Gain competence in evaluating chest pain Recognize features of moderate risk unstable angina Review initial management of UA and
Continuing Medical Education Post-Test
 Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
Continuing Medical Education Post-Test Based on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on
12/18/2009 Resting and Maxi Resting and Max mal Coronary Blood Flow 2
 Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Coronary Artery Pathophysiology ACS / AMI LeRoy E. Rabbani, MD Director, Cardiac Inpatient Services Director, Cardiac Intensive Care Unit Professor of Clinical Medicine Major Determinants of Myocardial
Acute coronary syndromes
 Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Acute coronary syndromes 1 Acute coronary syndromes Acute coronary syndromes results primarily from diminished myocardial blood flow secondary to an occlusive or partially occlusive coronary artery thrombus.
Belinda Green, Cardiologist, SDHB, 2016
 Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
Acute Coronary syndromes All STEMI ALL Non STEMI Unstable angina Belinda Green, Cardiologist, SDHB, 2016 Thrombus in proximal LAD Underlying pathophysiology Be very afraid for your patient Wellens
6/1/18 LEARNING OBJECTIVES PATIENT POPULATION PRESENTATIONS
 PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
PREVENTING HOSPITAL READMISSIONS IN CARDIOVASCULAR PATIENTS Christina Cortez Perry, MSN, FNP-C, CCCC Cardiology Coordinator- Corpus Christi Medical Center 1 2 LEARNING OBJECTIVES Identify the target patient
Chest pain and troponins on the acute take. J N Townend Queen Elizabeth Hospital Birmingham
 Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
Chest pain and troponins on the acute take J N Townend Queen Elizabeth Hospital Birmingham 3 rd Universal Definition of Myocardial Infarction Type 1: Spontaneous MI related to atherosclerotic plaque rupture
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
DISCUSSION QUESTION - 1
 CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
CASE PRESENTATION 87 year old male No past history of diabetes, HTN, dyslipidemia or smoking Very active Medications: omeprazole for heart burn Admitted because of increasing retrosternal chest pressure
Acute Coronary Syndrome
 Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
Acute Coronary Syndrome Vik Gongidi, DO FACOI, FACC Indian River Medical Center Vero Beach, FL Slides adapted from Robert Bender, DO, FACOI, FACC Definition: Acute Myocardial Ischemia Unstable Angina Non-ST-Elevation
ACS and Heart Failure
 ACS and Heart Failure Jonathon Firnhaber, MD, FAAFP Associate Professor The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives Establish the diagnosis and
ACS and Heart Failure Jonathon Firnhaber, MD, FAAFP Associate Professor The Brody School of Medicine at East Carolina University Greenville, North Carolina Learning Objectives Establish the diagnosis and
Otamixaban for non-st-segment elevation acute coronary syndrome
 Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Otamixaban for non-st-segment elevation acute coronary syndrome September 2011 This technology summary is based on information available at the time of research and a limited literature search. It is not
Early Management of Acute Coronary Syndrome
 Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Early Management of Acute Coronary Syndrome Connie Hess, MD, MHS University of Colorado Division of Cardiology Acute Coronary Syndrome (ACS) A range of conditions associated with sudden imbalance in myocardial
Disclosures. Theodore A. Bass MD, FSCAI. The following relationships exist related to this presentation. None
 SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
SCAI Fellows Course December 10, 2013 Disclosures Theodore A. Bass MD, FSCAI The following relationships exist related to this presentation None Current Controversies on DAPT in PCI Which drug? When to
Quinn Capers, IV, MD
 Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Heart Attacks Mended Hearts Presentation, January, 2017 Quinn Capers, IV, MD Associate Professor of Medicine (Cardiovascular Medicine) Director, Transradial Coronary Interventions Division of Cardiovascular
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
10/22/16. Lay of the land. Definition of ACS. Why do we worry about ST elevations?
 Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
Lay of the land Update on Acute Coronary Syndrome: Five Things Hospitalists Must Know Dhruv S. Kazi, MD, MSc, MS Assistant Professor Department of Medicine (Cardiology), Department of Epidemiology and
The PAIN Pathway for the Management of Acute Coronary Syndrome
 2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
2 The PAIN Pathway for the Management of Acute Coronary Syndrome Eyal Herzog, Emad Aziz, and Mun K. Hong Acute coronary syndrome (ACS) subsumes a spectrum of clinical entities, ranging from unstable angina
Preoperative Cardiac Risk Assessment: Approach & Guidelines
 Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
Preoperative Cardiac Risk Assessment: Approach & Guidelines By, Liam Morris, MD., FACC (02/03/18) CPG : Clinical Practice Guidelines GDMT : Guidelines Directed Medical Therapy GWC : Guideline Writing Committee
INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies.
 INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies. José G. Díez, MD, FACC, FSCAI Associate Professor of Medicine, Baylor College of Medicine Hall Garcia
INNOVATIONS 2017: Acute Coronary Syndrome Antiplatelet Therapies in Medical and Invasive Strategies. José G. Díez, MD, FACC, FSCAI Associate Professor of Medicine, Baylor College of Medicine Hall Garcia
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy
 Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
Recognizing the High Risk NSTEMI Patient for Early Appropriate Therapy Learning Objectives Learn to recognize the high risk patient Discuss effective management of a high risk NSTEMI patient Review CCS
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle
 Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle") ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) Gordon Kritzer, MD, FACC Virginia Mason Medical Center, Seattle STEMI ACS and STEMI History and physical, differential diagnosis ECGs Initial Therapy and management
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής. Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά
 Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Διάρκεια διπλής αντιαιμοπεταλιακής αγωγής Νικόλαος Γ.Πατσουράκος Καρδιολόγος, Επιμελητής Α ΕΣΥ Τζάνειο Γενικό Νοσοκομείο Πειραιά International ACS guidelines: Recommendations on duration of dual
Prehospital and Hospital Care of Acute Coronary Syndrome
 Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
Ischemic Heart Diseases Prehospital and Hospital Care of Acute Coronary Syndrome JMAJ 46(8): 339 346, 2003 Katsuo KANMATSUSE* and Ikuyoshi WATANABE** * Professor, Second Internal Medicine, Nihon University,
STEMI Presentation and Case Discussion. Case #1
 STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
STEMI Presentation and Case Discussion Scott M Lilly MD PhD, Interventional Cardiology The Ohio State University Contemporary Multidisciplinary Cardiovascular Conference Orlando, Florida September 17 th,
Adjunctive Antithrombotic for PCI. SCAI Fellows Course December 9, 2013
 Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Adjunctive Antithrombotic for PCI SCAI Fellows Course December 9, 2013 Theodore A Bass, MD FSCAI President SCAI Professor of Medicine, University of Florida Medical Director UF Shands CV Center,Jacksonville
Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines)
") Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
Cardiovascular Health Nova Scotia Guideline Update Nova Scotia Guidelines for Acute Coronary Syndromes (Updating the 2008 Antiplatelet Section of the Guidelines) Authors: Dr. M. Love, Dr. I. Bata, K. Harrigan
QUT Digital Repository:
 QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
QUT Digital Repository: http://eprints.qut.edu.au/ This is the author s version of this journal article. Published as: Doggrell, Sheila (2010) New drugs for the treatment of coronary artery syndromes.
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI
 The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
The Future of Oral Antiplatelets in PAD and CAD Christopher Paris, MD, FACC, FSCAI Interventional Cardiologist Cardiovascular Institute of the South Director of Cardiovascular Services St. Charles Parish
STEMI update. Vijay Krishnamoorthy M.D. Interventional Cardiology
 STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
STEMI update Vijay Krishnamoorthy M.D. Interventional Cardiology OVERVIEW Current Standard of Care in Management of STEMI Update in management of STEMI Pre-Cath Lab In the ED/Office/EMS. Cath Lab Post
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015
 Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Cangrelor: Is it the new CHAMPION for PCI? Robert Barcelona, PharmD, BCPS Clinical Pharmacy Specialist, Cardiac Intensive Care Unit November 13, 2015 Objectives Review the pharmacology and pharmacokinetic
Risk Stratification of ACS Patients. Frans Van de Werf, MD, PhD University of Leuven, Belgium
 Risk Stratification of ACS Patients Frans Van de Werf, MD, PhD University of Leuven, Belgium Which type of ACS patients are we talking about to day? 4/14/2011 STEMI and NSTEMI in the NRMI registry from
Risk Stratification of ACS Patients Frans Van de Werf, MD, PhD University of Leuven, Belgium Which type of ACS patients are we talking about to day? 4/14/2011 STEMI and NSTEMI in the NRMI registry from
Diagnosis and Management of Acute Myocardial Infarction
 Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Diagnosis and Management of Acute Myocardial Infarction Acute Myocardial Infarction (AMI) occurs as a result of prolonged myocardial ischemia Atherosclerosis leads to endothelial rupture or erosion that
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics
 Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
Managing Quality of ACS Care in VHA The IDH Guideline Key Points and Metrics Robert L. Jesse, MD, PhD National Program Director for Cardiology Veterans Health Administration Washington, DC Chief, Cardiology
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Essam Mahfouz, MD. Professor of Cardiology, Mansoura University
 By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
By Essam Mahfouz, MD. Professor of Cardiology, Mansoura University Agenda Definitions Classifications Epidemiology Risk stratification What is new? What is MI? Myocardial infarction is the death of part
Acute Coronary Syndrome (ACS): Disease Management. Acute Coronary Syndrome (ACS)
: Disease Management. Acute Coronary Syndrome (ACS)") Acute Coronary Syndrome (ACS): Disease Management Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com 2009 1 Acute Coronary Syndrome (ACS) ST Elevation STEMI No ST Elevation NSTEMI Unstable
Acute Coronary Syndrome (ACS): Disease Management Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com 2009 1 Acute Coronary Syndrome (ACS) ST Elevation STEMI No ST Elevation NSTEMI Unstable
The Window for Fibrinolysis. Frans Van de Werf, MD, PhD Leuven, Belgium
 The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
The Window for Fibrinolysis Frans Van de Werf, MD, PhD Leuven, Belgium ESC STEMI Guidelines : December 2008 Reperfusion Therapy: Fibrinolytic Therapy Recommendations Class LOE In the absence of contraindications
10 Steps to Managing Non-ST Elevation ACS
 Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Pathophysiology of Acute Coronary Syndromes and Potential Pharmacologic Interventions Acute Coronary Syndrome 4. Downstream from thrombus myocardial ischemia/necrosis (Beta-blockers, Nitrates etc) 3. Activation
Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network
 Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
Torino 6 Joint meeting with Mayo Clinic Great Innovation in Cardiology 14-15 Ottobre 2010 Optimal antiplatelet and anticoagulant therapy for patients treated in STEMI network Diego Ardissino Ischemic vs
2/17/2010. Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco
 Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
Modern Management of Patients with Stable Coronary Artery Disease Grace Lin, MD Assistant Professor of Medicine University of California, San Francisco Scope of the Problem Prevalence of CAD: 17.6 million
M/39 CC D. => peak CKMB (12 hr later) ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #
 ng/ml T.chol/TG/HDL/LDL 180/150/48/102 mg/dl #") Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Acute Coronary Syndrome - Case Review - Young-Guk Ko, MD Yonsei Cardiovascular Center Yonsei University College of Medicine Case 1 M/39 #4306212 CC D : Severe squeezing chest pain : 4 hours, aggravated
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina
 Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
Medicine Dr. Omed Lecture 2 Stable and Unstable Angina Risk stratification in stable angina. High Risk; *post infarct angina, *poor effort tolerance, *ischemia at low workload, *left main or three vessel
ACCP Cardiology PRN Journal Club
 ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
ACCP Cardiology PRN Journal Club 1 Optimising Crossover from Ticagrelor to Clopidogrel in Patients with Acute Coronary Syndrome [CAPITAL OPTI-CROSS] Monique Conway, PharmD, BCPS PGY-2 Cardiology Pharmacy
Therapies for ACS The Articles You ve Got to Know!!
 Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Therapies for ACS The Articles You ve Got to Know!! Amal Mattu, MD, FAAEM, FACEP Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine Baltimore, Maryland
Acute Coronary Syndrome
 Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Acute Coronary Syndrome Clinical Manifestation of CAD Silent Ischemia/asymptomatic Stable Angina Acute Coronary Syndrome (Non- STEMI/UA and STEMI) Arrhythmias Heart Failure Sudden Death Pain patterns with
Results of Ischemic Heart Disease
 Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
Ischemic Heart Disease: Angina and Myocardial Infarction Ischemic heart disease; syndromes causing an imbalance between myocardial oxygen demand and supply (inadequate myocardial blood flow) related to
CABG Surgery following STEMI
 CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction:
CABG Surgery following STEMI Susana Harrington, MS,APRN-NP Cardio-Thoracic Surgery Nebraska Methodist Hospital February 15, 2018 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: