DECLARATION OF CONFLICT OF INTEREST
|
|
|
- Sara Hunt
- 6 years ago
- Views:
Transcription
1 DECLARATION OF CONFLICT OF INTEREST
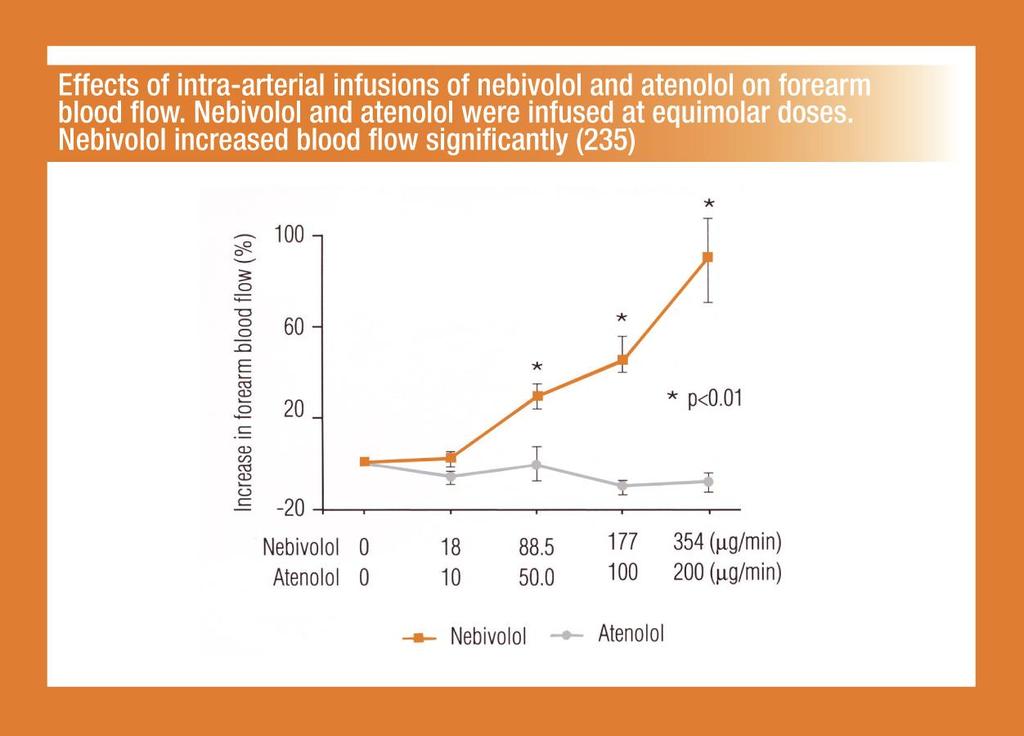
2 Third generation beta-blockers in the treatment of arterial hypertension Kurt Stoschitzky, MD, FESC Division of Cardiology Department of Internal Medicine Medical University, Graz, Austria
3 2007 ESC Guidelines for the management of arterial hypertension Because beta-blockers. have adverse effects on lipid metabolism and increase. the incidence of new onset diabetes they should not be preferred in hypertensives with multiple metabolic risk factors
4 2007 ESC Guidelines for the management of arterial hypertension Because beta-blockers. have adverse effects on lipid metabolism and increase. the incidence of new onset diabetes they should not be preferred in hypertensives with multiple metabolic risk factors It may not apply, however, to vasodilator beta-blockers, such as carvedilol and nebivolol, which have less or no dysmetabolic action as well as a reduced incidence of new onset diabetes compared with classical beta-blockers
5 The three generations of beta-blockers 1 st generation non-selective (Propranolol, Sotalol) 2 nd generation beta 1 -selective ( cardioselective ) (Atenolol, Metoprolol, Bisoprolol) 3 rd generation additional vasodilating effects (Carvedilol, Nebivolol, Labetalol)
6 Carvedilol Beta 1 + Beta 2 + Alpha blockade Predominantly oral administration
7 Carvedilol Beta 1 + Beta 2 + Alpha blockade Predominantly oral administration Nebivolol Beta 1 blockade + NO mediated vasodilation Predominantly oral administration
8 Carvedilol Beta 1 + Beta 2 + Alpha blockade Predominantly oral administration Nebivolol Beta 1 blockade + NO mediated vasodilation Predominantly oral administration Labetalol Beta 1 + Beta 2 + Alpha blockade Predominantly intravenous administration
9 General side effects of beta-blockers Bradycardia AV-block Heart failure Bronchospasm Peripheral vasoconstriction Increase of plasma glucose Increase of plasma lipids Erectile dysfunction Sleep disturbances (melatonin )
10 Atenolol in hypertension: Is it a wise choice? Our results cast doubts on atenolol as a suitable drug for hypertensive patients. Moreover, they challenge the use of atenolol as a reference drug in outcome trials in hypertension (Atenolol was used as a reference drug in the following outcome trials in hypertension: HEP 1986, HAPPHY 1989, STOP 1991, MRC 1992, TEST 1995, UKPDS 1998, STOP , NORDIL 2000, LIFE 2002, ELSA 2002, INVEST 2003, CONVINCE 2003, ASCOT 2005) Lancet 2004; 364:
11 Results of studies with Beta-Blockers versus other Antihypertenives Lancet 2005; 366:
12 Results of studies with Beta-Blockers without Atenolol versus other Antihypertenives Lancet 2005; 366:
13 Carvedilol Advantages: Additional α-blockade
14 Carvedilol Advantages: Additional α-blockade more blood pressure
15 Carvedilol Advantages: Additional α-blockade more blood pressure less heart rate (advantage?)
16 Carvedilol Advantages: Additional α-blockade more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose
17 Carvedilol Advantages: Additional α-blockade more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose Disadvantages: No β 1 -selectivity
18 Carvedilol Advantages: Additional α-blockade more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose Disadvantages: No β 1 -selectivity bronchospasms
19 Carvedilol Advantages: Additional α-blockade more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose Disadvantages: No β 1 -selectivity bronchospasms Dosing twice daily
20 Carvedilol Advantages: Additional α-blockade more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose Disadvantages: No β 1 -selectivity bronchospasms Dosing twice daily No large outcome trials in arterial hypertension
21 Heart rate (beats/min) * * * * * * * * 0 Placebo 25mg 50mg 100mg Carvedilol 50mg 100mg 200mg Metoprolol 2,5mg 5mg 10mg Bisoprolol Different effects on resting heart rate of increasing single oral doses of Carvedilol, Metoprolol und Bisoprolol (*, p < 0.05)
22 % Carvedilol Atenolol Atenolol Insulin- Sensitivitäts- Index Triglyceride im Plasma Carvedilol In patients with arterial hypertension and diabetes mellitus II the Insuline Sensitivity Index was decrased by Atenolol (-24%, p < 0.01) but increased by Carvedilol (+27%, p < 0.01); at the same time plasma concentrations of triglycerides were increased by Atenolol (+12%, p < 0.01) but decreased by Carvedilol (-20%, p < 0.01) Ann Intern Med 1997; 126:
23 Nebivolol Advantages: Vasodilation by an additional nitrate effect
24 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity
25 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure
26 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?)
27 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose
28 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose no erectile dysfunction
29 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose no erectile dysfunction Disadvantages: Rather weak beta-blockade
30 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose no erectile dysfunction Disadvantages: Rather weak beta-blockade No large outcome trials in arterial hypertension
31 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose no erectile dysfunction Disadvantages: Rather weak beta-blockade No large outcome trials in arterial hypertension Additional indication only in the elderly with heart failure
32 Nebivolol Advantages: Vasodilation by an additional nitrate effect highest β 1 -selectivity more blood pressure less heart rate (advantage?) no plasma levels of lipids and glucose no erectile dysfunction Disadvantages: Rather weak beta-blockade No large outcome trials in arterial hypertension Additional indication only in the elderly with heart failure Actually no indication in CAD
33
34
35 No influence of Nebivolol on FEV FEV Placebo Nebivolol t 0 t 1 t 3 t 6 t 12 t 24 (time = 1 / 3 / 6 / 12 / 24 hours) R.W.Dal Negro, et al., Clin Drug Invest 2002; 22 (3):
36 Forearm blood flow (ml / min / 100 g) p < 0.05 p < Before After iv Nitroglycerin with Placebo Before After iv Nitroglycerin with Nebivolol Increase of forearm blood flow (FBF) by iv administration of 0,4 mg/min Nitroglycerine following one week of daily intake of Placebo or 5mg Nebivolol: FBF increased significantly with Nebivolol (+96%) and more effectively (p < 0.05) than with Placebo (+54%) No nitrate tolerance with Nebivolol
37 ng/ml 280 Propranolol p < 0.01 p < 0.01 ng/ml Atenolol p < 0.01 p < 0.01 ng/ml 12 Bisoprolol p < 0.01 p < 0.01 Plasma concentrations 200 Plasma concentrations Plasma concentrations Rest Exercise Recovery Rest Exercise Recovery Rest Exercise Recovery Effects of exercise on plasma concentrations of beta-blockers
38 ng/ml 280 Propranolol p < 0.01 p < 0.01 ng/ml Atenolol p < 0.01 p < 0.01 ng/ml 12 Bisoprolol p < 0.01 p < 0.01 Plasma concentrations 200 Plasma concentrations Plasma concentrations Rest Exercise Recovery Rest Exercise Recovery Rest Exercise Recovery ng/ml 24 Plasma concentrations n.s. Carvedilol n.s. Plasma concentrations ng/ml 0,30 0,25 n.s. Nebivolol n.s Rest Exercise Recovery 0,00 Rest Exercise Recovery Effects of exercise on plasma concentrations of beta-blockers
39 30 n.s. n.s. amt6s in nocturnal urine (mg) * 5 0 Placebo Bisoprolol Carvedilol Nebivolol Influence of Bisoprolol, Carvedilol and Nebivolol on nocturnal melatonine release: Compared to Placebo, Bisoprolol decreased nocturnal melatonine release by 36 % (* p < 0.05) whereas Carvedilol und Nebivolol showed no effects (n.s.)
40 Labetalol Beta 1 + Beta 2 + Alpha blockade
41 Labetalol Beta 1 + Beta 2 + Alpha blockade predominantly intravenous administration
42 Labetalol Beta 1 + Beta 2 + Alpha blockade predominantly intravenous administration hypertensive emergencies, particularly in
43 Labetalol Beta 1 + Beta 2 + Alpha blockade predominantly intravenous administration hypertensive emergencies, particularly in phaeochromocytoma
44 Labetalol Beta 1 + Beta 2 + Alpha blockade predominantly intravenous administration hypertensive emergencies, particularly in phaeochromocytoma pre-eclampsia
45 Labetalol Beta 1 + Beta 2 + Alpha blockade predominantly intravenous administration hypertensive emergencies, particularly in phaeochromocytoma pre-eclampsia 20mg 3mg/kgBW
46 Labetalol Advantages: Additional α-blockade
47 Labetalol Advantages: Additional α-blockade The most effective beta-blocker in hypertensive emergencies
48 Labetalol Advantages: Additional α-blockade The most effective beta-blocker in hypertensive emergencies more blood pressure
49 Labetalol Advantages: Additional α-blockade The most effective beta-blocker in hypertensive emergencies more blood pressure less heart rate (advantage?)
50 Labetalol Advantages: Additional α-blockade The most effective beta-blocker in hypertensive emergencies more blood pressure less heart rate (advantage?) Disadvantages: No β 1 -selectivity
51 Labetalol Advantages: Additional α-blockade The most effective beta-blocker in hypertensive emergencies more blood pressure less heart rate (advantage?) Disadvantages: No β 1 -selectivity bronchospasms
52 Labetalol Advantages: Additional α-blockade The most effective beta-blocker in hypertensive emergencies more blood pressure less heart rate (advantage?) Disadvantages: No β 1 -selectivity bronchospasms No large outcome trials in arterial hypertension
53 Conclusions The three generations of beta-blockers are not equal
54 Conclusions The three generations of beta-blockers are not equal Third generation beta-blockers show more decrease of blood pressure
55 Conclusions The three generations of beta-blockers are not equal Third generation beta-blockers show more decrease of blood pressure less/no increase of plasma glucose
56 Conclusions The three generations of beta-blockers are not equal Third generation beta-blockers show more decrease of blood pressure less/no increase of plasma glucose less/no increase of plasma lipids
57 Conclusions The three generations of beta-blockers are not equal Third generation beta-blockers show more decrease of blood pressure less/no increase of plasma glucose less/no increase of plasma lipids less/no decrease of nocturnal melatonin
58 Conclusions The three generations of beta-blockers are not equal Third generation beta-blockers show more decrease of blood pressure less/no increase of plasma glucose less/no increase of plasma lipids less/no decrease of nocturnal melatonin no increase of plasma concentrations by exercise
59 Conclusions The three generations of beta-blockers are not equal Third generation beta-blockers show more decrease of blood pressure less/no increase of plasma glucose less/no increase of plasma lipids less/no decrease of nocturnal melatonin no increase of plasma concentrations by exercise Large clinical studies showing effects on morbidity and mortality are missing
60 Thank you very much for your attention!

61 Haemodynamic effects of beta-blockers Blood pressure Cardiac output Peripheral resistance Heart rate
62 Beta-blockers and erectile dysfunction Eur Heart J 2003; 24: males (age 52 ± 7 years) with CAD (60 %) or arterial hypertension (40 %) with no contraindications for beta-blockers and without erectile dysfunction (ED) received 50 mg Atenolol once daily over three months They were divided in 3 groups (32 patients each) as follows: Groupe 1 was blinded, i.e., patients did not know what they received Groupe 2 was informed about the substance but not about ED as a potential side effect Groupe 3 was informed about the substance and about ED as a potential side effect

63 Beta-blockers and erectile dysfunction Eur Heart J 2003; 24:
64 Beta-blockers and erectile dysfunction Eur Heart J 2003; 24: Patients who reported ED as a side effect received in a 2 nd phase 50 mg Sildenafil (Viagra ) or Placebo according to a double-blind, cross-over, placebo-controlled protocol with ongoing treatment with 50 mg Atenolol once daily in order to use it at least three times

65 Beta-blockers and erectile dysfunction Eur Heart J 2003; 24:
β adrenergic blockade, a renal perspective Prof S O McLigeyo
 β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS)
") DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
DRUG CLASSES BETA-ADRENOCEPTOR ANTAGONISTS (BETA-BLOCKERS) Beta-blockers have been widely used in the management of angina, certain tachyarrhythmias and heart failure, as well as in hypertension. Examples
Dr. Vishaal Bhat. anti-adrenergic drugs
 Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Dr. Vishaal Bhat anti-adrenergic drugs Divisions of human nervous system Human Nervous system Central Nervous System Peripheral Nervous System Autonomic Nervous System Nervous system Includes neurons and
Adrenergic Receptor as part of ANS
 Adrenergic Receptor as part of ANS Actions of Adrenoceptors Beta-1 adrenergic receptor Located on the myocytes of the heart Specific actions of the β1 receptor include: 0 Increase cardiac output, by 0
Adrenergic Receptor as part of ANS Actions of Adrenoceptors Beta-1 adrenergic receptor Located on the myocytes of the heart Specific actions of the β1 receptor include: 0 Increase cardiac output, by 0
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Beta blockers in primary hypertension. Dr. Md. Billal Alam Associate Professor of Medicine DMC
 Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Beta blockers in primary hypertension Dr. Md. Billal Alam Associate Professor of Medicine DMC Development of antihypertensive drugs Beta blockers 1958 - The first beta-blocker, dichloroisoproterenol, was
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?
 Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Metabolic Consequences of Anti Hypertensives: Is It Clinically Important?,FACA,FICA,MASH,FVBWG,MISCP CONSULTANT OF CARDIOLOGY DIRECTOR OF PORT-FOUAD HOSPITAL CCU Consideration of antihypertensive agents
Should beta blockers remain first-line drugs for hypertension?
 1 de 6 03/11/2008 13:23 Should beta blockers remain first-line drugs for hypertension? Maros Elsik, Cardiologist, Department of Epidemiology and Preventive Medicine, Monash University and The Alfred Hospital,
1 de 6 03/11/2008 13:23 Should beta blockers remain first-line drugs for hypertension? Maros Elsik, Cardiologist, Department of Epidemiology and Preventive Medicine, Monash University and The Alfred Hospital,
Core Safety Profile. Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg. Date of FAR:
/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg. Date of FAR:") Core Safety Profile Active substance: Bisoprolol Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg P - RMS: FI/H/PSUR/0002/002 Date of FAR: 13.12.2011
Core Safety Profile Active substance: Bisoprolol Pharmaceutical form(s)/strength: Film-coated tablets 1.25 mg, 2.5 mg, 3.75 mg, 5 mg, 7.5 mg and 10 mg P - RMS: FI/H/PSUR/0002/002 Date of FAR: 13.12.2011
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Beta-blockers in heart failure: evidence put into practice
 Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Inventory of paediatric therapeutic needs
 24 April 2013 EMA/PDCO/246339/2013 Human Medicines Development and Evaluation Cardiovascular therapeutic area Agreed by PDCO August 2012 Adopted by PDCO for release for consultation 15-17 August 2012 Start
24 April 2013 EMA/PDCO/246339/2013 Human Medicines Development and Evaluation Cardiovascular therapeutic area Agreed by PDCO August 2012 Adopted by PDCO for release for consultation 15-17 August 2012 Start
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Prof. Ramzy H. El Mawardy. Cairo Egypt 2009
 Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
CKD Satellite Symposium
 CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
CKD Satellite Symposium Recommended Therapy by Heart Failure Stage AHA/ACC Task Force on Practice Guideline 2001 Natural History of Heart Failure Patients surviving % Mechanism of death Sudden death 40%
Role of Sympathetic Nervous System in Hypertension
 Role of Sympathetic Nervous System in Hypertension BP = CO x PVR SV HR DEFENSE REACTION Suppressed vagal activity Increased sympathetic activity to heart, veins, kidneys, splachnic region, skin Skeletal
Role of Sympathetic Nervous System in Hypertension BP = CO x PVR SV HR DEFENSE REACTION Suppressed vagal activity Increased sympathetic activity to heart, veins, kidneys, splachnic region, skin Skeletal
B-blockers. Effects not related to Beta-Blockade
 B-blockers Effects not related to Beta-Blockade It has been suggested that some intrinsic sympathomimetic activity is desirable to prevent untoward effects such as asthma or excessive bradycardia. Pindolol
B-blockers Effects not related to Beta-Blockade It has been suggested that some intrinsic sympathomimetic activity is desirable to prevent untoward effects such as asthma or excessive bradycardia. Pindolol
sympathetic nerve impulses endogenous catecholamines beta adrenergic drugs
 Beta adrenergic blockers } These drugs will bind and prevent beta-receptors from responding to: sympathetic nerve impulses endogenous catecholamines beta adrenergic drugs the use of beta antagonists is
Beta adrenergic blockers } These drugs will bind and prevent beta-receptors from responding to: sympathetic nerve impulses endogenous catecholamines beta adrenergic drugs the use of beta antagonists is
Angina Pectoris Dr. Shariq Syed
 Angina Pectoris Dr. Syed 1 What is Angina Pectoris (AP)? Commonly known as angina is chest pain often due to ischemia of the heart muscle, Because of obstruction or spasm of the coronary arteries 2 What
Angina Pectoris Dr. Syed 1 What is Angina Pectoris (AP)? Commonly known as angina is chest pain often due to ischemia of the heart muscle, Because of obstruction or spasm of the coronary arteries 2 What
PERSISTENCE OF BETA BLOCKER TREATMENT AFTER A HEART ATTACK
 PERSISTENCE OF BETA BLOCKER TREATMENT AFTER A HEART ATTACK APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? HEDIS (Administrative) NCQA Accreditation (Medicare
PERSISTENCE OF BETA BLOCKER TREATMENT AFTER A HEART ATTACK APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? HEDIS (Administrative) NCQA Accreditation (Medicare
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Autonomic Pharmacology
 Autonomic Pharmacology ADRENERGIC RECEPTOR BLOCKERS Adrenergic-receptor antagonists block the effects of sympathetic stimulation and adrenergic agonists mediated through - and -receptors. Adrenergic receptor
Autonomic Pharmacology ADRENERGIC RECEPTOR BLOCKERS Adrenergic-receptor antagonists block the effects of sympathetic stimulation and adrenergic agonists mediated through - and -receptors. Adrenergic receptor
Pharmacology of the Sympathetic Nervous System II
 Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Pharmacology of the Sympathetic Nervous System II Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia
Use of Beta-blocker Monotherapy in Hypertension: Situation in a Local General Outpatient Clinic
 Use of Beta-blocker Monotherapy in Hypertension: Situation in a Local General Outpatient Clinic Dr. Dao Man Chi Resident Department of Family Medicine and Primary Health Care, KWC HA Convention 2014 Introduction
Use of Beta-blocker Monotherapy in Hypertension: Situation in a Local General Outpatient Clinic Dr. Dao Man Chi Resident Department of Family Medicine and Primary Health Care, KWC HA Convention 2014 Introduction
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
11/4/2017. but cocaine toxicity is complex: Pro thrombotic effects Progressive atherosclerosis Ventricular remodeling
 2 Learning Objectives ATRIUM Fall Patient Safety Webinar Cardiology Mythbusters: Vol 1 Brent N. Reed, PharmD, BCPS AQ Cardiology Associate Professor, University of Maryland School of Pharmacy This presentation
2 Learning Objectives ATRIUM Fall Patient Safety Webinar Cardiology Mythbusters: Vol 1 Brent N. Reed, PharmD, BCPS AQ Cardiology Associate Professor, University of Maryland School of Pharmacy This presentation
Heart failure. Complex clinical syndrome. Estimated prevalence of ~2.4% (NHANES)
") Heart failure Complex clinical syndrome caused by any structural or functional impairment of ventricular filling or ejection of blood Estimated prevalence of ~2.4% (NHANES) Etiology Generally divided into
Heart failure Complex clinical syndrome caused by any structural or functional impairment of ventricular filling or ejection of blood Estimated prevalence of ~2.4% (NHANES) Etiology Generally divided into
Cost effectiveness of beta blocker therapy for patients. with chronic severe heart failure. in Ireland. M. Barry
 IMJ June 2002;95(6):174-177 Cost effectiveness of beta blocker therapy for patients with chronic severe heart failure in Ireland M. Barry Irish National Centre for Pharmacoeconomics Address for correspondence
IMJ June 2002;95(6):174-177 Cost effectiveness of beta blocker therapy for patients with chronic severe heart failure in Ireland M. Barry Irish National Centre for Pharmacoeconomics Address for correspondence
Management of the coronary patient in Roberto Ferrari
 Management of the coronary patient in 2011 Roberto Ferrari What is new in treatment of stable CAD? In the era of interventional cardiology, is chronic stable angina a rare disease? Stable angina pectoris
Management of the coronary patient in 2011 Roberto Ferrari What is new in treatment of stable CAD? In the era of interventional cardiology, is chronic stable angina a rare disease? Stable angina pectoris
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Chapter 10. Learning Objectives. Learning Objectives 9/11/2012. Congestive Heart Failure
 Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Chapter 10 Congestive Heart Failure Learning Objectives Explain concept of polypharmacy in treatment of congestive heart failure Explain function of diuretics Learning Objectives Discuss drugs used for
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Heart rate lowering treatment in chronic heart failure
 Heart rate lowering treatment in chronic heart failure Jaromir Hradec 3rd Dept. Med., Charles Univ., Prague Czech Republic Things we knew, things we did Things we have learnt, things we should do What
Heart rate lowering treatment in chronic heart failure Jaromir Hradec 3rd Dept. Med., Charles Univ., Prague Czech Republic Things we knew, things we did Things we have learnt, things we should do What
Antihypertensive Agents
 Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Antihypertensive Agents Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 7, 08, presented by Ezra Levy, Pharm.D! Usual Dose,
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Supplementary Online Content
 Supplementary Online Content Jørgensen ME, Hlatky MA, Køber L, et al. β-blocker associated risks in patients with uncomplicated hypertension undergoing noncardiac surgery. JAMA Intern Med. Published online
Supplementary Online Content Jørgensen ME, Hlatky MA, Køber L, et al. β-blocker associated risks in patients with uncomplicated hypertension undergoing noncardiac surgery. JAMA Intern Med. Published online
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Effects of felodipine on haemodynamics and exercise capacity in patients with angina pectoris
 Br. J. clin. Pharmac. (1987), 23, 391-396 Effects of felodipine on haemodynamics and exercise capacity in patients with angina pectoris J. V. SHERIDAN, P. THOMAS, P. A. ROUTLEDGE & D. J. SHERIDAN Departments
Br. J. clin. Pharmac. (1987), 23, 391-396 Effects of felodipine on haemodynamics and exercise capacity in patients with angina pectoris J. V. SHERIDAN, P. THOMAS, P. A. ROUTLEDGE & D. J. SHERIDAN Departments
The Hearth Rate modulators. How to optimise treatment
 The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Treatment of Stable Coronary Artery Disease Pharmacotherapy
 Treatment of Stable Coronary Artery Disease Pharmacotherapy José López-Sendón Hospital Universitario La Paz. Madrid. Spain Conflict of interest: I will discuss off label use and/or investigational use
Treatment of Stable Coronary Artery Disease Pharmacotherapy José López-Sendón Hospital Universitario La Paz. Madrid. Spain Conflict of interest: I will discuss off label use and/or investigational use
New approaches to the uses of beta blocking drugs in hypertension
 (2000) 14, Suppl 1, S63 S68 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh New approaches to the uses of beta blocking drugs in hypertension BNC Prichard 1, BR
(2000) 14, Suppl 1, S63 S68 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh New approaches to the uses of beta blocking drugs in hypertension BNC Prichard 1, BR
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Elements for a public summary
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology High blood pressure, also known as hypertension, occurs in a large percentage of the adult population. Primary (essential) hypertension
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology High blood pressure, also known as hypertension, occurs in a large percentage of the adult population. Primary (essential) hypertension
Drug Class Review on Beta Adrenergic Blockers
 Drug Class Review on Beta Adrenergic Blockers Final Report May 2005 The purpose of this report is to make available information regarding the comparative effectiveness and safety profiles of different
Drug Class Review on Beta Adrenergic Blockers Final Report May 2005 The purpose of this report is to make available information regarding the comparative effectiveness and safety profiles of different
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Α Reapraisal on the Use of β-blockers
 Α Reapraisal on the Use of β-blockers Athanasios J. Manolis MD, FACC, FESC, FAHA Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece. Adj. Ass. Professor, Hypertension Section, Boston
Α Reapraisal on the Use of β-blockers Athanasios J. Manolis MD, FACC, FESC, FAHA Director of Cardiology Dept, Asklepeion General Hospital, Athens Greece. Adj. Ass. Professor, Hypertension Section, Boston
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Dr Noryani Mohd Samat
 Dr Noryani Mohd Samat CONTENT Sepsis pathophysiology revisit Rationale of beta blockers influencing sepsis s course Evidence so far Conclusion Sepsis still contributes to high morbidity & mortality Efforts
Dr Noryani Mohd Samat CONTENT Sepsis pathophysiology revisit Rationale of beta blockers influencing sepsis s course Evidence so far Conclusion Sepsis still contributes to high morbidity & mortality Efforts
Declaration of conflict of interest
 Declaration of conflict of interest Claudio Borghi Lectures fees: Menarini International, Servier International, Recordati International, Ely-Lilly USA, BMS, Boheringer Ingelheim, Novartis Pharma Research
Declaration of conflict of interest Claudio Borghi Lectures fees: Menarini International, Servier International, Recordati International, Ely-Lilly USA, BMS, Boheringer Ingelheim, Novartis Pharma Research
Semilogarithmic relation between rest heart rate and life expectancy
 The importance of heart rate in heart failure Karl Swedberg Professor of Medicine Department t of emergency and cardiovascular medicine i Sahlgrenska Academy University of Gothenburg, Sweden karl.swedberg@gu.se
The importance of heart rate in heart failure Karl Swedberg Professor of Medicine Department t of emergency and cardiovascular medicine i Sahlgrenska Academy University of Gothenburg, Sweden karl.swedberg@gu.se
Perioperative β blockers in patients having non-cardiac surgery: a meta-analysis
 Perioperative β blockers in patients having non-cardiac surgery: a meta-analysis Sripal Bangalore, Jørn Wetterslev, Shruthi Pranesh, Sabrina Sawhney, Christian Gluud, Franz H Messerli Summary Background
Perioperative β blockers in patients having non-cardiac surgery: a meta-analysis Sripal Bangalore, Jørn Wetterslev, Shruthi Pranesh, Sabrina Sawhney, Christian Gluud, Franz H Messerli Summary Background
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4)
 and The International Polycap Study 3 & 4 (TIPS 3 & 4)") The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
The Indian Polycap Study 1 & 2 (TIPS 1 & 2) and The International Polycap Study 3 & 4 (TIPS 3 & 4) Denis Xavier MD, MSc Professor and Head, Pharmacology, St. John's Medical College Coordinator, Division
Beta-blockers for hypertension(review)
") Cochrane Database of Systematic Reviews Beta-blockers for hypertension(review) WiysongeCS,BradleyHA,VolminkJ,MayosiBM,OpieLH Wiysonge CS, Bradley HA, Volmink J, Mayosi BM, Opie LH. Beta-blockers for hypertension.
Cochrane Database of Systematic Reviews Beta-blockers for hypertension(review) WiysongeCS,BradleyHA,VolminkJ,MayosiBM,OpieLH Wiysonge CS, Bradley HA, Volmink J, Mayosi BM, Opie LH. Beta-blockers for hypertension.
BETA-BLOCKERS IN CIRRHOSIS.PRO.
 BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
BETA-BLOCKERS IN CIRRHOSIS.PRO. Angela Puente Sánchez. MD PhD Hepatology Unit. Gastroenterology department Marques de Valdecilla University Hospital. Santander INTRODUCTION. Natural history of cirrhosis
Evidence Supporting Post-MI Use of
 Addressing the Gap in the Management of Patients After Acute Myocardial Infarction: How Good Is the Evidence Supporting Current Treatment Guidelines? Michael B. Fowler, MB, FRCP Beta-adrenergic blocking
Addressing the Gap in the Management of Patients After Acute Myocardial Infarction: How Good Is the Evidence Supporting Current Treatment Guidelines? Michael B. Fowler, MB, FRCP Beta-adrenergic blocking
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center
 Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center Beta-blockers: What s known 30 Years 30 Careers Physician clarity regarding
Beta-blockers: Now what? Annemarie Thompson, MD Assistant Professor of Anesthesia and Medicine Vanderbilt University Medical Center Beta-blockers: What s known 30 Years 30 Careers Physician clarity regarding
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Treatment of T Angina reatment of By Ali Alalawi
 Treatment of Angina By Ali Alalawi Determinants of Oxygen Demand Need to improve ratio of: Coronary blood flow / cardiac work Or Cardiac O2 Supply / Cardiac Requirement Coronary Circulation vs Other Circulation
Treatment of Angina By Ali Alalawi Determinants of Oxygen Demand Need to improve ratio of: Coronary blood flow / cardiac work Or Cardiac O2 Supply / Cardiac Requirement Coronary Circulation vs Other Circulation
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
100 mg atenolol equivalent to metoprolol
 100 mg atenolol equivalent to metoprolol Metoprolol is a selective beta-blocker at dosages usually prescribed to lower blood. For High Blood Pressure For 7 years I have been on 50 mg. of atenolol for.
100 mg atenolol equivalent to metoprolol Metoprolol is a selective beta-blocker at dosages usually prescribed to lower blood. For High Blood Pressure For 7 years I have been on 50 mg. of atenolol for.
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY
 CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
CHAPTER 12 HYPERTENSION IN SPECIAL GROUPS HYPERTENSION IN PREGNANCY v Mild preeclampsia is managed by close observation of the mother and fetus preferably in hospital. If the diastolic blood pressure remains
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes
 Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Beta-blockers in Patients with Mid-range Left Ventricular Ejection Fraction after AMI Improved Clinical Outcomes Seung-Jae Joo and other KAMIR-NIH investigators Department of Cardiology, Jeju National
Pharmacology. Drugs affecting the Cardiovascular system (Antianginal Drugs)
") Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Lecture 7 (year3) Dr Noor Al-Hasani Pharmacology University of Baghdad College of dentistry Drugs affecting the Cardiovascular system (Antianginal Drugs) Atherosclerotic disease of the coronary arteries,
Is there still a place for beta-blockers in perioperative cardioprotection?
 Is there still a place for beta-blockers in perioperative cardioprotection? 14 Michal Horacek Cardiovascular complications, such as hypertension or hypotension, myocardial infarction, left ventricular
Is there still a place for beta-blockers in perioperative cardioprotection? 14 Michal Horacek Cardiovascular complications, such as hypertension or hypotension, myocardial infarction, left ventricular
2008, American Heart Association. All rights reserved.
 AHA 2008 Cocaine-Associated Chest Pain and Myocardial Infarction Slide Set Based on the AHA 2008 Scientific Statement for Management of Cocaine-Associated Chest Pain and Myocardial Infarction George J.
AHA 2008 Cocaine-Associated Chest Pain and Myocardial Infarction Slide Set Based on the AHA 2008 Scientific Statement for Management of Cocaine-Associated Chest Pain and Myocardial Infarction George J.
Chapter 2 ~ Cardiovascular system
 Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Chapter 2 ~ Cardiovascular System: General Section 1 of 6 Chapter 2 ~ Cardiovascular system 2.1 Positive inotropic drugs 2.1.1 Cardiac glycosides DIGOXIN 2.2 Diuretics Elixir 50micrograms in 1ml Injection
Codes for a Medicare claims-based model to predict LVEF class- User Guide
 Description and citation: This guide accompanies our manuscript [Desai RJ, Lin KJ, Patorno E, et al. Development and Preliminary Validation of a Medicare Claims Based Model to Predict Left Ventricular
Description and citation: This guide accompanies our manuscript [Desai RJ, Lin KJ, Patorno E, et al. Development and Preliminary Validation of a Medicare Claims Based Model to Predict Left Ventricular
SMARTool clinical and biohumoral results. Chiara Caselli IFC-CNR
 SMARTool clinical and biohumoral results Chiara Caselli IFC-CNR SMARTool Flow chart EVINCI and ARTreat Populations SMARTool: WP1 and WP2 WP1 Objective: To collect retrospective EVINCI clinical and imaging
SMARTool clinical and biohumoral results Chiara Caselli IFC-CNR SMARTool Flow chart EVINCI and ARTreat Populations SMARTool: WP1 and WP2 WP1 Objective: To collect retrospective EVINCI clinical and imaging
7/21/2017. Learning Objectives. Current Cardiovascular Pharmacology. Epinephrine. Cardiotonic Agents. Epinephrine. Epinephrine. Arthur Jones, EdD, RRT
 Learning Objectives Current Cardiovascular Pharmacology Arthur Jones, EdD, RRT Explain the actions, effects, indications, adverse effects, & precautions for agents from the following drug categories Cardiotonic
Learning Objectives Current Cardiovascular Pharmacology Arthur Jones, EdD, RRT Explain the actions, effects, indications, adverse effects, & precautions for agents from the following drug categories Cardiotonic
Pharmacotherapy of Angina Pectoris
 Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
TRANSPARENCY COMMITTEE OPINION. 4 November 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 4 November 2009 RANEXA 375 mg extended release tablet Pack of 60 (CIP: 394 370-7) RANEXA 500 mg extended release tablet
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 4 November 2009 RANEXA 375 mg extended release tablet Pack of 60 (CIP: 394 370-7) RANEXA 500 mg extended release tablet
Optimal Adrenergic Blockades in Heart Failure. Jae-Joong Kim MD, PhD Asan Medical Center, University of Ulsan, Seoul, Korea
 Optimal Adrenergic Blockades in Heart Failure Jae-Joong Kim MD, PhD Asan Medical Center, University of Ulsan, Seoul, Korea Contents Harmful effects of adrenergic system in heart failure Clinical studies
Optimal Adrenergic Blockades in Heart Failure Jae-Joong Kim MD, PhD Asan Medical Center, University of Ulsan, Seoul, Korea Contents Harmful effects of adrenergic system in heart failure Clinical studies
Pharmacotherapy of Angina Pectoris
 Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Pharmacotherapy of Angina Pectoris Edward JN Ishac, Ph.D. Smith Building, Room 742 eishac@vcu.edu 828-2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia Commonwealth
Chapter / Section / Drug
 2 Cardiovascular System 2.1 Positive inotropic drugs Digoxin Digoxin specific antibody ( DigiFab ) 2.2 Diuretics 2.2.1 Thiazides and related diuretics Indapamide (1 st Line) Bendroflumethiazide Metolazone
2 Cardiovascular System 2.1 Positive inotropic drugs Digoxin Digoxin specific antibody ( DigiFab ) 2.2 Diuretics 2.2.1 Thiazides and related diuretics Indapamide (1 st Line) Bendroflumethiazide Metolazone
ST-elevation myocardial infarctions (STEMIs)
") Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Guidelines for Treating STEMI: Case-Based Questions As many as 25% of eligible patients presenting with STEMI do not receive any form of reperfusion therapy. The ACC/AHA guidelines highlight steps to improve
Adrenergic Receptor Antagonists
 Adrenergic Receptor Antagonists α-adrenergic Receptor Antagonists Unlike the β-adrenergic receptor antagonists, which bear clear structural similarities to the adrenergic agonists E, epinephrine, and isoproterenol,
Adrenergic Receptor Antagonists α-adrenergic Receptor Antagonists Unlike the β-adrenergic receptor antagonists, which bear clear structural similarities to the adrenergic agonists E, epinephrine, and isoproterenol,
β-blocker Use for the Stages of Heart Failure Mayo Clin Proc. August 2009;84(8):
:") REVIEW β-blocker USE FOR THE STAGES OF HF β-blocker Use for the Stages of Heart Failure MARC KLAPHOLZ, MD The 2005 American Heart Association/American College of Cardiology heart failure (HF) guidelines
REVIEW β-blocker USE FOR THE STAGES OF HF β-blocker Use for the Stages of Heart Failure MARC KLAPHOLZ, MD The 2005 American Heart Association/American College of Cardiology heart failure (HF) guidelines
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE
 June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
Case 1: A 76-year-old man was diagnosed with an
 CLINICIAN UPDATE -Blockers in the Post Myocardial Infarction Patient Mihai Gheorghiade, MD; Sidney Goldstein, MD Case 1: A 76-year-old man was diagnosed with an ST-segment elevation anterior wall myocardial
CLINICIAN UPDATE -Blockers in the Post Myocardial Infarction Patient Mihai Gheorghiade, MD; Sidney Goldstein, MD Case 1: A 76-year-old man was diagnosed with an ST-segment elevation anterior wall myocardial
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study
 Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Heart Failure and Cardiomyopathy Center, Division of Cardiology, North Shore University Hospital, Manhasset, NY
 NEUROHORMONAL ANTAGONISTS IN THE POST-MI PATIENT New Evidence from the CAPRICORN Trial: The Role of Carvedilol in High-Risk, Post Myocardial Infarction Patients Jonathan D. Sackner-Bernstein, MD, FACC
NEUROHORMONAL ANTAGONISTS IN THE POST-MI PATIENT New Evidence from the CAPRICORN Trial: The Role of Carvedilol in High-Risk, Post Myocardial Infarction Patients Jonathan D. Sackner-Bernstein, MD, FACC
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe