ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ
|
|
|
- Lisa Cox
- 6 years ago
- Views:
Transcription
1 ΥΠΕΡΤΑΣΗ ΚΑΙ ΣΤΕΦΑΝΙΑΙΑ ΝΟΣΟΣ Ι.Ε.ΚΑΝΟΝΙΔΗΣ
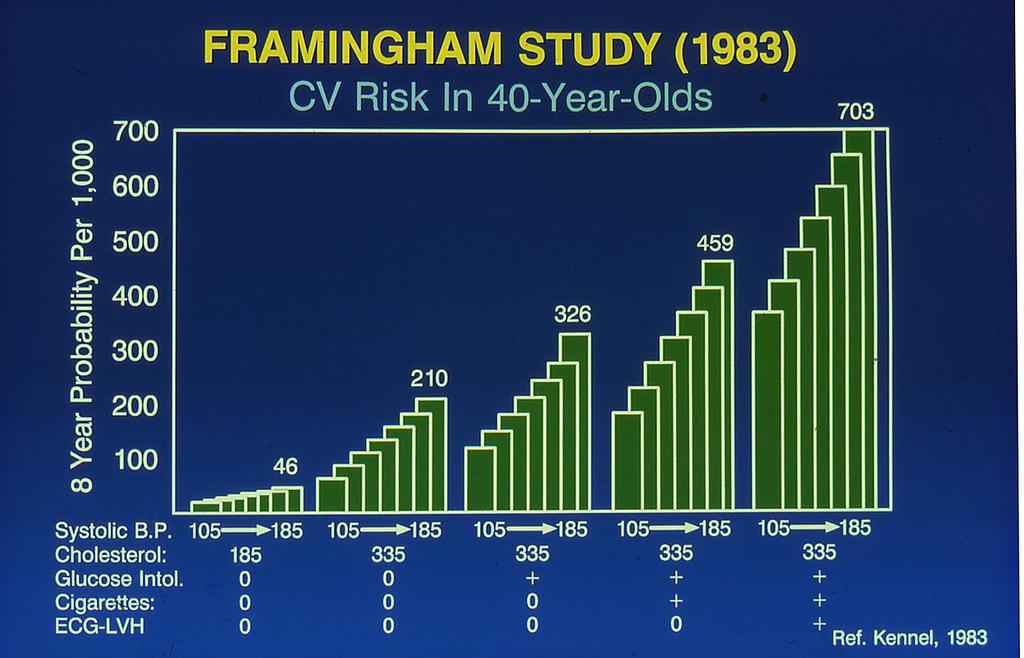
2 CAD: Statistics CAD is the largest killer of American males and females 13 million Americans have CAD 1.1 million MI s per year Every 26 seconds an American will suffer from a coronary event Every 60 seconds an American will die because of a coronary event 42% of those having a coronary event will die from it people die per year because of a coronary event in the Emergency Department before even being admitted to the hospital Death Rate in 2001: 177 in 100,000
3 CAD: Demographics and Statistics 84% of those who die from CAD are 65 or older Within 1 year of initial MI: 25% of men and 38% of women will die Within 8 years of initial MI: 50% of men and women under 65 will die An average of 11.5 years of life are lost due to an MI IMPORTANT: 50% of men and 64% of women who have died suddenly via CAD DID NOT HAVE ANY PREVIOUS SYMPTOMS Sudden Death: Those with a previous history of MI have a 5-6 times Sudden Death rate compared to the general population
4 Hypertension Hypertension( HTN) is the most common primary diagnosis in America. 35 million office visits are as the primary diagnosis of HTN. 50 million or more Americans have high BP. Worldwide prevalence estimates for HTN may be as much as 1 billion. 7.1 million deaths per year may be attributable to hypertension.
5 Ηypertension The estimated prevalence of hypertension in the United States in 2005 was : 35.3 million for men 38.3 million for women. Hypertension is more prevalent in black persons than in Hispanic and non-hispanic white persons. This prevalence is increasing. Data from and demonstrated an increased prevalence of hypertension in black individuals from 35.8% to 41.4%.
6 6 Hypertension: A Significant CV and Renal Disease Risk Factor Stroke CAD CHF LVH Renal disease Hypertension Peripheral vascular disease Morbidity Disability National High Blood Pressure Education Program Working Group. Arch Intern Med. 1993;153:
7 7
 70 74 <70 <120 120 139 140 159 160+ Systolic BP (mm Hg) Adapted from Neaton JD et al. Arch Intern Med.")
8 8 Hypertension and CHD : (MRFIT) SBP versus DBP in Risk of CHD Mortality CHD Death Rate Diastolic BP (mm Hg) <70 < Systolic BP (mm Hg) Adapted from Neaton JD et al. Arch Intern Med. 1992;152:56-64.

9 Biennial Age-Adjusted Rate per 1,000 9 Risk of Cardiovascular Events by Hypertensive Status 36-Year Follow-up in Patients Aged Years 50 Coronary Disease Stroke Peripheral Arterial 45.4 Disease Cardiac Failure Normotensive Hypertensive Men Women Men Women Men Women Men Women Reprinted with permission from Kannel WB. JAMA. 1996;275:
10 10 Elevated SBP Alone Is Associated With Increased Risk of Cardiovascular and Renal Disease Disease Relative Risk Kidney failure (ESRD) 2.8 Stroke 2.7 Heart failure 1.5 Peripheral vascular disease 1.8 Myocardial infarction* =1.6 Coronary artery disease 1.5 ESRD = end-stage renal disease; SBP 165 mm Hg. *Men only. Adapted from Kannel WB. Am J Hypertens. 2000;13:3S-10S; Perry HM Jr et al. Hypertension. 1995;25(part 1): ; Klag MJ et al. N Engl J Med. 1996;334:13-18; Nielsen WB et al. Ugeskr Laeger. 1996;158: ; Neaton JD et al. Arch Intern Med. 1992;152:56-64.
11
12 12 Benefits of Lowering BP Average Percent Reduction Stroke incidence 35 40% Myocardial infarction 20 25% Heart failure 50% TROPHY Study ACC 2006: Even lowering BP in those with pre-htn appears to reduce incidence of new HTN by up to 60%
13 INTERHEART study About 25% of the population-attributable risk of a myocardial infarction can be accounted for by hypertension
14 Pathophysiological Association of hypertension with IHD Atherogenesis Hypertrophy Endothelial dysfunction, which leads to the developement of atherosclerosis, Increased afterload leading to myocardial hypertrophy.
15 LVH The rate of LVH based on ECG findings 2.9% for men 1.5% for women. based on echocardiographic findings 15-20% 33% of patients without LVH have evidence of asymptomatic LV diastolicdysfunction.

16 ECG -Hypertension Electrocardiogram from a 46-year-old man with long-standing hypertension showing left atrial abnormality and left ventricular hypertrophy with strain.
17 17 Blood Pressure Classification BP Classification SBP mmhg DBP mmhg Normal <120 and <80 Prehypertension or Stage 1 HTN or Stage 2 HTN >160 or >100
18 BHS classification of blood pressure levels Category Systolic blood Diastolic blood pressure (mmhg) pressure Optimal blood pressure <120 <80 Normal blood pressure <130 <85 High-normal blood pressure Grade 1 Hypertension (mild) Grade 2 Hypertension (moderate) Grade 3 Hypertension (severe) >180 >110 Isolated Systolic Hypertension (Grade 1) <90 Isolated Systolic Hypertension (Grade 2) >160 <90

19 Total Cardiovascular risk in Hypertensive Patients

20 Treatment modalities in Hypertensive Patients
21 Non pharmacological Treatment of hypertension and lifestyle changes Lose weight, if overweight Increase physical activity Reduce salt intake Stop smoking Limit intake of foods rich in fats and cholesterol Increase consumption of fruits and vegetables Limit alcohol intake
22 Lifestyle Modification Modification Approximate SBP reduction (range) Weight reduction Adopt DASH eating plan Dietary sodium reduction Physical activity Moderation of alcohol consumption 5 20 mmhg / 10 kg weight loss 8 14 mmhg 2 8 mmhg 4 9 mmhg 2 4 mmhg
23 Drug therapy for hypertension Class of drug Example dose Initiating dose Usualmaintenance Diuretics Hydrochlorothiazide 12.5 mg o.d mg o.d. -blockers Atenolol mg o.d mg o.d. Calcium Amlodipine mg o.d mg o.d. channel blockers -blockers prazosin 2.5 mg o.d mg o.d. ACE- inhibitors ramipril mg o.d mg o.d. Angiotensin-II Losartan mg o.d mg o.d. receptor blockers
24 Pharmacological Treatment in Hypertension
25 J-Curve In favor Stewart Lancet 1979 Cruickshank et al Lancet 1987 Miller Hypertension 2000 Against Farnett et al JAMA 1991 McMahon et al Lancet 1990 J-Curve in HTN plus CAD INVEST TNT SMART
26 HOT Study: Significant Benefit From Intensive Treatment in the Diabetic Subgroup Major cardiovascular events/1,000 patient-years p=0.005 for trend Target Diastolic Blood Pressure mm Hg Hansson L et al. Lancet. 1998;351:
27 Recommendations. In patients with an elevated DBP and CAD with evidence of myocardial ischemia, the BP should be lowered slowly, and caution is advised in inducing decreases in DBP to <60 mm Hg in any patient with diabetes mellitus or who is >60 years of age. In older hypertensive individuals with wide pulse pressures, lowering SBP may cause very low DBP values (<60 mm Hg). This should alert the clinician to assess carefully any untoward signs or symptoms, especially those resulting from myocardial ischemia (Class Iia;Level of Evidence: C).
28
29
30 Best BP CAMELOT ACCORD SPRINT
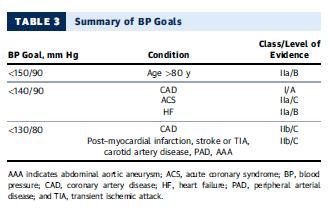
31 Recommendations 1. The <140/90-mm Hg BP target is reasonable for the secondary prevention of cardiovascular events in patients with hypertension and CAD (Class IIa; Level of Evidence: B). 2. A lower target BP (<130/80 mm Hg) may be appropriate in some individuals with CAD, previous MI, stroke or transient ischemic attack, or CAD risk equivalents (carotid artery disease, PAD, abdominal aortic aneurysm) (Class IIb; Level of Evidence: B).
32
33 Treatment of BP in pts with IHD Treatment of BP in primary prevention of IHD Treatment of BP in secondary prevention of IHD Treatment of BP in established IHD Treatment of BP in ACS
34 ΕΠΙΛΟΓΗ ΑΝΤΙΥΠΕΡΤΑΣΙΚΩΝ ΦΑΡΜΑΚΩΝ ΣΤΗΝ ΠΡΩΤΟΓΕΝΝΗ ΠΡΟΛΗΨΗ ΣΤΕΦΑΝΙΑΙΑΣ ΝΟΣΟΥ Δεν υπάρχει διαφορά μεταξύ των διαφόρων κατηγοριών αντιυπερτασικών φαρμάκων στην πρωτογενή πρόληψη, όσον αφορά την επίπτωση της στεφανιαίας νόσου και των καρδιαγγειακών επιπλοκών γενικώτερα.
35 ΕΠΙΛΟΓΗ ΑΝΤΙΥΠΕΡΤΑΣΙΚΩΝ ΦΑΡΜΑΚΩΝ ΣΤΗΝ ΔΕΥΤΕΡΟΓΕΝΝΗ ΠΡΟΛΗΨΗ ΣΤΕΦΑΝΙΑΙΑΣ ΝΟΣΟΥ B-blockers ACE Inhibitors ARBBs Diuretics CCB
36 Diuretics in secondary prevention THIAZIDES Veterans Administration MRC SHEP HYVET Chlorothalidone ALLHAT
37 ARBs VALUE OPTIMAAL VALIANT TRANSCEND
38 ACE Inhibitors in secondary prevention HOPE EUROPA PEACE ONTARGET
39 CCB ALLHAT amlodipine VS diuretic or ACE ASCOT amlodipine VS b-blockers CONNICLE verapamil VS b-blockers or diuretic INVEST verapamil VS NORDIL diltiazem VS b-blockers or diuretic
40 Recommendations I 1. Patients with hypertension and chronic stable angina should be treated with a regimen that includes: a) b-blocker in patients with a history of prior MI b) An ACE inhibitor or ARB if there is prior MI, LV systolic dysfunction, diabetes mellitus, or CKD; and c) A thiazide or thiazide-like diuretic (Class I; Level of Evidence: A). 2. The combination of a b-blocker, an ACE inhibitor or ARB, and a thiazide or thiazide-like diuretic should also be considered in the absence of a prior MI, LV systolic dysfunction, diabetes mellitus, or proteinuric CKD (Class IIa; Level of Evidence: B). 3. If b-blockers are contraindicated or produce intolerable side effects, a nondihydropyridine CCB (such as diltiazem or verapamil) may be substituted, but not if there is LV dysfunction (Class IIa; Level of Evidence: B).
41 Recommendations II 4. If either the angina or the hypertension remains uncontrolled, a long-acting dihydropyridine CCB can be added to the basic regimen of b-blocker, ACE inhibitor, and thiazide or thiazide-like diuretic. The combination of a b-blocker and either of the nondihydropyridine CCBs (diltiazem or verapamil) should be used with caution in patients with symptomatic CAD and hypertension because of the increased risk of significant bradyarrhythmias and HF (Class IIa; Level of Evidence: B). 5. For patients with stable angina, the BP target is <140/ 90 mm Hg. (Class I; Level of Evidence: A) A lower target BP (<130/80 mm Hg) may be considered in some individuals with CAD, with previous stroke or transient ischemic attack, or with CAD risk equivalents (carotid artery disease, PAD, abdominal aortic aneurysm) (Class IIb; Level of Evidence: B)..
42 Antiplatelet or Anticoagulant drugs 6. There are no special contraindications in hypertensive patients for the use of antiplatelet or anticoagulant drugs, except that in patients with uncontrolled severe hypertension who are taking antiplatelet or anticoagulant drugs, the BP should be lowered without delay to reduce the risk of hemorrhagic stroke (Class IIa; Level of Evidence: C).
43 ΕΠΙΛΟΓΗ ΑΝΤΙΥΠΕΡΤΑΣΙΚΩΝ ΦΑΡΜΑΚΩΝ ΣΤΑ ΟΞΕΑ ΙΣΧΑΙΜΙΚΑ ΣΥΝΔΡΟΜΑ B-blockers ACE Inhibitors ARBBs Diuretics Nitates
44 ACE inhibitors in ACS GISSI 3 ISSIS 4 CCS 1 ACE inh post ACS
45 . Recommendations 1. If there is no contraindication to the use of b-blockers, in patients with ACS, the initial therapy of hypertension should include a short-acting b1-selective b-blocker without intrinsic sympathomimetic activity (metoprolol tartrate or bisoprolol). b-blocker therapy should typically be initiated orally within 24 hours of presentation (Class I; Level of Evidence: A). For patients with severe hypertension or ongoing ischemia, an intravenous b-blocker (esmolol) can be considered (Class IIa; Level of Evidence: B). For hemodynamically unstable patients or when decompensated HF exists, the initiation of b-blocker therapy should be delayed until stabilization has been achieved (Class I; Level of Evidence: A).
46 2. In patients with ACS and hypertension, nitratesshould be considered to lower BP or to relieve ongoing ischemia or pulmonary congestion (Class I; Level of Evidence: C). Nitrates should be avoided in patients with suspected right ventricular infarction and inthose with hemodynamic instability. Sublingual or intravenous nitroglycerin is preferred for initial therapy and can be transitioned later to a longeracting preparation if indicated.
47 3. If there is a contraindication to the use of a b-blocker or intolerable side effects, then a nondihydropyridine CCB such as verapamil or diltiazem may be substituted for patients with ongoing ischemia, provided that LV dysfunction or HF is not present. If the angina or hypertension is not controlled on a b-blocker alone, a longer-acting dihydropyridine CCB may be added after optimal use of an ACE inhibitor (Class IIa; Level of Evidence: B). 4. An ACE inhibitor (Class I; Level of Evidence: A) or an ARB (Class I; Level of Evidence: B) should be added if the patient has an anterior MI, if hypertension persists, if the patient has evidence of LV dysfunction or HF, or if the patient has diabetes mellitus. For lowerrisk ACS patients with preserved LV ejection fraction and no diabetes mellitus, ACE inhibitors can be considered a first-line agent for BP control (Class IIa; Level of Evidence: A).
48 5. Aldosterone antagonists are indicated for patients who are already receiving b- blockers and ACE inhibitors after MI and have LV dysfunction and either HF or diabetes mellitus. Serum potassium levels must be monitored. These agents should be avoided in patients with elevated serum creatinine levels ( 2.5 mg/dl in men, 2.0 mg/dl in women) or elevated potassium levels ( 5.0 meq/l) (Class I; Level of Evidence: A). 6. Loop diuretics are preferred over thiazide and thiazide-type diuretics for patients with ACS who have HF (NYHA class III or IV) or for patients with CKD and an estimated glomerular filtration rate <30 ml/min. For patients with persistent hypertension not controlled with a b-blocker, an ACE inhibitor, and an aldosterone antagonist, a thiazide or thiazide-type diuretic may be added in selected patients for BP control (Class I; Level of Evidence: B). 7. The target BP is <140/90 mm Hg in patients with ACS who are hemodynamically stable (Class IIa; Level ofevidence: C). A BP target of <130/80 mm Hg at the time of hospital discharge is a reasonable option (Class IIb;Level of Evidence: C). The BP should be lowered slowly, and caution is advised to avoid decreases in DBP to <60 mm Hg because this may reduce coronary perfusion and worsen ischemia.
49 ΕΥΧΑΡΙΣΤΩ
SBP in range of 120 to 140 :no progression or regression of CAD. Sipahi et al., 2006
 Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
Management of Hypertension in Patients with CAD M. Mohsen Ibrahim, MD Cardiology Department- Cairo University 1. What is the optimal BP in patients with hypertension and CAD? 2. What is the minimum safe
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Prevention of Cardiovascular Events in Hypertension and CAD & Management of Hypertension in HF of Ischemic origin
 "Insight Heart" is also available at www.squarepharma.com.bd Vol: 911 No: 4; 4; 2012 2015 Prevention of Cardiovascular Events in Hypertension and CAD Drug-eluting & Management of Hypertension in HF of
"Insight Heart" is also available at www.squarepharma.com.bd Vol: 911 No: 4; 4; 2012 2015 Prevention of Cardiovascular Events in Hypertension and CAD Drug-eluting & Management of Hypertension in HF of
Μαρία Μαρκέτου Επιμ. Α Καρδιολογική Κλινική ΠαΓΝΗ
 Μαρία Μαρκέτου Επιμ. Α Καρδιολογική Κλινική ΠαΓΝΗ Ischemic Heart Disease Mortality Rate in Each Decade of Age IHD mortality (floating absolute risk and 95% CI) 256 128 64 32 16 8 4 2 SBP 256 128 64 32
Μαρία Μαρκέτου Επιμ. Α Καρδιολογική Κλινική ΠαΓΝΗ Ischemic Heart Disease Mortality Rate in Each Decade of Age IHD mortality (floating absolute risk and 95% CI) 256 128 64 32 16 8 4 2 SBP 256 128 64 32
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017
 Clinician Guide SEPTEMBER 2017") Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Coronary Artery Disease (CAD) Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide is based on the 2017 KP National Coronary Artery Disease
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Cardiovascular Health Practice Guideline Outpatient Management of Coronary Artery Disease 2003
 Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
Authorized By: Medical Management Guideline Committee Approval Date: 12/13/01 Revision Date: 12/11/03 Beta-Blockers Nitrates Calcium Channel Blockers MEDICATIONS Indicated in post-mi, unstable angina,
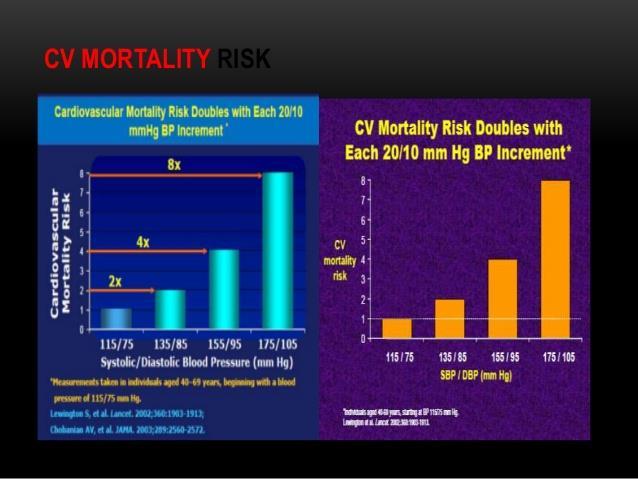
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Individual management of arterial hypertension. Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki
 Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Individual management of arterial hypertension Doumas Michael, Internist Lecturer, Aristotle University, Thessaloniki From Population to Individual Management of Arterial Hypertension Epidemiologic impact
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
What is hypertension?
 HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
HYPERTENSION What is hypertension? Abnormally elevated arterial blood pressure that is usually indicated by an adult systolic blood pressure of 140 mm Hg or greater or a diastolic blood pressure of 90
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
In the Literature 1001 BP of 1.1 mm Hg). The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi
. The trial was stopped early based on prespecified stopping rules because of a significant difference in cardi") Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
Is Choice of Antihypertensive Agent Important in Improving Cardiovascular Outcomes in High-Risk Hypertensive Patients? Commentary on Jamerson K, Weber MA, Bakris GL, et al; ACCOMPLISH Trial Investigators.
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Hypertension and CAD. Dr. Vinod Sharma. National Heart Institute New Delhi
 Hypertension and CAD Dr. Vinod Sharma National Heart Institute New Delhi Case History 1 AB 82 years female with - Hypertension 7 yrs treated with ACE inhibitors & Amlodipine, BP fluctuating between 160
Hypertension and CAD Dr. Vinod Sharma National Heart Institute New Delhi Case History 1 AB 82 years female with - Hypertension 7 yrs treated with ACE inhibitors & Amlodipine, BP fluctuating between 160
TREATMENT OF HYPERTENSION
 TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
TREATMENT OF HYPERTENSION Aim of treatment BP Goals Main items of treatment Lifestyle modification When to start drug Rx Pharmacological therapy 1. Relief of symptoms 2. Prevention of complications and
How clinically important are the results of the large trials in hypertension?
 How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
How clinically important are the results of the large trials in hypertension? Stéphane LAURENT, MD, PhD, FESC Pharmacology Department and PARCC / INSERM U970 Hôpital Européen Georges Pompidou, Université
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist. Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI
 Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
Medical Management of Acute Coronary Syndrome: The roles of a noncardiologist physician Norbert Lingling D. Uy, MD Professor of Medicine UERMMMCI Outcome objectives of the discussion: At the end of the
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
7/6/2012. University Pharmacy 5254 Anthony Wayne Drive Detroit, MI (313)
") University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Management of The Patients with Hypertension and High Risk Cardiovascular Disease
 Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Management of The Patients with Hypertension and High Risk Cardiovascular Disease Songsak Kiatchoosakun, MD. Cardiology, Medicine Khon Kaen University CVD and Hypertension: Worldwide Morbidity and Mortality
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study
 Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
Identification of patients with heart failure and PREserved systolic Function : an Epidemiologic Regional study Dr. Antonio Magaña M.D. (on behalf I-PREFER investigators group) Stockholm, Sweden, August
BLOOD PRESSURE-LOWERING TREATMENT
 BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
BLOOD PRESSURE-LOWERING TRIALS NUMBER OF PARTICIPANTS NUMBER OF PERCENTAGE OF MEAN AGE MEAN - (YEARS) TRIALS WITH ANALYSIS BY GENDER N, (%) 69,473 28,008 40.3% 70.2 3.2 3/5 (60%) APPENDIX 2 1 BLOOD PRESSURE-LOWERING
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Clinical Recommendations: Patients with Periodontitis
 The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
The American Journal of Cardiology and Journal of Periodontology Editors' Consensus: Periodontitis and Atherosclerotic Cardiovascular Disease. Friedewald VE, Kornman KS, Beck JD, et al. J Periodontol 2009;
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Υπέρταση στις γυναίκες
 Υπέρταση στις γυναίκες Ελένη Τριανταφυλλίδη Διευθύντρια ΕΣΥ Καρδιολογίας Υπεύθυνη Αντιυπερτασικού Ιατρείου Β Πανεπιστημιακή Καρδιολογική Κλινική Νοσοκομείο ΑΤΤΙΚΟΝ Cardiovascular disease is the Europe
Υπέρταση στις γυναίκες Ελένη Τριανταφυλλίδη Διευθύντρια ΕΣΥ Καρδιολογίας Υπεύθυνη Αντιυπερτασικού Ιατρείου Β Πανεπιστημιακή Καρδιολογική Κλινική Νοσοκομείο ΑΤΤΙΚΟΝ Cardiovascular disease is the Europe
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
How Low Do We Go? Update on Hypertension
 How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
How Low Do We Go? Update on Beth L. Abramson, MD, FRCPC, FACC As presented at the University of Toronto s Saturday at the University Session (September 2003) Arecent World Health Organization report states
Hypertension is a major risk factor for
 OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of